Introduction
Ovarian cancer (OC) represents a diverse group of
malignant diseases that arise from epithelial cells, stromal cells
or ova, and even from the fallopian tube and endometrium (1). Among these forms of OC, epithelial
ovarian cancer accounts for 90% (2).
According to histopathological classification, almost 75% of OC
cases are serous and 3% of all OC cases are mucinous (3). As 70% of cases are diagnosed at an
advanced stage, the fatality-to-case ratio of OC is high, even
following surgical debulking and adjuvant chemotherapy (4). It is the most lethal gynecologic
disease, with a 5-year survival rate of only 50%. OC affected
22,280 females in the United States of America in 2016 and caused
14,240 mortalities according to a report from the National Cancer
Institute (National Institutes of Health, Bethesda, MA, USA)
(5).
Although OC is one of the most chemo-sensitive types
of solid tumors and is associated with a high initial response,
chemoresistance and recurrence of OC are serious problems
associated with the current treatments (6,7).
Therefore, novel and effective therapies for OC are urgently
required. Cancer immunotherapy involves utilizing the immune system
of the patient to attack tumor cells by targeting tumor-specific
antigens. These strategies, which include therapeutic vaccines,
immunomodulators, immune checkpoint inhibitors and adoptive T cell
transfer, have yielded breakthroughs in the treatment of certain
types of cancer (8,9). OC is an ideal candidate for
immunotherapy due to the good performance of immunoregulatory cells
including T helper cells, the short average duration of the
decrease in the number of immunoregulatory cells following standard
cytotoxic therapy and the satisfactory nutritional status of the
patients even in the late course of OC; however, in general,
immune-based OC therapies have only been modestly successful
(8–10). Previously, the successful performance
of immune checkpoints, including the programmed cell death 1 (PD-1)
receptor, has attracted attention in the search for novel
treatments for certain types of cancer (11).
V-domain immunoglobulin suppressor of T cell
activation (VISTA) is a novel negative immune checkpoint regulator
that is homologous to programmed cell death ligand 1 (PD-L1)
(12). VISTA is highly expressed on
hematopoietic cells, with the greatest densities in myeloid and
granulocytic cells, and weaker expression on cluster of
differentiation (CD)4+ and CD8+ T cells (13). Similar to PD-L1, VISTA functions to
inhibit T cell activation to maintain tolerance and limit
immunopathology (14). The inhibition
of VISTA weakens the suppressive function of T cells, resulting in
a decrease in tumor growth (14,15). In
murine fibrosarcoma models, VISTA overexpression on tumor cells was
demonstrated to induce immune protection against the growth of
control tumor cells (12).
Additionally, the use of an anti-VISTA monoclonal antibody in
murine cancer models was suggested to impair tumor growth, with
particularly marked results when used in combination with a tumor
vaccine (12). These observation
indicate that VISTA is a promising target in cancer therapy
(16).
However, to the best of our knowledge, the VISTA
expression in OC and evidence for an association between VISTA and
OC has not yet been demonstrated. Therefore, in the present study,
the expression VISTA in tumor tissues samples from patients with OC
at different stages was examined, and the prognostic value of VISTA
in different types of OC was evaluated.
Materials and methods
Patients and tissue samples
In this retrospective study, archived formalin-fixed
paraffin-embedded OC specimens from 65 patients with OC treated
between June 2006 and June 2012 were obtained from the Pathology
Department of West China Second University Hospital, Sichuan
University (Chengdu, China). Patients were included based on the
following criteria: i) Accessible clinical data and at least 5
years of routine follow-ups; ii) no chemotherapy or radiation
therapy prior to oophorectomy; and iii) OC confirmed by
histopathological diagnosis. The characteristics of patients,
including age (age range, 19–80 years; median age, 53 years) and
stage of OC, are summarized in Table
I.
 | Table I.VISTA expression associated with
clinicopathological characteristics in patients with ovarian cancer
(n=65). |
Table I.
VISTA expression associated with
clinicopathological characteristics in patients with ovarian cancer
(n=65).
