Introduction
Lung cancer is one of the most fatal types of cancer
in developed countries; >25% of cancer-associated mortalities
are caused by lung cancer (1).
Non-small cell lung cancer (NSCLC) constitutes ~80% of lung cancer
cases. Lung adenocarcinoma (AC) is the main histological subtype of
NSCLC and its incidence rate is rising (2). Even in cases where patients undergo
complete resection by lymph node dissection, there is a 30–40%
chance of the patient succumbing to recurrent disease, and the
5-year survival rate for lung cancer is just 15.7% (3,4). In order
to identify the most effective clinical strategies, it is necessary
to predict which patients have a high risk of recurrence.
Certain defects, particularly the inclusion of
bronchioloalveolar carcinoma within AC subtypes, were present in
the 2004 World Health Organization classification system for lung
AC (5). To overcome these issues, a
new system was produced by the International Association for the
Study of Lung Cancer, the American Thoracic Society and the
European Respiratory Society (IASLC/ATS/ERS) in 2011. The new
International Multidisciplinary Lung Adenocarcinoma Classification
was published in the Journal of Thoracic Oncology, the official
journal of IASLC (5). This
classification is intended to support clinical practice as well as
research investigation and clinical trials (5). Most importantly, it may offer prognostic
information, such as grading lung ACs according to histological
architecture, which results in significant differences in prognoses
(6). In the present study, the new
classification system was used for introducing the research
results.
Tumors are composed of cancer cells and tumor stroma
that are disparate but interactive, just as normal tissue is
composed of parenchymal cells and surrounding supporting cells. The
extracellular matrix, vascular endothelial cells, immune cells,
inflammatory cells and cancer-associated fibroblasts are
constituents of tumor stroma (7–9). Cancer
cells are typically hyperproliferative, exhibit a high rate of
glycolysis and are resistant to apoptosis when compared with the
surrounding, normal cells. Glycolysis is a part of energy
metabolism and includes lactic acid fermentation, of which the end
product is lactate (10). In
mammalian cells, it is the most important step to obtain adenosine
triphosphate, including in cancer tissue. Tumor cells also undergo
proton efflux to prevent apoptosis due to acidosis through pH
regulators, including proton pumps, sodium-proton exchangers,
bicarbonate transporters and monocarboxylate transporters (MCTs),
which are previously demonstrated to be highly expressed in HeLa
tumor cells (11).
MCTs mediate the transport of various
monocarboxylates, including lactate, pyruvate and ketones, across
cell membranes. The transporter expression and function of MCTs in
various types of cancer has yet to be comprehensively studied,
although their function is well-characterized in normal tissue
(12). MCTs may serve a crucial
function in tumor biology according to recent observations
(12). The MCT family includes 14
members. Of these, only MCT 1–4 facilitate the proton-coupled
transport of lactate (13–17); although these proteins are all
transmembrane symporters, their specific distributions and
functions differ. MCT-1 and MCT-4 are situated in the cell
membrane. Utilizing the pH gradient, MCT-1 catalyzes the import and
export of lactate, whereas MCT-4 only exports lactate (13). MCT-2 is associated with importing
pyruvate following lactate oxidation, and is expressed in the
mitochondrial membrane (18,19). MCT-3 is restricted to the choroid
plexus and retinal pigment epithelia, and can only export lactate
(12).
MCT-4 is overexpressed in cells with upregulated
glycolysis, including in tumors (18,20,21), white
blood cells (13,16) and white muscle (22). A number of previous studies have
evaluated the immunohistochemical expression and prognostic
significances of MCT-4 in cancer, including gastrointestinal
(23,24), breast (23,25),
ovarian (23), lung (23), oral (26), prostate (27) cancer. However, the clinical relevance
of MCT-4 expression to lung AC has yet to be elucidated. Therefore,
the present study aimed to clarify the predictive role of MCT-4
expression level for the overall survival (OS) of patients with
lung AC, and to further assess its clinicopathological
significance, thus potentially identifying a novel potential
therapeutic target for the treatment of patients with lung AC.
Materials and methods
Patients and follow-up
A total of 146 lung AC patients, for which resected
tumor and corresponding normal lung tissues were available, were
retrospectively recruited from the Department of Pathology,
Zhongnan Hospital of Wuhan University (Wuhan, China). Patients with
lung AC were diagnosed between July 2004 to December 2011. All
these 146 patients were treated with lobectomy of lung AC, prior to
administration of chemotherapy or radiotherapy, and classified
according to the 7th edition TNM classification by IASLC (2009)
(28). The tumor specimens comprised
131 cases of invasive AC and 15 of variant invasive AC, in
accordance with the 2011 International Association for the Study of
Lung Cancer/American Thoracic Society/European Respiratory Society
system (5). Basic clinicopathological
information is presented in Table I.
Additionally, fresh lung AC and corresponding normal lung tissue
were harvested during resection from another 30 patients from
Zhongnan Hospital of Wuhan University, and stored at −80°C for
protein and total RNA extraction. These fresh tissues were obtained
between June 2014 and June 2017 by lobectomy prior to the
administration of chemotherapy or radiotherapy, and included 8
cases of lepidic predominant, 11 of acinar predominant, 3 of
micropapillary predominant and 8 of papillary predominant lung AC.
In the present study, the 30 patients were composed of 18 males and
12 females (mean age, 56; age range, 35–78). The present study was
permitted by the Institute Research Medical Ethics Committee of the
Medical College of Wuhan University, and informed consent was
obtained from each patient.
 | Table I.Patient clinicopathological
characteristics. |
Table I.
Patient clinicopathological
characteristics.
|
Characteristics | Value |
|---|
| Total, n | 146 |
| Age, median years
(range) | 59 (20–84) |
| Gender, n (%) |
|
|
Male | 80 (54.8) |
|
Female | 66 (45.2) |
| Survival status, n
(%) |
|
|
Alive | 81 (55.5) |
|
Deceased | 65 (44.5) |
| Invasion depth, n
(%) |
|
| T1 | 28 (19.2) |
| T2 | 101 (69.2) |
| T3 | 12 (8.2) |
| T4 | 5 (3.4) |
| Lymph node
metastasis, n (%) |
|
| N0 | 86 (58.9) |
| N1 | 38 (26.0) |
| N2 | 10 (6.8) |
| N3 | 1 (0.7) |
| NX | 11 (7.5) |
| Distant metastasis,
n (%) |
|
| M0 | 143 (97.9) |
| M1 | 3 (2.1) |
| TNM stage, n (%
total) |
|
|
IA/B | 25/18 (29.5) |
|
IIA/B | 50/29 (54.1) |
|
IIIA/B | 18/3 (14.4) |
| IV | 3 (2.1) |
| Histological type,
n (%) |
|
|
Invasive AC | 131 (89.7) |
|
Adherent | 16 (11.0) |
|
Acinar | 58 (39.7) |
|
Papillary | 24 (16.4) |
|
Micropapillary | 6 (4.1) |
|
Solid | 27 (18.5) |
| Variant
AC | 15 (10.3) |
|
Mucinous | 7 (4.8) |
|
Colloid | 5 (3.4) |
|
Lepidic | 1 (0.7) |
|
Intestinal | 2 (1.4) |
Follow-up began on the date of surgery and ended in
August 2012. OS time was defined as the period of time from initial
diagnosis to the date of the last follow-up or patient mortality.
