Introduction
Malignant melanoma (MM) is a highly aggressive
cancer derived from neural crest melanocytes and occurs most
frequently in the skin, digestive tract, eyes, genitals and nasal
cavity (1–3) The prognosis of patients with MM is poor
and the 5-year survival is reported to be <20% (4). Each year, ~20,000 cases of cutaneous MM
are reported in China and the incidence is growing by 3–5% per year
(5). The incidence of MM is lower in
China compared with Western countries, but survival is shorter in
Chinese patients (6,7). In addition, differences in incidence,
etiology and clinical characteristics between different races are
still poorly understood.
The development of prognostic markers of MM, such as
serum lactic dehydrogenase (LDH) and the identification of new
treatment targets; for example, melanogenesis, have improved the
treatments available for patients and patient outcomes (8,9). Serum
LDH appears to be an independent marker of stage IV MM and studies
have suggested that serum LDH may be used to identify patients
requiring complete mastectomy (1,2).
However, to the best of our knowledge, it is unclear whether serum
LDH can be used to predict the metastatic possibility in the early
stages of MM.
In the present study, the prognostic value of
commonly tested hematological and biochemical parameters were
investigated, including serum albumin and prealbumin, LDH, total
leukocyte count and serum D-dimer levels, a degradation product of
fibrinolysis. In addition, the albumin/D-dimer ratio [serum
albumin/D-dimer prognosis score (ADPS)] and the serum
prealbumin/D-dimer ratio [serum prealbumin/D-dimer prognosis score
(PDPS)] were determined. Serum albumin (10) and prealbumin levels (11) reflect the nutritional and
inflammatory status of the patient. Malnourished patients with
cancer often have poor immune function, drug tolerance and poor
response to treatments (12).
D-dimer has been found to be associated with malignancy and D-dimer
levels are associated with tumor stage, tumor prognosis, lymph node
involvement and survival of patients with several types of cancer,
including esophageal squamous cell carcinoma (13), gastric cancer (14), breast cancer (15), colorectal cancer (16), lung cancer (17) and ovarian cancer (18). Moreover, cancer-associated
inflammation is an important contributor to disease progression and
survival, and systemic inflammation is associated with alterations
in peripheral blood leukocytes (19). Therefore, in the present study, it
was hypothesized that a combination of D-dimer levels, leukocyte
count and albumin or prealbumin levels may be useful for predicting
prognosis of patients with MM.
The aim of the present study was: i) To explore the
characteristics of MM and the factors affecting prognosis in
Chinese patients with MM; ii) analyze the similarities and
differences in characteristics with patients with MM from other
regions of the world; and iii) to determine the value of commonly
tested hematological and biochemical parameters for predicting
metastasis in patients with MM.
Patients and methods
Patients
The present study was approved by The Ethics
Committee of the First Affiliated Hospital of Zhengzhou University
(Zhengzhou, China; trial registration no. 2018-LW-037). Written
informed consent was obtained from all participants included in the
study. A total of 176 patients at the First Affiliated Hospital of
Zhengzhou University were collected. Patients with a history of
other malignancies, autoimmune disease, chronic renal or hepatic
disease, diabetes, thyroid disorders and taking anti-inflammatory
drugs were excluded. A total of 167 patients were included in this
study, including 74 men (44.3%) and 93 women (55.7%). All patients
were diagnosed with cutaneous or mucosal MM according to the
criteria of the American Joint Committee on Cancer, 8th edition
(1) between April 2003 and April
2018. The age range of all patients was 22–92 years and the median
age was 56.81 years. The demographic and clinical data of these
patients was obtained from medical records for analysis; including
personal data (age at diagnosis, sex, living habits, family
history); blood test results (serum albumin and prealbumin, serum
LDH, total leukocyte count, serum D-dimer); tumor-related data
[tumor location and stage, presence of metastasis, Breslow level
(20), Clark level (3), presence of ulceration]; treatment
received (adjuvant therapy and type of surgery) and follow-up data
(current status, survival). Table I
summarizes the collected data.
 | Table I.Clinicopathological characteristics
of patients with MM from the experimental cohort. |
Table I.
Clinicopathological characteristics
of patients with MM from the experimental cohort.
| Variable | n | Mean ± standard
deviation/proportion, % |
|---|
| OS, months | 167 | 35.9±31.6 |
| DFS, months | 167 | 26.9±28.8 |
| Age, years | 167 | 56.8±15.0 |
|
≤40 | 23 | 13.8% |
|
40–50 | 39 | 22.7% |
|
50–60 | 33 | 20.4% |
|
60–70 | 44 | 26.3% |
|
70–80 | 20 | 12.0% |
|
>80 | 8 | 4.8% |
| Sex | 167 |
|
|
Male | 74 | 44.3% |
|
Female | 93 | 55.7% |
| Overall survival
status | 167 |
|
|
Alive | 85 | 50.9% |
|
Deceased | 82 | 49.1% |
| Family history of
tumor | 167 |
|
|
Yes | 24 | 14.4% |
| No | 97 | 58.1% |
|
Unknown | 46 | 27.5% |
| T stage | 167 |
|
|
pT0 | 13 | 7.9% |
|
pT1 | 42 | 25.1% |
|
pT2 | 57 | 34.1% |
|
pT3 | 36 | 21.5% |
|
pT4 | 19 | 11.4% |
| TNM stage | 167 |
|
| I or
II | 64 | 38.3% |
|
III | 38 | 22.8% |
| IV | 65 | 38.9% |
| Breslow, mm | 137 |
|
|
≤1.00 | 42 | 30.7% |
|
1.01–2.00 | 48 | 35.0% |
|
2.01–4.00 | 27 | 19.7% |
|
>4.00 | 20 | 14.6% |
| Clark | 138 |
|
| 1 | 30 | 21.7% |
| 2 | 34 | 24.6% |
| 3 | 41 | 29.7% |
| 4 | 16 | 11.6% |
| 5 | 17 | 12.3% |
| Histological
type | 167 |
|
|
ALM | 52 | 13.8% |
| NM | 24 | 22.7% |
|
SSM | 33 | 20.4% |
|
LMM | 22 | 26.3% |
|
MCM | 24 | 12.0% |
|
Unclassifiable | 12 | 4.8% |
| Growth phase | 130 |
|
|
Radial | 61 | 46.9% |
|
Vertical | 69 | 53.0% |
| Anatomic
region | 167 |
|
|
Trunk | 21 | 12.6% |
|
Head/neck | 14 | 8.4% |
|
Extremities | 97 | 58.1% |
|
Mucosal | 24 | 14.4% |
|
Unknown | 11 | 6.6% |
| Ulceration | 147 |
|
|
With | 88 | 52.7% |
|
Without | 59 | 35.3% |
|
Unknown | 20 | 13.0% |
| Metastasis |
|
|
|
With | 104 | 62.3% |
|
Without | 63 | 37.7% |
| Therapy | 167 |
|
|
Surgery | 59 | 35.3% |
|
Adjuvant therapy without
surgery | 14 | 8.4% |
|
Adjuvant therapy with
surgery | 88 | 52.7% |
| Without
therapy | 6 | 3.6% |
| Albumin, g/l | 109 | 42.83±3.32 |
| Prealbumin,
mg/l | 100 | 244.60±54.26 |
| D-dimer, ug/l | 105 | 0.208±0.209 |
| Leukocyte
109/l | 113 | 6.56±2.17 |
| LDH, U/l | 96 | 183.78±55.54 |
cBioPortal
The characteristics of the patients of the present
study were compared with patients around the world registered in
the cBioPortal for Cancer Genomics (cbioportal.org). cBioPortal combines a number of
large-scale cancer genomics projects, including The Cancer Genome
Atlas (https://www.cancer.gov/tcga) and The
International Cancer Genome Consortium (https://icgc.org/), and catalogues data on genetic,
epigenetic, gene expression and proteomic events. The portal also
provides graphical summaries of gene-level data from multiple
platforms, network visualization and analyses, survival analysis
(21) patient-centric queries and
software programmatic access (2).
