Introduction
Esophageal cancer (EC) is a malignant tumor on the
esophageal mucosa at the location of pathogenesis. It is one of the
most common digestive tract tumors, very common in most countries
and regions around the world, with a high mortality rate (1). The main clinical symptoms of EC are
pain, shortness of breath, cough, weight loss, and sometimes
patients may experience nausea, diarrhea and satiety (2). The incidence rates of EC has increased
over the years. It is a type of malignant tumor with fast growth
and high incidence. Also the five-year survival rate is only ~13%.
It is predicted that the incidence of EC adenocarcinoma will
increase 40–50% by 2026 (3). EC is
the most common digestive tract tumor, and has the 7th highest
mortality rate among all cancers in the world (4). The main reason for the high mortality
rate is that most patients are already in the advanced stage at the
time of diagnosis, missing the opportunity for surgery (5). In order to improve the prognosis of
patients with EC, chemotherapy is often used for the treatment of
cancer to achieve a reduction of the diameter of the tumor.
However, chemotherapy with concurrent radiotherapy will increase
the level of drug toxicity and other toxic side effects. This can
even lead to delayed surgery time of EC patients who are not
sensitive to chemotherapy and concurrent radiotherapy, which
further causes delayed treatment (6). Studies have shown that early EC has no
lymph node metastasis and no vascular infiltration, the five-year
survival rate of patients is generally high, 60–70%, with a good
prognosis (7). This shows that early
detection and early diagnosis of EC can improve the survival rate
of EC patients and increase the effectiveness of treatment, it has
an important significance in EC patients.
In order to diagnose EC as early as possible,
endoscopic biopsy is often used in high-risk patients for
diagnosis. However, this method is prone to sampling errors and the
accuracy of the method is also affected by the tester at the same
time (8). In recent years, the
diagnosis of EC tissue tumor markers related to gene and cell
abnormalities has also attracted the attention of the many medical
scientists. However, due to the limitations of current medical
technology, changes in EC tumor markers are difficult to detect in
the early stages of cancers, and are of little significance in the
diagnosis of early EC (9).
Identification of an early EC diagnostic method with higher
accuracy and more convenience has become a hot topic in EC
research.
Narrow Band Imaging (NBI) is an advanced endoscopic
technique. Compared to conventional white endoscopy, NBI technology
uses selective filtering of light, focuses light on the mucous
membrane surface and provides reliable sensing performance for
tissue biopsy (10). NBI is formed
by the three narrow-band light waves of green and blue with
wavelengths of 540 and 415 nm. Visually enhancing the affected area
with light sources of different wavelengths, is more convenient in
the application of qualitative and targeted biopsy on the lesion
(11). NBI, which has been widely
used, is easy to operate, with no dye agent required under the
endoscope, it has a similar imaging effect to white light stained
endoscope. Compared to white light staining endoscopy, it has a
better NBI detection, and the false positive detection rate is
similar to white light staining endoscopy (12).
This study examined the status of early EC and
benign lesions by using NBI, the value of NBI in the diagnosis of
early EC and benign lesions were analyzed, to provide evidence for
clinics.
Materials and methods
General information
Retrospective analysis was carried out on the
clinical data of 186 patients with early EC and benign lesions
diagnosed by the Department of Gastroenterology in Cangzhou Central
Hospital (Cangzhou, China) from February 2011 to April 2018. Among
them, 102 patients examined using NBI were regarded as the research
group, including 65 cases of males, 37 cases of females, with an
average age of 50.23±15.93 years. Eighty-four patients examined by
conventional white light staining endoscopy were regarded as the
control group, including 54 cases of males, 30 cases of females,
with an average age of 52.31±16.73 years. All patients voluntarily
accepted the necessary examinations, and all of them had signed the
informed consent form. The study was approved by the Ethics
Committee of Cangzhou Central Hospital.
Inclusion and exclusion criteria
Inclusion criteria
Age ≥18 years; the red and gray color appeared in
the area of esophageal and hypopharyngeal mucosa; the surface of
the esophagus and hypopharynx mucosa is not smooth, matte, or
accompanied by erosion; the mucosa of the esophagus and hypopharynx
was thickened, and the structure of the vascular network was
blurred or disappeared; and patients with complete clinical medical
records.
