Introduction
Wilms tumor (WT) is a retroperitoneal solid tumor
commonly identified in children and the most common type of renal
malignancy in children (1). Early
diagnosis of WT is dependent on clinical symptoms and physical and
imaging examinations, with pathological examination being the gold
standard in WT diagnosis. Although laboratory examination cannot
offer specific biomarkers for early diagnosis in WT, certain serum
and urine indicators, including α-fetoprotein, and catecholamine
metabolites can effectively be used for differential diagnosis
between hepatoblastoma and neuroblastoma. Complete resection and
chemotherapy are currently the major therapeutic strategies for
patients with WT. In addition, kidney transplantation is an
effective alternative for the treatment of WT.
The development of mass spectrometry (MS) provides a
novel platform for the investigation of diseases. Our group has
employed proteomics to screen serum biomarkers in patients with
breast cancer, thyroid cancer and WT, which may be useful for the
early diagnosis of malignancies (2–4). In
previous years, an increasing number of studies have confirmed that
inflammatory cytokines are closely associated with oncogenesis,
particularly to the growth, invasion, metastasis and immune escape
of different types of cancer (5–8). However,
the role of inflammatory cytokines in WT remains unclear. In the
present study, proteomics was employed to identify differentially
expressed inflammatory cytokines in WT and the results were
confirmed using immunohistochemistry. Subsequently, associations
between the altered expression of these cytokines with clinical
stage, pathological type and other characteristics of WT were
investigated, which may provide novel therapeutic targets for
WT.
Materials and methods
Patients
A total of 40 children (mean age, 2.5±1.5 years;
median, 2.5 years; range, 0.3–5.2 years), including 23 males and 17
females, with WT were recruited between January 2010 and December
2014. Adjacent normal tissues (1 cm away from the tumor) were
collected from 35 patients, of whom there were 20 males and 15
females with a mean age of 2.2±1.3 years (median, 2.1 years; range,
0.3–4.5 years). Normal kidney tissues (5 cm away from the tumor)
were collected from an additional 25 patients, of whom there were
14 males and 11 females with a mean age of 2.2±1.1 years (median,
2.4 years; range, 0.5–4.2 years). No patient received chemotherapy
or radiotherapy prior to enrollment into the study, and
pathological diagnosis of WT was confirmed by more than two
pathologists.
Clinical stage and pathological type were determined
according to the criteria described by the National Wilms Tumor
Study Group (1). Stage I WT was
identified in 6 patients, stage II WT in 12, stage II WT in 13 and
stage IV WT in 9. Favorable histology, as indicated by tissue
primarily consisting of embryonal, epithelial and stromal cells,
was noted in 33 patients, and unfavorable histology in 7 patients.
In addition, the absence of lymph node metastasis was noted in 23
patients while 17 exhibited lymph node metastasis. Of the 40
patients, vascular involvement was identified in 9. Fresh tissues
(20 mg) were lysed in 200 µl lysis buffer (50 mM Tris, 150 mM NaCl,
1% sodium deoxycholate, 0.1% SDS, 1% NP-40, 1 mM phenylmethane
sulfonyl fluoride), followed by centrifugation at 10,000 × g for 20
min at 4°C. The supernatant was harvested and stored at −80°C. The
present study was approved by the Ethics Committee of Zhengzhou
University, and written informed consent was obtained from the
patients parents prior to entry into the study.
Reagents and instruments
Surface-enhanced laser desorption/ionization-time of
flight mass spectrometry (SELDI-TOF-MS), weak cation exchange
(WCX)-2 SELDI protein chip and Bioprocessor equipment were
purchased from Ciphergen Biosystems, Inc., (Fremont, CA, USA).
Reagents used for SELDI-TOF-MS were obtained from Sigma-Aldrich;
Merck KGaA (Darmstadt, Germany). The Tangential flow ultrafilter
(Vivaflow 50) was purchased from Sartorius AG (Göttingen, Germany).
The solid phase extraction (SPE) column was purchased from
Sigma-Aldrich; Merck KGaA. A vacuum centrifugal concentrator and
the protein markers (cat. no. 26628) were purchased from Thermo
Fisher Scientific, Inc. (Waltham, MA, USA). The trypsin detection
kit was obtained from Promega Corporation (Madison, WI, USA), and
the matrix-assisted laser desorption/ionization-TOF-MS was from
Bruker AXS GmbH (Karlsruhe, Germany). A rabbit polyclonal antibody
[human macrophage migration inhibitory factor (MIF; cat. no.
ab65869) and C-X-C motif ligand 7 chemokine (CXCL7; cat. no.
ab169946)] and a goat anti-rabbit horseradish peroxidase-conjugated
secondary antibody (cat. no. ab205718) were purchased from Abcam
(Cambridge, UK).
Screening of inflammatory markers
Following lysis, samples were centrifuged at 4°C for
10 min at 10,000 × g, and the supernatant was collected and added
into 96-well plates (5 µl/well), followed by addition of U9 buffer
{9M urea, 2% 3-[(3-cholamidopropyl)
dimethylammonio]-1-propanesulfonate, 50 mM Tris-HCl, 1%
dithiotheritol (DTT), pH 9.0; 10 µl/well}. The plates were
incubated at 4°C with a constant agitation for 30 min, and 185 µl
NaAc (0.1 M sodium acetate, pH 4.0) was subsequently added and
vortexed for 5 min. The WCX-2 SELDI protein chip was fixed in the
Bioprocessor, and NaAc was added to each well (200 µl/well) and
vortexed at room temperature for 5 min in the rotating platform,
repeat once. The samples were added to the protein chip (100
µl/well) and vortexed at 4°C for 60 min. The chip was dried, and
NaAc was added (200 µl/well) and vortexed for 5 min. This was
repeated three times. Following two washes with 200 µl deionized
water to each well, 1 µl of saturated SPA solution [SPA, 50%
acetonitrile (ACN), 0.5% trifluoroacetic acid (TFA)] was added to
each well, and the chip was air-dried. Finally, the chip was placed
in the SELDI-TOF-MS machine for the detection of the protein
peaks.
Identification of inflammatory
cytokines
For sample processing, 1 ml protein sample was mixed
with 5 ml of deionized water. The peristaltic pumps and tangential
flow ultrafilter were connected, and the inlet and outlet tubes
were subsequently placed in the protein sample to form a loop. The
collection tube was placed in a centrifuge tube, and the filtrate
was collected without proteins >30 kDa. The filtrate was stored
at −80°C and freeze-dried. The dry powder was dissolved in
deionized water to a final volume of 250 µl.
