Introduction
Urothelial carcinoma (UC) is the most common cancer
of the bladder and upper urinary tract and is invasive and lethal,
especially in advanced and metastatic patients (1,2).
Advanced UC patients generally have a poor prognosis, and only a
few patients survive more than five years (3).
Pembrolizumab, a humanized monoclonal antibody that
targets programmed death receptor-1, was associated with a
significant overall survival (OS) benefit when compared with
docetaxel, paclitaxel and vinflunine in the second-line treatment
of metastatic UC in the Phase III trial KEYNOTE-045 (4). Since December 2017, pembrolizumab has
been approved in Japan as a second-line treatment for radical
unresectable UC that has become exacerbated after chemotherapy
(5). However, cisplatin-based
systemic chemotherapy is still the gold-standard approach for
patients with advanced or metastatic UC in the first line (6–9).
Combined chemotherapy with gemcitabine and cisplatin (GC) has been
accepted as another standard treatment for advanced UC, as this
therapy showed equivalent efficacy and less toxicity than combined
chemotherapy of methotrexate, vinblastine, doxorubicin and
cisplatin (MVAC) in a randomized phase 3 trial (10). However, there have been cases in
which GC chemotherapy was continuously administered or
re-administered because the optimum number of courses for GC
chemotherapy has not been determined and no second-line standard
therapy had been established before pembrolizumab was allowed to be
used in Japan.
In the present study, we retrospectively assessed
the clinical outcome in patients who received GC chemotherapy as
first-line treatment for advanced or metastatic UC in order to
clarify the timing of switching from GC chemotherapy.
Materials and methods
All of the patients provided their written informed
consent to participate in this study, and the study protocol was
approved by the Ethics Committee of the National Hospital
Organization Kyushu Cancer Center (Fukuoka, Japan).
The patients with locally advanced or metastatic UC
who received first-line chemotherapy with GC at our institution
between June 2009 and August 2017 were retrospectively evaluated.
UC was histopathologically diagnosed in all cases (11). In the GC regimen, gemcitabine (1,000
mg/m2) was administered intravenously on days 1, 8 and
15, and cisplatin (70 mg/m2) were administered
intravenously on day 2. The cycle was basically repeated every 28
days (7). Cisplatin dose reduction
was based on the estimated glomerular filtration rate (eGFR); the
cisplatin dose was reduced to 75% when the eGFR was 46–60
ml/min/1.73 m2 and to 50% when the eGFR was 30–45
ml/min/1.73 m2. When the eGFR was <30 ml/min/1.73
m2, cisplatin administration was basically prohibited
(12,13).
Decisions regarding adverse events were made based
on the Common Terminology Criteria for Adverse Events, version 4.0
(14). If Grade ≥2 adverse events
were observed, dose reduction of GC chemotherapy was performed to
ensure that adverse events were grade ≤1 in the next cycle. The GC
regimen was repeated until disease progression or unacceptable
adverse events occurred. Tumor measurements were generally
performed by computed tomography before and after every two to
three cycles. The tumor response was evaluated as the best response
according to the Response Evaluation Criteria In Solid Tumors,
version 1.1 (15). The overall
response rate is defined as the proportion of patients who achieve
a partial or complete response to GC chemotherapy.
Statistical analysis
Statistical analyses were performed using the
JMP® Pro, version 12.2.0, software package (SAS
Institute, Inc.). The OS was calculated from the day on which
chemotherapy was started until the date of the last follow-up
examination or death from any cause. The progression-free survival
(PFS) and OS were evaluated using the Kaplan-Meier method, and the
log-rank test was used to determine differences in the PFS and OS
among the primary tumor site groups. The significance of
associations between the clinical parameters and OS was assessed
using the Cox proportional hazards regression model. P<0.05 was
considered to indicate a statistically significant difference.
Results
Patients characteristics
The clinical characteristics of the 61 patients
(male, n=42; female, n=19; median age, 69 years; range, 49–86
years) are listed in Table I. All of
the patients received GC as the first-line chemotherapy for
advanced or metastatic UC. Thirty patients had upper urinary tract
UC, 25 had bladder UC, and 6 had both types of UC. Thirty patients
(49.2%) had visceral metastasis. The cisplatin dose was reduced in
31 patients (50.1%) due to renal dysfunction from the initial cycle
administration. The median cycle number for GC chemotherapy was 4
(range, 1–13).
 | Table I.Patients characteristics. |
Table I.
