Introduction
Esophageal cancer (including squamous cell carcinoma
and adenocarcinoma) is the eighth most frequently diagnosed cancer
globally (1). The incidence of
adenocarcinoma has rapidly increased in the Western world in recent
decades (2,3). In the United States of America, the
incidence increased from 3.6 per million in 1973 to 25.6 per
million in 2006 (4). The substantial
increase in esophageal adenocarcinoma (EAC) is presumably caused by
a higher incidence of known risk factors, including obesity and
gastroesophageal reflux (5). EAC is
thought to arise from Barrett's metaplasia, caused by chronic
gastroesophageal reflux. The accumulation of various mutations,
copy-number variations and chromothripsis causing genetic
instability finally result in carcinogenesis (6–8). Despite
improvements in perioperative treatments, the overall survival (OS)
time of patients with esophageal carcinomas remains low. The
relative 5 year survival rate remains poor, at 21% in both sexes
(20.2 and 22.8% for adenocarcinomas and squamous cell carcinomas,
respectively) (9,10).
Claudins are proteins required for the formation of
tight junctions and paracellular barriers (11–13). At
least 27 different claudins have been discovered in humans so far
(14). Claudins have four
transmembrane domains and a molecular mass ranging between 20 and
27 kDa (14). In 2008, Sahin et
al (15) identified isoform 2 of
claudin 18 (claudin 18.2) as a highly selective marker for
differentiated gastric mucosa epithelial cells. Claudin 18.2
expression was revealed to occur exclusively in normal gastric
tissue and was not detected in any other examined tissue. In
addition, the study demonstrated a significantly higher expression
of claudin 18.2 in gastric adenocarcinomas and their metastases,
including carcinomas of the pancreas, esophagus, ovaries and lungs.
Additionally, a correlation between the histological subtype of
carcinomas and expression of claudin 18.2 was revealed. EACs,
mucinous ovarian carcinomas and ductal adenocarcinomas of the
pancreas were positive for claudin 18.2 expression. By contrast, no
expression was detected in squamous cell carcinomas of the
esophagus, serous ovarian carcinomas and islet cell carcinomas of
the pancreas (15,16). As claudin 18.2 exhibits distinct
expression patterns and is located in the outer cell membrane, it
is an attractive target for targeted therapies (15,16). To
the best of our knowledge, the expression status of claudin 18.2 in
EAC has only been investigated in one previous study, in which
Sahin et al (15)
demonstrated the expression of claudin 18.2 in 17/22 EAC tissues
(78%) using an in-house developed mouse monoclonal antibody.
IMAB362 (claudiximab or zolbetuximab) is a novel
chimeric immunoglobulin G1 antibody, developed by Ganymed
Pharmaceuticals, which is able to specifically bind to claudin 18.2
on the cell surface (16,17). Subsequent to binding to claudin 18.2,
IMAB362 stimulates cellular and soluble immune effectors that
activate antibody- and complement-dependent cytotoxicity, induce
apoptosis and inhibit cell proliferation (16). Additionally, in combination with
chemotherapy, IMAB362 enhances T-cell infiltration and induces the
release of pro-inflammatory cytokines (16). IMAB362 is currently undergoing a
number of phase I and IIb trials, which have revealed that IMAB362
is well-tolerated, exhibits anti-tumor activity and improves the
disease control rate and progression-free survival time when
administered as a monotherapy or in combination with chemotherapy.
The most frequently observed treatment-associated adverse events
include nausea and vomiting (18–21).
The aim of the present study was to detect the
levels of claudin 18.2 expression in a large number of EAC samples,
in addition to investigating its expression in metastases.
Furthermore, these results were associated with clinicopathological
and molecular data.
Materials and methods
Patients and tumor samples
Formalin-fixed and paraffin- embedded primary tumor
tissue microarrays (TMA) obtained from 685 patients with EAC that
underwent primary surgical resection or resection following
neoadjuvant therapy between January 1999 and November 2012 at the
Department of General, Visceral and Cancer Surgery, University of
Cologne (Cologne, Germany) were analyzed in the present study.
Additionally, samples from 287 corresponding regional lymph node
metastases were available. The patients underwent laparotomic or
laparoscopic gastrolysis and right transthoracic en bloc
esophagectomy with two-field lymphadenectomy of the mediastinal and
abdominal lymph nodes. Reconstruction was performed by high
intrathoracic esophagogastrostomy as previously described (22). Patients with advanced esophageal
cancer (cT3, cNx and M0) received preoperative chemoradiotherapy
[according to the ChemoRadiotherapy for Oesophageal Cancer Followed
by Surgery Study protocol (23,24)] or
chemotherapy alone [according to the 5-fluorouracil, leucovorin,
oxaliplatin and docetaxel protocol (24)]. Follow-up data were available for all
patients. Patient characteristics are presented in Table I. Both Union for International Cancer
and pTNM classifications were used for tumor staging (25,26).
