Introduction
As the most prevalent cancer in women, breast cancer
affects >1 million women worldwide and accounts for ~23% of all
cases of cancer among women (1,2). In
addition, the annual incidence of breast cancer in China was
~20,8000 cases in 2010, which accounted for 16.2% of all cancer
cases in females (3). Breast cancer
has become one of the main causes of death among young women in
China (4). A multidisciplinary
comprehensive treatment model has gradually been developed,
including surgery, radiotherapy, chemotherapy and endocrine therapy
(5). These treatments have improved
the long-term survival of patients with breast cancer and reduced
the rates of recurrence and metastasis (6). Nevertheless, chemotherapy has several
side effects, and whether patients with low-risk early-stage breast
cancer benefit from chemotherapy remains to be determined.
Effective methods to accurately predict recurrence risk and
simultaneously provide appropriate treatment to patients have not
been established.
With the development of genomics (7), the treatment of breast cancer has
stepped into a new era. The 21-gene recurrence score (RS) assay for
patients with estrogen receptor (ER)-positive breast cancer has
been demonstrated to be more accurate than clinicopathological
indicators in predicting prognosis and metastasis (8–11). The
21-gene assay has already been recommended by the National
Comprehensive Cancer Network (NCCN) and the American Society of
Clinical Oncology for patients with early-stage breast cancer
(12,13). Based on the results of National
Surgical Adjuvant Breast and Bowel Project (NSABP) B-20 trials, a
score <18 was categorized as low risk, a score between 18 and 30
was considered intermediate risk and a score ≥31 was categorized as
high risk (8,14,15).
This test helps screen out patients with low recurrence risk,
thereby avoiding excessive chemotherapy. In a previous study, 70
surgeons at the Israeli Cancer clinics selected 300 Israeli
patients with breast cancer to perform 21-gene RS tests (16). The results demonstrated that age and
tumor size had no correlation with the RS value. In addition, the
NSABP B-20 and Southwest Oncology Group-8814 trials revealed that
the RS predicted benefit from adjuvant chemotherapy in
tumor-node-metastasis (TNM) node stage (N)0–3 patients (14,17).
The 21-gene RS detection was obtained from large
datasets abroad, but lacked the validation of large samples in
China. In addition, the clinicopathological characteristics
included in previous studies were limited. To the best of our
knowledge, there have been no studies regarding the relationship
between RS assay and chemotherapeutic efficacy-related target
genes. Therefore, the present study aimed to analyze
clinicopathological characteristics and chemotherapeutic
efficacy-related target genes with 21-gene RS in patients with
hormone receptor-positive early-stage breast cancer in China. The
changes of treatment decisions before and after the 21-gene RS test
were compared, and the prognostic value of chemotherapeutic
efficacy-related target genes was examined to aid in the evaluation
of the guiding significance of the 21-gene RS in the diagnosis and
treatment of patients with breast cancer in China and to aid in the
discovery of new prognostic markers.
Materials and methods
Data and patients
A retrospective, single-center study was conducted
at The First Affiliated Hospital of Xi'an Jiaotong University
(Xi'an, China). The data from 110 patients with ER-positive, human
epidermal growth factor receptor 2 (HER2)-negative, node-negative
T1-3N0M0 breast cancer who were tested for the 21-gene RS and
underwent surgical treatment between June 2013 and December 2016
were reviewed. Exclusion criteria were patients with T4 tumors,
those having received neoadjuvant therapy or those with distant
metastasis occurring at first diagnosis. The study was approved by
the Ethics Committee of the First Affiliated Hospital of Xi'an
Jiaotong University.
Clinicopathological data
Clinicopathological data were collected after
obtaining informed consent from patients. Pathological
examinations, including detection of ER, progesterone receptor
(PR), HER2, nuclear protein Ki67, tumor protein p53 and cytokeratin
5/6 (CK5/6) protein expressions by immunohistochemistry (IHC), were
conducted in the pathology department of The First Affiliated
Hospital of Xi'an Jiaotong University (Xi'an, China). The IHC
analysis was conducted prior to the study. ER+ or
PR+ results were defined as hormone receptor-positive.
For HER2, the cytomembrane of cancer cells without staining was
defined as HER2−. Any proportion of cancer cells
exhibiting weak or incomplete cytomembrane staining or <10% of
cancer cells exhibiting weak or complete cytomembrane staining were
defined as HER2+; ≥10% of cancer cells exhibiting weak
or moderately intact cytomembrane staining or <10% cancer cells
exhibiting uniform, strong and complete cytomembrane staining were
defined as HER2++; ≥10% of cancer cells exhibiting
consistent, strong and intact cytomembrane staining were defined as
HER2+++; HER2− or HER2+ was
considered as HER2 low expression, which was considered negative in
clinical therapy; HER2+++ was HER2 positive; and
HER2++ required further detection with fluorescent in
situ hybridization (FISH). If no gene expression was observed
in the FISH analysis, HER2 was categorized as negative; otherwise,
it was positive. For p53 and CK5/6, ≥10% staining of cancer cells
was defined as positive. In addition to pathological data, the
following data were recorded: Age, occupation, marital status, body
mass index (BMI), menopausal status, tumor discovery time, tumor
size, pathological type, histological grade, vascular tumor embolus
state, TNM stage, clinical stage, molecular type, surgical scheme
and tumor markers, including carcinoembryonic antigen and cancer
antigen 15-3 tested by chemiluminescence microparticle I2000
immunoassay (Abbott, Abbott Park, IL, USA).
Patient occupations were classified as manual
worker, skilled worker or unemployed. Manual workers included
laborers and farmers. Skilled workers included clerks, national
civil servants and professionals. The unemployed group also
included retirees. The BMI (kg/m2) categories were based
on the Working Group on Obesity in China with the support of the
International Life Science Institute Focal point in China.
Menopausal status referred to the definition of menopause as per
the NCCN Guidelines (version 2, 2017). Tumor discovery time was
calculated between the discovery of the breast lump and the initial
breast cancer diagnosis. The diagnosis of TNM stage was based on
the Cancer Staging Manual, Seventh Edition (American Joint
Committee on Cancer, 2010; Springer Science Business Media)
(18) and the Nottingham combined
histologic grade was referenced. The molecular type was based on
the St. Gallen International Expert Consensus on the Primary
Therapy of Early Breast Cancer (2013) (19).
Assay for 21-gene detection,
chemotherapeutic efficacy-related target gene detection and RS
definition
The 21-gene RS assay and the detection of
chemotherapeutic efficacy-related target genes were performed on
paraffin-embedded tumor samples at Surexam Medical Laboratory
(Medical Institution Licensing permit no. 440116PDY707461;
Guangzhou, China) using the DNA liquid chip technology to transfer
the probe of a traditional gene chip from a solid carrier to liquid
to increase the detection efficiency. The target genes were
thymidylate synthetase (TYMS), ribonucleotide reductase
catalytic subunit M1 (RRM1), tubulin β3 class III
(TUBB3), DNA topoisomerase IIα (TOP2A) and
phosphatase and tensin homolog (PTEN) (20–25).
Gene expression did not translate or equate to protein expression
of those markers by IHC due to differences in the detection
methods. The expression levels of the following 21 gene mRNAs,
which are related to recurrence risk, were detected and calculated
to determine the RS: Ki67, aurora kinase A (STK15),
Survivin, cyclin B1 (CCNB1), MYB proto-oncogene like 2
(MYBL2), growth factor receptor-bound protein 7
(GRB7), HER2, ER, PR, BCL2 apoptosis regulator
(BCL2), signal peptide, CUB domain and EGF-like
domain-containing 2 (SCUBE2), matrix metallopeptidase 11
(MMP11), cathepsin V (CTSL2), glutathione
S-transferase µ1 (GSTM1), scavenger receptor class D, member
1 (CD68), BCL2-associated athanogene 1 (BAG1),
β-actin (ACTB), GAPDH, ribosomal protein lateral stalk
subunit P0 (RPLP0), β-glucuronidase (GUS) and
transferrin receptor (TFRC). RS <18 was categorized as
low risk, RS between 18 and 30 was considered to be intermediate
risk, and RS ≥31 was categorized as high risk (8).
Kaplan-Meier Plotter database
As a tool for meta-analysis-based biomarker
assessment, the Kaplan-Meier Plotter (http://www.kmplot.com) (26) was used to analyze the prognostic
values of TYMS, RRM1, TUBB3, TOP2A and PTEN mRNA
expression levels in ER+ breast cancer. Kaplan-Meier
survival plots were drawn using data from the Kaplan-Meier
database. A log P-value <0.01 was considered to indicate a
statistically significant difference.
