Introduction
Globally, the incidence of colorectal cancer ranks
as the fifth highest of all malignant tumor types. Cancer mortality
caused by colorectal cancer accounts for the sixth highest cancer
mortality rate globally (1). One
previous study reported that the incidence of rectal cancer
accounts for ~40% of the total incidence of colorectal cancer, and
that there is a rising trend (2).
Locally advanced rectal cancer constitutes up to 50% of all rectal
cancer types and includes nonresectable and borderline-resectable
tumor types (3). Currently,
neoadjuvant chemoradiotherapy (NCRT) combined with postoperative
chemotherapy, or neoadjuvant chemotherapy combined with
postoperative chemoradiotherapy, are the standard treatments for
local advanced rectal cancer (LARC) in the National Comprehensive
Cancer Network (NCCN) guidelines (4).
Pathological complete response (pCR) following NCRT
is an important prognostic indicator for patients with excellent
treatment outcomes (5,6). Tumor regression occurs slowly.
Prolonging treatment intervals in rectal cancer may increase the
pCR of the patient, R0 resection, and anus preservation rates
(7,8).
To achieve an improved pCR rate, a number of studies recommend an
interval of 7–8 weeks between NCRT and surgery (7–9). However,
the high pCR rate obtained from long intervals between NCRT and
surgery is not associated with a survival benefit, with long and
short treatment intervals conferring a similar rate of overall
survival (OS) (10–12). Notably, Supiot et al (13) reported that OS and recurrence-free
survival (RFS) were slightly lower in the long-interval group
compared with those in the short-interval group, which may be due
to the prolonged resting period that may increase the probability
of distant metastases. This occurrence is more common in ypT3-4N0
and ypT0-4N+ patients who have high risk of distant metastases.
Preoperative chemotherapy may improve patient
tolerance to chemotherapy and reduce the incidence of distant
metastases. Therefore, theoretically, consolidation chemotherapy
between NCRT and surgery may increase the rate of OS and DFS, in
addition to distant metastases-free survival (DMFS). Although no
corresponding guidelines have been established to date,
consolidation chemotherapy is gradually attracting the attention of
the research community.
In the present study, the impact of adding
consolidation chemotherapy for rectal cancer during the resting
period was retrospectively analyzed in order to determine whether
consolidation chemotherapy resulted in higher rates of pCR and near
pCR and improved survival, and to assess the influence of
consolidation chemotherapy on chemotherapy toxicities, surgical
outcomes and postoperative complications.
Patients and methods
Patients
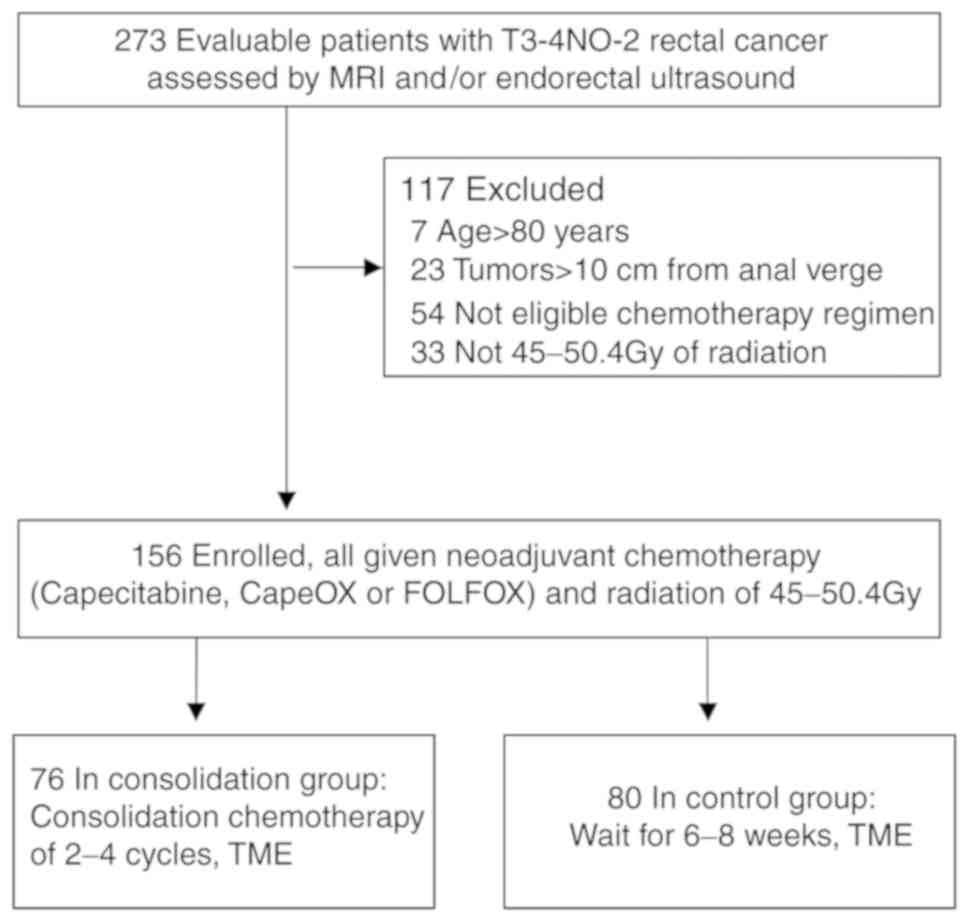
A total of 273 patients with cT3-4 N0-2 M0 LARC who
underwent neoadjuvant chemoradiation followed by radical resection
with total mesorectal excision (TME) at Nanfang Hospital of
Southern Medical University (Guangzhou, China) were reviewed. The
selection criteria were: i) Age ≤80 years; ii) cT3-4 N0-2 M0 LARC;
iii) tumor located 0–10 cm from anal verge; iv) underwent
neoadjuvant chemoradiation followed by TME; v) chemotherapeutic
regimen was capecitabine, CapeOX or FOLFOX; and vi) dose of
radiotherapy was 45–50.4 Gy. Of these patients, 117 were excluded
due to age >80 years (n=7), tumor located >10 cm from the
anal verge (n=23), or ineligibility due to either chemotherapeutic
regimen (n=54) or radiotherapy (not 45–50.4 Gy; n=33). Overall, 156
patients were included in the analysis. Patients were divided into
the following two groups according to whether they received
chemotherapy or not: Consolidation (n=76) or control (n=80) group
(Fig. 1). The following data were
reviewed: Sex, age, body mass index (BMI), pretreatment level of
carcinoembryonic antigen (CEA), histological type, clinical Tumor,
Nodule, Metastasis (TNM) stages graded according to the American
Joint Committee on Cancer (AJCC), 7th edition guidelines (14), pretreatment distance of the tumor from
the anal verge, NCRT regimen, interval between NCRT and surgery,
grades 3 or 4 toxicities, final pathological stage, postoperative
complications, disease recurrence, distant metastases, and
mortality. The tumor histology and TNM stages of patients were
confirmed by at least two relevant experts. Pathological reports
were reviewed to assess tumor-node (TN) downstaging and the pCR and
near pCR rates. Near pCR was defined as a finding of only isolated
residual tumor cells or small groups of residual cancer cells in
the rectal wall, with no tumor cells in the lymph nodes (9,15).
