Introduction
Breast cancer has the highest rate of incidence
among all types of cancer in women and it is also the primary cause
of death due to cancer worldwide (1).
Although primary breast cancer originated from breast tissue, not
all malignancies in breast tissues are primary breast cancer.
According to a previous study, ~0.43% of breast malignancies occur
as a result of metastatic lesions from extramammary tumors, such as
liver, lung and bone (2). In autopsy
studies, the incidence of extramammary malignancies metastasizing
to the breast was predicted to rise to ~7% (3). Therefore, differentiation between
primary breast cancer and metastatic breast malignancies is
important, in order to avoid misdiagnosis and subsequent
inappropriate treatment. Although physical examination and
radiological examination is important in the detection of breast
lesions, pathological examination is the most useful way for
definite diagnosis. Cases of primary colorectal cancer
metastasizing to the ovaries are not rare; however, cases of
primary colorectal cancer metastasizing to breast are very rare. In
1974, McIntosh et al (4) was
the first to describe a case of colon cancer metastasizing to the
breast. The present study reports an extremely rare case of
transverse colon cancer metastasizing to the bilateral ovaries and
the left breast, which was confirmed by a pathological examination
using immunohistochemistry.
Case report
A 47-year old female patient came to the outpatient
Department of The First Affiliated Hospital with Nanjing Medical
University (Jiangsu, China) on 8th July 2015, due to a breast lump.
Physical examination revealed a painless and mobile mass in the
outer lower quadrant of the left breast, with no skin dimpling,
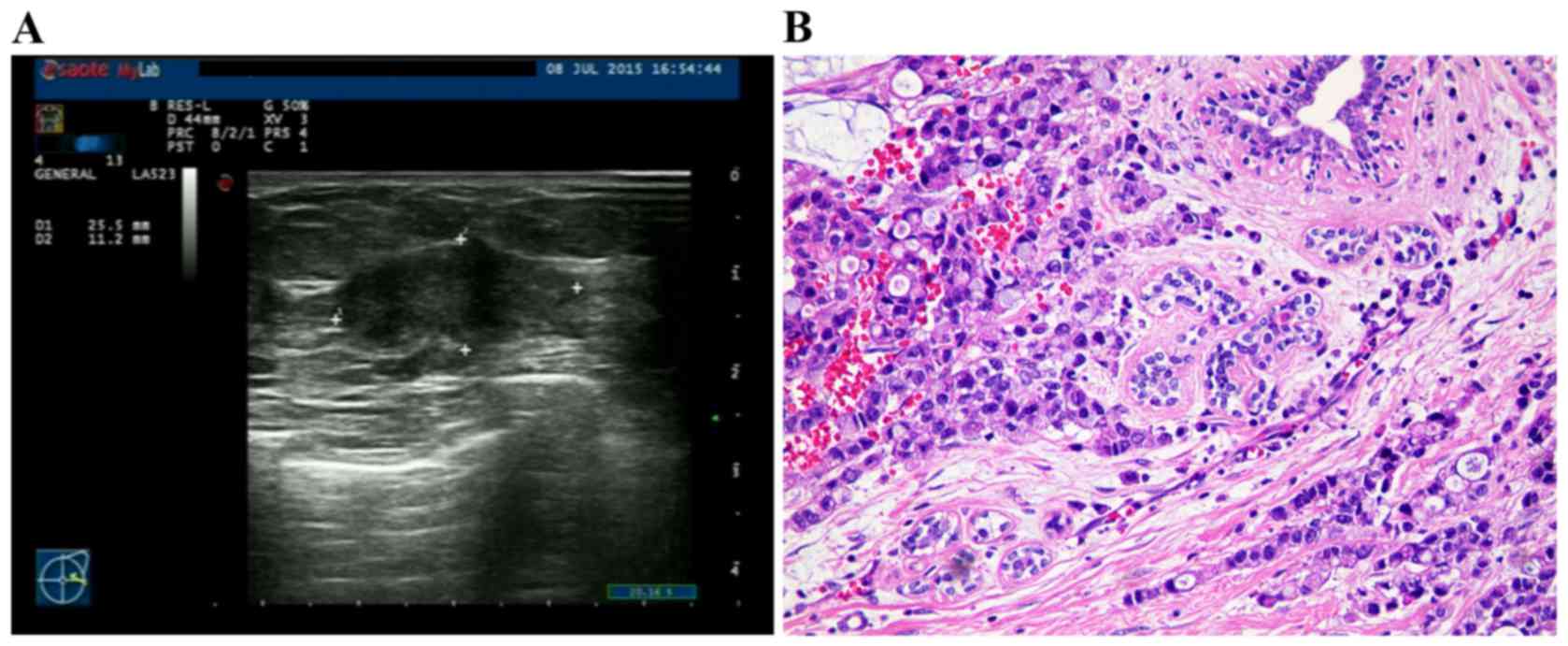
nipple retraction, or nipple discharge. An ultrasound scan detected
an irregular-shaped hypoechoic mass, which was category 4B
according to the Breast Imaging Reporting and Data System (5), 2.5×1.1 cm and without axillary
lymphadenopathy (Fig. 1A). A
serological test reported normal levels of the carbohydrate antigen
125 and the carbohydrate antigen 15–3, but elevated levels of the
carcinoembryonic antigen (CEA) of 5.36 ng/ml (reference range of
The First Affiliated Hospital with Nanjing Medical University is
0–4.7 ng/ml). The breast mass specimen was then obtained using
ultrasound guided core needle biopsy and submitted for pathological
examination. Hematoxylin and eosin (H&E) examination
demonstrated the breast mass to be an adenocarcinoma with a
mucinous adenocarcinoma component (Fig.