Patients who succumbed to other diseases or unexpected events were
excluded from the study.
Tissue microarray (TMA)
construction
Two separate TMAs were constructed using technology
and a TMA instrument from Guilin Fanpu Biotechnology, Inc. (Guilin,
China). Each of the TMAs contained 146 lung specimens, including 73
tumor and 73 corresponding normal tissue specimens. The hematoxylin
and eosin-stained tissue specimens were reviewed and the most
representative tumor parts were selected to construct TMAs based on
evaluation by two independent pathologists (H.C. and Z.C.). The
methods for constructing the TMAs were as previously described
(29,30). As controls, 1.5-mm diameter tumor
cores were extracted from each sample and inserted into empty
paraffin blocks. The blocks were cut into 4-µm thick sections and
used for quantum dots-based immunofluorescence histochemistry
(QD-IHC) staining.
QD-IHC
The QD-IHC of MCT-4 protein was performed with 4-µm
sections from formalin-fixed and paraffin-embedded tissues of the
two TMAs. The primary antibody was a polyclonal rabbit anti-human
MCT-4 antibody [cat no. sc-50329; Santa Cruz Biotechnology, Inc.,
Dallas, TX, USA; dilution, 1:100 in Tris-buffered saline (TBS)].
The QD-IHC staining was performed using QD-conjugated streptavidin
probes (QD-SA) with 605 nm emission wavelength [Wuhan Jiayuan
Quantum Dot Technological Development Co., Ltd., Wuhan, China;
dilution, 1:300 in 2% bovine serum albumin (BSA, Sigma-Aldrich;
Merck KGaA, Darmstadt, Germany).
The major procedures were as previously described
(31): The TMAs were deparaffinized
in xylene and rehydrated three times in graded alcohol washes
subsequent to heating at 65°C for 30 min. Antigen retrieval was
performed with citric acid buffer (10 mM, pH 6.0) and a microwave
for 15 min, followed by cooling by standing at room temperature for
30 min. TMAs were initially incubated with 2% BSA buffer at 37°C
for 30 min and then with the primary antibody at 4°C overnight.
TMAs were then washed in TBS with Tween-20 (TBS-T; 0.5% Tween, 0.1
M Tris-base, 0.9% NaCl, pH 7.6) three times, for 5 min per wash. A
further incubation was performed following the addition of
biotinylated goat anti-rabbit secondary antibody (dilution, 1:250;
cat no. ab64256; Abcam, Cambridge, UK) at 37°C for 30 min. In order
to conjugate QDs, antibody-bound TMAs were incubated with 2% BSA
buffer at 37°C for 10 min and then in QD-SA at 37°C for 40 min. The
final step was washing the TMAs three times with TBS-T, for 5 min
per wash, and sealing with 90% glycerin (Sigma-Aldrich; Merck
KGaA). The QD signal from the cells was observed with fluorescence
microscopy. The positive signal was a target-specific, photo-stable
bright red, whereas tissue-background autofluorescence was green.
The MCT-4 primary antibody was replaced with TBS buffer to produce
controls. This protocol was strictly according to the
manufacturer's protocol (Wuhan Jiayuan Quantum Dot Technological
Development Co., Ltd.).
Scoring of IHC results
The results of IHC staining were independently
analyzed by two experienced pathologists (H.C. and Z.C.) who were
blinded to the clinical features of the patients. The evaluation
was performed with a light microscope at magnification, ×200 and
×400 magnification; slight differences were re-evaluated with
simultaneous viewing by the pathologists. Sections were scored
semiquantitatively for the area of positive staining (AP) using a
grading system described previously (32): 0, no AP or AP <5%; 1, AP 5–25%; 2,
AP 26–50%; 3, AP 51–75%; and 4, AP >75%. In addition, the
intensity of staining (IS) for MCT-4 was scored semiquantitatively
as 0 (negative, no positive signal), 1 (weak, light red signal), 2
(intermediate, red signal), or 3 (strong, bright red signal). The
final immunoreactivity score for MCT-4 was defined by the following
formula: Intensity distribution (ID) = AP × IS. For determining the
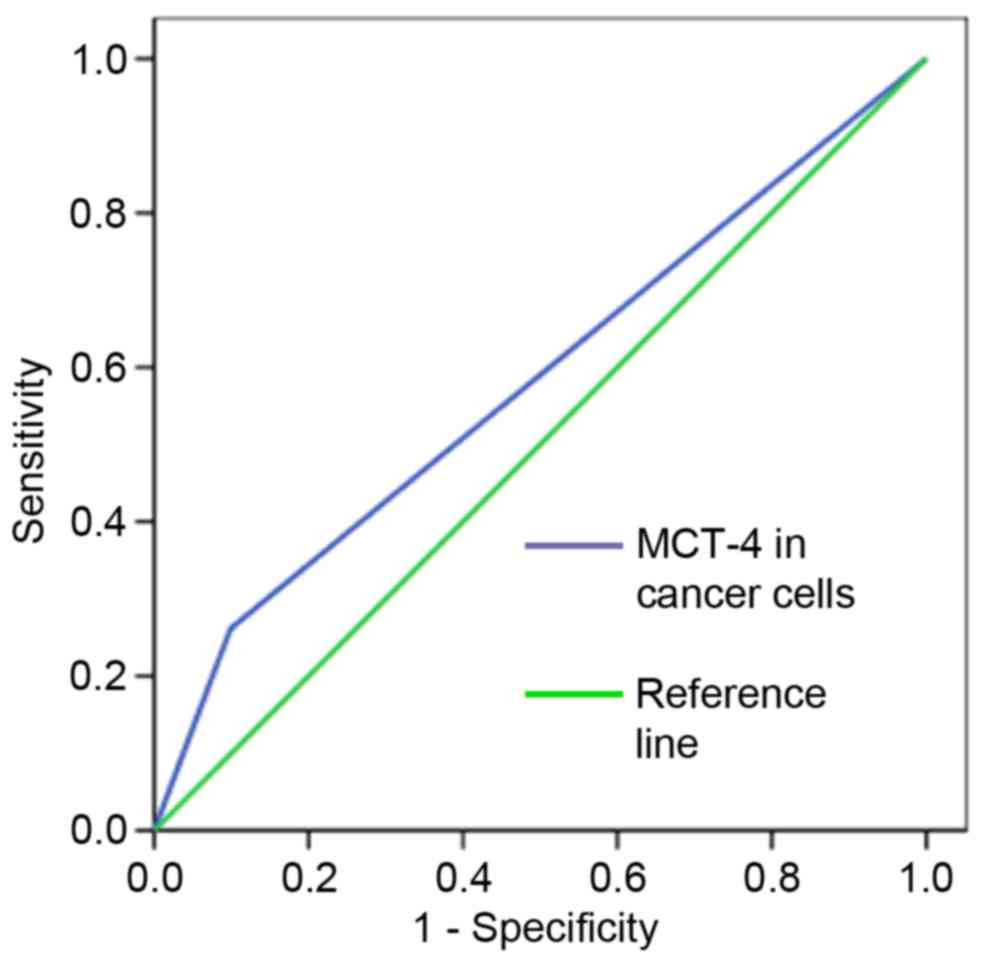
expression level of MCT-4 (high or low), a receiver operating
characteristic (ROC) curve analysis of OS rate was performed to
calculate the cutoff point.
