Introduction
Osteosarcoma is a primary malignant tumor of the
skeleton characterized by direct formation of bone or bone-like
tissue by tumor cells (1,2). Osteosarcoma predominantly occurs in
adolescents and is the most common type of primary bone tumor, with
an annual incidence of 1–3 cases per million individuals,
accounting for ~0.2% of malignant tumors and ~15% of primary bone
tumors (3–6). The most common sites for tumor
development are the long bones, typically the distal femur or
proximal humerus; manifestation at other sites is rare (7,8).
Hematogenous metastasis occurs early and has a high incidence,
rapid progression, high mortality and is difficult to treat
(9,10). Therefore, in recent years, the study
of osteosarcoma has become an important issue in the medical
community (11).
The age of onset of osteosarcoma has two peaks. The
first peak is in children and adolescents aged 10–20 years,
accounting for 60% of all cases of osteosarcoma; the second peak is
in adults aged >40 years, accounting for 13% of all
osteosarcomas (12). There are a
number of studies on osteosarcoma in children and adolescents. When
osteosarcoma occurs in patients aged >40 years, it is usually
considered to be secondary to Paget's disease of bone or irradiated
bone lesions (13); thus, primary
osteosarcoma in older adults is rare. Previous studies have
concluded that patients with osteosarcoma have a worse prognosis
with increasing age (14,15). Since 2007, 198 primary osteosarcomas
have been diagnosed and treated in the Department of Orthopedics,
The First Affiliated Hospital of Nanchang University, (Nanchang,
Jiangxi, China). The number of patients aged >50 years is <8,
including the 3 elderly patients described in the present report.
Currently, there are no reports of a patient aged >79 years with
a diagnosis of primary osteosarcoma. In the present study, the
clinical characteristics, imaging and pathological findings,
diagnosis and treatment of 3 cases of adult and elderly patients
with primary osteosarcoma are discussed. The First Affiliated
Hospital of Nanchang University ethical review committee approved
the present study, and written informed consent was obtained from
all patients.
Case report
Case 1
In December 2017, a 79-year-old Chinese female
retired worker (height, 155 cm; weight, 45 kg) visited the
Department of Orthopedics, The First Affiliated Hospital of
Nanchang University outpatient clinic with a 1-month history of