The proteins were next separated with a SPE column.
In brief, 250 µl samples were mixed with 500 µl U9 buffer, followed
by incubation at 4°C for 30 min with constant agitation, then 250
µl sample buffer was added (2% TFA and 20% ACN). Subsequently, 1
tube volume of activation solution (100% ACN) was added into the
tube. This step was repeated once, then 1 tube volume of
equilibration solution (0.5% TFA, 5% ACN) was added (this step was
repeated twice). Following this, 1 ml sample was added into the
tube and collected, and this step was repeated once more.
Subsequently, 2 ml equilibration solution was used to wash the
tube, and this step was repeated once. The elution buffer (250 µl)
at different concentrations (30, 50, 70 and 100% ACN containing
0.1% TFA) was added, which was repeated once, and the filtrate was
collected into a vacuum centrifugal concentrator. Centrifugation
was conducted at room temperature for 4–6 h at 10,000 × g.
Following centrifugation, 10 µl mixture was collected.
The target proteins were separated using 12% Tricine
SDS-PAGE (200 µg/lane) and stained with 0.25% Coomassie Brilliant
Blue. The target bands were collected into EP tubes, and 80 µl
washing buffer (50% ACN and 25 mM NH4HCO3)
was subsequently added at 37°C for 20 min with constant agitation.
Following three washes and drying at 90°C for 15 min, 20 µl
digestion buffer (100 mM NH4HCO3) and 2 µl
dilute reductant (100 mM DTT and 100 mM
NH4HCO3) were added, followed by incubation
at 37°C for 10 min. Subsequent to the mixture being allowed to cool
to room temperature, 2 µl blocker solution (550 mM
C2H4INO and 100 mM
NH4HCO3) was added at room temperature for 10
min, followed by 0.5 µl dilute trypsin solution to a final
concentration of trypsin at 8 ng/µl. Following centrifugation at
3,000 × g for 5 min, the in-gel digestion continued at 37°C for 12
h. Centrifugation was performed at 1,000 × g for 15 min, and the
supernatant was harvested.
Following digestion, the peptide mixture was
subjected to separation with nano-liquid chromatography (LC), and
the resultant mixture was added into a MALDI-TOF-MS. Subsequent to
MS/MS, the sequences of corresponding peptides were recognized and