cBioPortal contained 12 studies with a total of 1,566 patients,
focusing on melanoma of eye and skin (Table II). Following elimination of
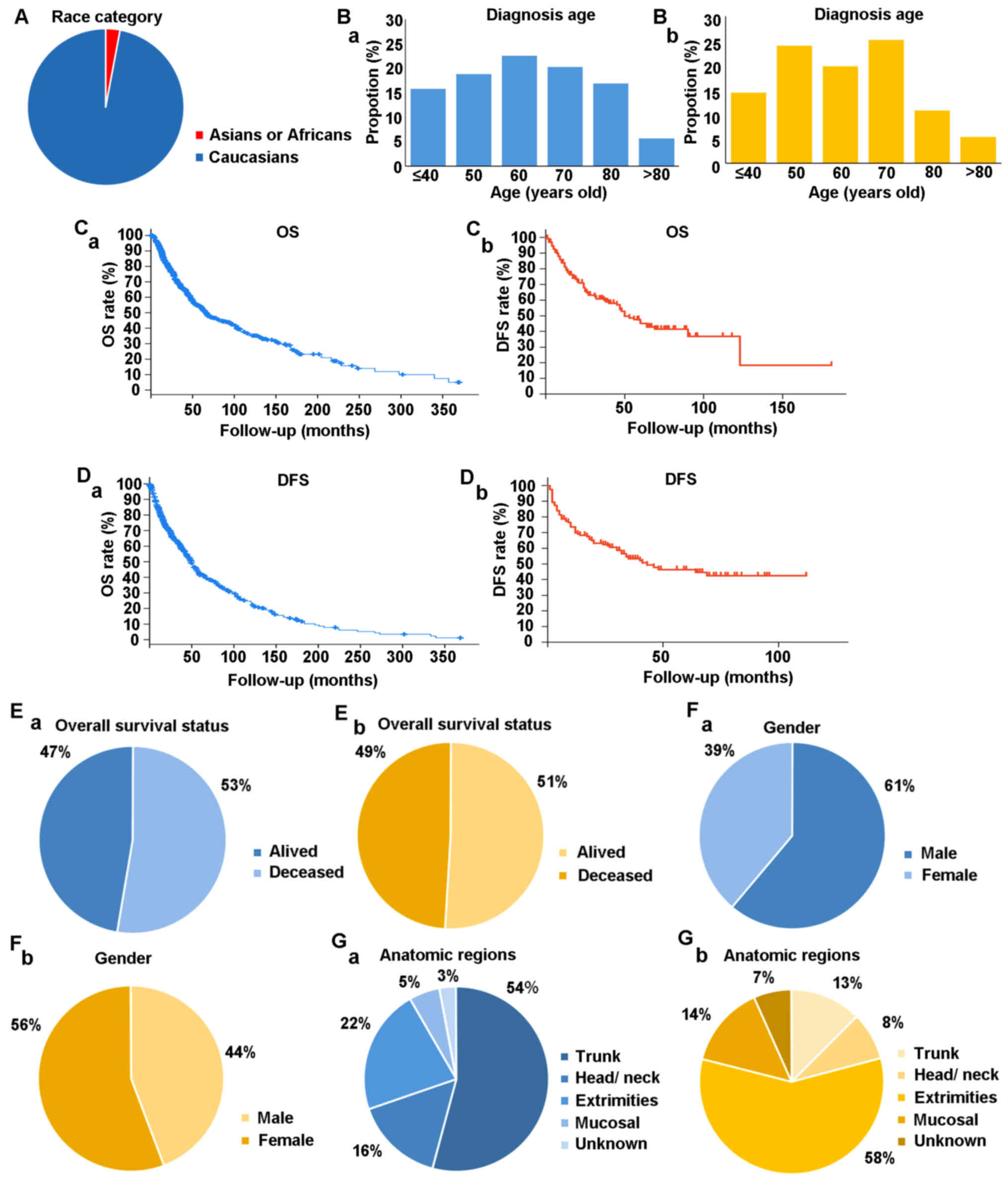
duplicate data, a total of 1,518 patients remained, including 97%
of Caucasian patients from America and Europe and 3% of Asian or
African patients (Fig. 1A).
| Table II.Results of tumor type and number of
cases from cBioPortal. |
Table II.
Results of tumor type and number of
cases from cBioPortal.
| Author, year | Source | Cancer type | No. of cases | (Refs.) |
|---|
| Taylor et
al, 2018; Sanchez-Vega et al, 2018; Liu et al,
2018; Hoadley et al, 2018; Gao et al, 2018; Ellrott
et al, 2018 | TCGA, PanCancer
Atlas | Uveal melanoma | 80 | (42–47) |
| 2018 | TCGA,
provisionala | Uveal melanoma | 80 |
|
| Liang et al,
2017 | TGEN, genome
research, 2017 | Paired-exome
sequencing of acral melanoma | 38 | (48) |
| Berger et
al, 2012 | Broad/Dana Farber,
nature 2012 | Cutaneous
melanoma | 26 | (49) |
| 2017 | MSKCC, JCO
precision oncology, 2017b | Next generation
sequencing (NGS) of pre-treatment metastatic melanoma samples | 66 |
|
| Hodis et al,
2012 | Broad, cell,
2012 | Skin cutaneous
melanoma | 121 | (50) |
| Taylor et
al, 2018; Sanchez-Vega et al, 2018; Liu et al,
2018; Hoadley et al, 2018; Gao et al, 2018; Ellrott
et al, 2018 | TCGA, PanCancer
Alas | Skin cutaneous
melanoma | 448 | (42–47) |
| 2018 | TCGA,
provisional | Skin cutaneous
melanomaa | 479 |
|
| Krauthammer et
al, 2012 | Yale, nat genet
2012 | Skin cutaneous
melanoma | 91 | (51) |
| Van Allen et
al, 2014 | Broad, cancer
discov 2014 | Skin cutaneous
melanoma | 78 | (52) |
| Hugo et al,
2016 | UCLA, cell
2016 | Whole-exome
sequences of pretreatment melanoma tumors | 39 | (53) |
| Shain et al,
2015 | Broad institute,
nat genet 2015 | Desmoplastic
melanoma | 20 | (54) |
Statistical analysis
Data were analyzed using Microsoft Excel 2007
(Microsoft Corporation), SPSS version 20.0 (IBM Corp.) and GraphPad
Prism version 5 (GraphPad Software Inc.). Quantitative variables
were presented as either mean ± standard deviation or median and
interquartile range, depending on the normality of the
distribution. Normally distributed quantitative variables were
analyzed using a Student's t test, data with unequal variance were
analyzed using a Welch's t-test. Non-normally distributed
continuous data were compared using a Mann-Whitney U test.
Qualitative variables were reported as frequencies and percentages
and compared using a χ2 test or the Fisher's exact test.
Receiver operating characteristic (ROC) analysis was used to
identify the ideal cutoff value of ADPS for distinguishing between
patients with and without metastasis. The Youden index
[(specificity + sensitivity)-1] was calculated as a measure of
overall efficacy. The area under curve (AUC) was used to assess the
predictive value of ADPS, serum prealbumin/D-dimer prognosis score
(PDPS) and D-dimer. Regression tree analysis was used to measure
the sensitivity, specificity and accuracy of the indicator for
predicting metastasis in patients with MM. Variables that were
significantly associated with tumor metastasis were analyzed using
multivariate Cox regression analysis to identify independent
predictors of metastasis. Kaplan-Meier curves were constructed for
survival analysis and a log-rank test was used to determine the
differences in survival rate. In Kaplan-Meier survival analysis of
prognostic factors for OS, the prognostic factors with multigroups
in T stage, TNM stage, Breslow thickness, Clark level, histological
type and anatomic region were analyzed by pooled over strata in
log-rank test. P<0.05 was considered to indicate a statistically
significant difference. In the comparison of MM patients with and
without metastasis, each numerical data was limited by the mean
difference and divided into higher group and lower group. Regarding
other statistic analyses, MM patients were divided into low or high
group according to the ADPS value (341.01), the ideal cutoff value
by ROC analysis, whereas other quantitative data were grouped by
mean value.
Results
Clinical characteristics of patients
with MM
A total of 85 patients (50.9%) were still alive at
the end of the study whereas 82 patients (49.1%) had died. Median
overall survival (OS) was 50 months (range, 0–181 months; Fig. 1C) and median disease-free survival
(DFS) was 35 months (range, 0–124 months; Fig. 1D). The proportion of patients with
tumor node metastasis (TNM) stage I/II, III or IV were 64/167
(38.3%), 38/167 (22.8%) and 65/167 (38.9%), respectively. Data on
Breslow thickness were available for 137 patients; the Breslow
thickness was <1 mm in 42/137 patients (30.7%), 1.01–2.00 mm in
48/137 patients (35.0%), 2.01–4.00 mm in 27/137 patients (19.7%)
and >4.00 mm in 20/137 patients (14.6%). Data on the Clark level
were available for 138 patients; 30/138 patients (21.7) were
classed as level 1, 34/138 patients (21.7%) were classed as level
2, 41/138 patients (29.7%) were classed as level 3, 16/138 patients
(11.6%) were classed as level 4 and 17/138 patients (12.3%) were
classed as level 5. The primary lesion was on the trunk in 21/167
patients (12.6%), in the head/neck region in 14/167 patients
(8.4%), in the extremities in 97/167 patients (58.1%), in the
mucosa in 24/167 patients (37.8%) and at unknown locations in
11/167 patients (6.6%). Ulcerative melanoma was observed in 88 out
of 167 patients (52.7%) and nonulcerative melanoma was observed in
59 out of 167 patients (35.3%). The mean total serum Albumin,
D-dimer and LDH were 42.83±3.32 g/l, 0.208±0.209 ug/l and
183.78±55.54 U/l, respectively. The clinicopathological
characteristics of patients and results of blood tests are
described in Table I.