Patients characteristics.
| Characteristics
(n=61) | Number of
patients |
|---|
| Sex |
| Male | 42 |
|
Female | 19 |
| Age, years |
| Median
(range) | 69 (49–86) |
| ECOG PS |
| 0 | 31 |
| 1 | 26 |
| ≥2 | 4 |
| Anemia (Hb <10
g/dl) |
| Yes | 8 |
| No | 53 |
| CRP (mg/dl) |
|
<0.3 | 15 |
| ≥0.3 | 46 |
| Albumin (g/dl) |
|
≥4.0 | 18 |
|
<4.0 | 43 |
| NLR |
| Median
(range) | 2.9 (0.7–17.3) |
| Primary tumor
site |
|
Bladder | 25 |
| Upper
urinary tract | 30 |
| Bladder
+ upper urinary tract | 6 |
| Clinical tumor
classification |
| Ta | 1 |
| T1 | 6 |
| T2 | 15 |
| T3 | 26 |
| T4 | 13 |
| Histologic
grade |
| G1 | 0 |
| G2 | 15 |
| G3 | 41 |
|
Unknown | 5 |
| Histology |
| Pure
UC | 45 |
| Mixed UC | 16 |
| Surgical treatment
for the primary tumor |
|
Cystectomy | 13 |
|
Cystectomy +
nephroureterectomy | 5 |
|
Nephrouureterectomy | 21 |
|
Transurethral resection | 12 |
| Visceral
metastasis |
|
Negative | 31 |
|
Positive | 30 |
| Cisplatin dose
reduction from initial administration |
|
Yes | 31 |
| No | 30 |
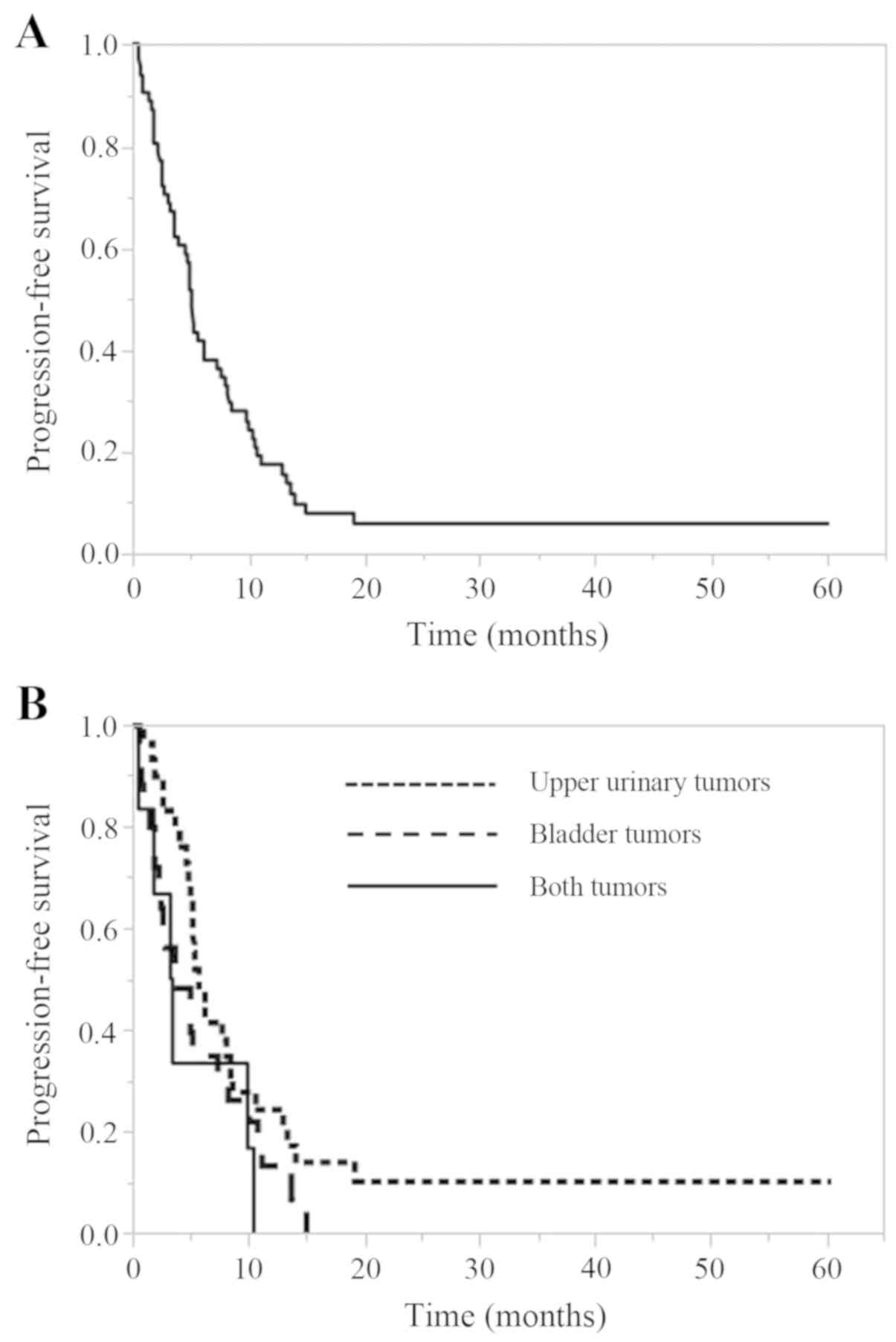
The PFS of all cases and according to
the primary tumor site
The PFS of all cases and according to the primary
tumor site is shown in Fig. 1. The
median PFS of all cases was 5.2 months (95% confidence interval
[CI], 3.7–7.5 months). The median PFS for upper urinary tumors was
5.7 months (95% CI, 4.8–8.4 months), that for bladder tumors was
3.7 months (95% CI, 2.3–7.5 months), and that for cases with both
tumors was 3.3 months (95% CI, 0.6–10.4). There was no significant
difference in the PFS among the 3 tumor site groups (P=0.132).
