Introduction
Gastrointestinal stromal tumors (GISTs) are the most
common mesenchymal tumors of the gastrointestinal tract, accounting
for 80% of all digestive mesenchymal tumors. It is widely accepted
that GISTs arise from the interstitial cells of Cajal, and the term
‘stromal tumor’ was first introduced by Mazur and Clark in 1983
(1). The incidence of GISTs has been
reported to range between 11 and 15 per million annually (2–4), and 60%
of GISTs are located in the stomach, 30% in the jejunum or ileum,
5% in the duodenum and 4% in the colorectum. Extragastrointestinal
GISTs (EGISTs) have been reported in the liver, omentum, mesentery,
gallbladder and urinary bladder (5–7).
The diagnosis of GISTs is based on morphology,
positive immunohistochemistry (IHC) results for CD117 and DOG1, and
mutation analyses of KIT and platelet-derived growth factor
receptor α polypeptide gene (PDGFRA) (7–9). With
increasing use of abdominal computed tomography (CT), magnetic
resonance imaging (MRI) and endoscopy, an increasing number of
asymptomatic GISTs are diagnosed at an early stage, although the
effect of early detection of GIST on the prognosis remains unclear.
The National Institutes of Health (NIH) and Armed Forces Institute
of Pathology (AFIP) risk classification criteria are commonly used
to predict the prognosis of GISTs (10–12). Large
tumor size, high mitotic rate, non-gastric tumor location and tumor
ulceration are commonly accepted to be associated with a poor
prognosis in patients with GIST. Other factors, including sex, age,
symptoms and IHC results are also reported to be associated with
patient outcomes (13,14). However, the biological behavior of
GISTs varies widely, with unclear risk predictors, and it is
difficult to predict their malignant potential with the currently
available risk classification criteria (15).
The number of studies on the clinicopathological
characteristics of GIST in China is limited. The aim of the present
study was to update the clinicopathological and immunophenotypic
characteristics of GISTs in mainland China, and to investigate the
prognostic factors of GISTs based on these patients.
Materials and methods
Patients and diagnosis
The present study was approved by the Institutional
Review Board of Changzheng Hospital. Written informed consent was
obtained from all patients involved for the publication of any
associated data and accompanying images. The clinicopathological
and survival data of 182 patients with GIST treated surgically at
Shanghai Changzheng Hospital between January 2011 and December 2014
were retrospectively reviewed. A total of 94 males and 88 females
were included. The mean age of the patients was 59.2±12.6 years
(range, 26–88 years). The diagnosis of each patient with GIST was
established based on the results of the histopathology and IHC.
Pathological samples were collected during surgical interventions.
If the diagnosis of GIST was uncertain based on pathology, mutation
analysis for the KIT and PDGFRA genes was performed. For 136
patients with mitotic rate data, the tumors were categorized into
different risk groups according to the modified NIH and AFIP risk
classification criteria.
The following details of these patients were
collected: Age, sex, symptoms and signs, preoperative
investigations, surgical details, pathology and follow-up data. The
tumor site was analyzed according to previous classification
methods (16,17). Preoperative investigations comprised
radiological and endoscopic examinations, including gastroscopy,
abdominal CT, MRI, colonoscopy, small intestinal endoscopy, capsule
endoscopy and positron emission tomography (PET)-CT.
Pathology and IHC
Tissues were fixed in formalin for 12–24 h at room
temperature then paraffin-embedded. Sections of 4 µM were stained
with Hematoxylin & Eosin at room temperature (3–5 min for
hematoxylin and 5–10 sec for eosin) (18). Tissue sections were deparaffined in
xylene and rehydrated in a descending alcohol series. Antigen
retrieval was performed by heating the sections for 30 min at 95°C
in 1 mM EDTA buffer (pH 8.0). Endogenous peroxidase activity was
eliminated by treating sections with 3% methanolic hydrogen
peroxide solution for 10 min. Thereafter, the slides were blocked
in 1/100 diluted goat serum (cat. no. kit-9710; Fuzhou Maixin
Biotech Co., Ltd., Fuzhou China) for 20 min at room temperature.
IHC analysis included common biomarkers for the diagnosis of GISTs,
including CD117 (dilution, 1:400; cat. no. kit-0029; Fuzhou Maixin,
Co., Ltd., Fuzhou, China), DOG1 (dilution, 1:400; cat. no.
kit-0035; Fuzhou Maixin Biotech Co., Ltd.), CD34 (dilution, 1:600;
cat. no. kit-0004; Fuzhou Maixin Biotech Co., Ltd.), smooth muscle
actin (SMA) (dilution, 1:600 dilution; cat. no. kit-0006; Fuzhou
Maixin Biotech Co., Ltd.), S-100 protein (dilution, 1:500; cat. no.
kit-0007; Fuzhou Maixin Biotech Co., Ltd.), Ki-67 (dilution, 1:500;
cat. no. kit-0005; Fuzhou Maixin Biotech Co., Ltd.) and desmin
(dilution, 1:600; cat. no. kit-0023; Fuzhou Maixin Biotech Co.,
Ltd.). The sections were incubated with the aforementioned
antibodies at 4°C overnight. Following 3 washes in PBS, the
sections were incubated with biotin-conjugated secondary antibody
(ready-to-use; 50 µl for each section; goat anti-mouse IgG
secondary antibody for CD34, SMA, S-100, Ki-67 and desmin; goat
anti-rabbit IgG secondary antibody for CD117 and DOG1) (cat. no.
kit-9710; Fuzhou Maixin Biotech Co., Ltd.) for 10 min at room
temperature, followed by incubation with peroxidase-conjugated
biotin-streptavidin complex (Fuzhou Maixin Biotech Co., Ltd.) for
10 min at room temperature, and finally stained with
diaminobenzidine at room temperature for 2 min, and counterstained
with hematoxylin at room temperature for 3–5 min. Mitoses were
counted in 50 high-power fields (HPF). Two professional
pathologists reviewed these results under a light microscope (×100
and ×400, magnification).
Treatment methods and follow-up
For localized primary GISTs, radical resection,
including open surgical resection and minimally invasive
techniques, were selected as the primary treatments (19). Minimally invasive techniques included
laparoscopic surgery, endoscopic surgery and endoscopy-assisted
laparoscopic surgery (20,21). For locally advanced unresectable or
metastatic GISTs, palliative surgery and/or imatinib treatment were
recommended, and imatinib adjuvant therapy following radical
resection was recommended for patients with
intermediate-to-high-risk GISTs (22). The final treatment decision was made
with the consent of the patients. The records of all surgical
procedures were reviewed. Patient follow-up was conducted by
regular hospital visits at 3, 6 and 12 months, and annually
thereafter. Each visit included a medical review, physical
examination and associated investigations. The patients' status was
confirmed by telephone communication at the end of the study.
Survival outcomes were assessed in terms of overall survival (OS)
and relapse-free survival (RFS). OS was defined as the time from
the date of initial treatment to the date of the last follow-up or
mortality, and RFS was defined as the time from the date of initial
treatment to the time of clinical or radiological evidence of
disease relapse or the date of the last follow-up.
