Introduction
Pancreatic ductal adenocarcinoma (PDAC) is known as
one of the most malignant types of neoplasm, with a 5-year survival
rate of <6%. In addition, there is an increasing number of
patients diagnosed annually with de novo PDAC (1,2).
Although radical resection provides a chance of successful
treatment, only 15–20% of patients with PDAC are candidates for
radical resection at the time of diagnosis (3–5). The
majority of unresectable patients present with distant metastasis
and others present with tumor invasion of surrounding vessels
(6).
In the past, patients with portal vein (PV)
involvement were deemed unresectable because PV invasion would be a
harbinger of metastatic disease and early attempts of
pancreaticoduodenectomy (PD) with PV resection (PVR) were always
coupled with worse survival time (211 vs. 374 days; P<0.001)
(7). With the development of
vascular reconstruction technique, PD combined with PVR has been
gradually carried out for selected patients with PDAC with PV
involvement (8). However, there
remains a debate on whether it is worthwhile to perform PD
synchronously with PVR knowing that local recurrence is not common
in patients with PV invasion (9). A
number of studies demonstrated that PD with PVR provided no
significant survival benefit at the expense of higher rates of
morbidity and mortality (10–12),
while others argued that PD with PVR was safe and feasible and
could offer improved survival outcomes (13–16).
A recent systemic review reported that the median
overall survival (OS) time was worse in patients with PVR (14.3 vs.
19.5 months) and the postoperative complication rate was higher
(odds ratio, 1.34; P=0.03) (17).
However, more patients in the PD+PVR group had larger tumors,
higher tumor grades, more plexus invasion and greater lymph node
(LN) metastasis (18–20). In addition, there was a notable
difference in baseline clinical characteristics between patients
with and without PVR (20). Due to
the poorer clinical characteristics, patients with PVR usually have
worse long-term prognosis (20).
Given this dilemma, propensity score matching (PSM),
which is the conditional probability of assignment to a particular
treatment given a vector of observed covariate (21), has been widely used to balance the
baselines between the experimental group and control group
(22,23) for the sake of reducing selection bias
and identifying the causal effect (21,24).
It was demonstrated in our previous study that PVR
could significantly improve the OS of patients with PV involvement
as compared with chemotherapy or surgical bypass (25). However, comparisons between patients
with or without PVR, to the best of our knowledge, have not been
reported. The aim of the present study was to compare the survival
outcomes between patients with or without PVR by using the PSM
method. This was done to determine whether patients with PV
involvement could achieve the same survival benefit from PVR as
patients without PV involvement, in order to verify the efficacy
and safety of PVR.
Patients and methods
Inclusion and exclusion criteria
The inclusion criteria for the patients enrolled in
the present study were as follows: i) Age >18 years; ii)
patients diagnosed with histopathologically confirmed resectable
PDAC; and iii) patients who underwent PD with or without PVR. The
exclusion criteria were as follows: i) Patients with severe medical
comorbidities and other uncontrolled malignancies; and ii) patients
with peri- or intra-operative evidence of distant metastasis and
arterial involvement. Before PSM, 377 patients (PVR group, n=138;
non-PVR group, n=239) from Huashan Hospital (Shanghai, China) were
enrolled in the present study from January 2011 to December 2013.
Among which, 231 patients were males (mean age, 61.8±8.7 years;
range, 34–84 years) and 146 patients were females (mean age,
62.3±8.8 years; range, 29–84 years). After PSM, 246 patients (PVR
group, n=123; non-PVR group, n=123) from Huashan Hospital
(Shanghai, China) were enrolled into the present study. Among
which, 151 patients were males (mean age, 62.0±9.2 years; range,
35–84 years) and 95 patients were females (mean age, 62.8±9.7
years; range, 29–83 years).
Tumor stage was assessed pathologically according to
the Tumor-Node-Metastasis (TNM) classification system published by
the American Joint Committee on Cancer, 8th edition (26). This study was approved and performed
in accordance with the Declaration of Helsinki and the Clinical
Research Ethics Committee of Huashan Hospital. All patients signed
informed consent for surgical treatment and pathological
examinations.
Preoperative detection and
evaluation
Ultrasonography, computed tomography (CT), MRI,
positron emission tomography-CT (PET-CT) and endoscopic sonography
were performed to evaluate local tumor extension and metastasis. A
high suspicion of PV involvement based on preoperative imaging,
such as CT or MRI, was determined. Nevertheless, the surgeon's
intraoperative visual judgments were also of great importance to
determine the possibility of PV involvement. Patient demographics
[serum leukocyte count, serum alanine aminotransferase (ALT), total
bilirubin (TBil), albumin (ALB), body mass index (BMI), serum
carbohydrate antigen (CA)125 and CA19-9], tumor characteristics,
intra-operative parameters and patient survival were compared
between the two groups.
Surgical procedures
Patients with resectable primary tumors and
preoperative evaluation of PV involvement (27) were divided into a PD+PVR group and a
PD group. All patients enrolled in this study underwent detailed
preoperative examination, including both blood tests and
imageological examinations (CT, MRI or PET-CT). Patients with
suspected metastasis were confirmed by pathological evidence
(biopsy or operation) and were excluded from this study. During the
operation, the surgeon's own visual judgments and intraoperative
ultrasound was used to detect remote metastasis. Patients with any
extra-pancreatic metastasis, which were not detected by
preoperative PET-CT scanning, were also excluded from this study.
Patients with PV involvement, but without possibility of
reconstruction (multiple branch involvement), underwent surgical
bypass (SB) procedure based on intra-operative judgment of the
surgeon, and were also excluded from this study.
In the PD group, patients underwent classical PD. In
the PD+PVR group, patients with PV involvement underwent radical
resection of PDAC and PVR. PVR was carried out en-bloc as
primary closure of the vein, and reconstructed with ePTFE vascular
grafts (Bard Peripheral Vascular, Inc.).
Follow-up observation and
complications
During the follow-up period (the last follow-up date
was December 2018), all patients were followed up for CT and blood
tests, and patients with PVR required an additional ultrasound to
detect patency of the artificial grafts. Patients were followed up
monthly postoperatively for the first 6 months, then every 3–6
months thereafter. All patients in PVR group were administrated
aspirin (100 mg a day) and received ultrasound examinations
postoperatively. OS time was the primary outcome of this study.