pain in the left groin that was relieved following rest. The pain
did not bother the patient at that time, but it had increased in
the previous week. The patient had no history of injuries or
illnesses, and no relevant family history. Physical examination
revealed that the skin around the left inguinal region was tender
to the touch, but displayed no redness, varicose veins or
hyperpigmentation. The left lower extremity motion and sensation
were within normal limits. There was no obvious abnormality in the
other extremities.
During laboratory examination, the following levels
were detected: Erythrocyte sedimentation rate, 85 mm/h; C-reactive
protein level, 25.20 mg/ml; serum alkaline phosphatase level, 214
units/l; carbohydrate antigen 724 level, 24.35 units/ml; and
squamous cell carcinoma-associated antigen level, 3.19 ng/ml; all
of which were higher than the normal ranges (0–20 mm/h, 0–8 mg/ml,
50–135 units/l, 0–6.9 units/ml, and 0–2.5 ng/ml, respectively).
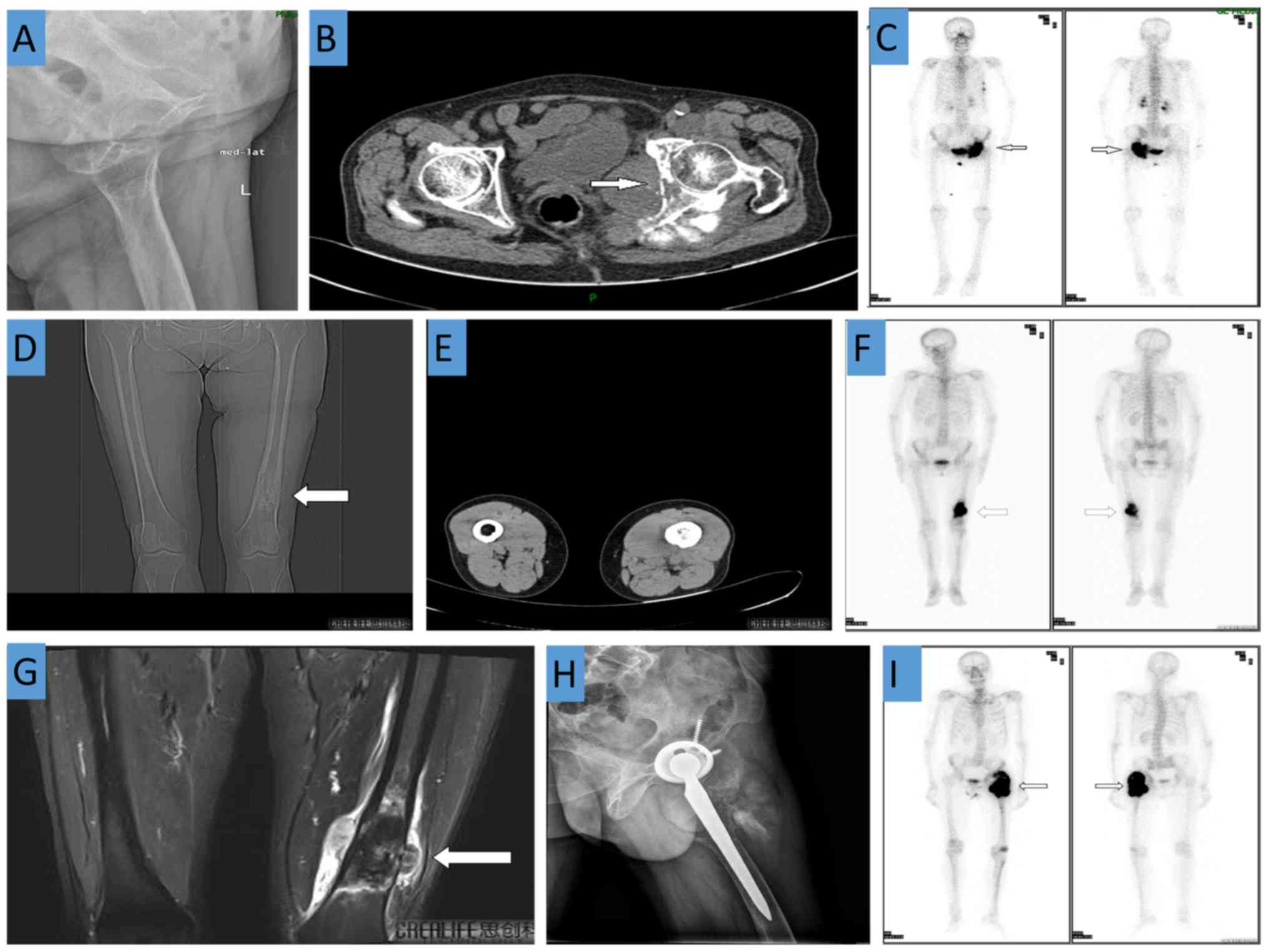
Radiography revealed bony changes of the upper left suprapubic
branch, ischium and acetabulum (Fig.
1A). CT demonstrated irregular bone destruction of the left
acetabulum and ischium, adjacent soft tissue swelling, and a
visible shadow. The soft tissue mass measured approximately 6.9×4.0
cm and had an ill-defined boundary. There were plaque-like,
cloud-shaped, needle-like, high-density shadows in the left hip
joint, but no obvious abnormalities in the right hip joint
(Fig. 1B). A whole body bone scan
revealed increased bone metabolism in the left acetabulum, ischium,
and femoral head, which was attributed to a malignant bone lesion.
Increased bone metabolism in the fourth and fifth ribs and T8
vertebra was also observed (Fig.
1C).
Using hematoxylin and eosin staining, the left ilium
bone tumor revealed heterogeneous cells diffusely distributed
between trabecular bone. In a fragment of fibrous tissue and muscle
tissue, oval-shaped tumor cells with large nuclei were distributed
in patches and karyolysis was present. The tumor cells had an
invasive growth pattern (Fig. 2A and
B). Taking into account the age and poor physical status of the
patient, chemoradiotherapy was recommended. However, the patient
and the patients' family did not wish to continue treatment and
requested to be discharged. The patient was discharged 2 weeks
after admission and was lost to follow-up.