Statistical analysis
SAS 9.3 software (SAS Institute, Inc., Cary, NC,
USA) and SPSS 23.0 (IBM Corp., Armonk, NY, USA) were used for
statistical analysis. Continuous variables are expressed as mean ±
standard deviation and were compared using an unpaired, two-tailed
Student's t-test. Categorical variables were compared using the
χ2 test or Fisher's exact test. The Kaplan-Meier method
and the log-rank test were used for survival analysis. Independent
factors were identified in multivariate analysis using the Cox
proportional hazard model. P<0.05 was considered to indicate a
statistically significant difference.
Results
Clinicopathological
characteristics
A total of 182 patients with GISTs were analyzed in
the present study. The stomach was the most common site, accounting
for 73.1% of the cases, followed by the jejunum and ileum (14.3%),
duodenum (5.5%), colorectum and anus (4.94%), esophagus (1.1%), and
EGISTs (1.1%). Abdominal pain, dyspepsia and gastrointestinal
bleeding were the main presenting complaints, reported in 30.2,
23.1 and 21.4% of the patients, respectively. The symptoms varied
according to the primary location. Patients with esophageal GISTs
often presented with dysphagia (2/2 patients), whereas patients
with GISTs of the colorectum or anal canal usually reported altered
bowel habits (4/9 patients; Table
I).
 | Table I.Clinical characteristics of 182
patients with gastrointestinal stromal tumor. |
Table I.
Clinical characteristics of 182
patients with gastrointestinal stromal tumor.
| Factor | n |
|---|
| Sex, n (%) |
|
|
Male | 94
(51.6) |
|
Female | 88
(48.4) |
| Age, years |
|
|
Median | 60 |
|
Range | 26–88 |
| Location, n
(%) |
|
|
Esophagus | 2
(1.10) |
|
Stomach | 133 (73.1) |
|
Duodenum | 10
(5.50) |
| Jejunum
and ileum | 26
(14.3) |
| Colon,
rectum and anus | 9
(4.94) |
| Other
(liver and omentum) | 2
(1.10) |
|
Immunohistochemistry, n (%) |
|
|
CD117 | 179 (98.4) |
|
DOG-1 | 177 (98.3) |
|
CD34 | 171 (94.5) |
|
Desmin | 24
(13.9) |
|
S-100 | 25
(14.2) |
|
SMA | 100 (57.5) |
| Symptoms, n
(%) |
|
|
Abdominal pain | 55
(30.2) |
|
Dyspepsia | 42
(23.1) |
|
Gastrointestinal bleeding | 39
(21.4) |
|
Regurgitation | 11
(6.04) |
|
Palpable mass | 8
(4.40) |
| Altered
bowel habit | 8
(4.40) |
| Weight
loss | 4
(2.20) |
|
Fever | 3
(1.65) |
|
Dysphagia | 2
(1.10) |
|
Vomiting | 2
(1.10) |
| Pre-operation
examinations, n (%)a |
|
|
Gastroscopy | 83
(54.6) |
|
Abdominal CT scan | 87
(57.2) |
|
Endoscopic
ultrasonography | 23
(15.1) |
|
Abdominal MRI | 13 (8.6) |
|
Abdominal ultrasound | 32
(21.1) |
|
Colonoscopy | 8
(5.3) |
| Small
intestine endoscopy | 7
(4.6) |
|
PET-CT | 5
(3.3) |
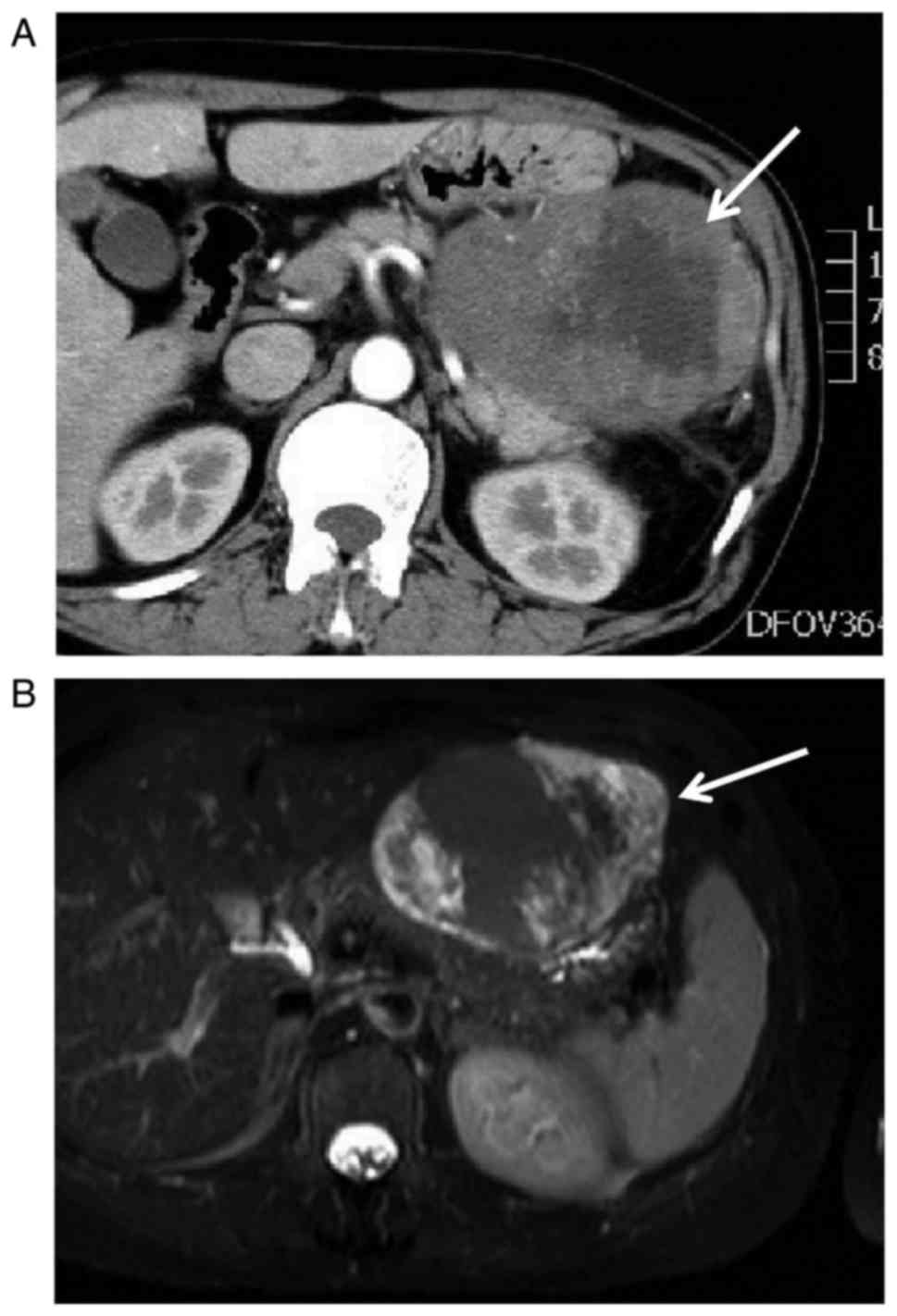
Gastroscopy and abdominal CT were used in 83 (54.6%)
and 87 (57.2%) patients, respectively, with a high diagnostic
accuracy of 62.7 and 74.7%, respectively. Other investigations,
including endoscopic ultrasonography, MRI, abdominal ultrasound,
colonoscopy, small intestinal endoscopy (or capsule endoscopy) and
PET-CT were used in 23 (15.1%), 13 (8.6%), 32 (21.1%), 8 (5.3%), 7
(4.6%) and 5 (3.3%) patients, respectively (Table I and Fig.