Postpancreatectomy hemorrhage (PPH), postoperative pancreatic
fistula (POPF), chylous fistula and delayed gastric emptying (DGE)
were defined according to International Study Group of Pancreatic
Surgery (28–31). In the present study, all patients
died from disease.
PSM analysis
There were statistically significant differences in
the baseline characteristics between the two groups, which would
affect the outcome of analysis. For continuous data, differences
between the two groups were analyzed using the independent
Student's t-test, and a χ2 test was used for categorical
variables. PSM was utilized to balance the baseline characteristics
between the two groups, in order to reduce the risk of selection
bias and mimic a controlled randomized trial. A logistic regression
model was used to estimate PSM based on age, sex, BMI, leukocyte,
ALT, TBil, ALB, CA125, CA19-9, tumor stage, LN metastasis and tumor
size. One-to-one matching without replacement conducted by a 0.1
caliper matching on the estimated propensity score generated 123
matched PVR and non-PVR units (32).
Statistical analysis
All demographic and clinicopathological data were
collected in the computer database of Huashan Hospital and analyzed
statistically using SPSS 23.0 (IBM, Corp.). In the case of
continuous data, differences between the two groups were analyzed
through the independent Student's t-test, and a χ2 test
was used for categorical variables. Survival curves were
established using the Kaplan-Meier method and compared with a
log-rank test. Continuous data were reported as mean ± standard
error. Significant risk factors were first identified using
univariate logistic regression, after which the significant
univariate factors were further examined using multivariate
analysis. The outcomes were presented using hazard ratios (HRs) and
associated 95% confidence intervals (CIs). A two-sided P<0.05
was considered to indicate a statistically significant
difference.
Results
Demographic and clinicopathological
parameters of the included patients before PSM
Between 2011 and 2013, there were 138 patients who
underwent PD+PVR and the remaining 239 received PD without PVR.
Patients in the PD+PVR group exhibited more tumor stage II patients
(P<0.001), smaller BMIs (P=0.015), significantly higher CA19-9
levels (P=0.040), significantly lower CA125 levels (P=0.010),
larger tumor sizes (P<0.001), longer operating durations
(P<0.001) and more intraoperative blood loss (P<0.001)
(Table I).
 | Table I.Baseline characteristics of all
patients who received PD with or without PVR. |
Table I.
Baseline characteristics of all
patients who received PD with or without PVR.
|
| Before PSM |
| After PSM |
|
|---|
|
|
|
|
|
|
|---|
| Index | PVR group
(n=138) | Non-PVR group
(n=239) | P-value | PVR group
(n=123) | Non-PVR group
(n=123) | P-value |
|---|
| Male, n (%) | 78 (56.5) | 153 (64.0) | 0.150 | 69 (56.1) | 82 (66.7) | 0.089 |
| Age, years | 62.75±8.22 | 61.54±9.01 | 0.197 | 62.70±8.53 | 61.95±10.22 | 0.534 |
| BMI,
kg/m2 | 21.70±2.91 | 22.41±2.56 | 0.015 | 21.80±2.95 | 21.80±2.53 | 0.996 |
| Leukocyte,
109/l | 5.82±1.67 | 5.82±1.84 | 0.966 | 5.91±1.68 | 5.95±1.86 | 0.861 |
| ALT, U/l | 35.50
(18.00–79.25) | 45.00
(21.00–84.00) | 0.904 | 39.00
(19.00–82.00) | 51.00
(21.00–115.00) | 0.302 |
| TBIL, µmol/l | 13.00
(8.00–31.13) | 13.70
(7.60–38.60) | 0.660 | 13.00
(8.00–31.00) | 21.70
(10.60–43.80) | 0.226 |
| ALB, g/l | 39.24±4.56 | 39.62±3.76 | 0.383 | 39.20±4.56 | 39.12±3.84 | 0.892 |
| CA125, U/ml | 14.50
(10.00–40.00) | 18.00
(12.00–26.00) | 0.010 | 14.00
(10.00–38.00) | 17.00
(12.00–31.00) | 0.413 |
| CA19-9, U/ml | 120.00
(36.75–642.25) | 86.00
(40.00–218.00) | 0.040 | 115.00
(40.00–642.00) | 100.00
(41.00–438.00) | 0.795 |
| TNM stage, n
(%) |
|
|
|
|
|
|
| Stage
I | 30 (21.7) | 106 (44.4) | <0.001 | 30 (24.4) | 33 (26.8) | 0.556 |
| Stage
II | 96 (69.6) | 114 (47.7) |
| 84 (68.3) | 77 (62.6) |
|
| Stage
III | 12 (8.7) | 19 (7.9) |
| 9 (7.3) | 13 (10.6) |
|
| LN metastasis, n
(%) | 66 (47.8) | 96 (40.2) | 0.148 | 56 (45.5) | 58 (47.2) | 0.798 |
| Tumor size, cm | 4.06±1.22 | 3.13±1.13 | <0.001 | 3.87±1.08 | 3.71±1.15 | 0.254 |
| R1 resection, n
(%) | 5 (3.6) | 14 (5.9) | 0.465 | 5 (4.1) | 7 (5.7) | 0.898 |
| PV invasion, n
(%) | 127 (92.0) | – | – | 112 (91.1) | – | – |
| Operating time,
min | 485.29±76.52 | 399.95±72.56 | <0.001 | 482.76±76.11 | 433.80±73.37 | <0.001 |
| Intraoperative
blood loss, ml | 600.00
(500.00–1000.00) | 460.00
(400.00–600.00) | <0.001 | 600.00
(500.00–900.00) | 460.00
(400.00–800.00) | <0.001 |
| Hospital stay,
days | 21.36±9.20 | 19.76±9.67 | 0.314 | 21.80±9.55 | 22.34±9.35 | 0.652 |
Survival analysis before PSM
analysis
Multivariate Cox regression model showed that
advanced tumor stages, lower BMI levels, LN metastasis, lower ALB
levels, higher CA125 and CA19-9 levels were independent prognostic
factors (Table II).
| Table II.Multivariate regression analysis of
prognostic factors. |
Table II.
