Introduction
Lung cancer is the leading cause of
cancer-associated mortality worldwide in males and females.
Non-small-cell lung cancer (NSCLC) accounts for ~85% of all lung
cancer cases (1,2). Despite continuous endeavors to develop
novel treatment strategies, the majority of patients with lung
cancer exhibit a poor prognosis (1,2). Basic
biological behaviors of cancer cells, including migration,
angiogenesis and cross-talk between cancer cells and their
microenvironment, serve critical roles in tumor growth and
metastasis; chemokines are considered to be specific major
modulators in these biological processes (3).
Chemokines, also referred to as chemotactic
cytokines, are proteins secreted into the blood circulation that
mediate numerous physiological and pathological processes primarily
associated with cell homing and migration through interactions with
the chemokine receptors present on target cells (4). Accumulating data have indicated that
tumor growth, invasion and metastasis may be facilitated by the
overexpression of chemokine receptors on cancer cells (3), among which CXCR4 is the most extensively
investigated. CXCR4, a type of 7-transmembrane G protein-coupled
receptor, is the cognate receptor for stromal cell-derived factor-1
(CXCL12) and is expressed on naive T cells, natural killer cells,
dendritic cells and monocytes (5).
Recently, it was also identified to be overexpressed in several
different types of human cancer, such as breast and pancreatic
cancer (6). Meta-analyses (7,8) and
clinical (9,10) have demonstrated that CXCR4 expression
is associated with organ-specific metastasis and poor survival in
patients with NSCLC. An increasing number of studies have
elucidated the mechanisms by which chemokine receptors are involved
in cancer progression, resulting in the design of corresponding
antagonists (11), several of which
have already been identified to be effective in certain tumor types
according to preliminary (12,13).
However, the data are conflicting and the knowledge is incomplete
regarding the complexity and diversity of the biological effects
induced by CXCR4-CXCL12 (3).
Additional studies are required to elucidate these interactions in
different types of human cancer prior to clinical application.
In the present study, A549, a cell strain
originating from human NSCLC, was used as an in vitro model.
The interaction of CXCR4 with CXCL12 was blocked by a CXCR4
antagonist, AMD3100, followed by evaluation of A549 cell
proliferation and migration towards CXCL12 with Cell Counting Kit-8
(CCK-8) and Transwell migration assays. In a preclinical model
developed by inoculating nude mice with A549 cells, tumor size and
microvessel density (MVD) were compared between experimental and
control mice. In addition, the effect of AMD3100 administration on
CXCR4 expression was also determined by joint evaluation of the
extent and intensity of immunohistochemical (IHC) staining. The
results of the present study demonstrated targeting CXCR4 decreased
the proliferation, migration and angiogenesis of lung cancer
cells.
Materials and methods
Reagents
A CCK-8 kit was purchased from Dojindo Molecular
Technologies, Inc. (Rockville, MD, USA). The Transwell chamber was
purchased from Corning Life Sciences (Corning, NY, USA). AMD3100
was supplied by MedChem Express (cat. no. HY-10046; Monmouth
Junction, NJ, USA) and dissolved in dimethyl sulfoxide (DMSO) for
the cell assay and in sterile PBS for animal administration.
Recombinant human CXCR12 protein was purchased from R&D
Systems, Inc. (cat. no. 350-NS; Minneapolis, MN, USA). Monoclonal
rabbit anti-human CXCR4 antibody was provided by Abcam (cat. no.
ab181020; Cambridge, UK). Mouse anti-human CD34 monoclonal antibody
(cat. no. GM716502), horseradish peroxidase (HRP)-labeled
anti-rabbit/mouse secondary antibody (cat. no. GP016129) and DAB
coloring agent (cat. no. GK500510A) were all purchased from Gene
Tech Biotechnology Co. Ltd. (Shanghai, China).
Animals and cell lines
The A549 human alveolar adenocarcinoma cell line was
a gift from Professor Liu Ming (Guangzhou Institute of Respiratory
Diseases, Guangzhou, China) and maintained in RPMI-1640 (Hyclone;
GE Healthcare Life Sciences, Logan, UT, USA) supplemented with 10%
fetal bovine serum (FBS; Gibco; Thermo Fisher Scientific, Inc.,
Waltham, MA, USA, cat. no. 10099–141), 100 U/ml penicillin and 100
µg/ml streptomycin at 37°C in a 5% CO2 incubator. Female
BALB/c nude mice (n=10, 4–6 weeks old, 15–18 g) were provided by
Beijing Vital River Laboratory Animal Technology Company (Beijing,
China) and housed under specific pathogen-free conditions at 25±2°C
in a 12 h night/dark cycle. All animals were fed sterilized rodent
food, and has unrestricted access to food and water. They were
cared for in accordance with the Animal Welfare Act guidelines
under an animal protocol approved by Guangzhou Medical University
Animal Care and Use Committee. For experimental end-points,
tumor-bearing mice were euthanized prior to the subcutaneous tumor
reaching 20 mm in any direction, but all animals exhibiting signs
including restriction of mobility, the inability to feed, pressure
on internal organs or sensitive regions of the body or a body
condition score (14) of <2 were
euthanized, even if the maximum tumor size had not been
reached.