Chemotherapy regimens included capecitabine (825 mg/m2
twice daily, 5 days/week for 5 weeks for concurrent
chemoradiotherapy; 1,250 mg/m2 twice daily on days 1–14,
every 3 weeks for consolidation chemotherapy and postoperative
therapy), CapeOX (oxaliplatin 130 mg/m2 IV, day 1;
capecitabine 1,000 mg/m2 twice daily on days 1–14/3
weeks), or FOLFOX (oxaliplatin 85 mg/m2 IV, day 1;
leucovorin 400 mg/m2 IV on days 1–2, and 5-FU 400
mg/m2 IV bolus on day 1 followed by continuous infusion
of 2,400 mg/m2 over 46–48 h, repeated every 2 weeks).
The actual cycles of consolidation chemotherapy varied due to
numerous reasons, including tumor response, clinician decision, and
patient economic status. The mean radiation dose was 50.4 Gy
(range, 45–50.4 Gy) with a daily fraction of 1.8 Gy using a 6-mV
linear accelerator. Surgery was performed approximately 6–8 weeks
following the completion of preoperative therapy, irrespective of
clinical tumor stage or response to NCRT. All the patients
underwent curative resection with TME. The Ethics Committee of
Nanfang Hospital of Southern Medical University approved the
present study.
Statistical analysis
Continuous variables are expressed as the median and
range and were analyzed using two-sample t-tests. Categorical
variables are expressed as numbers with percentages and were
analyzed using a χ2 or Fisher's exact test when
appropriate. Univariate analysis was used to preliminarily assess
the predictive value of variables for achieving pCR and near pCR.
Multivariate analysis was performed on variables with P<0.1 from
the univariate analysis to further analyze the independent
predictive factors of pCR and near pCR. All analyses were performed
using SPSS 21.0 software (IBM Corp., Armonk NY, USA) for Windows.
OS was calculated from the date of surgery to the date of mortality
from any cause or the last follow-up visit. Recurrence was
determined either via imaging studies or pathological findings.
DMFS was defined as the time from surgery to metastasis or
mortality, while DFS was defined as the time from surgery to local
recurrence, metastasis or mortality. The Kaplan-Meier method was
used to analyze the rate of patient survival, and comparisons were
performed using the Wilcoxon test. All statistical tests were
two-sided. P<0.05 was considered to indicate a statistically
significant difference.
Results
Clinicopathological
characteristics
Between January 2010 and July 2016, 156 patients
with local advanced (cT3-4 and/or cN0-2), low (0–5 cm from the anal
verge), and mid- (6–10 cm from the anal verge) rectal cancer were
enrolled in the present study. The baseline characteristics of the
patients were well balanced between the two groups (Table I). Abdominopelvic enhanced magnetic
resonance imaging (MRI) was performed on all patients prior to
treatment, and 148 (94.8%) patients underwent endoscopic
ultrasonography. The median age at diagnosis was 53 years (range,
22–80 years). The majority of the patients were male (69.2%), while
females comprised 30.8% of the study population. The majority of
tumors were staged as cT4 (76.3%) and III (83.3%). A total of 90
(57.7%) and 60 (42.3%) patients had a tumor located either between
0 and 5 cm, or 6 and 10 cm, respectively, from the anal verge. No
differences in stage were observed between the two groups
(P=0.567). The median interval between NCRT and TME was 8.7 weeks
(range, 5–12 weeks) in the consolidation group and 7.4 weeks
(range, 2.4–12.2 weeks) in the control group (P=0.17). A total of
89 (57.1%) patients had an interval of ≥8 weeks, while 67 (42.9%)
had an interval of <8 weeks. The majority of patients (64,
84.2%) received consolidation chemotherapy throughout the entire
resting period. The median interval between NCRT and TME was 8.7
weeks in the consolidation group. The majority of patients received
two cycles of capecitabine (40/42) or CapeOX (9/14), while 7/20
patients received three cycles of FOLFOX during the resting period.
Due to a prolonged resting period caused by swelling of the rectum
and surrounding tissues, 2/42 and 1/14 patients were administered
three cycles of capecitabine and CapeOX, respectively, and 5/20
patients administered four cycles of FOLFOX. All patients underwent
pelvic enhancement MRI following neoadjuvant chemoradiation. MRI
scans were reviewed by a radiologist with >5 years of experience
in the MRI assessment of rectal cancer, using MERCURY Experience
defined criteria (16). Levels of
mrTRG-4 and mrTRG-5 correspond to a response to concurrent
chemotherapy, hence the clinician decided to administer only one
cycle of consolidation chemotherapy to these patients (2/14 in
CapeOX and 2/20 in FOLFOX). Due to economic constraints, 2/14
patients were given one cycle of CapeOX and 6/20 patients given two
cycles of FOLFOX. All patients underwent optimal surgery with TME,
among which 36 (47.4%) patients in the consolidation group and 33
(41.2%) patients in the control group received >3 months of
adjuvant chemotherapy following surgery. The median follow-up time
was 31 months (range, 4–84 months).
 | Table I.Summary of patient
characteristics. |
Table I.