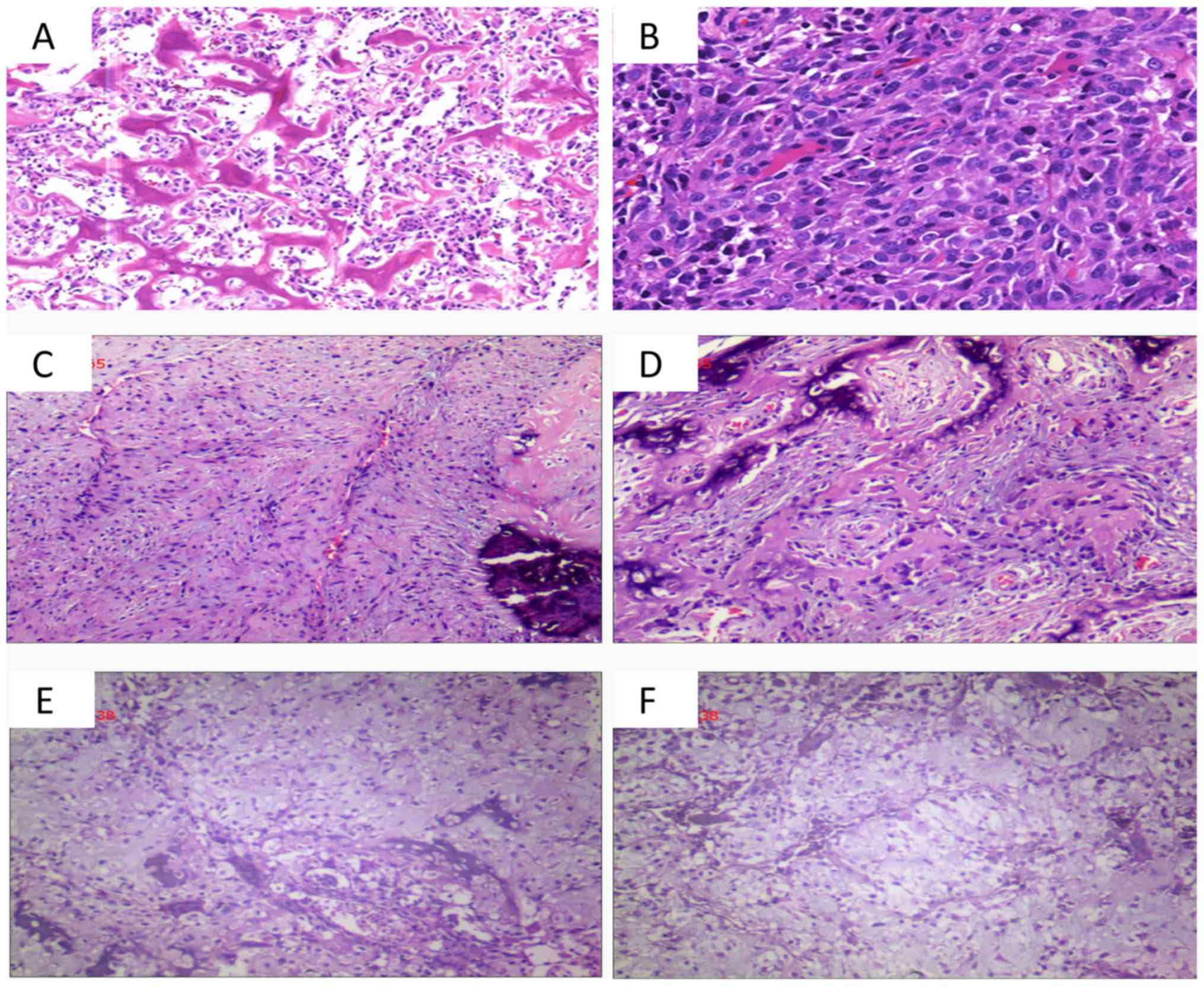 | Figure 2.Post-operative histological
observations. (A and B) Case 1, diffuse distribution of tumor cells
between the trabecular bone and tumor cells in fibrous tissue and
muscle tissue are distributed in patches and reveal infiltrating
growth (A, HE staining; magnification, ×100; B, HE staining;
magnification, ×200). (C and D) Case 2, spindle cells in the tissue
proliferating in bundles or weave patterns, adherent peripheral
osteoblasts, and calcification were observed (HE staining;
magnification, ×100). (E and F) Case 3, a large number of irregular
bone-like structures are arranged in trabecular or reticulated
patterns, and damaged bone tissue and immature cartilage (HE
staining; magnification, ×100). HE, hematoxylin and eosin. |
Case 2
In November 2016, a 62-year-old Chinese female
farmer (height, 157 cm; weight, 48 kg) presented with a left
femoral mass of uncertain etiology and pain in the left lower
extremity had been experienced for 2 months. The patient was
admitted at a The First People's Hospital of Xiaoshan City
(Xiaoshan, China), and a diagnosis of osteomyelitis was considered.
The patient was admitted to the Department of Orthopedics, The
First Affiliated Hospital of Nanchang University for further
treatment. The patient had no previous medical history.
The patient had no history of injury, past medical
illnesses or family history that were associated with disease.
Physical examination revealed a 10×5×5 cm hard mass of the distal
left femur; there was no obvious redness or ulceration in the
adjacent skin. There was also no significant limitation in the
activity level of the patient and no neurovascular defects in the
lower limbs.
Routine laboratory testing revealed a
neuron-specific enolase level of 24.26 units/ml (normal range,
0–16.3 units/ml) and an erythrocyte sedimentation rate of 26 mm/h
(normal range, 0–20 mm/h). Radiography performed at the local
hospital revealed a low-density shadow at the distal end of the
left femur. CT demonstrated a soft tissue mass shadow and a bony
mass shadow attached to the surface of the bone at the distal left
femur (Fig. 1D and E). Enhanced MRI
revealed an area of irregular bone destruction in the distal femur,
and an abnormal signal shadow was observed (Fig. 1G). A whole body bone scan revealed a
cluster of lesions at the distal end of the left femur (Fig. 1F).