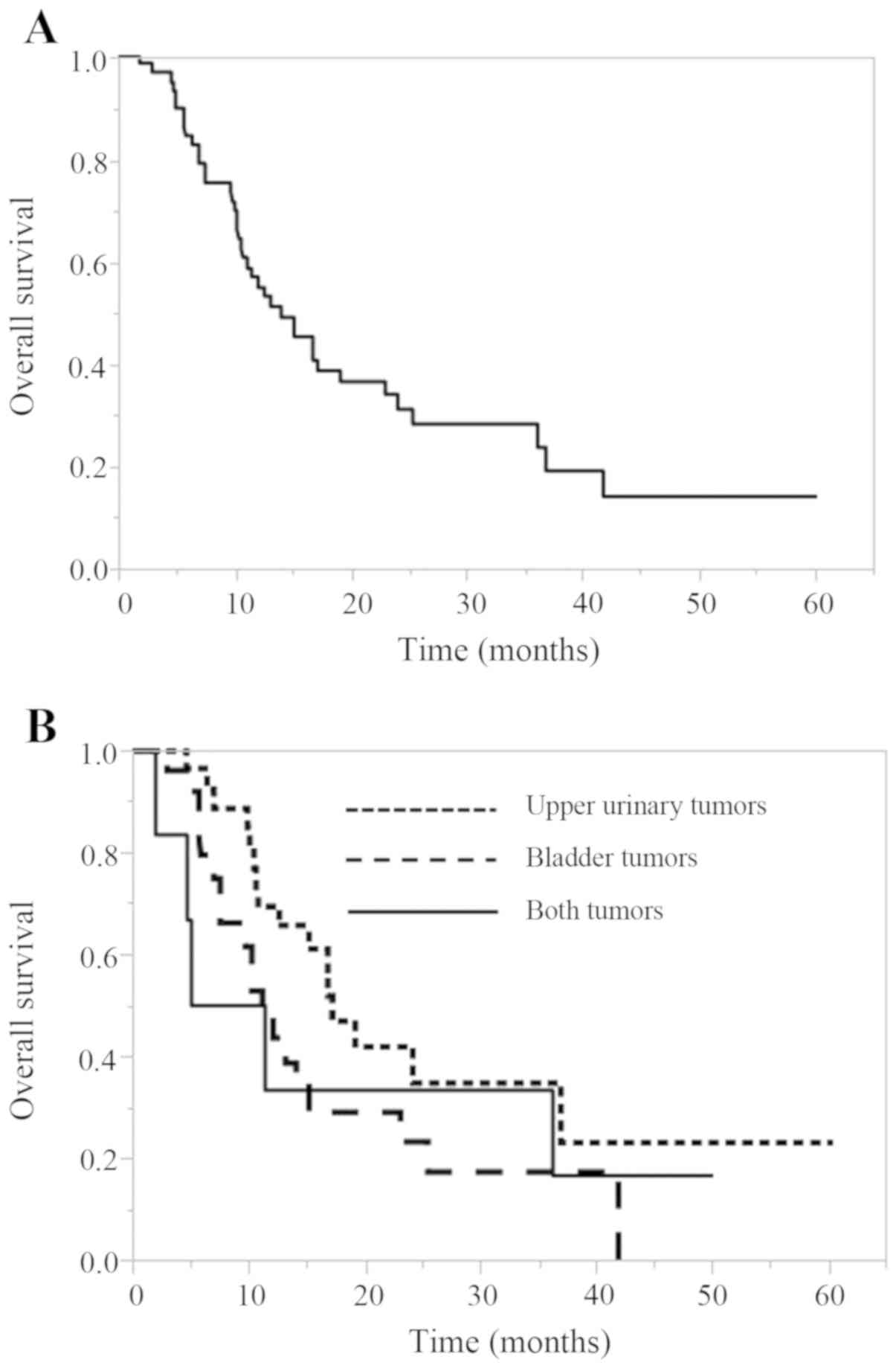
The OS of all cases and according to
the primary tumor site
The OS of all cases and according to the primary
tumor site is shown in Fig. 2. The
median OS of all cases was 14.1 months (95% CI, 10.7–19.3 months).
The median OS for upper urinary tumors was 17.2 months (95% CI,
10.8–36.9 months), that for bladder tumors was 11.2 months (95% CI,
7.5–15.2 months), and that for cases with both tumors was 8.3
months (95% CI, 1.9–36.2). There was no significant difference in
the OS among the 3 tumor site groups (P=0.157).