Exclusion criteria
Suffering from acute pharyngeal infection; patients
with iodine allergy or have had a history of hyperthyroidism;
patients cannot perform painless gastroscope operation for special
reasons; and the esophagus and hypopharyngeal mucosa were still
unclear after washing.
Experimental equipment
Gastroscope host (model: CV-260SL); HD electronic
magnifying endoscope (model: GIF-H260); light source (model:
CLV-260) (all from Olympus Japan Ltd., Tokyo, Japan); Rugo's iodine
solution (code: G1069; Beijing Suo Laibao Technology Co., Ltd.,
Beijing, China); simethicone (National Pharmacy: H20170002; Nanjing
Hanstone Pharmaceutical Co., Ltd., Nanjing, China); 2% lidocaine
gel (National Pharmaceutical code: H11022396; China Resources Zizhu
Pharmaceutical Co., Ltd., Beijing, China); butyl bromide
scopolamine injection (national medicine quasi-font: H32023810;
Jiangsu Ange Pharmaceutical Co., Ltd., Jiangsu, China); endoscopic
mist spray tube (model: AF-2416PB; Olympus Japan Ltd.) were used in
the present study. Dual system endoscope was used in this study,
and regular white endoscopy can be performed. The system was
switched to NBI mode for detection where necessary.
Method of detection
Preparation before detection
Before endoscopy, the patient was examined for blood
routine, liver and kidney function, chest CT, and coagulation
function, to ensure that endoscopic contraindications were
excluded. On the day of endoscopy, patients were inhibited for
drinking water and fasted for 10 h. Patients' blood pressure and
electrocardiogram were checked 60 min before the detection. If
there was no abnormality, patients took 30 ml of defoamer
simethicone and 1,000 ml of distilled water 30 min before the
detection in order to remove mucus and air bubbles from the
detection area, improve the vision and increase the disease
detection rate. Five minutes before the examination, patients were
given 2% of lidocaine gel for local pharyngeal anesthesia, the head
was placed in the back position and the drug kept in full contact
with the pharynx, an intravenous channel was established after
anesthesia, and intravenous injection of butyl bromide was used to
reduce gastrointestinal motility.
Detection process
The patient lay on the left side, leaning forward
and bending the legs inward. The research group was examined by
ordinary white light endoscopy. Then the presence of lesions was
carefully observed in the esophagus to the duodenum, the lesions
were rinsed, switching to NBI mode for detection. The clarity was
judged by observing the suspected lesion area, the lesion location,
size, edge, morphology, extent and mucosal characteristics were
recorded. Also the control group was examined by conventional white
light staining, the endoscopic mist spray tube was used to evenly
spray the Rugo's iodine solution to the detection area. The clarity
was judged by making the coloration contrast of the detection area
clearer, and the lesion location, size, edge, shape, extent and
mucosal characteristics were recorded. After the above operation
was completed, the two groups received two biopsies from the most
suspicious lesions under endoscopy, which were sent for condition
detection of the lesions.
Experimental evaluation criteria
Assessment of the clarity of lesion
boundary
Clear: The extent of the lesion is very clear, and
the boundary between the lesion and the normal tissue is clearly
defined. Blurry: The lesion range is unclear and the lesion
boundary is sticky with normal tissue. Pathological clarity of the
lesion = number of people with cleared clarity/total number of
people.
Evaluation of image clarity
1-point, blurred image; 2-points, faintly visible
image; 3-points, visible image; 4-points, clearly visible
image.
Diagnostic criteria
The research group used the NBI magnifying lens to
observe the intrappillary capillary loop (IPCL) on the lesion area.
The IPCL changes are classified into 4 types according to Swangsri
et al (13) standard: Type 1,
the capillaries in the papillary are in the shape of regularly
arranged thin ring. Type 2, the capillaries in the papillary are in
the shape of regularly arranged thin ring, however, it can be seen
that the pipe diameter is enlarged or extended. Type 3, destroyed
shape of capillaries in the papillary, uneven diameter size,
irregularly arranged and even appeared in a shape of a bended
snake. Type 4, destroyed capillaries in the papillary, blood
vascular appeared in an overlapped distribution, new tumor blood
vessels appeared and have irregular branches. Type 1 is considered
as normal esophageal mucosa; type 2 is considered to be a benign
lesion of the esophagus; type 3 and 4 is considered as EC; types 1
and 2 are classified as negative pathology and type 3 and 4 are
classified as positive pathology.