1B). IHC examination revealed negative estrogen receptor,
negative progesterone receptor and negative human epithelial growth
factor 2 (data not shown).
Investigations into the patient's history revealed
that the patient was admitted to Liyang City Traditional Chinese
Medicine Hospital (Changzhou, China) in September 2014 for a dull
persistent abdominal pain. Ultrasound identified a 5-cm mass and a
15-cm mass in the left and right pelvic cavity (data not
available). The patient then received surgery on September 25th,
2014. Intraoperative palpation revealed that the two pelvic masses
were on left and right ovaries, separately. The surgeon also found
one mass in the greater omentum, and another mass (~3×2 cm) inside
the transverse colon, which was inducing dilation in the ascending
and proximal transverse colon. Since the patient did not obtain
preoperative bowel preparation, the patient only received resection
of bilateral ovaries and some nodules in the greater omentum.
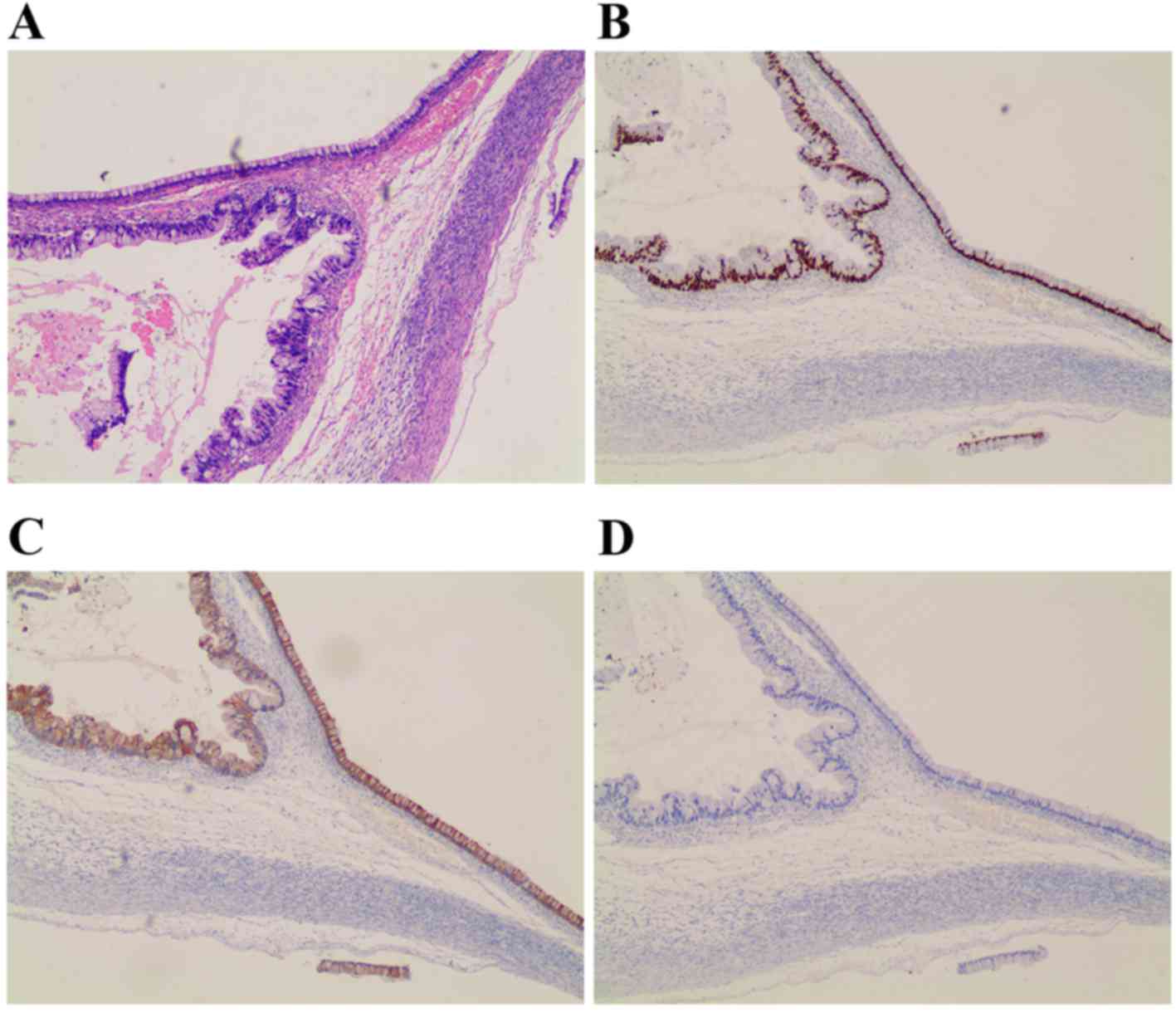
Postoperative pathology revealed that the tumor was
a metastatic adenocarcinoma (Fig.
2A). IHC examination identified that caudal-related homeobox
protein 2 (CDX2) and cytokeratin 20 (CK20) were positive, while
cytokeratin 7 (CK7) was negative (Fig.
2B-D). The patient was then transferred to The First Affiliated
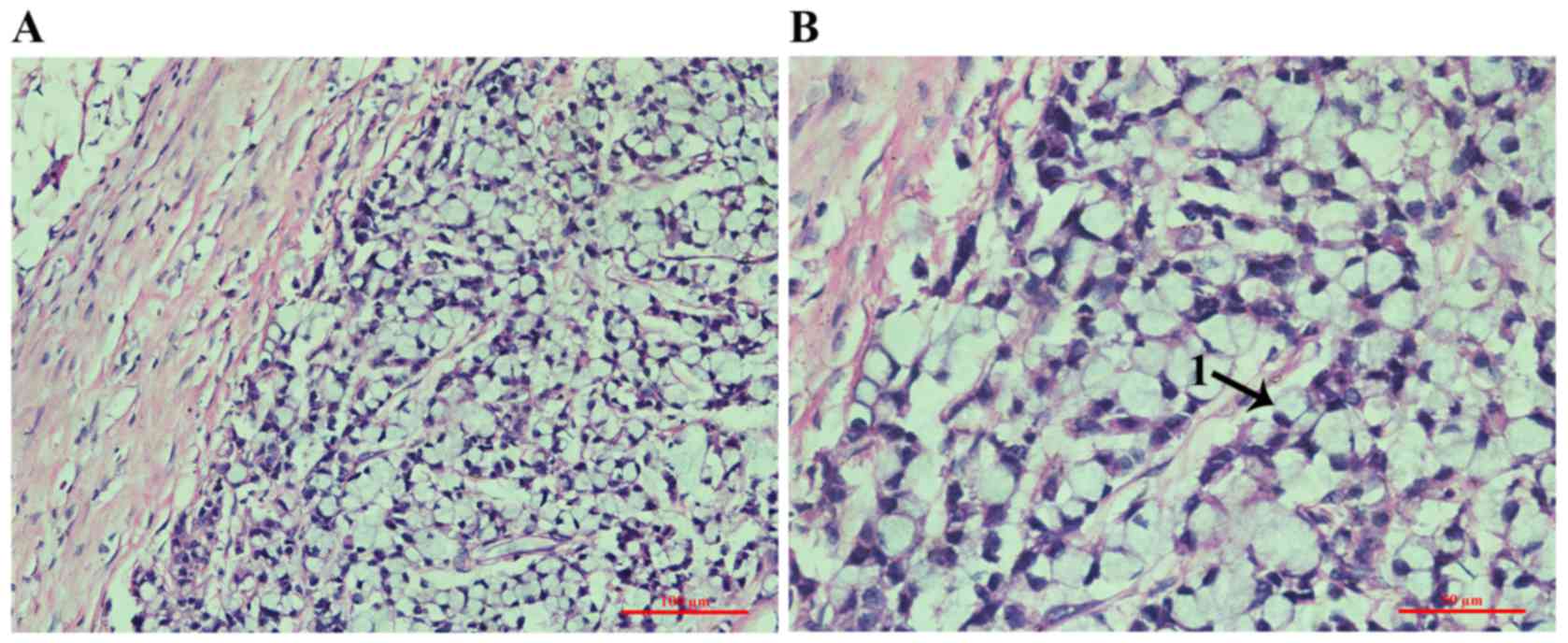
Hospital of Soochow University (Suzhou, China). Following a radical
laparoscopic resection of the colon cancer, pathological
examination confirmed the cancer to be a poorly to moderately
differentiated adenocarcinoma. Specific areas of the adenocarcinoma
were mucinous adenocarcinoma accompanied by signet ring cell
(Fig. 3). Lymph nodes (7/10) were
also involved. The patient then received 8 cycles of the systemic
chemotherapy of the folinic acid, fluorouracil and irinotecan