The response analysis in patients who
received GC chemotherapy
The objective tumor responses are shown in Table II. Among the 61 patients, a complete
response (CR) was confirmed in 7 patients (11.5%), while 20 (32.8%)
showed a partial response (PR), with an overall response rate of
44.3%.
| Table II.The analysis of the responses of
patients who received GC chemotherapy. |
Table II.
The analysis of the responses of
patients who received GC chemotherapy.
| Response | Number of
patients | Response rate
(%) |
|---|
| CR | 7 | 11.5 |
| PR | 20 | 32.8 |
| SD | 20 | 32.8 |
| PD | 14 | 22.9 |
| Overall response
rate (CR+PR) | 27 | 44.3 |
Univariate and multivariate analyses
of the associations between various factors and the OS with GC
chemotherapy
To identify the prognostic factors associated with
the OS with GC chemotherapy, univariate and multivariate analyses
using the Cox proportional hazards model were performed (Table III). Univariate analyses for
various factors revealed that history of nephrectomy, the Eastern
Cooperative Oncology Group Performance Status, the
neutrophil-to-lymphocyte ratio (NLR), presence of visceral
metastasis, presence of cisplatin dose reduction from initial
administration, number of GC cycles, and best response to GC
chemotherapy were prognostic variables. The multivariate analyses
revealed that an NLR ≥3.0 (hazard ratio [HR], 2.521, 95%
CI=1.179–5.624, P=0.017) and a best response to GC chemotherapy of
CR+PR (HR 0.110, 95% CI=0.028–0.411, P<0.001) were independent
prognostic factors. However, the number of GC cycles was not an
independent prognostic factor (P=0.387).
| Table III.The univariate and multivariate
analyses of the factors associated with OS in patients receiving GC
chemotherapy. |
Table III.
The univariate and multivariate
analyses of the factors associated with OS in patients receiving GC
chemotherapy.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (years) |
|
<70 | 1 |
|
|
|
|
≥70 | 1.029
(0.539–1.922) | 0.929 |
|
|
| Sex |
|
Male | 1 |
|
|
|
|
Female | 0.658
(0.305–1.305) | 0.239 |
|
|
| Primary tumor
site |
|
Bladder | 1 |
|
|
|
| Upper
urinary tract | 0.533
(0.269–1.039) | 0.065 |
|
|
| Bladder
+ upper urinary tract | 0.917
(0.298–2.335) | 0.866 |
|
|
| Histology |
| Pure
UC | 1 |
|
|
|
| Mixed
UC | 0.982
(0.4800–1.891) | 0.959 |
|
|
| ECOG PS |
| 0 | 1 |
| 1 |
|
| ≥1 | 2.976
(1.552–5.944) | 0.001 | 1.543
(0.682–3.598) | 0.301 |
| Anemia (Hb <10
g/dl) |
|
Negative | 1 |
|
|
|
|
Positive | 1.679
(0.715–3.498) | 0.218 |
|
|
| NLR |
|
<3.0 | 1 |
| 1 |
|
|
≥3.0 | 2.143
(1.142–4.129) | 0.018 | 2.521
(1.179–5.624) | 0.017 |
| Albumin (g/dl) |
| ≥4.0 | 1 |
|
|
|
|
<4.0 | 1.560
(0.801–3.270) | 0.197 |
|
|
| CRP (mg/dl) |
|
<0.3 | 1 |
|
|
|
|
≥0.3 | 1.536
(0.743–3.588) | 0.259 |
|
|
| Local excision
surgery |
|
Positive | 1 |
|
|
|
|
Negative | 1.386
(0.695–2.667) | 0.345 |
|
|
| Best response to GC
therapy |
| PD | 1 |
| 1 |
|
| SD | 0.266
(0.117–0.611) | 0.002 | 0.414
(0.164–1.035) | 0.059 |
|
CR+PR | 0.129
(0.054–0.308) | <0.001 | 0.110
(0.028–0.411) | <0.001 |
| Cisplatin dose
reduction from initial administration |
|
Negative | 1 |
| 1 |
|
|
Positive | 1.996
(1.065–3.845) | 0.031 | 1.831
(0.936–3.667) | 0.077 |
| No. GC cycles |
| ≤4 | 1 |
| 1 |
|
|
>4 | 0.448
(0.229–0.844) | 0.013 | 1.565
(0.572–4.472) | 0.387 |
| Visceral
metastases |
|
Negative | 1 |
| 1 |
|
|
Positive | 2.171
(1.141–4.268) | 0.018 | 0.997
(0.453–2.255) | 0.994 |
Discussion
Cisplatin-based systemic chemotherapy is the
gold-standard approach for treating patients with advanced or
metastatic UC (16,17). However, randomized trials to
determine the optimal number of cycles have not yet been performed.