Depending on the efficacy of neoadjuvant chemotherapy or
radiochemotherapy, minor responders were defined as exhibiting a
histopathological residual tumor of ≥10% (27).
 | Table I.Univariate analysis of clinical
parameters. Sum of patients do not add to 485 patients due to
missing clinical data or missing tumor spots on the tissue
microarray. |
Table I.
Univariate analysis of clinical
parameters. Sum of patients do not add to 485 patients due to
missing clinical data or missing tumor spots on the tissue
microarray.
|
| Claudin 18.2
expression in esophageal adenocarcinoma |
|---|
|
|
|
|---|
|
| Total | Negative | Positive |
|
|---|
|
|
|
|
|
|
|---|
| Clinical
parameters | n | % | n | % | n | % | P-value |
|---|
| Total number | 485 | 100 | 396 | 81.6 | 89 | 18.4 |
|
| Sex |
|
|
|
|
|
| 0.589 |
|
Female | 54 | 11.1 | 44 | 81.5 | 10 | 18.5 |
|
|
Male | 431 | 88.9 | 352 | 81.7 | 79 | 18.3 |
|
| Age group |
|
|
|
|
|
| 0.448 |
|
<65 | 251 | 51.8 | 204 | 81.4 | 47 | 18.6 |
|
|
>65 | 234 | 48.2 | 193 | 82.3 | 42 | 17.7 |
|
| pT stage |
|
|
|
|
|
| 0.289 |
| 0 | 1 | 0.2 | 1 | 100 | 0 | 0.0 |
|
| 1 | 67 | 13.8 | 51 | 76.1 | 16 | 23.9 |
|
| 2 | 54 | 11.2 | 44 | 81.5 | 10 | 18.5 |
|
| 3 | 344 | 71.1 | 281 | 81.7 | 63 | 18.3 |
|
| 4 | 18 | 3.7 | 18 | 100 | 0 | 0.0 |
|
| pN stage |
|
|
|
|
|
| 0.434 |
| 0
pos | 189 | 39.1 | 153 | 81.0 | 36 | 19.0 |
|
| 0
neg | 294 | 60.9 | 241 | 82.0 | 53 | 18.0 |
|
| UICC stage |
|
|
|
|
|
| 0.446 |
| 1 | 99 | 20.5 | 76 | 76.8 | 23 | 23.2 |
|
| 2 | 111 | 23.0 | 94 | 84.7 | 17 | 15.3 |
|
| 3 | 201 | 41.7 | 163 | 81.1 | 38 | 18.9 |
|
| 4 | 71 | 14.7 | 60 | 84.5 | 11 | 15.5 |
|
| neoadj. |
|
|
|
|
|
| 0.331 |
| No | 207 | 43.6 | 171 | 82.6 | 36 | 17.4 |
|
|
Yes | 268 | 56.4 | 216 | 80.6 | 52 | 19.4 |
|
|
Total | 475 | 100 | 387 | 81.5 | 88 | 18.5 |
|
| Her2 |
|
|
|
|
|
| 0.036 |
|
neg | 306 | 87.7 | 244 | 79.7 | 62 | 20.3 |
|
|
pos | 43 | 12.3 | 40 | 93.0 | 3 | 7.0 |
|
| TP53 |
|
|
|
|
|
| 0.493 |
|
neg | 150 | 41.9 | 119 | 79.3 | 31 | 20.7 |
|
|
pos | 208 | 58.1 | 172 | 82.7 | 36 | 17.3 |
|
|
Total | 358 | 100 | 291 | 81.3 | 67 | 18.7 |
|
| ARID1A |
|
|
|
|
|
| 0.240 |
|
neg | 48 | 10.0 | 36 | 75.0 | 12 | 25.0 |
|
|
pos | 432 | 90.0 | 355 | 82.2 | 77 | 17.8 |
|
The present study was ethically approved by the
University of Cologne Ethics Committee (reference no. 13-091) and
written informed consent was obtained from all patients. The
procedures followed were in accordance with the Declaration of
Helsinki.