Using hematoxylin and eosin staining, the left femur
bone biopsy revealed proliferating spindle cells in bundles or
braids. The tumor cells had lightly stained cytoplasm, oval nuclei
and no nuclear division. A red-stained matrix was visible,
peripheral osteoblasts were adhered to adjacent structures and
areas of calcification were observed (Fig. 2C and D). The patient received two
cycles of local arterial perfusion as follows: Cisplatin (DDP) was
administered at a dose of 120 mg on day 1, and the regimen was
repeated every 14 days. After 3 months, the patient was given six
cycles of DDP (120 mg) once daily for 1 day as systemic intravenous
chemotherapy; 20 mg doxorubicin once daily for 3 days, after 2
weeks of 2 g isophosphate for 5 days. After 2 weeks, the cycle was
repeated. At the follow-up 2.5 years after surgery, there was no
significant pain in the left lower extremity and no evidence of
local or distant recurrence following chemotherapy.
Case 3
In March 2013, a 51-year-old Chinese male teacher
(height, 168 cm; weight, 56 kg) sustained a left femoral neck
fracture due to a fall and underwent left total hip arthroplasty in
Xinjian County People's Hospital (Nanchang, China). The
postoperative recovery of the patient was unremarkable. However, at
2 years after surgery, the patient developed left hip pain of
unclear etiology with limited mobility. Due to the marked increase
in pain and limited mobility, the patient presented to the
Department of Orthopedics, The First Affiliated Hospital of
Nanchang University for further treatment and was admitted in
October 2015. The patient had no history of allergies or related
family history. Postoperative physical examination revealed a 15-cm
healing scar on the left hip, tenderness of the left femoral
trochanter, elevated local skin temperature, no redness of the
skin, limited left hip joint activity and normal left knee joint
activity. There were no obvious abnormalities of the muscles and
muscle tone of the lower limbs. There was also no significant
recent change in the weight of the patient.
Routine laboratory testing revealed a serum alkaline
phosphatase level of 785 units/l (normal range, 50–135 units/l) and
a C-reactive protein level of 10.8 mg/ml (normal range, 0–8 mg/l),
while the erythrocyte sedimentation rate and tumor markers
(including α-fetoprotein, carcinoembryonic antigen, carbohydrate
antigen 12-5, carbohydrate antigen 15-3 and carbohydrate antigen
19-9) were within the normal ranges. Radiography observed the
artificial hip joint replacement on the left side, as well as a
soft tissue mass shadow visible in the upper left femur, which
suggested malignancy (Fig. 1H). A
whole body bone scan revealed concentrated foci in the left upper
femur and the left knee joint, which were suggestive of ipsilateral
metastasis (Fig. 1I). The patient
was initially diagnosed with bone metastasis.
Following routine preoperative assessment,
continuous spinal dural anesthesia was used, and the patient was
placed in the right lateral position. Following the extension of
the original surgical incision, the skin, subcutaneous tissue, and
superficial fascia were dissected layer by layer; subsequently, the
fascia was opened, and the muscle fibers of the gluteus maximus
were dissected to reveal the proximal femur. The original femoral
prosthesis was removed, and upper femoral bone destruction was
visualized. In the surgical field of view, the tumor appeared
similar to the flesh of a fish and invaded the surrounding soft
tissue, with ill-defined margins. Moreover, intraoperative
cryosectioning revealed malignant tumor cells. Subsequently,
granulation tissue within the medullary cavity, the surrounding
tumor tissue, and the surrounding affected muscle tissue were
completely removed. Subsequently, a customized tumor prosthesis was
implanted into the medullary canal and fixed with bone cement. As
the original acetabular cup was tilted backward, polyethylene was
added to the trailing edge to prevent dislocation. Following
resetting of the cup, the hip joint was examined for completeness
and satisfactory mobility. Finally, the wound was soaked in
distilled water, and was repeatedly washed with hydrogen peroxide
and physiological saline. A drainage tube was placed under the
muscle layer, the fascia was sutured, and the incision was closed
layer by layer.
Histological examination [with hematoxylin and eosin
(HE) staining] of the tumor from the left proximal femur revealed
irregular, bone-like tissues arranged in a trabecular or mesh
shape. The tumor cells revealed large deeply stained nuclei,
abundant red-stained or translucent cytoplasm, and a large number
of giant tumor cells. In some areas, fragments of bone tissue and
immature cartilage tissue were visualized (Fig. 2E and F). Based on the medical history
of the patient, the imaging and laboratory findings, and the
pathological results, the final diagnosis of primary osteosarcoma
of the proximal left femur was established.