In addition, a standard second-line therapy had not been
established in Japan for a long time before the relatively recent
approval of pembrolizumab. Therefore, there were cases in which GC
chemotherapy was continuously administered until disease
progression or re-administered if a long time had passed since the
last GC chemotherapy session.
Immune checkpoint inhibitors have greatly improved
the survival of patients with several cancers (18–22). The
PD-1 and PD-L1 inhibitors atezolizumab and pembrolizumab were
approved for advanced UC by the United States Food and Drug
Administration and the European Medicines Agency (23–26).
Since December 2017, only pembrolizumab has been approved in Japan
as a second-line treatment for radical unresectable UC that has
become exacerbated after chemotherapy. Pembrolizumab was found to
be associated with a significant OS benefit in second-line therapy
for advanced or metastatic UC in the Phase III trial KEYNOTE-045
(4). In the present study, we
retrospectively assessed the clinical outcome in patients who
received GC chemotherapy as first-line treatment for advanced or
metastatic UC in order to clarify the proper timing of switching
from GC chemotherapy, with the aim of improving the efficacy of
subsequent pembrolizumab administration.
A previous study reported that the median PFS in
patients with locally advanced or metastatic UC who receive
cisplatin-based first-line treatment ranges from 7.7 to 8.3 months,
and the median OS ranges from 14.0 to 15.2 months (6). In the present study, the median PFS and
OS of all cases was 5.2 and 14.1 months, respectively (Figs. 1 and 2), and neither of these rates is
satisfactory.
To identify the prognostic factors associated with
the OS with GC chemotherapy, univariate and multivariate analyses
using the Cox proportional hazards model were performed (Table III). The multivariate analyses
revealed that the pretreatment factor NLR ≥3.0 (HR, 2.521, 95%
CI=1.179–5.624, P=0.017) and the posttreatment factor best response
to GC therapy of CR+PR (HR 0.110, 95% CI=0.028–0.411, P<0.001)
were independent prognostic factors. However, the number of GC
cycles was not an independent prognostic factor (P=0.387). These
findings suggest that regardless of the number of cycles of GC
chemotherapy, changes to therapy should be considered at an early
stage for cases with a therapeutic effect of stable disease (SD) or
less. In upper urinary tract UC, the cisplatin dose was reduced in
17 patients (56.7%) due to renal dysfunction after the initial
cycle administration. The median number of cycles for GC
chemotherapy was 4 (range, 2–10). According to the objective tumor
responses, a complete response (CR) was confirmed in 6 patients
(20.0%), while 8 (26.7%) showed a partial response (PR), with an
overall response rate of 46.7%. In the present study, these results
(rate of cisplatin reduction, cycle number and overall response
rate) for upper urinary tract UC were similar to those of all
cases.
A previous retrospective study reported that four
cycles of platinum-based first-line chemotherapy appeared adequate
for treating advanced UC and did not significantly compromise the
survival of these patients (27). A
prospective study of the ongoing phase III FOCUS trial in South
Korea to determine the optimal duration of chemotherapy in patients
with advanced UC showed a non-inferior OS between four and six
cycles of first-line cisplatin-based chemotherapy (https://clinicaltrials.gov/ct2/show/NCT03296306).
Further results of that study are awaited. In addition, clinical
investigations of second-line switching maintenance therapy with
PD-1 or PD-L1 inhibitors in patients with stable but responding
disease after first-line therapy are ongoing. Such trials,
including a Study of Avelumab in Patients with Locally Advanced or
Metastatic Urothelial Cancer (JAVELIN Bladder 100) (https://clinicaltrials.gov/ct2/show/NCT02603432) and
Testing the PD-1 Inhibitor Pembrolizumab as Maintenance Therapy
after Initial Chemotherapy in Metastatic Bladder Cancer (https://clinicaltrials.gov/ct2/show/NCT02500121), have
required at least 4 and not 6 cycles of prior platinum-based
chemotherapy. Furthermore, the purpose of the ongoing KEYNOTE-361
is to determine the efficacy and safety of pembrolizumab with or
without chemotherapy vs. chemotherapy alone in participants with
advanced or metastatic UC (https://clinicaltrials.gov/ct2/show/NCT02853305).
Depending on the results of these trials, the treatment policy for
advanced or metastatic UC may change significantly in the
future.
The omission of excessive cycles may avoid
unnecessary cumulative toxicity and facilitate a better transition
to second-line therapy and investigational switching maintenance
therapy strategies. Notably, however, the number of GC cycles was
not an independent prognostic factor in the present study (number
of GC cycles ≤4 vs. >4, P=0.387). We therefore believe that four
cycles of platinum-based first-line chemotherapy for advanced UC is
adequate. Cisplatin in particular is associated with significant
cumulative toxicity, especially neuropathy, venous thromboembolism
and renal dysfunction, which may be irreversible and sometimes
lethal, rendering it challenging to deliver the full course of six
cycles of treatment (28,29). Patients who tolerate the therapy
better may receive more cycles and, consequently, experience better
outcomes than less-tolerant patients. However, we were unable to
identify such an association in this study, although this
confounding factor would bias the analysis in favor of more
cycles.