Comparison of characteristics of
Chinese patients with MM with the cBioPortal data
The proportion of male patients was higher in the
cBioPortal cohort than in the experimental cohort (61% vs. 44%;
Fig. 1Fa and Fb). Age at diagnosis
of patients with MM ranged from 40–70 years in both the cBioPortal
cohort and in experimental cohort (Fig.
1Ba and Bb). MM was most commonly diagnosed in patients aged
50–60 years in the cBioPortal cohort (Fig. 1Ba); whereas, in the experimental
cohort MM was most commonly diagnosed in patients aged 60–70 years
(Fig. 1Bb). Median OS was 66.43
months (range, 0.36–369.65 months) in the cBioPortal cohort vs. 50
months (range, 0–181 months) in the experimental cohort. Median DFS
was 49.21 months (range, 0.46–386.50 months) in the cBioPortal
cohort vs. 35 months (range, 0–112 months) in experimental cohort.
The 3-, 5- and 10-year survival rates were 59.1, 47.7 and 31.6%,
respectively, in the cBioPortal cohort vs. 59.0, 43.0 and 13.5% in
the experimental cohort (Fig. 1C and
D). OS was 47% in the cBioPortal cohort vs. 49% in experimental
cohort (Fig. 1E). In the cBioPortal
cohort, the most common locations of melanoma were the trunk (54%),
followed by the extremities (22%), head and neck (16%) and mucosa
(5%) (Fig. 1Ga), whereas in the
experimental cohort the most common locations of melanoma were the
extremities (58.1%), followed by the mucosa (14%) and the trunk
(13%) (Fig. 1Gb). The reasons for
these differences remain unclear; however, a possible explanation
may be due to differences in lifestyle factors.
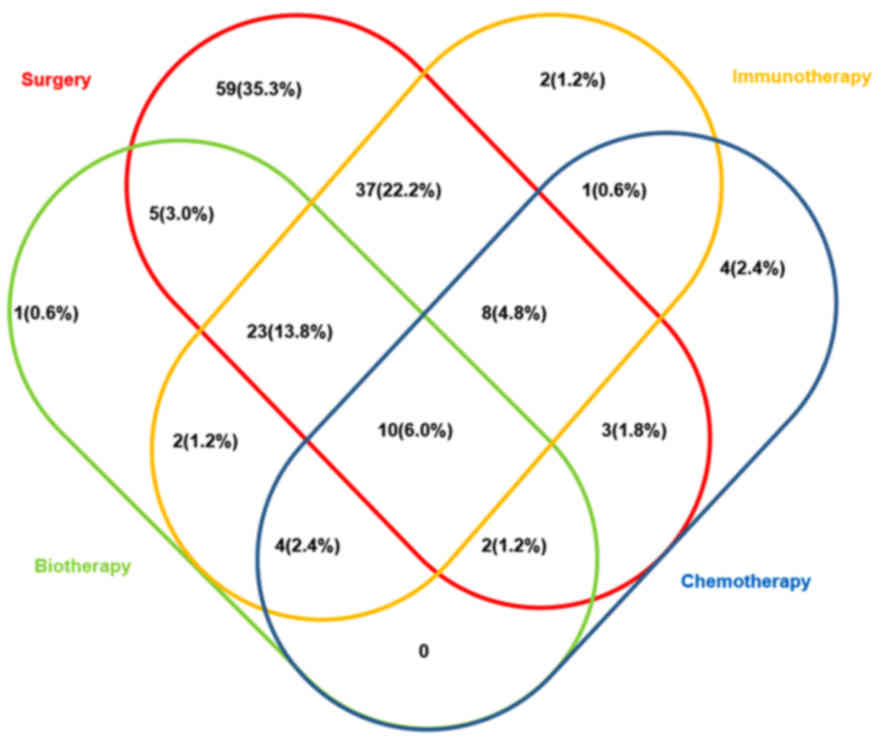
Melanoma treatment
Patients in the experimental cohort received a
variety of treatments, including combinations of surgery,
chemotherapy, immunotherapy and biotherapy. A total of 88/167
patients (52.7%) received surgery and adjuvant therapy, whereas
59/167 patients (35.3%) received only surgery and 14/167 patients
(8.4%) received only adjuvant therapy (Fig. 2); treatment details were not
available for 6/167 (3.6%) patients (Table I). Treatment selection for the
patients in the experimental cohort was in accordance with the 1st
edition of Consensus on the Diagnosis and Treatment of Melanoma in
China (August, 2008) (1).
Chemotherapeutic agents used included Taxol, Dacarbazine and
platinum-type drugs. Immunotherapeutic agents used included
thymopentin, and recombinant human interferon g and/or
interleukin-2. There were a total of 15 different combinations of
treatments; the most common treatment was surgery alone, followed
by surgery plus immunotherapy and then surgery plus
bioimmunotherapy (Fig. 2).
Comparison of patients with and
without metastasis
The experimental patients were separated into two
groups: Patients with metastasis (n=104) and those without
metastasis (n=63). Mean serum albumin (P=0.145), prealbumin
(P=0.752), LDH (P=0.150) and leukocyte count (P=0.224) did not
significantly differ between the two groups. However, patients with
metastasis had significantly higher D-dimer levels (0.237±0.217
µg/l vs. 0.151±0.134 µg/l; P<0.001), and a significantly lower
ADPS (328.61±235.72 vs. 452.46±302.07; P<0.001) and PDPS
(1,913.53±1,464.42 vs. 2,657.75±1,983.42; P<0.05) (Table III).
| Table III.Comparison between experimental
cohort patients with and without metastatic MM. |
Table III.
Comparison between experimental
cohort patients with and without metastatic MM.