Therapeutic decision making and
follow-up
Patients' data were discussed by the
Multidisciplinary team (MDT) of The First Affiliated Hospital of
Xi'an Jiaotong University. The MDT team independently made
therapeutic decisions before and after the RS test. The clinical
decision was made based on the Chinese Society of Clinical Oncology
Breast Cancer diagnosis and treatment guidelines and NCCN Clinical
Practice Guidelines in Oncology of Breast Cancer, St. Gallen
Consensus. Finalized therapeutic decisions were made by combining
the physician's clinical experience, the patients and their
families' expectations, and patients' individual situation.
Patients and their families were informed with the final decision
and informed consent was obtained. All patients were followed up by
a combination of outpatient and telephone visits to confirm
recurrence, metastasis or death of breast cancer.
Statistical analysis
All categorical variables are expressed as the means
of absolute numbers and percentages, whereas abnormally distributed
continuous variables are expressed as medians and ranges. The
associations between the 21-gene RS and clinicopathological
characteristics that were categorical variables were analyzed by
the χ2 test. Fisher's exact test was applied when the
theoretical frequency was <5 or the total observation frequency
was <20. For continuous variables, if they met the assumptions
of normality and homogeneity, Student's unpaired t-test was
performed. Otherwise, these variables were analyzed by the Wilcoxon
rank-sum test. The relationships between the 21-gene RS and
chemotherapeutic efficacy-related target genes were estimated using
the Wilcoxon rank-sum test, and correlations were tested using
Spearman's rank test. Univariate binary logistic regression of
clinicopathological characteristics and chemotherapeutic
efficacy-related target genes with 21-gene RSs and multivariate
logistic analysis of independent variables associated with the
21-gene RS were analyzed. Furthermore, the McNemar χ2
test was used to compare the differences in treatment decisions
before and after the 21-gene test. All statistical tests were two
sided. P<0.05 was considered to indicate a statistically
significant difference. All analyses were performed using SPSS 18.0
(SPSS, Inc., Chicago, IL, USA).
Results
Patient clinicopathological
characteristics
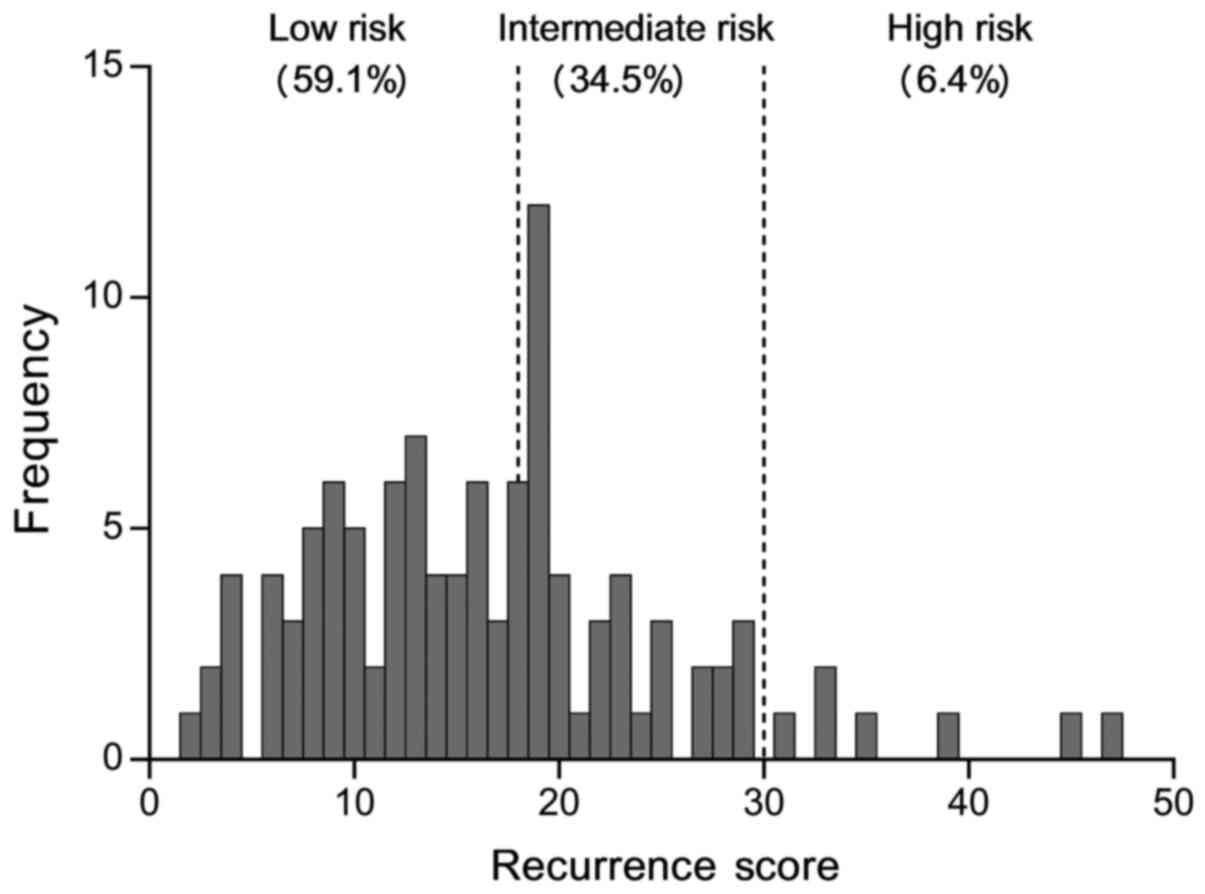
A total of 110 female patients with ER+
breast cancer who were tested with the 21-gene RS test and treated
at The First Affiliated Hospital of Xi'an Jiaotong University were
included in the present study (Fig.
1; Table I). Based on RS
criteria, the majority of patients (59.1%; 65/110) were classified
in the low-RS group, 34.5% (38/110) in the intermediate-RS group
and 6.4% (7/110) in the high-RS group. Most patients (30.9%;
34/110) were skilled workers. Nearly 96% of patients were married,
and the majority (60%; 66/110) had normal BMI. The proportions of
postmenopausal and premenopausal patients were 51% (56/110) and 48%
(53/110), respectively. A total of 93 (84.6%) patients had invasive
ductal carcinoma; none of the patients had lymph node metastasis or
a vascular tumor embolus. The clinical stages were I–II (100%). The
baseline data are presented in Table
I.
 | Table I.Clinicopathological characteristics
of patients with ER+ breast cancer. |
Table I.
Clinicopathological characteristics
of patients with ER+ breast cancer.
