Introduction
Intraductal tubulopapillary neoplasm (ITPN) is a
rare type of epithelial neoplasm of the pancreas that is
characterized by an intraductal, grossly visible, tubule-forming
epithelial neoplasm with cellular dysplasia and ductal
differentiation without overt mucin production (1). To the best of our knowledge, ITPN-like
intraductal neoplasm was first recognized by Japanese investigators
in the mid 1990s and was studied in 2009 by Yamaguchi et al
(2). Following these reports, ITPN
was adopted by the World Health Organization (WHO) classification,
which was revised in 2010, as a subclass of intraductal neoplasms
of the pancreas, along with intraductal papillary mucinous neoplasm
(IPMN). It is estimated that ITPNs account for <1% of all
pancreatic exocrine tumor cases and 3% of all pancreatic
intraductal neoplasm cases (2). Due
to the rarity of ITPN, information regarding the disease is
currently limited, and only a few reports, case series and reviews
are available (2,3); thus, the clinicopathological features of
ITPN remain to be elucidated. In this context, even a case report
of ITPN is essential for further characterizing this disease in
order to improve the management and treatment of patients with
ITPN. In this report we present a case of pancreatic ITPN with
associated invasive cancer that was successfully treated with total
pancreatectomy.
Case report
A 74-year-old male was admitted to the Departments
of Surgery, Toyonaka Municipal Hospital (Osaka, Japan) for
treatment of a pancreatic tumor. The patient's medical history
included alcoholic acute pancreatitis, a renal stone and cerebral
infarction. The patient did not exhibit any significant findings on
physical examination. The laboratory analysis results were within
the normal range, with the exception of the serum glucose level
(155 mg/dl; normal range 60–110 mg/dl) and HbA1c-NGSP (7.0%; normal
range 4.6–6.2%), which were elevated. The levels of various tumor
markers were within the normal range, including carcinoembryonic
antigen (2.8 ng/ml; normal range, <5.0 mg/dl), cancer antigen
19-9 (15 U/ml; normal range, <37 U/ml), s-pancreas-1 antigen
(8.6 U/ml; normal range, <30 U/ml) and duke pancreatic
monoclonal antigen type 2 (46 U/ml; normal range, <150 U/ml),
and the serum IgG4 level was also normal (42.8 mg/dl; normal range,
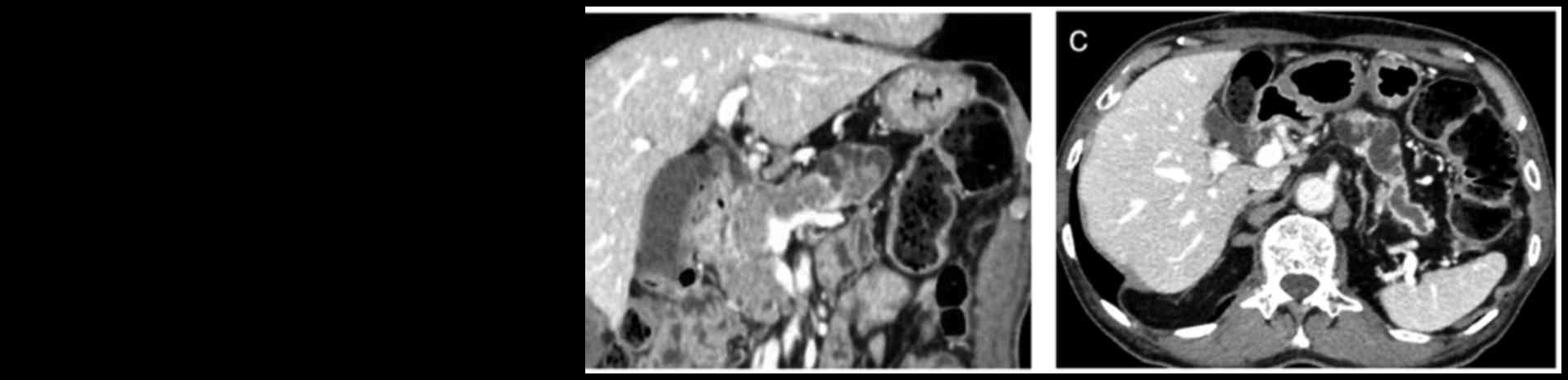
4.8–105 mg/dl). Contrast-enhanced computed tomography (CT) revealed
a mass with small cystic lesions in the pancreatic head and body
that exhibited a non-uniform contrast effect (Fig. 1A and B). The main pancreatic duct at
the peripheral side of the mass was dilated to 18 mm (Fig. 1C). Although the patient was not
jaundiced, the lower common bile duct was surrounded by the mass,
which was in contact with the portal vein and the superior
mesenteric vein. There were no visibly enlarged lymph nodes.