|
|
| VISTA-positive tumor
cells | VISTA-positive
ICs/200 ICs | Vascular endothelial
cells |
|---|
|
|
|
|
|
|
|---|
|
|
| Low, n (%) | High, n (%) |
| Low, n (%) | High, n (%) |
| Negative, n (%) | Positive, n (%) |
|
|---|
|
|
|
|
|---|
| Characteristics | Total (%) 65 | 49 (75.38) | 16 (24.62) | P-value | 36 (55.38) | 29 (44.62) | P-value | 50 (76.92) | 15 (23.08) | P-value |
|---|
| Age, years |
|
|
| 0.57 |
|
| 0.221 |
|
| 1 |
| ≤55 | 37 (56.92) | 29 | 8 |
| 23 | 14 |
| 28 | 9 |
|
|
>55 | 28 (43.08) | 20 | 8 |
| 13 | 15 |
| 22 | 6 |
|
| Stage |
|
|
| 0.043a |
|
| 0.047a |
|
| 0.075 |
|
I+II | 27 (41.54) | 24 | 3 |
| 19 | 8 |
| 24 | 3 |
|
|
III+IV | 38 (58.46) | 25 | 13 |
| 17 | 21 |
| 26 | 12 |
|
| Grade |
|
|
| 0.718 |
|
| 0.52 |
|
| 0.706 |
| Low
(G1+G2) | 11 (16.92) | 9 | 2 |
| 5 | 6 |
| 8 | 3 |
|
| High
(G3) | 54 (83.08) | 40 | 14 |
| 31 | 23 |
| 42 | 12 |
|
| Lymph node
metastasis |
|
|
| 0.015a |
|
| 0.042a |
|
| 0.001a |
|
Negative | 42 (64.62) | 36 | 6 |
| 28 | 14 |
| 38 | 4 |
|
|
Positive | 23 (35.38) | 13 | 10 |
| 8 | 15 |
| 12 | 11 |
|
| Histologic
type |
|
|
| 0.774 |
|
| 0.212 |
|
| 0.238 |
| Serous
adenocarcinoma | 26 (40.00) | 19 | 7 |
| 17 | 9 |
| 20 | 6 |
|
|
Non-serous adenocarcinoma | 39 (60.00) | 30 | 9 |
| 19 | 20 |
| 30 | 9 |
|
| Primary
therapy |
|
|
| 0.252 |
|
| 0.622 |
|
| 0.566 |
|
Surgery | 4 (6.15) | 2 | 2 |
| 3 | 1 |
| 4 | 0 |
|
| Surgery
+ others | 61 (93.85) | 47 | 14 |
| 33 | 28 |
| 46 | 15 |
|
| Residual tumor |
|
|
| 0.06 |
|
| 0.219 |
|
| 0.769 |
|
Negative | 35 (53.85) | 28 | 7 |
| 22 | 13 |
| 26 | 9 |
|
|
Positive | 30 (46.15) | 17 | 13 |
| 14 | 16 |
| 24 | 6 |
|
| Tumor-specific
survival, months |
|
|
| 0.594 |
|
| 0.232 |
|
| 0.459 |
|
Total/events/censored | 65/32/33 | 49/23/26 | 16/9/7 |
| 36/16/20 | 29/16/13 |
| 15/9/6 | 50/23/27 |
|
| Median
survival | 52.3±3.9 | 53.3±4.5 | 49.1±7.6 |
| 55.9±5.0 | 46.5±5.7 |
| 45.7±7.9 | 53.7±4.3 |
|
| 95%
confidence interval |
44.8–60.0 |
44.6–62.1 |
34.3–64.0 |
|
46.2–65.5 |
35.3–57.8 |
|
30.1–61.2 |
45.3–62.2 |
|
The present study was approved by the Ethics
Committee of West China Second Hospital of Sichuan University and
informed consent was obtained from all patients undergoing
surgery.
Immunohistochemistry (IHC)
VISTA expression in OC tissues was analyzed
immunohistochemically. The OC tissues were fixed in 10% (v/v)
formalin at room temperature for 48 h once being removed from the
patients during surgery, and embedded in paraffin until use. The
paraffin-embedded tissues were sectioned (thickness, 3–4 µm) and
mounted on poly-l-lysine-coated slides. Firstly, samples were
incubated at 37°C overnight prior to being deparaffinized with 99%
(v/v) xylene and sequentially rehydrated in a graded ethanol series
(100, 95, 80 and 50%). Slides were then rinsed twice with PBS
containing 0.1% Tween-20 (PBST). High-temperature antigen retrieval
was performed using 10 mmol/l boiling (~95°C) sodium citrate buffer
at pH 6.0 for 15 min. To block the endogenous peroxidase activity,
samples were immersed in 3% hydrogen peroxide for 30 min at room
temperature, followed by incubation in 5% bovine serum albumin
(BSA) (cat. no. 9048-46-8; Sigma-Aldrich; Merck KGaA, Darmstadt,
Germany) for 30 min to reduce non-specific binding. Slides were
then incubated with a primary monoclonal rabbit anti-human VISTA
antibody (cat. no. 64953, Cell Signaling Technology, Inc., Danvers,
MA, USA; 1:50 dilution in 5% BSA) at 4°C overnight. Following
rinsing in PBST 3 times for 5 min each, slides were incubated with
a secondary horseradish peroxidase-conjugated goat anti-rabbit IgG
(cat. no. A0208; Beyotime Institute of Biotechnology, Haimen,
China) for 1 h at room temperature. Slides were then rinsed
thoroughly in PBST 3 times for 5 min each prior to incubation with
streptavidin peroxidase for 30 min at room temperature. Subsequent
to thorough rinsing with PBST three times, slides were then
incubated with 1% (w/v) 3,3′-diaminobenzidine solution to develop
color for 10 min at room temperature. Finally, slides were
counter-stained with 0.5% (w/v) hematoxylin at room temperature for
5 min and mounted with neutral balsam prior to being examined under
a Leica DM1000 light microscope at a magnification of ×400 (Leica
Microsystems GmbH, Wetzlar, Germany). Stained cell cytoplasm was
considered to indicate positivity for VISTA expression, and
specimens from healthy ovarian tissues were used as controls. The
healthy controls (age range, 41 to 56; median age, 47.4) in the
present study were females from West China Second University
Hospital, Sichuan University with benign gynecological diseases
including uterine myoma or mesosalpinx cysts. Small pieces of
normal ovarian tissues were obtained subsequent to provision of
written informed consent prior to laparoscopic surgery. Patients
were fully informed of the disadvantages of the procedure and the
applications of the tissues prior to surgery.