| Clinicopathological
characteristic | N | % | Valid%a |
|---|
| Age (years) |
|
<45 | 33 | 30.00 | 30.00 |
|
45–59 | 50 | 45.45 | 45.45 |
|
≥60 | 27 | 24.55 | 24.55 |
|
Occupationb |
| Manual
worker | 28 | 25.45 | 31.11 |
| Skilled
worker | 34 | 30.91 | 37.78 |
|
Unemployed | 28 | 25.45 | 31.11 |
|
Other | 20 | 18.18 |
|
| Marital status |
|
Married | 106 | 96.36 | 96.36 |
|
Divorced | 2 | 1.82 | 1.82 |
| Not
married | 2 | 1.82 | 1.82 |
| BMIc |
|
Underweight: <18.5 | 6 | 5.45 | 5.45 |
| Normal
weight: 18.5–23.9 | 66 | 60.00 | 60.00 |
|
Overweight: ≥24.0 | 38 | 34.55 | 34.55 |
| Menopausal
stated |
|
Postmenopausal | 56 | 50.91 | 51.38 |
|
Premenopausal | 53 | 48.18 | 48.62 |
|
Other | 1 | 0.91 |
|
| Tumor discovery
time (days)e |
| t
<1week | 11 | 10.00 | 10.00 |
| 1 week
≤ t <2 weeks | 16 | 14.55 | 14.55 |
| 2 weeks
≤ t <1 month | 18 | 16.36 | 16.36 |
| 1 month
≤ t <6 months | 30 | 27.28 | 27.28 |
| 6
months ≤ t <1 year | 14 | 12.73 | 12.73 |
| t ≥1
year | 21 | 19.09 | 19.09 |
| Tumor size
(cm) |
| ≤2 | 73 | 66.36 | 66.36 |
|
>2 | 37 | 33.64 | 33.64 |
| Pathological
type |
|
IDC | 93 | 84.55 | 84.55 |
|
ILC | 9 | 8.18 | 8.18 |
|
IPC | 4 | 3.64 | 3.64 |
|
IMPC | 1 | 0.91 | 0.91 |
| MC | 3 | 2.73 | 2.73 |
| Vascular tumor
embolus |
|
Yes | 0 | 0 | 0 |
| No | 110 | 100 | 100 |
| Histological
gradef |
| I | 13 | 11.82 | 12.50 |
| II | 63 | 57.27 | 60.58 |
|
III | 28 | 25.45 | 26.92 |
|
Unknown | 6 | 5.45 |
|
| T
stageg |
| T1 | 73 | 66.36 | 66.36 |
| T2 | 36 | 32.73 | 32.73 |
| T3 | 1 | 0.91 | 0.91 |
| N
stageg |
| N0 | 110 | 100 | 100 |
|
N1-3 | 0 | 0 | 0 |
| M
stageg |
| M0 | 110 | 100 | 100 |
| M1 | 0 | 0 | 0 |
| Clinical
stageg |
| I | 73 | 66.36 | 66.36 |
| II | 37 | 33.64 | 33.64 |
|
III | 0 | 0 | 0 |
| Molecular
typeh |
| Luminal
A | 46 | 41.82 | 41.82 |
| Luminal
B | 64 | 58.18 | 58.18 |
| Luminal
B (−) | 57 | 51.82 | 51.82 |
| Luminal
B (+) | 7 | 6.36 | 6.36 |
| Surgical
scheme |
|
BCS | 16 | 14.55 | 14.55 |
|
BMS | 94 | 85.45 | 85.45 |
| ER |
|
Positive | 110 | 100 | 100 |
|
Negative | 0 | 0 | 0 |
| p53 |
|
≤10% | 74 | 67.27 | 71.84 |
|
11–50% | 20 | 18.18 | 19.42 |
|
≥51% | 9 | 8.18 | 8.74 |
|
Unknown | 7 | 6.36 |
|
| CK5/6 |
|
Positive | 9 | 8.18 | 8.65 |
|
Negative | 95 | 86.36 | 91.35 |
|
Unknown | 6 | 5.45 |
|
| Tumor markers CEA
(ng/ml) |
|
Negative, 0.00–3.40 | 100 | 90.91 | 92.59 |
|
Positive, >3.40 | 8 | 7.27 | 7.41 |
|
Unknown | 2 | 1.82 |
|
| Tumor markers
CA15-3 (ng/ml) |
|
Negative 0.00–25.00 | 105 | 95.45 | 97.22 |
|
Positive >25.00 | 3 | 2.73 | 2.78 |
|
Unknown | 2 | 1.82 |
|
Distribution of RS based on
clinicopathological characteristics
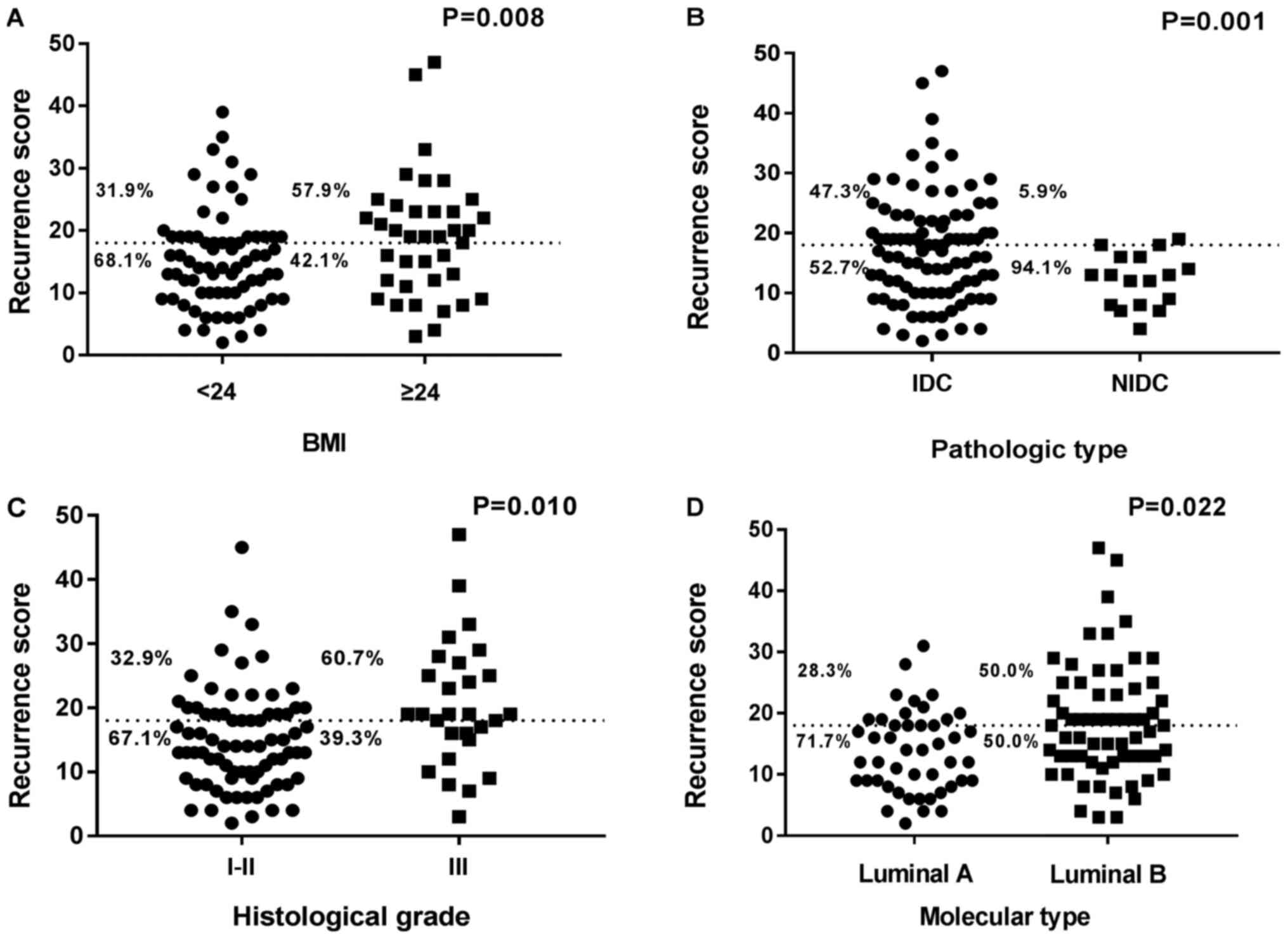
The associations between the 21-gene RS and
clinicopathological characteristics are shown in Tables II and III. Median age at initial diagnosis of
breast cancer in the low-RS group was 52 years old (range, 25–73),
whereas median age was 50 years (range, 30–70) in the
intermediate/high-RS group. The distribution of the 21-gene RS
varied significantly according to BMI, pathological type,
histological grade and molecular grade (P<0.05; Table II). Patients with higher BMI,
invasive ductal carcinoma type, higher histological grade and
luminal B molecular type were more likely to have higher RS
compared with patients with lower BMI, non-invasive ductal
carcinoma, lower histological grade and luminal A molecular type
(Fig. 2). In histological grade I–II
tumors, the proportions of low and intermediate/high RS were 67.1
and 32.9%, respectively, whereas in patients with histological
grade III tumors, the proportions were 39.3 and 60.7% respectively
(P=0.010; Fig. 2C). Similarly,
compared with patients with lower BMI, non-invasive ductal
carcinoma type and luminal A molecular type, patients with higher
BMI, invasive ductal carcinoma type and luminal B molecular type
were more likely to be categorized as the intermediate/high-RS
group and less likely to be categorized as the low-RS group
(P<0.05; Table II). In addition,
univariate binary logistic regression analysis revealed that higher
BMI [odds ratio (OR), 2.929; P=0.010], invasive ductal carcinoma
type (OR, 14.367; P=0.011), higher histological grade (OR, 3.153;
P=0.012) and luminal B molecular type (OR, 2.538; P=0.024) were
independent risk factors for higher RS (Table III).
| Table II.Relationship between 21-gene RS and
clinicopathological characteristics. |
Table II.