In reports of patients with other cancer type,
chemotherapy has demonstrated an excellent response after exposure
to immune checkpoint inhibitors (30,31).
Chemotherapies have been shown to exert immune-reactive effects,
such as the upregulation of MHC class molecules or tumor antigens,
causing an increase in tumor antigen presentation (32,33), and
these effects are theoretically beneficial for the
immunotherapeutic strategies.
On the other hand, chemotherapies have also been
shown to decrease the number of immunosuppressive cells in the
tumor microenvironment, such as regulatory T cells and
myeloid-derived suppressor cells, thereby increasing the helper
T-cell accumulation at the tumor site (34,35).
This may be one reason why chemotherapy is effective after immune
checkpoint inhibitor therapy. These results also suggest that it is
better to change the regimen when appropriate, regardless of the
number of first-line chemotherapy cycles, as part of sequence
treatment.
The pretreatment NLR was also an independent
prognostic factor in the present study (cut-off value ≥3.0, HR,
2.521, 95% CI=1.179–5.624, P=0.017) (Table III). Previous systemic reviews and
meta-analyses have found the NLR to be a prognostic indicator in
the upper urinary tract and bladder (36–38). The
NLR can be easily determined from a full blood count and can
potentially function as a simple and inexpensive assessment of the
cancer prognosis, but the optimal cut-off value for the NLR remains
to be established (39). In
addition, the NLR is a dynamic marker, varying across time points
during a patients treatment course. Although the NLR alone should
not be used to justify changing the treatment strategy, regimen
changes should be considered at an early stage while also taking
the NLR into consideration. Of note, a high NLR has also been
associated with a poor outcome across studies, even in immune
checkpoint inhibitor-treated patients (40).
As with similar previous studies, our study is
limited by its retrospective nature and its analysis of a limited
number of cases in a single institution. Confirmatory studies with
larger populations may be required.
In conclusion, these real-world findings indicate
that regardless of the number of cycles of GC chemotherapy for
advanced or metastatic UC, changes to the therapy should be
considered at an early stage for cases with a poor therapeutic
effect (SD or less). Future clinical trials will be needed in order
to determine the optimal number of GC chemotherapy courses.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors contributions
NF, TN and MN designed the study. DT and KI
extracted the data. DT, KI, TI and KT assisted with the data
processing and statistical analysis. NF and MN wrote the article.
TN and MN supervised the study and critically reviewed the
manuscript. All authors have read and approved the final version of
the manuscript.
Ethics approval and consent to
participate
The present case report was approved by the
Institutional Review Board of National Hospital Organization Kyushu
Cancer Center (2014-99), and written informed consent was obtained
from the patient.
Patient consent for publication
The patient provided written informed consent for
the publication of any associated data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lin T, Liu Z, Liu L, Yang L, Han P, Zhang
P and Wei Q: Prospective evaluation of fluorescence in situ
hybridization for diagnosing urothelial carcinoma. Oncol Lett.
13:3928–3934. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Niegisch G, Gerullis H, Lin SW, Pavlova J,
Gondos A, Rudolph A, Haas G, Hennies N and Kramer MW: A real-world
data study to evaluate treatment patterns, clinical characteristics
and survival outcomes for first- and second-line treatment in
locally advanced and metastatic urothelial cancer patients in
Germany. J Cancer. 9:1337–1348. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nakagawa T, Taguchi S, Kanatani A, Kawai
T, Ikeda M, Urakami S, Matsumoto A, Komemushi Y, Miyakawa J, Yamada
D, et al: Oncologic outcome of metastasectomy for urothelial
carcinoma: Who is the best candidate? Ann Surg Oncol. 24:2794–2800.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bellmunt J, de Wit R, Vaughn DJ, Fradet Y,
Lee JL, Fong L, Vogelzang NJ, Climent MA, Petrylak DP, Choueiri TK,
et al: Pembrolizumab as second-line therapy for advanced urothelial
carcinoma. N Engl J Med. 376:1015–1026. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yuasa T, Urakami S and Yonese J: Recent
advances in medical therapy for metastatic urothelial cancer. Int J
Clin Oncol. 23:599–607. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
von der Maase H, Sengelov L, Roberts JT,
Ricci S, Dogliotti L, Oliver T, Moore MJ, Zimmermann A and Arning
M: Long-term survival results of a randomized trial comparing