Evaluation of VISTA protein
expression
For evaluation of VISTA protein expression in OC
tissues, a reproducible semi-quantitative method that considered
the staining intensity (regardless of the positive subcellular
location) and numbers of positive tumor cells was adopted as
described previously (17,18). In brief, the VISTA staining intensity
was classified as follows: 0, negative staining; 1, weak staining
(light yellow); 2, moderate staining (yellow-brown); and 3, strong
staining (brown). In the same tumor tissue with different staining
intensities, only the highest intensity was recorded. The
percentage of VISTA-positive cells was also scored as follows: 0,
no stained cells; 1, 1–30% positive cells; 2, 31–60% positive
cells; 3, 61–90% positive cells; 4, 91–100% positive cells. The
final immunoreactivity score (IS) of each sample was calculated by
adding the scores for the staining intensity and the percentage of
VISTA-positive cells. Scores of 0–3 were defined as ‘negative
expression’ (−), scores of 4–5 as ‘weakly positive expression’ (+),
and scores of 6–7 as ‘strongly positive expression’ (++). In
addition, overall scores were dichotomized into two groups: Low
expression (IS <5); and high expression (IS ≥5) in OC
samples.
The proportion of VISTA-positive immune cells
(ICs)/200 ICs in the intratumoral hotspot regions, where the
highest density of VISTA-positive ICs accumulated, was considered
in the analysis, as described previously (19). Patients with OC with ≤35
VISTA-positive ICs were classified as exhibiting low VISTA
expression in terms of the proportion of VISTA-positive ICs/200
ICs. Immunostaining of vascular endothelial cells (VECs) was graded
as present or absent. Each sample was scored by two of the authors
with assitance from a pathologist (West China Second University
Hospital of Sichuan University).
Statistical analysis
In the present study, patients were followed until
mortality or to the end of the follow-up period (November 2012).
The overall survival (OS) was calculated from the date of the
initial diagnosis to the date of mortality or the last follow-up.