Summary of patient
characteristics.
| Parameter | Total (n=156) | Consolidation group
(n=76) | Control group
(n=80) | P-value |
|---|
| Age, median
(range) |
| 50 (22–70) | 55 (24–80) | 0.129 |
| Sex |
|
|
| − |
| Male | 108 (69.2%) | 57 (75%) | 51 (63.8%) | 0.128 |
|
Female | 48 (30.8%) | 19 (25%) | 29 (36.3%) | − |
| Clinical
T-stage |
|
|
| 0.130 |
|
cT3 | 37 (23.7%) | 14 (18.4%) | 23 (28.8%) | − |
|
cT4 | 119 (76.3) | 62 (81.6%) | 57 (71.2%) | − |
| Clinical
N-stage |
|
|
| 0.539 |
|
cN0 | 26 (16.7%) | 14 (18.4%) | 12 (15.0%) | − |
|
cN1 | 49 (31.4%) | 26 (34.2%) | 23 (28.7%) | − |
|
cN2 | 81 (51.9%) | 36 (47.4%) | 45 (56.3%) | − |
| AJCC/UICC
stage |
|
|
| 0.567 |
| II | 26 (16.7%) | 14 (18.4%) | 12 (15%) | − |
|
III | 130 (83.3%) | 62 (81.6%) | 68 (85%) | − |
|
Differentiation |
|
|
| 0.186 |
| Well
differentiated | 24 (15.4%) | 10 (13.2%) | 14 (17.5%) | − |
|
Moderately differentiated | 89 (57.1%) | 49 (64.5%) | 40 (50%) | − |
| Poorly
differentiated or mucinous adenocarcinoma | 43 (27.5%) | 17 (22.3%) | 26 (32.5%) | − |
| Distance from
anorectal verge |
|
|
| 0.307 |
| 0–5
cm | 90 (57.7%) | 47 (61.8%) | 43 (53.8%) | − |
| 6–10
cm | 66 (42.3%) | 29 (31.2%) | 37 (46.2%) | − |
| Pretreatment with
CEA |
|
|
| 0.312 |
| <5
ng/ml | 88 (56.4%) | 46 (60.5%) | 42 (52.3%) | − |
| ≥5
ng/ml | 68 (43.6%) | 30 (39.5%) | 38 (47.5%) | − |
| Neural
invasion |
|
|
| 0.221 |
| No | 146 (93.5%) | 73 (96.1%) | 73 (91.3%) | − |
|
Yes | 10 (6.5%) | 3 (3.9%) | 7 (8.7%) | − |
| Lymph vascular
invasion |
|
|
| 0.959 |
| No | 152 (97.4%) | 74 (97.4%) | 78 (97.5%) | − |
|
Yes | 4 (2.6%) | 2 (2.6%) | 2 (2.5%) | − |
| Interval NCRT and
TME |
|
|
| 0.908 |
| ≥8
weeks | 89 (57.1) | 43 (56.6%) | 46 (57.5%) | − |
| <8
weeks | 67 (42.9%) | 33 (43.4%) | 34 (42.5%) | − |
| BMI |
|
|
| 0.188 |
| ≥25
kg/m2 | 36 (23.1%) | 21 (27.6%) | 15 (18.8%) | − |
| <25
kg/m2 | 120 (76.9%) | 55 (72.4%) | 65 (81.3%) | − |
| Median follow-up
time (months) |
| 30 | 32 | 0.058 |
pCR and near PCR
A total of 38/156 (24.3%) patients had a pCR or near
pCR. Among them, a total of 16 (21.1%) patients in the
consolidation group and nine (11.25%) patients in the control group
achieved pCR, while nine (11.84%) patients in the consolidation
group and four (5%) patients in the control group achieved near
pCR. The rate of pCR and near pCR was significantly higher in
patients who underwent consolidation chemotherapy (25/76, 32.8%)
compared with that in patients who underwent NCRT only (13/80,
16.25%), (P=0.015). In the univariate analysis, age, sex,
differentiation, distance from the anorectal verge, lymphovascular
invasion and BMI were not associated with pCR and near pCR rates
(P=0.732, 0.780, 0.424, 0.139, 0.250 and 0.919, respectively).
Clinical T stage (T3 vs. T4, P=0.002), N stage (N0 vs. N1 vs. N2,
P=0.012), AJCC/Union for International Cancer Control (UICC) stage
(II vs. III, P=0.005), CEA level (<5 ng/ml vs. ≥5 ng/ml,
P=0.014), neural invasion (yes vs. no, P=0.064), interval between
NCRT and TME (≥8 weeks vs. <8 weeks, P=0.000), and given
consolidation chemotherapy (yes vs. no, P=0.015) were significantly
associated with pCR and near pCR rates. Multivariate analysis was
performed for the characteristics that had P<0.1 in the
univariate analysis (Table II).
Aside from neural invasion [OR: 0.447; 95% confidence interval
(CI): 0.070–2.838; P=0.393], N stage (OR: 0.729; 95% CI:
0.280–1.902; P=0.518), and AJCC/UICC stage (OR: 0.260; 95% CI:
0.041–1.661; P=0.155), clinical T stage (OR: 0.273; 95% CI:
0.110–0.677; P=0.005), CEA level (OR: 0.378, 95% CI: 0.151–0.944;
P=0.037), interval between CRT and TME (OR: 0.263; 95% CI:
0.088–0.785; P=0.017), and given consolidation chemotherapy (OR:
0.378; 95% CI: 0.151–0.944; P=0.037) were factors significantly
associated with pCR and near pCR.
| Table II.Multivariate analysis in relation to
pCR + near pCR rate. |
Table II.
