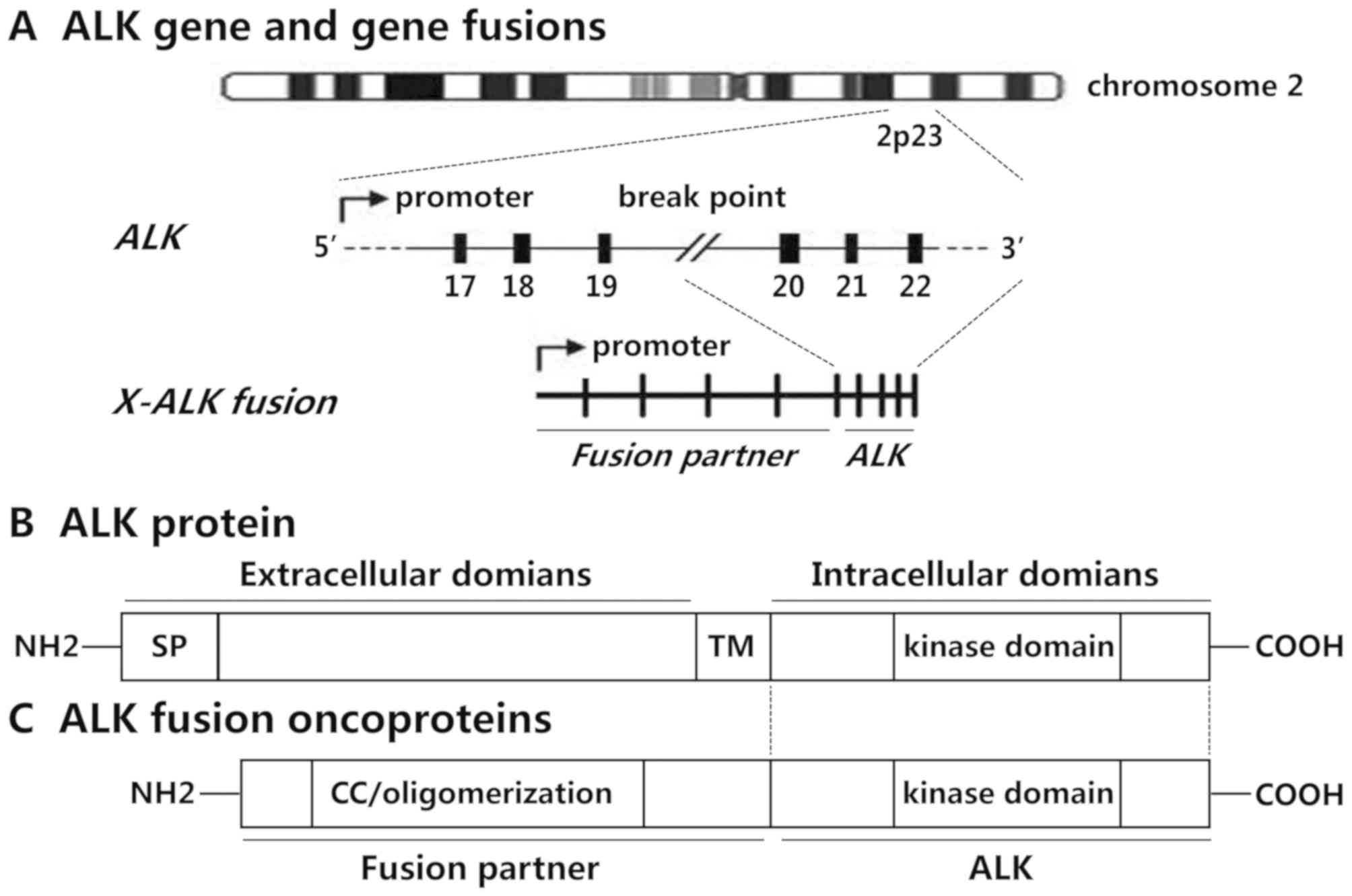
Located on chromosome 2p23, receptor tyrosine kinase
(RTK) anaplastic lymphoma kinase (ALK) is physiologically expressed
in fetal neural cells. Phosphorylated and activated ALK controls
the basic mechanisms of cell proliferation, survival and
differentiation during development of the nervous system (1). In 1994 ALK t(2;5) chromosomal
translocation was reported in anaplastic large cell lymphoma (ALCL)
(2). This translocation induced
formation of the nucleophosmin (NPM)-ALK chimeric protein (3). Over the ensuing two decades, ALK
fusion oncogenes have been associated with the development of
diverse tumor types of different lineages, including, but not
limited to, lymphoma, lung cancer, inflammatory myofibroblastic
tumors (IMTs), Spitz tumors, renal carcinoma, thyroid cancer,
digestive tract cancer, breast cancer, leukemia and ovarian
carcinoma. During this period, the discovery of EML4-ALK in
non-small cell lung cancer (NSCLC) was a major development that led
to significant diagnostic and therapeutic advances (4).
Lymphomas comprise a group of blood cancer types
that develop from lymphocytes and are classified as either
Hodgkin's lymphoma (HL, 10%) or non-Hodgkin's (NHL, 90%) lymphoma.
Based on the normal function of lymphocytes, NHL may be further
divided into three subtypes: i) B cell NHL; ii) T cell NHL; and
iii) natural killer cell NHL. Compared with HL, NHL patients have a
poor prognosis, and the five-year survival rate is ~69% (13,14).
Lung cancer is the most prevalent type of cancer and
the leading cause of mortality among all malignancies. Despite
tremendous progress in the diagnosis and treatment of lung cancer,
prognosis for these patients remains poor, with only 15% surviving
more than 5 years after initial diagnosis (28). NSCLC accounts for ~80-85% of these
cases of lung cancer, whereas the remainder involve small cell lung
cancer and lung carcinoid tumors (29).
IMT is a type of mesenchymal neoplasm composed of a
mixture of several inflammatory cells, which primarily occurs in
children (47,48). IMTs are generally benign or low-grade
malignant tumors, and patients usually only require surgical
treatment (49,50). According to certain statistics, ~50%
of IMTs are ALK-fusion-positive, and two of the most common fusion
partners are TPM3 and TPM4 (51). Similar to ALCL, various ALK
fusion partners have been identified in IMTs, including PPF1BP1,
PCTN1, RANBP2, EML4, CLTC, CARS, ATIC, SEC31A and FN1
(Table I). Additionally, a study
suggested that patients with ALK-fusion-positive IMT may exhibit a
more favorable prognosis compared with those with
ALK-fusion-negative IMT (52).
Spitz tumors are a type of melanocytic neoplasm that
tend to occur in younger people (2–35 years old). Spitz tumors may
be divided into three subtypes: i) Benign Spitz nevus; ii) atypical
Spitz tumor; and iii) Spitz malignant melanoma (53). In 2014, DCTN1-ALK and
TPM3-ALK were identified in Spitz tumors (53,54).
Follow-up studies have demonstrated that activation of the X-ALK
oncoprotein serves an important role in the pathogenesis of Spitz
tumors (55).
Renal carcinoma, a type of tumor that originates
from cells in the kidney, accounts for <2% of all cancer types.