Patients were censored at the date of the last visit or at the time
of mortality due to non-OC-associated causes.
The correlation between clinicopathological
characteristics and VISTA expression in OC was analyzed using the
Pearson's χ2 test or Fisher's exact test with
SPSS v22 software (IBM Corp., Armonk, NY, USA). Kaplan-Meier 5-year
survival curves were generated compared using log-rank tests to
assess OS. Univariate and multivariate Cox proportional hazard
models were used to estimate the associations between VISTA
expression and clinical characteristics with OS. P<0.05
(two-tailed) was considered to indicate a statistically significant
difference.
Results
Patient characteristics
A total of 65 patients with OC (aged 19–80 years,
median 53 years) were included in the present study. At the end of
the 6-year study period, 33 cases of survival were censored, while
the other 32 events were OC-associated mortalities. The median
survival time of this group was 52.3±3.9 months (95% CI, 44.8–60.0
months) and the 5-year OS rate was 47.7% (Fig. 1). The characteristics of the patients
included in the present study are summarized in Table I.
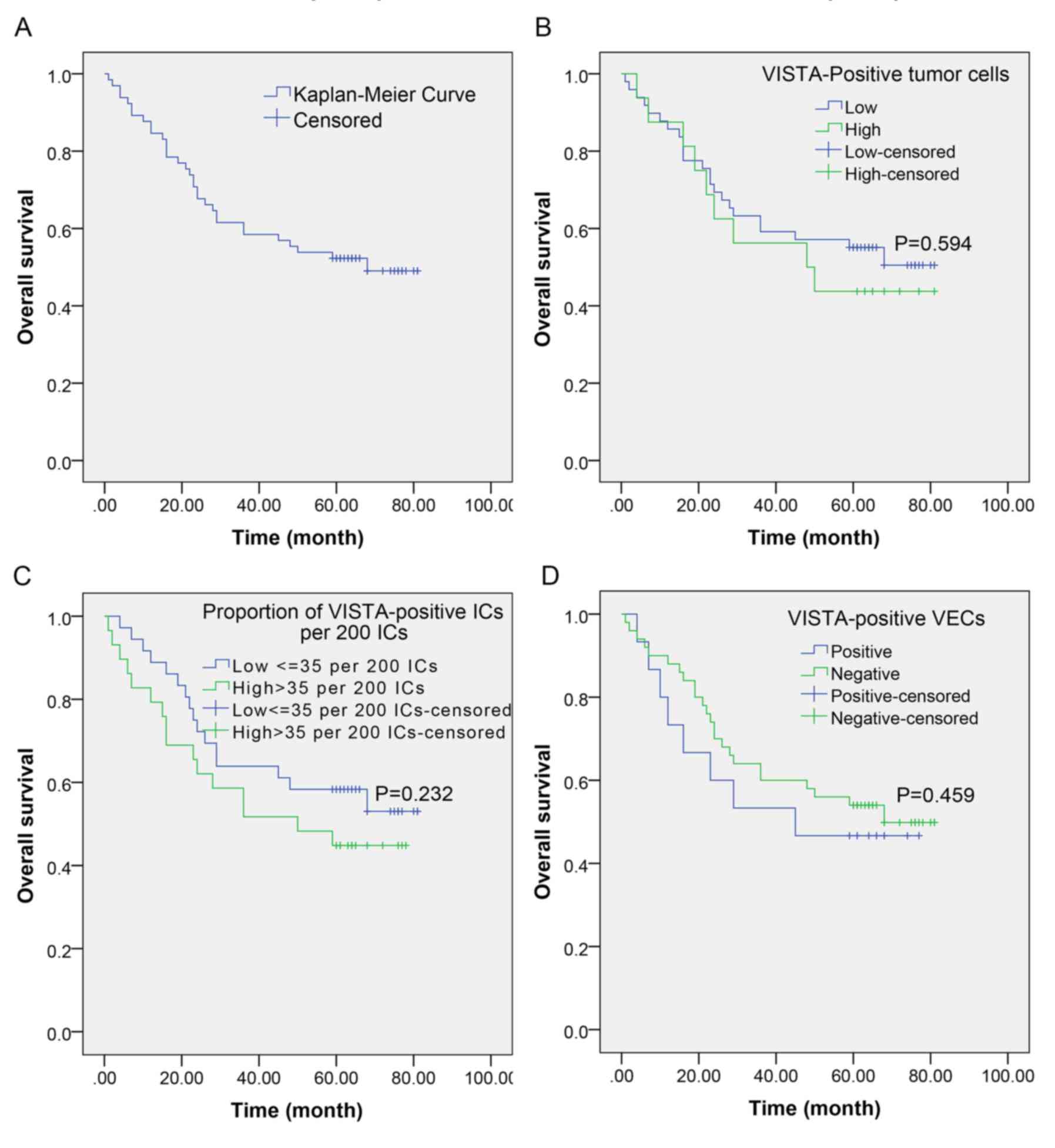 | Figure 1.Prognostic significance of VISTA
expression on tumor cells, ICs and VECs. (A) The median survival
time of the 65 patients with OC was 52.3±3.9 months (95% confidence
interval, 44.8–60.0 months) and the 5-year OS rate was 47.7%. No
significant associations between tumor-specific overall survival
and VISTA expression on (B) tumor cells (median survival, 49.1±7.6
vs. 53.3±4.5 months; P=0.594), (C) ICs (median survival, 46.5±5.7
vs. 55.9±5.0 months; P=0.232) or (D) VECs (median survival,
45.7±7.9 vs. 53.7±4.3 months; P=0.459) were observed, indicating
that none of the factors were prognostic predictors for the overall
survival in patients with ovarian cancer. VISTA, V-domain
immunoglobulin suppressor of T cell activation; ICs, immune cells;
VECs, vascular endothelial cells. |
VISTA expression in normal ovarian and
ovarian cancer tissues detected by IHC
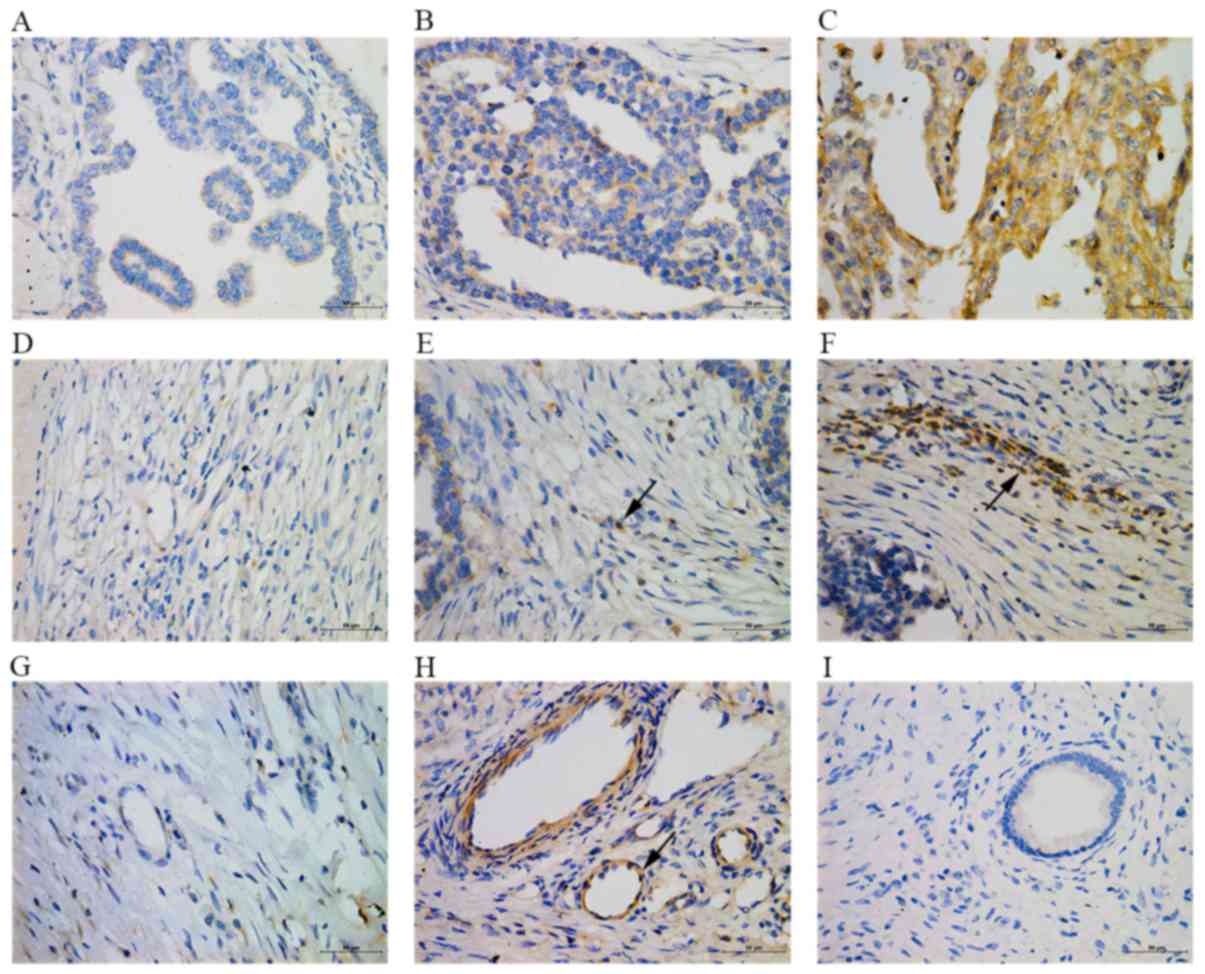
As demonstrated in Fig.