After the control group was stained with Rugo's
iodine solution, the stain appeared brown, light brown or no color.
Brown is an indication of normal esophageal mucosa, light brown
indicates benign lesion of the esophagus and no color indicates EC
(14). Brown and light brown were
considered as a negative case, and no color was considered as a
positive case.
Assessment of diagnostic results
Extract analysis of four tables of diagnostic
experiments, sensitivity calculation, specificity levels, positive
diagnostic and negative predictive value and diagnostic compliance
rate.
Nursing care after detection
After the detection, patients were sent to the
recovery room. Monitoring of the patient's vital signs was
continued until the patient had vomiting reflexes and pharyngeal
sensation recovery. Adverse reactions such as vomiting and
gastrointestinal bleeding in the patient were observed and recorded
within 1 h after the examination. Patients were left alone when
they had the ability to swallow.
Statistical analysis
Statistical analysis was performed using SPSS 17.0
(Beijing Sitron Weida Information Technology Co., Ltd., Beijing,
China). Countable data was expressed as a percentage, and
measurement data were expressed as mean ± standard deviation (means
± SD). The Chi-square test was used to compare countable data
between groups and t-test was used to compare the measurement data
between groups. The rank sum test was used to analyze the grade
data, expressed as Z. P<0.05, was considered as statistically
significant.
Results
Comparison of general baseline
data
The age, sex, body mass index, heart rate, smoking
status, fasting blood glucose level, hemoglobin (Hb) value, red
blood cell (RBC) value, platelet (PLT) value, and alcoholism were
compared between the research group and the control group. The
difference between two groups was not statistically significant
(P>0.05) (Table I).
 | Table I.Comparison of general baseline data
between the research group and the control group [n (%)] (mean ±
SD). |
Table I.
Comparison of general baseline data
between the research group and the control group [n (%)] (mean ±
SD).
| Types | Research group
(n=102) | Control group
(n=84) | χ2/T | P-value |
|---|
| Age (years) | 50.23±15.93 | 52.31±16.73 | 0.866 | 0.387 |
| Sex |
|
| 0.065 | 0.879 |
| Male | 65 (63.73) | 52 (61.90) |
|
|
|
Female | 37 (36.27) | 32 (38.10) |
|
|
| BMI
(kg/m2) |
|
| 0.060 | 0.850 |
|
<24 | 84 (82.35) | 68 (80.95) |
|
|
| ≥24 | 18 (17.65) | 16 (19.05) |
|
|