Cell proliferation assay
The cell proliferation assay was performed using a
CCK-8 kit, according to the manufacturer's protocol. Briefly, A549
cells grown to 80% confluence were rinsed with 0.25% Trypsin/EDTA
solution (Thermo Fisher Scientific Inc.,) and 2 ml of trypsin
solution was added to detach the cells. The detachment was
monitored under an inverted microscope for 2–5 min at a
magnification of ×100. A total of 8 ml of RPMI 1640 complete medium
were added to cease cell detachment and cells were washed twice
with phosphate-buffered saline (PBS) followed by centrifugation at
4°C, 100 × g for 5 min. The cells were suspended in complete medium
and plated in 96-well plates at a density of 10,000 cells/well and
cultured for 12 h in RPMI-1640 growth medium containing 10% FBS,
100 U/ml penicillin and 100 µg/ml streptomycin at 37°C in a 5%
CO2 incubator. The culture supernatant was removed and
growth medium with AMD3100 was added to a final concentration of 2
µmol/l for an additional 0, 24, 48, 72 or 96 h culture. An equal
volume of growth medium with vehicle alone was added to the control
wells. Each medium was added to triplicate wells. Prior to the end
of the culture (4 h), AMD3100-containing medium was replaced with
110 µl growth medium containing 10 µl CCK-8 solution. Following a 4
h incubation, the optical density (OD) of each well was determined
at 450 nm with an enzyme-linked immunometric meter (BIOBASE-EL10A,
BioBase, Jinan, China), and the average OD values were calculated
from triplicate wells. The experiment was repeated 3 times
independently.
Chemotaxis assay
A549 cells grown to 80% confluence were harvested as
described previously and resuspended in growth medium composed of 2
µmol/l AMD3100 under the aforementioned culture conditions. The
cells treated with vehicle alone (DMSO) were used as the control.
After 48 h, all cells were serum-starved and cultured for 12 h,
followed by assessing chemotaxis to CXCL12. A chemotaxis assay was
performed in triplicate in 24-well Transwell chambers with
polycarbonate membranes of 8-µm pore size. Briefly,
2×104 A549 cells in 100 µl serum-reduced RPMI-1640
medium containing 1% bovine serum albumin (MedChemExpress) were
added to the upper chamber of each well, and 700 µl RPMI-1640
medium containing 10% FBS and 10 ng/ml soluble CXCL12 was added to
the lower chamber. Chemotaxis was allowed at 37°C in a 5%
CO2 incubator for 12 h. Cells adhering to the upper
surface of the membrane were removed with a cotton swab. Cells that
had migrated through the filter and adhered to the lower surface of
the membrane were fixed by 4% paraformaldehyde at room temperature
(RT) for 30 min and stained with 0.1% crystal violet solution at RT
for min. Following continuous washing 3 times with running water
for 5 min each, the membranes were removed from the Transwell
inserts and Image-Pro Plus software (Ver. 6.0, Media Cybernetics,
Inc., Rockville, MD, USA) was used to count the cells under the
light microscope (Olympus BX53; Olympus Corporation, Tokyo, Japan)
in 6 randomly selected fields at a magnification of ×400.
Nude mice lung cancer model
For the xenograft model, 1×106 A549 cells
were inoculated subcutaneously in the right flank of each BALB/c
nude mouse. The length and width of the subcutaneous tumor were
measured regularly and the tumor volumes were calculated using the
formula: Volume=(length × width2)/2. Tumors were not
permitted to exceed 2 cm in diameter; all mice only developed one
subcutaneous tumor. Once the tumor width had reached 0.5 cm, the
mice were randomly divided into two groups (n=5/group). The mice in
the two groups received intraperitoneal administration of either
AMD3100 (1.25 mg/kg body weight; treatment group) or vehicle (100
µl sterile PBS; control group) twice daily for 20 (15). The tumor size was measured every other
day. At day 19 when the difference in tumor size became marked in
the two groups, all mice were euthanized by exposure to an overdose
of CO2, at a flow rate of 20% of the chamber volume per
minute. The tumor xenografts and lung tissues were excised and
fixed in 4% buffered paraformaldehyde at RT for 30 min, and
embedded in paraffin.
IHC staining for CXCR4 and CD34
expression
Staining procedures were performed according to the
antibody manufacturer's protocol. Briefly, tissues embedded in
paraffin were cut into 4-µm sections, deparaffinized and rehydrated
in a graded alcohol series (100, 95, 80 and 70%, for 1 min each at
RT), prepared from absolute alcohol (cat. no. 64–17-5; Shanghai
Macklin Biochemical Co., Ltd., Shanghai, China). Following antigen
retrieval in sodium citrate buffer (10 mM, pH 6.0; Haoran
Bio-Pharma Co., Ltd., Shanghai, China), endogenous peroxidase was
blocked by 3% H2O2 in methanol for 10 min at
RT. Tissue sections were then blocked with normal goat serum (cat.
no. ab7481; Abcam) for 30 min at 37°C and then incubated with
rabbit anti-human CXCR4 (1:400 dilution) or mouse anti-human CD34
(1:200 dilution) at 4°C overnight. Subsequent to washing (1× PBS,
three times, 5 min each), the tissue sections were incubated with
HRP-labeled goat anti-rabbit/mouse antibody (1:100 dilution) at
37°C for 15 min. The tissue sections were incubated with the
freshly prepared DAB coloring agent (50-100 µl) at room temperature
for 3–10 min, examined under a microscope (Olympus BX53; Olympus
Corporation, Tokyo, Japan) at a magnification of ×200 and
counterstained with 0.2% hematoxylin for 2 min at RT.