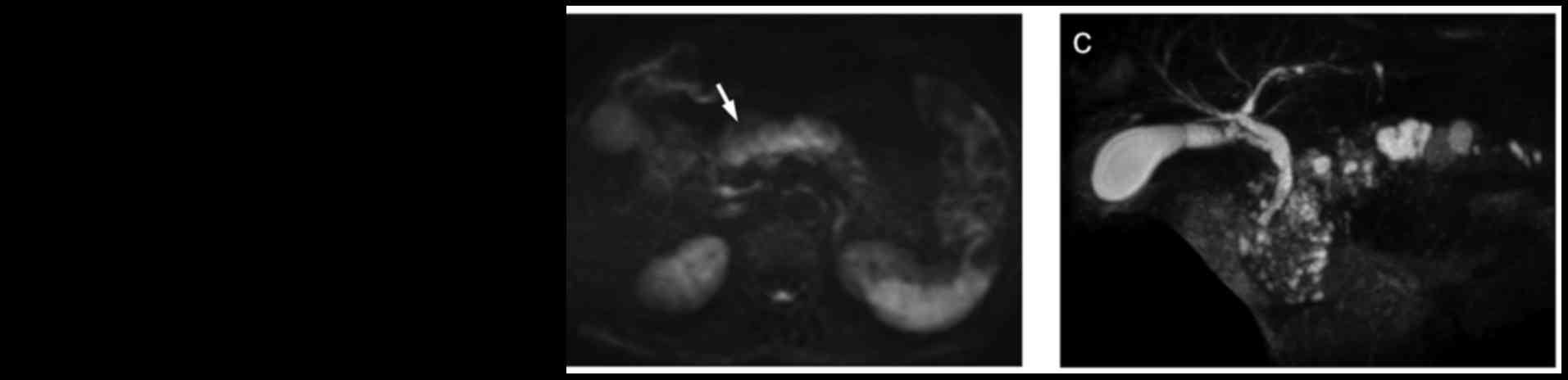
Magnetic resonance imaging (MRI), as with CT, revealed small cystic
lesions in the mass on T2-weighted images (Fig. 2A). The mass in the pancreatic head and
body was visualized with high signal intensity on
diffusion-weighted images (Fig. 2B).
On MR cholangiopancreatography (MRCP), there were small cystic
lesions present in the mass and dilatation of the main pancreatic
duct from the pancreatic body to the tail (Fig. 2C). Upper gastrointestinal endoscopy
revealed rough mucosa near the opening of the accessory pancreatic
duct and no mucus was observed (Fig.
