Introduction
Colon cancer has the second highest morbidity and
mortality rates in the United States with 102,000 new cases and
51,000 deaths (1,2), accounting for >1,000,000 newly
diagnosed cases and up to 500,000 cancer-associated mortality cases
estimated per year between 2016 and 2019 worldwide (3). Patients with early stage disease may
present with no specific symptoms or clinical manifestations;
however, once symptoms occur, the disease may have already
progressed to an advanced stage (4).
This delays the opportunity to provide the patient with curative
surgery, and thereby increases the risk of mortality (5). Early detection methods for colon cancer
include the fecal occult blood test, the analysis of certain
gastrointestinal tumor markers, such as CEA and CA19-9, in the
serum and the colonoscopy (6–11). Fiber
colonoscopy is the best screening method for the early diagnosis of
colon cancer, compared with the fecal occult blood test and
analysis of serum biomarkers, which are not very reliable due to
their low sensitivity and specificity; however, fiber colonoscopy
is an invasive and expensive procedure (9). Tumor metastasis, including lymph node
metastasis, is the first cause of mortality in these patients
(6–11). Further identification and evaluation
of serum biomarkers could therefore help clinicians to detect colon
cancer early or predict the prognosis and treatment responses in
order to successfully treat patients.
Currently, there are numerous approaches to detect
biological markers or metabolites in human fluid samples, including
serum, sputum, bile and aqueous humor for tumor diagnosis. For
example, the detection of gene mutations in serum samples could
specifically and sensitively differentiate the disease stages
(12–17), whereas analysis of serum metabolites
could help diagnose colon cancer early or predict disease
progression (18–22). Detection and evaluation of serum
metabolomics have been used to better understand the pathogenesis
and progression of colon cancer (23). Further studies could identify novel
biomarkers that may be used as diagnostic tools in patients with
colon cancer. To date, the popularity of modern chromatography,
mass spectrometry and other detection techniques, including nuclear
magnetic resonance (NMR), could help the discovery of numerous
biological metabolites, such as xanthine, hypoxanthine, succinate,
N2, N2-dimethylguanosine, adenine, citraconic acid,
1-methylguanosine and d-mannose, some of which were proven to be
specific and sensitive biomarkers in cancer research (18–22).
Previous studies analyzing serum metabolomics in patients with
colorectal cancer or colorectal polyps compared with healthy
subjects by using liquid chromatography-mass spectrometry (LC-MS),
NMR or mass spectrometry (MS) reported different metabolites,
including xanthine, hypoxanthine and d-mannose, as potential
biomarkers (18,19). However, to the best of our knowledge,
only a few studies compared the serum metabolomics of patients with
stage Tumor (T) 3 colon cancer with or without lymph node
metastasis (24). In the present
study, patients with T3 colon cancer were selected to assess their
serum metabolites in order to analyze patients with colon cancer at
an earlier disease stage, detect lymph node metastasis and predict
their prognosis.
Materials and methods
Study population
In the present study, 104 patients with stage T3
colon cancer treated at The Department of Gastric, Colonic, Rectal
and Anal Surgery, The First Hospital of Jilin University
(Changchun, China) between August 2008 and August 2012 were
selected. There were 58 males and 46 females with an age range of
49–74 years. Patients underwent tumor resection and were
histologically diagnosed with colon cancer according to the
American Joint Committee on Cancer Staging Manual (25). Among them, 52 patients were diagnosed
with T3 Node (N)0 Metastasis (M)0 and the remaining 52 patients
were diagnosed with T3NxM0 (N=1-3). Inclusion criteria were as
follows: The tumor was initially diagnosed as colon cancer by
endoscopy; and no history of tuberculosis, hepatitis, diabetes and
mental illness. The exclusion criteria were as follows: Patients
with abnormal data from routine blood, urine, liver and kidney
function analysis for whom other diseases could not be ruled out;
patients with distant tumor metastasis or other tumors detected by
CT or MRI imaging; and female patients who were pregnant,
breast-feeding, or for whom the possibility of pregnancy could not
be ruled out. These exclusion criteria resulted in 104 patients who
were suitable for the present study. The study protocol was
approved by the Ethics Committee of The First Hospital of Jilin
University (Changchun, China) and all participants provided written
informed consent prior to enrolment. The present study was in
strict accordance with the 1964 Helsinki Declaration and its later
amendments.
Blood sample processing and liquid
chromatography-mass spectrometry
Fasting blood samples (1.5 ml) were collected prior
to surgery, then centrifuged at 1,294 × g and the supernatant was
removed, leaving the serum which was stored at −80°C. Subsequently,
150 µl of serum from each participant was thawed at room
temperature and added to 500 µl acetonitrile (Merck KGaA) to
denature the sample at room temperature. Samples were centrifuged
at 10,878 × g for 5 min at −4°C, and supernatants were collected
and added to the Eclipse Plus C18 column (2.l × l50.0 mm, 3.5 µm;
Agilent Technologies, Inc.). High performance liquid chromatography
was performed with the Agilent 1200 system combined with a 6520
accurate electrospray ionization/quadrupole-time-of-flight mass
system (Agilent Technologies, Inc.). The gradient program consisted
of mobile phase A (0.1% formic acid solution) and mobile phase B
(99.9% acetonitrile) with a 0.8 ml/min flow rate, 45°C column
temperature and 20 µl injection volume. The gradient program was
started from 25% A for 0.0–1.5 min, linearly increased from 25 to
90% A for 1.5–7.0 min, kept at 90% A for 7.0–9.9 min, linearly
decreased from 90 to 25% A for 9.9–10.0 min, and equilibrated for
25% A for 10.0–11.0 min. The mass spectrometer was set to a
desolvation temperature of 350°C, source temperature of 100°C,
capillary voltage of 3.2 kv, mass range between 50 and 1,000, scan
time of 1 sec, inter-scan delay of 0.02 sec, desolvation gas
(nitrogen) flow rate of 650 l/h, cone voltage of 35 volts, and cone
gas (nitrogen) flow rate of 50 l/h. The LC-MS data were
subsequently analyzed.
Data processing and statistical
analysis
The raw mass spectra data collected with the
software analyst TF 1.5.1 (AB Sciex) were imported into the Marker
View 1.2 (AB Sciex) for processing and included the retention time,
peak area and m/z ratio. The Human Metabolome Database (HMDB;
www.hmdb.ca) was used to structurally confirm the
serum metabolites by comparing the m/z ratio and ion mode between
the results from this study and the HMDB. Principal component
analysis (PCA) was then applied to the data to distinguish the
similarities or differences in the scatterplots of patients with
different lymph node development stages. The potential biological
variables with statistically significant differences for patients
with T3 colon cancer with different lymph node development stages
were selected using the two-sample t-test. The data are expressed
as the mean ± standard deviation and statistically analyzed using
the two-sample t-test. Furthermore, hierarchical clustering
analysis was conducted using BRB-Array Tools version 3.6 software
(developed by Dr Richard Simo & BRB-Array Tools Development
Team) to distinguish patients with stage T3 colon cancer with and
without lymph node metastasis. The global median subtraction method
(26,27) was used to normalize the intensity of
the background interference. In addition, the clinicopathological
characteristics of the patients were collected, including sex, age,
tumor size, presence of invasion to the blood or lymph vessels, p53
expression, Ki-67 serum level, history of alcohol consumption,
tobacco smoking and family tumor history, analyzed using a
χ2 test or Fisher's exact test. Then independent factors
were used to calculate the risk scores for lymph node metastasis as
follows: Risk score = probability × 100; probability = eZ/(eZ +1),
where e indicates the natural logarithm and Z denotes the value of
the logistic regression; Z = B0 + B1X1 + B2X2 + B3X3 + … + BpXp,
where B0 denotes the regression coefficient of the constant for the
logistic regression, X1 … where Xp denotes the individual variable
in the logistic regression, and B1 … where Bp denote the
corresponding regression coefficients and P denotes the number of
vairables (26,27). The survival data were also collected
and analyzed using the Kaplan-Meier curves, the log rank test,
multivariate Cox regression and receiver operating characteristic
(ROC) curves. All statistical analyses were conducted using SPSS
22.0 (IBM Corp.) and P<0.05 was considered to indicate a
statistically significant difference.