2, brown positive immunostaining for VISTA was observed in the
tumor cells, ICs and VECs in the OC tissues. The final IS of each
sample was based on a combination of the staining intensity
[ranging from negative (0) to strong (3) (median, 0)] and the percentage of
VISTA-positive cells [ranging from 0 to 95% (median, 1)].
VISTA-positive tumor cells were detected in 20/65 patients (30.8%).
These cells were primarily located in the adenoid structure of the
tumor lesions. Only 16/65 cases (24.6%) were defined as high VISTA
expression (IS ≥5). Overall, the percentage of positive tumor cells
and the staining intensity were low in the ovarian adenocarcinoma
cases in the present study.
In the majority of cases, the tumor-infiltrating ICs
accumulated in the interstitial sites, which were defined as
intratumoral hotspot regions. VISTA-positive cells were detected in
59 cases (90.8%), and the proportion of VISTA-positive ICs/200 ICs
ranged from 5–86 (median, 33). A total of 29/65 cases (44.6%) were
classified as exhibiting high expression of VISTA-positive immune
cells (>35 ICs/200 ICs). In the normal ovarian tissue, several
sporadic VISTA-positive ICs were also observed. In addition,
VISTA-positive VEC (yellow-brown circles under light microscopy)
were identified in 15 cases (23.1%).
Clinical significance of VISTA
expression in OC
The results of the examination of VISTA expression
in OC are summarized in Table I.
VISTA expression on tumor cells was significantly increased in
patients with advanced-stage OC (III+IV) compared with those with
lower-stage disease (P=0.043). Furthermore, VISTA expression on
tumor cells was more prevalent in cases with LNM compared with
those without (P=0.015). High expression of VISTA on ICs was also
associated with the tumor stage and LNM, with significantly higher
frequencies of advanced stage disease (III+IV) (P=0.047) and LNM
(P=0.042) among cases with a high proportion of VISTA-positive
ICs/200 ICs compared with those with a low proportion. VISTA
expression on VECs was only associated with LNM status, with a
significantly increased frequency of VISTA-positive VECs in cases
with LNM compared with those without (P=0.001). However, there were
no significant associations between patient age, grade of tumor
cell differentiation, histologic type of adenocarcinoma, primary
therapy or residual tumor and VISTA expression on tumor cells, ICs
and VECs.
Survival analysis and prognostic
significance of VISTA expression in OC
To explore the potential association between VISTA
expression and the prognosis of OC, OS analysis was performed by
constructing Kaplan-Meier curves. As indicated in Table I, the median survival time was
slightly decreased in patients with high VISTA expression either in
tumor cells (49.1±7.6 vs. 53.3±4.5 months) or in ICs (46.5±5.7 vs.
55.9±5.0 months) compared with that in patients with lower VISTA
expression. There was no significant difference in the 5-year OS
rate of patients with high VISTA expression (n=16) in tumor cells
compared with those with low VISTA expression (n=49; 37.5% vs.
48.97%; P=0.594; Fig. 1B). Similarly,
there was no significant difference in the 5-year OS rates of
patients with low VISTA expression on intratumor ICs compared with
those with high VISTA expression (52.8 vs. 41.4%; P=0.232; Fig. 1C). Furthermore, there was no
significant difference in the 5-year OS rates of patients with and
without VISTA-positive VECs (52.0 vs. 40.0%; P=0.459; Fig. 1D). These results indicated that there
was no association between VISTA-positive tumor cells, ICs and VECs
and the prognosis of patients with OC.
The associations between the 10 clinicopathological
characteristics and OS in patients with OC were evaluated using a
univariate Cox regression model. The results in Table II suggested that advanced-stage
(III+IV) OC [hazard ratio (HR)=2.987; P=0.008], LNM (HR =2.218;
P=0.025) and the presence of residual tumor tissue following
primary surgery (HR=2.192; P=0.030) were associated with poor
prognosis. The role of these three factors in prognostic prediction
was additionally investigated using a multivariate Cox regression
model with the forward step-wise method. The results revealed that
only advance-stage (III+IV) OC (HR=2.445; P=0.032) was an
independent prognostic factor that may be used to predict poor
survival.
| Table II.Univariate and multivariate Cox
analyses for cancer-specific overall survival in patients with
ovarian cancer (n=65). |
Table II.