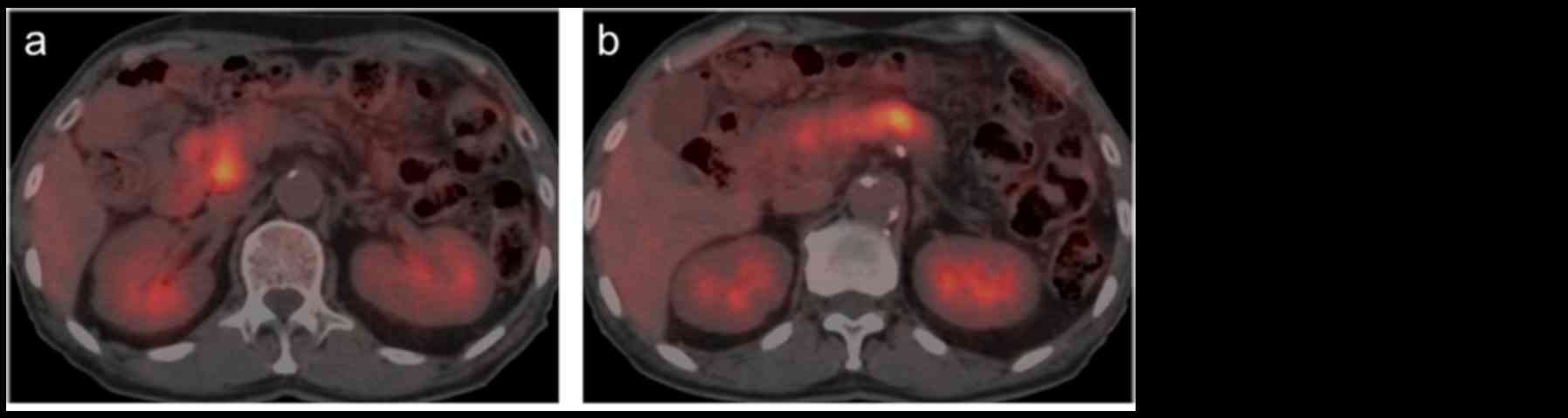
3A). Biopsy of the mucosa revealed adenocarcinoma. An
18F-fluorodeoxyglucose (FDG)-positron emission tomography scan
revealed abnormal FDG uptake with a maximum standardized uptake
value of 4.9 for the mass (Fig. 3B).
Based on the aforementioned findings, the pre-operative diagnosis
was pancreatic ITPN with associated cancer lesions. Although IPMN
was also considered as another possible differential diagnosis of
the mass, this diagnosis was rejected due to the lack of mucous
secretion identified. A laparotomy using an upper and middle
abdominal median incision was performed under general anesthesia.
The whole pancreas was hard, likely due to the patient's previous
pancreatitis. As the mass was located in the entire pancreatic head
and body, an attempt was made to resect the pancreas on the tail
side of the mass, in order to preserve the pancreatic tail.
However, it was problematic to separate the pancreatic body and the
splenic artery and vein, due to the tissue hardness. Therefore, it
was judged to be impossible to preserve the spleen, and a total
pancreatectomy with splenectomy was subsequently performed.
Lymphadenectomy was performed for dissecting regional lymph nodes.
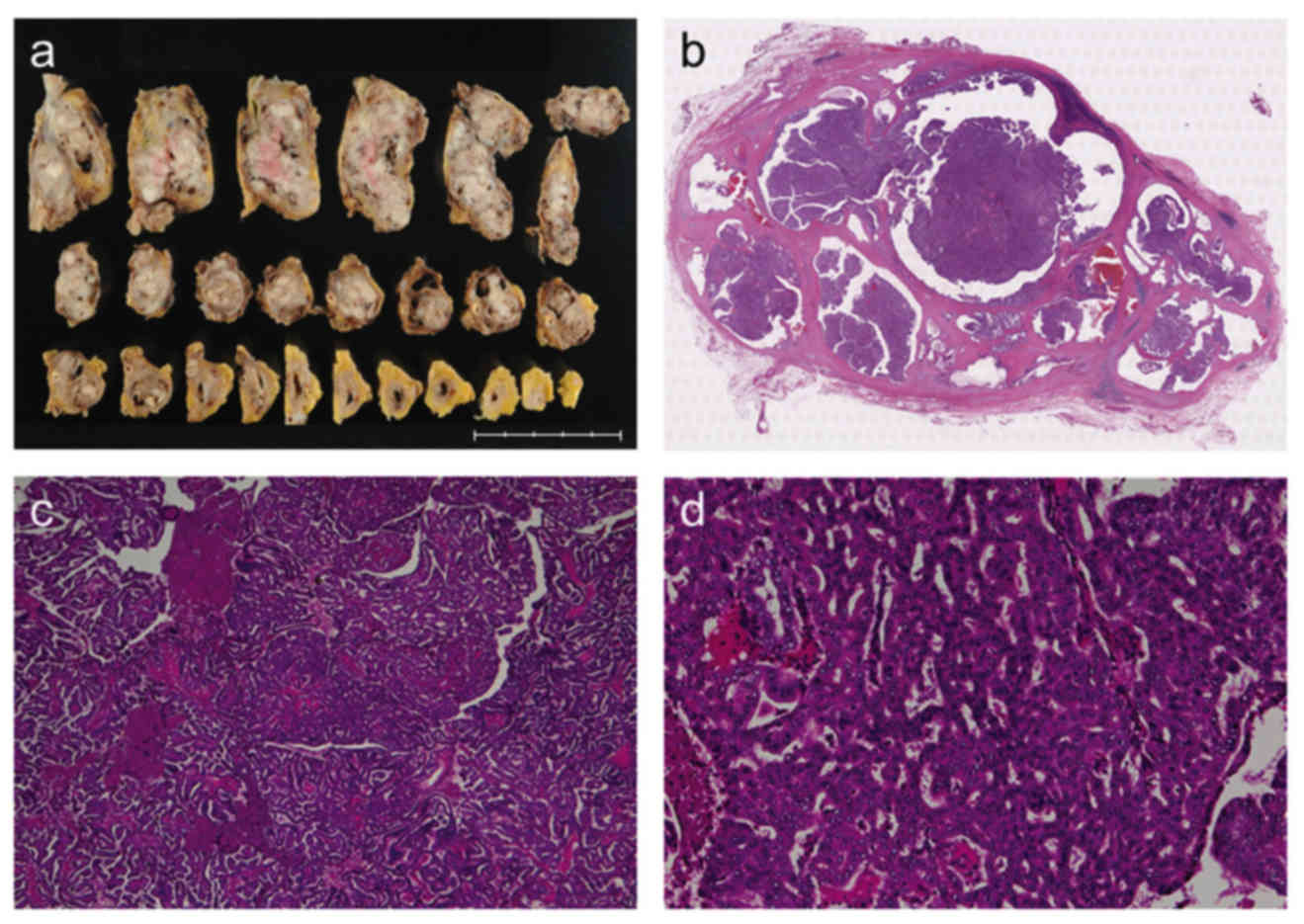
Macroscopic examination of the resected specimen indicated an
off-white solid tumor occupying the entire pancreas with
intraductal growth of the main pancreatic duct; mucin was not
identified (Fig. 4A and B).
Histological examination using hematoxylin and eosin staining
revelaed that the tumor exhibited high-grade dysplastic cells in a