Postoperatively, adjuvant chemotherapy was
recommended. However, the patient and the patient's family declined
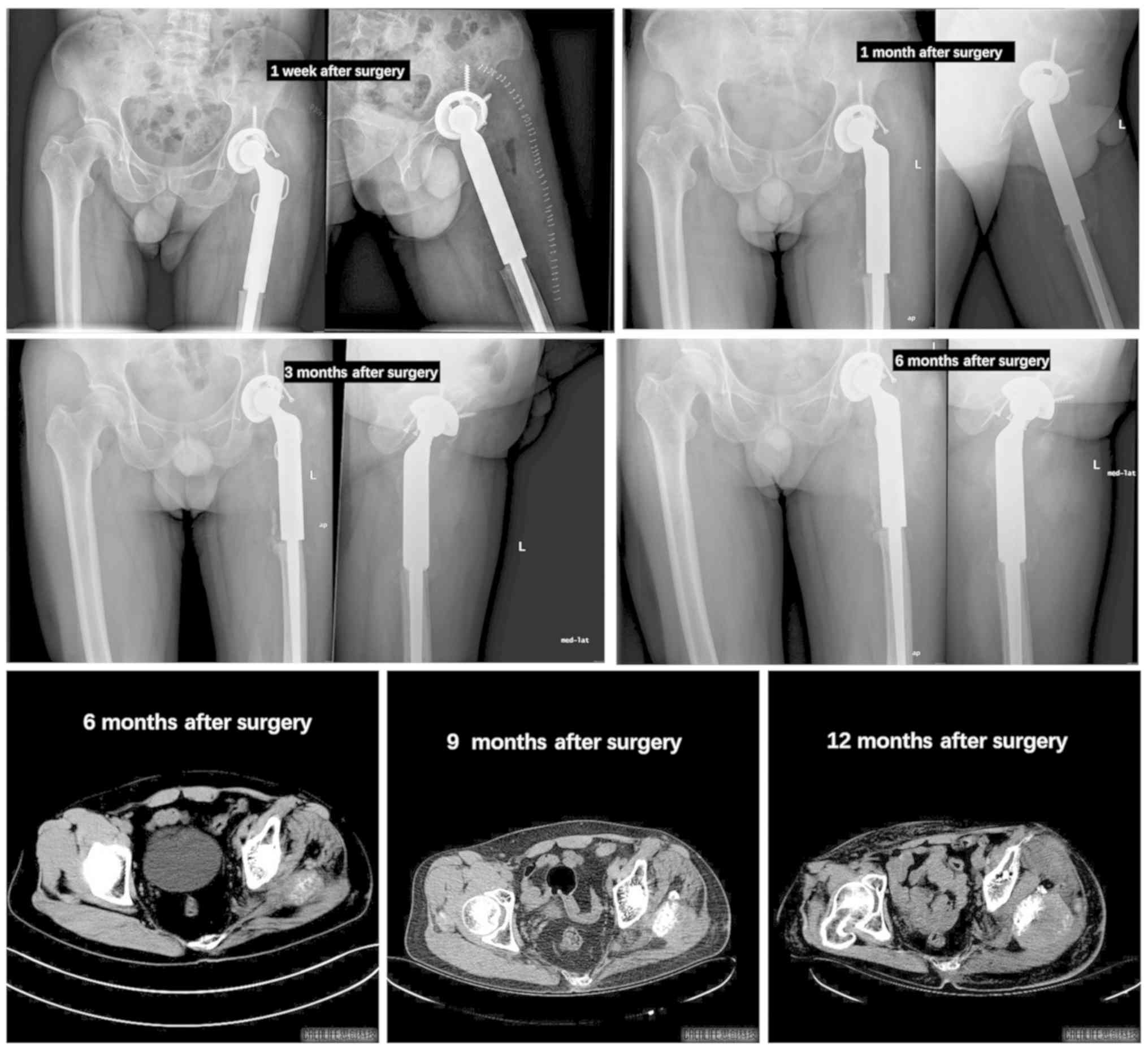
treatment and requested discharge, but agreed to follow-up. The
patient revealed no signs of recurrence within 3 months after
surgery and no signs of distant metastasis. However, 6 months after
surgery, the patient revealed evidence of tumor recurrence on the
postoperative follow-up imaging examination (Fig. 3). The patient received a combination
of gemcitabine/docetaxel as follows: 900 mg/m2
gemcitabine on days 1 and 8, and 120 mg/m2 docetaxel on
day 8. The regimen was repeated every 3 weeks, and although the
patient continued to be treated for 6 months, the left hip pain of
this patient did not improve following chemotherapy, and the
activity was limited.
Discussion
The majority of studies on the diagnosis and
treatment of osteosarcoma have focused on adolescents. Osteosarcoma
at other ages is rarely discussed, with the exception of
osteosarcoma secondary to Paget's disease (0.2% of osteosarcomas)
(16) or following radiotherapy
(17). In the present study, the
records of 3 patients with primary osteosarcoma >50 years of age
and treated in the Department of Orthopedics, The First Affiliated
Hospital of Nanchang University were reviewed, in order to
demonstrate the clinical features and prognostic factors of this
disease.