regimen. Subsequent to therapy, the examination revealed that
levels of CEA were 2.07 ng/ml (reference range of The First
Affiliated Hospital of Soochow University, 0–5 ng/ml).
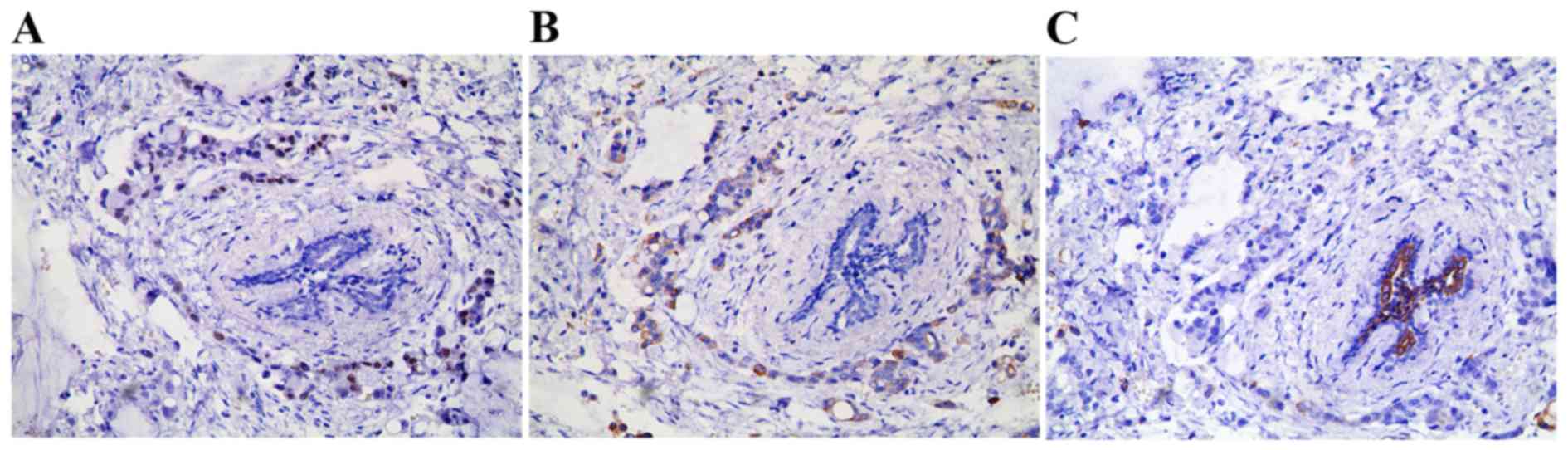
Since the patient had a history of Krukenberg tumor,
and exhibited elevated levels of CEA and an undetermined breast
malignancy, IHC examinations on a breast biopsy specimen were then
applied. Results demonstrated that the tumor cells were also
positive for CDX2 and CK20, but negative for CK7 (Fig. 4). The breast tumor was then confirmed
as being a metastatic lesion from the primary colon cancer. As a
result, a wide excision rather than a radical mastectomy was
performed. Following surgery, the patient underwent a positron
emission tomography/computed tomography (PET/CT) scan with
18F-fluorodeoxyglucose. Examination of the scan identified no
evidence of any other distant metastasis (including liver and
lung).