Multivariate regression analysis of
prognostic factors.
|
| Before PSM | After PSM |
|---|
|
|
|
|
|---|
|
| Multivariate
regression analysis | Multivariate
regression analysis |
|---|
|
|
|
|
|---|
| Risk factors | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Therapy |
|
|
|
|
|
|
|
PVR | 1.084 | 0.831–1.415 | 0.551 | – | – | – |
|
Non-PVR |
|
|
|
|
|
|
| TNM stage |
|
|
|
|
|
|
| Stage
I | 1.643 | 1.214–2.225 | 0.001 | 1.912 | 1.319–2.771 | 0.001 |
| Stage
II |
|
|
|
|
|
|
| Stage
III |
|
|
|
|
|
|
| BMI,
kg/m2 |
|
|
|
|
|
|
|
<18.5 | 0.652 | 0.436–0.974 | 0.037 | 0.601 | 0.388–0.931 | 0.023 |
|
≥18.5 |
|
|
|
|
|
|
| R1 resection |
|
|
|
|
|
|
| No | 1.685 | 0.957–2.966 | 0.071 | 1.955 | 1.018–3.755 | 0.044 |
|
Yes |
|
|
|
|
|
|
| LN metastasis |
|
|
|
|
|
|
|
Yes | 0.646 | 0.465–0.898 | 0.009 | 0.642 | 0.440–0.936 | 0.021 |
| No |
|
|
|
|
|
|
| ALB, g/l |
|
|
|
|
|
|
|
<35 | 0.568 | 0.371–0.868 | 0.009 | 0.569 | 0.350–0.923 | 0.022 |
|
≥35 |
|
|
|
|
|
|
| CA125 U/ml |
|
|
|
|
|
|
|
<35 | 1.475 | 1.082–2.011 | 0.014 | 1.49 | 1.038–2.139 | 0.031 |
|
≥35 |
|
|
|
|
|
|
| CA19-9 U/ml |
|
|
|
|
|
|
|
<37 | 1.708 | 1.396–2.089 | <0.001 | 1.485 | 1.178–1.872 | 0.001 |
|
37–200 |
|
|
|
|
|
|
|
>200 |
|
|
|
|
|
|
Survival analysis revealed that patients in the PVR
group had significantly worse survival outcomes compared with
patients in the non-PVR group (mean survival, 25.1 vs. 29.3 months;
P=0.038; Fig. 1). A number of other
factors associated with OS, such as TNM stage, BMI, ALB and LN
metastasis, were further analyzed as indicated in Fig. 1.
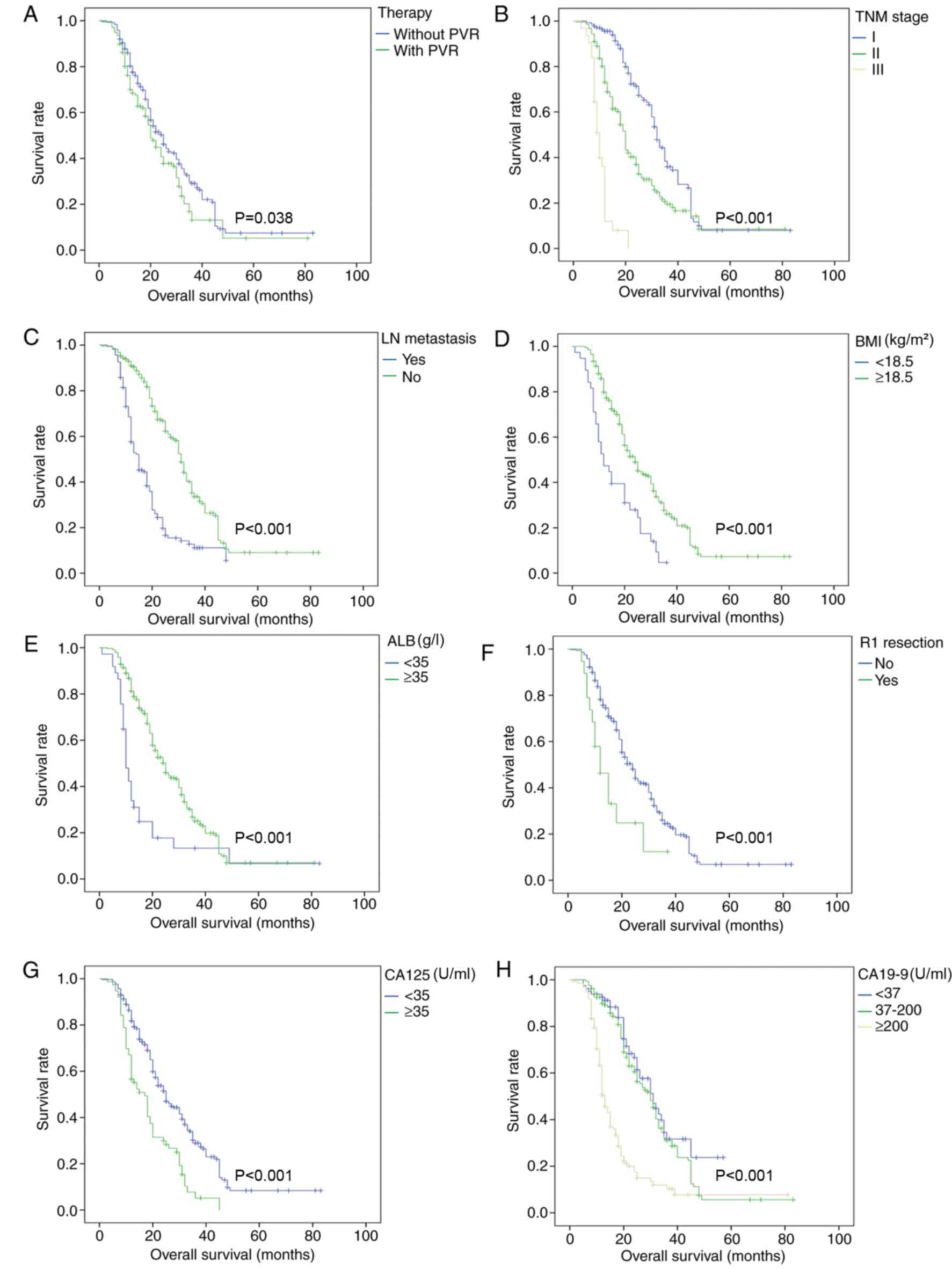 | Figure 1.Overall survival curves before
propensity score matching. Survival analysis was conducted in all
enrolled patients for various factors, including (A) therapy, (B)
TNM stage, (C) lymph node metastasis, (D) BMI (kg/m2),
(E) ALB (g/l), (F) R1 resection (microscopic positive margin), (G)
CA125 (U/ml) and (H) CA19-9 (U/ml) before propensity score
matching. PVR, portal vein resection; TNM, Tumor-Node-Metastasis;
BMI, body mass index; ALB, albumin; CA125, carbohydrate antigen
125; CA19-9, carbohydrate antigen 19-9; LN, lymph node. |
Logistic regression analysis identified two risk
factors that could predict PV invasion: advanced tumor stages (HR,
20.439; 95% CI, 4.166–100.271; P<0.001) and higher CA19-9 levels
(HR, 6.608; 95% CI, 2.064–21.154; P=0.001).