tubulopapillary growth pattern without the overt production of
mucin (Fig. 4C and D). The tumor had
infiltrated the main pancreatic duct, although the pre-operative CT
scan had not revealed any tumors in the main pancreatic duct of the
pancreatic tail. The tumor had invaded beyond this to the entire
pancreatic parenchyma and serosal invasion and retroperitoneal
invasion were observed, whereas vascular invasion was not
identified. Among 30 lymph nodes dissected, metastasis was verified
to be present in two lymph nodes. The metastases were also
identified in the lymph nodes along the common hepatic artery and
the splenic artery. No cancer cells were identified in the resected
cut end margin of bile duct or dissected peripancreatic tissue.
Immunohistochemical staining was positive for cytokeratin (CK)7
(Roche Diagnostics, Basel, Switzerland), CK19 (Leica Microsystems,
Ltd., Milton Keynes, UK) and mucin (MUC1) (Leica Microsystems
Ltd.), and negative for MUC2 (Leica Microsystems, Ltd.), MUC5AC
(Leica Microsystems, Ltd.), MUC6 (Leica Microsystems, Ltd.) and
caudal type homeobox 2 (Biocare Medical, LLC., Concord, CA, USA;
Fig. 5). The final diagnosis was
determined to be pancreatic ITPN with associated invasive cancer.
The patient progressed without post-operative complications.
Following the surgery, the serum glucose levels were managed with
subcutaneous insulin injections. At the time of this report (9
months post-surgery), the patient remains disease-free without
evidence of recurrence, and is being followed on an outpatient
basis (follow-up is ongoing for 5-years).