All procedures reported in the present study are in
accordance with the ethical guidelines of the Declaration of
Helsinki and were approved by the ethics and research committee of
the First Affiliated Hospital with Nanjing Medical University.
Informed consent to be involved in and publish the results of
present study was obtained from the patient.
Discussion
In the present case, the transverse colon cancer
first metastasized to the bilateral ovaries (Krukenberg tumor) and
then to the left breast. In general the liver, lung and bone are
the most frequent sites of metastasis from colorectal cancer
(6). The Krukenberg tumor was first
described by Friedrich Ernst Krukenberg in 1896 (7), and refers to a malignancy in the ovary
that had metastasized from a primary site. Krukenberg tumors are
known to originate from the stomach (~48.1% of cases), the
intestine (42.6% of cases), and other primary sites including the
breast, biliary system and the pancreas (8). Cases of primary colorectal cancer
metastasizing to breast are rare (2),
and simultaneous metastasis to the ovaries and breast tissues
occurs even more infrequently. Jiang et al (9) reported a young breastfeeding female (28
years old) suffering from a suspicious gastrointestinal tumor
metastasizing to the bilateral ovaries and the bilateral breasts.
However, the specimen of primary cancer was not obtained for
pathological examination due to cachexia. Vakili et al
(10) reported a 38-year old female
patient who received ascending colon cancer surgery, and 15 months
later developed metastases in the right ovary and left breast. To
the best of our knowledge, the present report is the first case of
transverse colon cancer metastasizing to bilateral ovaries and then
to the left breast.
A malignant mass in the breast may be misdiagnosed
as primary breast cancer due to its high rates of incidence
(11). Therefore, differentiation
between primary and metastatic breast cancer is important to avoid
misdiagnosis and subsequent inappropriate treatment. Physical and
radiological examination, detailed past tumor history, as well as
pathological examinations are helpful.
According to the literature, metastatic malignances
in breast are more common in the left breast compared with the
right (12). These metastases usually
grow rapidly, but do not induce skin dimpling, nipple retraction or
nipple discharge (13,14). Mammographies are helpful in achieving
a differential diagnosis, since a metastatic malignancy in the
breast is round and well circumscribed, with no speculation,
microcalcification or thickening of the skin (10). In addition, increased attention should
be paid to patients who exhibit a past history of extramammary
cancer. Lymphoma, melanoma, sarcoma, lung carcinoma and ovarian
cancer are the most common types of primary cancer that metastasize
to the breast (2,15,16).
Finally, pathological examination is the most useful diagnosis
technique. In H&E examination, metastatic tumor cells in the
breast are shown to usually locate in the periductal or perilobular
region, lacking in situ components and desmoplastic reaction
(11,17). IHC staining may also help in
differentiating the origin of the tumor. In the present case, IHC
examinations of the breast and ovarian tumor consistently
demonstrated that CK20 and CDX2 were positively stained, while CK7
was negatively stained. CK20 and CK7 are the widely used markers in
determining primary sites of metastatic adenocarcinoma (18,19). In
addition, CDX2 is also a highly specific and sensitive marker for
colorectal carcinoma (20). For
metastatic breast disease, diagnostic and palliative treatment for
local control is recommended (12),
rather than mastectomy and lymph node dissection (10). In the present case, a wide excision
alone was performed, without axillary dissection.
Due to the early screening, the use of advanced
equipment including PET-CT scans and the comprehensive treatment of
colorectal cancer, an increasing number of patients are able to
live longer. As a result, an increasing number of rare types of
metastatic tissues are becoming common. For clinicians, diagnosis
should be cautious, and differential diagnosis should always be
kept in mind.
Acknowledgements
The present study was supported in part by The
National Natural Science Foundation of China (grant nos. 81172502
and 81302305), The Natural Science Foundation of Jiangsu Province
(grant no. BK20131027), The Program for Development of Innovative
Research Team in the First Affiliated Hospital of Nanjing Medical
University (grant no. IRT-008), The Youth Talent Project (grant no.
FRC201308), and a project funded by the Priority Academic Program
Development of Jiangsu Higher Education Institutions (grant no.
20131107).
