Introduction
Oral cancer is one of the most aggressive, invasive
and deforming diseases. Therapeutic treatment results in the
functional impairment of vital functions of the human body, such as
swallowing, chewing and speech. Human papilloma virus
(HPV)-associated squamous cell carcinomas represent >90% of oral
mucosa neoplasms (1,2). Considering the increased metastatic
potential and the relatively unpredictable evolution of oral
squamous cell carcinoma (OSCC), even following successful treatment
(3), the discovery of novel and
precise diagnostic tools with which to identify OSCCs in the early
stages, should be prioritized in order to increase the therapeutic
potential and reduce disease progression and/or metastasis. The
conventional treatment of OSCC includes surgery (excision of the
primary tumor, associated with radical neck dissection for lymph
node involvement, based on clinical and surgical findings),
radiation therapy (external beam radiotherapy and/or
brachytherapy), and coadjutant therapy (chemotherapy with agents
such as cisplatin, carboplatin, 5-fluorouracil, paclitaxel and
docetaxel) (4). In oral mucosal
lesions, novel therapeutic modalities with natural compounds can be
used as a complementary therapy for standard treatment (5–7).
Untreated oral cavity tumors develop both locally and distant
severe complications, such as fistulas, increasing the risk of
aspiration, as well as challenging the treatment of bacterial and
fungal infections (8,9).
Previous studies have indicated that melatonin may
have oncostatic properties by altering the angiogenic mechanisms or
metastatic and proliferative properties of a number of cancer
types, including OSCC (10–12). Melatonin
(N-acetyl-5-methoxytryptamine) is an indolic compound
primarily secreted by the pineal gland in response to darkness
signals (13–15), although small amounts may be excreted
by the retina, the gastrointestinal tract, the skin, the bone
marrow (16) and the salivary glands
(17). Isola and Lilliu (18) analyzed fragments of salivary glands
obtained from male patients undergoing oral tumor resection surgery
and demonstrated melatonin subcellular localization in the
significant human salivary gland parenchyma (parotid, submandibular
and sublingual). There is also evidence to indicate the beneficial
and protective effects of melatonin, such as its antioxidant,
anti-inflammatory and anti-microbial effects on the oral mucosa
(10–12,19–21).
It was thus hypothesized that decreased circulating
melatonin levels could be observed in patients with cancer of the
oral cavity. The present study was thus carried out in order to
identify the clinical significance of serum melatonin
concentrations in predicting the severity of OSCC.
Patients and methods
Patients
A total of 40 male subjects with OSCC (aged 57±7
years) undergoing surgery at the Coltea Clinical Hospital,
Bucharest, Romania, between November, 2014 and March, 2015, were
included in this study. Clinical data were collected from the
patients' medical records. All patients had pathological
confirmation for diagnostic assessment, according to the 8th
Edition of the American Joint Cancer Committee (AJCC) Cancer
Staging Manual (22), which provides
a much more accurate and reasonable prediction of survival for
newly diagnosed subjects with OSCC than the previous edition. This
updated classification system has developed a modified staging
system that integrates the depth of invasion (DOI) into the tumor
size (T) category. Including DOI in the oral cavity better
discriminates the higher risk small cancers, as demonstrated by
deeply invasive tumors from those with less invasive cancers that
have an excellent prognosis (23).
For example, a patient with a tumor with a diameter of 2 cm and two
positive lymph nodes, diagnosed with tonsil cancer at stage IV
according to the 7th Edition, will be diagnosed with stage I
disease according to the 8th Edition. New cut-offs for the size and
extension of the tumor are 4 cm for size and 10 mm for depth.
According to these boundary lines, patients with OSCC were divided
into two subgroups as follows: T-DOI I [small tumors with less
invasive lesions (T ≤4 cm; DOI ≤10 mm)] and T-DOI II [large tumors
with invasive depth (T >4 cm; DOI >10 mm)]. The histological
grading of the tumors was performed according to the WHO
Classification of Head and Neck Tumors (24).
In addition, 30 healthy male subjects (aged 56±5
years) with no clinical evidence of ear, nose and throat disorders
were randomly selected over the same time period. OSCC is more
common among males than females, with a ratio ranging from 2:1 to
4:1 (22). Thus, only male subjects
were included in this study (patients and control groups) to avoid
inter sex-related variations (25,26).
All the procedures were performed, respecting the
principles outlined in the Declaration of Helsinki and were
approved by the Coltea Clinical Hospital Ethics Committee. Written
informed consent was obtained from each patient and volunteer prior
to sample collection.
Blood sample collection and
processing
Due to the fact that melatonin is a molecule
involved in the circadian and seasonal rhythm regulation of
physiological functions, including blood pressure and sleep timing,
blood collection was performed under the same conditions for both
patients and controls: Cold season (melatonin levels are higher in
the autumn and winter, when nights are longer than in the spring
and summer) and early in the morning, at 7 a.m. Fasting blood
specimens were collected prior to surgery by venipuncture into
Vacuette® polyethylene terephthalate glycol clot
activator tubes (Greiner Bio-One). Serum samples were obtained by
clotting (30 min, room temperature) and centrifugation (3,000 × g
for 10 min at 4°C), after which they were aliquoted into labeled
cryo-vials and frozen at −80°C for a variable period of a maximum
of 12 months.