| Heart rate
(times/min) |
|
| 0.941 | 0.411 |
|
<60 | 13 (12.75) | 15 (17.86) |
|
|
| ≥60 | 89 (87.25) | 69 (82.14) |
|
|
| Smoking status |
|
| 0.125 | 0.762 |
|
Smoking | 63 (61.76) | 54 (64.29) |
|
|
|
Non-smoking | 39 (38.24) | 30 (35.71) |
|
|
| Fasting blood sugar
(mmol/l) | 4.81±0.72 | 4.68±0.58 | 1.336 | 0.183 |
| Hb (g/l) | 121.48±17.27 | 125.93±14.71 | 1.868 | 0.063 |
| RBC
(×1012/l) | 4.48±0.46 | 4.53±0.41 | 0.775 | 0.440 |
| PLT
(×109/l) | 224.82±56.16 | 226.35±54.26 | 0.188 | 0.851 |
| Alcoholism |
|
| 0.033 | 0.883 |
|
Alcoholic | 56 (54.90) | 45 (53.57) |
|
|
| Non-alcoholic | 46 (45.10) | 39 (46.43) |
|
|
Comparison of clarity between the
research group and the control group
Comparison of the boundary definition
between the research group and the control group
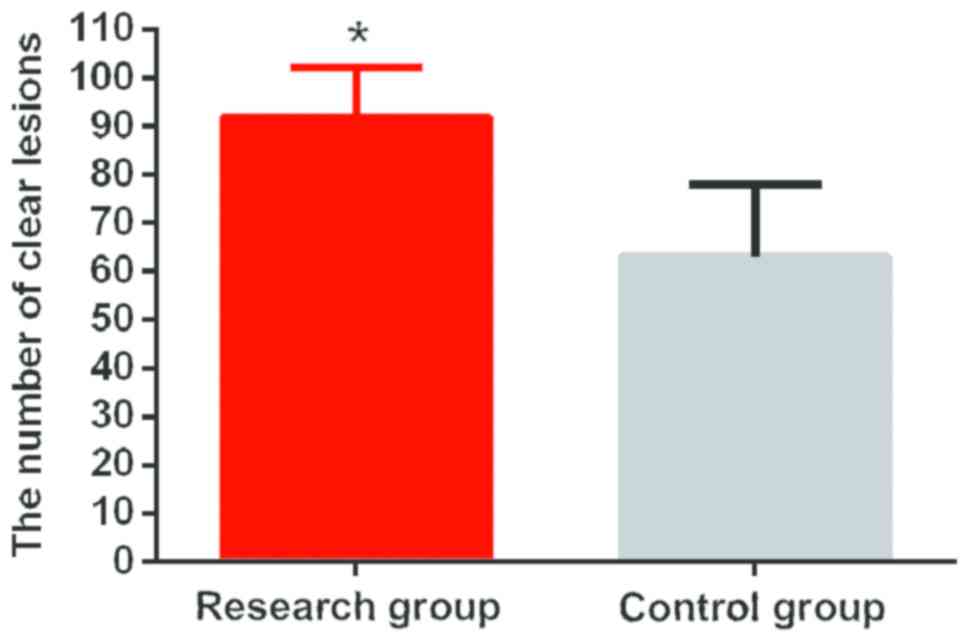
According to the result of images in both groups
under NBI endoscopy and ordinary white light staining endoscopy, in
the research group, there were 92 cases of cleared lesions and 10
blurred cases and the boundary definition of the lesion was 90.20%.
In the control group, there were 63 cases of clear lesions, 21
blurred cases and the boundary definition of the lesion was 75.00%.
The lesion boundary definition in the research group was higher
than that in the control group, and the difference between the two
groups was statistically significant (t=7.659, P<0.01) (Fig. 1).
Image clarity between the research
group and the control group
According to the results of imaging in both groups
under NBI endoscopy and ordinary white light staining endoscopy,
the image clarity in the research group was classified into 4
points, 3 points, 2 points and 1 point, each had 74 cases, 20
cases, 6 cases and 2 cases, respectively. The image clarity in the
control group was classified as 4 points, 3 points, 2 points and 1
point, each had 36 cases, 27 cases, 13 cases and 8 cases,
respectively. The image clarity in the research group was higher
than that in the control group, and the difference was
statistically significant (t=16.806, P<0.01). The 3 points, 2
points, and 1 point of image clarity in the research group were
lower than those in the control group. By contrast the 4 points was
higher than that of the control group. The difference was
statistically significant (P<0.05) (Table II).
| Table II.Comparison of the image clarity
between the research group and the control group. |
Table II.
Comparison of the image clarity
between the research group and the control group.