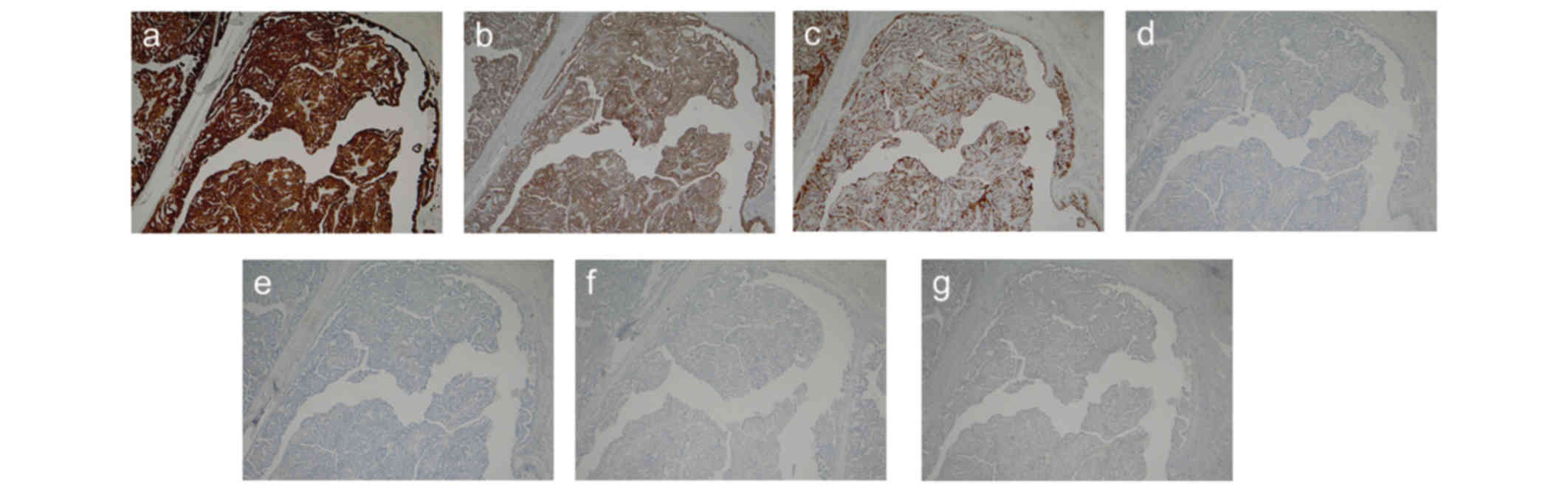 | Figure 5.Immunohistochemical staining of the
tumor. The tumor was immunohistochemically stained for (A) CK7, (B)
CK19, (C) MUC1, (D) MUC2, (E) MUC5AC, (F) MUC6 and (G) CDX2. The
staining was positive for CK7, CK19 and MUC1, and negative for
MUC2, MUC5AC, MUC6 and CDX2. CK, cytokeratin; MUC, mucin; CDX2,
caudal type homeobox 2. |
Discussion
Yamaguchi et al (2) reported 10 cases of pancreatic
intraductal neoplasms with predominantly tubular growth patterns
and a papillary component, and determined the neoplasm to be ITPN
of the pancreas. To the best of our knowledge, that was the first
report of ITPN. Intraductal neoplasms were classified as an IPMN or
ITPN in the 2010 WHO classification (1). ITPN is rare, accounting for <1% of
all pancreatic exocrine neoplasms and, to the best of our
knowledge, there has been only one case series of patients with
ITPN since the initial report by Yamaguchi et al (2). Date et al (3) recently analyzed the published data of 58
cases of ITPN, including their own case. In this study, they
searched MEDLINE and Igakuchuo-Zacchi (a database of Japanese
articles with English abstracts) for cases since 1980. The term
ITPN was first introduced by Yamaguchi et al (2) in 2009; although, cases reported prior to
2009 were included in the study. This suggests that the diagnosis
of ITPN in the cases reported prior to the definition may not be
accurate, as the authors noted in the report. Therefore, in the
present study, ITPN cases that had been reported in detail
following the definition in 2009 were searched for, and only cases
where the term ITPN was stated in the diagnosis were extracted.