The diagnosis of osteosarcoma is based on the
combination of clinical, radiography and pathological results.
Pathological confirmation of the formation of osteoid tissue and/or
bone by tumor cells is key to the diagnosis. Various unusual
histological subtypes were more common in these 3 older patients
compared with that in younger patients, and fibroblasts and
chondrocyte subtypes were observed in addition to the conventional
subtypes of osteoblasts. However, early diagnosis of osteosarcoma
in older patients is difficult, and misdiagnosis or a missed
diagnosis is common (15). This may
be associated with the following factors: i) The incidence of
osteosarcoma in elderly individuals is extremely rare (18,19); ii)
osteosarcoma in elderly individuals can be confused with
osteoarthropathy (15); iii)
following the discovery of lesions, clinicians tend to focus on
bone metastases and other primary tumors that occur more commonly
in elderly individuals (20). For
example, chondrosarcoma occurs predominantly in the elderly
(21). In some cases, focal
ossification can be visualized under the microscope; this feature
is similar to that observed for osteosarcoma (2). However, intraosseous ossification of
chondrosarcoma appears as trabecular bone in a background of
cartilage (22). In addition,
residual chondrocytes are observed in trabecular bone, as well as
around the stroma (23).
A key finding detected by light microscopy is the
absence of tumor osteogenesis in chondrosarcoma (24). For metastatic cancer, the primary
lesion should be identified, and the corresponding clinical
manifestations and histopathological features should be linked with
the bone tumor. Although malignant fibrous histiocytoma is more
common in the soft tissues, it can also occur in bone in elderly
populations. In these cases, it is easy to distinguish osteosarcoma
from malignant fibrous histiocytoma based on imaging and
pathological findings. Previous reports have focused on
osteosarcoma in children and adolescents; however, osteosarcoma is
often secondary to Paget's disease in elderly patients (12,25). In
Western populations, secondary primary osteosarcoma accounts for a
large proportion of elderly patients with osteosarcoma, usually due
to Paget's disease, benign bone disease or radiation complications
(26,27). No patients with primary osteosarcoma
had Paget's disease in the present study. Histologically, poor cell
differentiation, obvious polymorphism, large nuclei, irregularity
and matrix sclerosis were observed. However, in these 3 patients,
there was a large volume of immature or mature bone-like stroma
between the tumor cells, which is very different from the
appearance of osteosarcoma secondary to Paget's disease. As the
majority of patients with Paget's disease have no obvious symptoms,
when osteosarcoma occurs in older patients, the diagnosis of
primary osteosarcoma can be made following the exclusion of
osteosarcoma secondary to Paget's disease. Table I summarizes the differential
diagnosis of osteosarcoma in elderly patients.
 | Table I.Differential diagnosis of osteosarcoma
in middle-aged and elderly patients. |
Table I.
Differential diagnosis of osteosarcoma
in middle-aged and elderly patients.
| Differential
diagnosis | Details |
|---|
| Chondrosarcoma | Under light
microscopy, residual chondrocytes in the trabecular bone and matrix
are observed, with no osteoblasts identified |
| Paget's disease | Under the microscope,
poor cell differentiation, obvious polymorphism, large nuclei,
irregularity, and matrix sclerosis are observed |
| Metastatic
carcinoma | Primary lesion is
identified, with corresponding clinical manifestations and
histopathological features |
In the 1970s, the standard treatment for
osteosarcoma was amputation, but the 5-year survival rate was
<20% (28). In the 1980s, due to
advances in surgical techniques, the development of effective
chemotherapy, and improved preoperative and postoperative
chemoradiotherapy procedures, limb-salvage surgery gradually
replaced traditional amputation (29). The key to the success of limb salvage
surgery lies in the choice of the surgical method and removal of
the tumor according to the most appropriate surgical boundary
(30). Osteosarcoma should be
completely removed to avoid local recurrence and distant
metastasis, with the resection plane 5–7 cm from the end of the
lesion. If the lesion is not completely removed during surgery, the
local recurrence rate can be as high as 25% (31). Rosen et al (32). advocated neoadjuvant chemotherapy for
osteosarcoma. The 5-year survival rate in patients has increased
from 20 to 50–70%. In addition, up to 60–80% of patients can obtain
limb retention, which has become the standard treatment for
osteosarcoma currently accepted by the majority of scholars; namely
‘neoadjuvant chemotherapy + surgery (limb salvage or amputation) +
adjuvant chemotherapy’. Certain reports have stated that
chemotherapy is beneficial in elderly patients with primary
osteosarcoma (33,34). However, in 1986, Huvos (35) reported that among 117 cases of
osteosarcoma in bone and soft tissue that occurred in patients aged
>60 years, 44% had primary osteosarcoma; the 5-year survival
rate following treatment was 18%, and the 10-year survival rate was
7%, suggesting that patients had a poor prognosis. In the present
study, case 2 received systematic chemotherapy and achieved a good
therapeutic effect. However, case 3 also received chemotherapy but
did not achieve satisfactory results. Therefore, regarding the
effect of chemotherapy on osteosarcoma in elderly patients, the
number of studies is insufficient to show whether chemotherapy is
effective.