| Types | 1 point | 2 points | 3 points | 4 points | Z | P-value |
|---|
| The research group
(n=102) | 2 (1.96) | 6 (5.88) | 20 (19.61) | 74 (72.55) | −4.303 | <0.001 |
| The control group
(n=84) | 8 (9.52) | 13 (15.48) | 27 (32.14) | 36 (42.86) |
|
|
Detection of lesions between the
research group and the control group
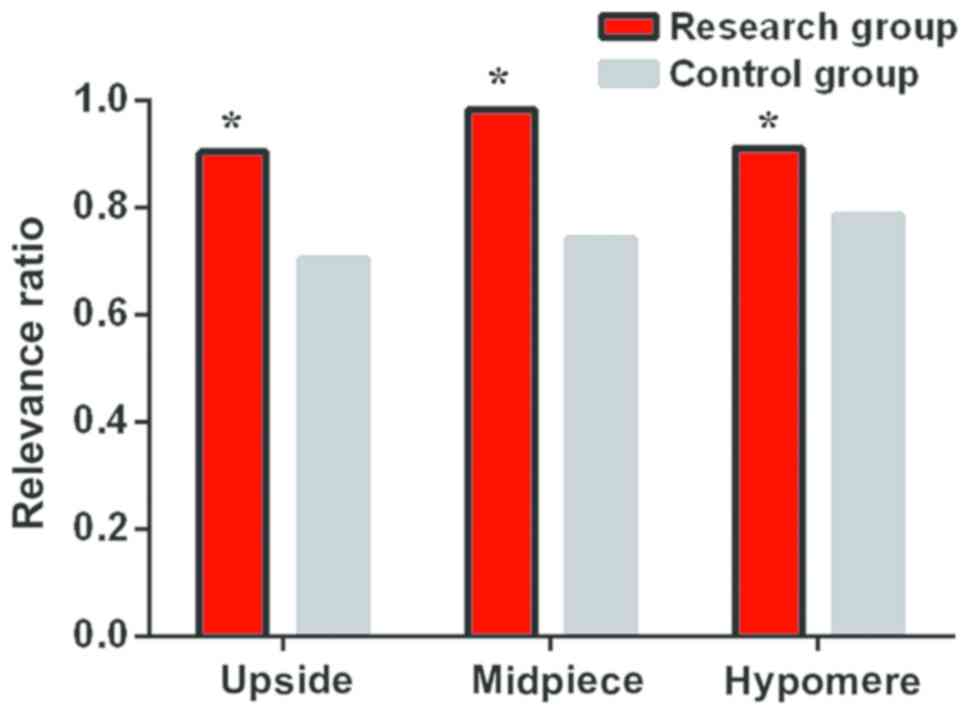
According to the results of histopathological
examination, in the study group, there were 21 cases of lesions in
the upper segment, 47 cases in the middle segment and 34 cases in
the lower segment. In the NBI test results of the research group,
there were 19 cases in the upper segment and the detection rate was
90.48%, 43 cases in the middle segment with a detection rate of
91.49%, 31 cases in the lower segment with a detection rate of
91.18. In the control group, there were 17 cases of lesions in the
upper segment, 39 cases in the middle segment and 28 cases in the
lower segment. In the results of white light staining endoscopy of
the control group, there were 12 cases in the upper segment with a
detection rate of 70.59%, 29 cases in the middle segment with a
detection rate of 74.36%, 22 cases in the lower segment with a
detection rate of 78.57%. The detection rate of the upper, middle
and lower lesions in the research group was higher than that in the
control group (Fig. 2).
Detection of early EC and precancerous
lesions between the research group and the control group
According to the results of the detection report
between the groups, the sensitivity, specificity, positive
predictive value, negative predictive value, and diagnostic
compliance rate in the research group were higher than those in the
control group, and the difference was statistically significant
(P<0.05) (Table III).
| Table III.Comparison of detection of early EC
and precancerous lesions between the research group and the control
group [n (%)]. |
Table III.
Comparison of detection of early EC
and precancerous lesions between the research group and the control
group [n (%)].