Multivariate analysis in relation to
pCR + near pCR rate.
| Parameter | No. of
patients | pCR + near
pCRa (N) | pCR + near pCR
(%) | OR | 95%CI | P-value |
|---|
| Clinical
T-stage |
|
|
| 0.273 | 0.110–0.677 | 0.005 |
|
cT3 | 37 | 16 | 43.2 |
|
|
|
|
cT4 | 119 | 22 | 18.5 |
|
|
|
| Clinical
N-stage |
|
|
| 0.729 | 0.280–1.902 | 0.518 |
|
cN0 | 26 | 12 | 46.1 |
|
|
|
|
cN1 | 49 | 12 | 24.5 |
|
|
|
|
cN2 | 81 | 14 | 17.3 |
|
|
|
| AJCC/UICC stage
(%) |
|
|
| 0.260 | 0.041–1.661 | 0.155 |
| II | 26 | 12 | 46.1 |
|
|
|
|
III | 130 | 26 | 20.0 |
|
|
|
| Pretreatment with
CEA |
|
|
| 0.378 | 0.151–0.944 | 0.037 |
| <5
ng/ml | 88 | 28 | 31.8 |
|
|
|
| ≥5
ng/ml | 68 | 10 | 14.7 |
|
|
|
| Neural
invasion |
|
|
| 0.447 | 0.07–2.838 | 0.393 |
| No | 146 | 38 | 26.0 |
|
|
|
|
Yes | 10 | 0 | 0.00 |
|
|
|
| Interval NCRT and
TME |
|
|
| 0.263 | 0.088–0.785 | 0.017 |
| ≥8
weeks | 89 | 31 | 34.8 |
|
|
|
| <8
weeks | 67 | 7 | 10.4 |
|
|
|
| Given consolidation
chemotherapy or not |
|
|
| 0.378 | 0.151–0.944 | 0.037 |
|
Consolidation group | 76 | 25 | 32.8 |
|
|
|
| Control
group | 80 | 13 | 16.25 |
|
|
|
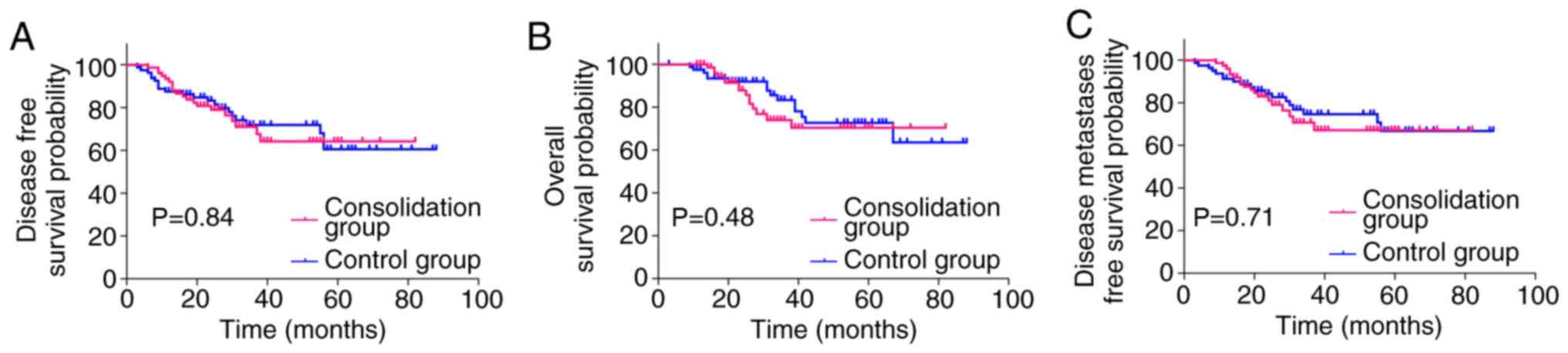
Survival
The Kaplan-Meier curves (Fig. 2) demonstrated that the 3-year DMFS
(70.72% vs. 74.64%; HR: 1.129; 95% CI: 0.5928–2.162; P=0.70), DFS
(70.95% vs. 71.89%; HR: 1.063; 95% CI: 0.5801–1.952; P=0.84), and
OS (73.99% vs. 83.40%; HR: 1.286; 95% CI: 0.6300–2.666; P=0.48) did
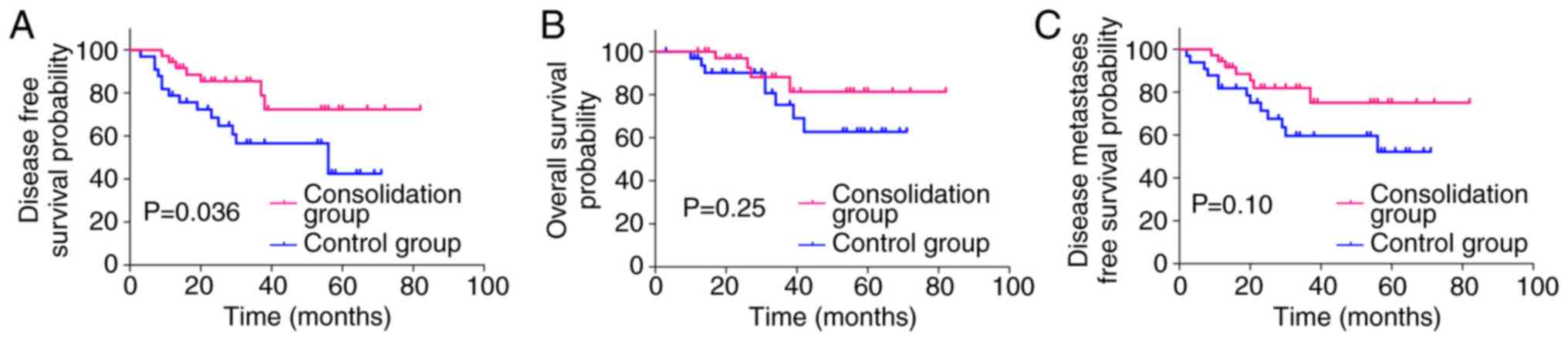
not differ significantly between the two groups. The decision for
adjuvant treatment was made on an individual basis according to
pathological staging. A total of 69 (44.23%) patients received
adjuvant chemotherapy for >3 months, implementing the same
regimen used for neoadjuvant chemotherapy (36 in the consolidation
group and 33 in the control group). The survival rate of the 69
patients was further analyzed, and distant metastasis was observed
in 20 (29.0%) patients [seven (19.4%) in the consolidation group
and 13 (39.4%) in the control group]. The estimated 3-year DMFS was
81.91% in the consolidation group compared with 59.66% in the
control group (HR: 0.4780; 95% CI: 0.2006–1.162; P=0.10). The
3-year OS was 88.15% in the consolidation group compared with
75.32% in the control group (HR: 0.5045; 95% CI: 0.1658–1.594;
P=0.25). Although the estimated 3-year DMFS and OS were not
significantly different between the two groups, the consolidation
group exhibited a higher rate of DMFS and OS. Local recurrence was
observed in 7 (10.1%) patients overall [three (8.3%) in the
consolidation group and four (12.1%) in the control group]. The
estimated 3-year DFS was 85.48% in the consolidation group, and
56.64% in the control group (HR: 0.3992; 95% CI: 0.1752–0.9366;
P=0.036, Fig. 3).