Renal carcinoma may be divided into two main subtypes: i) renal
cell carcinoma (RCC) with a poor prognosis; and ii) transitional
cell carcinoma (accounting for 5–10% of cases) (56). Due to the difficulty of early
diagnosis in renal carcinomas, their pathogenesis is not completely
known. ALK fusions have been documented in a small
percentage of RCCs (<1%) (57,58). Based
on clinical settings, RCCs with ALK translocation are
divided into two categories: i) RCCs with VCL-ALK, composed
of sickle cells; and ii) other fusions, which are not associated
with sickle cell composition (59,60). In
addition to ALK rearrangements, up to 10% of RCC cases show
a low level of ALK copy number gains (58). The therapeutic relevance of these
findings in RCC is yet to be established.
Thyroid cancer is a common type of endocrine tumor
that is classified as either benign thyroid adenoma or a thyroid
malignancy (61). Based on the cells
that comprise these tumors, thyroid malignancies can be further
divided into four subtypes: i) papillary (PTC; 80–85%); ii)
follicular (10–15%); iii) medullary (3%); and iv) anaplastic
thyroid cancer (ATC; 2%). Among these four types of tumor, the
degree of malignance of ATC is high, and its prognosis is poor,
with a median patient survival of only 5 months (62–64). In
2015, translocations involving ALK were detected by Chou
et al (65), in 2.2% of PTC
patients. Several other ALK fusion genes have been reported
in thyroid cancer, including EML4-ALK, TFG-ALK and
STRN-ALK (Table I).
Digestive tract cancer refers to neoplasms of the
digestive system, including cancer of the mouth, esophagus, stomach
and intestines. Epidemiological studies have indicated that the
frequency of different digestive tract cancer types differs widely
in different countries. A recent study illustrated that several
factors determine the prognosis of patients with digestive tract
cancer, including the location of the tumor, clinical stage and the
type of cancer cell (66). In 2006,
the TPM4-ALK fusion was first reported in esophageal squamous cell
carcinomas (67). Subsequently, other
fusion partners have been described in digestive tract cancer,
including EML4, CAD and SPTBN1 (68–70).
Surveys in which a variety of techniques have been
applied to a large series of tumors have revealed differentially
convincing evidence of ALK rearrangement in rare cases of
breast carcinoma (fusions in 5 out of 209 cases assessed by RT-PCR)
(71), leukemia (fusions in 3 out of
1,708 cases assessed by RT-PCR) (72)
and ovarian carcinoma (3 out of 69 tumors expressed ALK) (73). Although these reports are technically
sound, for the most part, the relevance of these findings remains
to be clarified through functional studies in pertinent models.
ALK is a compelling therapeutic target, as it is a
critical oncogenic driver in diverse tumor types of different
lineages. However, its expression and functions are limited in
normal tissues. Indeed, Bilsland et al (74) confirmed that ALK
double-knockout mice exhibited no significant phenotypic
differences, a normal life span, no structurally detectable defects
and minor behavioral abnormalities, which advocates a wide
non-toxic therapeutic window of ALK-specific inhibition. Various
therapeutic methods for tumor treatment are currently in
development, including direct targeting of activated ALK with
small-molecule inhibitors or immunotherapeutic agents and
modulation of downstream signaling intermediates in cancer types
with ALK rearrangement. In addition, the X-ALK fusion
oncoprotein predominantly activates the RAS/MAPK cell proliferation
pathway, in addition to the PI3K/AKT/mTOR and JAK/STAT cell
survival pathways. Therefore, an understanding of these downstream
effectors has prompted the development of novel therapeutic
strategies, some of which are being tested in preclinical/clinical
trials.
Multiple structurally distinct ALK drugs are being
developed based on a deep understanding of the structure of ALK
(Table II), three of which are
currently in clinical use for the treatment of
ALK-fusion-positive lung cancer, including crizotinib,
ceritinib and alectinib. Crizotinib, an oral ALK TKI, has been
extensively studied in preclinical and clinical settings. Early
phase I studies (PROFILE 1001) have indicted notable activity of
crizotinib, with satisfactory tolerability in patients with
ALK-fusion-positive NSCLC (75,76).
Two-phase III studies further demonstrated the superiority of
crizotinib to standard chemotherapy in patients with advanced NSCLC
with X-ALK. One of these studies (PROFILE 1007) illustrated
that crizotinib treatment significantly prolonged progression-free
survival (PFS), which was the primary end point, compared with
chemotherapy with either pemetrexed or docetaxel (7.7 vs. 3.0
months, respectively) (77). Another
study (PROFILE 1014) compared crizotinib with carboplatin or
cisplatin plus pemetrexed in 343 patients with advanced
X-ALK NSCLC, and clarified the significance of crizotinib as
a first-line treatment for these tumors (78). Furthermore, crizotinib displayed
excellent activity in IMT and ALCL cases harboring X-ALK
fusions (79).
Currently, multiple ALK TKIs, including ceritinib,
alectinib, lorlatinib, entrectinib, brigatinib, CEP-28122, TSR-011,
X-396 and ASP3026, are being investigated as potential therapies
for cancer types characterized by ALK rearrangement
(Table II). Ceritinib, a highly
potent and selective TKI, was approved by the Food and Drug
Administration (FDA) as a second-line treatment for patients with
X-ALK NSCLC, and following unsuccessful treatment with
crizotinib. A total of 114 patients with ALK-fusion-positive
NSCLC were enrolled in a global multi-institutional phase I trial,
among whom 70% were crizotinib-sensitive and 30% were
crizotinib-resistant. All patients received at least 400 mg of
crizotinib per day, and the overall response rate (ORR) was 59%
(90). Alectinib is a TKI used
clinically that exhibits minimal inhibitory activity against
kinases other than ALK and RET (91,92).
Furthermore, in vitro and in vivo studies have
demonstrated that alectinib effectively inhibits ALK with or
without the gatekeeper mutation L1196M (92). A separate clinical study was conducted
to investigate the safety and activity of alectinib in TKI-naive
patients with X-ALK NSCLC, with an ORR of 48% (93). Lorlatinib, which is structurally
similar to crizotinib, has been demonstrated to be active against
identified crizotinib-resistant ALK mutations, such as the most
common mutation seen clinically (G1202R) (94). In 2014, Brigatinib received
breakthrough therapy designation from the FDA and a nationwide
phase III clinical study in which brigatinib was compared with
crizotinib in patients with X-ALK NSCLC was recently
initiated (95). Furthermore, the
antitumor activities of at least 5 other novel ALK inhibitors,
including entrectinib, CEP-28122, TSR-011, X-396 and ASP3026, have
been shown in vitro, and these agents are currently under
clinical investigation (96–98). In addition to targeting ALK directly,
several pharmacological strategies allow its indirect targeting.
Specifically, HSP90 inhibitors, including retaspimycin and
tanespimycin, have displayed certain clinical efficacy in the
treatment of patients with ALK rearrangements (84,99,100).
ALK fusions are remarkably versatile oncoproteins
that may drive a variety of tumors of different lineages,
including, but not limited to, lymphoma, lung cancer, IMTs, Spitz
tumors, renal carcinoma, thyroid cancer, digestive tract cancer,
breast cancer, leukemia and ovarian carcinoma. Furthermore, a
profusion of ALK fusion partners has been consistently
identified in ALK-translocated cancer types, which are
unique neoplasms that can be effectively targeted by several
clinically available TKIs, including crizotinib, ceritinib and
alectinib. By using alternative methods of tumor detection, novel
ALK translocations may be discovered in upcoming years,
which may reveal novel aspects of ALK biology. Substantial efforts
are focused on therapeutic considerations and novel approaches to
target ALK, including rationally designed tyrosine kinase
inhibitors, the study of resistance mechanisms, the design of
dual-blockade therapeutic strategies that target downstream
signaling intermediates, and immunotherapy against activated
receptor tyrosine kinases.