Demographic and clinicopathological
parameters of the included patients after PSM
A total of 123 matched pairs of patients from the
PD+PVR and non-PVR groups were confirmed via PSM based on age, sex
BMI, leukocyte, ALT, TBil, ALB, CA125, CA19-9, tumor stage, LN
metastasis and tumor size. After PSM, a number of factors, which
may imply patients' pre-operative general status and have an effect
on survival, were balanced including age, BMI, ALB, CA125, CA19-9,
tumor stage, LN metastasis and tumor size (Table I).
Survival analysis after PSM
Multivariate Cox regression model showed that
advanced tumor stages, lower BMI levels, R1 resection (microscopic
positive margin), LN metastasis, lower ALB levels, higher CA125 and
CA19-9 levels were independent prognostic factors (Table II).
Survival analysis showed that the survival outcome
of patients in the PD+PVR group was similar to that of patients in
the non-PVR group (mean survival, 25.9 vs. 31.2 months; P=0.364;
Fig. 2). Other factors such as TNM
stage, LN metastasis, BMI, ALB, R1 resection, CA125 and CA19-9
associated with OS were further analyzed and were shown in Fig. 2.
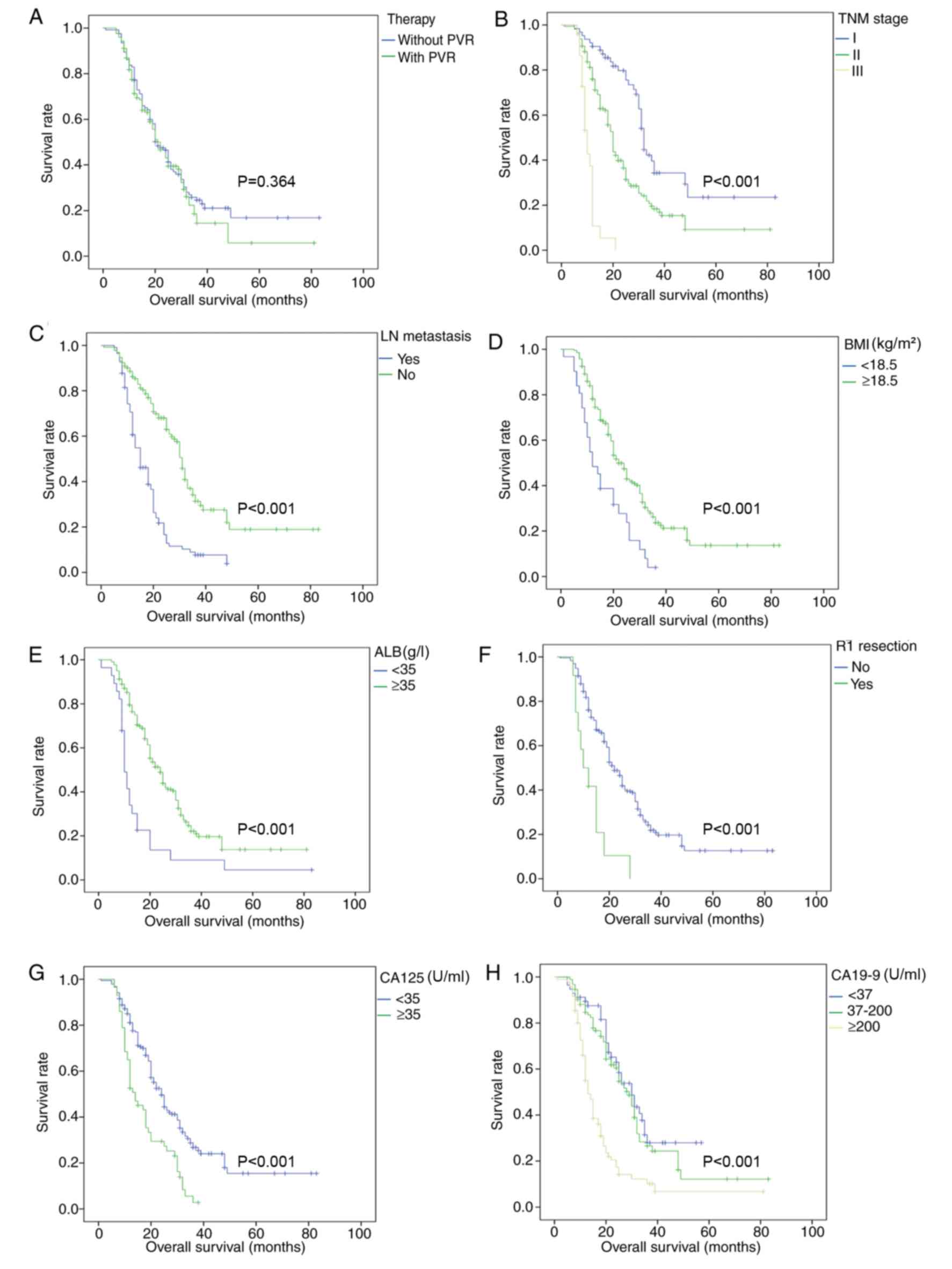 | Figure 2.Overall survival curves after
propensity score matching. Survival analysis was conducted in all
enrolled patients for various factors, including (A) therapy, (B)
TNM stage, (C) lymph node metastasis, (D) BMI (kg/m2),
(E) ALB (g/l), (F) R1 resection (microscopic positive margin), (G)
CA125 (U/ml) and (H) CA19-9 (U/ml) after propensity score matching.