Overall, 30 cases were extracted (2,3–20). The clinicopathological features of 31
cases, including the extracted 30 cases and the current case, are
presented in Table I. Among these 31
cases, 19 and 12 occurred in men and women, respectively. The age
range of the patients involved was 35–80 years, with a median age
at diagnosis of 66 years. The most frequently reported symptom was
abdominal pain, but there were also asymptomatic cases. Among the
31 patients, 29 patients had received surgery. The surgical
procedure was pancreaticoduodenectomy in 16 patients, distal
pancreatectomy in 8 patients and total pancreatectomy in 5
patients. Postoperatively, the overall 1-, 3- and 5-year survival
rates were all 92.3%. The summary of the clinicopathological
features of the 31 cases is similar to that reported by Date et
al (3). In addition, regardless
of the presence of the invasive component in the ITPN area, all of
the cases had associated cancer lesions. Therefore, all the cases
were intraductal tubulopapillary cancer with or without an invasive
component. There were no cases with intraductal tubulopapillary
adenoma. This finding suggests ITPN cases are not similar to IPMN
cases. The 2010 WHO classification categorizes IPMN cases according
to their malignant transformation into IPMN with low or
intermediate dysplasia, IPMN with high-grade dysplasia and IPMN
with invasive cancer (1). One
limitation was that a dedicated pathologist did not perform the
histopathological diagnosis in the 31 cases; thus, this
characteristic of ITPN must be validated in further and larger
studies. In conclusion, the current study presents a case of ITPN
with associated invasive cancer successfully treated with total
pancreatectomy. Further characterization of ITPN based on a
collection of cases, similar to that reported here, may lead to
improved management of this type of neoplasm.
 | Table I.Reported cases of intraductal
tubulopapillary neoplasm of the pancreas. |
Table I.
Reported cases of intraductal
tubulopapillary neoplasm of the pancreas.
| No. | Authors | Year | Age | Gender | Symptom | Location | Size (cm) | Invasion | Surgical
Procedure | Postoperative
survival (months) | Outcome | (Refs.) |
|---|
| 1 | Yamaguchi et
al | 2009 | 60 | F | None | H | 6.0 | − | PD | 19 | Mortality due to
other diseases | (2) |
| 2 | Yamaguchi et
al | 2009 | 35 | F | Abdominal pain | B | 1.0 | − | DP | 72 | Alive without
recurrence | (2) |
| 3 | Yamaguchi et
al | 2009 | 68 | F | None | H | 2.5 | − | PD | 29 | Alive without
recurrence | (2) |
| 4 | Yamaguchi et
al | 2009 | 53 | M | Abdominal pain | B | 2.0 | − | DP | 36 | Alive without
recurrence | (2) |
| 5 | Yamaguchi et
al | 2009 | 60 | F | Abdominal pain | H | 4.5 | − | PD | 24 | Alive without
recurrence | (2) |
| 6 | Yamaguchi et
al | 2009 | 73 | F | None | H | 5.2 | − | PD | 33 | Alive without
recurrence | (2) |
| 7 | Yamaguchi et
al | 2009 | 72 | M | None | B | 1.0 | + | DP | 33 | Alive without
recurrence | (2) |
| 8 | Yamaguchi et
al | 2009 | 44 | M | Abdominal pain | H | 6.0 | + | PD | 72 | Alive without
recurrence | (2) |
| 9 | Yamaguchi et
al | 2009 | 48 | M | Jaundice | HBT | 15.0 | + | TP | 7 | Disease-associated
mortality | (2) |
| 10 | Yamaguchi et
al | 2009 | 70 | M | Exacerbation of
diabetes mellitus | HB | 4.0 | − | PD | 24 | Alive without
recurrence | (2) |
| 11 | Bhuva et