In addition to disease-causing gene mutations,
genome-level alterations, including chromosomal imbalances and
instability, clonal chromosomal aberrations (CCAs, also known as
recurrent karyotypic alterations) and non-clonal chromosome
aberrations (NCCAs), also serve a significant role in
carcinogenesis and the development of malignant tumors. Since
cancer-specific aneuploidy catalyzes karyotypic variation, the
degree of aneuploidy predicts the clinical risk of tumor
progression. Increasing evidence has indicated the complexity of
cancer, which cannot be explained by somatic mutation theory. To
address this complexity, additional ad hoc explanations have been
postulated, and carcinogenesis is thought to represent a problem of
tissue organization on the basis of tissue organization field
theory (101–103). According to recent studies,
chromosomal aberration-mediated genome evolution is responsible for
all major transitions in cancer evolution, including phenotypic
plasticity, metastasis and drug resistance (104,105).
It is believed that the genome serves as the evolutionary platform
that links gene/epigene interaction and multiple levels of omics,
which can be driven by genome-level alteration rather than
individual hallmarks as gene mutation or epigenetic alteration.
Conclusively, ongoing research with the aim of characterizing the
clinicopathological and biological consequences of ALK
rearrangement may allow us to better understand the genome-mediated
evolutionary mechanism of cancer.
Not applicable.
The present review was supported by the National
Natural Science Foundation of China (grant no. 81728012), the
Natural Science Foundation of Zhejiang Province (grant no.
LY18H160065), the Zhejiang Medical and Health Science and
Technology Plan Project (grant no. 2018260845), the Science
Foundation of Zhejiang Sci-Tech University (grant no. 14042107-Y),
the National Undergraduate Training Program for Innovation and
Entrepreneurship and Graduate Research and Innovation Projects of
Zhejiang Sci-Tech University, China.
Not applicable.
ZFC and WBO drafted the manuscript. ZFC, QG, MXF, NN
and YTP were responsible for the collection of the relevant
literature. WBO designed the outline and revised the manuscript.
All authors have read and approved the final manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Yao S, Cheng M, Zhang Q, Wasik M, Kelsh R
and Winkler C: Anaplastic lymphoma kinase is required for
neurogenesis in the developing central nervous system of zebrafish.
PLoS One. 8:e637572013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Morris SW, Kirstein MN, Valentine MB,
Dittmer KG, Shapiro DN, Saltman DL and Look AT: Fusion of a kinase
gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin's
lymphoma. Science. 263:1281–1284. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Morris SW, Kirstein MN, Valentine MB,
Dittmer K, Shapiro DN, Look AT and Saltman DL: Fusion of a kinase
gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin's
lymphoma. Science. 267:316–317. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Soda M, Choi YL, Enomoto M, Takada S,
Yamashita Y, Ishikawa S, Fujiwara S, Watanabe H, Kurashina K,
Hatanaka H, et al: Identification of the transforming EML4-ALK
fusion gene in non-small-cell lung cancer. Nature. 448:561–566.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mariño-Enríquez A and Dal Cin P: ALK as a
paradigm of oncogenic promiscuity: Different mechanisms of
activation and different fusion partners drive tumors of different
lineages. Cancer Genet. 206:357–373. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ninomiya H, Kato M, Sanada M, Takeuchi K,
Inamura K, Motoi N, Nagano H, Nomura K, Sakao Y, Okumura S, et al:
Allelotypes of lung adenocarcinomas featuring ALK fusion
demonstrate fewer onco- and suppressor gene changes. BMC Cancer.
13:82013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bunting SF and Nussenzweig A: End-joining,
translocations and cancer. Nat Rev Cancer. 13:443–454. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shaw AT and Engelman JA: ALK in lung
cancer: Past, present, and future. J Clin Oncol. 31:1105–1111.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cui S, Zhang W, Xiong L, Pan F, Niu Y, Chu
T, Wang H, Zhao Y and Jiang L: Use of capture-based next-generation
sequencing to detect ALK fusion in plasma cell-free DNA of patients
with non-small-cell lung cancer. Oncotarget. 8:2771–2780.
2017.PubMed/NCBI
|
|
10
|
Pekar-Zlotin M, Hirsch FR, Soussan-Gutman
L, Ilouze M, Dvir A, Boyle T, Wynes M, Miller VA, Lipson D, Palmer
GA, et al: Fluorescence in situ hybridization,
immunohistochemistry, and next-generation sequencing for detection
of EML4-ALK rearrangement in lung cancer. Oncologist. 20:316–322.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hofman P, Ilie M, Hofman V, Roux S, Valent
A, Bernheim A, Alifano M, Leroy-Ladurie F, Vaylet F, Rouquette I,
et al: Immunohistochemistry to identify EGFR mutations or ALK
rearrangements in patients with lung adenocarcinoma. Ann Oncol.
23:1738–1743. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Li T, Maus MK, Desai SJ, Beckett LA,
Stephens C, Huang E, Hsiang J, Zeger G, Danenberg KD, Astrow SH and
Gandara DR: Large-scale screening and molecular characterization of
EML4-ALK fusion variants in archival non-small-cell lung cancer
tumor specimens using quantitative reverse transcription polymerase
chain reaction assays. J Thorac Oncol. 9:18–25. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jaffe ES, Harris NL, Stein H and Vardiman
JW: Pathology and genetics of tumours of haematopoietic and
lymphoid tissues. IARC Press. 2001.
|
|
14
|
Cheson BD, Fisher RI, Barrington SF,
Cavalli F, Schwartz LH, Zucca E, Lister TA; Alliance, Australasian
Leukaemia and Lymphoma Group; Eastern Cooperative Oncology Group;
European Mantle Cell Lymphoma Consortium, ; et al: Recommendations
for initial evaluation, staging, and response assessment of Hodgkin
and non-Hodgkin lymphoma: The Lugano classification. J Clin Oncol.
32:3059–3068. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Medeiros LJ and Elenitobajohnson KS:
Anaplastic large cell lymphoma. Am J Clin Pathol. 127:707–722.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gustafson S, Medeiros LJ, Kalhor N and
Buesoramos CE: Anaplastic large cell lymphoma: Another entity in
the differential diagnosis of small round blue cell tumors. Ann
Diagn Pathol. 13:413–427. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Damm-Welk C, Pillon M, Woessmann W and
Mussolin L: Prognostic factors in paediatric anaplastic large cell
lymphoma: Role of ALK. Front Biosci (Schol Ed). 7:205–216. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Holla VR, Elamin YY, Bailey AM, Johnson
AM, Litzenburger BC, Khotskaya YB, Sanchez NS, Zeng J, Shufean MA,
Shaw KR, et al: ALK: A tyrosine kinase target for cancer therapy.
Cold Spring Harb Mol Case Stud. 3:a0011152017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Savage KJ, Harris NL, Vose JM, Ullrich F,
Jaffe ES, Connors JM, Rimsza L, Pileri SA, Chhanabhai M, Gascoyne
RD, et al: ALK-anaplastic large-cell lymphoma is clinically and
immunophenotypically different from both ALK+ ALCL and peripheral
T-cell lymphoma, not otherwise specified: Report from the
International peripheral T-cell lymphoma project. Blood.
111:5496–5504. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Roskoski R Jr: Anaplastic lymphoma kinase
(ALK): Structure, oncogenic activation, and pharmacological
inhibition. Pharmacol Res. 68:68–94. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Delsol G, Lamant L, Mariamé B, Pulford K,
Dastugue N, Brousset P, Rigal-Huguet F, al Saati T, Cerretti DP,
Morris SW and Mason DY: A new subtype of large B-cell lymphoma
expressing the ALK kinase and lacking the 2; 5 translocation.