PVR, portal vein resection; TNM, Tumor-Node-Metastasis; BMI, body
mass index; ALB, albumin; CA125, carbohydrate antigen 125; CA19-9,
carbohydrate antigen 19-9; LN, lymph node. |
Logistic regression analysis also identified
advanced tumor stage (HR, 17.827; 95% CI, 3.627–87.627; P<0.001)
and higher CA19-9 levels (HR, 6.913; 95% CI, 2.124–22.503; P=0.001)
as the same two risk factors predicting PV invasion.
Subgroup analysis in the PD+PVR
group
Regardless to prior or latter PSM, patients with PV
invasion, advanced tumor stage, R1 resection, lower BMI levels,
lower ALB levels, LN metastasis, lower CA125 and CA19-9 levels had
poorer prognostic outcomes (Table
SI; Figs. S1 and S2).
Subgroup analysis in non-PVR
group
The results still indicated that patients with
advanced tumor stage, R1 resection, LN metastasis, lower CA125 and
CA19-9 levels had poorer prognostic outcomes, regardless to prior
or latter PSM. Lower ALB levels and lower BMI did not indicate a
worse prognosis in the non-PVR group (Table SII; Figs. S3 and S4).
Postoperative complications
Patients in the PD+PVR group did not have a
significantly higher overall complication rate or more severe
complications compared with patients in the non-PVR group (all
P>0.05). The postoperative complications in PD+PVR and non-PVR
groups were combined and the most frequent complication was POPF
(n=220; 58.4%). Other complications were chylous fistula in 10
patients (2.7%), DGE in 44 patients (11.7%), PPH in 22 patients
(5.8%), wound infection in 47 patients (12.5%), pleural effusion in
67 patients (17.8%) and abdominal infection in 11 patients (2.9%)
before PSM. After PSM, the most frequent combined complication
remained POPF (n=133; 54.1%), and other complications were chylous
fistula in 3 patients (1.2%), DGE in 27 patients (11.0%), PPH in 9
patients (3.7%), wound infection in 25 patients (10.2%), pleural
effusion in 44 patients (17.9%) and abdominal infection in 9
patients (3.7%) (Table III). There
was no 30-day mortality indicated in either group. Furthermore, no
graft infection, thrombosis, or serious graft-related complication
has been reported in patients in the PVR group.
| Table III.Complications of the PVR and non-PVR
groups. |
Table III.
Complications of the PVR and non-PVR
groups.
|
| Before PSM |
| After PSM |
|
|---|
|
|
|
|
|
|
|---|
| Postoperative
complications | PVR group
(n=138) | Non-PVR group
(n=239) | P-value | PVR group
(n=123) | Non-PVR group
(n=123) | P-value |
|---|
| POPF, n (%) |
|
|
|
|
|
|
|
None | 64 (46.4) | 93 (38.9) | 0.456 | 63 (51.3) | 50 (40.7) | 0.365 |
|
Biochemical leak | 49 (35.5) | 96 (40.2) |
| 40 (32.5) | 47 (38.2) |
|
| Grade B
POPF | 23 (16.7) | 48 (20.1) |
| 19 (15.4) | 25 (20.3) |
|
| Grade C
POPF | 2 (1.4) | 2 (0.8) |
| 1 (0.8) | 1 (0.8) |
|
| Chylous fistula, n
(%) |
|
|
|
|
|
|
|
None | 136 (98.6) | 231 (96.6) | 0.702 | 122 (99.2) | 121 (98.4) | >0.999 |
| Grade
A | 0 (0.0) | 1 (0.4) |
| 0 (0.0) | 0 (0.0) |
|
| Grade
B | 2 (1.4) | 7 (3.0) |
| 1 (0.8) | 2 (1.6) |
|
| Grade
C | 0 (0.0) | 0 (0.0) |
| 0 (0.0) | 0 (0.0) |
|
| DGE, n (%) |
|
|
|
|
|
|
|
None | 125 (90.6) | 208 (87.0) | 0.809 | 111 (90.2) | 108 (87.8) | 0.906 |
| Grade
A | 7 (5.1) | 16 (6.7) |
| 7 (5.7) | 8 (6.5) |
|
| Grade
B | 5 (3.6) | 11 (4.6) |
| 4 (3.3) | 6 (4.9) |
|
| Grade
C | 1 (0.7) | 4 (1.7) |
| 1 (0.8) | 1 (0.8) |
|
| PPH, n (%) |
|
|
|
|
|
|
|
None | 132 (95.7) | 223 (93.4) | 0.496 | 119 (96.8) | 118 (96.0) | >0.999 |
| Grade
A | 3 (2.2) | 12 (5.0) |
| 2 (1.6) | 3 (2.4) |
|
| Grade
B | 1 (0.7) | 2 (0.8) |
| 1 (0.8) | 1 (0.8) |
|
| Grade
C | 2 (1.4) | 2 (0.8) |
| 1 (0.8) | 1 (0.8) |
|
| Wound infection, n
(%) |
|
|
|
|
|
|
|
None | 122 (88.4) | 208 (87.0) | 0.697 | 111 (90.2) | 110 (89.4) | 0.833 |
|
Yes | 16 (11.6) | 31 (13.0) |
| 12 (9.8) | 13 (10.6) |
|
| Pleural effusion, n
(%) |
|
|
|
|
|
|
|
None | 112 (81.2) | 198 (82.8) | 0.680 | 102 (82.9) | 100 (81.3) | 0.739 |
|
Yes | 26 (18.8) | 41 (17.2) |
| 21 (17.1) | 23 (18.7) |
|
Discussion
Growing evidence has demonstrated that PV resection
is safe for the treatment of patients with borderline resectable
PDAC (33–35). PD combined with PVR is the only
radical therapy for PDAC patients with PV involvement at present
(7). Our previous study demonstrated
that patients with radical resection of PDAC and PVR had
significantly improved survival compared with patients with
chemotherapy or SB alone (25).
However, other studies drew controversial conclusions after
comparing the survival between patients with PVR and patients
undergoing pancreatectomy alone (7,16,36–44).
This discrepancy between different studies may mainly be due to
huge heterogenicity of patients between the study and control
groups. In the present study, the PSM method was used to balance
the baseline characteristics between the PVR and non-PVR groups,
and it was indicated that patients with PD combined with PVR could
achieve the same survival outcome as patients without PVR.