Western blotting
Samples of lung AC and corresponding normal lung
tissues (each ~100 mg) were harvested from 30 patients, cut into
pieces with surgical scissors, lysed in lysis buffer (1% Triton
X-100, 150 mM NaCl, 10 mM Tris pH 7.4, 1 mM EDTA, 1 mM EGTA pH 8.0,
0.2 mM sodium orthovanadate, protease inhibitors) and quantified
for protein concentration through the BCA Protein Assay kit
(Pierce; Thermo Fisher Scientific, Inc., Waltham, MA, USA).
Following 10% SDS-PAGE, 30 µg protein samples were transferred to
nitrocellulose membranes and incubated with primary antibodies
against MCT-4 (dilution, 1:1,000 in BSA, cat no. sc-50329; Santa
Cruz Biotechnology, Inc.) and monoclonal mouse anti-β-actin
(dilution, 1:5,000 in BSA, cat no. A2228; Sigma-Aldrich; Merck
KGaA) overnight at 4°C. Membranes were then incubated with
horseradish peroxidase-conjugated goat anti-rabbit (cat no. A0208)
or goat anti-mouse (cat no. A0216) secondary antibody (both at
1:5,000; Beyotime Institute of Biotechnology, Haimen, China) for 45
min at 37°C. They were visualized with Pierce enhanced
chemiluminescence reagent (cat no. 34080; Pierce; Thermo Fisher
Scientific, Inc.) and exposed to X-ray film in the dark. Protein
bands were quantitatively analyzed using Quantity One software
(version 4.62; Bio-Rad Laboratories, Inc., Hercules, CA, USA).
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Total RNA from 30 cases of fresh lung AC and
corresponding normal lung tissues was isolated with TRIzol reagent
(Invitrogen; Thermo Fisher Scientific, Inc.) and reverse
transcribed with the iScript cDNA Synthesis kit (Bio-Rad
Laboratories, Inc.) under the following temperature conditions: 5
min at 25°C, 30 min at 42°C, then 5 min at 85°C to terminate the
reaction, according to the manufacturer's protocol. MCT-4 and
β-actin mRNA expression levels were measured by qPCR using the
Bio-Rad MyiQ Single Color Real-Time PCR Detection System and iQ
SYBR Green SuperMix (Bio-Rad Laboratories, Inc.), according to the
manufacturer's protocol. All data were analyzed by using Opticon
Monitor software (version 3.1; Bio-Rad Laboratories, Inc.). All
primers were synthesized by the Shanghai Sangon Biological
Engineering Technology and Services Co., Ltd. (Shanghai, China)
according to the published sequence for MCT-4 (NM_004207). The
primer sequences were as follows: MCT-4 forward,
5′-TGTGTGCGTGAACCGCTTT-3′ and reverse, 5′-AAACCCAACCCCGTGATGAC-3′;
and β-actin forward, 5′-GGAAATCGTGCGTGACATT-3′ and reverse,
5′-GACTCGTCATACTCCTGCTTG-3′. The qPCR cycling conditions were as
follows: 95°C for 5 min, followed by 40 cycles of 95°C for 10 sec,
60°C for 15 sec and 72°C for 20 sec. Quantification cycle (Cq)
values were determined for the internal control (β-actin) and for
the test gene at the same threshold level in the exponential phase
of the PCR curves. Relative quantification (2−ΔΔCq
method) was used to compare the expression level of the test genes
with the internal control (33). A
total of 3–4 reactions (each in triplicate) were run and the
standard deviation was calculated.
Statistical analysis
All statistical analyses were estimated using SPSS
19.0 software (IBM SPSS, Armonk, NY, USA). ROC curve analysis was
conducted to determine the cut-off point for high or low MCT-4
level. The χ2 test or Fisher's exact test were used to
analyze the association between MCT-4 immunofluorescent staining
and the clinicopathological parameters of patients with lung AC. OS
rates were calculated using the Kaplan-Meier curve analysis and
statistical significance was calculated using the log-rank test.
Univariate and multivariate analyses of survival rate were
performed using the Cox proportional hazards model, in order to
analyze independent prognostic values. All values for MCT-4
expression detected by western blotting and RT-qPCR were expressed
as the mean ± standard error of the mean. Statistical analysis was
performed using one-way ANOVA, or by Student's t-test for two
groups. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
The patients had a mean age of 59 years (range,
20–84 years), and included 80 males (54.8%) and 66 females (45.2%).
At the end of follow-up, 81 patients (55.5%) were alive and 65
(44.5%) had succumbed to lung AC. The period of follow-up ranged
from 1–96 months (mean, 41 months). With regard to the depth of
invasion (T), 28 patients (19.2%) were T1, 101 (69.2%) were T2, 12
(8.2%) were T3 and 5 (3.4%) were T4. With regard to the extent of
lymph node metastasis (N), 86 (58.9%) patients were N0, 38 (26.1%)
were N1, 10 (6.8%) were N2, 1 (0.7%) was N3, and 11 (7.5%) were Nx.
Furthermore, 3 patients (2.1%) exhibited distant metastasis (M1)
whereas 143 patients (97.9%) did not (M0). When comprehensively
considering TNM stage based on these three aspects, 43 patients
(29.5%) were classified as stage I, 79 (54.1%) as stage II, 21
(14.4%) as stage III and 3 (2.0%) as stage IV. Other
clinicopathological factors are presented in detail in Table I.
Cut-off value of MCT-4 expression
level
To obtain the cut-off values for high and low
expression level accurately, a ROC curve analysis was performed
with OS (Fig. 1). An ID score of 3.5
was determined as the cut-off score for MCT-4 expression in lung AC
(an ID score ≥3.5 indicated high expression and <3.5, low
expression) according to the optimal sensitivity and specificity
based on the curve.