Results
Differential profiling of serum
metabolites between patients with T3N0M0 and T3N1-3M0 colon
cancer
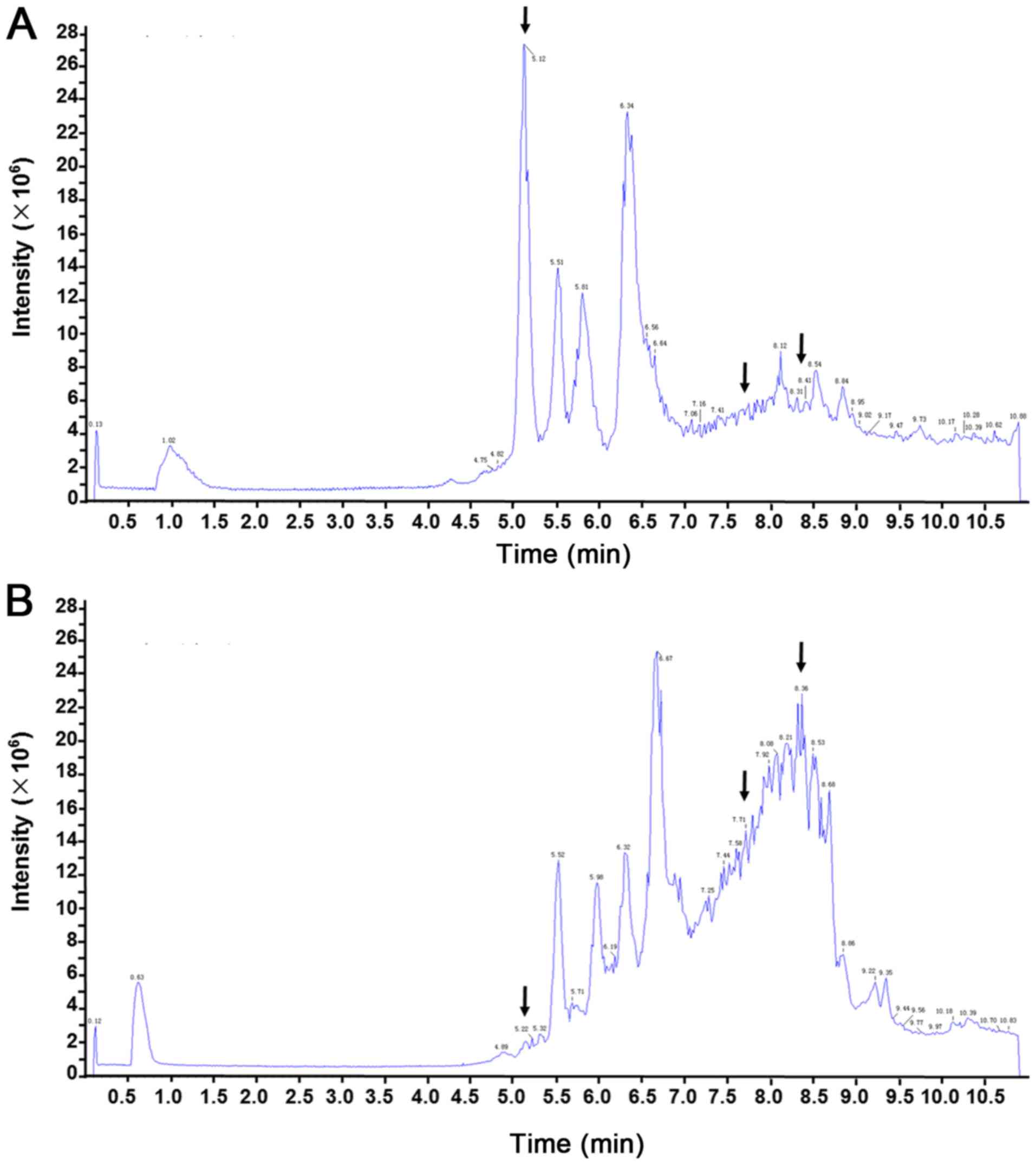
In the present study, LC-MS was performed to assess
the differential serum metabolite profile between blood samples
from patients with T3N0M0 and T3N1-3M0 colon cancer. Differences in
the total ion current spectra in the serum samples from patients
with stage T3 colon cancer and different lymph node development
stages were observed in the 11-min retention time, suggesting that
lymph node metastasis may induce important metabolic changes in
these patients (Fig. 1). A total of
227 metabolites were detected in the serum of patients with T3
colon cancer at different lymph node developmental stages and the
differences between the two groups were statistically significant
(data not shown; P<0.05). These 227 metabolites were
structurally confirmed by comparison with the data acquired from
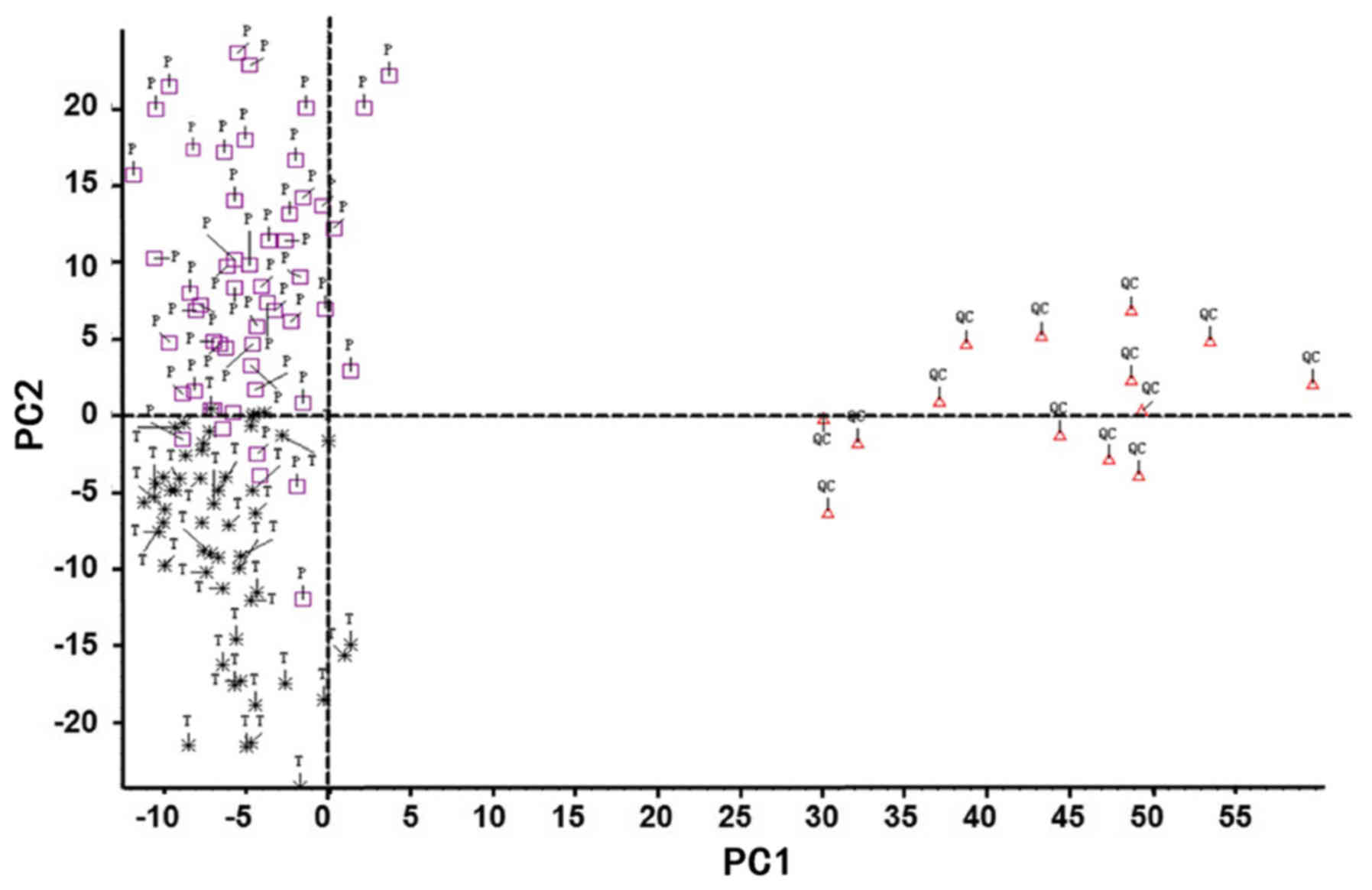
HMDB. PCA, which is a statistical method used to cluster the
detected serum metabolites into a smaller number of principal
components (PCs), was performed to determine specific metabolic
differences among patients. The outliers or discretization trends
in samples from patients were distinguished. Subsequently, almost
all samples were separated into 2 groups in the PCA plots,
suggesting that these serum metabolites may allow the
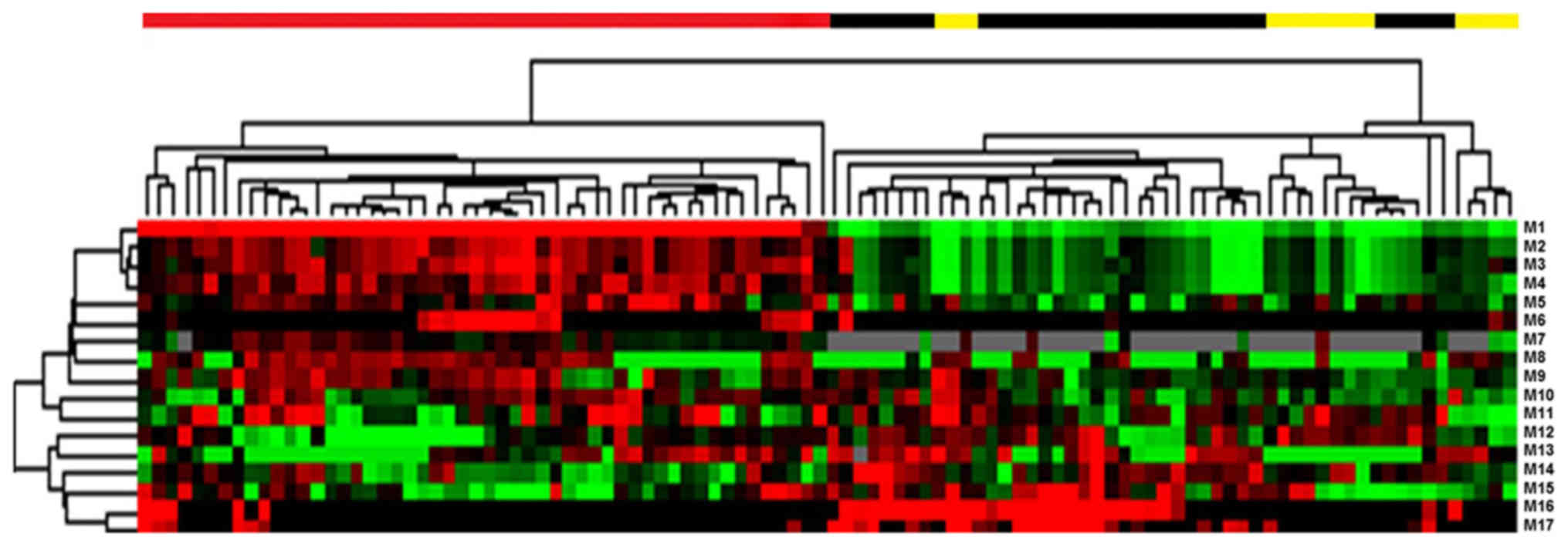
classification of patients according to their stage (Fig. 2). Furthermore, data demonstrated that
a total of 17 serum metabolites could potentially distinguish the
patients with lymph node metastasis from patients without following
two-sample t-test analysis (Fig. 3;
Table I).
 | Table I.Differential serum metabolites from
patients with stage T3 colon cancer and different lymph node
status. |
Table I.