Relationship between 21-gene RS and
clinicopathological characteristics.
|
| RS risk groups |
|
|---|
|
|
|
|
|---|
| Clinicopathological
characteristics | Low risk (RS
<18) | Intermediate/high
risk (RS ≥18) | P-value |
|---|
| Median age, years
(range) | 52 (25–73) | 50 (30–70) | 0.619 |
| Median tumor
discovery time, days (range) | 56 (2–1680) | 28 (2–1680) | 0.317 |
| Occupation |
|
| 0.507 |
| Manual
worker | 15 (26.8) | 13 (38.2) |
|
| Skilled
worker | 22 (39.3) | 12 (35.3) |
|
|
Unemployed | 19 (33.9) | 9
(26.5) |
|
| BMI |
|
| 0.008 |
|
<24 | 49 (75.4) | 23 (51.1) |
|
|
≥24 | 16 (24.6) | 22 (48.9) |
|
| Menopausal
state |
|
| 0.902 |
|
Postmenopausal | 34 (52.3) | 23 (51.1) |
|
|
Premenopausal | 31 (47.7) | 22 (48.9) |
|
| Tumor size |
|
| 0.113 |
| ≤2 | 47 (72.3) | 26 (57.8) |
|
|
>2 | 18 (27.7) | 19 (42.2) |
|
| Pathological
type |
|
| 0.001 |
|
IDC | 49 (75.4) | 44 (97.8) |
|
|
NIDC | 16 (24.6) | 1
(2.2) |
|
| Histological
grade |
|
| 0.010 |
|
I–II | 51 (82.3) | 25 (59.5) |
|
|
III | 11 (17.7) | 17 (40.5) |
|
| Clinical stage |
|
| 0.113 |
| Stage
I | 47 (72.3) | 26 (57.8) |
|
| Stage
II–III | 18 (27.7) | 19 (42.2) |
|
| Molecular type |
|
| 0.022 |
| Luminal
A | 33 (50.8) | 13 (28.9) |
|
| Luminal
B | 32 (49.2) | 32 (71.1) |
|
| Surgical
scheme |
|
| 0.764 |
|
BCS | 10 (15.4) | 6
(13.3) |
|
|
BMS | 55 (84.6) | 39 (86.7) |
|
| Median P53%
(range) | 8
(1–90) | 10 (1–90) | 0.099 |
| CK5/6 status |
|
Positive | 4
(6.8) | 5
(11.1) | 0.670 |
|
Negative | 55 (93.2) | 40 (88.9) |
|
| Median CEA, ng/ml
(range) | 1.50
(0.31–4.62) | 1.52
(0.20–5.73) | 0.771 |
| Median CA15-3,
ng/ml (range) | 9.37
(4.67–25.48) | 11.12
(4.85–28.48) | 0.215 |
| Table III.Univariate binary logistics
regression analysis of clinicopathological characteristics with
21-gene recurrence score. |
Table III.
Univariate binary logistics
regression analysis of clinicopathological characteristics with
21-gene recurrence score.
|
| High/intermediate
vs. low risk |
|
|---|
|
|
|
|
|---|
| Clinicopathological
characteristics | OR | 95% CI | P-value |
|---|
| Age | 0.991 | 0.955–1.028 | 0.616 |
| Tumor discovery
time | 1.000 | 0.998–1.001 | 0.664 |
| Occupation |
|
| 0.510 |
| Manual
worker | 1.830 | 0.617–5.423 | 0.276 |
| Skilled
worker | 1.152 | 0.399–3.324 | 0.794 |
|
Unemployed | Ref |
|
|
| BMI |
|
<24 | Ref |
|
|
|
≥24 | 2.929 | 1.300–6.601 | 0.010 |
| Menopausal
state |
|
Postmenopausal | Ref |
|
|
|
Premenopausal | 1.049 | 0.490–2.245 | 0.902 |
| Tumor size
(cm) |
| ≤2 | Ref |
|
|
|
>2 | 1.908 | 0.855–4.260 | 0.115 |
| Pathological
type |
|
NIDC | Ref |
|
|
|
IDC | 14.367 | 1.830–112.826 | 0.011 |
| Histological
grade |
|
I–II | Ref |
|
|
|
III | 3.153 | 1.286–7.729 | 0.012 |
| Clinical stage |
| Stage
I | Ref |
|
|
| Stage
II–III | 1.908 | 0.855–4.260 | 0.115 |
| Molecular type |
| Luminal
A | Ref |
|
|
| Luminal
B | 2.538 | 1.132–5.692 | 0.024 |
| Surgical
scheme |
|
BCS | Ref |
|
|
|
BMS | 1.182 | 0.397–3.523 | 0.764 |
| P53
(%) | 7.592 | 0.940–61.290 | 0.057 |
| CK5/6 status |
|
Positive | Ref |
|
|
|
Negative | 0.582 | 0.147–2.304 | 0.441 |
| CEA | 1.076 | 0.747–1.551 | 0.693 |
| CA15-3 | 1.042 | 0.971–1.118 | 0.254 |
Distribution of RS according to
chemotherapeutic efficacy-related target genes
Detection of PTEN, TYMS, RRM1, TUBB3 and
other genes related to the efficacy and/or side effects of
chemotherapeutic drugs predicted the therapeutic effects and/or
side effects of chemotherapeutic drugs for each patient; the
results were used to inform chemotherapy treatment. The
associations between RS and chemotherapeutic efficacy-related
target genes are demonstrated in Table
IV. Differences in TYMS and TOP2A gene expression
between the low- and intermediate/high-risk RS groups were
statistically significant (P<0.05; Table IV). Patients with higher TYMS
gene expression were more likely to have intermediate/high-risk RS
compared with patients with lower TYMS gene expression
(P=0.001; Table IV). In addition,
the proportion of intermediate/high-risk RS was significantly
higher among patients with higher TOP2A expression
(P<0.001; Table IV). PTEN,
RRM1 and TUBB3 had no impact on RS categories.
Furthermore, univariate binary logistic regression analysis showed
that TYMS (OR, 14.950; P=0.001) and TOP2A (OR,
14.846; P<0.001) gene expression levels were independent risk
factors for higher RS (Table V).
| Table IV.Relationship between 21-gene RS and
chemotherapeutic efficacy-related target genes. |
Table IV.
Relationship between 21-gene RS and
chemotherapeutic efficacy-related target genes.
|
| RS risk groups N
(%)a |
|
|---|
|
|
|
|
|---|
| Chemotherapeutic
efficacy-related target genes | Low risk (RS
<18) | Intermediate/high
risk (RS ≥18) | P-value |
|---|
| TYMS | 28.4 (1–89) | 45.8 (4.5–96) | 0.001 |
| RRM1 | 44.8 (1–98.1) | 43.5 (1–99) | 0.975 |
| TUBB3 | 39.6 (1–99) | 52.3 (0.8–99) | 0.337 |
| TOP2A | 35.9
(1.1–94.6) | 63.1
(2.7–98.1) |
<0.001 |
| PTEN | 64.7 (7.9–99) | 65.6 (1.4–99) | 0.681 |
| Table V.Univariate binary logistics
regression analysis of chemotherapeutic efficacy- related target
genes with 21-gene recurrence score. |
Table V.
Univariate binary logistics
regression analysis of chemotherapeutic efficacy- related target
genes with 21-gene recurrence score.
|
| High/intermediate
vs. low risk |
|
|---|
|
|
|
|
|---|
|
Chemotherapeuticefficacy-related target
genes | OR | 95% CI | P-value |
|---|
| TYMS | 14.950 | 2.863–78.082 | 0.001 |
| RRM1 |
0.972 | 0.257–3.670 | 0.966 |
| TUBB3 |
2.034 | 0.482–8.574 | 0.333 |
| TOP2A | 14.846 | 3.269–67.433 |
<0.001 |
| PTEN |
0.620 | 0.154–2.495 | 0.501 |
Multivariate analysis of independent
variables associated with the 21-gene RS
Multivariate logistic regression analysis
demonstrated that BMI, histological grade and TOP2A were
independent variables associated with RS (Table VI). Patients with BMI ≥24 were more
likely to have high/intermediate-risk RS compared with patients
with BMI <24 (OR, 3.590; 95% CI, 1.296–9.947; P=0.014).