|
| Pathological
diagnosis | Diagnostic result
(%) |
|---|
|
|
|
|
|---|
|
| Positive | Negative | Sensitivity | Negative
predictiveSpecificity | Positive predictive
value | Diagnostic
value | compliance
rate |
|---|
| The research group
(n=102) |
|
| 91.57 | 84.21 | 96.20 | 69.57 | 90.20 |
|
Positive | 76 | 3 |
|
|
|
|
|
|
Negative | 7 | 16 |
|
|
|
|
|
| The control group
(n=84) |
|
| 69.23 | 26.32 | 76.27 | 20.00 | 59.52 |
| Positive | 45 | 14 |
|
|
|
|
|
| Negative | 20 | 5 |
|
|
|
|
|
| χ2
test |
|
| 12.193 | 12.880 | 12.422 | 11.959 | 23.996 |
| P-value |
|
| <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
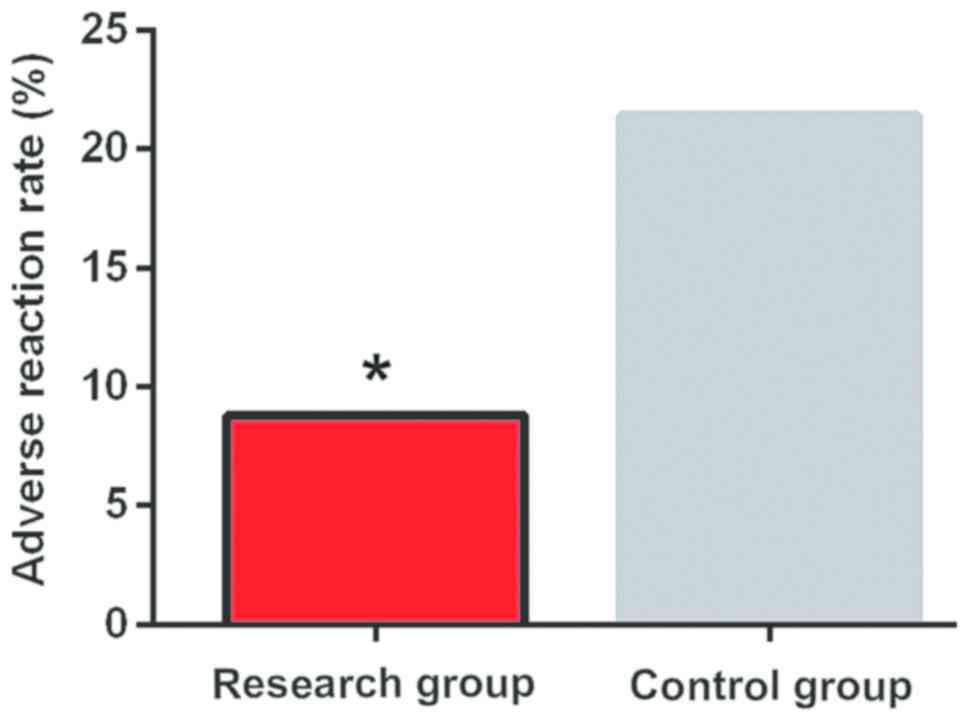
Incidence of adverse reactions after
the detection between the research group and the control group
According to the observations within 1 h between two
groups after the detection, in the research group, there were 9
cases of adverse reactions such as vomiting and gastrointestinal
bleeding, with an adverse reaction rate of 8.82%. There were 18
cases in the control group, with an adverse reaction rate of
21.43%. The incidence of adverse reactions in the research group
was better than that in the control group. The difference between
the groups was statistically significant (t=5.898, P=0.021)
(Fig. 3).
Discussion
EC is a very common malignant tumor with high
incidence rate, the pathogenesis is currently unclear, however, it
has been shown to be associated with genetic changes, such as
keratinocyte 7 and keratinocyte 20 (15). Studies have shown that due to the
complicated lymphatic system of esophagus, transverse longitudinal
connection and complicated pattern of lymph node metastasis, it has
become one of the most important factors affecting the prognosis of
EC. Particularly, long-term prognosis is affected by the number of
invaded lymph nodes (16). EC has a
slow development, with many steps and has been divided into
multiple stages. Early EC occurs only in the esophageal mucosa or
in the superficial layer of the esophagus. It can be cured with
endoscopic treatment, and the curative effect is equivalent to the
surgery effect. Also patients have less pain, less trauma and
faster recovery rate, according to statistics, the five-year
survival rate of patients is equivalent to surgery, the diagnosis
of early EC has a great significance for the treatment of EC
(17).
White light staining endoscopy is one of the
commonly used diagnostic methods for EC. However, the
microstructure of esophageal mucosa in this method is poorly
displayed, also the early EC and esophageal proximal lesions are
often missed, EC patients are easily misdiagnosed as benign
esophageal ulcers and the miss diagnosis rate is as high as 7.866%
(18). With the development of
endoscopy, Olympus Japan Ltd. has developed a new type of
magnifying endoscope system: NBI, a very effective non-invasive
diagnostic tool with high value for the diagnosis of early cancer
(19). The NBI endoscope system uses
415 and 540 nm narrow band illumination through the NBI filter, no
requirement for separate staining, easy to operate and has a high
accuracy in the diagnosis of EC (20).