Differential serum metabolites from
patients with stage T3 colon cancer and different lymph node
status.
| No. | Name | Molecular weight,
g/mol | Rain time, min | Response, T3Nx | Response, T3N0 | P-value |
|---|
| M1 | Tyramine | 137.179 | 10.56 | NA | 193.34±415.58 |
8.90×10−4 |
| M2 | Abscisic acid | 264.3169 |
9.81 | 1.51±6.79 | 18.2±38.94 |
2.40×10−3 |
| M3 | 3-hydroxynonanoyl
carnitine | 317.421 |
9.93 | 3.88±14.55 | 21.13±58.78 |
1.90×10−3 |
| M4 | Ethanolamine
Oleate | 61.0831 |
7.29 | 5.63±12.37 | 24.99±30.27 |
3.14×10−5 |
| M5 | Coutaric acid | 349.4247 |
9.93 | 0.65±2.77 | 13.91±33.18 |
4.20×10−3 |
| M6 | Sorgoleone | 358.4712 |
9.87 | 16.32±28.83 | 1.71±5.65 |
4.00×10−4 |
| M7 | Aldosterone | 360.444 |
7.32 | 56.22±66.11 | 5.35±16.2 |
2.75×10−7 |
| M8 | Calcitroic
acid | 374.5137 |
9.88 | 6.49±17.48 | 44.19±80.73 |
1.10×10−3 |
| M9 | Lithocholic
acid | 376.5726 |
9.89 | 3.92±14.50 | 35.54±68.93 |
1.32×10−3 |
| M10 | Cinncassiol C3 | 382.448 |
7.10 | 114.23±125.3 | 31.66±65.46 |
3.92×10−5 |
| M11 | Treprostinil | 390.5131 |
9.44 | 0.89±4.93 | 33.61±75.71 |
2.00×10−3 |
| M12 | Flavoxate | 391.4596 |
5.24 | 2.63±6.13 | 14.33±34.15 |
1.40×10−2 |
| M13 |
Hydroxy-5-(3′,5′-dihydroxyphenyl)-valeric
acid-O-glucuronide | 402.35 |
5.68 | 399.23±697.43 | 79.95±259.43 |
2.10×10−3 |
| M14 | Phenobarbital
O-glucuronide | 232.2353 |
5.69 | 148.41±291.76 | 17.46±68.4 |
1.70×10−3 |
| M15 | Pinostrobin
5-glucoside | 432.4206 |
5.85 | 43.13±100.18 | 5.8±16.01 |
7.90×10−3 |
| M16 | Lithocholic acid
glycine conjugate | 433.6239 |
9.91 | 2.66±9.79 | 24.6±49.85 |
1.90×10−3 |
| M17 |
Glucosylsphingosine | 461.6325 |
6.74 | 40.9±59.64 | 95.84±77.24 |
7.07×10−5 |
Association between differential serum
metabolites and lymph node metastasis
A total of 10 different metabolites from 17
metabolites were selected using the support vector machine method.