Histological grade III was associated with significantly higher
odds of high/intermediate-risk RS (OR, 3.478; 95% CI, 1.139–10.627;
P=0.029) compared with grade I–II. Additionally, the proportion of
high/intermediate-risk RS was significantly higher among patients
with high TOP2A gene expression compared with low
TOP2A expression (OR, 16.056; 95% CI, 1.961–131.451;
P=0.010).
| Table VI.Multivariate analysis of independent
variables associated with 21-gene recurrence score |
Table VI.
Multivariate analysis of independent
variables associated with 21-gene recurrence score
|
| High/intermediate
vs. low risk |
|
|---|
|
|
|
|
|---|
| Clinicopathological
characteristic | OR | 95% CI | P-value |
|---|
| BMI |
|
<24 | Ref |
|
|
|
≥24 | 3.590 | 1.296–9.947 | 0.014 |
| Histological
grade |
|
I–II | Ref |
|
|
|
III | 3.478 | 1.139–10.627 | 0.029 |
| Molecular type |
| Luminal
A | Ref |
|
|
| Luminal
B | 0.839 | 0.294–2.393 | 0.743 |
| TYMS | 3.865 | 0.401–37.294 | 0.242 |
| TOP2A | 16.056 | 1.961–131.451 | 0.010 |
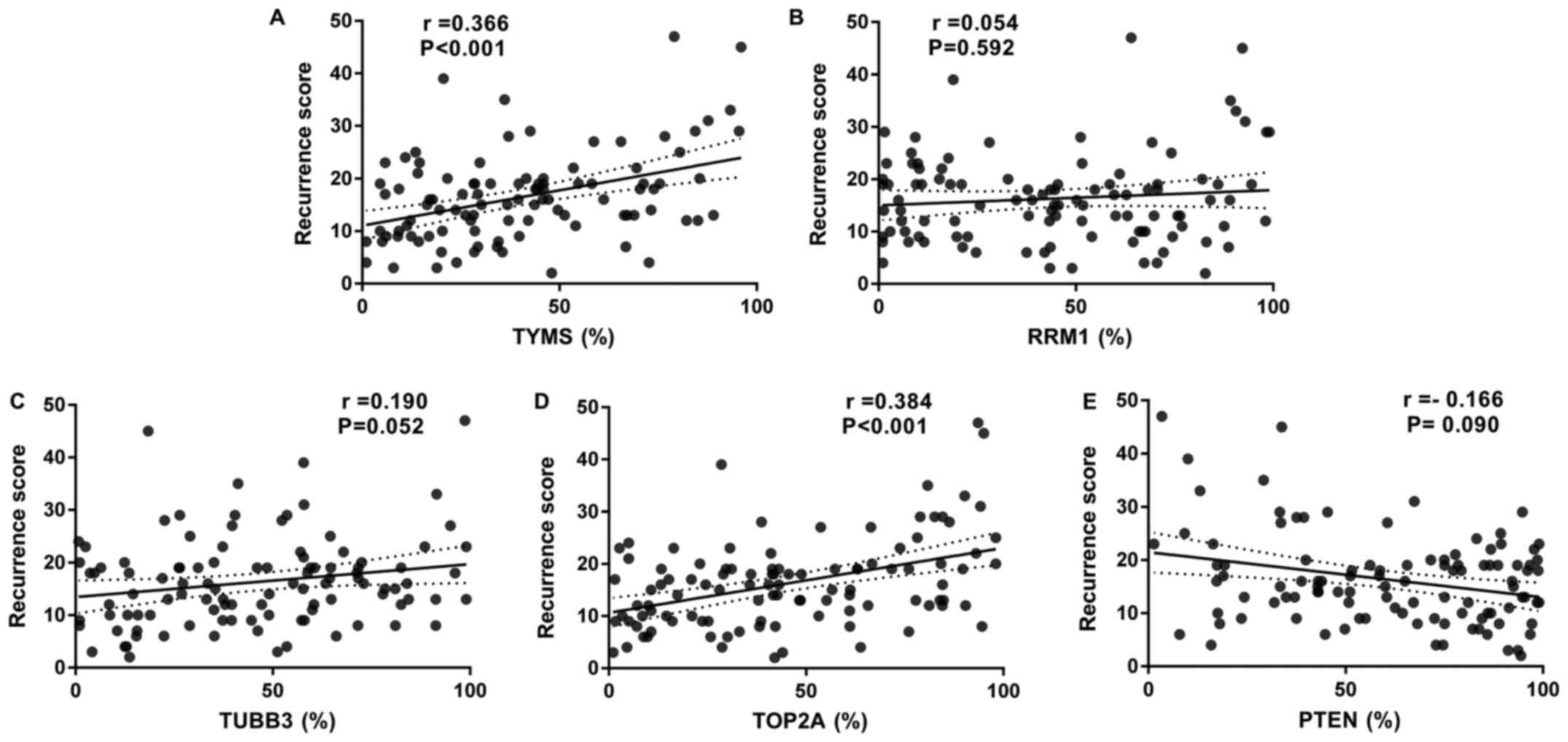
Correlation between RS and
chemotherapeutic efficacy-related target genes
The correlation between TYMS gene expression
and the RS value was determined to be statistically significant
(r=0.366; P<0.001; Fig. 3A).
Similar level of RRM1 gene expression was noted in both risk
groups (Table IV) and no
correlation was noted between RRM1 gene expression and the
RS value (P=0.592; Fig. 3B).
Although significantly higher TUBB3 gene expression was
observed in the intermediate/high-risk RS group, the absolute
difference between the two risk groups was not clinically
significant and had no correlation (P=0.052; Fig. 3C). The correlation between
TOP2A gene expression and the RS value was statistically
significant (r=0.384; P<0.001; Fig.
3D). Higher PTEN gene expression was observed in the
low-risk RS group, but there was no correlation (P=0.090; Fig. 3E).
Prognostic values of the mRNA expression levels of
chemotherapeutic efficacy-related target genes in ER+
breast cancer. Based on the correlations between RS and several of
the tested chemotherapeutic efficacy-related target genes, the
prognostic value of the mRNA expression levels of the five
chemotherapeutic efficacy-related target genes in 2,061 patients
with ER+ breast cancer was examined using a Kaplan-Meier
plotter database. Among these genes, three were associated with
relapse-free survival (RFS) for ER+ breast cancer
(Fig. 4A-E). For TYMS
(HR=1.63; 95% CI, 1.38–1.93; P<0.001; Fig. 4A), TUBB3 (HR=1.35; 95% CI,
1.15–1.59; P<0.001; Fig. 4B) and
TOP2A (HR=2.02; 95% CI, 1.71–2.39; P<0.001; Fig. 4C), higher mRNA expression levels were
associated with lower RFS in patients with ER+ breast
cancer. However, RRM1 (HR=1.13; 95% CI, 0.96–1.33; P=0.15;
Fig. 4D) and PTEN (HR=0.76;
95% CI, 0.57–1.01; P=0.061; Fig. 4E)
were not associated with RFS. The threshold values for high and low
expression levels were selected by the Kaplan-Meier plotter.