The present study found that the lesion boundary
definition of NBI endoscopy was higher than that of the ordinary
white staining endoscopy (P<0.05). The image clarity of NBI
endoscopy was higher than that of the ordinary white staining
endoscopy (P<0.05). According to the results of Gono et
al (21), compared with ordinary
white stained endoscopy; the NBI endoscopic EC patients have
clearer capillaries in the epithelial and mucosal layers. This is
similar to our research results, so it indicates that the NBI
endoscopy has a higher clarity, which is conducive to accurate
judgment of the lesion. This study also found that the sensitivity,
specificity, positive predictive value, negative predictive value
and diagnostic coincidence rate of NBI endoscopy in the diagnosis
of early EC and benign lesions were higher than those of the
ordinary white light staining endoscopy (P<0.05). The detection
rates of the upper, middle and lower segments of NBI endoscopic
lesions were higher than those of the white light stained
endoscopy. Ide et al (22),
reported similar results to the present study, and considered that
NBI technology has higher sensitivity and negative predictive value
for early squamous cell EC patients. Compared with conventional
white light staining endoscope, the differences were comparable,
the results showed that NBI has a higher value in the diagnosis of
EC. The occurrence of adverse reactions were further compared after
examination of the patients, the result showed that the incidence
of adverse reactions after NBI endoscopy was lower than the
conventional white light staining (P<0.05). We believe that the
high adverse reaction rates after conventional white light staining
endoscopy may be related to the Rugo's iodine solution used in the
examination. From the study of Matuszczyk et al (23), it was found that a man was induced by
iodine, and caused hyperthyroidism, arrhythmia and angina pectoris.
This indicates that iodine has a certain negative impact on the
human body.
Overall, the NBI endoscopes are clearer compared
with ordinary stained endoscopes, it has a higher levels of
sensitivity, specificity, positive predictive value, negative
predictive value and diagnostic coincidence rate for early
diagnosis of EC and benign lesions. Also it has a more accurate
detection rate of lesions and less occurrence of adverse reactions.
It can effectively detect and screen early EC and benign lesions,
it is worth promoting clinically.
Acknowledgements
Not applicable.
Funding
This study was supported by Science and Technology
Project of Cangzhou City, Hebei Province (no. 151302139).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZS, LW and SW were responsible for evaluation of
image clarity. ZS and XW collected and analyzed general data of
patients. YK and WW worked on judgment of the clarity of lesion
boundary. RG and XS helped with statistical analysis. The final
version was read and adopted by all the authors.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Cangzhou Central Hospital (Cangzhou, China). Signed informed
consents were obtained from the patients or the guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jain S and Dhingra S: Pathology of
esophageal cancer and Barrett's esophagus. Ann Cardiothorac Surg.
6:99–109. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ginex P, Thom B, Jingeleski M, Vincent A,
Plourde G, Rizk N, Rusch VW and Bains M: Patterns of symptoms
following surgery for esophageal cancer. Oncol Nurs Forum.
40:E101–E107. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Otterstatter MC, Brierley JD, De P,
Ellison LF, Macintyre M, Marrett LD, Semenciw R and Weir HK:
Esophageal cancer in Canada: Trends according to morphology and
anatomical location. Can J Gastroenterol. 26:723–727. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Spallone A and Izzo C: Esophageal cancer
presenting as a brain metastasis: A case report. Oncol Lett.
6:722–724. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wu SX and Wang LH: Current status and
perspectives of radiotherapy for esophageal cancer. Zhonghua Zhong
Liu Za Zhi. 38:650–654. 2016.(In Chinese). PubMed/NCBI
|
|
6
|
Huang FL and Yu SJ: Esophageal cancer:
Risk factors, genetic association, and treatment. Asian J Surg.
41:210–215. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang WP, Yang YS, He SL and Chen LQ:
Discussion of N staging category of the eighth edition of The AJCC
Esophageal Cancer Staging System. Zhonghua Wai Ke Za Zhi.
55:894–897. 2017.(In Chinese). PubMed/NCBI
|
|
8
|
Becker V, Bobardt J, Ott R, Rösch T and
Meining A: Long-term follow-up in patients with indeterminate
Barrett esophagus. Digestion. 88:161–164. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shah AK, Saunders NA, Barbour AP and Hill
MM: Early diagnostic biomarkers for esophageal adenocarcinoma - the
current state of play. Cancer Epidemiol Biomarkers Prev.