Scoring of CXCR4 expression
CXCR4 expression was quantified as previously
described (16,17), with modifications. In brief, two
scoring systems were used to quantify CXCR4 staining. The
percentage of positive tumor cells was referred to as staining
extent (E), which was graded on a scale of 0–3 as follows: 0, ≤5%;
1, 6–20%; 2, 21–50%; and 3, >50%. Staining intensity (I) was
also graded on a scale of 0–3 as follows: 0, none; 1, weak staining
(+); 2, moderate staining (++); and 3, strong staining (+++). The
product of E × I, referred to as the EI score, ranged from 0 to 9,
and was used to quantify the CXCR4 expression of each section. In
view of the heterogeneous expression of CXCR4 in tumor tissues, the
total EI score for any section was calculated as a sum of EI scores
for 2–3 different fields of view
Microvessel counting
Microvessel counting was performed as previously
described (18) under a microscope
(at ×40 and ×100 magnification, DM2500, Leica Microsystems
Inc.,Wetzlar, Germany) and pictures were taken by a color camera
(TK-C9501EC, Victor Company of Japan, Limited). In brief, the
slides were examined at low magnification (×40 and ×100) to
identify the highest vascular density areas (hot spots) within the
tumor, and then 3–4 areas of highest neovascularization were
selected for counting at a magnification of ×200 (0.739
mm2/field). The mean number of microvessels of these
areas was recorded as the MVD level. Any brown-stained endothelial
cell or endothelial cell cluster that was clearly separate from
adjacent microvessels, tumor cells and other connective tissue
elements, was considered as a single countable microvessel. Vessel
lumina and red blood cells were not necessary for defining a
microvessel. Macrovessels, characterized by thick muscular walls or
with lumina >8 red blood cells in diameter (~50 µm), were
excluded from the count.
Statistical analysis
All data were presented as mean ± standard error of
the mean. GraphPad Prism v. 5.01 (GraphPad Software, Inc., La
Jolla, CA, USA) software was used for graph plotting and
statistical analysis. Relative cell viability was compared using a
two-way analysis of variance, followed by Bonferroni's multiple