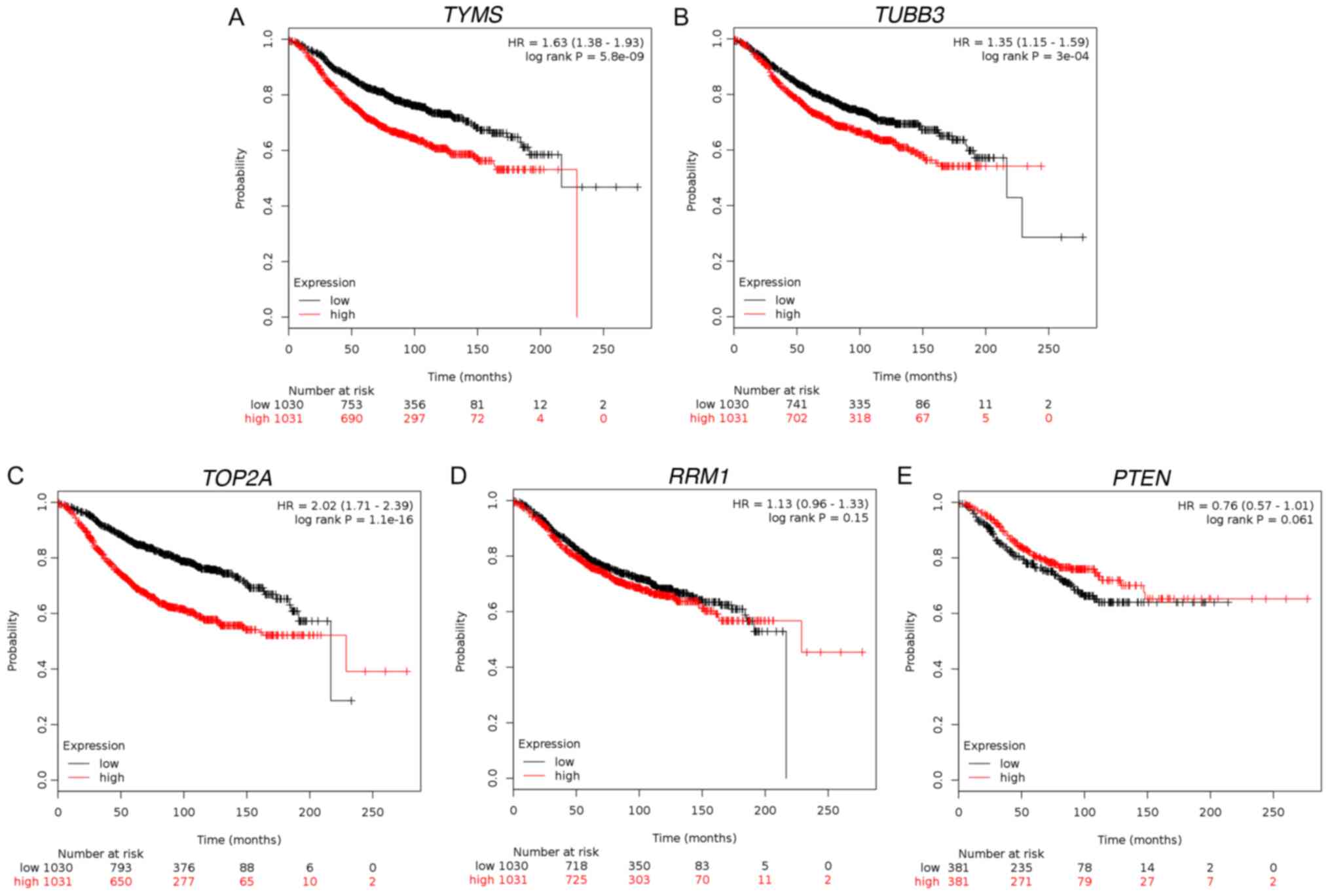 | Figure 4.Prognostic value of mRNA expression
of TYMS, RRM1, TUBB3, TOP2A and PTEN in
ER+ breast cancer. RFS curves of (A) TYMS
(Affymetrix ID: 202589_at; n=2061), (B) RRM1 (Affymetrix ID:
201477_at; n=2061), (C) TUBB3 (Affymetrix ID: 213476_x_at;
n=2061), (D) TOP2A (Affymetrix ID: 201292_at; n=2061) and
(E) PTEN (Affymetrix ID:225363_at; n=762). ER, estrogen
receptor; PTEN, phosphatase and tensin homolog; RFS,
relapse-free survival; RRM1, ribonucleotide reductase
catalytic subunit M1; RS, recurrence score; TOP2A, DNA
topoisomerase IIα; TUBB3, tubulin β3 class III; TYMS,
thymidylate synthetase. |
Changes in treatment decisions before
and after RS
The changes in doctor's treatment decision before
and after RS are presented in Table
VII. Among the patients who were classified as low risk group
and intermediate risk group, 24 (39%) and 8 (20%) patients,
respectively, were switched from adjuvant chemotherapy combined
with endocrine therapy to endocrine therapy alone following the
21-gene RS test. In contrast, in the high risk group, one
additional patient was prescribed adjuvant chemotherapy following
the 21-gene RS test. Prior to the 21-gene RS test, a total of 61
patients (55%) were recommended adjuvant chemotherapy combined with
endocrine therapy; following the 21-gene RS test, 32 patients (29%)
were treated with adjuvant endocrine therapy alone. Therefore, the
use of adjuvant chemotherapy was significantly reduced following
the 21-gene RS test (P<0.001).
| Table VII.Treatment decisions before and after
21-gene RS test. |
Table VII.
Treatment decisions before and after
21-gene RS test.
| Treatment
decisions | Low RS n=62, n
(%) | Intermediate RS
n=4, n (%) | High RS n=7, n
(%) | Total n=110, n
(%) |
|---|
| No C recommended
before RS | 34 (55) | 14 (34) | 1 (14) | 49 (45) |
| No C recommended
after RS | 34 (55) | 14 (34) | 0 (0) | 48 (44) |
| C recommended after
RS | 0
(0) | 0
(0) | 1 (14) | 1
(1) |
| C recommended
before RS | 28 (45) | 27 (66) | 6 (86) | 61 (55) |
| C recommended after
RS | 4
(6) | 19 (46) | 6 (86) | 29 (26) |
| No C recommended
after RS | 24 (39) | 8
(20) | 0 (0) | 32 (29) |
| Overall change | 24 (39) | 8
(20) | 1 (14) | 33 (30) |
Follow-up
By the end of August 2018, the median follow-up time
was 33 months. Two patients had local recurrence (their RSs were 22
and 45, respectively). One patient with an RS of 29 had recurrence
and liver metastasis. One patient with an RS of 29 had deceased.
Four patients received postoperative adjuvant chemotherapy. Three
patients (2.7%) were lost to follow-up due to change of contact
details. All other patients survived without breast cancer
recurrence or metastasis.
Discussion
In the present study, DNA liquid chip technology was
used to detect 21-gene RS and the expression profiles of
chemotherapeutic efficacy-related target genes as gene expression
did not translate or equate to protein expression of those markers
identified by IHC. This technology detected >30 genes
simultaneously without reverse transcription and polymerase chain
reaction. Therefore, the present study reflected the real-life
associations between RS and clinicopathological characteristics of
breast cancer with more clarity compared with previous studies. As
the DNA liquid chip technology had the advantages of parallel
detection, high sensitivity, simple operation and a wide linear
range, it was suitable for a number of types of samples. In
addition, it did not require RNA extraction, reverse transcription
and PCR, which reduced the multi-step error accumulation on the
results. In addition to the correlation between RS and
clinicopathological characteristics, chemotherapeutic
efficacy-related target genes were also included in the study.
In the present study, 59.1% of the patients were
classified as the low-risk RS group, which suggested that
chemotherapy may not have been beneficial to at least 59.1% of
patients examined between 2013 and 2016. Therefore, in clinical
practice, <50% of the patients may have been overtreated with
chemotherapy following surgery, resulting not only in adverse
reactions, but also increasing medical costs. Furthermore, the
present study also indicated that patients with higher BMI,
invasive ductal carcinoma type, higher histological grade and
luminal B molecular type were more likely to have higher RS.
Similarly, the National Surgical Adjuvant Breast and Bowel Project
B20 trial also found that patients with histological grade 3, T
stage 2–3 and PR-negative tumors were more likely to be categorized
as high-risk groups (14).
Correlations between low RS and non-invasive ductal carcinoma type
have also been reported (16). Owing
to the cost of 21-gene detection, the assay was only applied in
patients with ER+ early-stage breast cancer. The strong
correlation between BMI, invasive ductal carcinoma type,
histological grade, molecular type and recurrence score indicated
that the clinicopathological characteristics are also important in
the future recurrence risk prediction. Therefore, whether a model
can be built to predict the long-term recurrence risk of patients
with breast cancer who may not need or cannot afford the 21-gene RS
test was under consideration. In a study by Orucevic et al,
six clinicopathological variables of 27,719 21-gene-tested
ER+/HER2−, lymph node-negative patients with
6–50 mm tumor size acquired from the National Cancer Database
between 2010 and 2012 were assessed by logistic regression to
predict high-risk or low-risk 21-gene test results (27); the results revealed that grade and
progesterone receptor status were the highest predictors of both
low-risk and high-risk RS, followed by age, tumor size, histologic
tumor type and lymph-vascular invasion (27). The aforementioned study reported with
confidence that clinicopathological variables may be used for
prediction of low-risk or high-risk RS using nomogram models, which
may help physicians and patients decide whether further 21-gene RS
test is necessary and function as surrogates for patients for whom
21-gene RS test is not affordable or unavailable (27). Multivariate analysis in the present
study demonstrated that BMI, histological grade and TOP2A
were independent variables associated with RS. These results
suggested that the 21-gene RS effectively integrated
clinicopathological features and provided further information
regarding breast cancer. The correlations reported in the present
study indicated that traditional routine clinicopathological
characteristics may aid in the prediction of RS.