These data included metabolites, age, sex, tumor size, vascular
infiltration, P53, ki-67, history of alcohol consumption, smoking
history and family tumor history. These were then analyzed by
single-factor logistic regression (Table II). Five independent risk factors,
including presence of abscisic acid, calcitroic acid and
glucosylsphingosine in the serum, age and sex, were associated with
different status of lymph node metastasis in colon cancer were
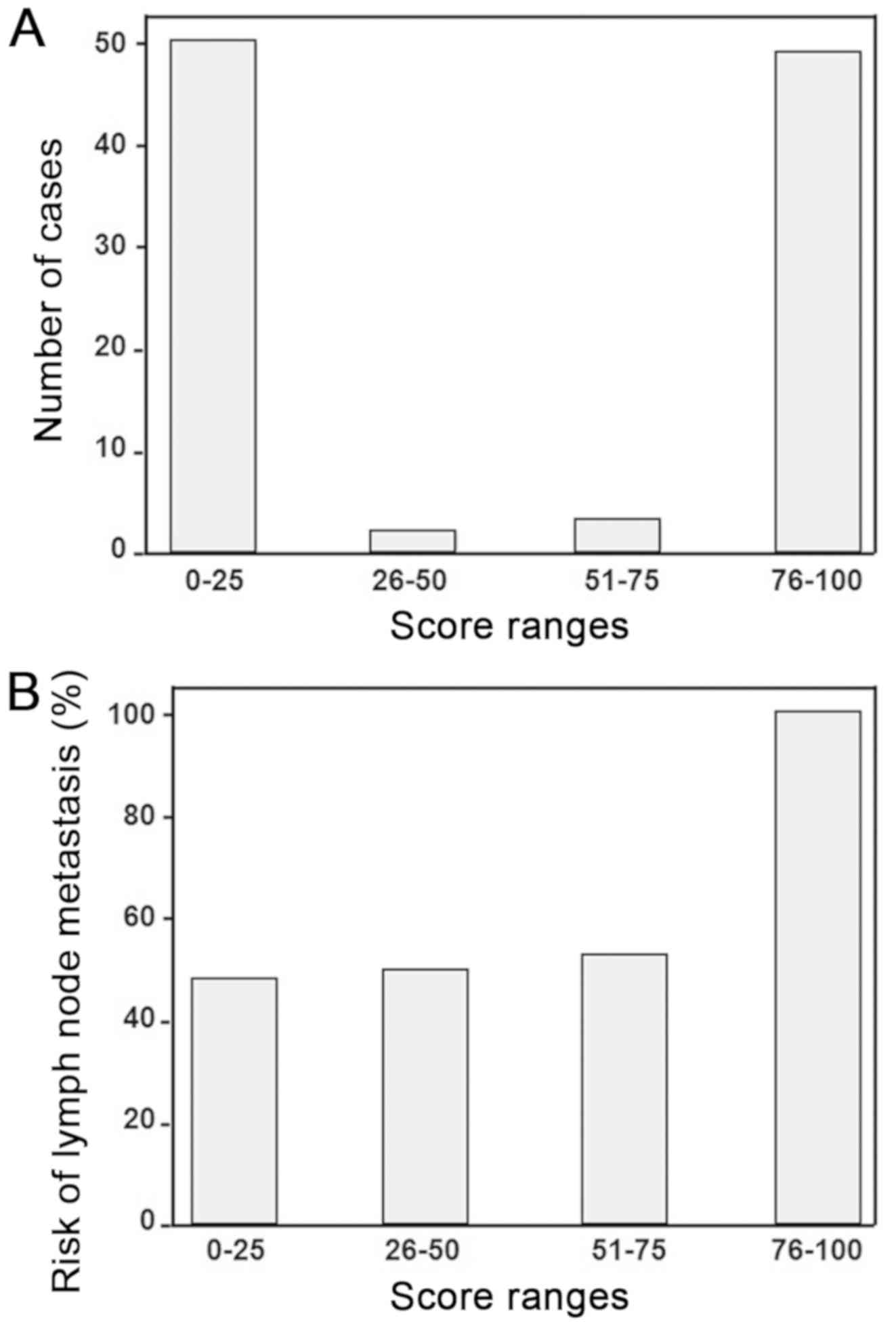
observed. Following multivariate logistic regression analysis, five
independent risk factors, including presence of abscisic acid,
calcitroic acid and glucosylsphingosine in the serum, age and sex
were identified as associated with lymph node metastasis
(P<0.05; Table III). These five
independent factors were used to calculate the risk scores for
lymph node metastasis. The results demonstrated that Z values =
−6.403 - 0.44 (abscisic acid) + 0.018 (calcitroic acid) - 0.012
(glucosylsphingosine) + 0.090 (age) −1.141 (sex). Each patient in
the present study was assigned a risk score using this formula
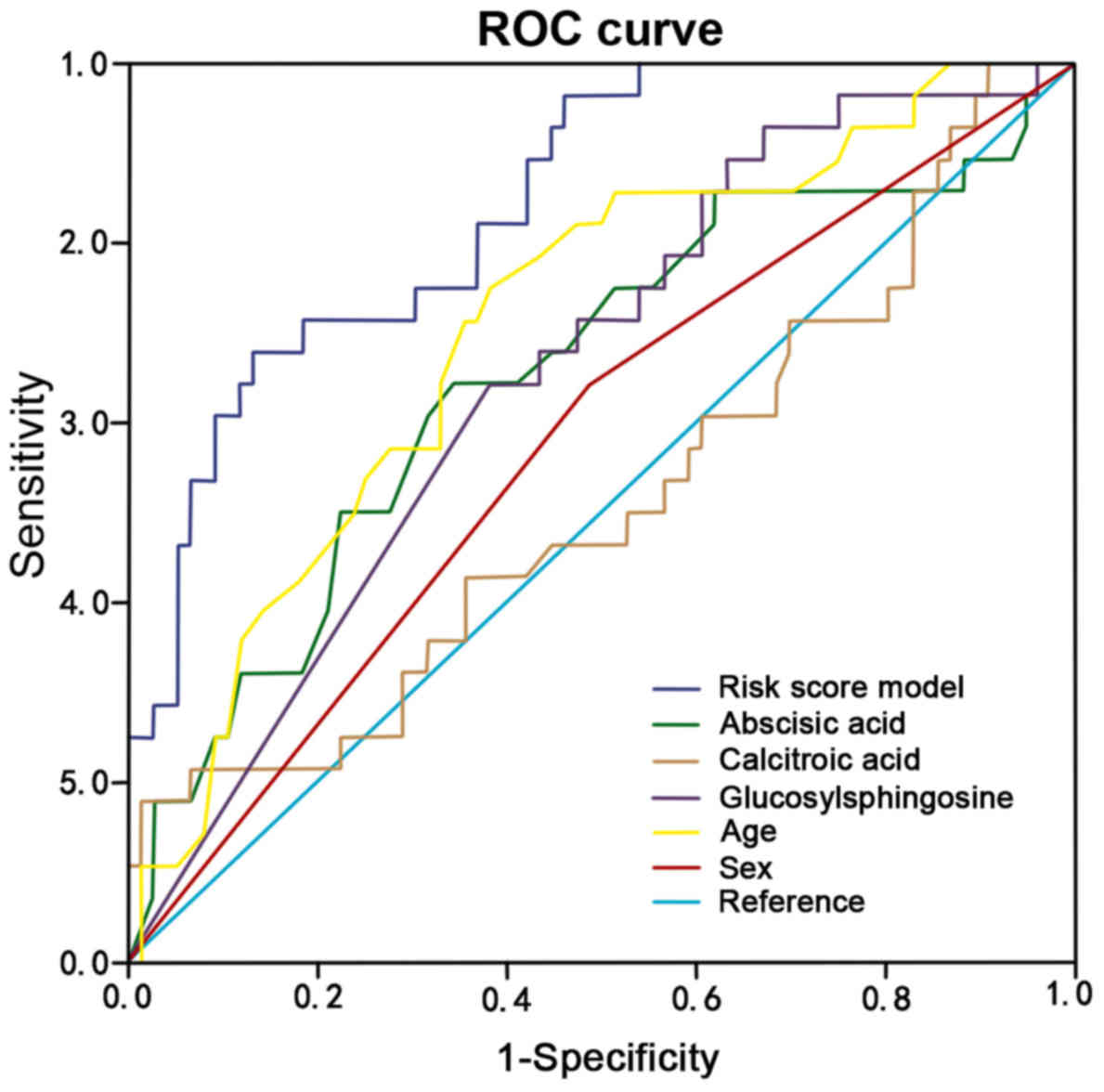
(Fig. 4). In addition, the results
from ROC curves confirmed that the presence of abscisic acid,
calcitroic acid and glucosylsphingosine in the serum, age and sex,
could be considered as factors for lymph node metastasis in these
patients (AUC of abscisic acid, calcitroic acid,
glucosylsphingosine, age and sex were 0.844, 0.655, 0.517, 0.655,
0.708 and 0.578, respectively; Fig.
5).
| Table II.Univariate logistic regression
analysis of differential serum metabolites and clinical features
for association with lymph node metastasis. |
Table II.
Univariate logistic regression
analysis of differential serum metabolites and clinical features
for association with lymph node metastasis.
|
|
|
|
|
|
| 95% CI |
|---|
|
|
|
|
|
|
|
|
|---|
| Variables | B | SE | Wald |
P-valuea | OR | Lower | Upper |
|---|
| Abscisic acid | −0.044 | 0.017 | 6.891 | 0.009 | 0.957 | 0.92 | 0.98 |
| Calcitroic
acid |
0.018 | 0.006 | 8.569 | 0.003 | 1.018 | 1.00 | 1.03 |
|
Glucosylsphingosine | −0.012 | 0.004 | 6.778 | 0.009 | 0.988 | 0.98 | 0.99 |
| Ethanolamine
Oleate | −0.019 | 0.009 | 3.909 | 0.048 | 0.982 | 0.964 | 1.000 |