Melatonin pre-purification by
solid-phase extraction
Since melatonin levels recorded in the morning are
low, its proper extraction from the blood is essential. In the
serum samples, melatonin was extracted through C18 columns from
R-Biopharm AG, with a recovery ranging from 87.5 to 94.8% for 10 to
200 pg melatonin/ml. The solid-phase extraction procedure consisted
of the following steps: Column conditioning (1 ml of water and 1 ml
of pure methanol), sample application [0.5 ml serum sample was
passed through a C18 column, which was then washed with 0.5 ml of
water and 2 ml of water-methanol (90:10, v/v)], elution of extract
(melatonin was eluted from the column with pure methanol),
evaporation and reconstitution of extract [the eluate was
evaporated to dryness, stored at 2–8°C until the following day (for
up to 24 h), and subsequently resuspended in 0.15 ml water for the
measurement of melatonin levels]. Melatonin pre-purification from
serum samples was essential for a better sensitivity of the
analysis method. The procedure described above allowed for the
detection of melatonin with high sensitivity and without
interference from other components in the sample.
Detection of serum melatonin by
enzyme-linked immunosorbent assay (ELISA)
Furthermore, the serum concentrations of melatonin
were measured using a commercially available quantitative ELISA kit
from DRG International, Inc. The lower limit of detection was 1.6
pg/ml. The sample contamination can cause falsely elevated
concentrations. As melatonin is also present in saliva, protective
measures were taken to prevent the contamination of the kit
reagents while running the tests. The assay was performed in
duplicate, following the manufacturer's recommendations.
Statistical analysis
Statistical analysis was performed using Statistica
8.0 software. Quantitative data are presented as the median
[interquartile range (IQR) 25–75%], while qualitative data as
numbers and percentages (%). Fisher's exact test was used for the
nominal data. The distribution of all variables was verified with
the Kolmogorov-Smirnov test. The non-parametric Kruskal-Wallis test
was used to compare the distribution of continuous variables
between different categories for independent samples (subgroups:
T-DOI I vs. T-DOI II; N0 vs. N1 + N2 + N3 or G1 vs. G2 vs. G3).
Pairwise comparisons with post hoc Bonferroni corrections were used
with the Kruskal-Wallis test. The cut-off value of serum melatonin
was calculated using the receiver operating characteristic (ROC)
curve with its validity parameters (sensitivity and specificity).
The area under the ROC curve (AUC) was used to assess the
diagnostic performance of melatonin in OSCC. The total AUC is an
overall summary of diagnostic accuracy as follows: An AUC >0.9
indicates an excellent diagnostic accuracy, an AUC between 0.7 and
0.9 indicates a good diagnostic accuracy, an AUC between 0.5 and
0.7 indicates a poor diagnostic accuracy, and an AUC <0.5
indicates the lack of a diagnostic value of the biomarker. For all
tests, a value of P<0.05 was considered to indicate a
statistically significant difference.
Results
Melatonin concentration is lower in
patients with OSCC than in healthy controls
The main clinical and histopathological
characteristics of the study subjects are presented in Table I. No significant differences were
observed between the ages of the patients and the controls
(P=0.13), whereas a significant difference was noted between the
risk factors in the two groups (P<0.001). As shown in Table I, 62.5% of patients were classified
as T-DOI II, while the remaining patients were classified as T-DOI
I. According to the tumor grading system, 55% of the patients had
well-differentiated tumors (G1), 20% moderately-differentiated (G2)
and 25% poorly-differentiated tumors (G3). The circulating levels
of melatonin were significantly lower in the patients with OSCC
than in the healthy controls (18.2 vs. 47.6 pg/ml, P<0.001).
Furthermore, within the OSCC group (Table II), the melatonin concentrations
were significantly lower in the T-DOI II subgroup than in the T-DOI
I group (P=0.012) and were also lower in the positive lymph nodes
subgroup than in the negative lymph node one (P<0.001). No
statistically significant differences were observed in the serum
levels of melatonin between the G1, G2 or G3 subgroups of
patients.
 | Table I.Clinical and histopathological
characteristics of patients with OSCC and healthy controls. |
Table I.