There were certain discrepancies between RS and
clinicopathological characteristics. A number of patients with risk
factors for recurrence demonstrated low RS. For example, 24.6%
(16/65) of patients with higher BMI (≥24) had RS <18. In
addition, 17.7% (11/62) of patients with histological grade III
tumors were categorized in the low-risk RS group. Therefore, the
use of one or several clinicopathological characteristics to
predict RS score may not be accurate; however, 21-gene test may
help avoid these deviations and may be more comprehensive. These
differences between RS and clinicopathological characteristics
demonstrated that the 21-gene RS may provide more accurate and
verifiable prognostic information compared with traditional
clinicopathological characteristics.
A retrospective study by Stemmer et al
demonstrated that in patients with ER+ breast cancer
with up to three positive nodes, including micrometastases, tested
using the Oncotype DX gene test, the chemotherapy use was lower
compared with untested patients (24.5 vs. 70.1%), which suggested
that Oncotype DX testing has a significant impact on reducing
chemotherapy use (28). A
retrospective analysis of a prospective designed registry, which
included 1,801 patients with ER+/HER2−, lymph
node-negative breast cancer (median follow-up, 6.2 years),
demonstrated that estimates for distant recurrence and breast
cancer mortality rate for the RS <18 patients were very low,
supporting the use of endocrine therapy alone (29). Additional findings from another study
supported the use endocrine therapy alone in patients with
ER+/HER2− breast cancer with micrometastases,
1–3 positive nodes and recurrence score <18 (30). When patients with RS 11–25 were
randomized to receive either chemotherapy or endocrine therapy, the
results revealed that chemotherapy was not more effective compared
with endocrine therapy (29). Lee
et al conducted a study of Korean breast cancer patients,
and the results demonstrated that 54.2% of the patients changed
their treatment decisions following the 21-gene test, among which
51.4% of patients switched to hormone therapy without chemotherapy
(31). Holt et al revealed
that the use of 21-gene detection had a considerable impact on
chemotherapy recommendation in early stage breast cancer (32). These data demonstrated that RS test
may be essential to avoid unnecessary chemotherapy. Similarly, the
present study revealed that for patients with hormone
receptor-positive and lymph node-negative early-stage breast
cancer, 21-gene RS test may aid to avoid excessive postoperative
adjuvant chemotherapy and lessen the side effects of chemotherapy.
The change rate of treatment decision before and after 21-gene RS
detection in China is in the top 8 in the world (UK 10%, Italy 12%,
USA 22%, Japan 26%, China 29%, Germany 30%, Spain 33% and South
Korea 51%) (31–37).
Notably, the distribution of RS according to
chemotherapeutic efficacy-related target genes was analyzed. The
detection of PTEN and other chemotherapeutic
efficacy-related target genes has been previously used to predict
the curative effect of target drugs and to inform their use to help
patients select appropriate chemotherapy drugs (21–25).
However, the data revealed that the proportion of
intermediate/high-risk RS was significantly higher among patients
with higher TYMS and TOP2A expression. TYMS
and TOP2A gene expression correlated with the RS value,
which suggested that TYMS and TOP2A gene expression
may also predict prognosis and recurrence risk in patients with
breast cancer. As the sample size of the present study was small,
these distinct gene expression profiles were further tested in
Kaplan-Meier for survival analysis. The data (n=2,061) demonstrated
that TYMS, TUBB3 and TOP2A gene expression levels
were significantly associated with RFS for ER+ breast
cancer. These results suggested that there may be more meaningful
tumor-related genes that may be used in RS classification and that
the criteria for RS categories may be worth reviewing.
The 21-gene RS test were mainly applied in patients
with ER+/HER2−, lymph node
metastasis-negative breast cancer. In the future, the scope of
application may be expanded to include patients with lymph node
metastasis into the analysis to explore the value of the RS assay
in these populations.
The 21-gene RS correlated significantly with BMI,
pathological type, histological grade, molecular grade and several
chemotherapeutic efficacy-related target genes, including
TYMS and TOP2A. These results may be used to provide
more information compared with clinicopathological indexes and
inform treatment plans. The 21-gene RS test may help avoid
excessive postoperative adjuvant chemotherapy. Large amounts of
data in the Kaplan-Meier plotter database demonstrated that
TYMS, TUBB3 and TOP2A gene expression levels were
significantly associated with RFS for ER+ breast cancer.
Therefore, TYMS, TUBB3 and TOP2A gene expression
levels may have prognostic value for ER+ breast
cancer.
Acknowledgements
The authors would like to thank the Department of
Statistics, The First Affiliated Hospital of Xi'an Jiaotong
University (Xi'an, China) for statistical support.
Funding
The study was funded by The National Natural Science
Fund of China (grant no. 81702633).
Availability of data and materials
The data generated or analyzed during this study are
included in this published article. The Kaplan-Meier used in the
present study are available at http://www.kmplot.com.
Authors' contributions
LZ and YR conceived and designed the study. LZ, BW,
KW and JH collected the data. LZ, BW and NM analyzed and
interpreted the data. CZ, YY and JH assisted in analyzing the data.
NM and YY did the follow-up of all patients. LZ, NM, BW, CZ, JH and
YY wrote the manuscript. LZ, YR, YY, JH and CZ revised the
manuscript. All authors have read and approved the final version of
this manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
The First Affiliated Hospital of Xi'an Jiaotong University (Xi'an,
China). This is a retrospective study, for which formal consent is
not required. The research (data analyses) complies with the
current laws of the country in which they were performed (The
People's Republic of China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Anderson BO and Jakesz R: Breast cancer
issues in developing countries: An overview of the Breast Health
Global Initiative. World J Surg. 32:2578–2585. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zeng H, Zheng R, Zhang S, Zou X and Chen
W: Female breast cancer statistics of 2010 in China: Estimates
based on data from 145 population-based cancer registries. J Thorac
Dis. 6:466–470. 2014.PubMed/NCBI
|
|
4
|
National Bureau of Statistics of China, .
China Statistical Yearbook, 2010. China Statistics Press; Beijing:
2010
|
|
5
|
Salek R, Shahidsales S and Mozafari V:
Changing pattern in the clinical presentation of breast cancer in
the absence of a screening program over a period of thirty-three
years in Iran. Breast. 28:95–99. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Somashekhar SP, Sepúlveda MJ, Puglielli S,
Norden AD, Shortliffe EH, Rohit Kumar C, Rauthan A, Arun Kumar N,
Patil P, Rhee K, et al: Watson for Oncology and breast cancer
treatment recommendations: Agreement with an expert
multidisciplinary tumor board. Ann Oncol. 29:418–423. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gray J and Druker B: Genomics: The breast
cancer landscape. Nature. 486:328–329. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Paik S, Shak S, Tang G, Kim C, Baker J,
Cronin M, Baehner FL, Walker MG, Watson D, Park T, et al: A
multigene assay to predict recurrence of tamoxifen-treated,
node-negative breast cancer. N Engl J Med. 351:2817–2826. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kondo M, Hoshi SL, Ishiguro H,
Yoshibayashi H and Toi M: Economic evaluation of 21-gene reverse
transcriptase-polymerase chain reaction assay in
lymph-node-negative, estrogen-receptor-positive, early-stage breast
cancer in Japan. Breast Cancer Res Treat. 112:175–187. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cronin M, Sangli C, Liu ML, Pho M, Dutta
D, Nguyen A, Jeong J, Wu J, Langone KC and Watson D: Analytical
validation of the Oncotype DX genomic diagnostic test for
recurrence prognosis and therapeutic response prediction in
node-negative, estrogen receptor-positive breast cancer. Clin Chem.
53:1084–1091. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cuzick J, Dowsett M, Pineda S, Wale C,
Salter J, Quinn E, Zabaglo L, Mallon E, Green AR, Ellis IO, et al:
Prognostic value of a combined estrogen receptor, progesterone
receptor, Ki-67, and human epidermal growth factor receptor 2
immunohistochemical score and comparison with the Genomic Health
recurrence score in early breast cancer. J Clin Oncol.