Univariate and multivariate Cox
analyses for cancer-specific overall survival in patients with
ovarian cancer (n=65).
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
|
Characteristics | N | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age, years |
| 1.260
(0.629–2.524) | 0.515 | – | – |
|
≤55 | 37 |
|
|
|
|
|
>55 | 28 |
|
|
|
|
| Stage |
| 2.987
(1.329–6.717) | 0.008a | 2.455
(1.080–5.584) | 0.032a |
|
I+II | 27 |
|
|
|
|
|
III+IV | 38 |
|
|
|
|
| Grade |
| 0.781
(0.321–1.899) | 0.585 | – | – |
| Low
(G1+G2) | 11 |
|
|
|
|
| High
(G3) | 54 |
|
|
|
|
| Lymph node
metastasis |
| 2.218
(1.105–4.451) | 0.025a | 1.664
(0.819–3.380) | 0.159 |
|
Negative | 42 |
|
|
|
|
|
Positive | 23 |
|
|
|
|
| Histologic
type |
| 1.066
(0.521–2.181) | 0.862 | – | – |
| Serous
adenocarcinoma | 26 |
|
|
|
|
|
Non-serous adenocarcinoma | 39 |
|
|
|
|
| Primary
therapy |
| 0.771
(0.184–3.228) | 0.721 |
|
|
|
Surgery | 4 |
|
|
|
|
| Surgery
+ others | 61 |
|
|
|
|
| Residual tumor |
| 2.192
(1.081–4.445) | 0.030a | 1.818
(0.890–3.713) | 0.101 |
|
Negative | 35 |
|
|
|
|
|
Positive | 30 |
|
|
|
|
| VISTA-positive
tumor cells |
| 1.241
(0.574–2.682) | 0.584 | – | – |
|
Low | 49 |
|
|
|
|
|
High | 16 |
|
|
|
|
| VISTA-positive
ICs/200 ICs |
| 1.621
(0.809–3.249) | 0.173 | – | – |
|
Low | 36 |
|
|
|
|
|
High | 29 |
|
|
|
|
| Vascular
endothelial cells |
| 1.105
(0.476–2.566) | 0.817 | – | – |
|
Negative | 50 |
|
|
|
|
|
Positive | 15 |
|
|
|
|
Discussion
VISTA is a novel immune checkpoint molecule, the
prevalence of which has been demonstrated previously in a cohort of
patients with human gastric carcinoma and oral squamous cell
carcinoma (19,20); however, the corresponding data for
human OC are presently unavailable. In the present study, the
expression of VISTA in tumor cells, ICs and VECs in patients with
OC with different clinicopathological characteristics was first
evaluated. This information is important for improving our
understanding of the role of VISTA in human OC.
Immunotherapy for various types of cancer has
evolved rapidly in previous years, due to critical advances in our
understanding of the immunomodulatory signaling pathways in immune
cells and the tumor microenvironment (9). In particular, immune checkpoints are a
group of molecules involved in the inhibitory pathways that
regulate self-tolerance and modulate the duration and amplitude of
physiological immune responses to heterogeneous tissues (21). Therefore, cancer immunotherapy
targeting immune checkpoints, including cytotoxic
T-lymphocyte-associated antigen 4 (CTLA-4), PD-1 and PD-L1, have
exhibited encouraging performances in a wide range of types of
cancer, particularly melanoma, and renal and lung cancer (11,22).
VISTA, having homology to the B7 family ligand PD-L1, exerts its
immunosuppressive activities on resting and activated human CD4+
and CD8+ T cells in vitro and in vivo (12,14). In a
murine melanoma model, the blockade of VISTA alone inhibited the
suppressive characteristics of the tumor microenvironment and
enhanced protective antitumor immunity. Furthermore, the growth of
transplantable and inducible tumors was also significantly
suppressed when VISTA blockade was administered concomitantly with
a peptide vaccine (23).
In humans and mice, VISTA is predominantly expressed
in the hematopoietic tissues, or in tissues that contain
significant numbers of infiltrating leukocytes (14). Wang et al (12) suggested that VISTA expression was
confined to the leukocytes infiltrating the tumor in a murine
cancer model; however, VISTA expression on tumor cells in human
gastric carcinoma has also been demonstrated (19). In accordance with these studies,
tumor-infiltrating VISTA-positive ICs were easy to detect in OC
tissues in the present study, with almost one-half (44.6%) defined
as exhibiting high VISTA expression. Additionally, cytoplasmic
VISTA expression on tumor cells was observed in OC cases, although
only a small subset (24.7%) were regarded as exhibiting high VISTA
expression. Notably, high VISTA expression on tumor cells and ICs
was positively associated with advanced-stage OC and the presence
of LNM, suggesting that VISTA is involved in OC progression. Wu
et al (20) also identified
that the expression of VISTA was associated with lymph node status
in human oral squamous cell carcinoma. Activated VISTA serves a
role in tumor evasion from the immune system by preventing
promiscuous resting T-cell responses to self-antigens (13). Furthermore, VISTA expression was
suggested to be associated with the expression of the PD-L1 in
gastric cancer, indicating that VISTA cooperates with PD-L1 in the
mechanism underlying immune evasion (19). Therefore, in OC, the association of
advanced disease stage with high VISTA expression may be explained
by the capacity of this molecule to protect VISTA-positive tumor
cells or ICs from the immune responses that inhibit tumor growth
and metastasis (23). VISTA-positive
VECs were also detected in certain OC tissues, although no
associations with any of the clinicopathological characteristics
were observed.