comparison test. The Mann-Whitney U test was used for comparison
between two means. P<0.05 was considered to indicate a
statistically significant difference.
Results
CXCR4 blockade effectively inhibits
in vitro proliferation of A549 cells and their migration
towards CXCL12
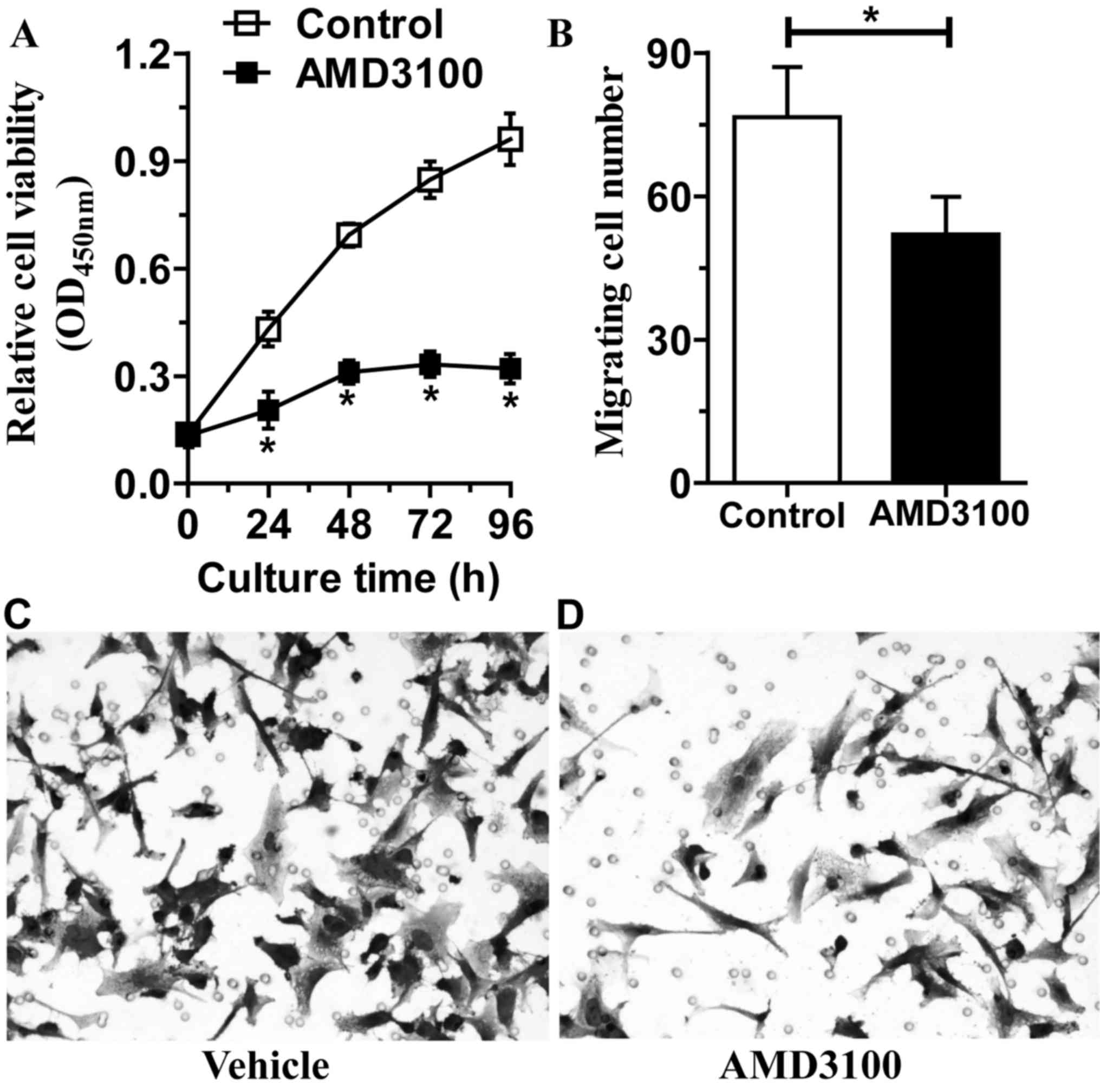
AMD3100, a selective small-molecule inhibitor of
CXCR4 signaling, was added into the culture medium of A549 cells,
and cell viability and migration were observed. As shown in
Fig. 1A, cell viability in the
control group increased rapidly with increases in culture time and
until the endpoint of incubation (>6-fold enhancement in
relative cell viability). Regarding the AMD3100-treated group,
relative cell viability exhibited a markedly slower increase,
followed by a decline 96 h later (P<0.05). At the end of the
incubation, the cell viability was increased by a little more than
1-fold. CXCR4-expressing A549 cells migrate towards their specific
ligand, CXCL12 (6); this phenomenon
is referred to as chemotaxis. However, when blocked by AMD3100, the
number of A549 cells that migrated through the chamber membrane was
markedly reduced compared with vehicle control (P=0.001; Fig. 1B). The crystal violet staining
demonstrated that cells that had migrated through the filter and
adhered to the lower surface of the membrane were increased in the
vehicle group (Fig. 1C) compared with
the AMD3100 group (Fig. 1D)
CXCR4 blockade decelerates tumor
growth in nude mice with NSCLC
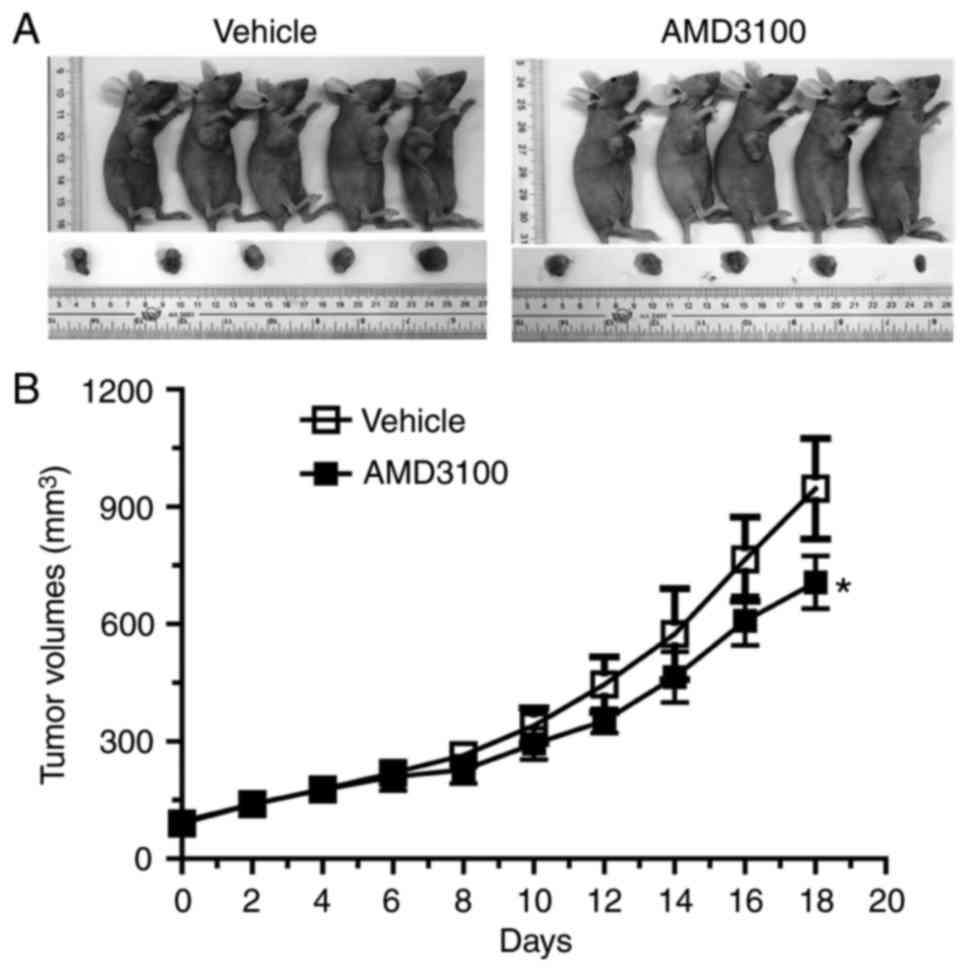
To determine whether AMD3100 was able to decelerate
tumor growth in vivo, a NSCLC xenograft model was
established by subcutaneously injecting nude mice with human A549
cells. Mice bearing xenograft tumors were treated with AMD3100 or
vehicle, and the tumor volumes were measured. At the endpoint of
the study (Day 19), all mice were sacrificed and larger tumor
masses were macroscopically observed in vehicle-treated mice than
AMD3100-treated mice (Fig. 2A). In
addition, tumor growth curve showed that tumor growth was
significantly slower in the AMD3100-treated mice compared with the
vehicle group (P=0.0247; Fig.
2B).