searched via Mascot. The corresponding proteins were searched in
the Swiss-Prot database (http://www.uniprot.org/).
Validation of inflammatory
cytokines
Fresh tissues were embedded in paraffin, 5-µm
sectioned, and deparaffinized with graded ethanol (100, 95, 85 and
75%). Antigen retrieval was performed in citrate buffer (0.01 M
Na3C6H5O7-2H2O,
pH 6.0) for 10 min. Subsequently, sections were treated with 3%
H2O2 for 30 min at room temperature to block
the endogenous peroxidase and subsequently blocked with goat serum
at room temperature for 30 min. Following incubation with the
anti-MIF and anti-CXCL7 primary antibodies (1:500 dilution) at 4°C
for 12 h, the sections were treated with secondary antibodies
(1:1,000 dilution) at 37°C for 30 min, followed by three washes in
PBS. Visualization was conducted with 3,3-diaminobenzidine for 3
min, which was stopped by washing with flowing water.
Counterstaining was performed using hematoxylin. Following
dehydration with ethanol and transparentization with xylene, the
sections were mounted in neutral gum.
Expression levels of MIF and CXCL7 depended on the
mean density of staining. The positive rates of MIF and CXCL7 was
determined on the basis of the staining intensity and number of
positive cells. Staining intensity: No staining, 0; yellow, 1;
yellow-brown, 2; and brown, 3. The number of positive cells:
<25%, 1; ≥25%, <50%, 2; ≥50%, <75%, 3; and ≥75%, 4. The
product of the two scores was the final score: -, 0–3; +, 3–6; ++,
6–9; and +++, >9.
Statistical analysis
Quantitative data were compared using two-tailed
Students t-tests with an α of 0.05 between two groups.
Kruskal-Wallis tests were employed for comparisons of the
quantitative data among groups, followed by paired comparisons with
Tamhanes T2 tests (α=0.05). Comparisons of qualitative
data among the groups were performed with χ2 tests with
an α of 0.05, and paired comparisons were performed with an α of
0.01 between two groups.
Results
Screening and identification of
inflammatory cytokines
Mass spectrometry data from WT tissues, adjacent
normal tissues and normal renal tissues were subjected to
standardization with the ZUCI-ProteinChip Data Analysis System, and