In patients with PV invasion, tumor cells are more
likely to invade the host stroma, penetrate blood vessels and enter
the circulation to produce metastasis by forming new colonies in
distant organs (45). We hypothesize
that this may be the reason for patients with PVR to have
significantly worse survival outcomes. In the present study, it was
indicated that before PSM, patients in the PVR group had poor
survival outcomes compared with patients in the non-PVR group.
However, it was identified that the poor prognosis may be due to
the fact that patients in the PVR group were accompanied with
higher CA19-9 levels, advanced tumor stages and bigger tumor sizes.
All these factors imply that patients in the PVR group were at a
more advanced stage of the disease, and certainly with a worse
survival outcome (P=0.038). In order to eliminate selection bias
between the two groups, the PSM method was used. After PSM,
although patients in the PVR group still had longer operation
durations and more blood loss, the other factors were balanced as
expected. The patients in the PVR group achieved the same survival
outcomes as the patients in the non-PVR group (P=0.364), indicating
that heterogeneity of the baseline characteristics between the two
groups did have a potential effect on survival. Through PSM, the
current study balanced the heterogeneity and provided a reliable
conclusion.
Other than the unbalanced baseline characteristics,
we hypothesize that the method of resection and reconstruction may
also have an effect on survival. In the present study, the patients
in the PVR group underwent radical resection of the primary PDAC,
PV resection and reconstruction with artificial blood vessels
(ePTFE vascular grafts). For PV reconstruction, self-anastomosis,
autogenous and allograft vessel grafts were used in different
circumstances (25). In the current
study, artificial blood vessels (ePTFE vascular grafts) were used
for reconstruction, in order to achieve the optimum tumor-free
margin. Notably, initial literature research demonstrated that all
studies reporting that patients with PVR, who suffered
significantly poor survival outcomes, were actually studies
reporting that positive surgical margin rate of patients with PVR,
who underwent self-anastomosis for PV reconstruction, was
relatively high (30–50%) (46–48). In
the present study, the R1 resection rate was 3.6% in the PVR group
compared with 5.9% in the non-PVR group (P=0.465). This lower R1
resection rate may to some extent be due to the artificial blood
vessels. With the artificial blood vessels, the tension of the
reconstructed PV and the length of resected PV were no longer a
problem for surgeons during the operation, therefore securing the
radical resection of the primary PDAC and invaded PV. However, this
study did not compare the benefits between autografts and
allografts and therefore further multiple-center studies are
required.
The biggest concern for the use of PVR is safety.
The complications between patients with PVR and patients with no
PVR were compared and it was indicated that regardless of PSM
status, there was no significant difference in the complication
rate in terms of POPF, chylous fistula, DGE, PPH, wound infection,
pleural effusion and abdominal infection between the two groups.
Therefore, this study suggested that PVR did not increase the
incidence of serious surgical complications. Previous studies have
reported that the use of artificial vascular grafts may run a
potential risk of infection and thrombosis (49,50). In
the present study, all patients in PVR group were administrated
aspirin and received ultrasound examinations. To the best of our
knowledge, no graft infection, thrombosis, or serious graft-related
complication has been reported. The aforementioned suggests that PD
combined with PVR and reconstruction with artificial blood vessels
is a safe and viable option for the treatment of patients with PV
invasion.
The biggest limitation of the current study was its
retrospective nature, although attempts were made to reduce or
eliminate the bias by utilizing the PSM method and enlarging the
sample size. It was indicated that the baseline characteristics
were well balanced after using the PSM method. To the best of our
knowledge, there is no prospective study design dealing with this
issue and therefore the present study is the only one to conduct a
comparison between patients with or without PVR using the PSM
method. Secondly, no comparison between patients with autograft and
allograft was conducted in the present study. Future multi-center
research will focus on such clinical experience and perform
respective comparisons.
In conclusion, PVR may offer patients with PV
involvement the same survival outcome as patients without PV
involvement, without increasing the incidence of serious
complications. PVR is a safe and viable option for patients with
PDAC and is effective for patients with PDAC with suspected PV
invasion.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was funded by grants from the
National Natural Science Foundation of China (grant no. 81472221)
and Clinical Key Projects of the National Health and Family
Planning (grant no. Oncology 2013–2015).
Availability of data and materials
All datasets generated and/or analyzed during this
study are included in this article and its supplementary
information file.
Authors' contributions
ZBX and DLF conceived and designed the study. ZBX,
JCG, JL and DLF provided administrative support. JCG, JL, CFZ, CJ
and DLF provided materials and/or patients for the study. ZBX, JCG,
CFZ, CJ and JL were responsible for the collection and assembly of
data. JCG, CFZ, CJ and JL conducted data analysis and
interpretation. ZBX, JCG and JL were responsible for manuscript
writing. All authors have read and approved the version of the
manuscript. All authors agree to be accountable for all aspects of
the work in ensuring that questions related to the accuracy or
integrity of any part of the work are appropriately investigated
and resolved.
Ethics approval and consent to
participate
This study was approved by the Clinical Research
Ethics Committee of Huashan Hospital (Shanghai, China). All
patients provided written informed consent to voluntarily donate
their clinical data and follow-up data for research-related
purposes.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kamisawa T, Wood LD, Itoi T and Takaori K:
Pancreatic cancer. Lancet. 388:73–85. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Winter JM, Cameron JL, Campbell KA, Arnold
MA, Chang DC, Coleman J, Hodgin MB, Sauter PK, Hruban RH, Riall TS,
et al: 1423 pancreaticoduodenectomies for pancreatic cancer: A
single-institution experience. J Gastrointest Surg. 10:1199–1211.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hidalgo M: Pancreatic cancer. N Engl J
Med. 362:1605–1617. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Han SS, Park SJ, Kim SH, Cho SY, Kim YK,
Kim TH, Lee SA, Woo SM, Lee WJ and Hong EK: Clinical significance
of portal-superior mesenteric vein resection in
pancreatoduodenectomy for pancreatic head cancer. Pancreas.