CXCR4 expression and vascularization
are inhibited by an antagonist
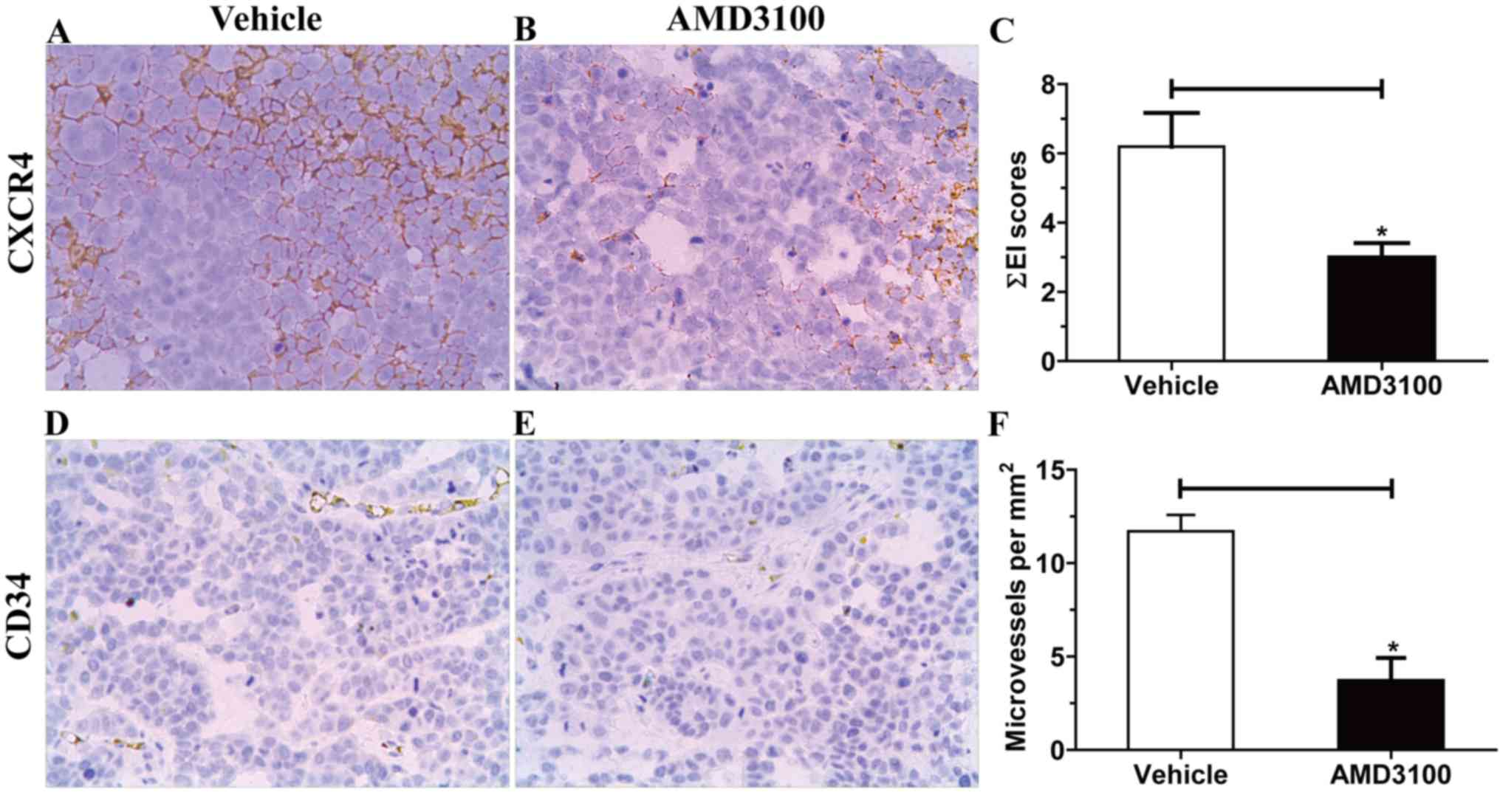
Tumor xenografts were removed from euthanized mice
and CXCR4 expression in tumor cells and MVD in the tumor mass were
additionally analyzed by IHC staining. It was demonstrated that
CXCR4 expression was localized to the cell membranes (Fig. 3A and B). Tumor sections from
AMD3100-treated mice exhibited significantly decreased total EI
scores of CXCR4 expression compared with those from control mice
(P=0.0179; Fig. 3C), the EI score is
considered to be positively associated with antigen expression
level (16). Subsequently, the
microvessels in the tumor mass were visualized by CD34 antigen
staining (Fig. 3D and E). By
calculating microvessel numbers per mm2 slice, a
decreased MVD was observed in AMD3100-treated mice compared with
that in control mice (P=0.0159, Fig.
3F). In summary, these data indicate that CXCR4 targeting is
likely to downregulate tumor expression of CXCR4 and impair tumor
vascularization.
Discussion
CXCR4 belongs to the superfamily of G
protein-coupled receptors (GPCRs) that possess seven transmembrane
domains (5). CXCR4 is constitutively
identified and widely expressed by numerous cell types, including
the majority of hematopoietic cell types in the blood and bone
marrow, vascular endothelial cells, Langerhans cells, neurons and
neuronal stem cells (4). Through
binding to CXCL12, which is widely expressed in multiple organs,
including the colon, liver, brain, lungs, heart, kidney and spleen,
CXCR4 is extensively involved in various physiological functions,
including embryonic hematopoiesis, organogenesis, vascularization
and immune surveillance, and pathological processes, including
inflammation, tumorigenesis and wound healing (4). The roles of chemokine/chemokine receptor
interactions in cancer biology have been attracting an increasing
amount of attention. As it is overexpressed in >23 different
types of human cancer (4), CXCR4 is
considered to contribute to tumor growth, angiogenesis, metastasis
and resistance to treatment (6,12). With
regards to lung cancer, clinical data indicated that CXCR4
overexpression was significantly associated with poorer
progression-free survival time and overall survival rate (OS)
(8,9,19). A
number of experimental studies demonstrated that in vitro or
in vivo inhibition of CXCR4/CXCL12 interaction via CXCR4
blockade (13,15,20,21)
attenuated NSCLC cell growth, migration, angiogenesis and
metastasis and increased the sensitivity of cancer cells to
chemotherapy (22). It appears that
this axis may represent a promising target for the development of
novel anticancer chemokine-based therapeutics. In fact, multiple
agents targeting CXCR4/CXCL12 signaling in cancer are currently
being developed (4), among which the
CXCR4 antagonist AMD3100 is the most extensively investigated
(12). AMD3100, also referred to as
plerixafor, was initially studied as an anti-HIV agent, and it was
then identified to increase the white blood cell count in the blood
and mobilize stem cells from the bone marrow (12). In 2008, AMD3100 gained Food and Drug
Administration approval for mobilization of hematopoietic stem
cells for bone marrow transplantation, rather than for cancer
treatment (23).