corresponding protein peaks were obtained using cluster analysis.
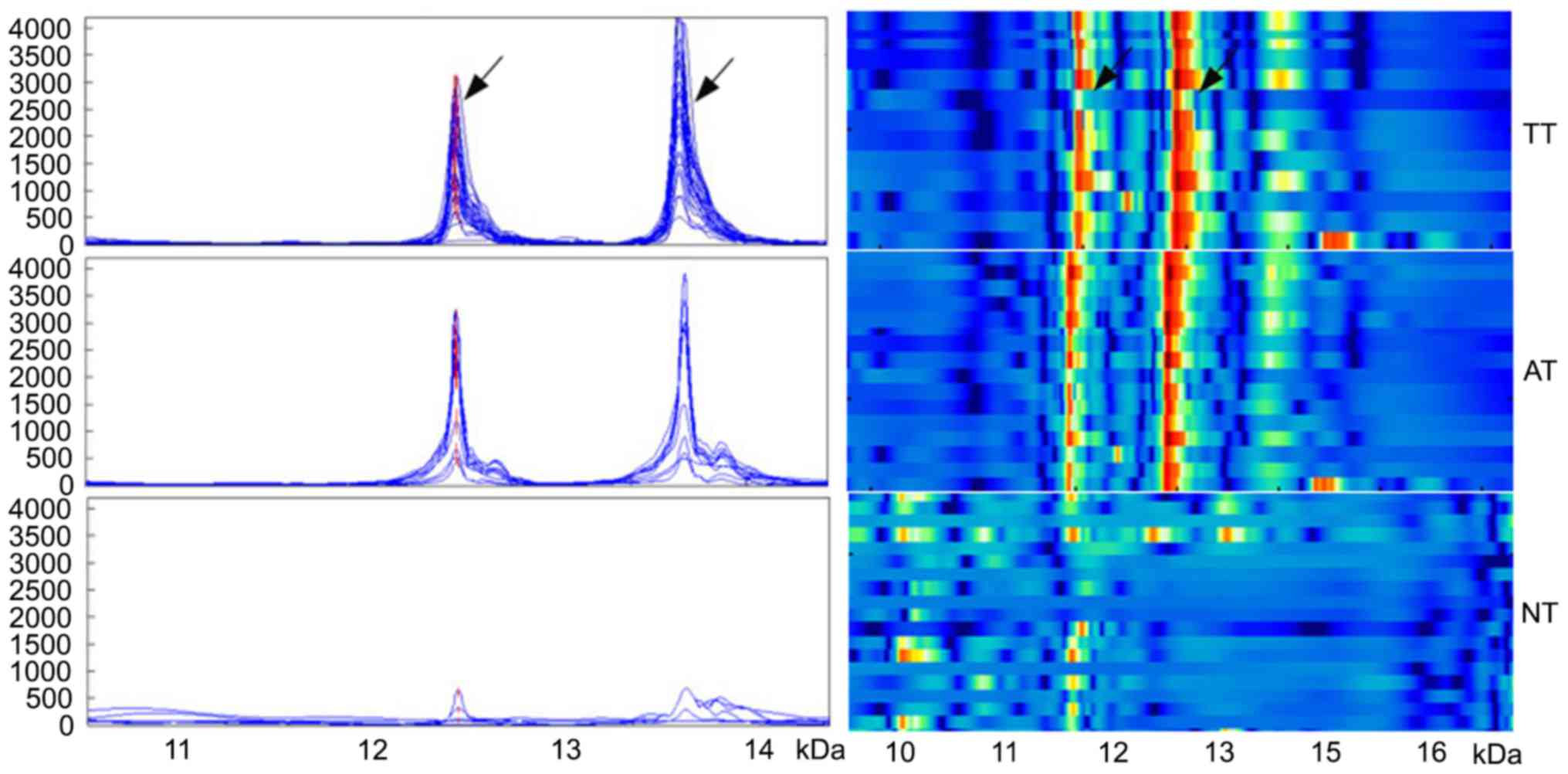
In WT tissues, five differentially strongly expressed protein peaks
were identified, including m/z12138 and m/z13462 that were
identified as being the MIF and the CXCL7 chemokine. The expression
of the two inflammation peaks was significantly increased in WT
tissues (1,437.8±997.3 and 1,730.4±1,147.8, respectively), compared
with adjacent normal tissues (952.6±591.2 and 1,031.1±1,120.8,
respectively) and normal renal tissues (315.4±296.5 and
114.7±118.9, respectively; all P<0.05; Fig. 1).
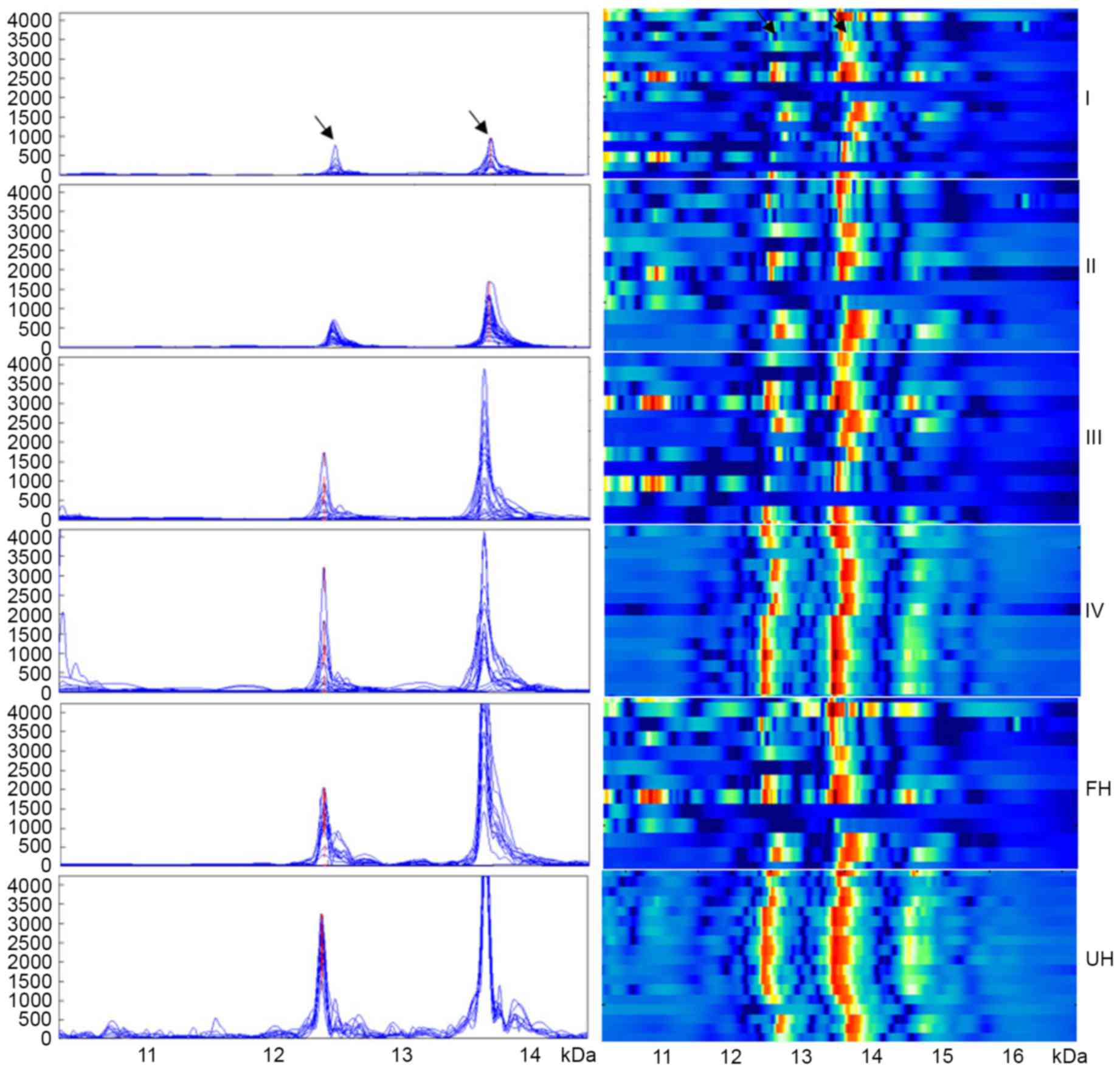
Although the expression of the two inflammation
peaks was not associated with age or gender (P>0.05), their
expression significantly increased with the progression of WT
(P<0.001): 678.8±189.0 and 746.2±238.7, respectively in stage I
WT; 664.0±202.0 and 1,180.7±404.9, respectively in stage II WT;
1,524.7±407.9 and 2,160.4±1,252.3, respectively in stage III WT;
and 2,850.2±861.2 and 2,498.4±1,290.5, respectively in stage IV WT
(Fig. 2). In addition, the expression
level of m/z12138 and m/z13462 was significantly lower in WT
patients with favorable histology compared with those with
unfavorable histology (1,152.3±735.5 and 1,281.0±630.6,
respectively vs. 2,783.9±872.4 and 3,848.8±310.2, respectively;
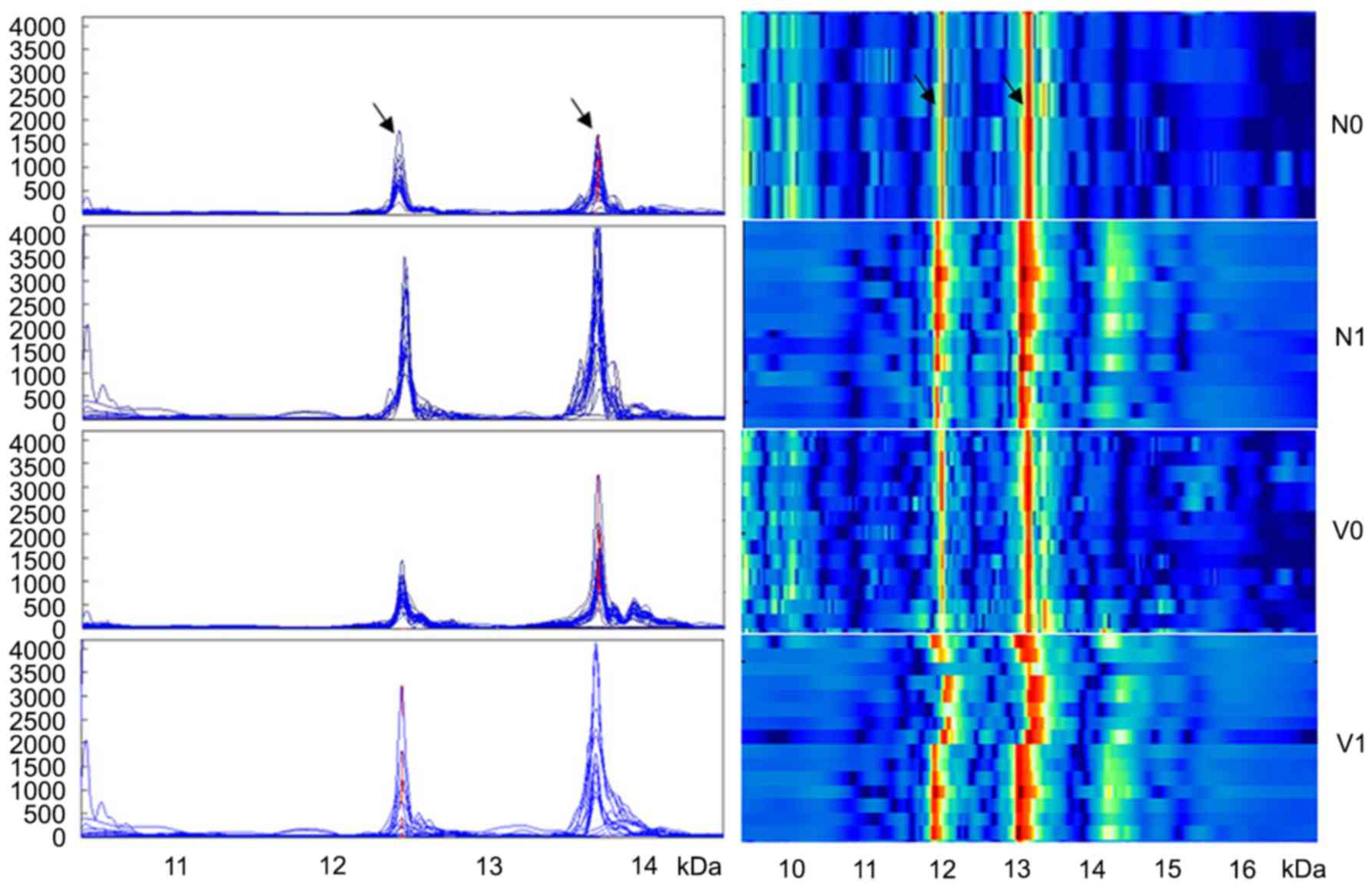
P<0.001; Fig. 2). Additionally,
the expression levels of the two peaks were significantly lower in
patients without lymph node metastasis compared with patients with
lymph node metastasis (869.2±474.6 and 1,110.2±433.6, respectively
vs. 2,207.1±961.7 and 2,569.5±1,285.2, respectively; P<0.01;
Fig. 3). m/z12138 and m/z13462
expression was also significantly lower in patients without
vascular involvement compared with those with vascular involvement
(1,027.8±521.3 and 1,507.5±1,019.9, respectively vs. 2,850.2±861.2
and 2,498.4±1,290.5, respectively; P≤0.021; Fig. 3). The characteristics of the patients
are summarized in Table I.
 | Table I.Association between the expression of
m/z12138 and m/z13462 peaks and clinical characteristics. |
Table I.
Association between the expression of
m/z12138 and m/z13462 peaks and clinical characteristics.