Blood. 89:1483–1490. 1997.PubMed/NCBI
|
|
22
|
Laurent C, Do C, Gascoyne RD, Lamant L,
Ysebaert L, Laurent G, Delsol G and Brousset P: Anaplastic lymphoma
kinase-positive diffuse large B-cell lymphoma: A rare
clinicopathologic entity with poor prognosis. J Clin Oncol.
27:4211–4216. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gascoyne RD, Lamant L, Martin-Subero JI,
Lestou VS, Harris NL, Müller-Hermelink HK, Seymour JF, Campbell LJ,
Horsman DE, Auvigne I, et al: ALK-positive diffuse large B-cell
lymphoma is associated with Clathrin-ALK rearrangements: Report of
6 cases. Blood. 102:2568–2573. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Van Roosbroeck K, Cools J, Dierickx D,
Thomas J, Vandenberghe P, Stul M, Delabie J, De Wolf-Peeters C,
Marynen P and Wlodarska I: ALK-positive large B-cell lymphomas with
cryptic SEC31A-ALK and NPM1-ALK fusions. Haematologica. 95:509–513.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bedwell C, Rowe D, Moulton D, Jones G,
Bown N and Bacon CM: Cytogenetically complex SEC31A-ALK fusions are
recurrent in ALK-positive large B-cell lymphomas. Haematologica.
96:343–346. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Takeuchi K, Soda M, Togashi Y, Ota Y,
Sekiguchi Y, Hatano S, Asaka R, Noguchi M and Mano H:
Identification of a novel fusion, SQSTM1-ALK, in ALK-positive large
B-cell lymphoma. Haematologica. 96:464–467. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
D'Amore ES, Visco C, Menin A, Famengo B,
Bonvini P and Lazzari E: STAT3 pathway is activated in ALK-positive
large B-cell lymphoma carrying SQSTM1-ALK rearrangement and
provides a possible therapeutic target. Am J Surg Pathol.
37:780–786. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ettinger DS, Akerley W, Borghaei H, Chang
AC, Cheney RT, Chirieac LR, D'Amico TA, Demmy TL, Ganti AK,
Govindan R, et al: Non-small cell lung cancer. J Natl Compr Canc
Netw. 10:1236–1271. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Koivunen JP, Mermel C, Zejnullahu K,
Murphy C, Lifshits E, Holmes AJ, Choi HG, Kim J, Chiang D, Thomas
R, et al: EML4-ALK fusion gene and efficacy of an ALK kinase
inhibitor in lung cancer. Clin Cancer Res. 14:4275–4283. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Rodig SJ, Mino-Kenudson M, Dacic S, Yeap
BY, Shaw A, Barletta JA, Stubbs H, Law K, Lindeman N, Mark E, et
al: Unique clinicopathologic features characterize ALK-rearranged
lung adenocarcinoma in the western population. Clin Cancer Res.
15:5216–5223. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Shaw AT, Yeap BY, Mino-Kenudson M,
Digumarthy SR, Costa DB, Heist RS, Solomon B, Stubbs H, Admane S,
McDermott U, et al: Clinical features and outcome of patients with
non-small-cell lung cancer who harbor EML4-ALK. J Clin Oncol.
27:4247–4253. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Li Y, Li Y, Yang T, Wei S, Wang J, Wang M,
Wang Y, Zhou Q, Liu H and Chen J: Clinical significance of EML4-ALK
fusion gene and association with EGFR and KRAS gene mutations in
208 Chinese patients with non-small cell lung cancer. PLoS One.
8:e520932013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Shaozhang Z, Xiaomei L, Aiping Z, Jianbo
H, Xiangqun S and Qitao Y: Detection of EML4-ALK fusion genes in
non-small cell lung cancer patients with clinical features
associated with EGFR mutations. Genes Chromosomes Cancer.
51:925–932. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhang X, Zhang S, Yang X, Yang J, Zhou Q,
Yin L, An S, Lin J, Chen S, Xie Z, et al: Fusion of EML4 and ALK is
associated with development of lung adenocarcinomas lacking EGFR
and KRAS mutations and is correlated with ALK expression. Mol
Cancer. 9:1882010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wong DW, Leung EL, So KK, Tam IY, Sihoe
AD, Cheng LC, Ho KK, Au JS, Chung LP and Pik Wong M: University of
Hong Kong Lung Cancer Study Group: The EML4-ALK fusion gene is
involved in various histologic types of lung cancers from
nonsmokers with wild-type EGFR and KRAS. Cancer. 115:1723–1733.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Guo Y, Ma J, Lyu X, Liu H, Wei B, Zhao J,
Fu S, Ding L and Zhang J: Non-small cell lung cancer with EML4-ALK
translocation in Chinese male never-smokers is characterized with
early-onset. BMC Cancer. 14:8342014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ou SH, Bartlett CH, Mino-Kenudson M, Cui J
and Iafrate AJ: Crizotinib for the treatment of ALK-rearranged
non-small cell lung cancer: A success story to usher in the second
decade of molecular targeted therapy in oncology. Oncologist.
17:1351–1375. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Rikova K, Guo A, Zeng Q, Possemato A, Yu
J, Haack H, Nardone J, Lee K, Reeves C, Li Y, et al: Global survey
of phosphotyrosine signaling identifies oncogenic kinases in lung
cancer. Cell. 131:1190–1203. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Takeuchi K, Choi YL, Togashi Y, Soda M,
Hatano S, Inamura K, Takada S, Ueno T, Yamashita Y, Satoh Y, et al:
KIF5B-ALK, a novel fusion oncokinase identified by an
immunohistochemistry-based diagnostic system for ALK-positive lung
cancer. Clin Cancer Res. 15:3143–3149. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Togashi Y, Soda M, Sakata S, Sugawara E,
Hatano S, Asaka R, Nakajima T, Mano H and Takeuchi K: KLC1-ALK: A
novel fusion in lung cancer identified using a formalin-fixed
paraffin-embedded tissue only. PLoS One. 7:e313232012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Nishino M, Klepeis VE, Yeap BY, Bergethon
K, Morales-Oyarvide V, Dias-Santagata D, Yagi Y, Mark EJ, Iafrate
AJ and Mino-Kenudson M: Histologic and cytomorphologic features of
ALK-rearranged lung adenocarcinomas. Mod Pathol. 25:1462–1472.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Lee JK, Kim TM, Koh Y, Lee SH, Kim DW,
Jeon YK, Chung DH, Yang SC, Kim YT, Kim YW, et al: Differential
sensitivities to tyrosine kinase inhibitors in NSCLC harboring EGFR
mutation and ALK translocation. Lung Cancer. 77:460–463. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Yang J, Zhang X, Su J, Chen H, Tian H,
Huang Y, Xu C and Wu YL: Concomitant EGFR mutation and EML4-ALK
gene fusion in non-small cell lung cancer. J Clin Oncol. 29 Suppl
15:S10517. 2011. View Article : Google Scholar
|
|
45
|
Popat S, Vieira de Araújo A, Min T,
Swansbury J, Dainton M, Wotherspoon A, Lim E, Nicholson AG and
O'Brien ME: Lung adenocarcinoma with concurrent exon 19 EGFR
mutation and ALK rearrangement responding to erlotinib. J Thorac
Oncol. 6:1962–1963. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kris MG, Johnson BE, Kwiatkowski DJ,
Iafrate AJ, Wistuba II, Aronson SL, Engelman JA, Shyr Y, Khuri FR,
Rudin CM, et al: Identification of driver mutations in tumor
specimens from 1,000 patients with lung adenocarcinoma: The NCI's
lung cancer mutation consortium (LCMC). J Clin Oncol.