1). In addition, 30 patients (16.5%) were diagnosed with GIST
by pathological examination following surgery for other
conditions.
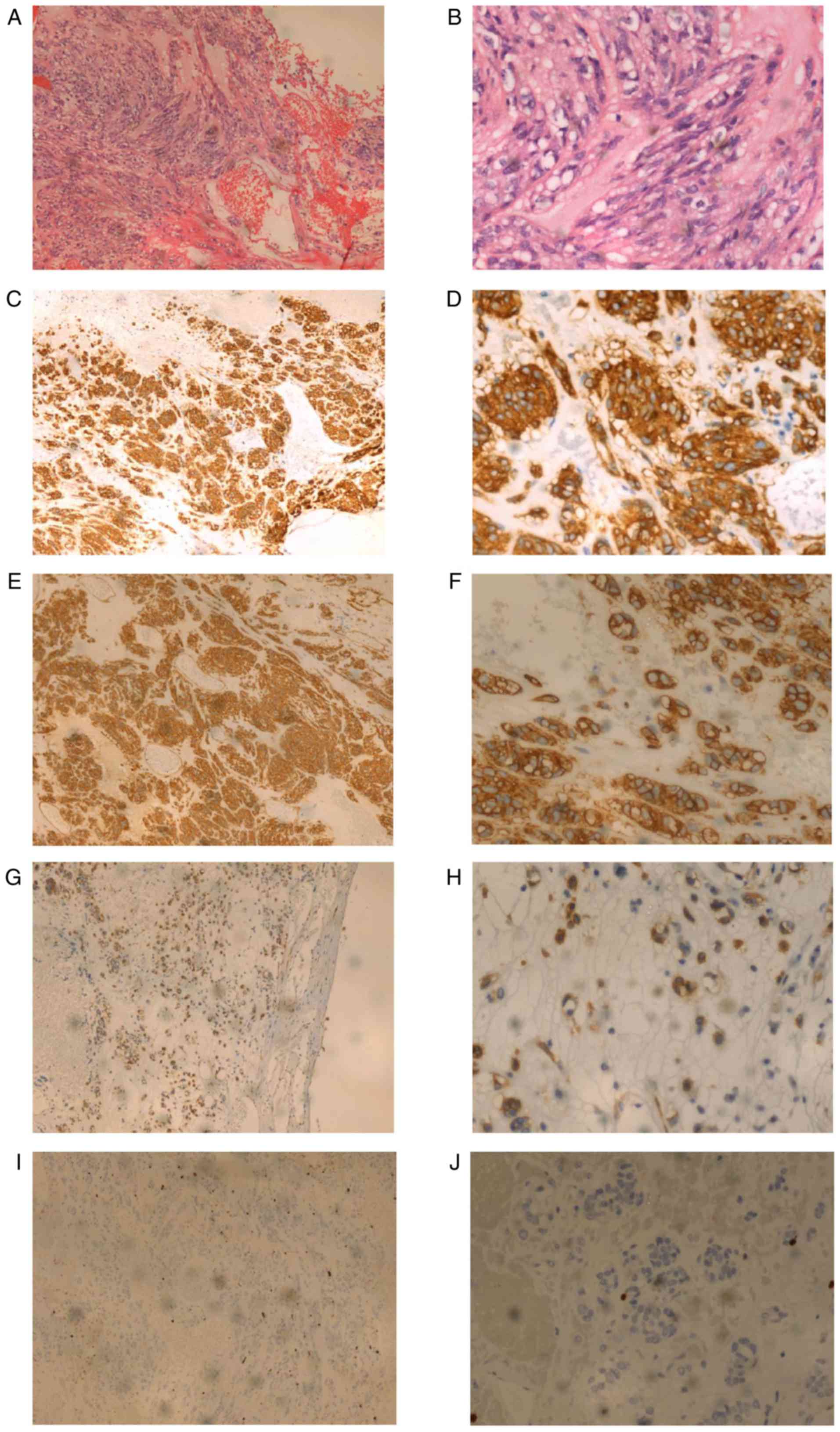
The majority of GIST samples were positive for CD117
and DOG1 according to the IHC analysis (98.4 and 98.3% cases,
respectively). In addition, 94.5% of the samples were positive for
CD34. Positive SMA, S-100 protein and desmin expression was also
detected in 57.5, 14.2 and 13.9% of the GISTs, respectively. The
Ki-67 index was 0–65%, with a mean of 7% (Table I and Fig.
2).
The malignant potential of 136 GISTs with data on
mitotic rate was evaluated. The distribution of risk groups was 17
(12.5%) in the very low-risk, 35 (25.7%) in the low-risk, 31
(22.8%) in the intermediate-risk and 53 (39.0%) in the high-risk
groups according to the NIH criteria. In addition, 72 cases (52.9%)
were classified in the benign group, 5 (3.68%) in the malignant
potential group and 59 (43.4%) in the malignancy group according to
the AFIP criteria. It was also demonstrated that larger GISTs
exhibited a higher mitotic rate (P<0.001). The NIH risk
classification of GISTs at different sites was significantly
different (P=0.006), with GISTs in the stomach or duodenum
exhibiting a lower risk of malignancy. However, the AFIP risk
classification and mitotic rate of GISTs did not differ
significantly by primary location (P=0.0996 and P=0.1203,
respectively). Based on the symptoms of the 136 patients when they
were admitted to Changzheng Hospital, the patients were divided
into the asymptomatic GIST group (asymptomatic patients and
patients accidentally diagnosed with co-existing disease; n=46) and
the symptomatic GIST group (n=90). Patients in the asymptomatic
group had a smaller tumor size (P=0.0245) and a lower risk of
malignancy according to the NIH (P=0.0327) and AFIP (P=0.0198) risk
classification criteria (Tables II
and III).
| Table II.Association between tumor site, tumor
size and mitotic rate. |
Table II.