|
|
| m/z12138 | m/z13462 |
|---|
|
|
|
|
|
|---|
| Variables | n | Intensity (x±s) | P-value | Intensity (x±s) | P-value |
|---|
| Tissue type |
|
| <0.001 |
| <0.001 |
| TT | 40 | 1,437.8±997.3 | 0.031a | 1,730.4±1,147.8 | 0.019a |
| AT | 35 | 952.6±591.2 |
<0.001b |
1,031.1±1,120.8 |
<0.001b |
| NT | 25 | 315.4±296.5 |
<0.001c | 114.7±118.9 |
<0.001c |
| Genderd |
|
| 0.496 |
| 0.677 |
|
Male | 23 | 1,339.3±773.0 |
|
1,796.7±1,063.9 |
|
|
Female | 17 |
1,571.1±1,214.0 |
|
1,640.7±1,280.6 |
|
| Age, years |
|
| 0.610 |
| 0.655 |
|
<2.5 | 20 | 1,518.0±821.2 |
|
1,813.0±1,310.1 |
|
|
≥2.5 | 20 |
1,357.6±1,128.1 |
| 1,647.8±986.6 |
|
| Clinical stage |
|
| <0.001 |
| <0.001 |
| I | 6 | 678.8±189.0 |
| 746.2±238.7 |
|
| II | 12 | 664.0±202.0 |
| 1,180.7±404.9 |
|
|
III | 13 | 1,524.7±407.9 |
|
2,160.4±1,252.3 |
|
| IV | 9 | 2,850.2±861.2 |
|
2,498.4±1,290.5 |
|
| Pathological
type |
|
| <0.001 |
| <0.001 |
| FH | 33 | 1,152.3±735.5 |
| 1,281.0±630.6 |
|
| UH | 7 | 2,783.9±872.4 |
| 3,848.8±310.2 |
|
| Lymph node
metastasis |
|
| <0.001 |
| <0.001 |
| N | 23 | 869.2±474.6 |
| 1,110.2±433.6 |
|
| Y | 17 | 2,207.1±961.7 |
|
2,569.5±1,285.2 |
|
| Vascular
invasion |
|
| <0.001 |
| 0.021 |
| N | 31 | 1,027.8±521.3 |
|
1,507.5±1,019.9 |
|
| Y | 9 | 2,850.2±861.2 |
|
2,498.4±1,290.5 |
|
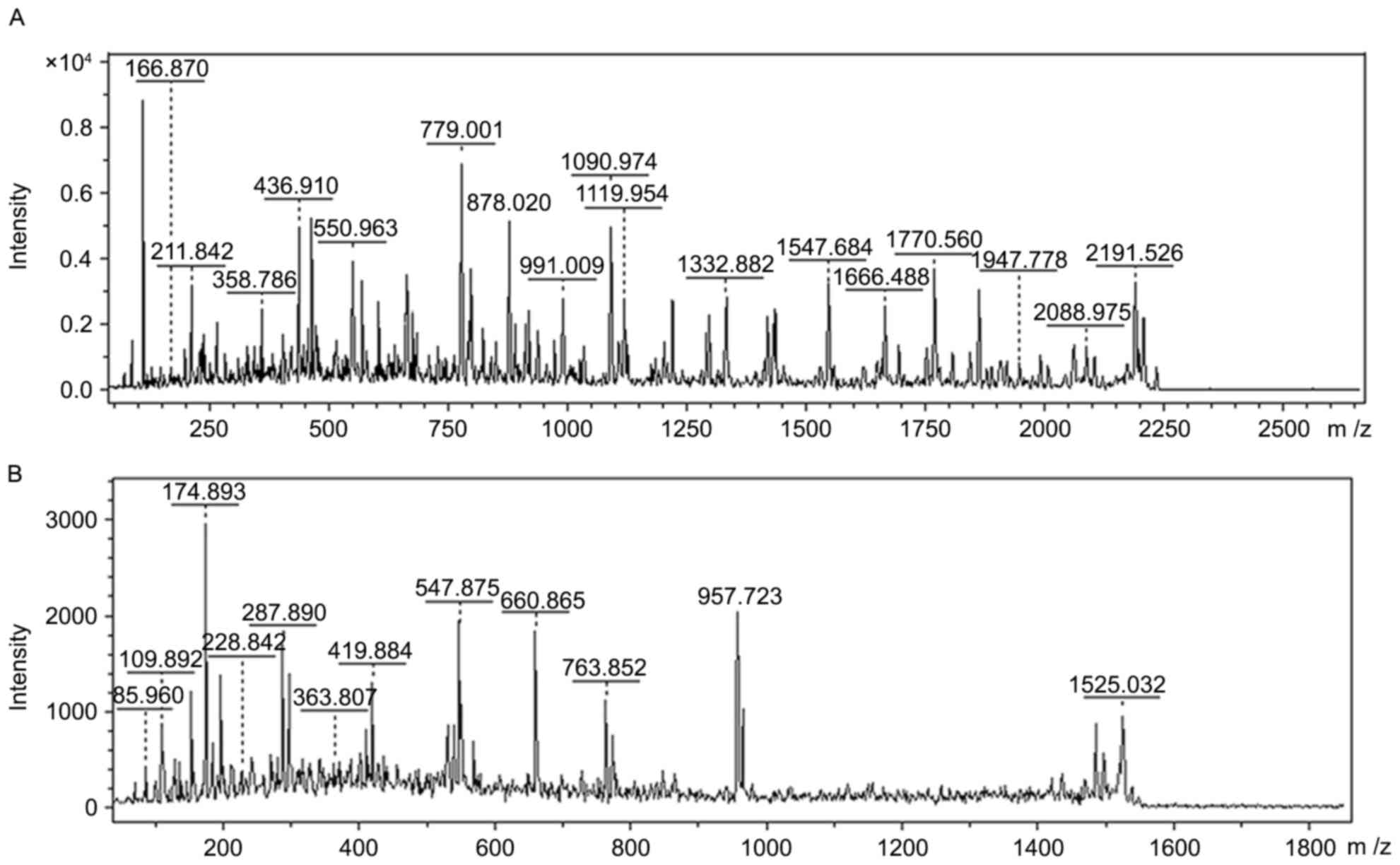
Upregulated proteins of m/z12138 and m/z13462 in WT
were separated and purified by SPE and Tricine-SDS-PAGE,
respectively. Following in-gel digestion, the peptide mixture was
subjected to LC-MS/MS. Finally, proteins of m/z12138 and m/z13462
were identified as MIF and CXCL7 on the basis of their amino acid
sequences through matrix-assisted laser
desorption/ionization-TOF-MS (Fig. 4;
Table II).
| Table II.Identification of the two
inflammation protein biomarkers with identified peptides and
covered sequence. |
Table II.
Identification of the two
inflammation protein biomarkers with identified peptides and
covered sequence.