22:1185–1209. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Machida H, Sano Y, Hamamoto Y, Muto M,
Kozu T, Tajiri H and Yoshida S: Narrow-band imaging in the
diagnosis of colorectal mucosal lesions: A pilot study. Endoscopy.
36:1094–1098. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ladabaum U, Fioritto A, Mitani A, Desai M,
Kim JP, Rex DK, Imperiale T and Gunaratnam N: Real-time optical
biopsy of colon polyps with narrow band imaging in community
practice does not yet meet key thresholds for clinical decisions.
Gastroenterology. 144:81–91. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen G, Wang B, Li H, Ma X, Shi T and
Zhang X: Applying narrow-band imaging in complement with
white-light imaging cystoscopy in the detection of urothelial
carcinoma of the bladder. Urol Oncol. 31:475–479. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Swangsri J, Nakajima Y, Kawada K, Tokairin
Y, Suzuki T, Miyawaki Y, Hoshino A, Okada T, Ota S, Ryotokuji T, et
al: Changes in the microvascular structure of mucosal squamous cell
carcinoma of the esophagus and their significance in tumor
progression. J Med Dent Sci. 60:83–91. 2014.PubMed/NCBI
|
|
14
|
Dawsey SM, Fleischer DE, Wang GQ, Zhou B,
Kidwell JA, Lu N, Lewin KJ, Roth MJ, Tio TL and Taylor PR: Mucosal
iodine staining improves endoscopic visualization of squamous
dysplasia and squamous cell carcinoma of the esophagus in Linxian,
China. Cancer. 83:220–231. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Moreno Racionero F, de Andres Asenjo B,
Bedate Nuñez M, Legido Moran P, Ortega Loubon C, Rabadán Jimenez J
and Beltran de Heredía Y Rentería J: Unusual relationship between
skin lesions and esophageal cancer: A case report and review of
literature. Z Gastroenterol. 53:115–119. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cho JW, Choi SC, Jang JY, Shin SK, Choi
KD, Lee JH, Kim SG, Sung JK, Jeon SW, Choi IJ, et al Korean ESD
Study Group, : Lymph node metastases in esophageal carcinoma: An
endoscopist's view. Clin Endosc. 47:523–529. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yu X and Wang G: Endoscopic treatment of
early esophageal cancer. Zhonghua Wei Chang Wai Ke Za Zhi.
18:860–863. 2015.(In Chinese). PubMed/NCBI
|
|
18
|
Chadwick G, Groene O, Hoare J, Hardwick
RH, Riley S, Crosby TD, Hanna GB and Cromwell DA: A
population-based, retrospective, cohort study of esophageal cancer
missed at endoscopy. Endoscopy. 46:553–560. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shibahara T, Yamamoto N, Yakushiji T,
Nomura T, Sekine R, Muramatsu K and Ohata H: Narrow-band imaging
system with magnifying endoscopy for early oral cancer. Bull Tokyo
Dent Coll. 55:87–94. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Muto M: Endoscopic diagnostic strategy of
superficial esophageal squamous cell carcinoma. Dig Endosc. 25
(Suppl 1):1–6. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gono K, Obi T, Yamaguchi M, Ohyama N,
Machida H, Sano Y, Yoshida S, Hamamoto Y and Endo T: Appearance of
enhanced tissue features in narrow-band endoscopic imaging. J
Biomed Opt. 9:568–577. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ide E, Carneiro FO, Frazão MS, Chaves DM,
Sallum RA, de Moura EG, Sakai P, Cecconello I and Maluf-Filho F:
Endoscopic detection of early esophageal squamous cell carcinoma in
patients with achalasia: Narrow-band imaging versus Lugol's
staining. J Oncol. 2013:7367562013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Matuszczyk A, Hahn S, Böse D, Eggebrecht
H, Schmermund A, Quadbeck B, Wieneke H, Petersenn S, Janssen OE and
Mann K: Gadolinium as an alternative contrast agent during cardiac
catheterization in patient with iodine-induced hyperthyroidism. Exp
Clin Endocrinol Diabetes. 114:336–338. 2006. View Article : Google Scholar : PubMed/NCBI
|