Association between tumor site, tumor
size and mitotic rate.
| Factor | n | 0-5/50 HPF | 5-10/50 HPF | >10/50 HPF |
|---|
| Location |
|
Stomach | 101 | 59 | 33 | 9 |
|
Duodenum | 9 | 7 | 1 | 1 |
| Jejunum
and ileum | 21 | 10 | 7 | 4 |
| Colon,
rectum and anus | 4 | 0 | 3 | 1 |
|
Omentum | 1 | 1 | 0 | 0 |
| Tumor size, cm |
|
0–2 | 15 | 14 | 1 | 0 |
|
2–5 | 59 | 36 | 18 | 5 |
|
5–10 | 40 | 22 | 16 | 2 |
|
≥10 | 22 | 5 | 9 | 8 |
|
Total | 136 | 77 | 44 | 15 |
| Table III.Association between symptoms, tumor
site and NIH or AFIP risk classification criteria. |
Table III.
Association between symptoms, tumor
site and NIH or AFIP risk classification criteria.
|
|
| NIH | AFIP |
|---|
|
|
|
|
|
|---|
| Factor | n | Very low | Low | Middle | High | Benign | Malignant
potential | Malignancy |
|---|
| Location |
|
Stomach | 101 | 16 | 25 | 29 | 31 | 56 | 3 | 42 |
|
Duodenum | 9 | 1 | 5 | 1 | 2 | 7 | 0 | 2 |
| Jejunum
and ileum | 21 | 0 | 5 | 0 | 16 | 8 | 1 | 12 |
| Colon,
rectum and anus | 4 | 0 | 0 | 1 | 3 | 0 | 1 | 3 |
|
Omentum | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 |
| Symptoms |
|
Asymptomatic | 46 | 8 | 13 | 14 | 11 | 31 | 1 | 14 |
|
Symptomatic | 90 | 9 | 22 | 17 | 42 | 41 | 4 | 45 |
| Total | 136 | 17 | 35 | 31 | 53 | 72 | 5 | 59 |
Treatment
Numerous surgical procedures were performed,
including partial gastric resection, total gastric resection,
partial intestinal resection, hemicolectomy, sigmoid colon
resection, abdomino-perineal rectum resection,
pancreatoduodenectomy, distal pancreatectomy and endoscopic
submucosal dissection. The choice of surgical procedure was
individualized, depending on the tumor location, size and
possibility of complete resection. Excluding the 30 patients who
were incidentally diagnosed with GIST while treated for other
conditions, 125 of the remaining 152 patients underwent radical
resection of the primary tumor. Among these patients, 71 underwent
open surgical resection; 47 underwent laparoscopic resection; 3
underwent endoscopic surgery; and 4 underwent endoscopic-assisted
laparoscopic surgery. An additional 27 patients with unresectable
tumors received palliative surgery, including 19 open surgery and 8
laparoscopic surgery. In 24 of the patients, the tumors displayed
clear malignant characteristics during surgery, including local
invasion and metastasis. Additionally, 5 patients were revealed to
have tumor bleeding and ulceration. Imatinib as adjuvant therapy
was administered to 15 patients with intermediate-to-high-risk
GISTs, including 6 patients with advanced disease. No neoadjuvant
imatinib therapy was used in the patients enrolled in the present
study.
Survival analysis
Based on the 152 patients without co-existing
diseases, the median follow-up time was 48 months (range, 3–81
months), and the 5-year OS and RFS rates were 85.4% (95% CI:
79.5–91.3) and 83.8% (95% CI: 77.5–90.1), respectively. A total of
21 patients succumbed during the follow-up period as a result of
various causes (disease progression, other chronic diseases,
including diabetes mellitus, cardiovascular and cerebral disorders,
other malignancies and trauma). A total of 4 patients developed
metastases in the abdominopelvic cavity and 3 in the liver during
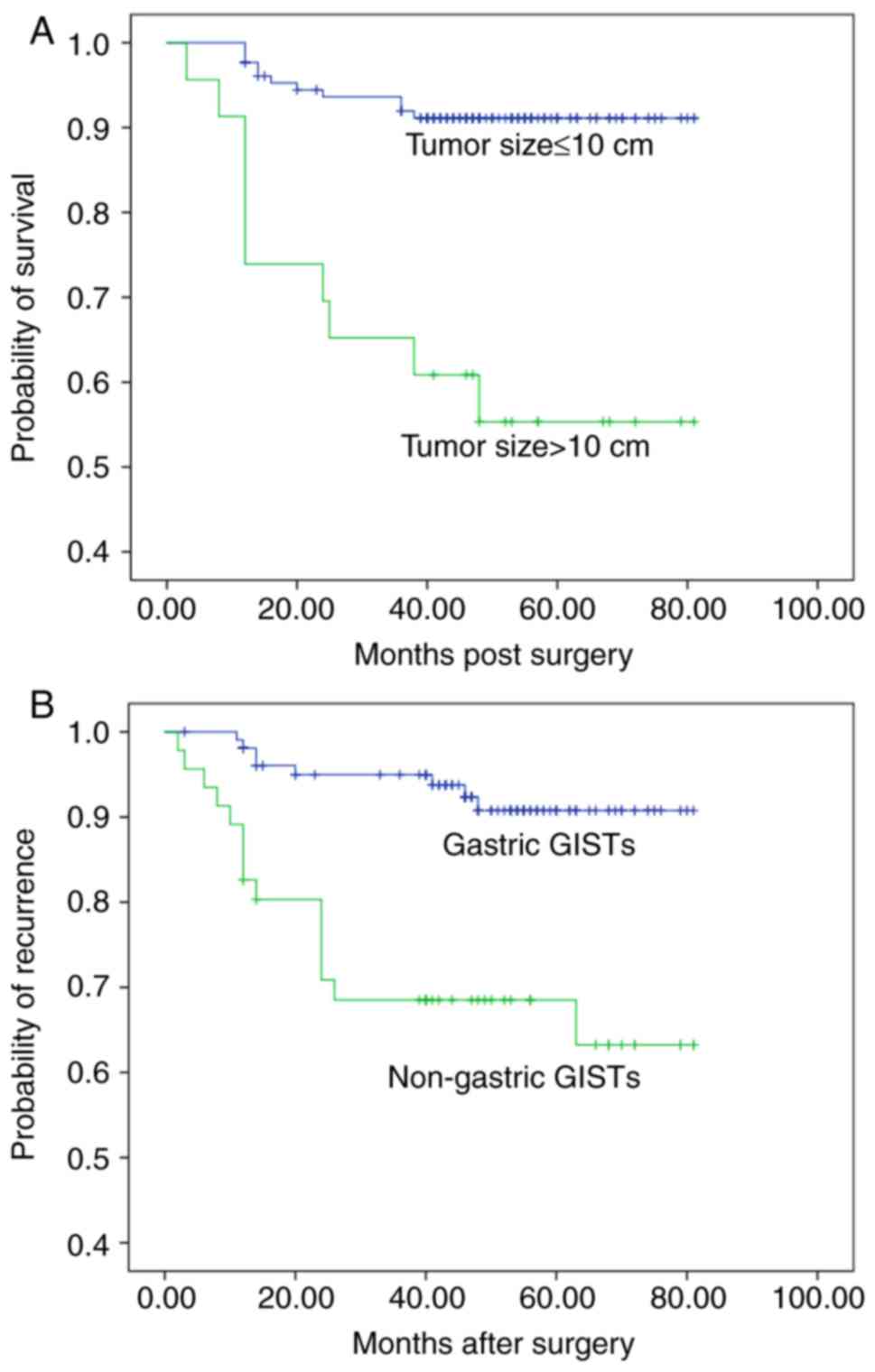
follow-up. The results of the univariate analysis of potential
prognostic factors are presented in Table IV and Fig.