| Variable | Metastatic, mean ±
SD |
Non-metastatich, mean ± SD or mean (n=%) | P-value |
|---|
| Albumin,
g/ld | 42.12±4.35 | 42.99±2.90 | 0.145 |
| Prealbumin,
mg/le | 246.90±57.58 | 243.70±50.70 | 0.752 |
| LDH,
U/lf | 191.43±59.86 | 176.56±37.22 | 0.150 |
| D-dimer,
ug/lf | 0.43±0.85 | 0.16±0.13 | <0.001 |
| Leukocyte,
109/lf | 6.77±4.58 | 5.93±1.97 | 0.224 |
| ADPSf | 290.46±241.84 | 434.35±276.99 | <0.001 |
| PDPSe |
1,789.50±1,449.42 |
2,521.04±1,809.78 | 0.018a |
| Sex |
|
|
<0.001c |
|
Male | 57 (54.8%) | 17 (25.8%) |
|
|
Female | 47 (45.2%) | 49 (74.2%) |
|
|
Breslowg |
|
|
<0.001c |
|
≤1.00 | 12 (16.0%) | 29 (50.0%) |
|
|
1.01–2.00 | 28 (37.3%) | 19 (32.8%) |
|
|
2.01–4.00 | 18 (24.0%) | 8 (13.8%) |
|
|
>4.00 | 17 (22.7%) | 2 (3.4%) |
|
| Clark
levelg |
|
|
<0.010a |
| 1 | 12 (16.0%) | 17 (29.8%) |
|
| 2 | 14 (18.7%) | 19 (33.3%) |
|
| 3 | 25 (33.3%) | 15 (26.3%) |
|
| 4 | 11 (14.7%) | 4 (7.0%) |
|
| 5 | 13 (17.3%) | 2 (3.5%) |
|
| Anatomic
regiong |
|
| 0.078 |
|
Truck | 16 (17.0%) | 5 (7.9%) |
|
|
Head/neck | 10 (10.6%) | 4 (6.3%) |
|
|
Extremities | 51 (54.3%) | 47 (74.6%) |
|
|
Mucosal | 7 (18.1%) | 7 (11.1%) |
|
|
Ulcerationg |
|
|
<0.001c |
|
With | 69 (80.2%) | 19 (31.1%) |
|
|
Without | 17 (19.8%) | 42 (68.9%) |
|
| T
stageg |
|
| 0.003b |
|
pT0 | 13 (7.8%) | 0 (0) |
|
|
pT1 | 11 (6.6%) | 31 (18.6%) |
|
|
pT2 | 38 (22.8%) | 19 (11.4%) |
|
|
pT3 | 25 (15.0%) | 11 (6.6%) |
|
|
pT4 | 17 (10.2%) | 2 (1.2%) |
|
| Histological
typeg |
|
|
<0.001c |
|
ALM | 21 (13.5%) | 31 (20.0%) |
|
| NM | 23 (14.8%) | 1 (0.6%) |
|
|
SSM | 17 (11.0%) | 16 (10.3%) |
|
|
LMM | 14 (9.0%) | 8 (5.1%) |
|
|
MCM | 17 (11.0%) | 7 (4.5%) |
|
| Growth
phaseg |
|
|
<0.001c |
|
Radial | 15 (20.3%) | 46 (82.1%) |
|
|
Vertical | 59 (79.7%) | 10 (17.9%) |
|
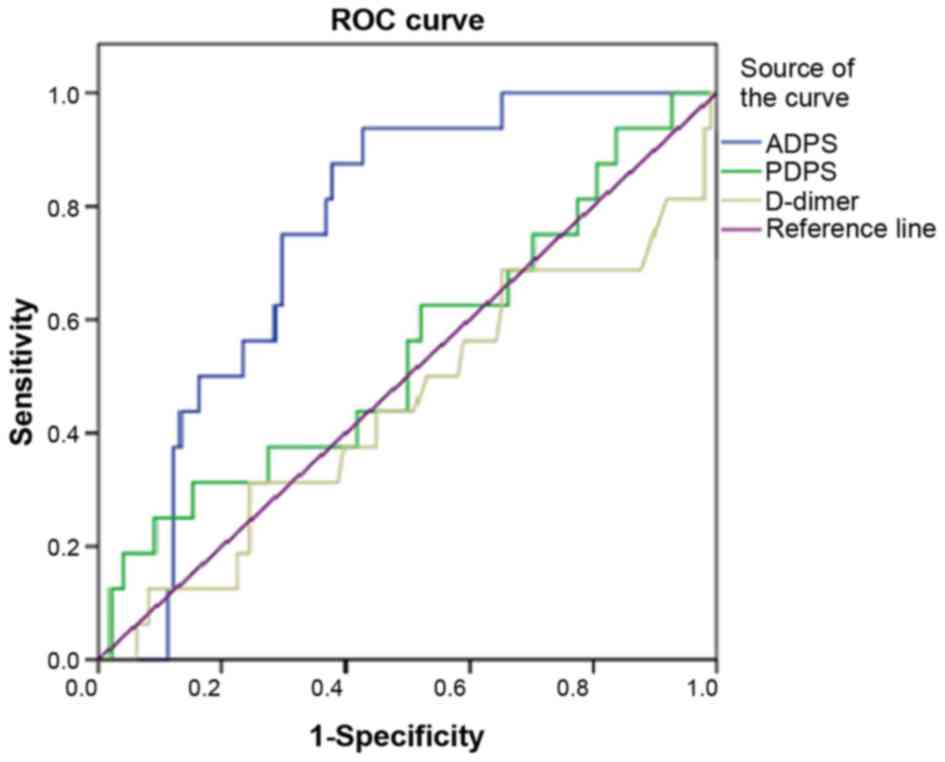
ROC analysis
ROC analysis showed an ADPS of 341.01 to be the
ideal cutoff value for differentiating between patients with and
without metastasis and the AUC for ADPS was 0.773 (Fig. 3). For prediction of metastasis, ADPS
had 93.8% sensitivity, 59.6% specificity, 54.6% accuracy and a
Youden index of 53.40%. The AUC for PDPS was 0.547. For prediction
of metastasis, PDPS had 31.3% sensitivity, 84.7% specificity, 9.4%
accuracy and a Youden index of 16.0%. The AUC for D-dimer was
0.447. For prediction of metastasis, D-dimer had 31.35%
sensitivity, 75.5% specificity, 10.6% accuracy and a Youden index
of 6.9% (Table IV).
| Table IV.ROC analysis of metastasis in
patients with MM. |
Table IV.
ROC analysis of metastasis in
patients with MM.
|
| AUC | SEa | Cut off value | Acurrency ratio,
% | Sensitivity, % | Specificity, % | LB | UB | Youden index
(%) |
|---|
| ADPS | 0.773 | 0.045 | 457.38 | 54.60 | 93.8 | 59.6 | 0.686 | 0.861 | 53.40 |
| PDPS | 0.547 | 0.082 | 3,456.61 | 9.40 | 31.30 | 84.70 | 0.386 | 0.707 | 16.00 |
| D-dimer | 0.447 | 0.084 | 0.238 | 10.60 | 31.35 | 75.50 | 0.282 | 0.611 |
6.85 |
Univariate and multivariable Cox
regression analyses for metastasis of patients with MM
Univariate Cox regression analyses were performed to
screen the potential predictors of metastasis for patients with MM.
A total of 9 clinicopathological predictors for overall survival
were ascertained through multivariate Cox regression analysis and 3
variables were shown to be independently associated with
metastasis; including ADPS Group [hazard ratio (HR)=8.534; 95%
confidence interval (CI)= 3.109–23.425], ulceration (HR=4.287; 95%
CI=2.204–8.953) and vertical growth phase (HR=2.324; 95%
CI=1.067–5.063). In contrast, sex, Breslow thickness, Clark level,
histological type, anatomic location and T stage were not shown to
be independent predictors of metastasis (Tables V and VI).
| Table V.Univariate Cox regression analyses of
metastasis in patients with MM. |
Table V.
Univariate Cox regression analyses of
metastasis in patients with MM.
|
| Univariate
analysis |
|---|
|
|
|
|---|
| Variables | HR | 95% CI | P-value |
|---|
| ADPS group | 13.611 | 6.707–27.622 | 0.000 |
| Ulceration | 5.257 | 3.036–9.102 | 0.000 |
| Growth phase | 5.475 | 3.074–9.752 | 0.000 |
| Sex | −0.580 | 0.339–0.737 | 0.000 |
| Breslow | 1.749 | 1.415–2.162 | 0.000 |
| Clark level | 1.507 | 1.261–1.801 | 0.000 |
| T stage | 1.423 | 1.272–1.592 | 0.000 |
| Histological
type |
|
|
|
|
ALM | −0.114 | 0.054–0.242 | 0.000 |
| NM | −0.556 | 0.273–1.131 | 0.105 |
|
SSM | −0.167 | 0.077–0.361 | 0.000 |
|
LMM | −0.207 | 0.093–0.462 | 0.000 |
|
MCM | −0.226 | 0.104–0.492 | 0.000 |
| Anatomic
region |
|
|
|
|
Trunk | −0.311 | 0.142–0.682 | 0.004 |
|
Head/neck | −0.303 | 0.126–0.729 | 0.008 |
|
Extremities | −0.189 | 0.096–0.375 | 0.000 |
|
Mucosal | −0.259 | 0.118–0.568 | 0.001 |
| Table VI.Multivariate Cox regression analyses
of metastasis in patients with MM. |
Table VI.
Multivariate Cox regression analyses
of metastasis in patients with MM.
|
| Multivariate
analysis |
|---|
|
|
|
|---|
| Variables | Coefficient | HR | 95% CI | P-value |
|---|
| ADPS group | 2.144 | 8.534 | 3.109–23.425 | 0.000 |
| Ulceration | 1.567 | 4.792 | 2.204–8.953 | 0.000 |
| Growth phase | 0.843 | 2.324 | 1.067–5.063 | 0.034 |
| Sex | −0.535 | 0.586 | 0.314–1.092 | 0.092 |
| Breslow | 0.339 | 1.404 | 0.739–2.666 | 0.300 |
| Clark level | 0.047 | 1.048 | 0.820–1.339 | 0.708 |
| T stage | 0.498 | 1.645 | 0.857–3.158 | 0.134 |
| Histological
type | −0.109 | 0.896 | 0.653–1.230 | 0.498 |
| Anatomic
region | 0.035 | 1.035 | 0.718–1.493 | 0.853 |
Kaplan-Meier survival analysis of
prognostic factors for OS
A 10-year Kaplan-Meier survival analysis was
performed and a Log-rank test was used to compare the survival
curves of two or more groups. Survival of patients with high ADPS
was significantly longer compared with patients with low ADPS. The
OS was significantly worse for MM patients with ulcerated melanoma
(compared with patients without ulceration; P<0.001; Fig. 4I), MM patients with metastasis
(compared with patients without metastasis; P<0.001; Fig. 4J), female patients (compared with
male patients; P=0.0062; Fig. 4A),
Clark level >3 (compared with Clark level 3 and 4; P<0.001;
Fig. 4E) and patients with vertical
growth phase (compared with radial; P<0.001; Fig. 4G). The Kaplan-Meier survival curves
also demonstrated significant difference in distinct TNM stage
(multiple comparison; P<0.001; Fig.