Despite the collective aforementioned evidence
mentioned supporting the potential efficacy of CXCR4 inhibition for
the treatment of cancer, there remains controversy and uncertainty
regarding the role of the CXCR4/CXCL12 axis in cancer growth and
metastasis. For example, regarding the prognostic value of CXCR4
overexpression, a number of studies concluded that CXCR4 expression
was associated with unfavorable prognosis (8–10,13). However, a number of studies also
reported different, even opposite conclusions: CXCR4 was detected
on the cell membrane, in the cytoplasm and in the nucleus of
gastric cancer and NSCLC cells, and strong CXCR4-positive nuclear
staining was associated with a significantly improved OS rate
(24,25), although the underlying mechanisms
remain unclear. In addition, there are data indicating that CXCR4
expression exerted no significant effect on patient survival and
was not significantly associated with any other clinicopathological
variables (26). Furthermore,
increased levels of CXCR4 expression in the tumor cells in
comparison with tumor cells with no or low levels of CXCR4
expression from the patients with lung adenocarcinoma, were even
identified to be an independent predictor of an improved prognosis
in patients with lung adenocarcinoma (27), whereas epigenetic silencing of CXCR4
expression facilitated metastasis and progression of cervical
cancer by causing loss of cell-to-cell adhesions (28). Additionally, contradictory data have
also been demonstrated regarding the association between CXCL12
expression and clinical outcome (26,29).
Despite laboratory data supporting the inhibition of tumor growth
and metastasis by CXCL12 expression (30,31), it is
reasonable to hypothesize that the CXCR4/CXCL12 axis may exhibit an
important antitumor role under certain conditions (32). Discrepancies in observations indicate
that our knowledge of certain aspects of this chemokine axis
remains incomplete, and additional investigations are required. The
therapeutic strategies that block CXCR4 signaling must undergo
continued evaluation prior to clinical application, due to the
ubiquitous expression of CXCR4 in normal tissues and the functional
importance of CXCR4-CXCL12 interaction.
In our previous study (33), 61 patients with NSCLC were analyzed
with IHC staining for CXCR4 expression. An increased CXCR4
expression rate was observed in tumor tissues compared with normal
lung tissue and a positive association of CXCR4 expression with
tumor stage and lymph node metastasis was identified. Despite the
lack of data on the association between CXCR4 expression and
prognosis, it is well-established that a more advanced tumor stage
is associated with poorer survival (9). In the present study, the data indicated
that CXCR4 blockade markedly attenuated in vitro cell
proliferation and migration towards CXCL12, which was consistent
with the aforementioned observations described by a number of
studies (4,11–13). In
addition, in the present study a xenograft tumor model was
established to mimic patients with NSCLC. Following continuous
intraperitoneal administration of a CXCR4 antagonist, tumor growth
in nude mice was demonstrated to be markedly decreased compared
with control mice due to the pronounced inhibition of CXCR4
expression and neovascularization in the tumor mass.
It was demonstrated previously that CXCR4 engagement
facilitates cancer cell proliferation, survival, angiogenesis and
migration by stimulating multiple downstream signaling pathways,
including the phosphatidylinositol-3-kinase (PI3K) and
mitogen-activated protein kinase (MAPK) pathways (12). AMD3100 prevented CXCR4 from binding to
CXCL12 by occupying the ligand-binding pocket, thereby blocking the
generation and downward transduction of activation signals
(12). Cancer cell migration was
previously identified as one of the key steps of distant cancer
spread (34). CXCR4-expressing lung
cancer cells migrated to tissues or organs with a high level of
CXCL12, including lymph nodes, contralateral lung, liver and brain,
finally forming metastatic loci (10,34). The
CXCR4 antagonist was previously demonstrated to attenuate tumor
metastasis by disrupting the interaction between CXCR4 and CXCL12
(15). Of note, the current
immunostaining data demonstrated that CXCR4 blockade significantly
downregulated CXCR4 expression by tumor tissues. Based on this
result, it is reasonable to infer that decreased CXCR4 expression
resulted in weakened CXCR4-CXCL12 interaction and resultant
decreased metastasis. At present, little is known about how AMD3100
downregulates CXCR4 expression. Theoretically, CXCR4-associated
downstream signaling pathways, including PI3K/Akt, MAPK and Janus
kinase/Signal transducer and activator of transcription, all
promote anti-apoptosis; therefore, apoptosis induction by signal
inhibition is likely to be involved in this downregulation effect.
In fact, previous data demonstrated that AMD3100 resulted in
increased tumor apoptosis and necrosis (35), although knockdown of CXCR4 by small
interfering RNA did not affect tumor cell apoptosis induced by
chemotherapeutic agents (36). In the
present study, large necrotic areas were observed in tumor tissue
sections from mice treated with AMD3100 (data not shown), however
the apoptosis data were not obtained and this result requires
additional investigation. In addition, it must be mentioned that in
the present study CXCR4 expression was only localized to cell
membranes, which was not consistent with previous studies (24,25). In
the experiment with human NSCLC tissues, positive CXCR4 staining
was not observed in the nucleus, but in the cell membrane or the
cytoplasm. This result may partly explain our conclusion that high
CXCR4 expression was associated with advanced tumor stage, in that
patients with nuclear CXCR4 expression were identified to have an
improved OS rate compared with those with membranous or cytoplasmic
expression (24). Neovascularization
is key process in cancer survival and metastatic spread (15,18). The
CXCR4/CXCL12 axis was recognized as an important modulator of the
angiogenesis/angiostasis balance (37). MVD, a measure of tumor angiogenesis,
was reported by various studies (18,38,39) to be
closely associated with the incidence of metastases and clinical
outcome. By means of immunostaining against the CD34 antigen, a
sensitive biomarker for blood vessels, the present study
demonstrated a marked reduction of MVD in the tumor masses
following treatment with the CXCR4 antagonist. Based on this
result, a similar conclusion may be drawn that the CXCR4 blockade
may decrease metastasis through inhibition of angiogenesis, in
accordance with the findings of previous studies (11,15).