3. Larger tumor size (>10 cm; P<0.001), higher mitotic
rate (>10/50 HPF; P<0.001), aggressive behavior, including
tumor metastasis or local invasion prior to treatment (P<0.001)
and negative SMA expression (P=0.009) contributed toward poorer
survival of patients with GIST. In addition, non-gastric disease
location (P<0.001), larger tumor size (>10 cm; P<0.001),
higher mitotic rate (>10/50 HPF; P=0.004) and aggressive
behavior (P<0.001) were associated with higher risk of
recurrence. Patients receiving palliative tumor resection had a
significantly shorter survival time (P<0.001) and a higher risk
of recurrence (P<0.001). When therapeutic factors were included
in the multivariate analysis, palliative surgical resection was the
only independent risk factor for OS (HR=9.196, 95% CI:
3.327–25.417, P<0.001) and RFS (HR=16.42, 95% CI: 6.065–44.454,
P<0.001). If the therapeutic factors were excluded, the
multivariate analysis indicated that the mitotic rate (HR=3.761,
95% CI: 1.288–10.987, P=0.015) and aggressive behavior (HR=3.916,
95% CI: 1.389–11.044, P=0.010) were independent risk factors for
OS. Non-gastric disease location (HR=4.740, 95% CI: 1.747–12.857,
P=0.002) and aggressive behavior (HR=4.009, 95% CI: 1.538–10.449,
P=0.004) were independent risk factors for RFS (Table V).
| Table IV.Univariate analysis of prognostic
factors for OS and RFS in 152 GIST patients. |
Table IV.
Univariate analysis of prognostic
factors for OS and RFS in 152 GIST patients.
|
|
| OS | RFS |
|---|
|
|
|
|
|
|---|
| Group | N | 5-year OS | P-value | 5-year RFS | P-value |
|---|
| Sex |
|
Male | 69 | 84.0 | 0.724 | 81.8 | 0.361 |
|
Female | 83 | 86.5 |
| 85.5 |
|
| Age (years) |
|
≤60 | 83 | 88.5 | 0.177 | 87.1 | 0.360 |
|
>60 | 69 | 81.3 |
| 79.5 |
|
| Disease
location |
|
Gastric | 106 | 87.8 | 0.192 | 90.8 |
<0.001a |
|
Non-gastric | 46 | 79.9 |
| 68.5 |
|
| Tumor size
(cm) |
|
≤10 | 129 | 91.1 |
<0.001a | 87.6 |
<0.001a |
|
>10 | 23 | 55.3 |
| 60.1 |
|
| Mitotic rate (/50
HPF) |
|
≤10 | 107 | 89.3 |
<0.001a | 87.3 | 0.004a |
|
>10 | 14 | 54.5 |
| 58.9 |
|
| Metastatic disease
or local invasion |
|
Yes | 24 | 49.0 |
<0.001a | 44.9 |
<0.001a |
| No | 128 | 91.9 |
| 90.2 |
|
| Ulceration |
|
Yes | 5 | 80.0 | 0.664 | 80.0 | 0.120 |
| No | 147 | 85.5 |
| 84.0 |
|
| Desmin |
|
Positive | 19 | 82.6 | 0.841 | 85.9 | 0.539 |
|
Negative | 130 | 85.7 |
| 83.3 |
|
| S-100 |
|
Positive | 23 | 85.6 | 0.907 | 95.5 | 0.132 |
|
Negative | 126 | 86.0 |
| 82.1 |
|
| SMA |
|
Positive | 89 | 91.4 | 0.009a | 85.4 | 0.448 |
|
Negative | 58 | 76.7 |
| 80.3 |
|
| Symptom |
|
Asymptomatic | 36 | 91.2 | 0.301 | 93.0 | 0.077 |
|
Symptomatic | 116 | 83.6 |
| 81.0 |
|
| Resection
margin |
|
Radical | 125 | 93.4 |
<0.001a | 94.4 |
<0.001a |
|
Palliative | 27 | 46.6 |
| 28.4 |
|
| Surgical
procedures |
|
Open | 90 | 82.6 | 0.232 | 82.8 | 0.587 |
|
Minimally invasive | 62 | 89.7 |
| 85.0 |
|
| Imatinib
therapyb |
|
Yes | 15 | 86.2 | 0.388 | 54.3 | 0.052 |
| No | 71 | 77.0 |
| 83.0 |
|
| Table V.Multivariate analysis of prognostic
factors for OS and RFS in 152 patients with gastrointestinal
stromal tumors (therapeutic factors excluded). |
Table V.
Multivariate analysis of prognostic
factors for OS and RFS in 152 patients with gastrointestinal
stromal tumors (therapeutic factors excluded).
|
| OS | RFS |
|---|
|
|
|
|
|---|
| Factor | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Disease location
(gastric vs. non-gastric) | – | – | – | 4.740 | 1.747–12.857 | 0.002a |
| Mitotic rate
(≤10/50 HPF vs. >10/50 HPF) | 3.761 | 1.288–10.987 | 0.015a | – | – | – |
| Metastatic disease
or adjacent involvement (no vs. yes) | 3.916 | 1.389–11.044 | 0.010a | 4.009 | 1.538–10.449 | 0.004a |
Discussion
The present retrospective study, based on 182
Chinese patients with GIST, aimed to investigate the
clinicopathological and prognostic characteristics of this disease.
The results are comparable with those of previous studies in other
populations (23–27). The median age of the patients in the
present study was 60 years. The stomach was the most common primary
site of GISTs, while patients with GIST usually lack specific
symptoms. In line with the results of a Japanese study that
indicated that GISTs may be incidentally discovered during gastric
cancer screening (28), 36 patients
in the present study were asymptomatic without co-existing diseases
and their GISTs were detected during their annual physical exam.
Radical tumor resection is the most important factor affecting
patient prognosis. Furthermore, non-gastric disease location,
higher mitotic rate and tumor metastasis or local invasion prior to
treatment were revealed to be predictors of a poor prognosis.
For GIST patients with clinical symptoms and those
with incidentally detected tumors during physical examination,
further radiological and endoscopic examinations are required
(29). In the present study, 52
patients were diagnosed with GIST by gastroscopy and 65 by
abdominal CT. Gastroscopic and endoscopic ultrasonography can
detect mostly intramural tumors and enable acquisition of
cytological or histological samples, while the use of endoscopy is
limited when evaluating metastasis outside the digestive tract
(30). Abdominal CT can scan the
whole abdomen and is able to detect small lesions, providing
valuable information on the size, morphology, aggressiveness and
metastasis of the tumors (31,32).