Clinical and histopathological
characteristics of patients with OSCC and healthy controls.
|
| Patients with
OSCC | Healthy
controls | P-value |
|---|
|
|
|
|
|
|---|
| Patient
characteristic | n=40 |
| % | n=30 |
| % |
|
|---|
| Mean age
(years) |
| 57±7 |
|
| 56±5 |
| 0.130 |
| Risks factors |
|
|
|
|
|
|
|
| Tobacco
consumption | 38 |
| 95.0 | 4 |
| 13.3 | <0.001 |
| Alcohol
consumption | 32 |
| 80.0 | 0 |
| 0 | <0.001 |
| Location of
tumor |
|
|
|
|
|
|
|
| Base of
tongue | 18 |
| 45.0 | − |
| − | − |
|
Tonsil | 15 |
| 37.5 | − |
| − | − |
|
Tongue | 5 |
| 12.5 | − |
| − | − |
|
Lip | 2 |
| 5.0 | − |
| − | − |
| Tumor
differentiation grading |
|
|
|
|
|
|
|
| G1 | 22 |
| 55.0 | − |
| − | − |
| G2 | 8 |
| 20.0 | − |
| − | − |
| G3 | 10 |
| 25.0 | − |
| − | − |
| Tumor size-depth of
invasion |
|
|
|
|
|
|
|
| T-DOI I
(T ≤4 cm; DOI ≤10 mm) | 15 |
| 37.5 | − |
| − | − |
| T-DOI
II (T >4 cm; DOI >10 mm) | 25 |
| 62.5 | − |
| − | − |
| Lymph node
involvement |
|
|
|
|
|
|
|
|
Negative (N0) | 17 |
| 42.5 | − |
| − | − |
|
Positive (N1 + N2 + N3) | 23 |
| 57.5 | − |
| − | − |
| Melatonin
(pg/ml)a |
| 18.2
(11.0–39.2) |
|
| 47.6
(37.7–66.4) |
| <0.001 |
| Table II.Association between melatonin and
histopathological features in OSCC patients. |
Table II.
Association between melatonin and
histopathological features in OSCC patients.