| Coutaric acid | −0.008 | 0.008 | 0.838 | 0.360 | 0.992 | 0.977 | 1.009 |
| Aldosterone |
0.005 | 0.002 | 5.497 | 0.019 | 1.005 | 1.001 | 1.008 |
| Lithocholic
acid |
0.001 | 0.002 | 0.357 | 0.550 | 1.001 | 0.997 | 1.006 |
| Cinncassiol C3 |
0.003 | 0.002 | 3.565 | 0.059 | 1.003 | 1.000 | 1.007 |
| Treprostinil |
0.001 | 0.002 | 0.083 | 0.773 | 1.001 | 0.996 | 1.005 |
| Flavoxate |
0.002 | 0.004 | 0.254 | 0.614 | 1.002 | 0.994 | 1.010 |
| Age |
0.072 | 0.024 | 9.371 | 0.002 | 1.075 | 1.026 | 1.126 |
| Sex | −1.141 | 0.600 | 3.829 | 0.050 | 0.320 | 0.101 | 1.007 |
| Tumor size | −0.113 | 0.101 | 1.256 | 0.262 | 0.893 | 0.732 | 1.089 |
| P53 |
0.000 | 0.006 | 0.002 | 0.964 | 1.000 | 0.988 | 1.011 |
| Ki-67 |
0.007 | 0.017 | 0.163 | 0.686 | 1.007 | 0.974 | 1.041 |
| Vascular
infiltration |
0.323 | 0.457 | 0.499 | 0.480 | 1.381 | 0.564 | 3.385 |
| Alcohol
consumption | −0.214 | 0.620 | 0.119 | 0.731 | 0.808 | 0.240 | 2.723 |
| Smoking
history | −0.054 | 0.473 | 0.013 | 0.909 | 0.947 | 0.375 | 2.394 |
| Family tumor
history | −0.643 | 1.119 | 0.330 | 0.566 | 0.526 | 0.059 | 4.710 |
| Table III.Multivariate Cox regression analysis
of differential serum metabolites and clinical features for
association with lymph node metastasis. |
Table III.
Multivariate Cox regression analysis
of differential serum metabolites and clinical features for
association with lymph node metastasis.
|
|
|
|
|
|
| 95% CI |
|---|
|
|
|
|
|
|
|
|
|---|
| Variables | B | SE | Wald |
P-valuea | OR | Lower | Upper |
|---|
| Abscisic acid | −0.044 | 0.017 |
6.891 | 0.009 | 0.957 | 0.92 | 0.98 |
| Calcitroic
acid |
0.018 | 0.006 |
8.569 | 0.003 | 1.018 | 1.00 | 1.03 |
|
Glucosylsphingosine | −0.012 | 0.004 |
6.778 | 0.009 | 0.988 | 0.98 | 0.99 |
| Age |
0.090 | 0.028 | 10.444 | 0.001 | 1.094 | 1.03 | 1.15 |
| Sex | −1.141 | 0.586 |
3.793 | 0.051 | 0.320 | 0.10 | 1.00 |
Association between differential serum
metabolites and patient survival
The association between differential serum
metabolites and patient survival was determined. The results
demonstrated that the three serum metabolites abscisic acid,
calcitroic acid and glucosylsphingosine were independent risk
predictors for patient survival (Fig.