al | 2011 | 50 | M | Abdominal pain,
jaundice, Anemia | H | NA | + | PD | 28 | Alive with
recurrence | (4) |
| 12 | Jokoji et
al | 2012 | 68 | M | Abdominal pain | BT | 10.0 | + | DP | 15 | Alive without
recurrence | (5) |
| 13 | Urata et
al | 2012 | 78 | F | None | BT | 2.2 | + | DP | 43 | Alive with
recurrence | (6) |
| 14 | Tajiri et
al | 2012 | 66 | M | Appetite loss | H | NA | − | PD | 12 | Alive without
recurrence | (7) |
| 15 | Guan et
al | 2012 | 41 | F | None | H | 2.3 | − | PD | NA | NA | (8) |
| 16 | Kasugai et
al | 2013 | 69 | F | Excessive
thirst | HBT | 12.0 | + | TP | 24 | Alive without
recurrence | (9) |
| 17 | Furuhata et
al | 2013 | 74 | M | Fever | H | 7.0 | + | NA | NA | NA | (10) |
| 18 | Someya et
al | 2014 | 74 | M | Fever | H | 7.0 | + | PD | 24 | Alive without
recurrence | (11) |
| 19 | Del chiaro et
al | 2014 | 78 | M | Abdominal pain | HBT | 1.1 | − | TP | NA | NA | (12) |
| 20 | Ahls et
al | 2014 | 43 | F | Abdominal pain | H | 2.6 | − | PD | 24 | Alive without
recurrence | (13) |
| 21 | Zhao et
al | 2014 | 48 | M | Abdominal pain | B | 1.3 | − | DP | NA | NA | (14) |
| 22 | Takayama et
al | 2015 | 54 | F | Severe
diarrhea | H | 5.0 | + | PD | 10 | Alive without
recurrence | (15) |
| 23 | Yoshida et
al | 2015 | 75 | M | None | H | 1.2 | − | PD | NA | NA | (16) |
| 24 | Kitaguchi et
al | 2015 | 61 | M | None | H | 1.2 | + | PD | 22 | Alive without
recurrence | (17) |
| 25 | Kitaguchi et
al | 2015 | 75 | F | None | B | 10.0 | + | DP | 51 | Alive without
recurrence | (17) |
| 26 | Kitaguchi et
al | 2015 | 67 | M | Anemia | HBT | 6.5 | + | TP | 84 | Alive without
recurrence | (17) |
| 27 | Matthews et
al | 2015 | 55 | M | Abdominal pain | T | 10.0 | + | DP | 36 | Alive with
recurrence | (18) |
| 28 | Kölby et
al | 2015 | 42 | M | Abdominal pain | HBT | 3.5 | + | PD | 19 | Alive without
recurrence | (19) |
| 29 | Tajima et
al | 2015 | 80 | M | NA | HB | 0.5 | NA | NA | 12 | Alive without
recurrence | (20) |
| 30 | Date et
al | 2016 | 54 | F | Abdominal pain | H | 5.5 | + | PD | 24 | Alive without
recurrence | (3) |
| 31 | Present case | 2016 | 74 | M | Weight loss | HBT | 17.5 | + | TP | 9 | Alive without
recurrence |
|
References
|
1
|
Adsay NV, Fukushima N, Furukawa T, Hruban
RH, Klimstra DS, Klöppel G, et al: Intraductal neoplasms of the
pancreasWorld Health Organization Classification of Tumours of the
Digestive System. Bosman FT, Carneiro F, Hruban RH and Theise ND:
4th. IARC; Lyon, France: pp. 304–313. 2010;
|
|
2
|
Yamaguchi H, Shimizu M, Ban S, Koyama I,
Hatori T, Fujita I, Yamamoto M, Kawamura S, Kobayashi M, Ishida K,
et al: Intraductal tubulopapillary neoplasms of the pancreas
distinct from pancreatic intraepithelial neoplasia and intraductal
papillary mucinous neoplasms. Am J Surg Pathol. 33:1164–1172. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Date K, Okabayashi T, Shima Y, Iwata J,
Sumiyoshi T, Kozuki A, Morita S, Hata Y, Noda Y, Nishioka A and
Matsumoto M: Clinicopathological features and surgical outcomes of
intraductal tubulopapillary neoplasm of the pancreas: A systematic
review. Langenbecks Arch Surg. 401:439–447. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bhuva N, Wasan H, Spalding D, Stamp G and
Harrison M: Intraductal tubulopapillary neoplasm of the pancreas as
a radiation induced malignancy. BMJ Case Rep pii. bcr0920114777.