Immunohistochemistry
TMA construction was performed as previously
described (28,29). In brief, tissue cylinders with a
diameter of 1.2 mm were punched from selected tumor tissue blocks
using an in-house developed semi-automated precision instrument and
embedded in empty recipient paraffin blocks (4% formalin for 24 h
at room temperature). Paraffin blocks were cut into 4 µm-thick
sections, which were transferred onto an adhesive coated slide
system. Freshly cut TMA sections were immunostained in one day and
in one experiment. Slides were deparaffinized using standard
protocols with Dewax (Leica Microsystems, Inc.) and 100% ethanol,
denaturated and exposed to heat-induced antigen retrieval for 5 min
in an autoclave at 121°C and pH 9 (Tris-EDTA-buffer). The TMA
slides were incubated with a primary rabbit recombinant monoclonal
antibody specific for claudin 18.2 (clone EPR 19202; 1:200; Abcam;
cat. no. ab222512) using a Leica Bond Max automated system (35578;
Leica Microsystems GmbH) for 20 min 37°C. As a secondary antibody,
the Bond polymer refine detection kit (Leica Microsystems GmbH;
cat. no DS9800) was used for 5 min at 37°C. The primary antibody
detects the same isoform 2 of Claudin 18 as described in clinical
studies previously (19,30). Normal gastric mucosa served as an
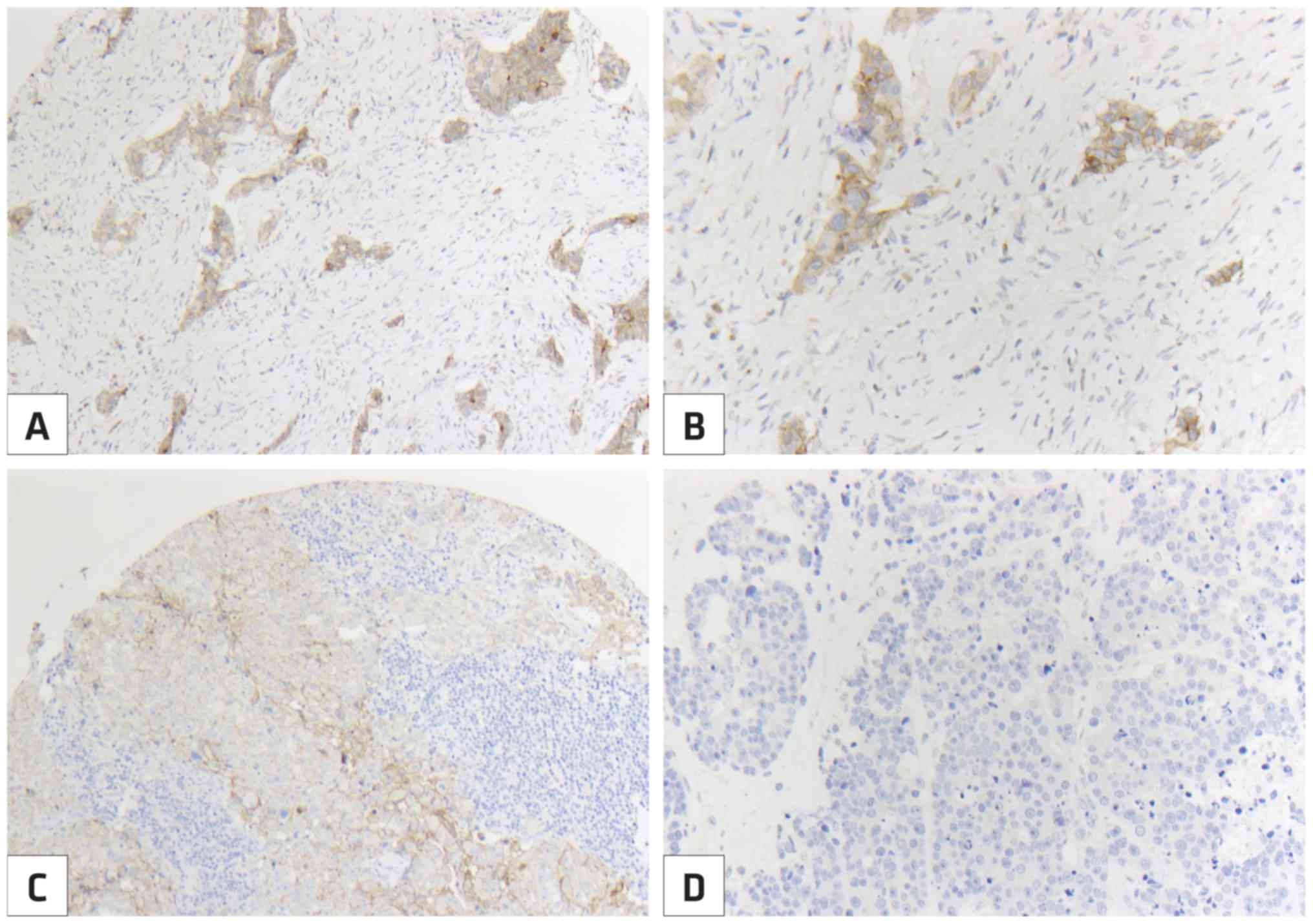
internal control. The claudin 18.2 staining intensity was scored by
two pathologists (AQ and HL) using a two-tier scoring system. The
staining was described as follows: i) Negative, no claudin 18.2
expression; ii) low-grade expression, claudin 18.2 expression of
any intensity in 5–49% of tumor cells; and iii) high-grade
expression, claudin 18.2 expression of any intensity in >49% of
tumor cells (Fig. 1).