In summary, the data of the present study lead to
the conclusion that CXCR4 expression facilitates tumor growth and
metastasis, and its targeting may induce antitumor effects to a
certain extent by impairing tumor proliferation, migration and
angiogenesis. However, despite the encouraging results of the
present study and other preclinical data, it is too early to draw
definitive conclusions on the role of the CXCR4/CXCL12 axis and its
inhibition for cancer treatment. Increased efforts should be
focused on elucidating conflicting aspects and improving the
understanding of this axis, in order that targeted therapies may be
safely applied in clinical settings.
Acknowledgements
The authors would like to thank Guangzhou Vipotion
Biotechnology Company, Limited for the technical support.
Funding
The present study was supported by the Medical
Scientific Research Foundation of Guangdong Province, China (grant
no. A2015375 to Dr Wei He).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WH conceived the experimental design and wrote the
manuscript, and WH, TY, XHG, RZQ, XDZ and WDL conducted the
experiments. WH and TY analyzed the obtained data. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
Animal experiments were performed in accordance with
the Animal Welfare Act guidelines under an animal protocol approved
by Guangzhou Medical University Animal Care and Use Committee
(Guangzhou, China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J Clin. 62:10–29. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel R, DeSantis C, Virgo K, Stein K,
Mariotto A, Smith T, Cooper D, Gansler T, Lerro C, Fedewa S, et al:
Cancer treatment and survivorship statistics, 2012. CA Cancer J
Clin. 62:220–241. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Roy I, Evans DB and Dwinell MB: Chemokines
and chemokine receptors: Update on utility and challenges for the
clinician. Surgery. 155:961–973. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chatterjee S, Azad Behnam B and Nimmagadda
S: The intricate role of CXCR4 in cancer. Adv Cancer Res.
124:31–82. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Muller A, Homey B, Soto H, Ge N, Catron D,
Buchanan ME, McClanahan T, Murphy E, Yuan W and Wagner SN:
Involvement of chemokine receptors in breast cancer metastasis.
Nature. 410:50–56. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sarvaiya PJ, Guo D, Ulasov I, Gabikian P
and Lesniak MS: Chemokines in tumor progression and metastasis.
Oncotarget. 4:2171–2185. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wu Y, Zhang C, Xu W, Zhang J, Zheng Y, Lu
Z, Liu D and Jiang K: CXC motif chemokine receptor 4 gene
polymorphism and cancer risk. Medicine (Baltimore). 95:e53172016.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhao H, Guo L, Zhao H, Zhao J, Weng H and
Zhao B: CXCR4 over-expression and survival in cancer: A system
review and meta-analysis. Oncotarget. 6:5022–5040. 2015.PubMed/NCBI
|
|
9
|
Zhou XM, He L, Hou G, Jiang B, Wang YH and
Zhao L: Clinicopathological significance of CXCR4 in non-small cell
lung cancer. Drug Des Devel Ther. 9:1349–1358. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang L, Wang Z, Liu X and Liu F:
High-level C-X-C chemokine receptor type 4 expression correlates
with brain-specific metastasis following complete resection of
non-small cell lung cancer. Oncol Lett. 7:1871–1876. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wald O, Shapira OM and Izhar U:
CXCR4/CXCL12 axis in non small cell lung cancer (NSCLC) pathologic
roles and therapeutic potential. Theranostics. 3:26–33. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liu T, Li X, You S, Bhuyan SS and Dong L:
Effectiveness of AMD3100 in treatment of leukemia and solid tumors:
From original discovery to use in current clinical practice. Exp
Hematol Oncol. 5:192016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Brennecke P, Arlt MJ, Campanile C, Husmann
K, Gvozdenovic A, Apuzzo T, Thelen M, Born W and Fuchs B: CXCR4
antibody treatment suppresses metastatic spread to the lung of
intratibial human osteosarcoma xenografts in mice. Clin Exp
Metastasis. 31:339–349. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ullman-Cullere MH and Foltz CJ: Body
conditioning scoring: A rapid and accurate method for assessing
health status in mice. Lab Anim Sci. 49:319–323. 1999.PubMed/NCBI
|
|
15
|
Sun X, Charbonneau C, Wei L, Yang W, Chen
Q and Terek RM: CXCR4-targeted therapy inhibits VEGF expression and
chondrosarcoma angiogenesis and metastasis. Mol Cancer Ther.
12:1163–1170. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Marechal R, Demetter P, Nagy N, Berton A,
Decaestecker C, Polus M, Closset J, Devière J, Salmon I and Van
Laethem JL: High expression of CXCR4 may predict poor survival in
resected pancreatic adenocarcinoma. Br J cancer 5. 100:1444–1451.
2009. View Article : Google Scholar
|
|
17
|
Sood AK, Fletcher MS, Gruman LM, Coffin
JE, Jabbari S, Khalkhali-Ellis Z, Arbour N, Seftor EA and Hendrix
MJ: The paradoxical expression of maspin in ovarian carcinoma. Clin
Cancer Res. 8:2924–2932. 2002.PubMed/NCBI
|
|
18
|
Weidner N, Semple JP, Welch WR and Folkman
J: Tumor angiogenesis and metastasis-correlation in invasive breast
carcinoma. N Engl J Med. 324:1–8. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Liu Y, Wu BQ, Geng H, Xu ML and Zhong HH:
Association of chemokine and chemokine receptor expression with the
invasion and metastasis of lung carcinoma. Oncol Lett.