|
| T-DOI |
| Nodal
involvement |
|
Differentiationb |
|---|
|
|
|
|
|
|
|
|---|
| Variable | T-DOI I n=15 | T-DOI II n=25 | P-value | No n=17 | Yes n=23 | P-value | G1 n=22 | G2 n=8 | G3 n=10 |
|---|
| Melatonin
(pg/ml)a | 36.8 | 13.4 | 0.012 | 37.9 | 12.4 | <0.001 | 21.4 | 14.3 | 18.5 |
|
| (14.5–46.7) | (9.4–28.9) |
| (21.5–46.7) | (9.4–22.3) |
| (13.1–42.7) | (9.0–30.0) | (9.4–38.6) |
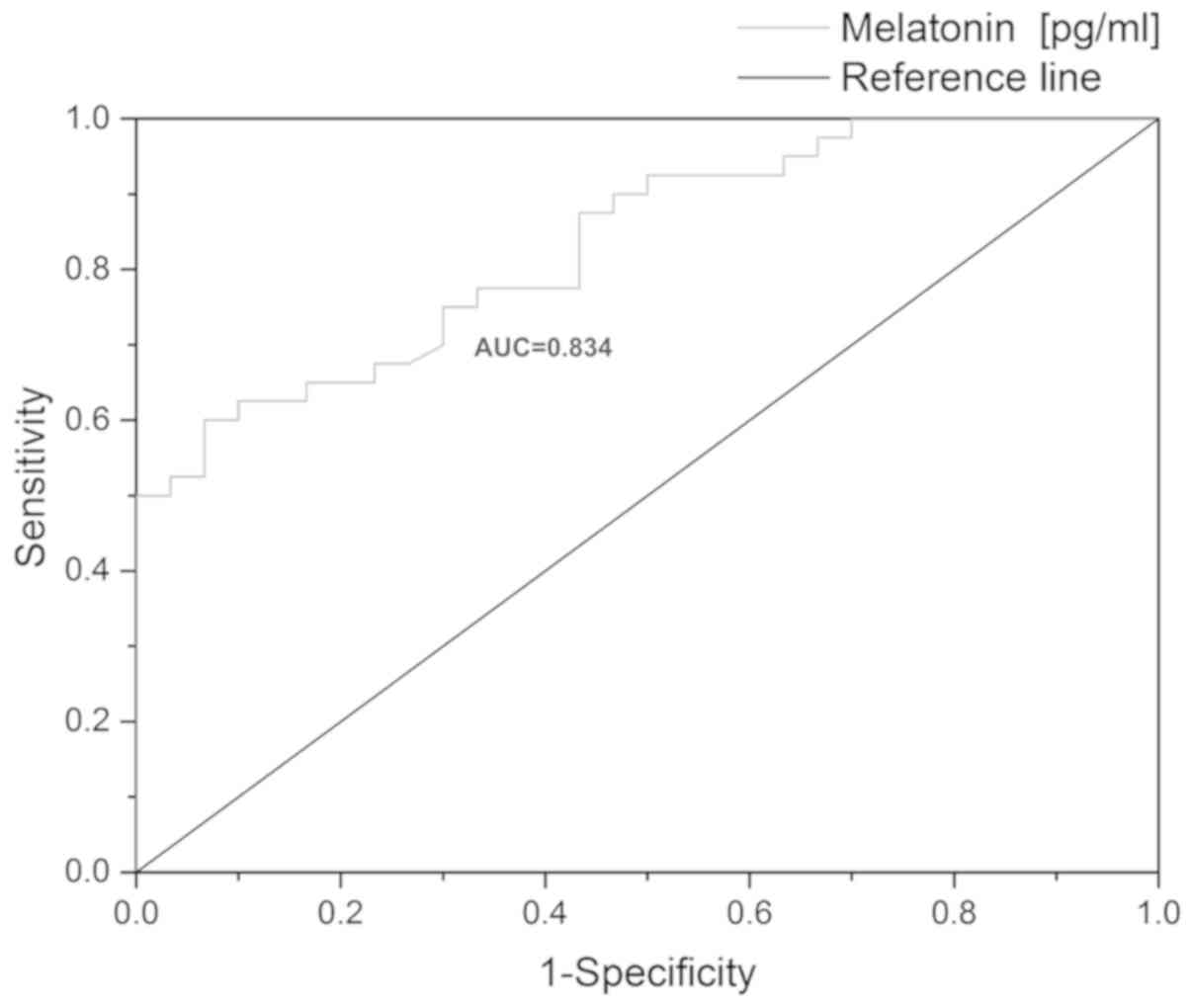
Melatonin concentration-based AUC may
discriminate patients with OSCC from healthy controls
As shown in Fig. 1,
the AUC value for discriminating patients with OSCC from healthy
controls was high (0.834). The subjects with serum melatonin levels
<38.9 pg/ml had an increased risk of OSCC incidence
(sensitivity, 75%; specificity, 76.6%).
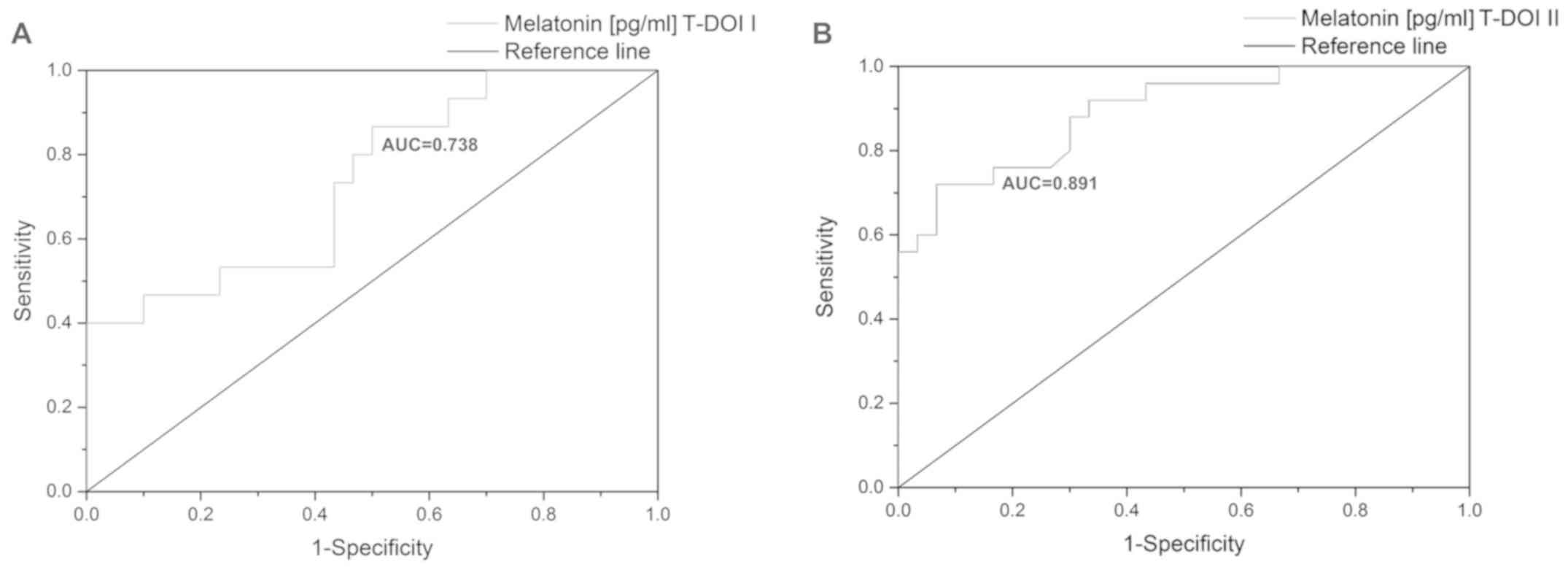
Melatonin has the highest predictive
accuracy for discriminating patients with OSCC with T-DOI II from
healthy controls
The potential utility of melatonin for
discriminating patients with OSCC with T-DOI II and T-DOI I from
the healthy controls is presented in Fig. 2. It was found that the predictive
accuracy of serum melatonin for discriminating subjects with T-DOI
II from the healthy controls was higher than that for
discriminating subjects with T-DOI I from the healthy controls (AUC
=0.891 vs. AUC =0.738).