29:CRA75062011. View Article : Google Scholar
|
|
47
|
Leuschner I: Inflammatory myofibroblastic
tumor. Pathologe. 31:106–108. 2010.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Coffin CM, Watterson J, Priest JR and
Dehner LP: Extrapulmonary inflammatory myofibroblastic tumor
(inflammatory pseudotumor). A clinicopathologic and
immunohistochemical study of 84 cases. Am J Surg Pathol.
19:859–872. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Coffin CM, Hornick JL and Fletcher CD:
Inflammatory myofibroblastic tumor: Comparison of
clinicopathologic, histologic, and immunohistochemical features
including ALK expression in atypical and aggressive cases. Am J
Surg Pathol. 31:509–520. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Sokai A, Enaka M, Sokai R, Mori S, Mori S,
Gunji M, Fujino M and Ito M: Pulmonary inflammatory myofibroblastic
tumor harboring EML4-ALK fusion gene. Jpn J Clin Oncol. 44:93–96.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Griffin CA, Hawkins AL, Dvorak C, Henkle
C, Ellingham T and Perlman EJ: Recurrent involvement of 2p23 in
inflammatory myofibroblastic tumors. Cancer Res. 59:2776–2780.
1999.PubMed/NCBI
|
|
52
|
Chun YS, Wang L, Nascimento AG, Moir CR
and Rodeberg DA: Pediatric inflammatory myofibroblastic tumor:
Anaplastic lymphoma kinase (ALK) expression and prognosis. Pediatr
Blood Cancer. 45:796–801. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Busam KJ, Kutzner H, Cerroni L and Wiesner
T: Clinical and pathologic findings of Spitz nevi and atypical
Spitz tumors with ALK fusions. Am J Surg Pathol. 38:925–933. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Wiesner T, He J, Yelensky R, Esteve-Puig
R, Botton T, Yeh I, Lipson D, Otto G, Brennan K, Murali R, et al:
Kinase fusions are frequent in Spitz tumours and spitzoid
melanomas. Nat Commun. 5:31162014. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Yeh I, de la Fouchardiere A, Pissaloux D,
Mully TW, Garrido MC, Vemula SS, Busam KJ, LeBoit PE, McCalmont TH
and Bastian BC: Clinical, histopathologic, and genomic features of
Spitz tumors with ALK fusions. Am J Surg Pathol. 39:581–591. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Seo AN, Yoon G and Ro JY:
Clinicopathologic and molecular pathology of collecting duct
carcinoma and related renal cell carcinomas. Adv Anat Pathol.
24:65–77. 2017.PubMed/NCBI
|
|
57
|
Stöhr CG, Amann K and Hartmann A:
Histopathologie des Nierenzellkarzinoms. Der Urologe. 52:942–948.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Sukov WR, Hodge JC, Lohse CM, Akre MK,
Leibovich BC, Thompson RH and Cheville JC: ALK alterations in adult
renal cell carcinoma: Frequency, clinicopathologic features and
outcome in a large series of consecutively treated patients. Mod
Pathol. 25:1516–1525. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Mariño-Enríquez A, Ou WB, Weldon CB,
Fletcher JA and Pérez-Atayde AR: ALK rearrangement in sickle cell
trait-associated renal medullary carcinoma. Genes Chromosomes
Cancer. 50:146–153. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Debelenko LV, Raimondi SC, Daw N,
Shivakumar BR, Huang D, Nelson M and Bridge JA: Renal cell
carcinoma with novel VCL-ALK fusion: New representative of
ALK-associated tumor spectrum. Mod Pathol. 24:430–442. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Xing M: Molecular pathogenesis and
mechanisms of thyroid cancer. Nat Rev Cancer. 13:184–199. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Smallridge RC and Copland JA: Anaplastic
thyroid carcinoma: Pathogenesis and emerging therapies. Clin Oncol
(R Coll Radiol). 22:486–497. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Kelly LM, Barila G, Liu P, Evdokimova VN,
Trivedi S, Panebianco F, Gandhi M, Carty SE, Hodak SP, Luo J, et
al: Identification of the transforming STRN-ALK fusion as a
potential therapeutic target in the aggressive forms of thyroid
cancer. Proc Natl Acad Sci USA. 111:4233–4238. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Baudin E and Schlumberger M: New
therapeutic approaches for metastatic thyroid carcinoma. Lancet
Oncol. 8:148–156. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Chou A, Fraser S, Toon CW, Clarkson A,
Sioson L, Farzin M, Cussigh C, Aniss A, O'Neill C, Watson N, et al:
A detailed clinicopathologic study of ALK-translocated papillary
thyroid carcinoma. Am J Surg Pathol. 39:652–659. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Rassouli FB, Matin MM and Saeinasab M:
Cancer stem cells in human digestive tract malignancies. Tumor
Biol. 37:7–21. 2016. View Article : Google Scholar
|
|
67
|
Jazii FR, Najafi Z, Malekzadeh R, Conrads
TP, Ziaee AA, Abnet C, Yazdznbod M, Karkhane AA and Salekdeh GH:
Identification of squamous cell carcinoma associated proteins by
proteomics and loss of beta tropomyosin expression in esophageal
cancer. World J Gastroenterol. 14:7104–7112. 2006. View Article : Google Scholar
|
|
68
|
Aisner DL, Nguyen TT, Paskulin DD, Le AT,
Haney J, Schulte N, Chionh F, Hardingham J, Mariadason J, Tebbutt
N, et al: ROS1 and ALK fusions in colorectal cancer, with evidence
of intratumoral heterogeneity for molecular drivers. Mol Cancer
Res. 12:111–118. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Amatu A, Somaschini A, Cerea G, Bosotti R,
Valtorta E, Buonandi P, Marrapese G, Veronese S, Luo D, Hornby Z,
et al: Novel CAD-ALK gene rearrangement is drugable by entrectinib
in colorectal cancer. Br J Cancer. 113:1730–1734. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Ying J, Lin C, Wu J, Guo L, Qiu T, Ling Y,
Shan L, Zhou H, Zhao D, Wang J, et al: Anaplastic lymphoma kinase
rearrangement in digestive tract cancer: Implication for targeted
therapy in Chinese population. PLoS One. 10:e01447312015.
View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Lin E, Li L, Guan Y, Soriano R, Rivers CS,
Mohan S, Pandita A, Tang J and Modrusan Z: Exon array profiling
detects EML4-ALK fusion in breast, colorectal, and non-small cell
lung cancers. Mol Cancer Res. 7:1466–1476. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Röttgers S, Gombert M, Teigler-Schlegel A,
Busch K, Gamerdinger U, Slany R, Harbott J and Borkhardt A: ALK
fusion genes in children with atypical myeloproliferative leukemia.
Leukemia. 24:1197–1200. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Ren H, Tan ZP, Zhu X, Crosby K, Haack H,
Ren JM, Beausoleil S, Moritz A, Innocenti G, Rush J, et al:
Identification of anaplastic lymphoma kinase as a potential
therapeutic target in ovarian cancer. Cancer Res. 72:3312–3323.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Bilsland JG, Wheeldon A, Mead A,
Znamenskiy P, Almond S, Waters KA, Thakur M, Beaumont V, Bonnert
TP, Heavens R, et al: Behavioral and neurochemical alterations in
mice deficient in anaplastic lymphoma kinase suggest therapeutic
potential for psychiatric indications. Neuropsychopharmacology.