Surgical outcome and
complications
All patients underwent optimal surgery with TME,
among which 56 (73.6%) patients in the consolidation group and 53
(66.2%) patients in the control group received a sphincter-saving
procedure (P=0.312). A total of 73 (96.1%) patients in the
consolidation group and 72 (90.0%) patients in the control group
obtained R0 resection of the primary tumor, with negative distal
and radial margins. Comparing postoperative pathological findings
with clinical status based on imaging prior to NCRT, a higher rate
of downstaging for tumor (65.8% vs. 48.6%, P=0.032) and node (55.3%
vs. 35%, P=0.011) category was observed in the consolidation group
compared with the control group (Table
III). No perioperative mortality occurred in this cohort. A
total of 25/156 (16.02%) patients developed postoperative
complications, including intestinal obstruction (6.5% vs. 7.5%,
P=0.822), anastomosis fistula (1.31% vs. 1.25%, P=0.971), infection
(6.57% vs. 2.5%, P=0.219), urinary complications (0% vs. 1.25%,
P=1.000), and pelvic fibrosis (2.63% vs. 2.5%, P=1.000). The
incidence rate of complications did not differ significantly
between the two groups (Table
IV).
| Table III.Summary of surgical outcome in the
consolidation group compared with the control group. |
Table III.
Summary of surgical outcome in the
consolidation group compared with the control group.
| Parameter | Consolidation
group, no. (%) | Control group, no.
(%) | P-value |
|---|
| No. of
patients | 76 | 80 | − |
| pCR + near
pCRa | 25 (32.80) | 13 (16.25) | 0.015 |
| Anal
preservation | 56 (73.60) | 53 (66.20) | 0.312 |
| Resection with
negative margins | 73 (96.10) | 72 (90.00) | 0.140 |
| T downstaging
(ypT<cT) | 50 (65.8) | 39 (48.6) | 0.032 |
| N downstaging
(ypN<cN) | 42 (55.30) | 28 (35.00) | 0.011 |
| Table IV.Summary of complications in the
consolidation group compared with the control group. |
Table IV.
Summary of complications in the
consolidation group compared with the control group.
| Parameter | Consolidation
group, no. (%) | Control group, no.
(%) | P-value |
|---|
| No. of
patients | 76 | 80 | − |
| Intestinal
obstruction | 5 (6.50) | 6 (7.50) | 0.822 |
| Anastomotic
fistula | 1 (1.31) | 1 (1.25) | 0.971 |
| Infection | 5 (6.57) | 2 (2.50) | 0.219 |
| Urinary
complications | 0 (0.00) | 1 (1.25) | 1.000 |
| Pelvic
fibrosis | 2 (2.63) | 2 (2.50) | 1.000 |
Toxicity
The grade 3 or 4 toxicities that developed during
neoadjuvant treatment are described in Table V. The rates of hematological toxicity
and non-hematological toxicity were not influenced by the
administration of consolidation chemotherapy. A total of nine
(11.8%) and six (7.5%) patients in the consolidation and control
groups had grade 3 or 4 leukopenia, respectively (P=0.358). Grade
3–4 anemia was observed in four patients (5.3%) in the
consolidation group and in one patient (1.3%) in the control group
(P=0.155). Thrombocytopenia was observed in eight patients (10.5%)
and six patients (7.5%) in the consolidation and control group,
respectively (P=0.509). Overall, grade 3–4 nausea or vomiting,
radiation proctitis, diarrhea, dermatitis, hand-foot syndrome, and
peripheral neuropathy occurred in two (2.6%), five (6.6%), 15
(19.7%), one (1.3%), five (6.6%), and two (2.6%) patients in the
consolidation group and in one (1.3%, P=0.530), four (5.0%,
P=0.67), nine (11.3%, P=0.142), one (1.3%, P=0.971), two (2.5%,
P=0.219), and zero (0%, P=0.236) patients in the control group,
respectively. Neither a life-threatening decrease in blood count
nor febrile neutropenia was observed. No other grade 3 or 4
toxicities were recorded.
| Table V.Preoperative chemoradiotherapy grade
3 or 4 toxicities in the consolidation group compared with the
control group. |
Table V.
Preoperative chemoradiotherapy grade
3 or 4 toxicities in the consolidation group compared with the
control group.
| Parameter | Consolidation
group, no. (%) | Control group, no.