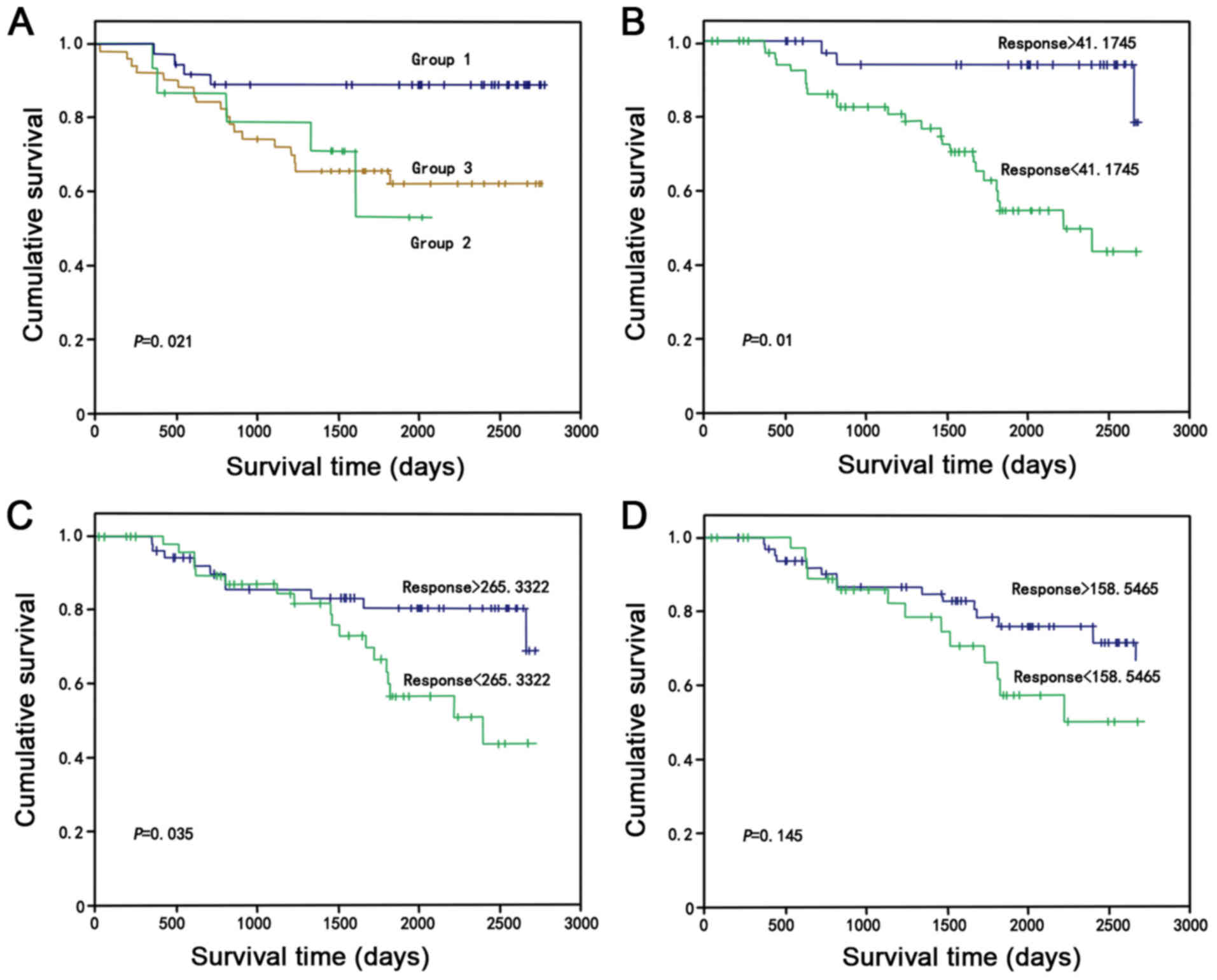
6; P<0.05). The hierarchical clustering analysis data are
presented in Fig. 6. The results
from the Kaplan-Meier curves demonstrated that survival was
significantly improved for patients with high levels of these three
metabolites compared with patients with medium and low levels
(P=0.021; Fig. 7A). The results were
also consistent when only one serum metabolite was selected
(Fig. 7B, abscisic acid, P=0.01;
Fig. 7C, calcitroic acid, P=0.035;
Fig. 7D, glucosylsphingosine,
P=0.145), and abscisic acid, calcitroic acid and
glucosylsphingosine may be considered as potential prognostic
markers for all patients with colon cancer (χ2=7.725;
P=0.021).
Discussion
The incidence of colon cancer has increased each
year over the last decades, and this disease, which markedly alters
the quality of life of patients, is associated with a high
mortality rate (1,2). Patients with advanced stages of colon
cancer cannot receive surgery and are also resistant to
chemoradiation therapy; however, recent targeting or immune therapy
may serve to control the progression of colon cancer in certain
patients (6–11). The present study therefore aimed to
establish the profile of serum metabolites of patients with colon
cancer, in order to identify biomarkers that may be used in the
early detection of lymph node metastasis in these patients. A total
of 227 different metabolites were identified in the serum of
patients with stage T3 colon cancer with or without lymph node
metastasis, of which, 17 were able to distinguish patients with
lymph node metastasis from those without. Five factors, including
the presence of abscisic acid, calcitroic acid and
glucosylsphingosine in the serum, age and sex were independent
predictors for lymph node metastasis, and the three metabolites
abscisic acid, calcitroic acid and glucosylsphingosine were
independent predictors for the survival of patients. Increased
serum levels of abscisic acid, calcitroic-acid and
glucosylsphingosine may therefore be considered as potential
biomarkers to predict lymph node metastasis and survival in
patients with colon cancer. The results from the present study
provided crucial information regarding the use of serum metabolites
as biomarkers for patients with colon cancer; however, further
investigation is required to validate the present data before
clinically applying this method.
Previous studies have identified different serum
metabolites biomarkers of colon cancer or predictive markers for
colon cancer prognosis (18–22,28). For
example, a previous study demonstrated that the Fourier transform
ion cyclotron resonance mass spectrometry can determine serum
metabolites for the early detection and screening of colorectal
cancer (18). Furthermore, a recent
study identified 404 serum metabolites, of which 50 were
differentially represented between patients with colorectal cancer
or colorectal adenoma polyps and healthy subjects (19). Another study used NMR and LC-MS
spectra for the determination of serum metabolites, in order to
distinguish patients with normal colorectum from those with
colorectal adenoma polyps or colorectal cancer (20). A previous study reported that five
metabolites, including succinate, N2,N2-dimethylguanosine, adenine,
citraconic acid and 1-methylguanosine, can be used to detect
colorectal cancer with a sensitivity of 0.83, specificity of 0.94
and area under the receiver operator characteristic curve (AUROC)
of 0.91. Conversely, the values of sensitivity, specificity and
AUROC for carcinoembryonic antigen as a biomarker of colorectal
cancer are 0.75, 0.76 and 0.80, respectively (21,22).