4C) and Breslow thickness (multiple comparison; P<0.001;
Fig. 4D). The median OS by stage was
as follows: T0 stage, 8 months; T1 stage, 108 months; T2 stage, 60
months; T3 stage, 27 months; and T4 stage, 19 months (multiple
comparison; P<0.001; Fig. 4B).
Median overall survival by histological type was as follows: Acral
lentiginous melanoma, 82 months; nodular melanoma, 21 months;
superficial spreading melanoma, 74 months; Lentigo malignant
melanoma, 50 months; Mucosal melanoma, 47 months; and indeterminate
types, 6 months (multiple comparison; P<0.001; Fig. 4H). Anatomic region of the MM was not
associated with OS (multiple comparison; P=0.171; Fig. 4F; Table
VII).
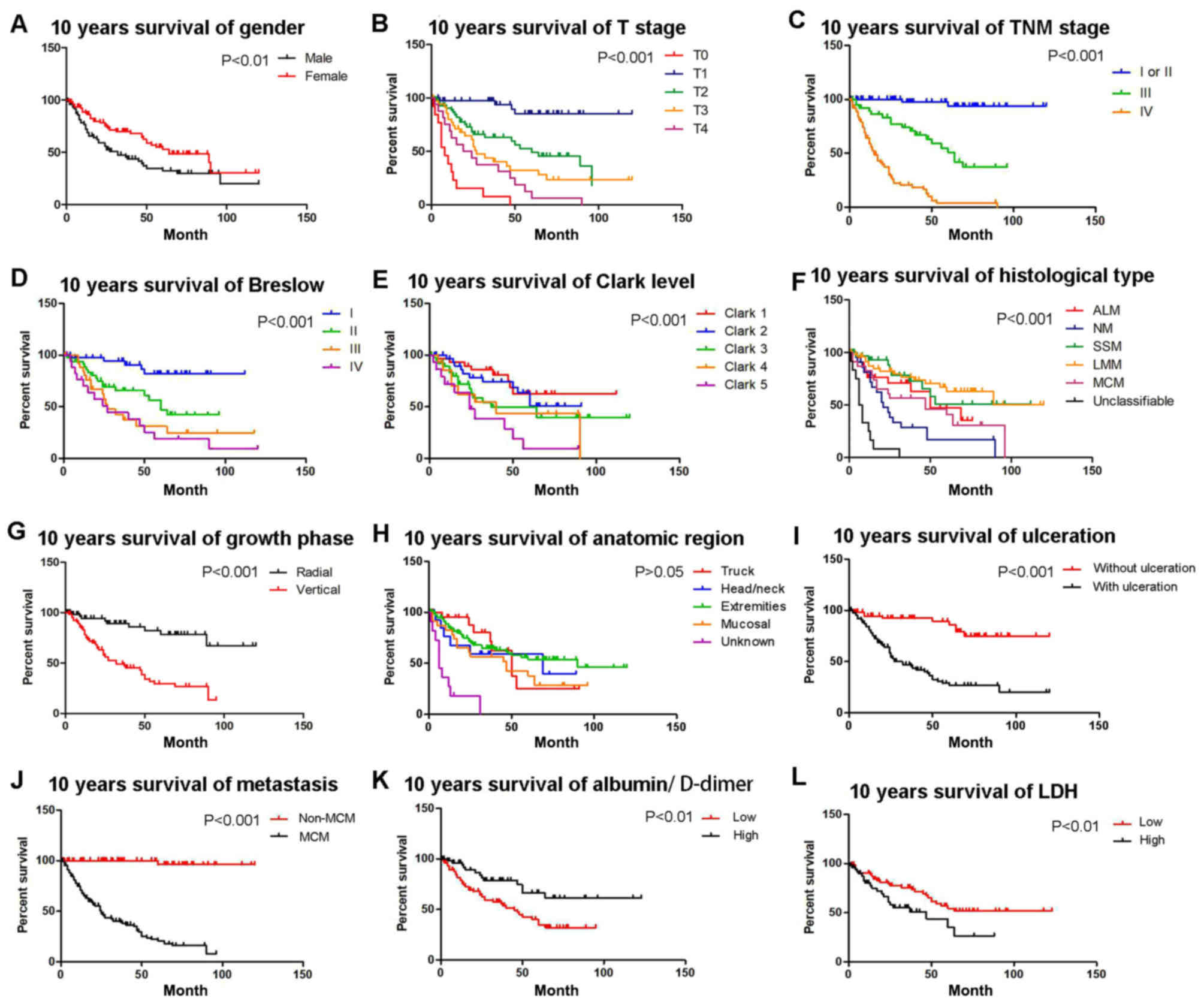 | Figure 4.Kaplan-Meier analyses of 10-year OS
for the entire cohort of patients according to different stratums
by prognostic factors. OS of patients based on (A) sex (P<0.01),
(B) T stage (compared with T0, T1, T2, T3 and T4; P<0.001), (C)
TNM stage (compared with TNM stage I/II, III and IV; P<0.001),
(D) Breslow thickness (compared with Breslow I, II, III and IV;
P<0.001), (E) Clark level (compared with Clark level 1, 2, 3, 4
and 5; P<0.001), (F) histological type (compared with ALM, NM,
SSM, LMM, MCM and unclassifiable; P<0.001), (G) growth phase
(P<0.001), (H) anatomic region (compared with trunk, head/neck,
extremities, mucosal and unknown; P>0.05), (I) ulceration
(P<0.001), (J) metastasis (P<0.001), (K) albumin/D-dimer
(P<0.01), (L) LDH levels (P<0.01). OS, overall survival; T,
Tumor; TNM, tumor node metastasis; LDH, lactate dehydrogenase; ALM,
acral lentiginous melanoma; NM, nodular melanoma; SSM, superficial
spreading melanoma; MCM, mucosal melanoma. |
| Table VII.Kaplan-Meier survival analysis of
prognostic factors for OS. |
Table VII.
Kaplan-Meier survival analysis of
prognostic factors for OS.
| Variables | Median OS,
months | df | Log-rank analysis,
P value |
|---|
| Sex |
| 1 | 0.0062b |
|
Male | 32 |
|
|
|
Female | 64 |
|
|
| T stage |
| 4 |
<0.001c |
|
pT0 | 8 |
|
|
|
pT1 | 108 |
|
|
|
pT2 | 60 |
|
|
|
pT3 | 27 |
|
|
|
pT4 | 19 |
|
|
| TNM stage |
| 2 |
<0.001c |
| I or
II | 120 |
|
|
|
III | 60 |
|
|
| IV | 14 |
|
|
| Breslow, mm,
n=137 |
| 3 |
<0.001c |
|
≤1.00 | 98 |
|
|
|
1.01–2.00 | 60 |
|
|
|
2.01–4.00 | 27 |
|
|
|
>4.00 | 24 |
|
|
| Clack level,
n=138 |
| 4 |
<0.001c |
| 1 | 83 |
|
|
| 2 | 60 |
|
|
| 3 | 37 |
|
|
| 4 | 40 |
|
|
| 5 | 24 |
|
|
| Histological
type |
| 5 |
<0.001c |
|
ALM | 82 |
|
|
| NM | 21 |
|
|
|
SSM | 74 |
|
|
|
LMM | 50 |
|
|
|
MCM | 47 |
|
|
|
Unclassifiable | 6 |
|
|
| Growth phase |
| 1 |
<0.001c |
|
Radial | 98 |
|
|
|
Vertical | 32 |
|
|
| Anatomic
region |
| 3 | 0.171 |
|
Trunk | 48 |
|
|
|
Head/neck | 69 |
|
|
|
Extremities | 89 |
|
|
|
Mucosal | 45 |
|
|
| Ulceration,
n=147 |
| 1 |
<0.001c |
|
With | 79 |
|
|
|
Without | 27 |
|
|
| Metastasis |
| 1 |
<0.001c |
|
With | 24 |
|
|
|
Without | 113 |
|
|
| ADPS group |
|
| 0.0035b |
|
Low | 24 | 1 |
|
|
High | 99 |
|
|
| LDH group |
| 1 | 0.010a |
|
Low | 89 |
|
|
|
High | 37 |
|
|
Comparison between patients with low
and high ADPS
ADPS was calculated for 124 patients. There were 24
patients with low ADPS (<341.01) and 99 patients with high ADPS
(≥341.01). Patients with high ADPS level were more likely to have a
longer OS (P=0.016), DFS (P=0.001) and earlier TNM stage (TNM
stages I and II) of MM (24.2% vs. 17.4%; P=0.008), whereas these
patients were less likely to have an ulcerated melanoma (19.9% vs.