(%) | P-value |
|---|
| No. of
patients | 76 | 80 | − |
| Hematologic
toxicity |
|
|
|
|
Leukopenia | 9 (11.8) | 6 (7.5) | 0.358 |
|
Anemia | 4 (5.3) | 1 (1.3) | 0.155 |
|
Thrombocytopenia | 8 (10.5) | 6 (7.5) | 0.509 |
| Nonhematologic
toxicity |
|
|
|
| Nausea
or vomiting | 2 (2.6) | 1 (1.3) | 0.530 |
|
Radiation proctitis | 5 (6.6) | 4 (5.0) | 0.67 |
|
Diarrhea | 15 (19.7) | 9 (11.3) | 0.142 |
|
Dermatitis | 1 (1.3) | 1 (1.3) | 0.971 |
|
Hand-foot syndrome | 5 (6.6) | 2 (2.5) | 0.219 |
|
Peripheral neuropathy | 2 (2.6) | 0 (0.0) | 0.236 |
Discussion
Preoperative 45–50.4 Gy pelvic irradiation combined
with fluorouracil or capecitabine monotherapy is the current
conventional treatment regimen for LARC. However, a number of
studies have reported that this treatment modality yields low pCR
rate (12–20%), and this treatment regimen has not significantly
improved patients' survival (5,6). Systemic
metastasis is closely associated with long-term survival. However,
the majority of patients with rectal cancer may have early
micrometastases on initial diagnosis (17,18).
Previous studies have revealed that, although preoperative
radiotherapy and TME surgery can improve the local control rate,
they are inadequate for the treatment of systemic micrometastases
(17,18). Previous studies have also demonstrated
that the later postoperative systemic chemotherapy was given, the
higher the risk of postoperative metastases (19,20). It
has also been demonstrated that the addition of chemotherapy either
before or following chemoradiotherapy may increase the pCR rate,
indicating a synergistic response of additional chemotherapy to
standard chemoradiation (8,21). However, few studies regarding
consolidation chemotherapy have been published, and even fewer
studies concerning the survival of patients who underwent
consolidation chemotherapy have been performed to date.
In the present study, a statistically significant
increase in the rate of pCR and near pCR in patients administered
consolidation chemotherapy compared with those administered
conventional neoadjuvant treatment (32.8% vs. 16.25%,
respectively), was observed, which largely coincides with the
results of previous studies (22,23).
Habr-Gama et al (24) first
reported the strategy of consolidation chemotherapy in the resting
period between the completion of NCRT and surgery. In their cohort,
14 (48%) patients achieved complete clinical response, and five
(17%) patients achieved pCR of the primary lesion following
surgery. In 2015, Garcia-Aguilar et al (8) published a nonrandomized trial in which
the addition of two to six cycles of infusional fluorouracil,
leucovorin, and oxaliplatin was associated with an increased pCR
rate (18–38%), without increasing complications, compared with the
strategy of traditional NCRT in patients with LARC. However, there
was a major limitation to this study; as the number of cycles of
consolidation chemotherapy increased, the interval between
neoadjuvant therapy and surgery also increased, which may lead to a
high pCR rate. Nonetheless, it has been demonstrated that the
increased pCR rate may depend on the timing of response assessment
(15). In the present study, the
median time interval between the two groups was 8.7 weeks in the
consolidation group and 7.4 weeks in the control group (P=0.218).
The majority of patients (72%) received two cycles of consolidation
chemotherapy, which may reduce the impact of the number of cycles
and the treatment interval on pCR and near pCR. Consolidation
chemotherapy may improve the pCR rate, and this may be due to
numerous reasons. Firstly, extending chemotherapy to the resting
period may also allow further exposure of irradiated tumor cells to
chemotherapy and eradicate the minimal residual tumor cells
(24). Additionally, administering
preoperative chemotherapy is conducive to further reducing the
tumor burden, as the tumor has a rich blood supply in the
preoperative phase, which is beneficial to the distribution of
chemotherapy drugs. Lastly, the general condition of the patient is
likely to be improved, and thus chemotherapy is better tolerated at
this stage.
Data on the impact of consolidation chemotherapy on
long-term disease recurrence and survival are limited. The present
study has demonstrated an improved DFS (85.48% vs. 56.64%, P=0.036)
in patients administered consolidation chemotherapy following
stratified analysis by selecting patients with >3 months of
adjuvant chemotherapy. OS and DMFS were not significantly different
between the two groups, although the consolidation group displayed
a higher rate of DMFS and OS (81.91% vs. 59.66%, P=0.10; 88.15% vs.
75.32%, P=0.25) compared with conventional NCRT. The results from
the present study verified that consolidation chemotherapy may be
associated with improved local control rate and favorable DFS. It
may represent a subgroup of LARC with an improved biological
behavior. Larsen et al (25)
evaluated the prognostic value of CapeOX regimen before, during and
after NCRT in LARC and reported a 5-year OS and PFS of 72 and 62%,
respectively. Garcia-Aguilar et al (8) recently published a nonrandomized trial
in which the addition of 2–6 cycles of FOLFOX was associated with
an increased pCR rate (from 18–38%), however the study did not
provide evidence of a benefit to long-term survival.
One concern with the use of consolidation
chemotherapy is that it may significantly increase toxicity, reduce
tolerance and compromise the treatment effect. In the present
study, consolidation chemotherapy was well tolerated. Grade 3–4
toxicities were also comparable with those using conventional NCRT
(8). This result may be attributed to
the following factors: Firstly, modern, highly conformal radiation
therapy planning and delivery techniques may potentially reduce the
radiation dose to the bowel and pelvis, consequently reducing
gastrointestinal side effects and hematological toxicity (26); Secondly, consolidation chemotherapy
may be better tolerated following NCRT, as patients have not been
affected by surgical trauma or complications (27).