Statistical analysis
For the statistical analyses, a long follow-up
period of the patients was available. Follow-up times ranged from a
minimum of 48 months to 204 months. The follow-up of all patients
was performed according to a standardized protocol. During the
first two years, the clinical follow-up of patients was performed
in the hospital every three months. Subsequently, annual
examinations were performed. Follow-up examinations included
obtaining a detailed history, clinical evaluation, abdominal
ultrasound, chest X-ray and additional diagnostic procedures as
required. Follow-up data were available for all patients. SPSS
Statistics for Mac (Version 21; IMB Corp., Armonk, NY, USA) was
used for statistical analysis. Data were presented as the means ±
standard deviation or median with range (min-max).
Immunohistochemistry data were displayed as categorial variables
(0, 1 and 2). All data were collected prospectively according to a
standardized clinical protocol. Interdependence was calculated
using a χ2 and Fisher's exact tests and displayed using
cross-tables. Survival curves were plotted using the Kaplan-Meier
method and analyzed using the log-rank test. Analyses were
performed for independent prognostic factors of OS time, using the
Cox regression model. All tests were two-sided. P<0.05 was
considered to indicate a statistically significant difference.
Results
Expression of claudin 18.2
The present study investigated 685 primary tumor
types and 236 corresponding regional lymph node metastasis samples
obtained from patients with EAC. However, a total of 485/685
primary tumor type TMAs (88.0%) and 195/236 lymph node metastasis
TMAs (82.7%) were analyzed for claudin 18.2 expression. This was
due to a lack of tissue or absence of unequivocal cancer tissue in
certain TMAs. The median follow-up time for the entire cohort was
57.7 months with a calculated 5 year survival rate of 26.6%.
The expression of claudin 18.2 was observed in
89/485 (18.4%) primary tumor TMAs and in 35/195 (17.9%) regional
lymph node metastasis TMAs. There was no significant difference
between the claudin 18.2 expression pattern in primary tumor types
and corresponding lymph node metastases (P=1.000). No significant
differences between claudin 18.2 expression and clinicopathological
data (sex, age, pT stage, lymph node metastasis and grading) were
observed (Table I). Additionally, no
significant differences with tumor protein p53 (TP53) or AT-rich
interaction domain 1A (ARID1A) mutations were identified.
Furthermore, the administration of neoadjuvant treatment did not
significantly influence claudin 18.2 expression (P=0.331).
Interestingly, the analyses revealed significantly decreased
claudin 18.2 expression in human epidermal growth factor receptor 2
(HER2) positive tumors (P=0.036; Table
I).