In conclusion, one of the main limitations of the
present study is its insufficient number of cases. In addition, the
3 patients had different treatments therefore no comparisons could
be determined. Osteosarcoma in elderly patients is a possible cause
of pain and should not be ignored. Given its rarity, primary
osteosarcoma should be carefully evaluated. We hypothesize that
with increased awareness, it is possible to reach a correct
diagnosis in advance to avoid over-treatment. Finally, osteosarcoma
in elderly patients is rare; in order to improve the understanding
of this condition, more case studies are required. Plastic surgeons
and radiologists should consider the possibility of osteosarcoma
diagnosis in this age group.
Acknowledgements
Not applicable.
Funding
The present study was supported by Health and Family
Planning Commission of Jiangxi Province on Traditional Chinese
Medicine (grant no. 2016A073).
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
MD, and JZ performed the surgery and managed the
patients postoperatively. QX and TG contributed to the concept and
design of the study and to the acquisition, analysis or
interpretation of working data. BZ analyzed the patient's data. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethical Institutional
Review Board of the First Affiliated Hospital of Nanchang
University, and written informed consent was obtained from all
study participants.
Patient consent for publication
The consent for publication of the manuscript and
the related images from the patients and/or their relatives was
obtained by the First Affiliated Hospital of Nanchang
University.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kansara M, Teng MW, Smyth MJ and Thomas
DM: Translational biology of osteosarcoma. Nat Rev Cancer.
14:722–735. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
2
|
Poletajew S, Fus L and Wasiutynski A:
Current concepts on pathogenesis and biology of metastatic
osteosarcoma tumors. Ortop Traumatol Rehabil. 13:537–545. 2011.(In
English, Polish). View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Centrella M, Horowitz MC, Wozney JM and
McCarthy TL: Transforming growth factor-beta gene family members
and bone. Endocr Rev. 15:27–39. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bismar H, Klopinger T, Schuster EM,
Balbach S, Diel I, Ziegler R and Pfeilschifter J: Transforming
growth factor beta (TGF-beta) levels in the conditioncd mcdia of
human bone cclls relationship to donor age bone volvme and
cconcentration of TGF-beta in human bone matrix in vivo. Bone.
24:565–569. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Savage SA and Mirabello L: Using
epidemiology and genomics to understand osteosarcoma etiology.
Sarcoma. 2011:5481512011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Meyers PA and Gorlick R: Osteosarcoma.
Pediatr Clin North Am. 44:973–989. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Damron TA, Ward WG and Stewart A:
Osteosarcoma, chondrosarcoma, and Ewing's sarcoma: National cancer
data base report. Clin Orthop Relat Res. 459:40–47. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Anil S, Krishnan AP and Rajendran R:
Osteosarcoma of the mandible masquerading as a dental abscess:
Report of a case. Case Rep Dent. 2012:6350622012.PubMed/NCBI
|
|
9
|
Tsuchiya H, Kanazawa Y, Abdel-Wanis ME,
Asada N, Abe S, Isu K, Sugita T and Tomita K: Effect of timing of
pulmonary metastases identification on prognosis of patients with
osteosarcoma: The japanese musculoskeletal oncology group study. J
Clin Oncol. 20:3470–3477. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Williams RF, Fernandez-Pineda I and Gosain
A: Pediatric sarcomas. Surg Clin North Am. 96:1107–1125. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Haduong JH, Martin AA, Skapek SX and
Mascarenhas L: Sarcomas. Pediatr Clin North Am. 62:179–200. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Duffaud F, Digue L, Baciuchka-Palmaro M,
Volot F, Perles-Daniel C, Garbe L and Favre R: Osteosarcomas of
flat bones in adolescents and adults. Cancer. 88:324–332. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ek ET, Ojaimi J, Kitagawa Y and Choong PF:
Outcome of patients with osteosarcoma over 40 years of age: Is
angiogenesis a marker of survival? Int Semin Surg Oncol. 3:72006.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Durnali A, Alkis N, Cangur S, Yukruk FA,
Inal A, Tokluoglu S, Seker MM, Bal O, Akman T, Inanc M, et al:
Prognostic factors for teenage and adult patients with high-grade
osteosarcoma: An analysis of 240 patients. Med Oncol. 30:6242013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sadoghi P, Leithner A, Clar H, Glehr M,
Wibmer C, Bodo K, Quehenberger F and Windhager R: The threat of
misdiagnosis of primary osteosarcoma over the age of 60: A series
of seven cases and review of the literature. Arch Orthop Trauma
Surg. 130:1251–1256. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wick MR, Siegal GP, Unni KK, McLeod RA and
Greditzer HG III: Sarcomas of bone complicating osteitis deformans
(Paget's disease): Fifty years' experience. Am J Surg Pathol.