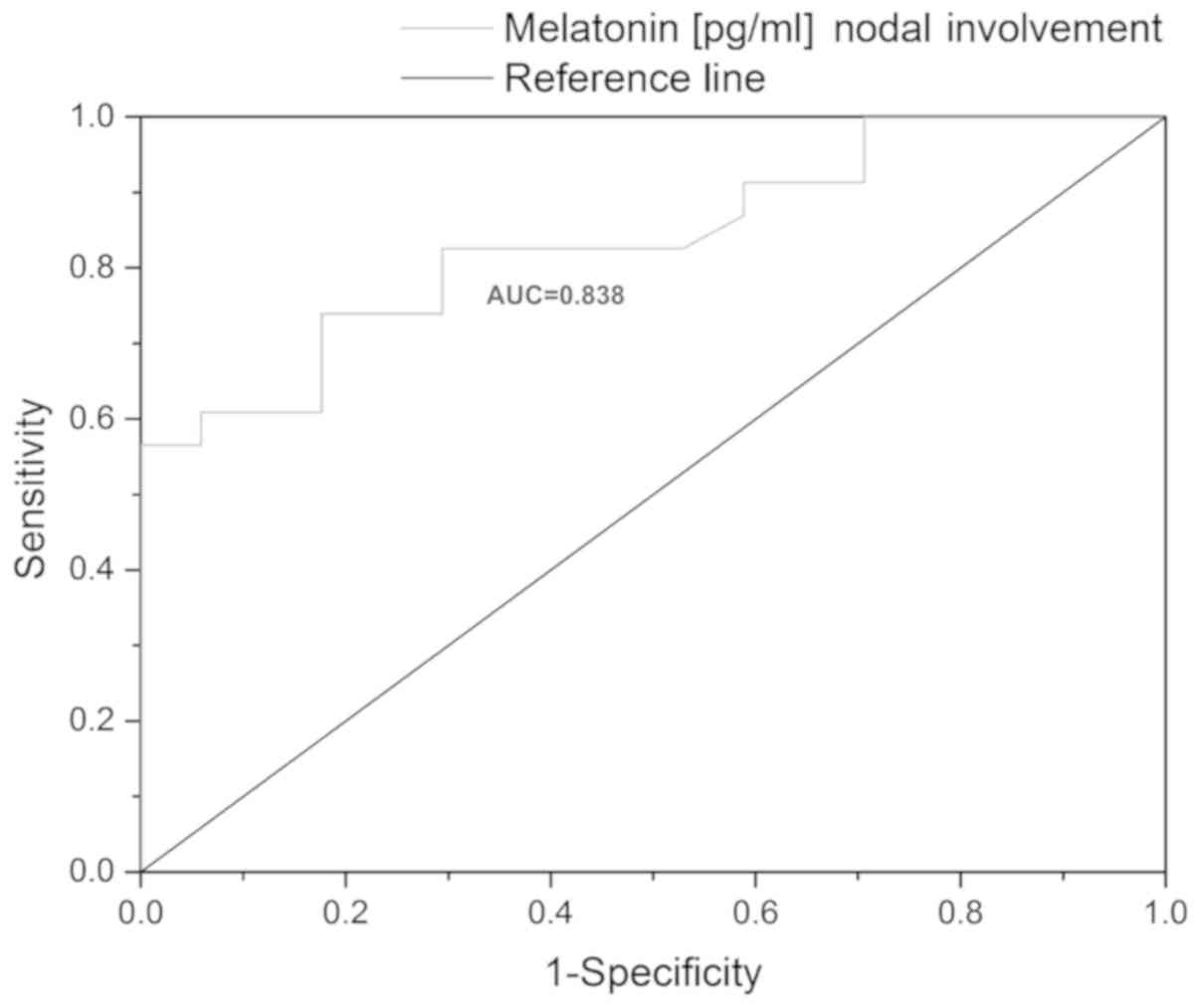
Melatonin concentration-based AUC may
discriminate patients with nodal metastasis from those without
nodal metastasis
As shown in Fig. 3,
the predictive accuracy of serum melatonin for discriminating
subjects with nodal metastasis from those without nodal metastasis
was high (AUC =0.838).
Discussion
The main findings of the current study were the
following: i) The serum melatonin concentration was significantly
lower in the patients with OSCC than in the healthy controls; ii)
the melatonin concentration-based AUC may discriminate patients
with OSCC with T-DOI II from healthy controls; iii) the melatonin
concentration-based AUC may distinguish patients with nodal
metastasis from those without nodal metastasis.