Following the implementation of cytoreductive
surgery and adjuvant chemotherapy, the 5-year survival rate of
patients with OC has increased to ~50%; however, this improvement
does not match the rates for thyroid or prostate cancer (5,24).
Advanced stage, poor tumor differentiation and large tumor size are
suggested to be associated with poor prognosis in patients with OC,
and other pathological data, including the increased expression of
cleaved caspase-3 and the PD-L1 in OC, have also been identified as
predictive factors for OC prognosis (4,25,26). In the univariate and multivariate Cox
regression analyses of the patient cohort in the present study,
advanced OC stage was the only independent factor that predicted
poor OS. Apart from this predictor, there was no significant
association between VISTA expression and OS of patients with OC in
the present study. However, due to the small cohort (n=65) of
patients included in these analyses, the conclusion that VISTA
expression is not involved in the progression of OC requires
additional confirmation. Nevertheless, two other studies revealed
that the expression of VISTA alone was not associated with OS, but
functioning together with CD8+ T cells in the prediction of overall
survival in human oral squamous cell carcinoma (20).
Although there was no association between VISTA
expression and OS, positive VISTA expression increased with
advanced stage, indicating a potential role of VISTA in OC
progression. Therefore, it may be speculated that VISTA represents
a candidate biomarker of advanced tumor stage in OC. More
importantly, it has been demonstrated that OC is an immunogenic
tumor that induces a spontaneous antitumor immune response
(27). Therefore, VISTA is also
implicated as a potential target for OC immunotherapy. Although the
mechanisms of immunotherapy targeting immune checkpoints, including
PD-L1 and CTLA-4, remain to be defined, initial results appear
promising (28,29). A particular challenge in the
application of immunotherapy in OC is the identification of the
patients who will benefit from the immune checkpoint therapy.
Therefore, the measurement of VISTA expression in the tumor tissue
may be a potential biomarker used to evaluate patients for
inclusion in VISTA-associated therapy and contribute to the
development of personalized treatment programs.
In conclusion, VISTA-positive tumor cells, ICs and
VECs were detected in OC tissues. In addition, VISTA expression on
tumor cells and ICs was associated with advanced OC stage and the
presence of LNM, suggesting that this immune checkpoint molecule
may be involved in the progression of OC. In the present study,
advanced stage (III+IV) was identified as an independent prognostic
factor for the prediction of poor survival in OC. Although
unsuitable as a prognostic marker of OC, VISTA represents a
potential biomarker for selection of patients for VISTA-associated
therapy in the future.
Acknowledgements
The authors thank the Pathology Department of West
China Second University Hospital, Sichuan University (Chengdu,
China) for proving paraffin-embedded OC tissues, and Dr Zhun Wei
for his suggestions regarding data analysis.
Funding
The present study was supported by a grant from the
National Natural Science Foundation of China (grant no.
81270060).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HL performed case collecting, experiments, specimen
observing, data analysis and paper writing. HZ analysed the
specimens and collected data. HW performed data analysis. SL
designed the study, performed case collecting and assisted with
writing the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of West China Second Hospital of Sichuan University and
informed consent was obtained from all patients undergoing surgery
and control patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
VISTA
|
V-domain immunoglobulin suppressor of
T cell activation
|
|
OC
|
ovarian cancer
|
|
PD-1
|
programmed cell death 1
|
|
IS
|
immunoreactivity score
|
|
ICs
|
immune cells
|
|
VECs
|
vascular endothelial cells
|
|
LNM
|
lymph node metastasis
|
References
|
1
|
Erickson BK, Conner MG and Landen CN Jr:
The role of the fallopian tube in the origin of ovarian cancer. Am
J Obstet Gynecol. 209:409–414. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kurman RJ and Shih IM: The origin and
pathogenesis of epithelial ovarian cancer: A proposed unifying
theory. Am J Surg Pathol. 34:433–443. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Prat J: New insights into ovarian cancer
pathology. Ann Oncol. 23 Suppl 10:x111–x117. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Eltabbakh GH and Awtrey CS: Current
treatment for ovarian cancer. Expert Opin Pharmacother. 2:109–124.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Noone AM, Howlader N, Krapcho M, Miller D,
Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, et al:
SEER Cancer Statistics Review, 1975–2015. National Cancer
Institute; Bethesda, MD: 2018, https://seer.cancer.gov/csr/1975_2015/April.
2018
|
|
6
|
Komiyama S, Katabuchi H, Mikami M, Nagase
S, Okamoto A, Ito K, Morishige K, Suzuki N, Kaneuchi M, Yaegashi N,
et al: Japan society of gynecologic oncology guidelines 2015 for
the treatment of ovarian cancer including primary peritoneal cancer
and fallopian tube cancer. Int J Clin Oncol. 21:435–446. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kigawa J: New strategy for overcoming
resistance to chemotherapy of ovarian cancer. Yonago Acta Med.