OS time
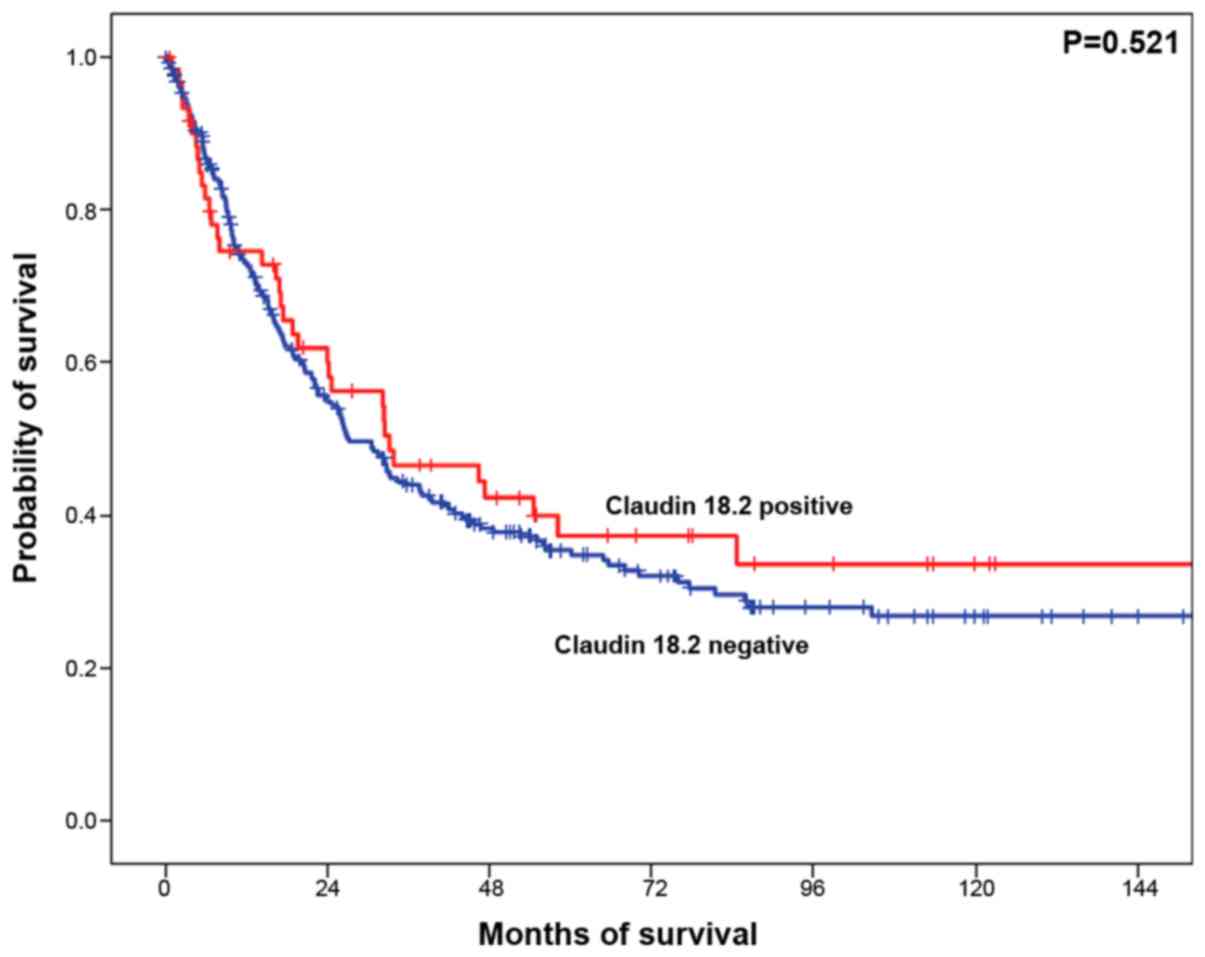
Expression of claudin 18.2 in primary tumor types or
lymph node metastases was not associated with a prolonged or
shortened OS time in patients with EAC. The median OS time in
patients with claudin 18.2 expression was 33.1 months [95%
confidence interval (CI), 8.8–57.5 months] compared with 27.1
months (95% CI, 21.5–32.8 months; P=0.521) in patients with
negative claudin 18.2 expression (Fig.
2). A number of subgroup analyses were performed in order to
detect specific interactions between differences in OS time and
claudin 18.2 expression. However, none of the analyzed co-variables
(including T-cell inflammation, mutations in TP53 and ARID1A and
HER2 expression) affected the OS time in relation to claudin 18.2
expression (data not shown).
Discussion
Personalized therapy approaches for patients with
EAC are urgently required due to the poor prognosis and increasing
incidence of the disease. Comparative molecular analyses of gastric
adenocarcinomas have revealed important differences between gastric
and esophageal adenocarcinomas, including the absence of the
Epstein-Barr virus and microsatellite instability in EAC. Therefore
gastric cancer expression data cannot be applied for the
investigation of EAC (31–33).
Claudin 18.2 is an interesting tight-junction
protein that may be therapeutically modifiable and whose relevance
is currently being tested in studies on gastric cancer (16,18–21,28). In
these studies, the response to therapy is associated with the
measurable presence of the protein in the tumor (16,18–21,30).