Decreased circulating levels of melatonin have been
associated with a high risk of breast (27,28),
prostate (29), ovarian (30), or oral cancer (10–12,19,20,31–33). In
line with these observations, the findings of this study
demonstrated that the serum melatonin concentrations were
significantly lower in patients with OSCC compared to the healthy
controls (18.2 vs. 47.6 pg/ml, P<0.001). Moreover, the median
circulating melatonin concentrations in the T-DOI I (≤36.8 pg/ml)
or negative lymph node (≤37.9 pg/ml) subgroups of patients with
OSCC (Table II) were similar to
those obtained in the study by Yang et al (27) in breast cancer patients (≤39.5
pg/ml).
The ROC curve is the most useful tool with which to
evaluate the melatonin diagnostic utility in different diseases.
The AUC can range from 0.5 to 1, with values close to 1 indicating
a high discriminatory ability. In this study, the AUC (0.834) and
cut-off level (38.9 pg/ml) for patients with OSCC were similar to
those measured in previous studies for systemic lupus erythematosus
(AUC =0.710, cut-off =18.51 pg/ml) (34) and breast cancer (AUC =0.72672,
cut-off =39.5 pg/ml) (27).
The results of the present study demonstrated that
the under expression of melatonin was related to large invasive
tumors (T-DOI II). It was found that serum melatonin had the
highest predictive accuracy for discriminating patients with OSCC
with T-DOI II from healthy controls (AUC =0.891) (Fig. 2B). In line with this study, several
authors (10–12) have reported an inverse association
between melatonin and the clinicopathological features of OSCC.
Local or distant metastases are aggressive hallmarks
of OSCC. As regards metastatic dissemination to regional lymph
nodes, in this study, melatonin was inversely associated with the
presence of lymph node metastases in patients with OSCC (Table II). Therefore, the potential utility
of melatonin for predicting the presence or absence of lymph node
metastasis was analyzed using the ROC curve. The results revealed
that the melatonin concentration-based AUC (0.838) may discriminate
patients with nodal metastasis from those without nodal
metastasis.
These findings highlight the importance of the human
endocrine system in the progression of OSCC (T-DOI II vs. T-DOI I
and positive lymph-nodes vs. negative lymph-nodes). In addition,
the findings of the present study are in line with those of other
studies that depict the high importance of determining the
melatonin serum concentration as a robust and reliable biochemical
marker in the prevention, diagnosis and evolution assessment of
different physiological or pathological conditions (35–38). The
results are based on an individual proficient and high-fidelity
profile that is accurately modified on a daily circadian base, due
to normal activities and light-dark cycles, modulating almost
entirely the endocrine human environment. Moreover, melatonin may
be a marker of physiological aging, pregnancy, oxidative stress
imbalances, or a clinically relevant consequence of a series of
diseases (35,39,40).
The main limitation of this study is related to the
small number of patients included. However, despite the small
sample size, a homogenous population was used, represented only by
males in both groups. The samples were collected in the same season
(winter), and at the same time in the morning, to discard an
artefactual effect.
In conclusion, the findings of this study suggest
that serum melatonin concentrations are closely related to the
severity of OSCC and may be used to assess different stages of oral
cancer progression objectively and accurately. The present study
indicates that melatonin may be a predictive biomarker for OSCC
metastasis and a potential therapeutic agent for OSCC
prevention-progression. The results of the current study however,
need to be reinforced by further studies using larger study
populations.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included within the manuscript.
Authors' contributions
The manuscript was written through contributions of
all authors. All authors have given approval to the final version
of the manuscript. AES, AZCA and DCG conceived and planned the
experiments. AZCA and DCG collected data. Experiments were
performed by AES. AES and MMS performed statistical analysis of the
results. AES, AZCA, MMS, APS, VJ, CN, AB, TSP, ALA, CMD, RH, ACN,
MG, DCG, DAS, AT, MP and ND contributed to the interpretation of
the results. AES took the lead in writing the manuscript. AES,
AZCA, MMS, APS, VJ, CN, AB, TSP, ALA, CMD, RH, ACN, MG, DCG, DAS,
AT, MP and ND provided critical feedback and helped shape the
research, analysis, and manuscript. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
The study conformed to the principles outlined in
the Declaration of Helsinki and was approved by the Coltea Clinical
Hospital ethics committee. Enrolled patients and volunteers signed
an informed consent.
Patient consent for publication
Not applicable.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this article.
All the other authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
Statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Boda D, Docea AO, Calina D, Ilie MA,
Caruntu C, Zurac S, Neagu M, Constantin C, Branisteanu DE,
Voiculescu V, et al: Human papilloma virus: Apprehending the link
with carcinogenesis and unveiling new research avenues (Review).
Int J Oncol. 52:637–655. 2018.PubMed/NCBI
|
|
3
|
Thomson PJ: Perspectives on oral squamous
cell carcinoma prevention-proliferation, position, progression and
prediction. J Oral Pathol Med. 47:803–807. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Stanciu AE, Zamfir-Chiru-Anton A, Stanciu
MM, Popescu CR and Gheorghe DC: Imbalance between matrix
metalloproteinases and tissue inhibitors of metalloproteinases
promotes invasion and metastasis of head and neck squamous cell
carcinoma. Clin Lab. 63:1613–1620. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Salehi B, Lopez-Jornet P, Pons-Fuster
López E, Calina D, Sharifi-Rad M, Ramírez-Alarcón K, Forman K,
Fernández M, Martorell M, Setzer WN, et al: Plant-derived
bioactives in oral mucosal lesions: A key emphasis to curcumin,
lycopene, chamomile, aloe vera, green tea and coffee properties.