In the present study, the R0 resection rate of
patients in the consolidation chemotherapy group was 96.1%. This
corresponds to study of Gao et al (23). Engineer et al (28) previously demonstrated that the
addition of chemotherapy following neoadjuvant radiochemotherapy
for patients with poor or no response to NCRT may achieve a
considerable R0 resection rate (62%). A modest increase in the rate
of R0 resection in patients treated with consolidation chemotherapy
compared with those treated with traditional neoadjuvant
chemoradiotherapy (96.1% vs. 90%, respectively), was observed in
the present study; however, it did not reach statistical
significance (P=0.14). This may be a result of different attending
surgeons and the small sample size of the study. The present study
demonstrated an increase in the rate of anal preservation in
patients administered consolidation chemotherapy, although the
increase also did not reach statistical significance (73.6% vs.
66.2%; P=0.321).
The present study poses a number of limitations.
Firstly, as it is a retrospective study, it may have certain
disadvantages, including potential selection bias, recall bias and
censored data. However, considering the lack of prospectively
collected data available, the results may be interpreted as
clinically significant. Secondly, owing to the paucity of
conclusive data on the use of chemotherapy regimens in patients
with stage II/III rectal cancer, FOLFOX, CapeOx, 5-FU/leucovorin or
capecitabine are all recommended by the NCCN panel, therefore the
protocols of consolidation chemotherapy included in the present
study are somewhat heterogeneous. Thirdly, although the results
appeared promising, the cohort was too small and the follow-up
period too short to confirm whether this strategy yields an
improved survival benefit compared with conventional NCRT. Due to
the limited sample size and the short follow-up period, it was not
possible to adequately analyze all of the results. Therefore,
further investigations are required.
In conclusion, this preliminary study revealed that
consolidation chemotherapy administered between NCRT and surgery
may be associated with improved rates of pCR and near pCR, TN
downstaging and DFS. Furthermore, the addition of chemotherapy did
not lead to higher toxicity, complications, or worse quality of
mesorectal excision. Consolidation chemotherapy is safe and
associated with improved oncological outcomes, and may reduce the
number of required cycles of postoperative chemotherapy or
eliminate the need for such a treatment modality.
Acknowledgements
Not applicable.
Funding
This study was supported by National Natural Science
Foundation of China (grant nos. 81672756 and 81472711).
Availability of data and material
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HQL and DHW conceived and designed the experiments.
HQL and PYL collected the data. JL performed the pathological
evaluation. HQL and QZ conducted the clinical follow-up. ZJL and
ZYD performed the statistical analyses. HQL and ZYD drafted and
revised the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The Ethics Committee of Nanfang Hospital of Southern
Medical University (Guangzhou, China) approved the present
study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
NCRT
|
neoadjuvant chemoradiotherapy
|
|
LARC
|
local advanced rectal cancer
|
|
NCCN
|
National Comprehensive Cancer
Network
|
|
pCR
|
pathological complete response
|
|
OS
|
overall survival
|
|
DFS
|
disease-free survival
|
|
DMFS
|
distant metastases-free survival
|
|
TME
|
total mesorectal excision
|
|
BMI
|
body mass index
|
|
AJCC
|
American Joint Committee on Cancer
|
|
CEA
|
carcinoembryonic antigen
|
|
TN
|
tumor-node
|
|
UICC
|
Union for International Cancer
Control
|
References
|
1
|
Bray F, Sankila R, Ferlay J and Parkin DM:
Estimates of cancer incidence and mortality in Europe in 1995. Eur
J Cancer. 38:99–166. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Heald RJ, Husband EM and Ryall RD: The
mesorectum in rectal cancer surgery-the clue to pelvic recurrence?
Br J Surg. 69:613–616. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Havenga K, Enker WE, Norstein J, Moriya Y,
Heald RJ, van Houwelingen HC and van de Velde CJ: Improved survival
and local control after total mesorectal excision or D3
lymphadenectomy in the treatment of primary rectal cancer: An
international analysis of 1,411 patients. Eur J Surg Oncol.
25:368–374. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Benson AB, Venook AP, Cederquist L, Chan
E, Chen YJ, Cooper HS, Deming D, Engstrom PF, Enzinger PC, Fichera
A and Grem JL: Colon cancer, version 1.2017, NCCN clinical practice
guidelines in oncology. J Natl Comp Cancer Network. 15:370–398.
2017. View Article : Google Scholar
|
|
5
|
Chua YJ: Pathological complete response:
Still a relevant endpoint in rectal cancer? The Lancet Oncology.
11:807–808. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Maas M, Nelemans PJ, Valentini V, Das P,
Rödel C, Kuo LJ, Calvo FA, García-Aguilar J, Glynne-Jones R,
Haustermans K, et al: Long-term outcome in patients with a
pathological complete response after chemoradiation for rectal
cancer: A pooled analysis of individual patient data. Lancet Oncol.
11:835–844. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Francois Y, Nemoz CJ, Baulieux J, Vignal
J, Grandjean JP, Partensky C, Souquet JC, Adeleine P and Gerard JP:
Influence of the interval between preoperative radiation therapy
and surgery on downstaging and on the rate of sphincter-sparing
surgery for rectal cancer: The Lyon R90-01 Randomized Trial. J Clin
Oncol. 17:23961999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Garcia-Aguilar J, Chow OS, Smith DD,
Marcet JE, Cataldo PA, Varma MG, Kumar AS, Oommen S, Coutsoftides
T, Hunt SR, et al: Effect of adding mFOLFOX6 after neoadjuvant
chemoradiation in locally advanced rectal cancer: A multicentre,
phase 2 trial. Lancet Oncol. 16:957–966. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tulchinsky H, Shmueli E, Figer A, Klausner
JM and Rabau M: An interval >7 weeks between neoadjuvant therapy
and surgery improves pathologic complete response and disease-free
survival in patients with locally advanced rectal cancer. Ann Surg
Oncol. 15:2661–2667. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Swellengrebel HA, Bosch SL, Cats A,
Vincent AD, Dewit LG, Verwaal VJ, Nagtegaal ID and Marijnen CA:
Tumour regression grading after chemoradiotherapy for locally
advanced rectal cancer: A near pathologic complete response does
not translate into good clinical outcome. Radiother Oncol.