gemcitabine plus cisplatin, with methotrexate, vinblastine,
doxorubicin, plus cisplatin in patients with bladder cancer. J Clin
Oncol. 23:4602–4608. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sternberg CN, de Mulder P, Schornagel JH,
Theodore C, Fossa SD, van Oosterom AT, Witjes JA, Spina M, van
Groeningen CJ, Duclos B, et al: Seven year update of an EORTC phase
III trial of high-dose intensity M-VAC chemotherapy and G-CSF
versus classic M-VAC in advanced urothelial tract tumours. Eur J
Cancer. 42:50–54. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Saxman SB, Propert KJ, Einhorn LH,
Crawford ED, Tannock I, Raghavan D, Loehrer PJ Sr and Trump D:
Long-term follow-up of a phase III intergroup study of cisplatin
alone or in combination with methotrexate, vinblastine, and
doxorubicin in patients with metastatic urothelial carcinoma: A
cooperative group study. J Clin Oncol. 15:2564–2569. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bellmunt J, von der Maase H, Mead GM,
Skoneczna I, De Santis M, Daugaard G, Boehle A, Chevreau C,
Paz-Ares L, Laufman LR, et al: Randomized phase III study comparing
paclitaxel/cisplatin/gemcitabine and gemcitabine/cisplatin in
patients with locally advanced or metastatic urothelial cancer
without prior systemic therapy: EORTC intergroup study 30987. J
Clin Oncol. 30:1107–1113. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
von der Maase H, Hansen SW, Roberts JT,
Dogliotti L, Oliver T, Moore MJ, Bodrogi I, Albers P, Knuth A,
Lippert CM, et al: Gemcitabine and cisplatin versus methotrexate,
vinblastine, doxorubicin, and cisplatin in advanced or metastatic
bladder cancer: Results of a large, randomized, multinational,
multicenter, phase III study. J Clin Oncol. 18:3068–3077. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Moch H, Cubilla AL, Humphrey PA, Reuter VE
and Ulbright TM: The 2016 WHO classification of tumours of the
urinary system and male genital organs-part A: Renal, penile and
testicular tumours. Eur Urol. 70:93–105. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Merchan JR: Chemotherapy-related
nephrotoxicity and dose modification n patients with renal
insufficiency. UpToDate. Post TW: UpToDate; 2016
|
|
13
|
The Japanese Society of Nephrology and
Pharmacotherapy. http://jsnp.org/July 15–2019
|
|
14
|
http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_40
|
|
15
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
National Comprehensive Cancer Network:
Guidelines on bladder cancer. 2019 Jun 1. https://www.nccn.org/professionals/physician_gls/pdf/bladder.pdf
|
|
17
|
European Association of Urology:
Guidelines on bladder cancer. 2019 Jun 1. https://uroweb.org/guideline/bladder-cancer-muscle-invasive-and-metastatic/
|
|
18
|
Hodi FS, ODay SJ, McDermott DF, Weber RW,
Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel
JC, et al: Improved survival with ipilimumab in patients with
metastatic melanoma. N Engl J Med. 363:711–723. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Larkin J, Chiarion-Sileni V, Gonzalez R,
Grob JJ, Cowey CL, Lao CD, Schadendorf D, Dummer R, Smylie M,
Rutkowski P, et al: Combined nivolumab and ipilimumab or
monotherapy in untreated melanoma. N Engl J Med. 373:23–34. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Brahmer J, Reckamp KL, Baas P, Crinò L,
Eberhardt WE, Poddubskaya E, Antonia S, Pluzanski A, Vokes EE,
Holgado E, et al: Nivolumab versus Docetaxel in advanced
squamous-cell non-small-cell lung cancer. N Engl J Med.
373:123–135. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Borghaei H, Paz-Ares L, Horn L, Spigel DR,
Steins M, Ready NE, Chow LQ, Vokes EE, Felip E, Holgado E, et al:
Nivolumab versus Docetaxel in advanced nonsquamous non-small-cell
lung cancer. N Engl J Med. 373:1627–1639. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Motzer RJ, Escudier B, McDermott DF,
George S, Hammers HJ, Srinivas S, Tykodi SS, Sosman JA, Procopio G,
Plimack ER, et al: Nivolumab versus everolimus in advanced
renal-cell carcinoma. N Engl J Med. 373:1803–1813. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
De Santis M, Bellmunt J, Mead G, Kerst JM,
Leahy M, Maroto P, Gil T, Marreaud S, Daugaard G, Skoneczna I, et
al: Randomized phase II/III trial assessing gemcitabine/carboplatin
and methotrexate/carboplatin/vinblastine in patients with advanced
urothelial cancer who are unfit for cisplatin-based chemotherapy:
EORTC study 30986. J Clin Oncol. 30:191–196. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Balar AV, Galsky MD, Rosenberg JE, Powles
T, Petrylak DP, Bellmunt J, Loriot Y, Necchi A, Hoffman-Censits J,
Perez-Gracia JL, et al: Atezolizumab as first-line treatment in
cisplatin-ineligible patients with locally advanced and metastatic
urothelial carcinoma: A single-arm, multicentre, phase 2 trial.