| m/z | Protein name | Identified
peptides | Sequence |
|---|
| 12138 | MIF | PMFIVNTNVPR |
MFIVNTNVPRASVPDGFLSELTQQLAQATGKPPQYIA |
|
|
|
RASVPDGFLSELTQQLAQATGK |
VHVVPDQLMAFGGSSEPCALCSLHSIGKIGGAQNRSYS |
|
|
| RSYSKLLCGLLAER |
KLLCGLLAER |
|
|
| LLCGLLAER |
|
| 13462 | CXCL7 |
GKEESLDSDLYAELR |
GKEESLDSDLYAELRCMCIKTTSGIHPKNIQSLEVIGK |
|
|
| NIQSLEVIGK |
GTHCNQVEVIATLKDGRKICLDPDAPR |
|
|
|
| GTHCNQVEVIATLK |
|
|
|
| KICLDPDAPR |
|
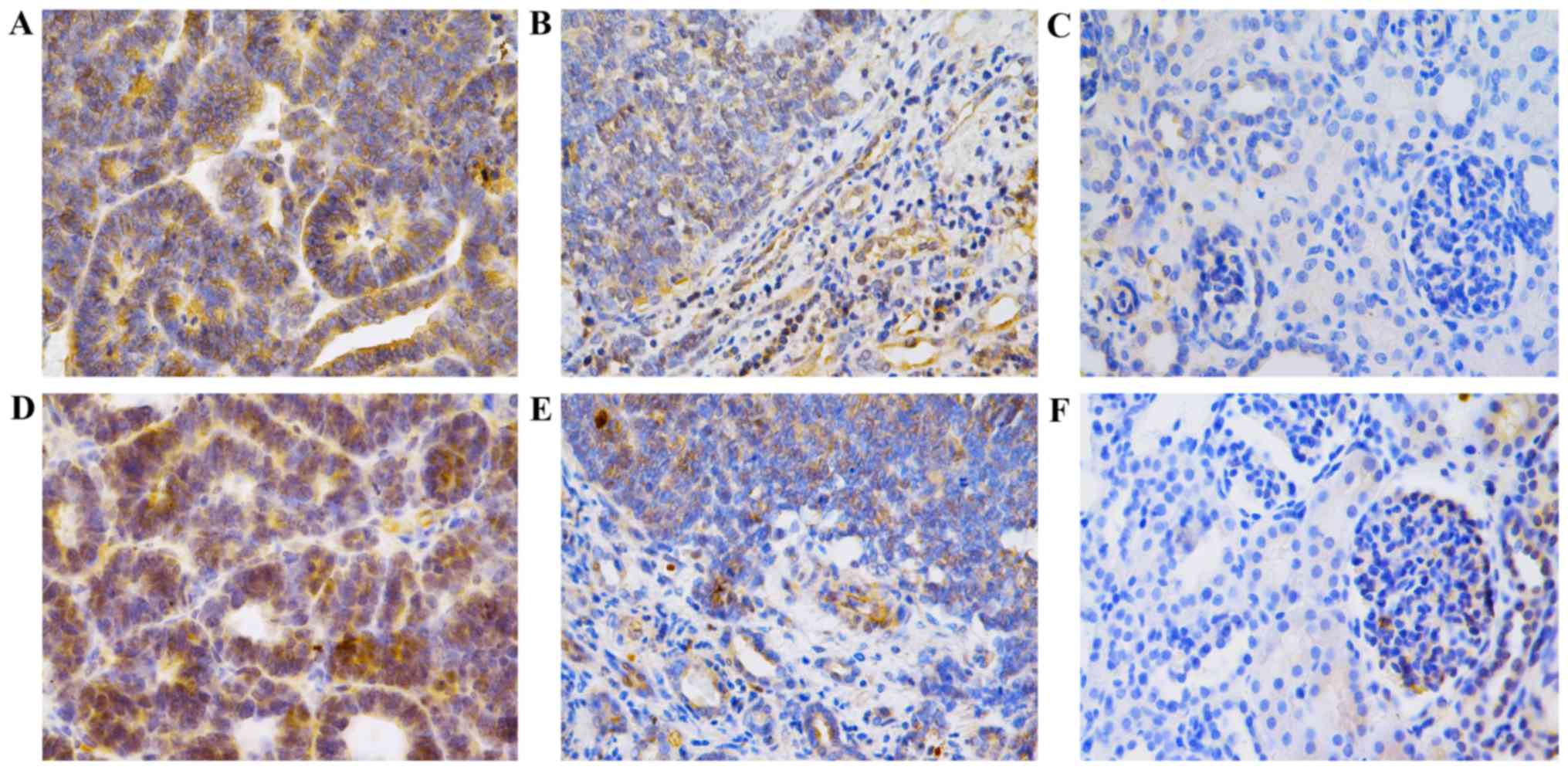
Detection of MIF and CXCL7 by
immunohistochemistry
MIF expression was 0.0530±0.0145 in WT tissues,
0.0106±0.0042 in adjacent normal tissues and 0.0008±0.0006 in
normal renal tissues (P<0.001). In addition, CXCL7 expression
was 0.0495±0.0240 in WT tissues, 0.0138±0.0063 in adjacent normal
tissues and 0.0009±0.0005 in normal renal tissues, (P<0.001)
(Fig. 5; Table III), confirming that the expression
levels of the two cytokines were significantly increased in WT.
| Table III.Expression of MIF and CXCL7 in TT, AT
and NT through immunohistochemistry. |
Table III.
Expression of MIF and CXCL7 in TT, AT
and NT through immunohistochemistry.
|
|
| MIF | CXCL7 |
|---|
|
|
|
|
|
|---|
| Tissue type | n | Mean density | P-value | Mean density | P-value |
|---|
| TT | 40 | 0.0530±0.0145 |
<0.001a | 0.0495±0.0240 |
<0.001a |
| AT | 35 | 0.0106±0.0042 |
<0.001b | 0.0138±0.0063 |
<0.001b |
| NT | 25 | 0.0008±0.0006 |
<0.001c | 0.0009±0.0005 |
<0.001c |
The number of cells positive for MIF was 92.5%
(37/40) in WT tissues, 57.1% (20/35) in adjacent normal tissues and
16.0% (4/25) in normal renal tissues (P<0.01). In addition, the
number of cells positive for CXCL7 was 87.5% (35/40) in WT tissues,
48.6% (17/35) in adjacent normal tissues, and 12.0% (3/25) in
normal tissues (P<0.01; Table
IV).
| Table IV.Positive rate of MIF and CXCL7 in TT,
AT and NT through immunohistochemistry. |
Table IV.
Positive rate of MIF and CXCL7 in TT,
AT and NT through immunohistochemistry.
|
|
| MIF | CXCL7 |
|---|
|
|
|
|
|
|---|
| Tissue type | n | Positive (%) | Negative (%) | P-value | Positive (%) | Negative (%) | P-value |
|---|
| TT | 40 | 37 (92.5) | 3 (7.5) |
<0.001a | 35 (87.5) | 5 (12.5) |
<0.001a |
| AT | 35 | 20 (57.1) | 15 (42.9) |
<0.001b | 17 (48.6) | 18 (51.4) |
<0.001b |
| NT | 25 | 4 (16.0) | 21 (84.0) | 0.001c | 3 (12.0) | 21 (88.0) | 0.007c |
Discussion
Proteomics has been employed to investigate the
structure, function and characteristics of the proteome in tissues,
organs and cells, and has become an important technique in life
sciences in the post-genomics era. In our previous studies
(2–4),
several serum protein markers were identified to be associated with
the occurrence and development of breast and thyroid cancer and WT.