Abdominal MRI and PET-CT also have high diagnostic sensibility,
particularly in intestinal GISTs or EGISTs, and were used in 13 and
5 patients, respectively. MRI is affected by peristalsis of the
gastrointestinal tract, which limits its applicability, although it
has been reported that, for lesions of the rectum and liver, MRI
may offer more detailed images compared with CT (33). PET-CT is applied for evaluating tumor
metastasis and response following the initiation of targeted
therapy (34). Among patients with
intestinal GISTs, the diagnosis of 7 patients in the present study
series was confirmed by small intestinal endoscopy or capsule
endoscopy, as their tumors were relatively difficult to
diagnose.
There are no standard criteria for assessing the
aggressive behavior and predicting the clinical prognosis of GISTs,
although the NIH and AFIP criteria are widely recommended (35). It is commonly accepted that all GISTs
are considered to have malignant potential (36). Through multivariate analysis, higher
mitotic rate and tumor metastasis or local invasion prior to
treatment were revealed to be associated with poor survival in GIST
patients, and non-gastric disease location was associated with
tumor recurrence, which is consistent with the results of previous
studies (16). Similarly, one British
study (17) identified high mitotic
index as an independent poor prognostic factor in these patients.
Miettinen and Lasota (37) also
demonstrated that small intestinal GISTs behave more aggressively
than gastric GISTs, and small intestinal GISTs tend to be larger
and more advanced at diagnosis. Liu et al (35) suggested that gastrointestinal bleeding
is a prognostic factor. However, preoperative symptoms did not
appear to affect the outcome of patients with GIST in our analysis.
Large tumor size is considered to be a prognostic factor in the NIH
and AFIP risk classification criteria. However, it failed to be an
independent risk factor in the present study. Notably, patients
with SMA-negative tumors exhibited a shorter survival time.
Similarly, Demir et al (38)
reported that patients with SMA-positive GISTs tended to survive
longer and had significantly longer disease-free survival (DFS)
times than the SMA-negative cases. Fujimoto et al (39) reported no association between SMA IHC
analysis and the prognosis of patients with GIST. However, Bertin
et al (40) reported that SMA
positivity is significantly associated with a lower 5-year survival
rate (39 vs. 100%). Differences in the selected population, tumor
location, disease stage and treatment between these studies may
affect these conclusions.
GISTs are usually asymptomatic until they reach a
large size, at which point they may cause non-specific symptoms or
be detected as a palpable mass (41).
Compared with patients diagnosed with clinical symptoms,
asymptomatic patients are considered to have early-stage disease. A
total of 46 patients in the present study were asymptomatic or
accidentally diagnosed with co-existing disease, and these GISTs
were smaller in size and exhibited a lower risk based on the NIH
and AFIP risk classification criteria, although no significant
effect on OS and RFS was observed. A study by Yamamoto et al
(28) reported that GISTs are
incidentally observed during gastric cancer screenings in Japan.
Over half of these patients are asymptomatic and have smaller
tumors (P<0.001) and lower recurrence rates (P=0.017), compared
with symptomatic patients. Therefore, the Japanese gastric cancer
screening system contributes toward the early detection of gastric
GISTs and favorable treatment outcomes by identifying asymptomatic
patients. Scherubl et al (30)
demonstrated that early asymptomatic GISTs have an excellent
GIST-specific prognosis. The results of the present study also
suggested that detecting GISTs at an early stage may improve
patient outcome.
For resectable localized GISTs, radical surgery is
the standard and first choice of treatment (42). Radical tumor resection significantly
improved survival and reduced tumor recurrence, in univariate or
multivariate analyses. Different surgical approaches, including
open and laparoscopic surgery and endoscopic procedures, were
performed in the present study. No statistically significant
difference was observed in OS or RFS among these surgical
strategies. A number of studies have been performed comparing the
effect of minimally invasive and open surgery in the treatment of
GISTs (42–44). It is generally accepted that minimally
invasive surgery has similar or even superior perioperative
outcomes, without compromising the oncological outcomes; it may
also be safely used for larger tumors or tumors located in
unfavorable sites. Imatinib serves an important role in the
treatment of advanced GISTs and in the adjuvant setting, reducing
the risk of recurrence and metastasis (16,45). In
the present study, not all the patients with intermediate-to-high
risk GIST received imatinib as adjuvant therapy. However, there was
no observed improvement in OS and RFS in the 15 patients who were
administered adjuvant imatinib therapy. One possible reason may be
that the selection of candidates for adjuvant therapy was not
standardized and the sample size was limited. Imatinib was also
recommended to patients receiving palliative surgery and those with
disease progression. Advanced GISTs will inevitably progress and
reduce the OS and RFS rates (16).
GISTs are widely considered to have a low risk of
lymph node metastasis; therefore, lymphadenectomy is not deemed
necessary during surgical resection (46,47).
However, GIST cases with lymph node metastasis have been reported.
Tashiro et al (48) and
Shafizad et al (49) reported
two cases of lymph node involvement in gastric GISTs. In addition,
Gong et al (50) reported that
6 of 29 (20.7%) patients with GIST were revealed to have lymph node
metastasis on PET-CT imaging. In the present study, lymph node
metastasis was detected in only 1 patient with a history of
intestinal GIST resection 2 years prior. Palliative surgery was
performed and two main masses were removed from the small
intestine. Tumor ulceration and bleeding were observed
intraoperatively, and liver, peritoneal and pelvic cavity
metastasis were confirmed. All 7 mesenteric lymph nodes resected
during surgery were positive. Despite these reports, however, GISTs
rarely metastasize to the lymph nodes, and regional lymph node
resection is of unproven value (16).
There were certain limitations to the present study:
The design of the study was retrospective; the selection of
surgical approach and adjuvant therapy were not standardized; and
the use of imatinib as an adjuvant therapy was limited to 15
patients with a potential selection bias; therefore, the benefit of
using imatinib as adjuvant therapy cannot be evaluated based on
this study. In summary, the present study updated the
clinicopathological and immunophenotypic characteristics of GISTs
in mainland China. Asymptomatic GISTs may be of smaller size and
have a lower risk of malignancy according to the NIH and AFIP risk
classification criteria. Clinical and immunohistochemical results
were used for survival analysis, and positive SMA was associated
with an improved survival in univariate analysis. Higher mitotic
rate and tumor metastasis or local invasion prior to treatment were
revealed to be independent risk factors for a poor OS, whereas
non-gastric disease location and aggressive behavior were
independent risk factors for a poor RFS. Large tumor size, a
prognostic factor in the NIH and AFIP risk classification criteria,
failed to reveal significant impact on OS and RFS in multivariate
analysis. The present study may aid clinicians with an improved
understanding of the diagnosis and treatment of GISTs.
Acknowledgements
Not applicable.
Funding
This study was supported by the Project of
Innovation Incubation Base of Second Military Medical University
(grant no. FH2016183).
Availability of data and materials
All data generated and/or analyzed during this study
are included in this published article.