29:4273–4278. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Harris L, Fritsche H, Mennel R, Norton L,
Ravdin P, Taube S, Somerfield MR, Hayes DF and Bast RC Jr; American
Society of Clinical Oncology, : American Society of Clinical
Oncology 2007 update of recommendations for the use of tumor
markers in breast cancer. J Clin Oncol. 25:5287–5312. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Győrffy B, Hatzis C, Sanft T, Hofstatter
E, Aktas B and Pusztai L: Multigene prognostic tests in breast
cancer: Past, present, future. Breast Cancer Res. 17:112015.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Paik S, Tang G, Shak S, Kim C, Baker J,
Kim W, Cronin M, Baehner FL, Watson D, Bryant J, et al: Gene
expression and benefit of chemotherapy in women with node-negative,
estrogen receptor-positive breast cancer. J Clin Oncol.
24:3726–3734. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Paik S: Development and clinical utility
of a 21-gene recurrence score prognostic assay in patients with
early breast cancer treated with tamoxifen. Oncologist. 12:631–635.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wolf I, Ben-Baruch N, Shapira-Frommer R,
Rizel S, Goldberg H, Yaal-Hahoshen N, Klein B, Geffen DB and
Kaufman B: Association between standard clinical and pathologic
characteristics and the 21-gene recurrence score in breast cancer
patients: A population-based study. Cancer. 112:731–736. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Albain KS, Barlow WE, Shak S, Hortobagyi
GN, Livingston RB, Yeh IT, Ravdin P, Bugarini R, Baehner FL,
Davidson NE, et al Breast Cancer Intergroup of North America, :
Prognostic and predictive value of the 21-gene recurrence score
assay in postmenopausal women with node-positive,
oestrogen-receptor-positive breast cancer on chemotherapy: A
retrospective analysis of a randomised trial. Lancet Oncol.
11:55–65. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: The Eighth Edition AJCC Cancer Staging Manual:
Continuing to build a bridge from a population-based to a more
‘personalized’ approach to cancer staging. CA Cancer J Clin.
67:93–99. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Goldhirsch A, Winer EP, Coates AS, Gelber
RD, Piccart-Gebhart M, Thürlimann B, Senn HJ, Albain KS, André F,
Bergh J, et al Panel members, : Personalizing the treatment of
women with early breast cancer: Highlights of the St Gallen
International Expert Consensus on the Primary Therapy of Early
Breast Cancer 2013. Ann Oncol. 24:2206–2223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tsunoda Y, Suzuki K, Tsunoda A, Takimoto M
and Kusano M: Evaluation of 5-fluorouracil related genes in breast
cancer to predict the effect of adjuvant therapy with oral
fluorouracil derivatives. Oncol Rep. 23:771–777. 2010.PubMed/NCBI
|
|
21
|
Yu Z, Sun J, Zhen J, Zhang Q and Yang Q:
Thymidylate synthase predicts for clinical outcome in invasive
breast cancer. Histol Histopathol. 20:871–878. 2005.PubMed/NCBI
|
|
22
|
Metro G, Zheng Z, Fabi A, Schell M,
Antoniani B, Mottolese M, Monteiro AN, Vici P, Lara Rivera S,
Boulware D, et al: In situ protein expression of RRM1, ERCC1, and
BRCA1 in metastatic breast cancer patients treated with
gemcitabine-based chemotherapy. Cancer Invest. 28:172–180. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Galmarini CM, Treilleux I, Cardoso F,
Bernard-Marty C, Durbecq V, Gancberg D, Bissery MC, Paesmans M,
Larsimont D, Piccart MJ, et al: Class III beta-tubulin isotype
predicts response in advanced breast cancer patients randomly
treated either with single-agent doxorubicin or docetaxel. Clin
Cancer Res. 14:4511–4516. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nitiss JL: Targeting DNA topoisomerase II
in cancer chemotherapy. Nat Rev Cancer. 9:338–350. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Braybrooke JP, Levitt NC, Joel S, Davis T,
Madhusudan S, Turley H, Wilner S, Harris AL and Talbot DC:
Pharmacokinetic study of cisplatin and infusional etoposide
phosphate in advanced breast cancer with correlation of response to
topoisomerase IIalpha expression. Clin Cancer Res. 9:4682–4688.
2003.PubMed/NCBI
|
|
26
|
Lánczky A, Nagy Á, Bottai G, Munkácsy G,
Szabó A, Santarpia L and Győrffy B: miRpower: A web-tool to
validate survival-associated miRNAs utilizing expression data from
2178 breast cancer patients. Breast Cancer Res Treat. 160:439–446.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Orucevic A, Bell JL, McNabb AP and Heidel
RE: Oncotype DX breast cancer recurrence score can be predicted
with a novel nomogram using clinicopathologic data. Breast Cancer
Res Treat. 163:51–61. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Stemmer SM, Klang SH, Ben-Baruch N, Geffen
DB, Steiner M, Soussan-Gutman L, Merling S, Svedman C, Rizel S and
Lieberman N: The impact of the 21-gene Recurrence Score assay on
clinical decision-making in node-positive (up to 3 positive nodes)
estrogen receptor-positive breast cancer patients. Breast Cancer
Res Treat. 140:83–92. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Stemmer SM, Steiner M, Rizel S,
Soussan-Gutman L, Ben-Baruch N, Bareket-Samish A, Geffen DB,
Nisenbaum B, Isaacs K, Fried G, et al: Clinical outcomes in
patients with node-negative breast cancer treated based on the
recurrence score results: Evidence from a large prospectively
designed registry. NPJ Breast Cancer. 3:332017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Stemmer SM, Steiner M, Rizel S, Geffen DB,
Nisenbaum B, Peretz T, Soussan-Gutman L, Bareket-Samish A, Isaacs
K, Rosengarten O, et al: Clinical outcomes in ER+ HER2
-node-positive breast cancer patients who were treated according to
the Recurrence Score results: Evidence from a large prospectively
designed registry. NPJ Breast Cancer. 3:322017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lee MH, Han W, Lee JE, Kim KS, Park H, Kim
J, Bae SY, Shin HJ, Lee JW and Lee ES: The clinical impact of
21-gene recurrence score on treatment decisions for patients with
hormone receptor-positive early breast cancer in Korea. Cancer Res
Treat. 47:208–214. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Holt S, Bertelli G, Humphreys I, Valentine
W, Durrani S, Pudney D, Rolles M, Moe M, Khawaja S, Sharaiha Y, et
al: A decision impact, decision conflict and economic assessment of
routine Oncotype DX testing of 146 women with node-negative or
pNImi, ER-positive breast cancer in the U.K. Br J Cancer.
108:2250–2258. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lo SS, Mumby PB, Norton J, Rychlik K,
Smerage J, Kash J, Chew HK, Gaynor ER, Hayes DF, Epstein A, et al:
Prospective multicenter study of the impact of the 21-gene
recurrence score assay on medical oncologist and patient adjuvant
breast cancer treatment selection. J Clin Oncol. 28:1671–1676.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Martínez Del Prado P, Alvarez-López I,
Domínguez-Fernández S, Plazaola A, Ibarrondo O, Galve-Calvo E,
Ancizar-Lizarraga N, Gutierrez-Toribio M, Lahuerta-Martínez A and
Mar J: Clinical and economic impact of the 21-gene recurrence score
assay in adjuvant therapy decision making in patients with
early-stage breast cancer: Pooled analysis in 4 Basque Country
university hospitals. Clinicoecon Outcomes Res. 10:189–199. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Dieci MV, Guarneri V, Giarratano T, Mion
M, Tortora G, De Rossi C, Gori S, Oliani C, Merlini L, Pasini F, et
al: First prospective nulticenter Italian study on the impact of
the 21-gene recurrence score in adjuvant clinical decisions for
patients with ER positive/HER2 negative breast cancer. Oncologist.
23:297–305. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yamauchi H, Nakagawa C, Takei H, Chao C,
Yoshizawa C, Yagata H, Yoshida A, Hayashi N, Hell S and Nakamura S:
Prospective study of the effect of the 21-gene assay on adjuvant
clinical decision-making in Japanese women with estrogen
receptor-positive, node-negative, and node-positive breast cancer.
Clin Breast Cancer. 14:191–197. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Eiermann W, Rezai M, Kümmel S, Kühn T,
Warm M, Friedrichs K, Schneeweiss A, Markmann S, Eggemann H,
Hilfrich J, et al: The 21-gene recurrence score assay impacts
adjuvant therapy recommendations for ER-positive, node-negative and
node-positive early breast cancer resulting in a risk-adapted
change in chemotherapy use. Ann Oncol. 24:618–624. 2013. View Article : Google Scholar : PubMed/NCBI
|