As the molecular weights of inflammatory cytokines ranges between
10 and 30 kDa, the molecular weight was adjusted to a range of 3–30
kDa in the SELDI-TOF-MS. In addition, prior to the separation and
purification of the target proteins, proteins >30 kDa were
removed to avoid interference in subsequent gel electrophoresis and
purification using a tangential flow ultrafilter, which is a
reliable biological membrane that may be used to remove proteins
>30 kDa. The separation and purification of target proteins is
dependent on SPE and gel electrophoresis, so that the subsequent
identification may have improved accuracy.
Of the differentially expressed proteins that were
upregulated in WT, proteins at m/z12138 and m/z13462 were
identified as MIF and CXCL7; their upregulation in WT was confirmed
by immunohistochemistry. The expression of these two cytokines was
reduced in the adjacent normal tissues and again in the normal
tissues compared with the WT tissues, suggesting that the two
cytokines are closely associated with the occurrence and
development of WT. In addition, their expression increased with the
WT progression and increased malignancy. Thus, these cytokines may
represent markers indicative of clinical stage and pathological
type. Additionally, their expression in tumor samples from patients
with WT with lymph node metastasis/vascular involvement was
significantly increased compared with adjacent tissue samples,
suggesting that each may perform important roles in the invasion
and metastasis of WT.
MIF is a multifunctional protein that is primarily
synthesized by activated lymphocytes and macrophages (9). It may also be synthesized in the
parenchymal cells of the liver, spleen and kidney (10). MIF is an important regulator of
inflammation and the immune response, and may also be a key
negative regulator that blocks the anti-inflammatory effect of
glucocorticoids (10). A previous
study has confirmed that MIF may act as a specific biomarker in
inflammation-mediated diseases (11).
In addition, MIF performs important roles in the proliferation,
metastasis, immune escape and angiogenesis of cancer cells,
including studies in prostate (12),
bladder (13) and lung cancer
(14–16), melanoma (17), colon (18), oral (19), breast (20,21) and
head and neck squamous cell cancer (22). In glioma (23), ovarian cancer (24) and neuroblastoma (25), MIF may inhibit the cytotoxicity of NK
cells and T-lymphocytes, facilitating the immune escape of cancer
cells and compromising the clearance of cancer cells by the immune
system. Thus, MIF may represent a biomarker for the diagnosis of
malignancies, and a novel therapeutic target that may improve the
killing of cancer cells by the immune system.
CXCL7, a member of the CXC chemokine subfamily, is
involved in inflammation. CXCL7 as a chemical irritant may induce
the directional migration of leukocytes, and is primarily secreted
by macrophages, lymphocytes, endothelial cells and fibroblasts.
CXCL7, as an important cytokine, is not only involved in a variety
of physiological and pathological processes including hemopoiesis
and inflammation reaction (26–30), but
is also closely associated with the occurrence and development of
numerous types of cancer (31–35).
However, to the best of our knowledge, the roles of MIF and CXCL7
in WT have not previously been examined.
Pathological examination is the most commonly used
method for the diagnosis of WT. However, there is no widely
accepted pathological marker indicative of cancer progression. The
results of the present study demonstrated that MIF and CXCL7 may
become important biomarkers indicative of clinical stage and
pathological type of WT. Chemotherapy and immune therapy are the
main strategies used for patients with WT. The wide application of
an MIF blocker (36) provides a novel
prospect for the therapy of WT. However, the specific biological
roles of MIF and CXCL7 in WT remain poorly understood, and
additional studies are required to confirm them.
References
|
1
|
Metzger ML and Dome JS: Current therapy
for Wilms tumor. Oncologist. 10:815–826. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fan Y, Shi L, Liu Q, Dong R, Zhang Q, Yang
S, Fan Y, Yang H, Wu P, Yu J, et al: Discovery and identification
of potential biomarkers of papillary thyroid carcinoma. Molecular
Cancer. 8:792009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zhang Q, Wang J, Dong R, Yang S and Zheng
S: Identification of novel serum biomarkers in child nephroblastoma
using proteomics technology. Mol Biol Rep. 38:631–638. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fan Y and Wang J, Yang Y, Liu Q, Fan Y, Yu
J, Zheng S, Li M and Wang J: Detection and identification of
potential biomarkers of breast cancer. J Cancer Res Clin.
136:1243–1254. 2010. View Article : Google Scholar
|
|
5
|
Mitchell JK, Lemon SM and McGivern DR: How
do persistent infections with hepatitis C virus cause liver cancer?
Curr Opin Virol. 14:101–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Umansky V and Sevko A: Overcoming
immunosuppression in the melanoma microenvironment induced by
chronic inflammation. Cancer Immunol Immunother. 61:275–282. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kanterman J, Sade-Feldman M and Baniyash
M: New insights into chronic inflammation-induced
immunosuppression. Semin Cancer Biol. 22:307–318. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ringelhan M, OConnor T, Protzer U and
Heikenwalder M: The direct and indirect roles of HBV in liver
cancer: Prospective markers for HCC screening and potential
therapeutic targets. J Pathol. 235:355–367. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lue H, Kleemann R, Calandra T, Roger T and
Bernhagen J: Macrophage migration inhibitory factor (MIF):
Mechanisms of action and role in disease. Microbes Infect.
4:449–460. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Calandra T and Roger T: Macrophage
migration inhibitory factor: A regulator of innate immunity. Nat
Rev Immunol. 3:791–800. 2003. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Grieb G, Merk M, Bernhagen J and Bucala R:
Macrophage migration inhibitory factor (MIF): A promising
biomarker. Drug News Perspect. 23:257–264. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Meyer-Siegler KL, Iczkowski KA, Leng L,
Bucala R and Vera PL: Inhibition of macrophage migration inhibitory
factor or its receptor (CD74) attenuates growth and invasion of
DU-145 prostate cancer cells. J Immunol. 177:8730–8739. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Choudhary S, Hegde P, Pruitt JR, Sielecki
TM, Choudhary D, Scarpato K, Degraff DJ, Pilbeam CC and Taylor JA
III: Macrophage migratory inhibitory factor promotes bladder cancer
progression via increasing proliferation and angiogenesis.