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Georgiannos SN, Chin J, Goode AW and
Sheaff M: Secondary neoplasms of the breast: A survey of the 20th
century. Cancer. 92:2259–2266. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ahmad A, Baiden-Amissah K, Oyegade A,
Absar M, Swainson K and Titi S: Primary sigmoid adenocarcinoma
metastasis to the breast in a 28-year-old female: A case study and
a review of literature. Korean J Pathol. 48:58–61. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
McIntosh IH, Hooper AA, Millis RR and
Greening WP: Metastatic carcinoma within the breast. Clin Oncol.
2:393–401. 1976.PubMed/NCBI
|
|
5
|
Mendelson E, Bohm-Velez M, Berg W, et al:
ACR BI-RADS® ultrasoundAtlas, Breast Imaging Reporting
and Data System American College of Radiology. Reston VA: pp.
1492013
|
|
6
|
Selcukbiricik F, Tural D, Bay A, Sahingoz
G, Ilvan S and Mandel NM: A malignant mass in the breast is not
always breast cancer. Case Rep Oncol. 4:521–525. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Israel SL, Helsel EV Jr and Hausman DH:
The challenge of metastatic ovarian carcinoma. Am J Obstet Gynecol.
93:1094–1101. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jiang R, Tang J, Cheng X and Zang RY:
Surgical treatment for patients with different origins of
Krukenberg tumors: Outcomes and prognostic factors. Eur J Surg
Oncol. 35:92–97. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jiang Q, Liu S, Xiong H, Pen J, Cai K,
Yang Y and Xiong Z: Metastatic signet ring cell carcinoma of the
bilateral breasts and ovaries from gastrointestinal tract in a
young breastfeeding female - a case report. J Cancer. 2:484–489.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Vakili SM, Sharbatdaran M, Noorbaran A,
Siadati S, Moslemi D and Shafahi S: A case of colon cancer with
breast metastasis and krukenberg tumor. Int J Hematol Oncol Stem
Cell Res. 8:46–50. 2014.PubMed/NCBI
|
|
11
|
Noh KT, Oh B, Sung SH, Lee RA, Chung SS,
Moon BI and Kim KH: Metastasis to the breast from colonic
adenocarcinoma. J Korean Surg Soc. 81 Suppl 1:S43–S46. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fernández de Bobadilla L, García
Villanueva A, Collado M, De Juan A, Rojo R, Pérez J, Lisa E,
Aguilera A, Mena A and González-Palacios F: Breast metastasis of
primary colon cancer. Rev Esp Enferm Dig. 96:415–419. 2004.(In
English, Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Vergier B, Trojani M, De Mascarel I,
Coindre JM and Le Treut A: Metastases to the breast: Differential
diagnosis from primary breast carcinoma. J Surg Oncol. 48:112–116.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hajdu SI and Urban JA: Cancers metastatic
to the breast. Cancer. 29:1691–1696. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Williams SA, Ehlers RA II, Hunt KK, Yi M,
Kuerer HM, Singletary SE, Ross MI, Feig BW, Symmans WF and
Meric-Bernstam F: Metastases to the breast from nonbreast solid
neoplasms: Presentation and determinants of survival. Cancer.
110:731–737. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Vizcaino I, Torregrosa A, Higueras V,
Morote V, Cremades A, Torres V, Olmos S and Molins C: Metastasis to
the breast from extramammary malignancies: A report of four cases
and a review of literature. Eur Radiol. 11:1659–1665. 2011.
View Article : Google Scholar
|
|
17
|
Ho YY and Lee WK: Metastasis to the breast
from an adenocarcinoma of the colon. J Clin Ultrasound. 37:239–241.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kende AI, Carr NJ and Sobin LH: Expression
of cytokeratins 7 and 20 in carcinomas of the gastrointestinal
tract. Histopathology. 42:137–140. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Park SY, Kim BH, Kim JH, Lee S and Kang
GH: Panels of immunohistochemical markers help determine primary
sites of metastatic adenocarcinoma. Arch Pathol Lab Med.
131:1561–1567. 2007.PubMed/NCBI
|
|
20
|
Werling RW, Yaziji H, Bacchi CE and Gown
AM: CDX2, a highly sensitive and specific marker of adenocarcinomas
of intestinal origin: An immunohistochemical survey of 476 primary
and metastatic carcinomas. Am J Surg Pathol. 27:303–310. 2003.
View Article : Google Scholar : PubMed/NCBI
|