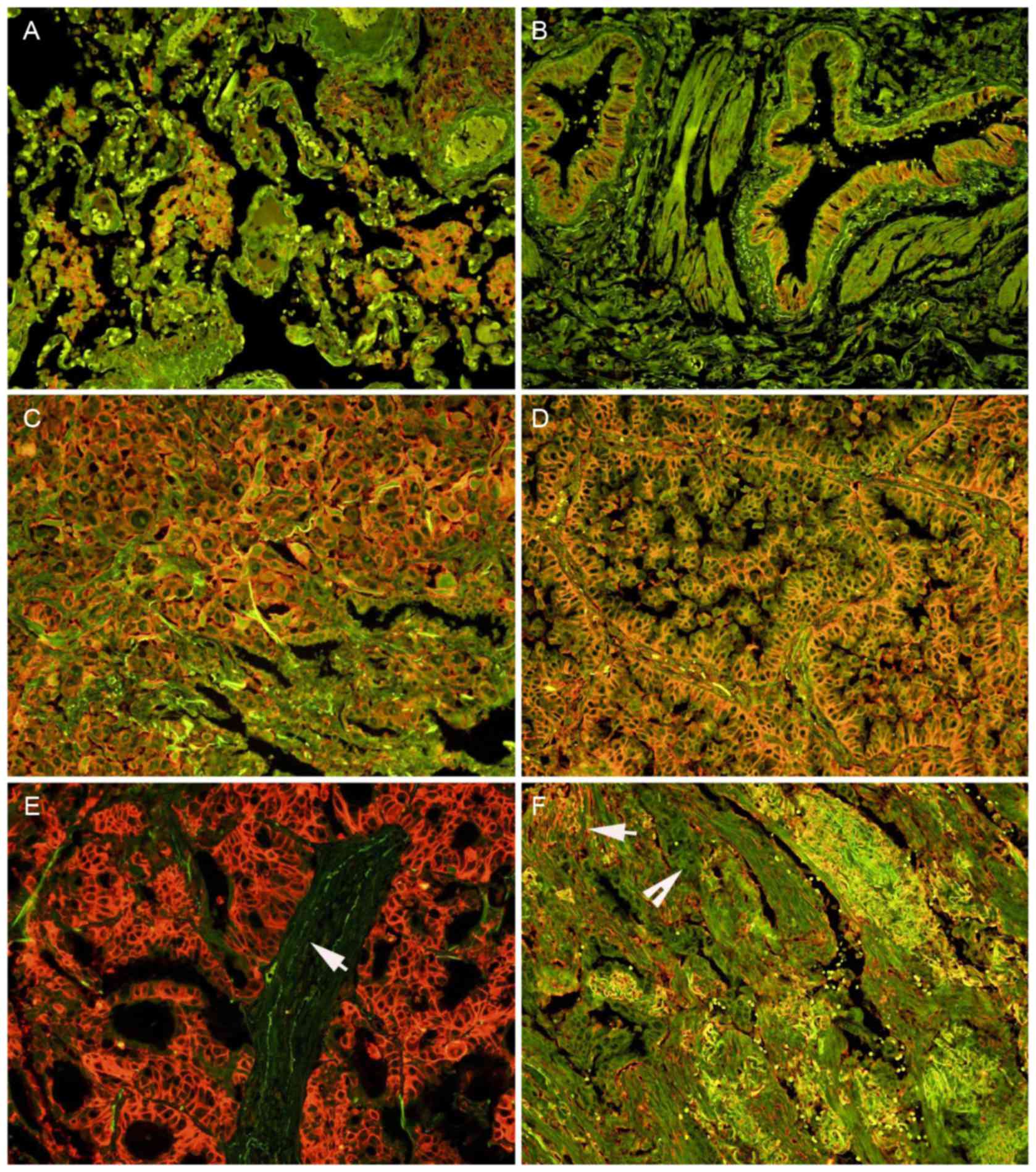
Expression of MCT-4 in normal lung and
AC tissues
The expression of MCT-4 protein was detected in the
cell membrane and cytoplasm of some of the alveolar macrophages
(Fig. 2A) and bronchial epithelial
cells (Fig. 2B), but no expression of
MCT-4 protein was detected in the alveolar epithelial cells
(Fig. 2A), as identified using
QD-IHC. Positive MCT-4 signals were predominantly observed on the
cell membrane, with weak staining also visible in the cytoplasm of
the tumor cells (Fig. 2C and D).
Notably, positive signals were not identified in stromal cells in a
number of cases (Fig. 2E), whereas
they were visible in others (Fig.
2F). A total of 25 (17.1%) cases were determined to exhibit
high MCT-4 expression, and 121 cases (82.9%) exhibited low MCT-4
expression from the 146 lung AC tissues. No high MCT-4 expression
(>3.5) was detected in the corresponding normal lung
tissues.
Clinical significance and prognostic
value of MCT-4 protein
For analyzing the effect of MCT-4 expression on
tumor aggressiveness, the χ2 test or Fisher's exact test
was used to evaluate the association between MCT-4 expression and
clinicopathological features (Table
II). A significant correlation was detected between high MCT-4
expression and advanced depth of invasion (T3/4 vs. T1/2; P=0.034).
However, no significant associations were identified between MCT-4
expression levels and any other clinicopathological variables.
| Table II.Correlations between MCT-4 expression
and clinicopathological parameters of lung AC. |
Table II.
Correlations between MCT-4 expression
and clinicopathological parameters of lung AC.