20.6%; P<0.001) or a metastatic melanoma (17.4% vs. 24.2%;
P=0.002; Table VIII).
| Table VIII.Comparison between patients with high
ADPS level and low ADPS. |
Table VIII.
Comparison between patients with high
ADPS level and low ADPS.
|
| Low ADPS level | High ADPS
level | P-value |
|---|
| OSc, mean ± SD | 26.96±23.67 | 41.34±30.65 | 0.139 |
| DFSc, mean ± SD | 15.46±17.13 | 34.88±26.03 | 0.733 |
| TNM
staged, n (%) |
|
| 1.000 |
| I or II | 25 (18.9%) | 32 (24.2%) |
|
| III | 20 (15.2%) | 12 (9.1%) |
|
| IV | 32 (24.2%) | 11 (8.3%) |
|
| Sexd, n (%) |
|
| 0.644 |
| Male | 30 (25.6%) | 21 (17.9%) |
|
| Female | 36 (56.4%) | 30 (25.6%) |
|
|
Breslowd |
|
| 0.335 |
| ≤1.00 | 20 (17.1%) | 17 (14.5%) |
|
| 1.01–2.00 | 19 (16.2%) | 21 (17.9%) |
|
| 2.01–4.00 | 16 (13.7%) | 8 (6.8%) |
|
| >4.00 | 11 (9.4%) | 5 (4.3%) |
|
| Clark
leveld |
|
| 0.713 |
| 1 | 18 (14.9%) | 9 (7.4%) |
|
| 2 | 15 (12.4%) | 15 (12.4%) |
|
| 3 | 17 (14.0%) | 16 (13.2%) |
|
| 4 | 7 (5.8%) | 6 (5.0%) |
|
| 5 | 9 (7.4%) | 9 (7.4%) |
|
| Anatomic
regiond |
|
| 0.132 |
| Truck | 16 (10.9%) | 5 (3.4%) |
|
| Head/neck | 10 (6.8%) | 4 (2.7%) |
|
| Extremities | 51 (34.7%) | 47 (32.0%) |
|
| Mucosal | 7 (4.8%) | 7 (4.8%) |
|
|
Ulcerationd |
|
| 0.001a |
| With | 68 (51.9%) | 26 (19.9%) |
|
| Without | 10 (7.6%) | 27 (20.6%) |
|
|
Metastasisd |
|
| 0.002b |
| With | 53 (40.2%) | 23 (17.4%) |
|
| Without | 24 (18.2%) | 24 (18.2%) |
|
| T
staged |
|
| 0.706 |
| pT0 | 4 (3.0%) | 0 |
|
| pT1 | 21 (15.9%) | 16 (12.1%) |
|
| pT2 | 22 (16.6%) | 23 (17.4%) |
|
| pT3 | 19 (14.4%) | 11 (8.3%) |
|
| pT4 | 11 (8.3%) | 5 (11.0%) |
|
| Histological
typed |
|
| 0.294 |
| ALM | 26 (22.2%) | 16 (13.7%) |
|
| NM | 1 (0.8%) | 6 (5.1%) |
|
| SSM | 15 (12.8%) | 14 (12.0%) |
|
| LMM | 6 (5.1%) | 13 (11.1%) |
|
| MCM | 11 (9.4%) | 6 (5.1%) |
|
| Unclassifiable | 3 (2.7%) | 0 |
|
| Growth
phased |
|
| 0.065 |
| Radial | 22 (19.8%) | 26 (23.4%) |
|
| Vertical | 40 (36.0%) | 23 (20.7%) |
|
Discussion
Due to the low incidence of MM in China there is
still no standard approach for diagnosis and treatment, and this is
partly due to a lack of reliable indicators of metastasis in the
early stages of disease. The aim of the present study was to
determine the prognostic value of specific hematological and
biochemical parameters routinely assessed at admission to hospital,
and their predictive value for prognosis of patients with MM.
Prognostic markers of MM, such as serum LDH, and the
identification of new treatment targets including melanogenesis,
serve important roles in the treatment and prognosis of MM
(9). Melanogenesis is a highly
regulated multistep biochemical process of melanin production by
melanocytes (22,23). Previous studies have indicated that
melanin pigment increases the resistance of melanoma cells to
different types of therapy including chemo- or radiotherapy
(22). Regarding the role of melanin
pigment in chemoresistance of melanoma cells, it was reported that
melanogenesis can generate cytotoxic, genotoxic or mutagenic
intermediates, which influence tumor microenvironment and tumor
immunity (24). Furthermore, studies
have shown that melanogenesis reduces OS and DFS in patients with
MM (23).
Serum albumin is synthesized in the liver and
participates in numerous biological functions in the body,
including maintenance of plasma osmotic pressure and regulation of
the dynamic balance between tissue fluid and blood vessels
(25,26). Serum albumin is also essential for
the transport of a number of substances, including hormones,
long-chain fatty acids to the liver, unconjugated bilirubin, metals
and ions (27,10). Decreases in plasma albumin levels can
result in decreased activity of enzymes essential for metabolism of
organisms (28). Serum albumin
levels can be used to assess nutritional and inflammatory status
(28). It has also been demonstrated
that malnourished cancer patients often have reduced immune
function, poor drug tolerance and poor response to treatments
(12,29).
D-dimer is a by-product of fibrinolysis and
increases in the levels of D-dimers suggest the presence of
coagulation and fibrinolysis (30).
Plasma D-dimer levels are useful for monitoring the state of
thrombotic diseases and disseminated intravascular coagulation
(13). Several studies have shown
that the levels of D-dimer are associated with tumor stage, tumor
prognosis, lymph node involvement and survival of patients with
ovarian cancer (18). In addition,
increased D-dimer levels are associated with the degree of
malignancy of tumors. Tumor cells or necrotic tissues stimulate the
generation and release of coagulation-promoting substances, which
activate exogenous coagulation factors resulting in abnormal
coagulation and thus activation of the plasminogen activator
(30,31). Locally synthesized fibrinolytic
enzymes degrade the extracellular matrix and facilitate tumor
invasion (14).
In the present study, significant differences in
D-dimer levels, ADPS and PDPS were observed in patients with
metastasis compared with those without metastasis (Table III). ROC analysis and multivariate
Cox regression analysis showed that ADPS was an independent
predictor of metastasis for patients with MM. Previous studies
reported that albumin and D-dimer served as independent prognostic
predictors of prognosis of patients with miliary tuberculosis
(32) and the postoperative survival
of patients with esophageal squamous cell carcinoma (13). In other studies investigating MM, low
serum albumin levels are predictors of morbidity and mortality in
patients with MM (33) and elevated
D-dimer levels indicated a poor prognosis (32). However, to the best of our knowledge,
the present study is the first to show ADPS as an independent
predictor of MM metastasis.
In the present study, the highest incidence of MM
was observed in individuals aged between 40–70 years, similar to
the reports from other studies with Chinese cohorts (32). Statistical analysis showed ulceration
and vertical growth phase were independent risk factors for tumor
metastasis in patients with MM and previous studies have also
identified ulceration as an independent prognostic factor in
patients with melanoma (34). In
certain Chinese studies >4 mm tumor thickness and clinical stage
III and IV were also found to be significant predictive factors
(5).
In the experimental cohort used in the present
study, surgery was the most common treatment, followed by surgery
combined with immunotherapy, and surgery combined with
bioimmunotherapy. To the best of our knowledge, it is unclear if
surgery is the best choice to completely remove all lesions in
patients with MM with locally advanced or early disease and in
patients with distant MM metastasis. However, previous studies have
shown that patients with MM with distant metastasis may still
benefit from surgery (35,36). Patients with stage IV MM are usually
treated with systemic biologics and/or chemotherapy; however,
treatment for patients with metastatic MM has been a challenge as
aggressive treatments, including combination of immunotherapy with
other therapies, have failed to show satisfactory efficacy
(37,38).
The cohort of the present study was compared with
the cohort of patients with MM in cBioPortal and significant
differences were found, including differences in OS, DFS, age at
diagnosis and anatomic locations of metastasis between the two
groups of patients. There may be several reasons for these
differences, for example the sample size of the experimental cohort
in the present study was small, and Caucasians comprised a majority
of the patients in the cBioPortal cohort, whereas all the patients
in the present study were Chinese. Melanoma is more common in
light-skinned individuals, as individuals lacking protective
melanin pigments are more susceptible to cutaneous melanoma
compared with darker-skinned individuals (22). Therefore lower quantities of
protective melanin pigment may increase the susceptibility of
Caucasians to damage caused by ultraviolet radiation (22,24).