This may make claudin 18.2 a relevant biomarker, as we have known
for years with programmed death-ligand 1, HER2/neu or hormone
receptors in breast carcinoma. An important goal of the present
study was to demonstrate how frequently claudin 18.2 expression may
be expected in adenocarcinomas of the esophagus.
To best of our knowledge, the present study is the
largest systematic investigation of claudin 18.2 protein expression
in EAC (n=485) in addition to the first study to detect claudin
18.2 expression in corresponding regional lymph node metastases
using a commercially available monoclonal antibody, which was also
used in other studies on gastric cancer (18–20,30). The
present study demonstrated detectable claudin 18.2 expression in up
to 18.4% of EAC cases. The only other study that has analyzed EAC
so far selected a substantially smaller number of tumor samples
(n=22), used a self-developed antibody, and identified an
expression of claudin 18.2 in 78% of all samples (15). The different expression rates may be
due to the smaller number of tissue samples analyzed and/or due to
a different antibody used in this previous study (15). Additionally, the present study
revealed an expression of claudin 18.2 in a significant number of
the corresponding lymph node metastases, highlighting the
importance of claudin 18.2 for the development of novel targeted
therapies for both primary tumor types and lymph node
metastases.
Since clinical and molecular data on the patient
populations in the present study were available, the potential to
perform statistical analyses in parallel was an option. The
decisive characteristic of a therapy-relevant biomarker is
ultimately its presence and the associated response to therapy.
Whether it allows additional prognostic statements is at best of
secondary academic interest but not biologically significant. For
this reason, however, the present study aimed to address the
academically interesting secondary question and it may be stated
that there is no additional prognostic relevance of claudin 18.2.
This in no way diminishes its importance as a therapeutic
biomarker. Nevertheless, the present study identified a
statistically measurable association between missing claudin 18.2
expression and the presence of Her2/neu expression/amplification
without serious pathophysiological explanations. It may be
hypothesized that an ultimately proliferation-increasing tyrosine
kinase, including Her2/neu, benefits from a missing tight-junction
protein, since a rapidly dividing tumor cell may be impeded in its
invasiveness by an existing cell-cell contact via tight-junctions,
so that an additive effect beneficial for the tumor cells is formed
here.
Regarding claudin 18.2 as a potential target for
immunotherapy, the present results have an impact on potential
future therapeutic strategies. IMAB362, a novel antibody targeting
claudin 18.2, has been investigated in various phase I and phase II
studies for patients with gastric and/or gastro-esophageal junction
cancer and has exhibited anti-tumor activity (16,18–21,28).
Gastrointestinal toxicities were the most commonly observed
treatment-associated adverse events (18–20,30).
The studies cited above exhibited good overall
tolerability of IMAB362. In three of the studies listed here, the
antitumor activity of IMAB362 was demonstrated in gastric
adenocarcinoma and gastroesophageal transition. Serious side
effects were not observed. The most frequently observed side
effects, including nausea and vomiting, should be easily treatable
by already well-known potent anti-emetics (18–20,30).
These results provide an outlook for an effective and low-side
effect therapy in patients with advanced or metastatic EAC, which
should be investigated in future clinical trials.
In conclusion, targeted therapies with manageable
side effects are urgently required to improve the outcome of
patients with locally advanced or metastasized esophageal
carcinomas. The results obtained in the present study suggested
that claudin 18.2 may serve as a novel therapeutic target in
EAC.
Acknowledgements
Not applicable.
Funding
Not applicable.
Availability of data and materials
The datasets used and/or analyzed in the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
AQ designed the study. AQ and HL scored the staining
intensity for the immunohistochemistry. FG, VM and AQ analyzed and
interpreted the data. VM and FG wrote the manuscript. AQ, VM, EC,
HL, CB, WS and RB: made substantial contributions to conception and
design and acquisition of data. FG, TZ, AT and HA: made substantial
contributions to analysis and interpretation of data. All authors
reviewed the final manuscript for publication.
Ethics approval and consent to
participate
Procedures were followed as outlined in accordance
with ethical standards formulated in the Helsinki Declaration 1995
(and revised in 2000). Written informed consent was obtained from
all patients for the usage of their tumor specimens; and ethical
approval was obtained from the University of Cologne Ethics
Committee (reference number: 13-091).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Global Burden of Disease Cancer
Collaboration, ; Fitzmaurice C, Akinyemiju TF, Al Lami FH, Alam T,
Alizadeh-Navaei R, Allen C, Alsharif U, Alvis-Guzman N, Amini E, et
al: Global, regional, and national cancer incidence, mortality,
years of life lost, years lived with disability, and
disability-adjusted life-years for 29 cancer groups, 1990 to 2016:
A systematic analysis for the global burden of disease study. JAMA
Oncol. 1:1533–1568. 2018.
|
|
2
|
Lepage C, Rachet B, Jooste V, Faivre J and
Coleman MP: Continuing rapid increase in esophageal adenocarcinoma
in England and Wales. Am J Gastroenterol. 103:2694–2649. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Edgren G, Adami HO, Weiderpass E and Nyren
O: A global assessment of the oesophageal adenocarcinoma epidemic.