5:47–59. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Frassica FJ, Frassica DA, Wold LE, Beabout
JW and Sim FH: Postradiation sarcoma of bone. Orthopedics.
16:105–109. 1993.PubMed/NCBI
|
|
18
|
Ogura K, Higashi T and Kawai A: Statistics
of bone sarcoma in Japan: Report from the bone and soft tissue
tumor registry in Japan. J Orthop Sci. 22:133–143. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ishikawa Y, Tsukuma H and Miller RW: Low
rates of Paget's disease of bone and osteosarcoma in elderly
Japanese. Lancet. 347:15591996. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jeon DG, Lee SY, Cho WH, Song WS and Park
JH: Primary osteosarcoma in patients older than 40 years of age. J
Korean Med Sci. 21:715–718. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nie Z, Lu Q and Peng H: Prognostic factors
for patients with chondrosarcoma: A survival analysis based on the
Surveillance, Epidemiology, and End Results (SEER) database
(1973–2012). J Bone Oncol. 13:55–61. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sergi C and Zwerschke W: Osteogenic
sarcoma (osteosarcoma) in the elderly: Tumor delineation and
predisposing conditions. Exp Gerontol. 43:1039–1043. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lex JR, Evans S, Stevenson JD, Parry M,
Jeys LM and Grimer RJ: Dedifferentiated chondrosarcoma of the
pelvis: Clinical outcomes and current treatment. Clin Sarcoma Res.
8:232018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gumay S: Pathological diagnosis of bone
sarcoma. Gan To Kagaku Ryoho. 27 (Suppl 2):S420–S426. 2000.
|
|
25
|
Bielack SS, Kempf-Bielack B, Heise U,
Schwenzer D and Winkler K: Combined modality treatment for
osteosarcoma occurring as a second malignant disease. Cooperative
German-Austrian-Swiss Osteosarcoma Study Group. J Clin Oncol.
17:11641999. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Grimer RJ, Cannon SR, Taminiau AM, Bielack
S, Kempf-Bielack B, Windhager R, Dominkus M, Saeter G, Bauer H,
Meller I, et al: Osteosarcoma over the age of forty. Eur J Cancer.
39:157–163. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
deSantos LA, Rosengren JE, Wooten WB and
Murray JA: Osteogenic sarcoma after the age of 50: A radiographic
evaluation. AJR Am J Roentgenol. 131:481–484. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ferrari S and Palmerini E: Adjuvant and
neoadjuvant combination chemotherapy for osteogenic sarcoma. Curr
Opin Oncol. 19:341–346. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wittig JC, Bickels J, Priebat D, Jelinek
J, Kellar-Graney K, Shmookler B and Malawer MM: Osteosarcoma: A
multidisciplinary approach to diagnosis and treatment. Am Fam
Physician. 65:1123–1132. 2002.PubMed/NCBI
|
|
30
|
Agarwal M, Anchan C, Shah M, Puri A and
Pai S: Limb salvage surgery for osteosarcoma: Effective low-cost
treatment. Clin Orthop Relat Res. 459:82–91. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kim HJ, Chalmers PN and Morris CD:
Pediatric osteogenic sarcoma. Curr Opin Pediatr. 22:612010.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Rosen G, Caparros B, Huvos AG, Kosloff C,
Nirenberg A, Cacavio A, Marcove RC, Lane JM, Mehta B and Urban C:
Preoperative chemotherapy for osteogenic sarcoma: Selection of
postoperative adjuvant chemotherapy based on the response of the
primary tumor to preoperative chemotherapy. Cancer. 49:1221–1230.
1982. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bacci G, Ferrari S, Donati D, Longhi A,
Bertoni F, Di Fiore M, Comandone A, Cesari M and Campanacci M:
Neoadjuvant chemotherapy for osteosarcoma of the extremity in
patients in the fourth and fifth decade of life. Oncol Rep.
5:1259–1263. 1998.PubMed/NCBI
|
|
34
|
Manoso MW, Healey JH, Boland PJ,
Athanasian EA, Maki RG, Huvos AG and Morris CD: De novo osteogenic
sarcoma in patients older than forty: Benefit of multimodality
therapy. Clin Orthop Relat Res. 438:110–115. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Huvos AG: Osteogenic sarcoma of bones and
soft tissues in older persons. A clinicopathologic analysis of 117
patients older than 60 years. Cancer. 57:1442–1449. 1986.
View Article : Google Scholar : PubMed/NCBI
|