Previous epidemiological and experimental data have indicated that
ultraviolet light, through its mutagenic activity, is the most
likely cause of cutaneous melanoma in Caucasian patients (39). MM in Caucasian patients also
predominantly occurs on the trunk and the most common type is the
superficial spreading type (40);
however, in Chinese patients, MM occurs most frequently on the
extremities or the mucosa (41).
Moreover, the majority of Caucasian patients are diagnosed at stage
I (20), whereas the majority of
Chinese patients are diagnosed at stage II or III (41). The reasons for these ethnic
differences should be a focus of future studies.
The present study has certain limitations. First,
the sample size was small, and all patients were recruited from a
single institution. However, the First Affiliated Hospital of
Zhengzhou University is a major referral center for MM treatment in
central China, and the study population can be considered
representative of this region. Second, some patients were lost to
follow-up as a number of patients failed to comply with regular
follow-up due to economic reasons or lack of awareness.
Overall, there are significant differences between
patients with MM from central China and those from other parts of
the world. ADPS may be a useful predictor of MM metastasis in the
early stages of disease.
Acknowledgements
Not applicable.
Funding
The present study was supported by grants from
Science and Technology Project of Henan (grant no. 182102310085)
and the Scientific Research Team Construction Foundation of Henan
Province (grant no. TD2011010).
Availability of data and materials
The datasets used or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
GSL and LBL designed the study. KS analyzed and
interpreted the patient data, and was a major contributor in
writing the manuscript. XRZ, ZYL, NS, LSG and YW analyzed and
interpreted the patient data. XC, ZWZ, BHX and SXY performed the
histological examination of the samples. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by The Ethics Committee of
the First Affiliated Hospital of Zhengzhou University (Zhengzhou,
China). Written informed consent was obtained from all individual
participants included in the study. The trial registration no. is
2018-LW-037 and this clinical trial was registered in the First
Affiliated Hospital of Zhengzhou University Clinical Trial Registry
in March 2018.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
OS
|
overall survival
|
|
DFS
|
disease free survival
|
|
MM
|
malignant melanoma
|
|
LDH
|
lactate dehydrogenase
|
|
ADPS
|
serum albumin/D-dimer prognosis
score
|
|
PDPS
|
serum prealbumin/D-dimer prognosis
score
|
|
AUC
|
area under the curve
|
|
HR
|
hazard ratio
|
|
CI
|
confidence interval.
|
References
|
1
|
Gershenwald JE, Scolyer RA, Hess KR,
Sondak VK, Long GV, Ross MI, Lazar AJ, Faries MB, Kirkwood JM,
McArthur GA, et al: Melanoma staging: Evidence-based changes in the
American joint committee on cancer eighth edition cancer staging
manual. CA Cancer J Clin. 67:472–492. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gao J, Aksoy BA, Dogrusoz U, Dresdner G,
Gross B, Sumer SO, Sun Y, Jacobsen A, Sinha R, Larsson E, et al:
Integrative analysis of complex cancer genomics and clinical
profiles using the cBioPortal. Sci Signal. 6:12013. View Article : Google Scholar
|
|
3
|
Thompson JF, Soong SJ, Balch CM,
Gershenwald JE, Ding S, Coit DG, Flaherty KT, Gimotty PA, Johnson
T, Johnson MM, et al: Prognostic significance of mitotic rate in
localized primary cutaneous melanoma: An analysis of patients in
the multi-institutional American joint committee on cancer melanoma
staging database. J Clin Oncol. 29:2199–2205. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Temam S, Mamelle G, Marandas P, Wibault P,
Avril MF, Janot F, Julieron M, Schwaab G and Luboinski B:
Postoperative radiotherapy for primary mucosal melanoma of the head
and neck. Cancer. 103:313–319. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yu J, Luo X, Huang H, Zhai Z, Shen Z and
Lin H: Clinical characteristics of malignant melanoma in southwest
China: A single-center series of 82 consecutive cases and a
meta-analysis of 958 reported cases. PLoS One. 11:e01655912016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shoo BA and Kashani-Sabet M: Melanoma
arising in African-, Asian-, Latino- and Native-American
populations. Semin Cutan Med Surg. 28:96–102. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hao M, Zhao G, Du X, Yang Y and Yang J:
Clinical characteristics and prognostic indicators for metastatic
melanoma: Data from 446 patients in north China. Tumor Biol.
37:10339–10348. 2016. View Article : Google Scholar
|
|
8
|
Iacono D, Basile D, Gerratana L, Vitale
MG, Pelizzari G, Cinausero M, Poletto E, Puglisi F, Fasola G and
Minisini AM: Prognostic role of disease extent and
lymphocyte-monocyte ratio in advanced melanoma. Melanoma Res.
29:510–515. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Daneshmandi S, Wegiel B and Seth P:
Blockade of lactate dehydrogenase-a (LDH-A) improves efficacy of
anti-programmed cell death-1 (PD-1) therapy in melanoma. Cancers
(Basel). 11:E4502019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fanali G, di Masi A, Trezza V, Marino M,
Fasano M and Ascenzi P: Human serum albumin: From bench to bedside.
Mol Aspects Med. 33:209–290. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mittman N, Avram MM, Oo KK and
Chattopadhyay J: Prealbumin as an important predictor for survival
and nutritional status in hemodialysis and peritoneal dialysis
patients. Improving Prognosis for Kidney Disorders. Avram MM:
Springer; Dordrecht: pp. 61–67. 2002, View Article : Google Scholar
|
|
12
|
Fan L, Wang X, Chi C, Wang Y, Cai W, Shao
X, Xu F, Pan J, Zhu Y, Shangguan X, et al: Prognostic nutritional
index predicts initial response to treatment and prognosis in
metastatic castration-resistant prostate cancer patients treated
with abiraterone. Prostate. 77:1233–1241. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liu DQ, Li FF and Jia WH: Cumulative
scores based on plasma D-dimer and serum albumin levels predict
survival in esophageal squamous cell carcinoma patients treated
with transthoracic esophagectomy. Chin J Cancer. 35:112016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Diao D, Wang Z, Cheng Y, Zhang H, Guo Q,
Song Y, Zhu K, Li K, Liu D and Dang C: D-dimer: Not just an
indicator of venous thrombosis but a predictor of asymptomatic
hematogenous metastasis in gastric cancer patients. PLoS One.
9:e1011252014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Batschauer AP, Figueiredo CP, Bueno EC,
Ribeiro MA, Dusse LM, Fernandes AP, Gomes KB and Carvalho MG:
D-dimer as a possible prognostic marker of operable hormone
receptor-negative breast cancer. Ann Oncol. 21:1267–1272. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kilic M, Yoldas O, Keskek M, Ertan T, Tez
M, Gocmen E and Koc M: Prognostic value of plasma D-dimer levels in
patients with colorectal cancer. Colorectal Dis. 10:238–241. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Altiay G, Ciftci A, Demir M, Kocak Z, Sut
N, Tabakoglu E, Hatipoglu ON and Caglar T: High plasma D-dimer
level is associated with decreased survival in patients with lung
cancer. Clin Oncol (R Coll Radiol). 19:494–498. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Mirshahi SS, Pujade-Lauraine E, Soria C,
Mirshahi M, Fretault J, Bernadou A and Soria J: D-dimer and CA-125
levels in patients with ovarian cancer during antineoplastic
therapy. Prognostic significance for the success of anti-cancer
treatment. Cancer. 69:2289–2292. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ferrucci PF, Gandini S, Battaglia A,
Alfieri S, Di Giacomo AM, Giannarelli D, Cappellini GC, De Galitiis
F, Marchetti P, Amato G, et al: Baseline neutrophil-to-lymphocyte
ratio is associated with outcome of ipilimumab-treated metastatic
melanoma patients. Br J Cancer. 112:1904–1910. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schuurman MS, de Waal AC, Thijs EJM, van
Rossum MM, Kiemeney LALM and Aben KKH: Risk factors for second
primary melanoma among Dutch patients with melanoma. Br J Dermatol.
176:971–978. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cerami E, Gao J, Dogrusoz U, Gross BE,
Sumer SO, Aksoy BA, Jacobsen A, Byrne CJ, Heuer ML, Larsson E, et
al: The cBio cancer genomics portal: An open platform for exploring
multidimensional cancer genomics data. Cancer Discov. 2:401–404.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Brożyna AA, Jóźwicki W, Roszkowski K,
Filipiak J and Slominski AT: Melanin content in melanoma metastases
affects the outcome of radiotherapy. Oncotarget. 7:17844–17853.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Brozyna AA, Jozwicki W, Carlson JA and
Slominski AT: Melanogenesis affects overall and disease-free
survival in patients with stage III and IV melanoma. Hum Pathol.