Gut. 62:1406–1414. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Al-Batran SE, Goetze TO, Mueller DW, Vogel
A, Winkler M, Lorenzen S, Novotny A, Pauligk C, Homann N, Jungbluth
T, et al: The RENAISSANCE (AIO-FLOT5) trial: Effect of chemotherapy
alone vs. Chemotherapy followed by surgical resection on survival
and quality of life in patients with limited-metastatic
adenocarcinoma of the stomach or esophagogastric junction-a phase
III trial of the German AIO/CAO-V/CAOGI. BMC Cancer. 17:8932017.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pohl H, Sirovich B and Welch HG:
Esophageal adenocarcinoma incidence: Are we reaching the peak?
Cancer Epidemiol Biomarkers Prev. 19:1468–1470. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Barrett JC: Mechanisms of multistep
carcinogenesis and carcinogen risk assessment. Environ Health
Perspect. 100:9–20. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nones K, Waddell N, Wayte N, Patch AM,
Bailey P, Newell F, Holmes O, Fink JL, Quinn MCJ, Tang YH, et al:
Genomic catastrophes frequently arise in esophageal adenocarcinoma
and drive tumorigenesis. Nat Commun. 5:52242014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Li X, Galipeau PC, Paulson TG, Sanchez CA,
Arnaudo J, Liu K, Sather CL, Kostadinov RL, Odze RD, Kuhner MK, et
al: Temporal and spatial evolution of somatic chromosomal
alterations: A case-cohort study of barrett's esophagus. Cancer
Prev Res (Phila). 7:114–127. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Robert Koch-Institut (Hrsg) und die
Gesellschaft der epidemiologischen Krebsregister in Deutschland
e.V. (Hrsg). Berlin: Krebs in Deutschland für. 2013/2014. 2017
|
|
10
|
Tustumi F, Kimura CM, Takeda FR, Uema RH,
Salum RA, Ribeiro-Junior U and Cecconello I: Prognostic factors and
survival analysis in esophageal carcinoma. Arq Bras Cir Dig.
29:138–141. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tsukita S, Furuse M and Itoh M:
Multifunctional strands in tight junctions. Nat Rev Mol Cell Biol.
2:285–293. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tsukita S, Yamazaki Y, Katsuno T, Tamura A
and Tsukita S: Tight junction-based epithelial microenvironment and
cell proliferation. Oncogene. 27:6930–6938. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Van Itallie CM and Anderson JM: Claudins
and epithelial paracellular transport. Annu Rev Physiol.
68:403–429. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mineta K, Yamamoto Y, Yamazaki Y, Tanaka
H, Tada Y, Saito K, Tamura A, Igarashi M, Endo T, Takeuchi K and
Tsukita S: Predicted expansion of the claudin multigene family.
FEBS Lett. 585:606–612. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sahin U, Koslowski M, Dhaene K, Usener D,
Brandenburg G, Seitz G, Huber C and Türeci O: Claudin-18 splice
variant 2 is a pan-cancer target suitable for therapeutic antibody
development. Clin Cancer Res. 14:7624–7634. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Singh P, Toom S and Huang Y: Anti-Claudin
18.2 antibody as new targeted therapy for advanced gastric cancer.
J Hematol Oncol. 10:1052017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Woll S, Schlitter AM, Dhaene K, Roller M,
Esposito I, Sahin U and Türeci Ö: Claudin 18.2 is a target for
IMAB362 antibody in pancreatic neoplasms. Int J Cancer.