Biomolecules. 9:1062019. View Article : Google Scholar
|
|
6
|
Sani TA, Mohammadpour E, Mohammadi A,
Memariani T, Vatanchian Yazd M, Rezaee R, Calina D, Docea AO,
Goumenou M, Etemad L, et al: Cytotoxic and apoptogenic properties
of Dracocephalum kotschyi aerial part different fractions on
calu-6 and mehr-80 lung cancer cell lines. Farmacia. 65:189–199.
2017.
|
|
7
|
Hsieh MJ, Chen YH, Lee IN, Huang C, Ku YJ
and Chen JC: Secreted amphiregulin promotes vincristine resistance
in oral squamous cell carcinoma. Int J Oncol. 55:949–959.
2019.PubMed/NCBI
|
|
8
|
Ungureanu A, Zlatian O, Mitroi G, Drocaş
A, Ţîrcă T, Călina D, Dehelean C, Docea AO, Izotov BN, Rakitskii
VN, et al: Staphylococcus aureus colonisation in patients from a
primary regional hospital. Mol Med Rep. 16:8771–8780. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zlatian O, Balasoiu AT, Balasoiu M,
Cristea O, Docea AO, Mitrut R, Spandidos DA, Tsatsakis AM, Bancescu
G and Calina D: Antimicrobial resistance in bacterial pathogens
among hospitalised patients with severe invasive infections. Exp
Ther Med. 16:4499–4510. 2018.PubMed/NCBI
|
|
10
|
Yeh CM, Lin CW, Yang JS, Yang WE, Su SC
and Yang SF: Melatonin inhibits TPA-induced oral cancer cell
migration by suppressing matrix metalloproteinase-9 activation
through the histone acetylation. Oncotarget. 7:21952–21967. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lu H, Wu B, Ma G, Zheng D, Song R, Huang
E, Mao M and Lu B: Melatonin represses oral squamous cell carcinoma
metastasis by inhibiting tumor-associated neutrophils. Am J Transl
Res. 9:5361–5374. 2017.PubMed/NCBI
|
|
12
|
Yang CY, Lin CK, Tsao CH, Hsieh CC, Lin
GJ, Ma KH, Shieh YS, Sytwu HK and Chen YW: Melatonin exerts
anti-oral cancer effect via suppressing LSD1 in patient-derived
tumor xenograft models. Oncotarget. 8:33756–33769. 2017.PubMed/NCBI
|
|
13
|
James P, Bertrand KA, Hart JE,
Schernhammer ES, Tamimi RM and Laden F: M and Laden F: Outdoor
light at night and breast cancer incidence in the Nurses' Health
Study II. Environ Health Perspect. 125:0870102017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Papantoniou K, Pozo OJ, Espinosa A, Marcos
J, Castaño-Vinyals G, Basagaña X, Juanola Pagès E, Mirabent J,
Martín J, Such Faro P, et al: Increased and mistimed sex hormone
production in night shift workers. Cancer Epidemiol Biomarkers
Prev. 24:854–863. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Voiculescu SE, Le Duc D, Roșca AE, Zeca V,
Chiţimuș DM, Arsene AL, Drăgoi CM, Nicolae AC, Zăgrean L,
Schöneberg T, et al: Behavioral and molecular effects of prenatal
continuous light exposure in the adult rat. Brain Res. 1650:51–59.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Acuña-Castroviejo D, Escames G, Venegas C,
Díaz-Casado ME, Lima-Cabello E, López LC, Rosales-Corral S, Tan DX
and Reiter RJ: Extrapineal melatonin: Sources, regulation, and
potential functions. Cell Mol Life Sci. 71:2997–3025. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Isola M, Ekström J, Isola R and Loy F:
Melatonin release by exocytosis in the rat parotid gland. J Anat.
234:338–345. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Isola M and Lilliu MA: Melatonin
localization in human salivary glands. J Oral Pathol Med.
45:510–515. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cengiz MI, Cengiz S and Wang HL: Melatonin
and oral cavity. Int J Dent. 2012:4918722012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gómez-Moreno G, Guardia J, Ferrera MJ,
Cutando A and Reiter RJ: Melatonin in diseases of the oral cavity.
Oral Dis. 16:242–247. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dragoi CM, Nicolae AC, Dumitrescu IB, Popa
DE, Ritivoiu M and Arsene AL: DNA targeting as a molecular
mechanism underlying endogenous indoles biological effects.