|
|
| Expression of
MCT-4 |
|---|
|
|
|
|
|---|
| Features | n | Low, n (%) | High, n (%) | P-value |
|---|
| Gender |
|
|
| 0.145 |
|
Male | 80 | 63 (78.8) | 17 (21.2) |
|
|
Female | 66 | 58 (87.9) | 8 (12.1) |
|
| Age, years |
|
|
| 0.715 |
|
≤63 | 98 | 82 (83.7) | 16 (16.3) |
|
|
>63 | 48 | 39 (81.3) | 9 (18.7) |
|
| Invasion depth |
|
|
| 0.034 |
|
T1/2 | 129 | 110 (85.3) | 19 (14.7) |
|
|
T3/4 | 17 | 11 (64.7) | 6 (35.3) |
|
| Lymph node
metastasis |
|
|
| 0.746 |
| N0 | 86 | 72 (83.7) | 14 (16.3) |
|
|
N1/2/3/X | 60 | 49 (81.7) | 11 (18.3) |
|
| Distant
metastasis |
|
|
| 0.426 |
| M0 | 143 | 118 (82.5) | 25 (17.5) |
|
| M1 | 3 | 3 (100.0) | 0 (0.0) |
|
| TNM stage |
|
|
| 0.948 |
|
I/II | 122 | 101 (82.8) | 21 (17.2) |
|
|
III/IV | 24 | 20 (83.3) | 4 (16.7) |
|
| Histological
type |
|
|
| 0.256 |
|
Invasive AC | 131 | 107 (81.7) | 24 (18.3) |
|
| Variant
invasive AC | 15 | 14 (93.3) | 1 (6.7) |
|
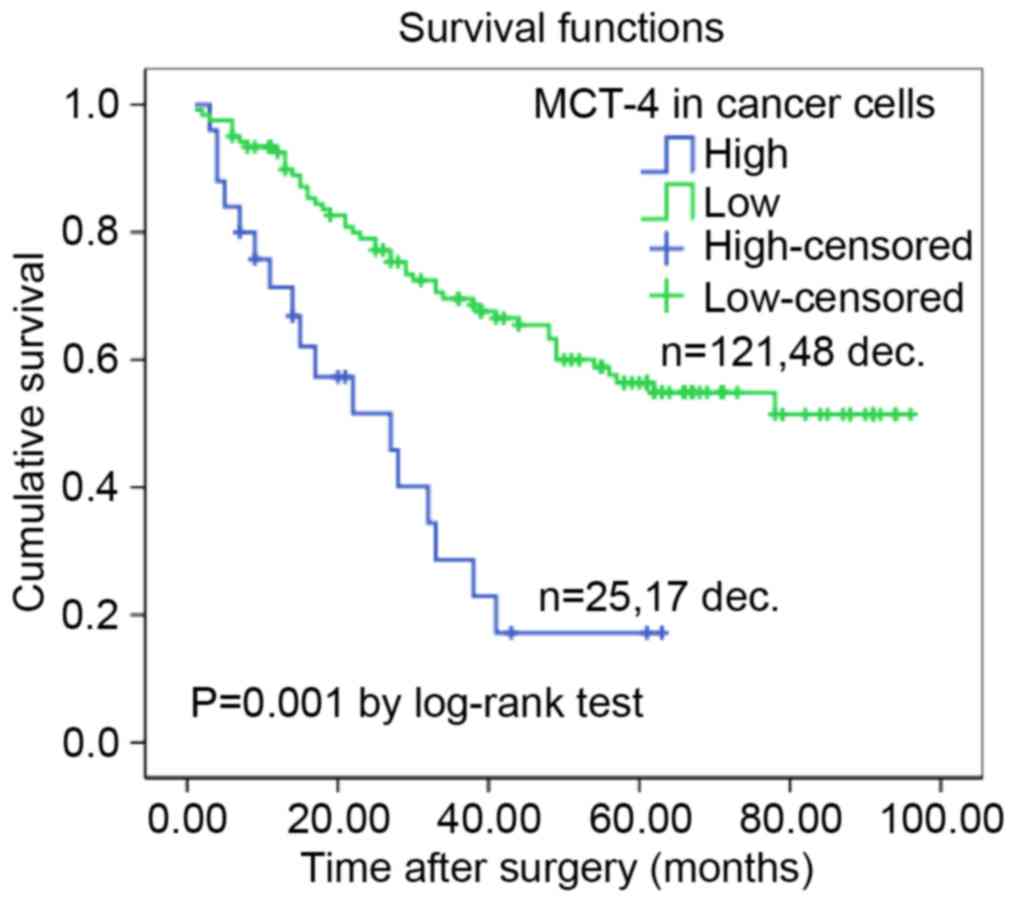
Additionally, the Kaplan-Meier method with the
log-rank test was performed to estimate a survival curve for OS
rate and assess the difference in survival rate between patients
with high and low MCT-4 expression levels. The mean OS time of the
high MCT-4 expression group was only 27.4 months (95% CI,
18.995–35.902 months), whereas the low MCT-4 expression level was
64.8 months (95% CI, 58.072–71.584). After the final follow-up, the
survival rate of the high MCT-4 expression group was 31.8%, which
was decreased compared with that of the group with low MCT-4
expression (60.3%; Fig. 3). The
survival curve indicated that high MCT-4 expression in lung AC
significantly predicts a decreased likelihood of survival (P=0.001;
Fig. 3).
Furthermore, a Cox proportional hazard regression
model was conducted for OS to investigate independent prognostic
factors of lung AC patients. From a univariate analysis, it was
identified that clinicopathological features including MCT-4
expression levels, depth of invasion, lymph node metastasis and TNM
stage were significantly associated with the OS of lung AC patients
(P=<0.001, P=0.026, P=0.018 and P=0.005, respectively; Table III). However, other
clinicopathological features failed to independently predict lung
AC prognosis (Table III). The
results indicated that low MCT-4 expression diminished the risk of
mortality significantly compared to high MCT-4 expression in lung
AC patients. In addition, a multivariate analysis was subsequently
performed. As indicated by Table
III, only MCT-4 expression (HR, 3.192; 95% CI, 1.804–5.646;
P=0.001) and TNM stage (HR, 2.084; 95% CI, 1.217–3.569; P=0.007)
were statistically significant independent predictors for lung AC
prognosis.
| Table III.Cox proportional hazard models on the
overall survival rate of lung AC patients. |
Table III.
Cox proportional hazard models on the
overall survival rate of lung AC patients.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Factor | P-value | HR (95% CI) | P-value | HR (95% CI) |
|---|
| Gender (male vs.
female) | 0.983 | 1.005
(0.616–1.640) | 0.855 | 0.922
(0.386–2.202) |
| Age, years (<63
vs. ≥63) | 0.055 | 0.618
(0.378–1.010) | 0.115 | 2.287
(0.817–6.402) |
| MCT-4 expression
(low vs. high) | 0.000 | 3.267
(1.851–5.767) | 0.001 | 3.192
(1.804–5.646) |
| Invasion depth
(T1/2 vs. T3/4) | 0.026 | 0.501
(0.272–0.921) | 0.314 | 1.433
(0.711–2.887) |
| Lymph node
metastasis (N0 vs. N1/2/3/X) | 0.018 | 0.554
(0.340–0.904) | 0.057 | 0.272
(0.071–1.041) |
| Distant metastasis
(M0 vs. M1) | 0.948 | 1.048
(1.048–4.288) | 0.633 | 0.821
(0.365–1.847) |
| TNM stage (I/II vs.