2011. View Article : Google Scholar
|
|
5
|
Jokoji R, Tsuji H, Tsujimoto M, Shinno N
and Tori M: Intraductal tubulopapillary neoplasm of pancreas with
stromal osseous and cartilaginous metaplasia; a case report. Pathol
Int. 62:339–343. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Urata T, Naito Y, Nagamine M, Izumi Y,
Tonaki G, Iwasaki H, Sasaki A, Yamasaki A, Minami N, Yoshioka R, et
al: Intraductal tubulopapillary neoplasm of the pancreas with
somatic BRAF mutation. Clin J Gastroenterol. 5:413–420. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tajiri T, Tate G, Matsumoto K, Hoshino H,
Iwamura T, Kodaira Y, Takahashi K, Ohike N, Kunimura T, Mitsuya T
and Morohoshi T: Diagnostic challenge: Intraductal neoplasms of the
pancreatobiliary system. Pathol Res Pract. 208:691–696. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Guan H, Gurda G, Lennon AM, Hruban RH and
Erozan YS: Intraductal tubulopapillary neoplasm of the pancreas on
fine needle aspiration: Case report with differential diagnosis.
Diagn Cytopathol. 42:156–160. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kasugai H, Tajiri T, Takehara Y, Mukai S,
Tanaka J and Kudo SE: Intraductal tubulopapillary neoplasms of the
pancreas: Case report and review of the literature. J Nippon Med
Sch. 80:224–229. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Furuhata A, Minamiguchi S, Mikami Y,
Kodama Y, Sumiyoshi S, Adachi S and Haga H: Intraductal
tubulopapillary neoplasm with expansile invasive carcinoma of the
pancreas diagnosed by endoscopic ultrasonography-guided fine needle
aspiration: A case report. Diagn Cytopathol. 42:314–320. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Someya Y, Nakamoto Y, Nakatani K,
Kawaguchi M, Minamiguchi S and Togashi K: 18F-FDG uptake in
intraductal tubulopapillary neoplasm of the pancreas. Clin Nucl
Med. 39:e277–e280. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Del Chiaro M, Mucelli RP, Blomberg J,
Segersvärd R and Verbeke C: Is intraductal tubulopapillary
neoplasia a new entity in the spectrum of familial pancreatic
cancer syndrome? Fam Cancer. 13:227–229. 2014.PubMed/NCBI
|
|
13
|
Ahls MG, Niedergethmann M, Dinter D, Sauer
C, Lüttges J, Post S, Marx A and Gaiser T: Case report: Intraductal
tubulopapillary neoplasm of the pancreas with unique clear cell
phenotype. Diagn Pathol. 9:112014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhao L, Hart J, Xiao SY and Antic T:
Cytological features of pancreatic intraductal tubulopapillary
neoplasm and an unexpected immunohistochemical profile. Pathology.
46:662–665. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Takayama S, Maeda T, Nishihara M, Kanazawa
A, Chong HS, Oka H, Hirota S and Ishikawa O: A case of intraductal
tubulopapillary neoplasm of pancreas with severe calcification, a
potential pitfall in diagnostic imaging. Pathol Int. 65:501–506.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yoshida Y, Matsubayashi H, Sasaki K,
Kanemoto H, Uesaka K and Ono H: Intraductal tubulopapillary
neoplasm of the pancreatic branch duct showing atypical images. J
Dig Dis. 16:357–361. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kitaguchi K, Kato Y, Kojima M, Okubo S,
Takahashi D, Okada R, Nakayama Y, Nishida Y, Gotohda N, Takahashi S
and Konishi M: A resected case of intraductal tubulopapillary
neoplasm of the pancreas: Report of a case. Int Surg. 100:281–286.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Matthews Y, McKenzie C, Byrne C and Kench
JG: Intraductal tubulopapillary neoplasm of pancreas with
associated invasive carcinoma, lymph node, rectal and hepatic
metastases. Pathology. 47:169–171. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kölby D, Thilén J, Andersson R, Sasor A
and Ansari D: Multifocal intraductal tubulopapillary neoplasm of
the pancreas with total pancreatectomy: Report of a case and review
of literature. Int J Clin Exp Pathol. 8:9672–9680. 2015.PubMed/NCBI
|
|
20
|
Tajima S: Intraductal tubulopapillary
neoplasm of the pancreas suspected by endoscopic
ultrasonography-fine-needle aspiration cytology: Report of a case
confirmed by surgical specimen histology. Diagn Cytopathol.
43:1003–1006. 2015. View
Article : Google Scholar : PubMed/NCBI
|