Metabolomics research is feasible and has great potential in the
diagnosis of colon cancer, for example a previous study screened a
group of urinary metabolites as biomarkers for the early detection
of colorectal cancer (18–22,28). The
group compared the expression levels of metabolite markers of
patients with CRC, including citrate, hippurate, p-cresol,
2-aminobutyrate, myristate, putrescine and kynurenate, with healthy
individuals. However, all these studies used a small number of
patients (18–22). The present study included a unique
cohort of patients with stage T3 colon cancer with and without
lymph node metastasis (there were no patients with T3NxM0 colon
cancer included). In this regard, the present data are novel and
provide useful information. Similarly, a previous study assessed
the use of serum metabolites for colorectal cancer staging;
however, this study contained only 16 cases (29). A previous study involving 14 patients
with stages I–V colorectal cancer identified 139 known metabolites,
of which 16 can predict colorectal cancer staging (24). However, the previous and present
studies identified very few overlapped metabolites, which may be
due to the different populations, the diet and lifestyle of
patients, and the methodologies used. The definitive establishment
of serum metabolites as biomarkers in colon cancer staging and
prognosis is therefore challenging. In addition, a previous study
reported that ultra-performance liquid chromatography and
quadrupole time-of-fight mass spectrometry with positive
electrospray ionization analysis can identify 18 biomarkers with
the potential to diagnose ovarian cancer. The metabolites were
potential biomarkers to diagnose ovarian cancer, of which 12 were
confirmed in the validation cohort of patients (30).
Analysis of the metabolic profile in patients with
colon cancer can be used to investigate the underlying metabolic
mechanisms of colon cancer, help clinicians better understand the
role of different metabolites in carcinogenesis and the progression
of colon cancer, and discover candidate biomarkers for the early
detection of tumors or metastasis and of treatment responses
(31–36). In the present study, 17 serum
metabolites were found to be significantly different between
patients with colon cancer and lymph node metastasis and patients
without. The analysis of the clinicopathological characteristics of
these patients, including sex, age, p53 expression, Ki-67 serum
level, tumor vessel infiltration, alcohol consumption, smoking
history and family history of cancer, demonstrated that sex and age
were associated with colon cancer lymph node metastasis. However,
these two factors failed to independently predict patient survival,
and further investigation is required in order to confirm these
findings.
The metabolites identified in the present study
included vitamin D metabolic end product calcitroic acid, further
confirming the protective role of vitamin D in colon cancer
(37,38). Although the underlying mechanism of
vitamin D in the prevention of colon cancer remains unclear, some
possible mechanisms include inhibition of cell proliferation and
stimulation of cell differentiation and apoptosis by vitamin D,
which can subsequently inhibit colon carcinogenesis (37,38). A
previous study reported that vitamin D and its derivatives can
induce the expression of bone morphogenetic protein (BMP) and
activate the BMP-Smad signaling pathway (39). The BMP-Smad signaling pathway is
involved in the pathway for enzyme-coupled receptor signal
transduction, and BMP is one β-tumor necrosis factor (38,40) that
regulates cell proliferation, differentiation and apoptosis.
Furthermore, previous in vitro experiments demonstrated that
vitamin D and its metabolites or analogs induce BMP overexpression
and activates BMP-Smad signaling pathway to suppress the
development of colon cancer (41,42).
The present study presented some limitations. First,
the cohort of patients lacked those with early stage colon cancer,
distant tumor metastases and the serum was not compared with the
postoperative serum. Secondly, the use of Matrix Assisted Laser
Desorption Ionisation-Time of Flight (TOF)/TOF-MS may be more
appropriate to precisely analyse the two-dimensional difference gel
electrophoresis dissected protein spots; however, since this
material was not available at the The First Hospital of Jilin
University, the present study used LC-MS to analyze the serum
samples. Thirdly, some in vitro studies are required to
further elucidate the pathophysiology of colon cancer.
In conclusion, LC-MS possesses a high potential to
analyze clinical samples and investigate the changes in serum
metabolites of patients. The present study identified three
metabolites, including abscisic acid, calcitroic acid and
glucosylsphingosine, as independent risk factors for lymph node
metastasis and prognosis in patients with colon cancer. Further
investigation using a larger number of sample from numerous
institutions is required to validate these finding.
Acknowledgements
The authors would like to thank Dr Jingkai Gu from
the Department of Life Sciences, Jilin University (Changchun,
China) for his assistance with experiments.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JS, DW and WL conceived and designed the
experiments. YZ, YD and ZS performed the experiments. YZ and ZS
analyzed the data. SL collected raw data. YZ and YD wrote the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
The First Hospital of Jilin University (Changchun, China) and all
participants provided written informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Qiu Y, Cai G, Su M, Chen T, Zheng X, Xu Y,
Ni Y, Zhao A, Xu LX, Cai S, et al: Serum metabolite profiling of
human colorectal cancer using GC-TOFMS and UPLC-QTOFMS. J Proteome
Res. 8:4844–4850. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Miller KD, Nogueira L, Mariotto AB,
Rowland JH, Yabroff KR, Alfano CM, Jemal A, Kramer JL and Siegel
RL: Cancer treatment and survivorship statistics, 2019. CA Cancer J
Clin. 69:363–385. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang J, Yan F, Zhao Q, Zhan F, Wang R,
Wang L, Zhang Y and Huang X: Circulating exosomal miR-125a-3p as a
novel biomarker for early-stage colon cancer. Sci Rep. 7:41502017.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jiménez B, Mirnezami R, Kinross J, Cloarec
O, Keun HC, Holmes E, Goldin RD, Ziprin P, Darzi A and Nicholson
JK: 1H HR-MAS NMR spectroscopy of tumor-induced local metabolic
‘field-effects’ enables colorectal cancer staging and
prognostication. J Proteome Res. 12:959–968. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kotronoulas G, Papadopoulou C,
Burns-Cunningham K, Simpson M and Maguire R: A systematic review of
the supportive care needs of people living with and beyond cancer
of the colon and/or rectum. Eur J Oncol Nurs. 29:60–70. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pignone M and Levin B: Recent developments
in colorectal cancer screening and prevention. Am Fam Physician.
66:297–302. 2002.PubMed/NCBI
|
|
8
|
Kronborg O: Colon polyps and cancer.
Endoscopy. 36:3–7. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pellino G, Simillis C, Kontovounisios C,
Baird DL, Nikolaou S, Warren O, Tekkis PP and Rasheed S: Colorectal
cancer diagnosed during pregnancy: Systematic review and treatment
pathways. Eur J Gastroenterol Hepatol. 29:743–753. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Seeber A and Gastl G: Targeted Therapy of
Colorectal Cancer. Oncol Res Treat. 39:796–802. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pohl M and Schmiegel W: Therapeutic
Strategies in Diseases of the Digestive Tract - 2015 and Beyond
Targeted Therapies in Colon Cancer Today and Tomorrow. Dig Dis.