III/IV) | 0.005 | 2.150
(1.258–3.674) | 0.007 | 2.084
(1.217–3.569) |
| Histological type
(invasive AC vs. variant invasive AC) | 0.627 | 1.215
(0.554–2.663) | 0.431 | 0.502
(0.090–2.791) |
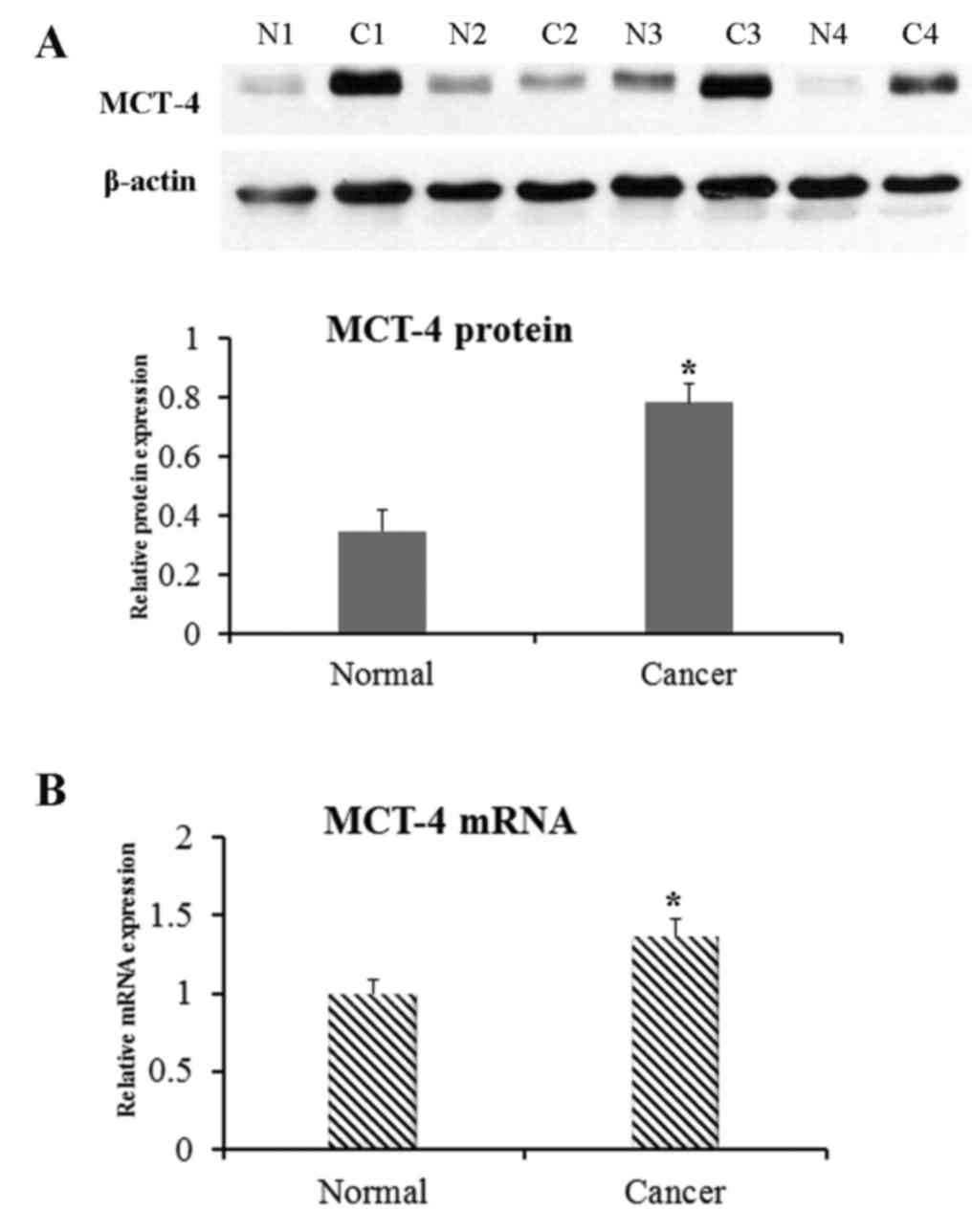
MCT-4 protein and mRNA expression
MCT-4 protein expression in lung AC was revealed to
be significantly increased based on the western blotting results
(P=0.046 compared to normal lung tissues; Fig. 4A). Additionally, MCT-4 mRNA level, as
detected by RT-qPCR, was significantly higher in lung AC compared
with normal lung tissue (P=0.035; Fig.
4B).
Discussion
In the present study, it was revealed that MCT-4
immunoreactivity was predominantly observed at the cell membrane
and cytoplasm of the tumor cells, as well as in the alveolar
macrophages and bronchial epithelium. Additionally, it was mildly
expressed in stromal cells of lung AC tissues and negative in
alveolar epithelial cells. The results suggested that MCT-4 protein
and mRNA level were significantly increased in AC tissue, compared
with corresponding normal lung tissues. High MCT-4 level was also
associated with an advanced (T3/4) depth of invasion, and high
expression in tumor cells predicted poor prognosis. Based on this
data, MCT-4 may be a candidate therapeutic target for lung AC
patients.
Lung AC is one of the most deadly and widespread
diseases and remains a significant concern for public health
(1). In recent years, the clinical
and prognostic value of MCT-4 has been identified for certain types
of cancer (23–27), and the tumor-promoting role of high
MCT-4 expression has also been clarified (24,26,27,34).
Although experimental evidence appears to indicate that MCTs are
potential targets for cancer therapy (35,36), the
function of these membrane proteins in lung AC is not understood
clearly. Therefore, the present study attempted to clarify the
effect of MCT-4 on prognosis in lung AC. For this purpose, the
expression of MCT-4 in lung ACs and corresponding normal lung
tissues was analyzed.
In the present study, 17.1% (25/146) of lung AC
cases exhibited high MCT-4 expression, which was lower than a
previous report in which 48.78% (20/41) of lung AC cases exhibited
high MCT-4 expression (34). This
discrepancy may be explained by different IHC scoring methods.
Positive rates of MCT-4 protein in lung AC samples were increased,
compared to normal lung tissues in the present study, which
demonstrated that there is a different mechanism for metabolism
between normal lung and lung AC cells. Western blot results
confirmed the specificity of the MCT-4 antibodies, providing
further evidence for the validity of the data of the present study.
It was also identified that high MCT-4 level is associated with an
advanced depth of invasion (T3/4) and that a high expression level
of MCT-4 was an independent prognostic marker for a poor prognosis
in lung AC. Another study has reported that high GLUT1 and MCT-4
expression levels are closely associated with poor disease-specific
survival (DSS) time in lung ACs, but not in lung squamous cell
carcinomas (34). In another study,
MCT-4 expression in cancer cells is significantly associated with a
poor DSS time in NSCLC (37). The
aforementioned results imply that MCT-4 may be a candidate
therapeutic target for the treatment of patients with lung AC.
MCT-4 mediates the efflux of lactate, which is
produced during glycolysis, across cell membranes (38). A previous study demonstrated that
cells that expressed MCT-4 exhibit increased invasive behavior
compared with cells that no express MCT-4 (39). Tumors consist of stromal cells and
tumor cells; the former may constitute >50% of the tumor mass.