41:102–106. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhang XM, Fan H, Kou JT, Zhang XX, Li P,
Dai Y and He Q: Resection of portal and/or superior mesenteric vein
and reconstruction by using allogeneic vein for pT3 pancreatic
cancer. J Gastroenterol Hepatol. 31:1498–1503. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Allema JH, Reinders ME, van Gulik TM, van
Leeuwen DJ, de Wit LT, Verbeek PC and Gouma DJ: Portal vein
resection in patients undergoing pancreatoduodenectomy for
carcinoma of the pancreatic head. Br J Surg. 81:1642–1646. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tseng JF, Raut CP, Lee JE, Pisters PW,
Vauthey JN, Abdalla EK, Gomez HF, Sun CC, Crane CH, Wolff RA and
Evans DB: Pancreaticoduodenectomy with vascular resection: Margin
status and survival duration. J Gastrointest Surg. 8:935–950. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Müller SA, Hartel M, Mehrabi A, Welsch T,
Martin DJ, Hinz U, Schmied BM and Büchler MW: Vascular resection in
pancreatic cancer surgery: Survival determinants. J Gastrointest
Surg. 13:784–792. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Castleberry AW, White RR, De La Fuente SG,
Clary BM, Blazer DG III, McCann RL, Pappas TN, Tyler DS and
Scarborough JE: The impact of vascular resection on early
postoperative outcomes after pancreaticoduodenectomy: An analysis
of the American College of Surgeons National Surgical Quality
Improvement Program database. Ann Surg Oncol. 19:4068–4077. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Worni M, Castleberry AW, Clary BM, Gloor
B, Carvalho E, Jacobs DO, Pietrobon R, Scarborough JE and White RR:
Concomitant vascular reconstruction during pancreatectomy for
malignant disease: A propensity score-adjusted, population-based
trend analysis involving 10,206 patients. JAMA Surg. 148:331–338.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Roch AM, House MG, Cioffi J, Ceppa EP,
Zyromski NJ, Nakeeb A and Schmidt CM: Significance of portal vein
invasion and extent of invasion in patients undergoing
pancreatoduodenectomy for pancreatic adenocarcinoma. J Gastrointest
Surg. 20:479–487. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhou Y, Zhang Z, Liu Y, Li B and Xu D:
Pancreatectomy combined with superior mesenteric vein-portal vein
resection for pancreatic cancer: A meta-analysis. World J Surg.
36:884–891. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Turrini O, Ewald J, Barbier L, Mokart D,
Blache JL and Delpero JR: Should the portal vein be routinely
resected during pancreaticoduodenectomy for adenocarcinoma? Ann
Surg. 257:726–730. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Selvaggi F, Mascetta G, Daskalaki D, dal
Molin M, Salvia R, Butturini G, Cellini C and Bassi C: Outcome of
superior mesenteric-portal vein resection during pancreatectomy for
borderline ductal adenocarcinoma: Results of a prospective
comparative study. Langenbecks Arch Surg. 399:659–665. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ravikumar R, Sabin C, Abu Hilal M,
Bramhall S, White S, Wigmore S, Imber CJ and Fusai G; UK Vascular
Resection in Pancreatic Cancer Study Group, : Portal vein resection
in borderline resectable pancreatic cancer: A United Kingdom
multicenter study. J Am Coll Surg. 218:401–411. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Giovinazzo F and Turri G: Meta-analysis of
benefits of portal-superior mesenteric vein resection in pancreatic
resection for ductal adenocarcinoma. Br J Surg. 103:179–191. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Capussotti L, Massucco P, Ribero D, Vigano
L, Muratore A and Calgaro M: Extended lymphadenectomy and vein
resection for pancreatic head cancer: Outcomes and implications for
therapy. Arch Surg. 138:1316–1322. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Siriwardana HP and Siriwardena AK:
Systematic review of outcome of synchronous portal-superior
mesenteric vein resection during pancreatectomy for cancer. Br J
Surg. 93:662–673. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kaneoka Y, Yamaguchi A and Isogai M:
Portal or superior mesenteric vein resection for pancreatic head
adenocarcinoma: Prognostic value of the length of venous resection.
Surgery. 145:417–425. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rosenbaum PR and Rubin DB: The central
role of the propensity score in observational studies for causal
effects. Biometrika. 70:41–55. 1983. View Article : Google Scholar
|
|
22
|
Ruzzenente A, Guglielmi A, Sandri M,
Campagnaro T, Valdegamberi A, Conci S, Bagante F, Turcato G,
D'Onofrio M and Iacono C: Surgical resection versus local ablation
for HCC on cirrhosis: Results from a propensity case-matched study.
J Gastrointest Surg. 16:301–311. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Guo Z, Zhong JH, Jiang JH, Zhang J, Xiang
BD and Li LQ: Comparison of survival of patients with BCLC stage A
hepatocellular carcinoma after hepatic resection or transarterial
chemoembolization: A propensity score-based analysis. Ann Surg
Oncol. 21:3069–3076. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhong JH, Ke Y, Gong WF, Xiang BD, Ma L,
Ye XP, Peng T, Xie GS and Li LQ: Hepatic resection associated with
good survival for selected patients with intermediate and
advanced-stage hepatocellular carcinoma. Ann Surg. 260:329–340.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Xie ZB, Gu JC, Zhang YF, Yao L, Jin C,
Jiang YJ, Li J, Yang F, Zou CF and Fu DL: Portal vein resection and
reconstruction with artificial blood vessels is safe and feasible
for pancreatic ductal adenocarcinoma patients with portal vein
involvement: Chinese center experience. Oncotarget. 8:77883–77896.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chun YS, Pawlik TM and Vauthey JN: 8th
edition of the AJCC cancer staging manual: Pancreas and
hepatobiliary cancers. Ann Surg Oncol. 25:845–847. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nakao A, Harada A, Nonami T, Kaneko T,
Inoue S and Takagi H: Clinical significance of portal invasion by
pancreatic head carcinoma. Surgery. 117:50–55. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wente MN, Veit JA, Bassi C, Dervenis C,
Fingerhut A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, Sarr
MG, et al: Postpancreatectomy hemorrhage (PPH): An International
Study Group of Pancreatic Surgery (ISGPS) definition. Surgery.
142:20–25. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Besselink MG, van Rijssen LB, Bassi C,
Dervenis C, Montorsi M, Adham M, Asbun HJ, Bockhorn M, Strobel O,
Büchler MW, et al: Definition and classification of chyle leak
after pancreatic operation: A consensus statement by the
International Study Group on pancreatic surgery. Surgery.