33:685–700. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Camidge DR, Bang YJ, Kwak EL, Iafrate AJ,
Varella-Garcia M, Fox SB, Riely GJ, Solomon B, Ou SH, Kim DW, et
al: Activity and safety of crizotinib in patients with ALK-positive
non-small-cell lung cancer: Updated results from a phase 1 study.
Lancet Oncol. 13:1011–1019. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Kwak EL, Bang YJ, Camidge DR, Shaw AT,
Solomon B, Maki RG, Ou SH, Dezube BJ, Jänne PA, Costa DB, et al:
Anaplastic lymphoma kinase inhibition in non-small-cell lung
cancer. N Engl J Med. 363:1693–1703. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Shaw AT, Kim DW, Nakagawa K, Seto T, Crinó
L, Ahn MJ, De Pas T, Besse B, Solomon BJ, Blackhall F, et al:
Crizotinib versus chemotherapy in advanced ALK-positive lung
cancer. N Engl J Med. 368:2385–2394. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Solomon BJ, Mok T, Kim DW, Wu YL, Nakagawa
K, Mekhail T, Felip E, Cappuzzo F, Paolini J, Usari T, et al:
First-line crizotinib versus chemotherapy in ALK-positive lung
cancer. N Engl J Med. 371:2167–2177. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Godbert Y, Henriques de Figueiredo B,
Bonichon F, Chibon F, Hostein I, Pérot G, Dupin C, Daubech A,
Belleannée G, Gros A, et al: Remarkable response to crizotinib in
woman with anaplastic lymphoma kinase-rearranged anaplastic thyroid
carcinoma. J Clin Oncol. 33:e84–e87. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Choi YL, Soda M, Yamashita Y, Ueno T,
Takashima J, Nakajima T, Yatabe Y, Takeuchi K, Hamada T, Haruta H,
et al: EML4-ALK mutations in lung cancer that confer resistance to
ALK inhibitors. N Engl J Med. 363:1734–1739. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Heuckmann JM, Hölzel M, Sos ML, Heynck S,
Balke-Want H, Koker M, Peifer M, Weiss J, Lovly CM, Grütter C, et
al: ALK mutations conferring differential resistance to
structurally diverse ALK inhibitors. Clin Cancer Res. 17:7394–7401.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Doebele RC, Pilling AB, Aisner DL,
Kutateladze TG, Le AT, Weickhardt AJ, Kondo KL, Linderman DJ,
Heasley LE, Franklin WA, et al: Mechanisms of resistance to
crizotinib in patients with ALK gene rearranged non-small cell lung
cancer. Clin Cancer Res. 18:1472–1482. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Katayama R, Shaw AT, Khan TM,
Mino-Kenudson M, Solomon BJ, Halmos B, Jessop NA, Wain JC, Yeo AT,
Benes C, et al: Mechanisms of acquired crizotinib resistance in
ALK-rearranged lung cancers. Sci Transl Med. 4:120ra1172012.
View Article : Google Scholar
|
|
84
|
Sasaki T, Okuda K, Zheng W, Butrynski J,
Capelletti M, Wang L, Gray NS, Wilner K, Christensen JG, Demetri G,
et al: The neuroblastoma associated F1174L ALK mutation causes
resistance to an ALK kinase inhibitor in ALK translocated cancers.
Cancer Res. 70:10038–10043. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Crystal AS, Shaw AT, Sequist LV, Friboulet
L, Niederst MJ, Lockerman EL, Frias RL, Gainor JF, Amzallag A,
Greninger P, et al: Patient-derived models of acquired resistance
can identify effective drug combinations for cancer. Science.
346:1480–1486. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Ji C, Zhang L, Cheng Y, Patel R, Wu H,
Zhang Y, Wang M, Ji S, Belani CP, Yang JM and Ren X: Induction of
autophagy contributes to crizotinib resistance in ALK-positive lung
cancer. Cancer Biol Ther. 15:570–577. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Mengoli MC, Barbieri F, Bertolini F, Tiseo
M and Rossi G: K-RAS mutations indicating primary resistance to
crizotinib in ALK-rearranged adenocarcinomas of the lung: Report of
two cases and review of the literature. Lung Cancer. 93:55–58.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Sequist LV, Gettinger S, Senzer NN,
Martins RG, Jänne PA, Lilenbaum R, Gray JE, Iafrate AJ, Katayama R,
Hafeez N, et al: Activity of IPI-504, a novel heat-shock protein 90
inhibitor, in patients with molecularly defined non-small-cell lung
cancer. J Clin Oncol. 28:4953–4960. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Normant E, Paez G, West KA, Lim AR, Slocum
KL, Tunkey C, McDougall J, Wylie AA, Robison K, Caliri K, et al:
The Hsp90 inhibitor IPI-504 rapidly lowers EML4-ALK levels and
induces tumor regression in ALK-driven NSCLC models. Oncogene.
30:2581–2586. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Shaw AT, Kim DW, Mehra R, Tan DS, Felip E,
Chow LQ, Camidge DR, Vansteenkiste J, Sharma S, De Pas T, et al:
Ceritinib in ALK-rearranged non-small-cell lung cancer. N Engl J
Med. 370:1189–1197. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Kodama T, Tsukaguchi T, Satoh Y, Yoshida
M, Watanabe Y, Kondoh O and Sakamoto H: Alectinib shows potent
antitumor activity against RET-rearranged non-small cell lung
cancer. Mol Cancer Ther. 13:2910–2918. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Sakamoto H, Tsukaguchi T, Hiroshima S,
Kodama T, Kobayashi T, Fukami TA, Oikawa N, Tsukuda T, Ishii N and
Aoki Y: CH5424802, a selective ALK inhibitor capable of blocking
the resistant gatekeeper mutant. Cancer Cell. 19:679–690. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Shaw AT, Gandhi L, Gadgeel S, Riely GJ,
Cetnar J, West H, Camidge DR, Socinski MA, Chiappori A, Mekhail T,
et al: Alectinib in ALK-positive, crizotinib-resistant,
non-small-cell lung cancer: A single-group, multicentre, phase 2
trial. Lancet Oncol. 17:234–242. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Zou HY, Friboulet L, Kodack DP, Engstrom
LD, Li Q, West M, Tang RW, Wang H, Tsaparikos K, Wang J, et al:
PF-06463922, an ALK/ROS1 inhibitor, overcomes resistance to first
and second generation ALK inhibitors in preclinical models. Cancer
Cell. 28:70–81. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Huang WS, Liu S, Zou D, Thomas M, Wang Y,
Zhou T, Romero J, Kohlmann A, Li F, Qi J, et al: Discovery of
Brigatinib (AP26113), a phosphine oxide-containing, potent, orally
active inhibitor of anaplastic lymphoma kinase. J Med Chem.