There is evidence to suggest that stromal cells serve an important
function in tumor metastasis and invasion through tumor-stroma
interactions (40). It has recently
reported that stromal MCT-4 has promise as a biomarker for
predicting the prognosis of patients with gastric cancer (41). MCT-4 expression in stroma is also
independently associated with a worse biochemical failure-free
survival time in prostate cancer (42). In the present study, weak MCT-4
expression was detected in the stroma of only a small number of
lung AC samples; it may be difficult to meaningfully analyze this
further from the low number of samples. However, in a previously
study, decreased expression of MCT-1 in cancer cells, decreased
expression of stromal MCT-2 and −3, and increased expression of
stromal MCT-1 have been identified as significant independent
prognostic markers for poor DSS in NSCLC, although no significant
association is observed between stromal MCT-4 expression and DSS
time in NSCLC (37). Thus, many
aspects of the association between stromal MCT-4 expression and the
invasive activity of lung AC cells have yet to be explored.
In summary, high expression of MCT-4 is associated
with a high depth of invasion (T3/4) of lung ACs. Expression of
MCT-4 protein in tumor cells predicts a poor prognosis for patients
with lung AC. Multivariate analysis demonstrated that high
expression of MCT-4 is an independent poor prognostic predictor for
lung AC patients. The results suggest a novel biomarker for lung
AC, and are in agreement with previous data indicating that MCT-4
may mediate the transport of lactate from tumor cells to the
extracellular matrix (12,43). The transport of lactate, in addition
to protons exported by proton pumps, increase the acidity of the
extracellular environment (12).
Consequently, a number of cytokines from the extracellular membrane
are activated via MMPs or other proteases. In turn, these cytokines
mediate neovascularization, cell survival and
epithelial-mesenchymal transition, to assist the survival of cancer
cells (44). Furthermore, patients
with lung AC with high MCT-4 expression may benefit from MCT-4
inhibitors or other novel treatment approaches based on MCT-4
expression. It is necessary to conduct further studies and
investigate the molecular mechanisms associated with MCT-4
expression to develop biomarkers and prospective clinical trials to
fully explore the significance of MCT-4 level in lung AC
prognosis.
Acknowledgements
The present study was supported by grants from the
National Natural Science Foundation of China (grant no. 30900652)
and Shenzhen R&D Technology Research Projects (grant no.
JCYJ20140416122812024).
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA A Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar
|
|
2
|
Thomas A, Liu SV, Subramaniam DS and
Giaccone G: Refining the treatment of NSCLC according to
histological and molecular subtypes. Nat Rev Clin Oncol.
12:511–526. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sica G, Yoshizawa A, Sima CS, Azzoli CG,
Downey RJ, Rusch VW, Travis WD and Moreira A: A grading system of
lung adenocarcinomas based on histologic pattern is predictive of
disease recurrence in stage I tumors. Am J Surg Patho.
34:1155–1162. 2010. View Article : Google Scholar
|
|
4
|
Alberg AJ, Ford JG and Samet JM: American
College of Chest Physicians: Epidemiology of lung cancer: ACCP
evidence-based clinical practice guidelines. Chest. 132:29S–55S.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Travis WD, Brambilla E, Noguchi M,
Nicholson AG, Geisinger K, Yatabe Y, Powell CA, Beer D, Riely G,
Garg K, et al: International Association for the Study of Lung
Cancer/American Thoracic Society/European Respiratory Society:
International multidisciplinary classification of lung
adenocarcinoma: executive summary. Proc Am Thorac Soc. 8:381–385.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sterlacci W, Savic S, Schmid T, Oberaigner
W, Auberger J, Fiegl M and Tzankov A: Tissue-sparing application of
the newly proposed IASLC/ATS/ERS classification of adenocarcinoma
of the lung shows practical diagnostic and prognostic impact. Am J
Clin Pathol. 137:946–956. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bissell MJ and Radisky D: Putting tumours
in context. Nat Rev Cancer. 1:46–54. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mueller MM and Fusenig NE: Friends or
foes-bipolar effects of the tumour stroma in cancer. Nat Rev
Cancer. 4:839–849. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dvorak HF, Weaver VM, Tlsty TD and Bergers
G: Tumor microenvironment and progression. J Surg Oncol.
103:468–474. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Vaupel P, Kallinowski F and Okunieff P:
Blood flow, oxygen and nutrient supply and metabolic
microenvironment of human tumors: A review. Cancer Res.
49:6449–6465. 1989.PubMed/NCBI
|
|
11
|
Izumi H, Torigoe T, Ishiguchi H, Uramoto
H, Yoshida Y, Tanabe M, Ise T, Murakami T, Yoshida T, Nomoto M and
Kohno K: Cellular pH regulators: Potentially promising molecular
targets for cancer chemotherapy. Cancer Treat Rev. 29:541–549.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pinheiro C, Longatto-Filho A,
Azevedo-Silva J, Casal M, Schmitt FC and Baltazar F: Role of
monocarboxylate transporters in human cancers: State of the art. J
Bioenerg Biomembr. 44:127–139. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Halestrap AP and Price NT: The
proton-linked monocarboxylate transporter (MCT) family: Structure,
function and regulation. Biochem J. 343:281–299. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Broer S, Bröer A, Schneider H, Stegen C,
Halestrap A and Deitmer J: Characterization of the high-affinity
monocarboxylate transporter MCT2 in Xenopus laevis oocytes. Biochem
J. 341:529–535. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Grollman EF, Philp NJ, McPhie P, Ward RD
and Sauer B: Determination of transport kinetics of chick MCT3
monocarboxylate transporter from retinal pigment epithelium by
expression in genetically modified yeast. Biochemistry.
39:9351–9357. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dimmer KS, Friedrich B, Lang F, Deitmer JW
and Bröer S: The low-affinity monocarboxylate transporter MCT4 is
adapted to the export of lactate in highly glycolytic cells.
Biochem J. 350:219–227. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fox JEM, Meredith D and Halestrap AP:
Characterisation of human monocarboxylate transporter 4
substantiates its role in lactic acid efflux from skeletal muscle.
J Physiol. 529:285–293. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Koukourakis MI, Giatromanolaki A, Harris
AL and Sivridis E: Comparison of metabolic pathways between cancer
cells and stromal cells in colorectal carcinomas: A metabolic
survival role for tumor-associated stroma. Cancer Res. 66:632–637.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lin RY, Vera JC, Chaganti RS and Golde DW:
Human monocarboxylate transporter 2 (MCT2) is a high affinity
pyruvate transporter. J Biol Chem. 273:28959–28965. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lambert DW, Wood IS, Ellis A and
Shirazi-Beechey S: Molecular changes in the expression of human
colonic nutrient transporters during the transition from normality
to malignancy. Br J Cancer. 86:1262–1269. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pinheiro C, Longatto-Filho A, Scapulatempo
C, Ferreira L, Martins S, Pellerin L, Rodrigues M, Alves VA,
Schmitt F and Baltazar F: Increased expression of monocarboxylate
transporters 1, 2 and 4 in colorectal carcinomas. Virchows Archiv.