Carcinogenesis. 34:2891–2899. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Arenberg D, Luckhardt TR, Carskadon S,
Zhao L, Amin MA and Koch AE: Macrophage migration inhibitory factor
promotes tumor growth in the context of lung injury and repair. Am
J Resp Crit Care. 182:1030–1037. 2010. View Article : Google Scholar
|
|
15
|
Gámez-Pozo A, Sánchez-Navarro I, Calvo E,
Agulló-Ortuño MT, López-Vacas R, Díaz E, Camafeita E, Nistal M,
Madero R, Espinosa E, et al: PTRF/Cavin-1 and MIF proteins are
identified as non-small cell lung cancer biomarkers by label-free
proteomics. PLoS One. 7:e337522012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
McClelland M, Zhao L, Carskadon S and
Arenberg D: Expression of CD74, the receptor for macrophage
migration inhibitory factor, in non-small cell lung cancer. Am J
Pathol. 174:638–646. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tanese K, Hashimoto Y, Berkova Z, Wang Y,
Samaniego F, Lee JE, Ekmekcioglu S and Grimm EA: Cell Surface
CD74-MIF interactions drive melanoma survival in response to
interferon-γ. J Invest Dermatol. 135:2775–2784. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gordon-Weeks AN, Lim SY, Yuzhalin AE,
Jones K and Muschel R: Macrophage migration inhibitory factor: A
key cytokine and therapeutic target in colon cancer. Cytokine
Growth Factor Rev. 26:451–461. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chang KP, Lin SJ, Liu SC, Yi JS, Chien KY,
Chi LM, Kao HK, Liang Y, Lin YT, Chang YS and Yu JS:
Low-molecular-mass secretome profiling identifies HMGA2 and MIF as
prognostic biomarkers for oral cavity squamous cell carcinoma. Sci
Rep. 5:116892015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Verjans E, Noetzel E, Bektas N, Schütz AK,
Lue H, Lennartz B, Hartmann A, Dahl E and Bernhagen J: Dual role of
macrophage migration inhibitory factor (MIF) in human breast
cancer. BMC Cancer. 9:2302009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Richard V, Kindt NG, Decaestecker C,
Gabius HJ, Laurent G, Noël JC and Saussez S: Involvement of
macrophage migration inhibitory factor and its receptor (CD74) in
human breast cancer. Oncol Rep. 32:523–529. 2014.PubMed/NCBI
|
|
22
|
Kindt N, Lechien JR, Nonclercq D, Laurent
G and Saussez S: Involvement of CD74 in head and neck squamous cell
carcinomas. J Cancer Res Clin. 140:937–947. 2014. View Article : Google Scholar
|
|
23
|
Mittelbronn M, Platten M, Zeiner P,
Dombrowski Y, Frank B, Zachskorn C, Harter PN, Weller M and
Wischhusen J: Macrophage migration inhibitory factor (MIF)
expression in human malignant gliomas contributes to immune escape
and tumour progression. Acta Neuropathol. 122:353–365. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Krockenberger M, Dombrowski Y, Weidler C,
Ossadnik M, Hönig A, Häusler S, Voigt H, Becker JC, Leng L, Steinle
A, et al: Macrophage migration inhibitory factor (MIF) contributes
to the immune escape of ovarian cancer by downregulating NKG2D1. J
Immunol. 180:7338–7348. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhou Q, Yan X, Gershan J, Orentas RJ and
Johnson BD: Expression of macrophage migration inhibitory factor by
neuroblastoma leads to the inhibition of antitumor T cell
reactivity in vivo. J Immunol. 181:1877–1886. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pillai MM, Iwata M, Awaya N, Graf L and
Torok-Storb B: Monocyte-derived CXCL7 peptides in the marrow
microenvironment. Blood. 107:3520–3526. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pecks U, Kirschner I, Wölter M, Schlembach
D, Koy C, Rath W and Glocker MO: Mass spectrometric profiling of
cord blood serum proteomes to distinguish infants with intrauterine
growth restriction from those who are small for gestational age and
from control individuals. Transl Res. 164:57–69. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ehlken C, Grundel B, Michels D, Junker B,
Stahl A, Schlunck G, Hansen LL, Feltgen N, Martin G, Agostini HT
and Pielen A: Increased expression of angiogenic and inflammatory
proteins in the vitreous of patients with ischemic central retinal
vein occlusion. PLoS One. 10:e01268592015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yeo L, Adlard N, Biehl M, Juarez M,
Smallie T, Snow M, Buckley CD, Raza K, Filer A and Scheel-Toellner
D: Expression of chemokines CXCL4 and CXCL7 by synovial macrophages
defines an early stage of rheumatoid arthritis. Ann Rheum Dis.
75:763–771. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ghasemzadeh M, Kaplan ZS, Alwis I,
Schoenwaelder SM, Ashworth KJ, Westein E, Hosseini E, Salem HH,
Slattery R, McColl SR, et al: The CXCR1/2 ligand NAP-2 promotes
directed intravascular leukocyte migration through platelet
thrombi. Blood. 121:4555–4566. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Giuliano S, Guyot M, Grépin R and Pagès G:
The ELR+CXCL chemokines and their receptors CXCR1/CXCR2: A
signaling axis and new target for the treatment of renal cell
carcinoma. OncoImmunology. 3:e283992014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Matsubara J, Honda K, Ono M, Tanaka Y,
Kobayashi M, Jung G, Yanagisawa K, Sakuma T, Nakamori S, Sata N, et
al: Reduced plasma level of CXC chemokine ligand 7 in patients with
pancreatic cancer. Cancer Epidemiol Biomarkers Prev. 20:160–171.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Tang Z, Yu M, Miller F, Berk RS, Tromp G
and Kosir MA: Increased invasion through basement membrane by
CXCL7-transfected breast cells. Am J Surg. 196:690–696. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Grépin R, Guyot M, Giuliano S, Boncompagni
M, Ambrosetti D, Chamorey E, Scoazec JY, Negrier S, Simonnet H and
Pagès G: The CXCL7/CXCR1/2 axis is a key driver in the growth of
clear cell renal cell carcinoma. Cancer Res. 74:873–883. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Desurmont T, Skrypek N, Duhamel A,
Jonckheere N, Millet G, Leteurtre E, Gosset P, Duchene B, Ramdane
N, Hebbar M, et al: Overexpression of chemokine receptor CXCR2 and
ligand CXCL7 in liver metastases from colon cancer is correlated to
shorter disease-free and overall survival. Cancer Sci. 106:262–269.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Xu L, Li Y, Sun H, Zhen X, Qiao C, Tian S
and Hou T: Current developments of macrophage migration inhibitory
factor (MIF) inhibitors. Drug Discov Today. 18:592–600. 2013.
View Article : Google Scholar : PubMed/NCBI
|