134:731–739. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sahin U, Schuler M, Richly H, Bauer S,
Krilova A, Dechow T, Jerling M, Utsch M, Rohde C, Dhaene K, et al:
A phase I dose-escalation study of IMAB362 (Zolbetuximab) in
patients with advanced gastric and gastro-oesophageal junction
cancer. Eur J Cancer. 100:17–26. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Al-Batran S, Al-Batran SE, Schuler MH, et
al: FAST: An international, multicenter, randomized, phase II trial
of epirubicin, oxaliplatin, and capecitabine (EOX) with or without
IMAB362, a first-in-class anti-CLDN18.2 antibody, as first-line
therapy in patients with advanced CLDN18.2+ gastric and
gastroesophageal junction (GEJ) adenocarcinoma. J Clin Oncol. 34
(no. 18-Suppl):2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Trarbach T, Schuler M, Zvirbule Z, Lordick
F, Krilova A, Helbig U, Schulze-Bergkamen H, Thuss-Patience PC,
Wichert G, Schmiegel W, et al: 636P-Efficacy and safety of multiple
doses of IMAB362 in patients with advanced gastro-esophageal
cancer: Results of a phase II study. Ann Oncol. 25 (Suppl
4):iv210–iv253. 2014. View Article : Google Scholar
|
|
21
|
Sahin U, Al-Batran SE, Hozaeel W, et al:
IMAB362 plus zoledronic acid (ZA) and interleukin-2 (IL-2) in
patients (pts) with advanced gastroesophageal cancer (GEC):
Clinical activity and safety data from the PILOT phase I trial. J
Clin Oncol. 33 (no. 15_Suppl):2015. View Article : Google Scholar
|
|
22
|
Holscher AH, Schneider PM, Gutschow C and
Schroder W: Laparoscopic ischemic conditioning of the stomach for
esophageal replacement. Ann Surg. 245:241–246. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shapiro J, van Lanschot JJB, Hulshof MCCM,
van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, van Laarhoven
HWM, Nieuwenhuijzen GAP, Hospers GAP, Bonenkamp JJ, et al:
Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for
oesophageal or junctional cancer (CROSS): Long-term results of a
randomised controlled trial. Lancet Oncol. 16:1090–1098. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hoeppner J, Lordick F, Brunner T, Glatz T,
Bronsert P, Rothling N, Schmoor C, Lorenz D, Ell C, Hopt UT and
Siewert JR: ESOPEC: Prospective randomized controlled multicenter
phase III trial comparing perioperative chemotherapy (FLOT
protocol) to neoadjuvant chemoradiation (CROSS protocol) in
patients with adenocarcinoma of the esophagus (NCT02509286). BMC
Cancer. 16:5032016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wittekind C and Oberschmid B: Pathology
and new UICC classification of esophageal carcinoma. Onkologe.
16:453–461. 2010. View Article : Google Scholar
|
|
26
|
UICC, . TNM: Klassifikation maligner
Tumoren. 8th. Wiley; 2017
|
|
27
|
Schneider PM, Metzger R, Schaefer H,
Baumgarten F, Vallbohmer D, Brabender J, Wolfgarten E,
Bollschweiler E, Baldus SE, Dienes HP and Hoelscher AH: Response
evaluation by endoscopy, rebiopsy, and endoscopic ultrasound does
not accurately predict histopathologic regression after neoadjuvant
chemoradiation for esophageal cancer. Ann Surg. 248:902–908. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Simon R, Mirlacher M and Sauter G: Tissue
microarrays. Method Mol Med. 114:257–268. 2005.
|
|
29
|
Helbig D, Ihle MA, Putz K, Tantcheva-Poor
I, Mauch C, Buttner R and Quaas A: Oncogene and therapeutic target
analyses in atypical fibroxanthomas and pleomorphic dermal
sarcomas. Oncotarget. 7:21763–21774. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tureci O, Sahin U, Schulze-Bergkamen H,
Zvirbule Z, Lordick F, Koeberle D, Thuss-Patience P, Ettrich T,
Arnold D, Bassermann F, et al: A multicentre, phase IIa study of
zolbetuximab as a single agent in patients with recurrent or
refractory advanced adenocarcinoma of the stomach or lower
oesophagus: The MONO study. Ann Oncol. 30:1487–1495. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Fukayama M and Ushiku T: Epstein-Barr
virus-associated gastric carcinoma. Pathol Res Pract. 207:529–537.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Cancer Genome Atlas Research Network, .
Comprehensive molecular characterization of gastric adenocarcinoma.
Nature. 513:202–209. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hewitt LC, Inam IZ, Saito Y, Yoshikawa T,
Quaas A, Hoelscher A, Bollschweiler E, Fazzi GE, Melotte V, Langley
RE, et al: Epstein-Barr virus and mismatch repair deficiency status
differ between oesophageal and gastric cancer: A large multi-centre
study. Eur J Cancer. 94:104–114. 2018. View Article : Google Scholar : PubMed/NCBI
|