10:1315–1322. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gil M, Seshadri M, Komorowski MP, Abrams
SI and Kozbor D: Targeting CXCL12/CXCR4 signaling with oncolytic
virotherapy disrupts tumor vasculature and inhibits breast cancer
metastases. Proc Natl Acad Sci USA. 110:E1291–E1300. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Choi WT, Yang Y, Xu Y and An J: Targeting
chemokine receptor CXCR4 for treatment of HIV-1 infection, tumor
progression, and metastasis. Curr Top Med Chem. 14:1574–1589. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Liang S, Peng X, Li X, Yang P, Xie L, Li
Y, Du C and Zhang G: Silencing of CXCR4 sensitizes triple-negative
breast cancer cells to cisplatin. Oncotarget. 6:1020–1030. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
DiPersio JF, Stadtmauer EA, Nademanee A,
Micallef IN, Stiff PJ, Kaufman JL, Maziarz RT, Hosing C, Früehauf
S, Horwitz M, et al: Plerixafor and G-CSF versus placebo and G-CSF
to mobilize hematopoietic stem cells for autologous stem cell
transplantation in patients with multiple myeloma. Blood.
113:5720–5726. 2009.PubMed/NCBI
|
|
24
|
Nikkhoo B, Jalili A, Fakhari S,
Sheikhesmaili F, Fathi F, Rooshani D, Feizi Hoseinpour MA and
Nikzaban M: Nuclear pattern of CXCR4 expression is associated with
a better overall survival in patients with gastric cancer. J Oncol.
2014:8080122014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Spano JP, Andre F, Morat L, Sabatier L,
Besse B, Combadiere C, Deterre P, Martin A, Azorin J, Valeyre D, et
al: Chemokine receptor CXCR4 and early-stage non-small cell lung
cancer: Pattern of expression and correlation with outcome. Ann
Oncol. 15:613–617. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Popple A, Durrant LG, Spendlove I, Rolland
P, Scott IV, Deen S and Ramage JM: The chemokine, CXCL12, is an
independent predictor of poor survival in ovarian cancer. Br J
Cancer. 106:1306–1313. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Minamiya Y, Saito H, Takahashi N, Ito M,
Imai K, Ono T, Motoyama S and Ogawa J: Expression of the chemokine
receptor CXCR4 correlates with a favorable prognosis in patients
with adenocarcinoma of the lung. Lung Cancer. 68:466–471. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yadav SS, Prasad SB, Das M, Kumari S,
Pandey LK, Singh S, Pradhan S and Narayan G: Epigenetic silencing
of CXCR4 promotes loss of cell adhesion in cervical cancer. Biomed
Res Int. 2014:5814032014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mirisola V, Zuccarino A, Bachmeier BE,
Sormani MP, Falter J, Nerlich A and Pfeffer U: CXCL12/SDF1
expression by breast cancers is an independent prognostic marker of
disease-free and overall survival. Eur J Cancer. 45:2579–2587.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Roy I, Zimmerman NP, Mackinnon AC, Tsai S,
Evans DB and Dwinell MB: CXCL12 chemokine expression suppresses
human pancreatic cancer growth and metastasis. PLoS One.
9:e904002014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wendt MK, Johanesen PA, Kang-Decker N,
Binion DG, Shah V and Dwinell MB: Silencing of epithelial CXCL12
expression by DNA hypermethylation promotes colonic carcinoma
metastasis. Oncogene. 25:4986–4997. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Williams SA, Harata-Lee Y, Comerford I,
Anderson RL, Smyth MJ and McColl SR: Multiple functions of CXCL12
in a syngeneic model of breast cancer. Mol Cancer. 9:2502010.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gong X, Yang T, Liu W, Liao K and He W:
Expression and clinical significance of chemokine receptor CXCR4 in
non-small cell lung cancer. J Trop Med. 16:829–831. 2016.(In
Chinese).
|
|
34
|
Popper HH: Progression and metastasis of
lung cancer. Cancer Metastasis Rev. 35:75–91. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Righi E, Kashiwagi S, Yuan J, Santosuosso
M, Leblanc P, Ingraham R, Forbes B, Edelblute B, Collette B, Xing
D, et al: CXCL12/CXCR4 blockade induces multimodal antitumor
effects that prolong survival in an immunocompetent mouse model of
ovarian cancer. Cancer Res. 71:5522–5534. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Choi YH, Burdick MD, Strieter BA, Mehrad B
and Strieter RM: CXCR4, but not CXCR7, discriminates metastatic
behavior in non-small cell lung cancer cells. Mol Cancer Res.
12:38–47. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Rivas-Fuentes S, Salgado-Aguayo A, Belloso
Pertuz S, Rosete Gorocica P, Alvarado-Vasquez N and Aquino-Jarquin
G: Role of chemokines in non-small cell lung cancer: Angiogenesis
and inflammation. J Cancer. 6:938–952. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Iakovlev VV, Gabril M, Dubinski W,
Scorilas A, Youssef YM, Faragalla H, Kovacs K, Rotondo F, Metias S,
Arsanious A, et al: Microvascular density as an independent
predictor of clinical outcome in renal cell carcinoma: An automated
image analysis study. Lab Invest. 92:46–56. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Weidner N, Carroll PR, Flax J, Blumenfeld
W and Folkman J: Tumor angiogenesis correlates with metastasis in
invasive prostate carcinoma. Am J Pathol. 143:401–409.
1993.PubMed/NCBI
|