Authors' contributions
YML analyzed and interpreted the patient data
regarding GIST disease, performed statistical analysis and wrote
the manuscript. WJC recorded the follow-up information, performed
statistical analysis and wrote the manuscript. ZWB analyzed and
interpreted the data and critically reviewed the manuscript. YDK
designed the study and the quality control of data and algorithms,
and reviewed the manuscript. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The present retrospective study was approved by
Changzheng Hospital Medical Committee. Written informed consent was
obtained from all participating patients.
Patient consent for publication
The patient or parent, guardian or next of kin
provided written informed consent for the publication of any
associated data and accompanying images. All identifying
information was removed.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Mazur MT and Clark HB: Gastric stromal
tumors. Reappraisal of histogenesis. Am J Surg Pathol. 7:1–519.
1983. View Article : Google Scholar
|
|
2
|
Goettsch WG, Bos SD, Breekveldt-Postma N,
Casparie M, Herings RM and Hogendoorn PC: Incidence of
gastrointestinal stromal tumours is underestimated: Results of a
nation-wide study. Eur J Cancer. 41:2868–2872. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wang M, XU J, Zhang Y, Tu L, Qiu WQ, Wang
CJ, Shen YY, Liu Q and Cao H: Gastrointestinal stromal tumor:
15-years' experience in a single center. BMC Surg. 14:932014.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pisters PW, Blanke CD, von Mehren M, Picus
J, Sirulnik A, Stealey E and Trent JC; reGISTry Steering Committee,
: A USA registry of gastrointestinal stromal tumor patients:
Changes in practice over time and differences between community and
academic practices. Ann Oncol. 22:2523–2529. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Miettinen M, Monihan JM, Sarlomo-Rikala M,
Kovatich AJ, Carr NJ, Emory TS and Sobin LH: Gastrointestinal
stromal tumors/smooth muscle tumors (GISTs) primary in the omentum
and mesentery: Clinicopathologic and immunohistochemical study of
26 cases. Am J Surg Pathol. 23:1109–1118. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miettinen M, Makhlouf H, Sobin LH and
Lasota J: Gastrointestinal stromal tumors of the jejunum and ileum:
A clinicopathologic, immunohistochemical, and molecular genetic
study of 906 cases before imatinib with long-term follow-up. Am J
Surg Pathol. 30:477–489. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhao X and Yue C: Gastrointestinal stromal
tumor. J Gastrointest Oncol. 3:189–208. 2012.PubMed/NCBI
|
|
8
|
Blay JY, Shen L, Kang YK, Rutkowski P, Qin
S, Nosov D, Wan D, Trent J, Srimuninnimit V, Pápai Z, et al:
Nilotinib versus imatinib as first-line therapy for patients with
unresectable or metastatic gastrointestinal stromal tumours
(ENESTg1): A randomised phase 3 trial. Lancet Oncol. 16:550–560.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cassier PA, Ducimetiere F, Lurkin A,
Ranchère-Vince D, Scoazec JY, Bringuier PP, Decouvelaere AV, Méeus
P, Cellier D, Blay JY and Ray-Coquard I: A prospective
epidemiological study of new incident GISTs during two consecutive
years in rhone alpes region: Incidence and molecular distribution
of GIST in a european region. Br J Cancer. 103:165–170. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Joensuu H: Risk stratification of patients
diagnosed with gastrointestinal stromal tumor. Hum Pathol.
39:1411–1419. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Goh BK, Chow PK, Yap WM, Kesavan SM, Song
IC, Paul PG, Ooi BS, Chung YF and Wong WK: Which is the optimal
risk stratification system for surgically treated localized primary
GIST? Comparison of three contemporary prognostic criteria in 171
tumors and a proposal for a modified armed forces institute of
pathology risk criteria. Ann Surg Oncol. 15:2153–2163. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Belfiori G, Sartelli M, Cardinali L, Tranà
C, Bracci R, Gesuita R and Marmorale C: Risk stratification systems
for surgically treated localized primary gastrointestinal stromal
tumors (GIST). Review of literature and comparison of the three
prognostic criteria: MSKCC nomogramm, NIH-fletcher and
AFIP-miettinen. Ann Ital Chir. 86:219–227. 2015.PubMed/NCBI
|
|
13
|
Wang YP, Li YI and Song C:
Clinicopathological features and prognosis of small
gastrointestinal stromal tumors outside the stomach. Oncol Lett.
10:2723–2730. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang P, Deng R, Liu K, Shuai XM, Bai J,
Chang WL, Gao JB, Cai KL, Wang GB and Tao KX: Clinicopathologic
features and prognosis of primary gastrointestinal stromal tumor
patients under 35 years of age: A 10-year retrospective study. J
Surg Oncol. 114:977–981. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liu X, Qiu H, Zhang P, Feng X, Chen T, Li
Y, Tao K, Li G, Sun X and Zhou Z; China Gastrointestinal Stromal
Tumor Study Group (CN-GIST), : Ki-67 labeling index may be a
promising indicator to identify ‘very high risk’ gastrointestinal
stromal tumor: A multicenter retrospective study of 1022 patients.
Hum Pathol. 74:17–24. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cao H, Zhang Y, Wang M, Shen DP, Sheng ZY,
Ni XZ, Wu ZY, Liu Q, Shen YY and Song YY: Prognostic analysis of
patients with gastrointestinal stromal tumors: A single unit
experience with surgical treatment of primary disease. Chin Med J
(Engl). 123:131–136. 2010.PubMed/NCBI
|
|
17
|
Mrowiec S, Jabłońska B, Liszka L, Pająk J,
Leidgens M, Szydło R, Sandecka A and Lampe P: Prognostic factors
for survival post surgery for patients with gastrointestinal
stromal tumors. Eur Surg Res. 48:3–9. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang X, Li WQ, Yan HZ, Li YM, He J, Liu HM
and Yu HY: Alveolar adenoma combined with multifocal cysts: Case
report and literature review. J Int Med Res. 41:895–906. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Badic B, Gancel Ch, Thereaux J, Joumond A,
Bail JP, Meunier B and Sulpice L: Surgical and oncological long
term outcomes of gastrointestinal stromal tumors (GIST)
resection-retrospective cohort study. Int J Surg. 53:257–261. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tan Y, Tan L, Lu J, Huo J and Liu D:
Endoscopic resection of gastric gastrointestinal stromal tumors.
Transl Gastroenterol Hepatol. 2:1152017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Koh YX and Goh B: Minimally invasive
surgery for gastric gastrointestinal stromal tumors. Transl
Gastroenterol Hepatol. 2:1082017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ford SJ and Gronchi A: Indications for
surgery in advanced/metastatic GIST. Eur J Cancer. 63:154–167.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tran T, Davila Ja and El-serag HB: The
epidemiology of malignant gastrointestinal stromal tumors: An
analysis of 1,458 cases from 1992 to 2000. Am J Gastroenterol.
100:162–168. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tryggvason G, Gislason HG, Magnusson MK
and Jonasson JG: Gastrointestinal stromal tumors in Iceland,
1990–2003: The icelandic GIST study, a population-based incidence
and pathologic risk stratification study. Int J Cancer.