Lancet. 389:67–76. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Balar AV, Castellano D, ODonnell PH,
Grivas P, Vuky J, Powles T, Plimack ER, Hahn NM, de Wit R, Pang L,
et al: First-line pembrolizumab in cisplatin-ineligible patients
with locally advanced and unresectable or metastatic urothelial
cancer (KEYNOTE-052): A multicentre, single-arm, phase 2 study.
Lancet Oncol. 18:1483–1492. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Galsky MD, Hahn NM, Rosenberg J, Sonpavde
G, Hutson T, Oh WK, Dreicer R, Vogelzang N, Sternberg CN, Bajorin
DF and Bellmunt J: Treatment of patients with metastatic urothelial
cancer ‘unfit’ for Cisplatin-based chemotherapy. J Clin Oncol.
29:2432–2438. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sonpavde GP, Mariani L, Lo Vullo S, Raggi
D, Giannatempo P, Bamias A, Crabb SJ, Bellmunt J, Yu EY, Niegisch
G, et al: Impact of the number of cycles of platinum based first
line chemotherapy for advanced urothelial carcinoma. J Urol.
200:1207–1214. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chovanec M, Abu Zaid M, Hanna N, El-Kouri
N, Einhorn LH and Albany C: Long-term toxicity of cisplatin in
germ-cell tumor survivors. Ann Oncol. 28:2670–2679. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Seng S, Liu Z, Chiu SK, Proverbs-Singh T,
Sonpavde G, Choueiri TK, Tsao CK, Yu M, Hahn NM, Oh WK and Galsky
MD: Risk of venous thromboembolism in patients with cancer treated
with Cisplatin: A systematic review and meta-analysis. J Clin
Oncol. 30:4416–4426. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Dwary AD, Master S, Patel A, Cole C,
Mansour R, Mills G, Koshy N, Peddi P, Burton G, Hammoud D and
Beedupalli K: Excellent response to chemotherapy post
immunotherapy. Oncotarget. 8:91795–91802. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Alsuwaigh R, Lee J, Chan G, Chee CE and
Choo SP: Response to targeted therapy or chemotherapy following
immunotherapy in patients with gastrointestinal cancers-a case
series. J Immunother Cancer. 27:1622019. View Article : Google Scholar
|
|
32
|
Ohtsukasa S, Okabe S, Yamashita H, Iwai T
and Sugihara K: Increased expression of CEA and MHC class I in
colorectal cancer cell lines exposed to chemotherapy drugs. J
Cancer Res Clin Oncol. 129:719–726. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wan S, Pestka S, Jubin RG, Lyu YL, Tsai YC
and Liu LF: Chemotherapeutics and radiation stimulate MHC class I
expression through elevated interferon-beta signaling in breast
cancer cells. PLoS One. 7:e325422012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Suzuki E, Kapoor V, Jassar AS, Kaiser LR
and Albelda SM: Gemcitabine selectively eliminates splenic
Gr-1+/CD11b+ myeloid suppressor cells in tumor-bearing animals and
enhances antitumor immune activity. Clin Cancer Res. 11:6713–6721.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Ghiringhelli F, Larmonier N, Schmitt E,
Parcellier A, Cathelin D, Garrido C, Chauffert B, Solary E,
Bonnotte B and Martin F: CD4+CD25+ regulatory T cells suppress
tumor immunity but are sensitive to cyclophosphamide which allows
immunotherapy of established tumors to be curative. Eur J Immunol.
34:336–344. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Marchioni M, Cindolo L, Autorino R,
Primiceri G, Arcaniolo D, De Sio M and Schips L: High
Neutrophil-to-lymphocyte ratio as prognostic factor in patients
affected by upper tract urothelial cancer: A systematic review and
Meta-analysis. Clin Genitourin Cancer. 15:343–349.e1. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Li X, Ma X, Tang L, Wang B, Chen L, Zhang
F and Zhang X: Prognostic value of neutrophil-to-lymphocyte ratio
in urothelial carcinoma of the upper urinary tract and bladder: A
systematic review and meta-analysis. Oncotarget. 8:62681–62692.
2016.PubMed/NCBI
|
|
38
|
Wu S, Zhao X, Wang Y, Zhong Z, Zhang L,
Cao J, Ai K and Xu R: Pretreatment Neutrophil-Lymphocyte ratio as a
predictor in bladder cancer and metastatic or unresectable
urothelial carcinoma patients: A pooled analysis of comparative
studies. Cell Physiol Biochem. 46:1352–1364. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Faria SS, Fernandes PC Jr, Silva MJ, Lima
VC, Fontes W, Freitas-Junior R, Eterovic AK and Forget P: The
neutrophil-to-lymphocyte ratio: A narrative review.
Ecancermedicalscience. 10:7022016.PubMed/NCBI
|
|
40
|
Sacdalan DB, Lucero JA and Sacdalan DL:
Prognostic utility of baseline neutrophil-to-lymphocyte ratio in
patients receiving immune checkpoint inhibitors: A review and
meta-analysis. Onco Targets Ther. 11:955–965. 2018. View Article : Google Scholar : PubMed/NCBI
|