Farmacia. 67:367–377. 2019. View Article : Google Scholar
|
|
22
|
AJCC Cancer Staging Manual, ; Amin MB,
Edge SB, Greene FL, et al: 8th. Springer; New York, NY: 2017
|
|
23
|
Lydiatt WM, Patel SG, O'Sullivan B,
Brandwein MS, Ridge JA, Migliacci JC, Loomis AM and Shah JP: Head
and neck cancers-major changes in the American Joint Committee on
cancer eighth edition cancer staging manual. CA Cancer J Clin.
67:122–137. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
El-Naggar AK, Chan JK, Grandis JR, Takata
T and Slootweg PJ: WHO Classification of Head and Neck Tumours. WHO
Classification of Tumours. 9. 4th. WHO Press; Geneva: 2017
|
|
25
|
Stanciu AE, Vatasescu RG, Stanciu MM,
Serdarevic N and Dorobantu M: The role of pro-fibrotic biomarkers
in paroxysmal and persistent atrial fibrillation. Cytokine.
103:63–68. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tulin A, Slavu I, Tulin R, Alecu L, Jecan
RC, Orlov C, Iaciu CI, Stanculeanu DL, Hainarosie R, Pituru S, et
al: Does sex of the patient play a role in survival for MSI
colorectal cancer? J Mind Med Sci. 5:102–108. 2018. View Article : Google Scholar
|
|
27
|
Yang WS, Deng Q, Fan WY, Wang WY and Wang
X: Light exposure at night, sleep duration, melatonin, and breast
cancer: A dose-response analysis of observational studies. Eur J
Cancer Prev. 23:269–276. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Minea LN, Stanculeanu DL, Cringeanu A and
Anghel RM: Capecitabine monotherapy for elderly patients with
metastatic breast cancer. J Clin Oncol. 22 (Suppl 14):7972004.
View Article : Google Scholar
|
|
29
|
Tai SY, Huang SP, Bao BY and Wu MT:
Urinary melatonin-sulfate/cortisol ratio and the presence of
prostate cancer: A case-control study. Sci Rep. 6:296062016.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhao M, Wan J, Zeng K, Tong M, Lee AC,
Ding J and Chen Q: The reduction in circulating melatonin level may
contribute to the pathogenesis of ovarian cancer: A retrospective
study. J Cancer. 7:831–836. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Cutando A, López-Valverde A, DE Vicente J,
Gimenez JL, Carcía IA and DE Diego RG: Action of melatonin on
squamous cell carcinoma and other tumors of the oral cavity
(Review). Oncol Lett. 7:923–926. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Fan T, Pi H, Li M, Ren Z, He Z, Zhu F,
Tian L, Tu M, Xie J, Liu M, et al: Inhibiting MT2-TFE3-dependent
autophagy enhances melatonin-induced apoptosis in tongue squamous
cell carcinoma. J Pineal Res. 64:642018. View Article : Google Scholar
|
|
33
|
Ciolofan S, Ioniţă E, Mogoantă CA, Popescu
FC, Anghelina F, Chiuţu L and Stanciu G: Malignant melanoma of
nasal cavity. Rom J Morphol Embryol. 52:679–684. 2011.PubMed/NCBI
|
|
34
|
Rasheed AB, Daoud MS and Gorial FI:
Diagnostic utility of serum melatonin levels in systemic lupus
erythematosus: A case-control study. Reumatismo. 69:170–174. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Nicolae AC, Dragoi CM, Ceausu I,
Poalelungi C, Iliescu D and Arsene AL: Clinical implications of the
indolergic system and oxidative stress in physiological gestational
homeostasis. Farmacia. 63:46–51. 2015.
|
|
36
|
Tong J, Sheng S, Sun Y, Li H, Li WP, Zhang
C and Chen ZJ: Melatonin levels in follicular fluid as markers for
IVF outcomes and predicting ovarian reserve. Reproduction.
153:443–451. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Hobson SR, Gurusinghe S, Lim R, Alers NO,
Miller SL, Kingdom JC and Wallace EM: Melatonin improves
endothelial function in vitro and prolongs pregnancy in women with
early-onset preeclampsia. J Pineal Res. 65:e125082018. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Stefanescu H, Muntean D, Pilut C, Diaconu
M, Popescu R, Hutanu D, Moise M, Diana L, Nitu R, Cherecheanu AP,
et al: Using blood and plasma MicroRNAs as a non-invasive biomarker
in patients with colorectal cancer. Clin Lab. 64:257–262. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Thériault S, Giguère Y, Massé J, Girouard
J and Forest JC: Early prediction of gestational diabetes: A
practical model combining clinical and biochemical markers. Clin
Chem Lab Med. 54:509–518. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Dragoi CM, Morosan E, Dumitrescu IB,
Nicolae AC, Arsene AL, Draganescu D, Lupuliasa D, Ionita AC, Pantea
Stoian A, Nicolae C, et al: Insights into chrononutrition: The
innermost interplay amongst nutrition, metabolism and the circadian
clock, in the context of epigenetic reprogramming. Farmacia.
67:557–571. 2019. View Article : Google Scholar
|