117:289–293. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Rubio J, Marcos-Gragera R, Ortiz MR, Miró
J, Vilardell L, Gironès J, Hernandez-Yagüe X, Codina-Cazador A,
Bernadó L, Izquierdo A and Colomer R: Population-based incidence
and survival of gastrointestinal stromal tumours (GIST) in girona,
spain. Eur J Cancer. 43:144–148. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mucciarini C, Rossi G, Bertolini F, Valli
R, Cirilli C, Rashid I, Marcheselli L, Luppi G and Federico M:
Incidence and clinicopathologic features of gastrointestinal
stromal tumors. A population-based study. BMC Cancer. 7:2302007.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Chiang NJ, Chen LT, Tsai CR and Chang JS:
The epidemiology of gastrointestinal stromal tumors in taiwan,
1998–2008: A nation-wide cancer registry-based study. BMC Cancer.
14:1022014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yamamoto K, Tsujinaka T, Takahashi T, Sato
S, Nishiguchi Y, Nakashima Y, Muguruma K, Hirota S and Nishida T:
Impact of the Japanese gastric cancer screening system on treatment
outcomes in gastric gastrointestinal stromal tumor (GIST): An
analysis based on the GIST registry. Ann Surg Oncol. 22:232–239.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sandrasegaran K, Rajesh A, Rydberg J,
Rushing DA, Akisik FM and Henley JD: Gastrointestinal stromal
tumors: Clinical, radiologic, and pathologic features. AJR Am J
Roentgenol. 184:803–811. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Scherubl H, Faiss S, Knoefel WT and
Wardelmann E: Management of early asymptomatic gastrointestinal
stromal tumors of the stomach. World J Gastrointest Endosc.
6:266–271. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Horton KM, Juluru K, Montogomery E and
Fishman EK: Computed tomography imaging of gastrointestinal stromal
tumors with pathology correlation. J Comput Assist Tomogr.
28:811–817. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Shi Z and Zhuang Q: Computed tomography
imaging characteristics of synchronous gastrointestinal stromal
tumors in patients with gastric cancer and correlation with
clinicopathological findings. Mol Clin Oncol. 3:1311–1314. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lamba G, Gupta R, Lee B, Ambrale S and Liu
D: Current management and prognostic features for gastrointestinal
stromal tumor (GIST). Exp Hematol Oncol. 1:142012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Tokumoto N, Tanabe K, Misumi T, Fujikuni
N, Suzuki T and Ohdan H: The usefulness of preoperative 18FDG
positron- emission tomography and computed tomography for
predicting the malignant potential of gastrointestinal stromal
tumors. Dig Surg. 31:79–86. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Liu Q, Li Y, Dong M, Kong F and Dong Q:
Gastrointestinal bleeding is an independent risk factor for poor
prognosis in GIST patients. Biomed Res Int.
2017:71524062017.PubMed/NCBI
|
|
36
|
Yamamoto H and Oda Y: Gastrointestinal
stromal tumor: Recent advances in pathology and genetics. Pathol
Int. 65:9–18. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumors: Review on morphology, molecular pathology,
prognosis, and differential diagnosis. Arch Pathol Lab Med.
130:1466–1478. 2006.PubMed/NCBI
|
|
38
|
Demir L, Ekinci N, Erten C, Kucukzeybek Y,
Alacacioglu A, Somali I, Can A, Dirican A, Bayoglu V, Akyol M, et
al: Does immunohistochemistry provide additional prognostic data in
gastrointestinal stromal tumors? Asian Pac J Cancer Prev.
14:4751–4758. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Fujimoto Y, Nakanishi Y, Yoshimura K and
Shimoda T: Clinicopathologic study of primary malignant
gastrointestinal stromal tumor of the stomach, with special
reference to prognostic factors: Analysis of results in 140
surgically resected patients. Gastric Cancer. 6:39–48. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Bertin M, Angriman I, Scarpa M, Mencarelli
R, Ranzato R, Ruffolo C, Polese L, Iacobone M and D'Amico DF:
Prognosis of gastrointestinal stromal tumors.
Hepatogastroenterology. 54:124–128. 2007.PubMed/NCBI
|
|
41
|
Dematteo RP, Heinrich MC, El-Rifai WM and
Demetri G: Clinical management of gastrointestinal stromal tumors:
Before and after STI-571. Hum Pathol. 33:466–477. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Novitsky YW, Kercher KW, Sing RF and
Heniford BT: Long-term outcomes of laparoscopic resection of
gastric gastrointestinal stromal tumors. Ann Surg. 243:738–745,
745–747. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Lin J, Huang C, Zheng C, Li P, Xie J, Wang
J and Lu J: Laparoscopic versus open gastric resection for larger
than 5 cm primary gastric gastrointestinal stromal tumors (GIST): A
size-matched comparison. Surg Endosc. 28:2577–2583. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Liao GQ, Chen T, Qi XL, Hu YF, Liu H, Yu J
and Li GX: Laparoscopic management of gastric gastrointestinal
stromal tumors: A retrospective 10-year single-center experience.
World J Gastroenterol. 23:3522–3529. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Blay JY, Le Cesne A, Ray-Coquard I, Bui B,
Duffaud F, Delbaldo C, Adenis A, Viens P, Rios M, Bompas E, et al:
Prospective multicentric randomized phase III study of imatinib in
patients with advanced gastrointestinal stromal tumors comparing
interruption versus continuation of treatment beyond 1 year: The
french sarcoma group. J Clin Oncol. 25:1107–1113. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Papalambros A, Petrou A, Brennan N, Bramis
K, Felekouras E and Papalambros E: GIST suture-line recurrence at a
gastrojejunal anastomosis 8 years after gastrectomy: Can GIST ever
be described as truly benign? A case report. World J Surg Oncol.
8:902010. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Demetri GD, Benjamin RS, Blanke CD, Blay
JY, Casali P, Choi H, Corless CL, Debiec-Rychter M, DeMatteo RP,
Ettinger DS, et al: NCCN task force report: Management of patients
with gastrointestinal stromal tumor (GIST)-update of the NCCN
clinical practice guidelines. J Natl Compr Canc Netw. 2 Suppl
5:S1–S29, S30. 2007.
|
|
48
|
Tashiro T, Hasegawa T, Omatsu M, Sekine S,
Shimoda T and Katai H: Gastrointestinal stromal tumour of the
stomach showing lymph node metastases. Histopathology. 47:438–439.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Shafizad A, Mohammadianpanah M, Nasrolahi
H, Mokhtari M and Mousavi SA: Lymph node metastasis in
gastrointestinal stromal tumor (GIST): To report a case. Iran J
Cancer Prev. 7:171–174. 2014.PubMed/NCBI
|
|
50
|
Gong N, Wong CS and Chu YC: Is lymph node
metastasis a common feature of gastrointestinal stromal tumor?
PET/CT correlation. Clin Nucl Med. 36:678–682. 2011. View Article : Google Scholar : PubMed/NCBI
|