452:139–146. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Juel C and Halestrap AP: Lactate transport
in skeletal muscle-role and regulation of the monocarboxylate
transporter. J Physiol. 517:633–642. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pinheiro C, Reis RM, Ricardo S,
Longatto-Filho A, Schmitt F and Baltazar F: Expression of
monocarboxylate transporters 1, 2 and 4 in human tumours and their
association with CD147 and CD44. J Biomed Biotechnol.
2010:4276942010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nakayama Y, Torigoe T, Inoue Y, Minagawa
N, Izumi H, Kohno K and Yamaguchi K: Prognostic significance of
monocarboxylate transporter 4 expression in patients with
colorectal cancer. Exp Ther Med. 3:25–30. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kim MJ, Kim DH, Jung WH and Koo JS:
Expression of metabolism-related proteins in triple-negative breast
cancer. Int J Clin Exp Pathol. 7:301–312. 2013.PubMed/NCBI
|
|
26
|
Zhu J, Wu YN, Zhang W, Zhang XM, Ding X,
Li HQ, Geng M, Xie ZQ and Wu HM: Monocarboxylate transporter 4
facilitates cell proliferation and migration and is associated with
poor prognosis in oral squamous cell carcinoma patients. PLoS One.
9:e879042014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pértega-Gomes N, Vizcaíno JR,
Miranda-Gonçalves V, Pinheiro C, Silva J, Pereira H, Monteiro P,
Henrique RM, Reis RM, Lopes C and Baltazar F: Monocarboxylate
transporter 4 (MCT4) and CD147 overexpression is associated with
poor prognosis in prostate cancer. BMC Cancer. 11:3122011.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sobin LH, Gospodarowicz MK and Wittekind
C: International Union against CancerTNM classification of
malignant tumours. 7th. Chichester, Hoboken NJ: Wiley-Blackwell;
2010
|
|
29
|
Kononen J, Bubendorf L, Kallionimeni A,
Bärlund M, Schraml P, Leighton S, Torhorst J, Mihatsch MJ, Sauter G
and Kallioniemi OP: Tissue microarrays for high-throughput
molecular profiling of tumor specimens. Nat Med. 4:844–847. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Li M, Chen H, Diao L, Zhang Y, Xia C and
Yang F: Caveolin-1 and VEGF-C promote lymph node metastasis in the
absence of intratumoral lymphangiogenesis in non-small cell lung
cancer. Tumori. 96:7342010.PubMed/NCBI
|
|
31
|
Chen H, Xue J, Zhang Y, Zhu X, Gao J and
Yu B: Comparison of quantum dots immunofluorescence histochemistry
and conventional immunohistochemistry for the detection of
caveolin-1 and PCNA in the lung cancer tissue microarray. J Mol
Histol. 40:261–268. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhao X, He Y, Gao J, Fan L, Li Z, Yang G
and Chen H: Caveolin-1 expression level in cancer associated
fibroblasts predicts outcome in gastric cancer. PLoS One.
8:e591022013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Meijer TW, Schuurbiers OC, Kaanders JH,
Looijen-Salamon MG, de Geus-Oei LF, Verhagen AF, Lok J, van der
Heijden HF, Rademakers SE, Span PN and Bussink J: Differences in
metabolism between adeno-and squamous cell non-small cell lung
carcinomas: Spatial distribution and prognostic value of GLUT1 and
MCT4. Lung Cancer. 76:316–323. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Mathupala SP, Parajuli P and Sloan AE:
Silencing of monocarboxylate transporters via small interfering
ribonucleic acid inhibits glycolysis and induces cell death in
malignant glioma: An in vitro study. Neurosurgery. 55:1410–1419.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sonveaux P, Végran F, Schroeder T, Wergin
MC, Verrax J, Rabbani ZN, De Saedeleer CJ, Kennedy KM, Diepart C,
Jordan BF, et al: Targeting lactate-fueled respiration selectively
kills hypoxic tumor cells in mice. J Clin Invest. 118:3930–3942.
2008.PubMed/NCBI
|
|
37
|
Eilertsen M, Andersen S, Al-Saad S,
Kiselev Y, Donnem T, Stenvold H, Pettersen I, Al-Shibli K,
Richardsen E, Busund LT and Bremnes RM: Monocarboxylate
transporters 1–4 in NSCLC: MCT1 is an independent prognostic marker
for survival. PLoS One. 9:e1050382014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Garcia CK, Goldstein JL, Pathak RK,
Anderson RG and Brown MS: Molecular characterization of a membrane
transporter for lactate, pyruvate and other monocarboxylates:
Implications for the Cori cycle. Cell. 76:865–873. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Izumi H, Takahashi M, Uramoto H, Nakayama
Y, Oyama T, Wang KY, Sasaguri Y, Nishizawa S and Kohno K:
Monocarboxylate transporters 1 and 4 are involved in the invasion
activity of human lung cancer cells. Cancer Sci. 102:1007–1013.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Lorusso G and Rüegg C: The tumor
microenvironment and its contribution to tumor evolution toward
metastasis. Histochem Cell Biol. 130:1091–1103. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhao Z, Han F, He Y, Yang S, Hua L, Wu J
and Zhan W: Stromal-epithelial metabolic coupling in gastric
cancer: Stromal MCT4 and mitochondrial TOMM20 as poor prognostic
factors. Eur J Surg Oncol. 40:1361–1368. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Andersen S, Solstad Ø, Moi L, Donnem T,
Eilertsen M, Nordby Y, Ness N, Richardsen E, Busund LT and Bremnes
RM: Organized metabolic crime in prostate cancer: The coexpression
of MCT1 in tumor and MCT4 in stroma is an independent
prognosticator for biochemical failure. Urol Oncol. 33:338.e9–17.
2015. View Article : Google Scholar
|
|
43
|
Sanità P, Capulli M, Teti A, Galatioto GP,
Vicentini C, Chiarugi P, Bologna M and Angelucci A: Tumor-stroma
metabolic relationship based on lactate shuttle can sustain
prostate cancer progression. BMC Cancer. 14:154–167. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
San-Millán I and Brooks GA: Reexamining
cancer metabolism: Lactate production for carcinogenesis could be
the purpose and explanation of the Warburg Effect. Carcinogenesis.
38:119–133. 2017.PubMed/NCBI
|