44:2071–2074. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Slominski A, Kim TK, Brożyna AA,
Janjetovic Z, Brooks DL, Schwab LP, Skobowiat C, Jóźwicki W and
Seagroves TN: The role of melanogenesis in regulation of melanoma
behavior: Melanogenesis leads to stimulation of HIF-1α expression
and HIF-dependent attendant pathways. Arch Biochem Biophys.
563:79–93. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gatta A, Verardo A and Bolognesi M:
Hypoalbuminemia. Intern Emerg Med. 7 (Suppl 3):193–199. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Moujaess E, Fakhoury M, Assi T, Elias H,
El Karak F, Ghosn M and Kattan J: The Therapeutic use of human
albumin in cancer patients' management. Crit Rev Oncol Hematol.
120:203–209. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Li S, Xu H, Wu C, Wang W, Jin W, Gao H, Li
H, Zhang S, Xu J, Zhang W, et al: Prognostic value of
γ-glutamyltransferase-to-albumin ratio in patients with pancreatic
ductal adenocarcinoma following radical surgery. Cancer Med.
8:572–584. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Matsuda S, Takeuchi H, Kawakubo H, Fukuda
K, Nakamura R, Takahashi T, Wada N, Saikawa Y, Omori T and Kitagawa
Y: Cumulative prognostic scores based on plasma fibrinogen and
serum albumin levels in esophageal cancer patients treated with
transthoracic esophagectomy: Comparison with the glasgow prognostic
score. Ann Surg Oncol. 22:302–310. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Forrest LM, Mcmillan DC, Mcardle CS,
Angerson WJ and Dunlop DJ: Comparison of an inflammation-based
prognostic score (GPS) with performance status (ECOG) in patients
receiving platinum-based chemotherapy for inoperable non-small-cell
lung cancer. Br J Cancer. 90:1704–1706. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Desch A, Gebhardt C, Utikal J and
Schneider SW: D-dimers in malignant melanoma: Association with
prognosis and dynamic variation in disease progress. Int J Cancer.
140:914–921. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kwon HC, Oh SY, Lee S, Kim SH, Han JY, Koh
RY, Kim MC and Kim HJ: Plasma levels of prothrombin fragment F1+2,
D-dimer and prothrombin time correlate with clinical stage and
lymph node metastasis in operable gastric cancer patients. Jpn J
Clin Oncol. 38:2–7. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Deng W, Yu M, Ma H, Hu LA, Chen G, Wang Y,
Deng J, Li C, Tong J and Wang DX: Predictors and outcome of
patients with acute respiratory distress syndrome caused by miliary
tuberculosis: A retrospective study in Chongqing, China. BMC Infect
Dise. 12:1212012. View Article : Google Scholar
|
|
33
|
Datta M, Savage P, Lovato J and Schwartz
GG: Serum calcium, albumin and tumor stage in cutaneous malignant
melanoma. Future Oncol. 12:2205–2214. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhang M and Zhang N: Clinical and
prognostic factors in 98 patients with malignant melanoma in China.
J Int Med Res. 45:1369–1377. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Raigani S, Cohen S and Boland GM: The role
of surgery for melanoma in an era of effective systemic therapy.
Curr Oncol Rep. 19:172017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Saranga-Perry V, Ambe C, Zager JS and
Kudchadkar RR: Recent developments in the medical and surgical
treatment of melanoma. Ca Cancer J Clin. 64:172–185. 2014.
View Article : Google Scholar
|
|
37
|
Flaherty KT, Puzanov I, Kim KB, Ribas A,
McArthur GA, Sosman JA, O'Dwyer PJ, Lee RJ, Grippo JF, Nolop K and
Chapman PB: Inhibition of mutated, activated BRAF in metastatic
melanoma. N Engl J Med. 363:809–819. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Nestle FO, Alijagic S, Gilliet M, Sun Y,
Grabbe S, Dummer R, Burg G and Schadendorf D: Vaccination of
melanoma patients with peptide- or tumor lysate-pulsed dendritic
cells. Nat Med. 4:328–332. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Slominski AT and Carlson JA: Melanoma
resistance: A bright future for academicians and a challenge for
patient advocates. Mayo Clinic Proc. 89:429–433. 2014. View Article : Google Scholar
|
|
40
|
Huang K, Xu Y, Joseph R, Bagaria SP, Misra
S and Chen Y: Comparative analysis of acral melanoma in Chinese and
caucasian patients. Ann Surg Oncol. 26:S158–S159. 2019.
|
|
41
|
Huang YS, Chen XX, Yang SX, Wu LS, Zhao
JY, Li XY, Tu P and Li H: Preliminary exploration of the clinical
features of Chinese patients with skin malignancies and
premalignancies: A retrospective study of 1420 cases from peking
university first hospital. J Eur Acad Dermatol Venereol.
27:1114–1119. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Taylor AM, Shih J, Ha G, Gao GF, Zhang X,
Berger AC, Schumacher SE, Wang C, Hu H, Liu J, et al: Genomic and
functional approaches to understanding cancer aneuploidy. Cancer
Cell. 33:676–689.e673. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Sanchez-Vega F, Mina M, Armenia J, Chatila
WK, Luna A, La KC, Dimitriadoy S, Liu DL, Kantheti HS, Saghafinia
S, et al: Oncogenic signaling pathways in the cancer genome atlas.
Cell. 173:321–337.e310. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Liu J, Lichtenberg T, Hoadley KA, Poisson
LM, Lazar AJ, Cherniack AD, Kovatich AJ, Benz CC, Levine DA, Lee
AV, et al: An integrated TCGA pan-cancer clinical data resource to
drive high-quality survival outcome analytics. Cell.
173:400–416.e411. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Hoadley KA, Yau C, Hinoue T, Wolf DM,
Lazar AJ, Drill E, Shen R, Taylor AM, Cherniack AD, Thorsson V, et
al: Cell-of-origin patterns dominate the molecular classification
of 10,000 tumors from 33 types of cancer. Cell. 173:291–304.e296.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Gao Q, Liang WW, Foltz SM, Mutharasu G,
Jayasinghe RG, Cao S, Liao WW, Reynolds SM, Wyczalkowski MA, Yao L,
et al: Driver fusions and their implications in the development and
treatment of human cancers. Cell Rep. 23:227–238.e223. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Ellrott K, Bailey MH, Saksena G, Covington
KR, Kandoth C, Stewart C, Hess J, Ma S, Chiotti KE, McLellan M, et
al: Scalable open science approach for mutation calling of tumor
exomes using multiple genomic pipelines. Cell Syst. 6:271–281.e277.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Liang WS, Hendricks W, Kiefer J, Schmidt
J, Sekar S, Carpten J, Craig DW, Adkins J, Cuyugan L, Manojlovic Z,
et al: Integrated genomic analyses reveal frequent TERT aberrations
in acral melanoma. Genome Res. 27:524–532. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Berger MF, Hodis E, Heffernan TP, Deribe
YL, Lawrence MS, Protopopov A, Ivanova E, Watson IR, Nickerson E,
Ghosh P, et al: Melanoma genome sequencing reveals frequent PREX2
mutations. Nature. 485:502–506. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Hodis E, Watson IR, Kryukov GV, Arold ST,
Imielinski M, Theurillat JP, Nickerson E, Auclair D, Li L, Place C,
et al: A landscape of driver mutations in melanoma. Cell.
150:251–263. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Krauthammer M, Kong Y, Ha BH, Evans P,
Bacchiocchi A, McCusker JP, Cheng E, Davis MJ, Goh G, Choi M, et
al: Exome sequencing identifies recurrent somatic RAC1 mutations in
melanoma. Nat Genetics. 44:1006–1014. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Van Allen EM, Wagle N, Sucker A, Treacy
DJ, Johannessen CM, Goetz EM, Place CS, Taylor-Weiner A, Whittaker
S, Kryukov GV, et al: The genetic landscape of clinical resistance
to RAF inhibition in metastatic melanoma. Cancer Discov. 4:94–109.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Hugo W, Zaretsky JM, Sun L, Song C, Moreno
BH, Hu-Lieskovan S, Berent-Maoz B, Pang J, Chmielowski B, Cherry G,
et al: Genomic and transcriptomic features of response to anti-PD-1
therapy in metastatic melanoma. Cell. 165:35–44. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Shain AH, Garrido M, Botton T, Talevich E,
Yeh I, Sanborn JZ, Chung J, Wang NJ, Kakavand H, Mann GJ, et al:
Exome sequencing of desmoplastic melanoma identifies recurrent
NFKBIE promoter mutations and diverse activating mutations in the
MAPK pathway. Nat Genetics. 47:1194–1199. 2015. View Article : Google Scholar : PubMed/NCBI
|