56:43–50. 2013.PubMed/NCBI
|
|
8
|
Kandalaft LE, Powell DJ Jr, Singh N and
Coukos G: Immunotherapy for ovarian cancer: What's next? J Clin
Oncol. 29:925–933. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang RF and Wang HY: Immune targets and
neoantigens for cancer immunotherapy and precision medicine. Cell
Res. 27:11–37. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Drerup JM, Liu Y, Padron AS, Murthy K,
Hurez V, Zhang B and Curiel TJ: Immunotherapy for ovarian cancer.
Curr Treat Options Oncol. 16:3172015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chen L and Han X: Anti-PD-1/PD-L1 therapy
of human cancer: Past, present, and future. J Clin Invest.
125:3384–3391. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang L, Rubinstein R, Lines JL, Wasiuk A,
Ahonen C, Guo Y, Lu LF, Gondek D, Wang Y, Fava RA, et al: VISTA, a
novel mouse Ig superfamily ligand that negatively regulates T cell
responses. J Exp Med. 208:577–592. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lines JL, Sempere LF, Broughton T, Wang L
and Noelle R: VISTA is a novel broad-spectrum negative checkpoint
regulator for cancer immunotherapy. Cancer Immunol Res. 2:510–517.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lines JL, Pantazi E, Mak J, Sempere LF,
Wang L, O'Connell S, Ceeraz S, Suriawinata AA, Yan S, Ernstoff MS
and Noelle R: VISTA is an immune checkpoint molecule for human T
cells. Cancer Res. 74:1924–1932. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Deng J, Le Mercier I, Kuta A and Noelle
RJ: A New VISTA on combination therapy for negative checkpoint
regulator blockade. J Immunother Cancer. 4:862016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Okudaira K, Hokari R, Tsuzuki Y, Okada Y,
Komoto S, Watanabe C, Kurihara C, Kawaguchi A, Nagao S, Azuma M, et
al: Blockade of B7-H1 or B7-DC induces an anti-tumor effect in a
mouse pancreatic cancer model. Int J Oncol. 35:741–749.
2009.PubMed/NCBI
|
|
17
|
Hu Q, Peng J, Liu W, He X, Cui L, Chen X,
Yang M, Liu H, Liu S and Wang H: Lin28B is a novel prognostic
marker in gastric adenocarcinoma. Int J Clin Exp Pathol.
7:5083–5092. 2014.PubMed/NCBI
|
|
18
|
Wang Q, Li J, Li G, Li Y, Xu C, Li M, Xu G
and Fu S: Prognostic significance of sphingosine kinase 2
expression in non-small cell lung cancer. Tumour Biol. 35:363–368.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Böger C, Behrens HM, Krüger S and Röcken
C: The novel negative checkpoint regulator VISTA is expressed in
gastric carcinoma and associated with PD-L1/PD-1: A future
perspective for a combined gastric cancer therapy? Oncoimmunology.
6:e12932152017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wu L, Deng WW, Huang CF, Bu LL, Yu GT, Mao
L, Zhang WF, Liu B and Sun ZJ: Expression of VISTA correlated with
immunosuppression and synergized with CD8 to predict survival in
human oral squamous cell carcinoma. Cancer Immunol Immunother.
66:627–636. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pardoll DM: The blockade of immune
checkpoints in cancer immunotherapy. Nat Rev Cancer. 12:252–264.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ni L and Dong C: New checkpoints in cancer
immunotherapy. Immunol Rev. 276:52–65. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Le Mercier I, Chen W, Lines JL, Day M, Li
J, Sergent P, Noelle RJ and Wang L: VISTA regulates the development
of protective antitumor immunity. Cancer Res. 74:1933–1944. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nicklin JL, McGrath S, Tripcony L, Garrett
A, Land R, Tang A, Perrin L, Chetty N, Jagasia N, Crandon AJ, et
al: The shift toward neo-adjuvant chemotherapy and interval
debulking surgery for management of advanced ovarian and related
cancers in a population-based setting: Impact on clinical outcomes.
Aust N Z J Obstet Gynaecol. 57:651–658. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hu Q, Peng J, Liu W, He X, Cui L, Chen X,
Yang M, Liu H, Liu S and Wang H: Elevated cleaved caspase-3 is
associated with shortened overall survival in several cancer types.
Int J Clin Exp Pathol. 7:5057–5070. 2014.PubMed/NCBI
|
|
26
|
Webb JR, Milne K, Kroeger DR and Nelson
BH: PD-L1 expression is associated with tumor-infiltrating T cells
and favorable prognosis in high-grade serous ovarian cancer.
Gynecol Oncol. 141:293–302. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Markman M: Immunotherapy in ovarian
cancer-where are we going? Am J Hematol Oncol. 12:2016.
|
|
28
|
Kandalaft LE, Motz GT, Duraiswamy J and
Coukos G: Tumor immune surveillance and ovarian cancer: Lessons on
immune mediated tumor rejection or tolerance. Cancer Metastasis
Rev. 30:141–151. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
De Felice F, Marchetti C, Palaia I, Musio
D, Muzii L, Tombolini V and Panici PB: Immunotherapy of ovarian
cancer: The role of checkpoint inhibitors. J Immunol Res.
2015:1918322015. View Article : Google Scholar : PubMed/NCBI
|