112:44–51. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wolthuis AM, Penninckx F, Haustermans K,
De Hertogh G, Fieuws S, Van Cutsem E and D'Hoore A: Impact of
interval between neoadjuvant chemoradiotherapy and TME for locally
advanced rectal cancer on pathologic response and oncologic
outcome. Ann Surg Oncol. 19:2833–2841. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Habr-Gama A, Perez RO, Proscurshim I,
Nunes Dos Santos RM, Kiss D, Gama-Rodrigues J and Cecconello I:
Interval between surgery and neoadjuvant chemoradiation therapy for
distal rectal cancer: Does delayed surgery have an impact on
outcome? Int J Radiat Oncol Biol Phys. 71:1181–1188. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Supiot S, Bennouna J, Rio E, Meurette G,
Bardet E, Buecher B, Dravet F, Le Neel JC, Douillard JY, Mahé MA
and Lehur PA: Negative influence of delayed surgery on survival
after preoperative radiotherapy in rectal cancer. Colorectal Dis.
8:430–435. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Edge SB and Compton CC: The american joint
committee on cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Moore HG, Gittleman AE, Minsky BD, Wong D,
Paty PB, Weiser M, Temple L, Saltz L, Shia J, Shia J and Guillem
JG: Rate of pathologic complete response with increased interval
between preoperative combined modality therapy and rectal cancer
resection. Dis Colon Rectum. 47:279–286. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Patel UB, Taylor F, Blomqvist L, George C,
Evans H, Tekkis P, Quirke P, Sebag-Montefiore D, Moran B, Heald R,
et al: Magnetic resonance imaging-detected tumor response for
locally advanced rectal cancer predicts survival outcomes: MERCURY
experience. J Clin Oncol. 29:3753–3760. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sauer R, Becker H, Hohenberger W, Rodel C,
Wittekind C, Fietkau R, Martus P, Tschmelitsch J, Hager E, Hess CF,
et al: Preoperative versus postoperative chemoradiotherapy for
rectal cancer. N Engl J Med. 351:1731–1740. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cienfuegos JA, Baixauli J, Pastor C,
Arredondo J, Sola JJ, Arbea L, Chopitea A and Hernandez-Lizoain JL:
Long-term oncologic results in cancer of the rectum treated by
preoperative chemoradiotherapy and surgery: An analysis of 500
cases. Rev Esp Enferm Dig. 107:340–346. 2015.PubMed/NCBI
|
|
19
|
Lima IS, Yasui Y, Scarfe A and Winget M:
Association between receipt and timing of adjuvant chemotherapy and
survival for patients with stage III colon cancer in Alberta,
Canada. Cancer. 117:3833–3840. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tevis SE, Kohlnhofer BM, Stringfield S,
Foley EF, Harms BA, Heise CP and Kennedy GD: Postoperative
complications in patients with rectal cancer are associated with
delays in chemotherapy that lead to worse disease-free and overall
survival. Dis Colon Rectum. 56:1339–1348. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chau I, Brown G, Cunningham D, Tait D,
Wotherspoon A, Norman AR, Tebbutt N, Hill M, Ross PJ, Massey A and
Oates J: Neoadjuvant capecitabine and oxaliplatin followed by
synchronous chemoradiation and total mesorectal excision in
magnetic resonance imaging-defined poor-risk rectal cancer. J Clin
Oncol. 24:668–674. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gao YH, Zhang X, An X, Cai MY, Zeng ZF,
Chen G, Kong LH, Lin JZ, Wan DS, Pan ZZ and Ding PR: Oxaliplatin
and capecitabine concomitant with neoadjuvant radiotherapy and
extended to the resting period in high risk locally advanced rectal
cancer. Strahlenther Onkol. 190:158–164. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gao YH, Lin JZ, An X, Luo JL, Cai MY, Cai
PQ, Kong LH, Liu GC, Tang JH, Chen G, et al: Neoadjuvant sandwich
treatment with oxaliplatin and capecitabine administered prior to,
concurrently with, and following radiation therapy in locally
advanced rectal cancer: A prospective phase 2 trial. Int J Radiat
Oncol Biol Phys. 90:1153–1160. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Habr-Gama A, Perez RO, Sabbaga J, Nadalin
W, São Julião GP and Gama-Rodrigues J: Increasing the rates of
complete response to neoadjuvant chemoradiotherapy for distal
rectal cancer: Results of a prospective study using additional
chemotherapy during the resting period. Dis Colon Rectum.
52:1927–1934. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Larsen FO, Markussen A, Jensen BV, Fromm
AL, Vistisen KK, Parner VK, Linnemann D, Hansen RH, Johannesen HH
and Schou JV: Capecitabine and oxaliplatin before, during, and
after radiotherapy for High-Risk rectal cancer. Clin Colorectal
Cancer. 16:e7–e14. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wan J, Liu K, Li K, Li G and Zhang Z: Can
dosimetric parameters predict acute hematologic toxicity in rectal
cancer patients treated with intensity-modulated pelvic
radiotherapy? Radiat Oncol. 10:1622015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Helbling D, Bodoky G, Gautschi O, Sun H,
Bosman F, Gloor B, Burkhard R, Winterhalder R, Madlung A, Rauch D,
et al: Neoadjuvant chemoradiotherapy with or without panitumumab in
patients with wild-type KRAS, locally advanced rectal cancer
(LARC): A randomized, multicenter, phase II trial SAKK 41/07. Ann
Oncol. 24:718–725. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Engineer R, Ostwal V, Arya S, Gupta P,
Chopra S, Patil P, Jatal S and Saklani A: Additional chemotherapy
and salvage surgery for poor response to chemoradiotherapy in
rectal cancers. Asia Pac J Clin Oncol. 13:322–328. 2017. View Article : Google Scholar : PubMed/NCBI
|