34:574–579. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Courant F, Antignac JP, Monteau F and Le
Bizec B: Metabolomics as a potential new approach for investigating
human reproductive disorders. J Proteome Res. 12:2914–2920. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Manna SK, Krausz KW, Bonzo JA, Idle JR and
Gonzalez FJ: Metabolomics reveals aging-associated attenuation of
noninvasive radiation biomarkers in mice: Potential role of
polyamine catabolism and incoherent DNA damage-repair. J Proteome
Res. 12:2269–2281. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang X, Yang B, Sun H and Zhang A: Pattern
recognition approaches and computational systems tools for ultra
performance liquid chromatography-mass spectrometry-based
comprehensive metabolomic profiling and pathways analysis of
biological data sets. Anal Chem. 84:428–439. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang A, Sun H, Wang P, Han Y and Wang X:
Modern analytical techniques in metabolomics analysis. Analyst
(Lond). 137:293–300. 2012. View Article : Google Scholar
|
|
16
|
Mondul AM, Moore SC, Weinstein SJ,
Männistö S, Sampson JN and Albanes D: 1-stearoylglycerol is
associated with risk of prostate cancer: Results from serum
metabolomic profiling. Metabolomics. 10:1036–1041. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Aboud OA and Weiss RH: New opportunities
from the cancer metabolome. Clin Chem. 59:138–146. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ritchie SA, Ahiahonu PWK, Jayasinghe D,
Heath D, Liu J, Lu Y, Jin W, Kavianpour A, Yamazaki Y, Khan AM, et
al: Reduced levels of hydroxylated, polyunsaturated ultra
long-chain fatty acids in the serum of colorectal cancer patients:
Implications for early screening and detection. BMC Med. 8:132010.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Long Y, Sanchez-Espiridion B, Lin M, White
L, Mishra L, Raju GS, Kopetz S, Eng C, Hildebrandt MAT, Chang DW,
et al: Global and targeted serum metabolic profiling of colorectal
cancer progression. Cancer. 123:4066–4074. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Deng L, Gu H, Zhu J, Nagana Gowda GA,
Djukovic D, Chiorean EG and Raftery D: Combining NMR and LC/MS
using backward variable elimination: Metabolomics analysis of
colorectal cancer, polyps, and healthy controls. Anal Chem.
88:7975–7983. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhu J, Djukovic D, Deng L, Gu H, Himmati
F, Abu Zaid M, Chiorean EG and Raftery D: Targeted serum metabolite
profiling and sequential metabolite ratio analysis for colorectal
cancer progression monitoring. Anal Bioanal Chem. 407:7857–7863.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhu J, Djukovic D, Deng L, Gu H, Himmati
F, Chiorean EG and Raftery D: Colorectal cancer detection using
targeted serum metabolic profiling. J Proteome Res. 13:4120–4130.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Uchiyama K, Yagi N, Mizushima K,
Higashimura Y, Hirai Y, Okayama T, Yoshida N, Katada K, Kamada K,
Handa O, et al: Serum metabolomics analysis for early detection of
colorectal cancer. J Gastroenterol. 52:677–694. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nishiumi S, Kobayashi T, Kawana S, Unno Y,
Sakai T, Okamoto K, Yamada Y, Sudo K, Yamaji T, Saito Y, et al:
Investigations in the possibility of early detection of colorectal
cancer by gas chromatography/triple-quadrupole mass spectrometry.
Oncotarget. 8:17115–17126. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Singletary SE, Greene FL and Sobin LH:
Classification of isolated tumor cells: Clarification of the 6th
edition of the American Joint Committee on Cancer Staging Manual.
Cancer. 98:2740–2741. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Li W, Ye F, Wang D, Sun X, Tong W, Lian G,
Jiang J, Suo J and Zhang DY: Protein predictive signatures for
lymph node metastasis of gastric cancer. Int J Cancer.
132:1851–1859. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wang D, Ye F, Sun Y, Li W, Liu H, Jiang J,
Zhang Y, Liu C, Tong W, Gao L, et al: Protein signatures for
classification and prognosis of gastric cancer a signaling
pathway-based approach. Am J Pathol. 179:1657–1666. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cheng Y, Xie G, Chen T, Qiu Y, Zou X,
Zheng M, Tan B, Feng B, Dong T, He P, et al: Distinct urinary
metabolic profile of human colorectal cancer. J Proteome Res.
11:1354–1363. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Vahabi F, Sadeghi S, Arjmand M, Mirkhani
F, Hosseini E, Mehrabanfar M, Hajhosseini R, Iravani A, Bayat P and
Zamani Z: Staging of colorectal cancer using serum metabolomics
with 1HNMR Spectroscopy. Iran J Basic Med Sci. 20:835–840.
2017.PubMed/NCBI
|
|
30
|
Yang W, Mu T, Jiang J, Sun Q, Hou X, Sun
Y, Zhong L, Wang C and Sun C: Identification of Potential
Biomarkers and Metabolic Profiling of Serum in Ovarian Cancer
Patients Using UPLC/Q-TOF MS. Cell Physiol Biochem. 51:1134–1148.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ma Y, Zhang P, Wang F, et al: An
integrated proteomics and metabolome approach for defining
oncofetal biomarkers in the CC. Ann Surg. 255:720–730. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Carloni V, Luong TV and Rombouts K:
Hepatic stellate cells and extracellular matrix in hepatocellular
carcinoma: More complicated than ever. Liver Int. 34:834–843. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bertorelle R, Briarava M, Rampazzo E,
Biasini L, Agostini M, Maretto I, Lonardi S, Friso ML, Mescoli C,
Zagonel V, et al: Telomerase is an independent prognostic marker of
overall survival in patients with colorectal cancer. Br J Cancer.
108:278–284. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Koga Y, Yamazaki N, Yamamoto Y, Yamamoto
S, Saito N, Kakugawa Y, Otake Y, Matsumoto M and Matsumura Y: Fecal
miR-106a is a useful marker for colorectal cancer patients with
false-negative results in immunochemical fecal occult blood test.
Cancer Epidemiol Biomarkers Prev. 22:1844–1852. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zheng X, Xie G and Jia W: Metabolomic
profiling in colorectal cancer: Opportunities for personalized
medicine. Per Med. 10:741–755. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wang H, Tso VK, Slupsky CM and Fedorak RN:
Metabolome and detection of CC in humans: A systematic review.
Future Oncol. 6:1395–1406. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Bell SJ: The Effect of Vitamin D3 on
Hepcidin and IL-8 Expression in Monocytes. J Hematol (Brossard).
2:1–7. 2013.
|
|
38
|
Liang CJ, Yen YH, Hung LY, Wang SH, Pu CM,
Chien HF, Tsai JS, Lee CW, Yen FL and Chen YL: Thalidomide inhibits
fibronectin production in TGF-β1-treated normal and keloid
fibroblasts via inhibition of the p38/Smad3 pathway. Biochem
Pharmacol. 85:1594–1602. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hedger MP, Winnall WR, Phillips DJ and de
Kretser DM: The regulation and functions of activin and follistatin
in inflammation and immunity. Vitam Horm. 85:255–297. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Xu Q, Tan Y, Zhang K and Li Y: Crosstalk
between p38 and Smad3 through TGF-β1 in JEG-3 choriocarcinoma
cells. Int J Oncol. 43:1187–1193. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Kikuta J, Kawamura S, Okiji F, Shirazaki
M, Sakai S, Saito H and Ishii M: Sphingosine-1-phosphate-mediated
osteoclast precursor monocyte migration is a critical point of
control in antibone-resorptive action of active vitamin D. Proc
Natl Acad Sci USA. 110:7009–7013. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Yang S and Qiu MX: Progress on the
development of relations of Smad4 protein and tumorigenesis. Pract
J Clin Med. 1:158–160,161. 2015.(In Chinese).
|