59:4948–4964. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
George SK, Vishwamitra D, Manshouri R, Shi
P and Amin HM: The ALK inhibitor ASP3026 eradicates NPM-ALK+ T-cell
anaplastic large-cell lymphoma in vitro and in a systemic xenograft
lymphoma model. Oncotarget. 5:5750–5763. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Lee J, Kim HC, Hong JY, Wang K, Kim SY,
Jang J, Kim ST, Park JO, Lim HY, Kang WK, et al: Detection of novel
and potentially actionable anaplastic lymphoma kinase (ALK)
rearrangement in colorectal adenocarcinoma by immunohistochemistry
screening. Oncotarget. 6:24320–24332. 2015.PubMed/NCBI
|
|
98
|
Lovly CM, Heuckmann JM, de Stanchina E,
Chen H, Thomas RK, Liang C and Pao W: Insights into ALK-driven
cancers revealed through development of novel ALK tyrosine kinase
inhibitors. Cancer Res. 71:4920–4931. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Sang J, Acquaviva J, Friedland JC, Smith
DL, Sequeira M, Zhang C, Jiang Q, Xue L, Lovly CM, Jimenez JP, et
al: Targeted inhibition of the molecular chaperone Hsp90 overcomes
ALK inhibitor resistance in non-small cell lung cancer. Cancer
Discov. 3:430–443. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Bonvini P, Gastaldi T, Falini B and
Rosolen A: Nucleophosmin-anaplastic lymphoma kinase (NPM-ALK), a
novel Hsp90-client tyrosine kinase: Down-regulation of NPM-ALK
expression and tyrosine phosphorylation in ALK(+) CD30(+) lymphoma
cells by the Hsp90 antagonist 17-allylamino,
17-demethoxygeldanamycin. Cancer Res. 62:1559–1566. 2002.PubMed/NCBI
|
|
101
|
Bloomfield M and Duesberg P: Inherent
variability of cancer-specific aneuploidy generates metastases. Mol
Cytogenet. 9:902016. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Heng HH, Regan SM, Liu G and Ye CJ: Why it
is crucial to analyze non clonal chromosome aberrations or NCCAs?
Mol Cytogenet. 9:152016. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Ye CJ, Regan S, Liu G, Alemara S and Heng
HH: Understanding aneuploidy in cancer through the lens of system
inheritance, fuzzy inheritance and emergence of new genome systems.
Mol Cytogenet. 11:312018. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Bloomfield M and Duesberg P: Is cancer
progression caused by gradual or simultaneous acquisitions of new
chromosomes? Mol Cytogenet. 11:42018. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Horne SD, Pollick SA and Heng HH:
Evolutionary mechanism unifies the hallmarks of cancer. Int J
Cancer. 136:2012–2021. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Tort F, Pinyol M, Pulford K, Roncador G,
Hernandez L, Nayach I, Kluin-Nelemans HC, Kluin P, Touriol C,
Delsol G, et al: Molecular characterization of a new ALK
translocation involving moesin (MSN-ALK) in anaplastic large cell
lymphoma. Lab Invest. 81:419–426. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Lamant L, Gascoyne RD, Duplantier MM,
Armstrong F, Raghab A, Chhanabhai M, Rajcan-Separovic E, Raghab J,
Delsol G and Espinos E: Non-muscle myosin heavy chain (MYH9): A new
partner fused to ALK in anaplastic large cell lymphoma. Genes
Chromosomes Cancer. 37:427–432. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Cools J, Wlodarska I, Somers R, Mentens N,
Pedeutour F, Maes B, De Wolf-Peeters C, Pauwels P, Hagemeijer A and
Marynen P: Identification of novel fusion partners of ALK, the
anaplastic lymphoma kinase, in anaplastic large-cell lymphoma and
inflammatory myofibroblastic tumor. Genes Chromosomes Cancer.
34:354–362. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Feldman AL, Vasmatzis G, Asmann YW, Davila
J, Middha S, Eckloff BW, Johnson SH, Porcher JC, Ansell SM and
Caride A: Novel TRAF1-ALK fusion identified by deep RNA sequencing
of anaplastic large cell lymphoma. Genes Chromosomes Cancer.
52:1097–1102. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Trinei M, Lanfrancone L, Campo E, Pulford
K, Mason DY, Pelicci PG and Falini B: A new variant anaplastic
lymphoma kinase (ALK)-fusion protein (ATIC-ALK) in a case of
ALK-positive anaplastic large cell lymphoma. Cancer Res.
60:793–798. 2000.PubMed/NCBI
|
|
111
|
Bridge JA, Kanamori M, Ma Z, Pickering D,
Hill DA, Lydiatt W, Lui MY, Colleoni GW, Antonescu CR, Ladanyi M
and Morris SW: Fusion of the ALK gene to the clathrin heavy chain
gene, CLTC, in inflammatory myofibroblastic tumor. Am J Pathol.
159:411–415. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Iyevleva AG, Raskin GA, Tiurin VI,
Sokolenko AP, Mitiushkina NV, Aleksakhina SN, Garifullina AR,
Strelkova TN, Merkulov VO, Ivantsov AO, et al: Novel ALK fusion
partners in lung cancer. Cancer Lett. 362:116–121. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Hernández L, Pinyol M, Hernández S, Beà S,
Pulford K, Rosenwald A, Lamant L, Falini B, Ott G, Mason DY, et al:
TRK-fused gene (TFG) is a new partner of ALK in anaplastic large
cell lymphoma producing two structurally different TFG-ALK
translocations. Blood. 94:3265–3268. 1999.PubMed/NCBI
|
|
114
|
Liang X, Meech SJ, Odom LF, Bitter MA,
Ryder JW, Hunger SP, Lovell MA, Meltesen L, Wei Q, Williams SA, et
al: Assessment of t(2;5)(p23;q35) translocation and variants in
pediatric ALK+ anaplastic large cell lymphoma. Am J Clin Pathol.
121:496–506. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Lawrence B, Perez-Atayde A, Hibbard MK,
Rubin BP, Dal Cin P, Pinkus JL, Pinkus GS, Xiao S, Yi ES, Fletcher
CD and Fletcher JA: TPM3-ALK and TPM4-ALK oncogenes in inflammatory
myofibroblastic tumors. Am J Pathol. 157:377–384. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Lamant L, Dastugue N, Pulford K, Delsol G
and Mariamé B: A new fusion gene TPM3-ALK in anaplastic large cell
lymphoma created by a (1;2)(q25;p23) translocation. Blood.
93:3088–3095. 1999.PubMed/NCBI
|
|
117
|
Onoda T, Kanno M, Sato H, Takahashi N,
Izumino H, Ohta H, Emura T, Katoh H, Ohizumi H, Ohtake H, et al:
Identification of novel ALK rearrangement A2M-ALK in a neonate with
fetal lung interstitial tumor. Genes Chromosomes Cancer.
53:865–874. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Ou SH, Klempner SJ, Greenbowe JR, Azada M,
Schrock AB, Ali SM, Ross JS, Stephens PJ and Miller VA:
Identification of a novel HIP1-ALK fusion variant in non-small-cell
lung cancer (NSCLC) and discovery of ALK I1171 (I1171N/S) mutations
in two ALK-rearranged NSCLC patients with resistance to Alectinib.
J Thorac Oncol. 9:1821–1825. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Fang DD, Zhang B, Gu Q, Lira M, Xu Q, Sun
H, Qian M, Sheng W, Ozeck M, Wang Z, et al: HIP1-ALK, a novel ALK
fusion variant that responds to crizotinib. J Thorac Oncol.
9:285–294. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Choi YL, Lira ME, Hong M, Kim RN, Choi SJ,
Song JY, Pandy K, Mann DL, Stahl JA, Peckham HE, et al: A novel
fusion of TPR and ALK in lung adenocarcinoma. J Thorac Oncol.
9:563–566. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Ji JH, Oh YL, Hong M, Yun JW, Lee HW, Kim
D, Ji Y, Kim DH, Park WY, Shin HT, et al: Identification of driving
ALK fusion genes and genomic landscape of medullary thyroid cancer.