161:365–372. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wente MN, Bassi C, Dervenis C, Fingerhut
A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, Sarr MG,
Traverso LW, et al: Delayed gastric emptying (DGE) after pancreatic
surgery: A suggested definition by the International Study Group of
Pancreatic Surgery (ISGPS). Surgery. 142:761–768. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bassi C, Marchegiani G, Dervenis C, Sarr
M, Abu Hilal M, Adham M, Allen P, Andersson R, Asbun HJ, Besselink
MG, et al: The 2016 update of the International Study Group (ISGPS)
definition and grading of postoperative pancreatic fistula: 11
years after. Surgery. 161:584–591. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Austin PC, Grootendorst P and Anderson GM:
A comparison of the ability of different propensity score models to
balance measured variables between treated and untreated subjects:
A Monte Carlo study. Stat Med. 26:734–753. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Marangoni G, O'Sullivan A, Faraj W, Heaton
N and Rela M: Pancreatectomy with synchronous vascular resection-an
argument in favour. Surgeon. 10:102–106. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sgroi MD, Narayan RR, Lane JS, Demirjian
A, Kabutey NK, Fujitani RM and Imagawa DK: Vascular reconstruction
plays an important role in the treatment of pancreatic
adenocarcinoma. J Vasc Surg. 61:475–480. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Barreto SG and Windsor JA: Justifying vein
resection with pancreatoduodenectomy. Lancet Oncol. 17:e1182016.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yekebas EF, Bogoevski D, Cataldegirmen G,
Kunze C, Marx A, Vashist YK, Schurr PG, Liebl L, Thieltges S, Gawad
KA, et al: En bloc vascular resection for locally advanced
pancreatic malignancies infiltrating major blood vessels:
Perioperative outcome and long-term survival in 136 patients. Ann
Surg. 247:300–309. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Turley RS, Peterson K, Barbas AS, Ceppa
EP, Paulson EK, Blazer DG III, Clary BM, Pappas TN, Tyler DS,
McCann RL and White RR: Vascular surgery collaboration during
pancreaticoduodenectomy with vascular reconstruction. Ann Vasc
Surg. 26:685–692. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Cheung TT, Poon RT, Chok KS, Chan AC,
Tsang SH, Dai WC, Chan SC, Fan ST and Lo CM:
Pancreaticoduodenectomy with vascular reconstruction for
adenocarcinoma of the pancreas with borderline resectability. World
J Gastroenterol. 20:17448–17455. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Jeong J, Choi DW, Choi SH, Heo JS and Jang
KT: Long-term outcome of portomesenteric vein invasion and
prognostic factors in pancreas head adenocarcinoma. ANZ J Surg.
85:264–269. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Elberm H, Ravikumar R, Sabin C, Abu Hilal
M, Al-Hilli A, Aroori S, Bond-Smith G, Bramhall S, Coldham C,
Hammond J, et al: Outcome after pancreaticoduodenectomy for T3
adenocarcinoma: A multivariable analysis from the UK vascular
resection for pancreatic cancer study group. Eur J Surg Oncol.
41:1500–1507. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Kulemann B, Hoeppner J, Wittel U, Glatz T,
Keck T, Wellner UF, Bronsert P, Sick O, Hopt UT, Makowiec F and
Riediger H: Perioperative and long-term outcome after standard
pancreaticoduodenectomy, additional portal vein and multivisceral
resection for pancreatic head cancer. J Gastrointest Surg.
19:438–444. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Wang WL, Ye S, Yan S, Shen Y, Zhang M, Wu
J and Zheng SS: Pancreaticoduodenectomy with portal vein/superior
mesenteric vein resection for patients with pancreatic cancer with
venous invasion. Hepatobiliary Pancreat Dis Int. 14:429–435. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Beltrame V, Gruppo M, Pedrazzoli S,
Merigliano S, Pastorelli D and Sperti C: Mesenteric-Portal vein
resection during pancreatectomy for pancreatic cancer.
Gastroenterol Res Pract. 2015:6597302015. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Fang JZ, Lu CD, Wu SD, Huang J and Zhou J:
Portal vein/superior mesenteric vein resection in pancreatic cancer
treatment in the elderly. Medicine (Baltimore). 96:e73352017.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Prakash LR, Wang H, Zhao J,
Nogueras-Gonzalez GM, Cloyd JM, Tzeng CD, Kim MP, Lee JE and Katz
MHG: Significance of cancer cells at the vein edge in patients with
pancreatic adenocarcinoma following pancreatectomy with vein
resection. J Gastrointest Surg. Feb 28–2019.Doi:
10.1007/s11605-019-04126-y (Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Murakami Y, Satoi S, Motoi F, Sho M, Kawai
M, Matsumoto I and Honda G; Multicentre Study Group of
Pancreatobiliary Surgery (MSG-PBS), : Portal or superior mesenteric
vein resection in pancreatoduodenectomy for pancreatic head
carcinoma. Br J Surg. 102:837–846. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Murakami Y, Uemura K, Sudo T, Hashimoto Y,
Nakashima A, Kondo N, Nakagawa N and Sueda T: Benefit of portal or
superior mesenteric vein resection with adjuvant chemotherapy for
patients with pancreatic head carcinoma. J Surg Oncol. 107:414–421.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Shimada K, Sano T, Sakamoto Y and Kosuge
T: Clinical implications of combined portal vein resection as a
palliative procedure in patients undergoing pancreaticoduodenectomy
for pancreatic head carcinoma. Ann Surg Oncol. 13:1569–1578. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Dang XW, Xu PQ and Ma XX: Splenocaval
versus mesocaval shunt with artificial vascular graft for the
treatment of Budd-Chiari syndrome. Hepatobiliary Pancreat Dis Int.
4:68–70. 2005.PubMed/NCBI
|
|
50
|
Katayama Y, Minato N, Kawasaki H and
Sakaguchi M: Surgical strategy for impending rupture of an infected
anastomotic pseudoaneurysm of the aorta 9 years after a Bentall
procedure: Radical surgery involving en bloc resection of the
infected sternum, pseudoaneurysm, and artificial vascular graft.
Gen Thorac Cardiovasc Surg. 56:584–588. 2008. View Article : Google Scholar : PubMed/NCBI
|