PLoS Genet. 11:e10054672015. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Wang X, Krishnan C, Nguyen E, Meyer KJ,
Oliveira JL, Yang P, Yi ES, Yaszemski MJ, Maran A, Erickson-Johnson
MR and Oliveira AM: Fusion of dynactin 1 (DCTN1) to ALK in
inflammatory myofibroblastic tumor. Lab Invest. 2011.
|
|
123
|
Shimada Y, Kohno T, Ueno H, Ino Y, Hayashi
H, Nakaoku T, Sakamoto Y, Kondo S, Morizane C, Shimada K, et al: An
oncogenic ALK fusion and an RRAS mutation in KRAS mutation-negative
pancreatic ductal adenocarcinoma. Oncologist. 22:158–164. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Takeuchi K, Soda M, Togashi Y, Sugawara E,
Hatano S, Asaka R, Okumura S, Nakagawa K, Mano H and Ishikawa Y:
Pulmonary inflammatory myofibroblastic tumor expressing a novel
fusion, PPFIBP1-ALK: Reappraisal of Anti-ALK immunohistochemistry
as a tool for novel ALK fusion identification. Clin Cancer Res.
17:3341–3348. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Panagopoulos I, Nilsson T, Domanski HA,
Isaksson M, Lindblom P, Mertens F and Mandahl N: Fusion of the
SEC31L1 and ALK genes in an inflammatory myofibroblastic tumor. Int
J Cancer. 118:1181–1186. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Ouchi K, Miyachi M, Tsuma Y, Tsuchiya K,
Iehara T, Konishi E, Yanagisawa A and Hosoi H: FN1: A novel fusion
partner of ALK in an inflammatory myofibroblastic tumor. Pediatric
Blood Cancer. 62:909–911. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Ma Z, Hill DA, Collins MH, Morris SW,
Sumegi J, Zhou M, Zuppan C and Bridge JA: Fusion of ALK to the
Ran-binding protein 2 (RANBP2) gene in inflammatory myofibroblastic
tumor. Genes Chromosomes Cancer. 37:98–105. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Kusano H, Togashi Y, Akiba J, Moriya F,
Baba K, Matsuzaki N, Yuba Y, Shiraishi Y, Kanamaru H, Kuroda N, et
al: Two cases of renal cell carcinoma harboring a novel STRN-ALK
fusion gene. Am J Surg Pathol. 40:761–769. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Lovly CM, Mcdonald NT, Chen H,
Ortiz-Cuaran S, Heukamp LC, Yan Y, Florin A, Ozretić L, Lim D, Wang
L, et al: Rationale for co-targeting IGF-1R and ALK inALKfusion
positive lung cancer. Nat Med. 20:1027–1034. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Di Paolo D, Yang D, Pastorino F, Emionite
L, Cilli M, Daga A, Destafanis E, Di Fiore A, Piaggio F, Brignole
C, et al: New therapeutic strategies in neuroblastoma: Combined
targeting of a novel tyrosine kinase inhibitor and liposomal siRNAs
against ALK. Oncotarget. 6:28774–28789. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
Seto T, Kiura K, Nishio M, Nakagawa K,
Maemondo M, Inoue A, Hida T, Yamamoto N, Yoshioka H, Harada M, et
al: CH5424802 (RO5424802) for patients with ALK-rearranged advanced
non-small-cell lung cancer (AF-001JP study): A single-arm,
open-label, phase 1–2 study. Lancet Oncol. 14:590–598. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Gadgeel SM, Gandhi L, Riely GJ, Chiappori
AA, West HL, Azada MC, Morcos PN, Lee RM, Garcia L, Yu L, et al:
Safety and activity of alectinib against systemic disease and brain
metastases in patients with crizotinib-resistant ALK-rearranged
non-small-cell lung cancer (AF-002JG): Results from the
dose-finding portion of a phase 1/2 study. Lancet Oncol.
15:1119–1128. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Johnson TW, Richardson PF, Bailey S,
Brooun A, Burke BJ, Collins MR, Cui JJ, Deal JG, Deng YL, Dinh D,
et al: Discovery of
(10R)-7-amino-12-fluoro-2,10,16-trimethyl-15-oxo-10,15,16,17-tetrahydro-2H-8,4-(metheno)pyrazolo[4,3-h][2,5,11]-benzoxadiazacyclotetradecine-3-carbonitrile
(PF-06463922), a macrocyclic inhibitor of anaplastic lymphoma
kinase (ALK) and c-ros oncogene 1 (ROS1) with preclinical brain
exposure and broad-spectrum potency against ALK-resistant
mutations. J Med Chem. 57:4720–4744. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Mologni L, Ceccon M, Pirola A, Chiriano G,
Piazza R, Scapozza L and Gambacorti-Passerini C: NPM/ALK mutants
resistant to ASP3026 display variable sensitivity to alternative
ALK inhibitors but succumb to the novel compound PF-06463922.
Oncotarget. 6:5720–5734. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Basit S, Ashraf Z, Lee K and Latif M:
First macrocyclic 3rd-generation ALK inhibitor for treatment of
ALK/ROS1 cancer: Clinical and designing strategy update of
lorlatinib. Eur J Med Chem. 134:348–356. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
136
|
Katayama R, Khan TM, Benes C, Lifshits E,
Ebi H, Rivera VM, Shakespeare WC, Iafrate AJ, Engelman JA and Shaw
AT: Therapeutic strategies to overcome crizotinib resistance in
non-small cell lung cancers harboring the fusion oncogene EML4-ALK.
Proc Natl Acad Sci USA. 108:7535–7540. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
137
|
Ceccon M, Mologni L, Bisson W, Scapozza L
and Gambacorti-Passerini C: Crizotinib-resistant NPM-ALK mutants
confer differential sensitivity to unrelated Alk inhibitors. Mol
Cancer Res. 11:122–132. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
138
|
Cheng M, Quail MR, Gingrich DE, Ott GR, Lu
L, Wan W, Albom MS, Angeles TS, Aimone LD, Cristofani F, et al:
CEP-28122, a highly potent and selective orally active inhibitor of
anaplastic lymphoma kinase with antitumor activity in experimental
models of human cancers. Mol Cancer Ther. 11:670–679. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
139
|
Arkenau HT, Sachdev JC, Mita MM,
Dziadziuszko R, Lin CC, Yang JC, Infante JR, Anthony SP,
Voskoboynik M, Su WC, et al: Phase (Ph) 1/2a study of TSR-011, a
potent inhibitor of ALK and TRK, in advanced solid tumors including
crizotinib-resistant ALK positive non-small cell lung cancer. J
Clin Oncol. 33:8063. 2015.
|
|
140
|
Mori M, Ueno Y, Konagai S, Fushiki H,
Shimada I, Kondoh Y, Saito R, Mori K, Shindou N, Soga T, et al: The
selective anaplastic lymphoma receptor tyrosine kinase inhibitor
ASP3026 induces tumor regression and prolongs survival in non-small
cell lung cancer model mice. Mol Cancer Ther. 13:329–340. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Katayama R, Friboulet L, Koike S,
Lockerman EL, Khan TM, Gainor JF, Iafrate AJ, Takeuchi K, Taiji M,
Okuno Y, et al: Two novel ALK mutations mediate acquired resistance
to the next-generation ALK inhibitor alectinib. Clin Cancer Res.
20:5686–5696. 2014. View Article : Google Scholar : PubMed/NCBI
|