Introduction
Colorectal cancer (CRC) is the third most frequently
diagnosed tumor, with the second highest mortality rate globally in
2018 (1). Due to its distinct
molecular characteristics and genetic heterogeneity, patients with
CRC often have different natural processes and clinical outcomes.
Therefore, there is an urgent requirement to explore the molecular
subtypes of CRC for precise therapy. Recently, several studies have
reported some distinct subtypes of CRC. However, the subclasses
generated from these studies either lack in the analysis of
different molecular mechanisms (2,3) or have
insufficient independent samples for validation (4,5). Thus, a
more effective and credible subgroup is required for the treatment
of patients with CRC.
In recent years, owing to the further understanding
of the interactions between the immune system and tumor cell
environment, immunotherapies such as anti-programmed cell death
protein 1 (PD-1), anti-programmed cell death 1 ligand 1 (PD-L1) and
anti-cytotoxic T-lymphocyte protein 4 (CTLA-4) have markedly
revolutionized the therapeutic approaches in several cancer types,
including lung cancer (6,7), melanoma (8,9), head
and neck cancer (10), bladder
cancer (11), kidney cancer
(12) and CRC with deficient
mismatch repair (13,14). An ~50% elevated response rate was
found, which is a noteworthy improvement in patients who received
ICI treatment due to the reversion of an immunosuppressive
microenvironment (15,16). However, only a small number of CRC
patients exhibit a clinical response to ICI treatment, with the
majority of patients not benefiting from the therapy (17). The therapeutic effect of ICI agents
is ascribed to several important factors, such as expression of
PD-L1, proportion of tumor-infiltrating lymphocytes (TILs) and
tumor mutation burden (TMB). High PD-L1 expression is an essential
factor in the use of pembrolizumab, which is approved by the Food
and Drug Administration (FDA) for patients with non-small cell lung
cancer (NSCLC) (18). Several
studies have also reported the vital roles of TIL and TMB in the
response to ICI agents (19–21). In summary, the exploration of the CRC
subtype that is suitable to receive ICI therapy is important and
urgently required.
In the present study, immune-related gene expression
profiles of four independent CRC cohorts were used to identify the
potential subtype which may be sensitive to immune checkpoint
blockade. Findings of the present study have implications for
guiding clinical immunotherapy for patients with CRC.
Materials and methods
Acquisition of genomic data
Gene expression data of 662 CRC samples with overall
survival time and status from TCGA cohort (https://gdc.cancer.gov) and 619 samples of three
datasets (GSE103479, GSE38832 and GSE87211) (22–24) from
the Gene Expression Omnibus (https://www.ncbi.nlm.nih.gov/geo/) were
retrospectively acquired. TCGA cohort (mean age, 66.33; age range:
31–90; sex distribution: 355 male and 307 female patients);
GSE103479 dataset (mean age: 64.26; age range: 35–88; sex
distribution: 83 male and 72 female patients); GSE8832 dataset
(mean age: 59.63; age range: 32–89; sex distribution: 69 male and
53 female patients) and GSE87211 dataset (mean age: 63.16; age
range: 38–88; sex distribution: 182 male and 160 female patients).
Clinical characteristics of these four cohorts are presented in
Table SI. Finally, a total of 1,281
CRC samples with gene expression data and survival information from
four independent datasets were obtained (Table SII). Complete clinical data were
available for all patients included in the present study. Gene
expression profiles were consistently normalized to reduce
variance. Expression levels of genes with multiple probes were
presented as the mean expression of all probes.
Immune-related prognostic signature
used for molecular subtyping
A prognostic signature was established based on a
previously conducted immune-related genes study (25). The aforementioned previous study
comprehensively described the immune landscape of >10,000
samples, comprising 33 different cancer types, and integrated 160
immune-related signatures containing 2,995 immune genes. Univariate
Cox proportional hazards model was used to evaluate the association
between the expression of these genes and the overall survival of
patients with CRC. Genes with P<0.01 were included in the
signature to perform molecular subtyping.
NMF clustering analysis
Molecular subtyping was performed applying
non-negative matrix factorization (NMF) (26,27). A
binary matrix (A) describing the expression of
immune-related genes (rows) across CRC samples (columns) was
established. Subsequently, the expression matrix A was
factorized into two non-negative matrices (W and H;
A≈WH). Matrix H was applied to cluster samples
into distinct subtypes. The values of cophenetic, dispersion and
silhouette coefficients were used to select the optimal number of
subtypes. The NMF clustering analysis was performed with the R
package ‘NMF’ v.0.21.0 (28).
Prediction of response to ICI
treatment
The tumor immune dysfunction and exclusion (TIDE)
algorithm (29) was applied to
predict potential distinct responses to ICI therapy. TIDE is a gene
expression biomarker for predicting the response to immune
checkpoint blockade in patients. A low TIDE prediction score
represents weak potential immune escape, and therefore these
patients would potentially exhibit a greater immune therapy
response. TIL proportion was analyzed using the CIBERSORT algorithm
(30), which is a useful analytical
tool to provide an evaluation of the abundances of 22 immune cell
types in a mixed cell population, using gene expression data.
Gene set enrichment analysis
(GSEA)
Patients with CRC were partitioned into two groups,
according to the subtyping results clustered with the molecular
expression features. ‘DEseq2’ v.1.26.0 (31) and ‘limma’ v.3.34.8 (32) packages were applied to calculate the
differential t statistics of the RNA sequencing and microarray
data. The t statistic was used as the input to R function in the
‘fgsea’ v.1.12.0 package (http://bioconductor.org/packages/release/bioc/html/fgsea.html)
to perform GSEA. The pathway annotation signatures from the Kyoto
Encyclopedia of Genes and Genomes (KEGG) and Gene Ontology (GO)
databases in Molecular Signatures Database (MSigDB) (33) were used.
Normalization of gene expression
data
In the present study, the molecular subtyping of CRC
samples was conducted using the NMF algorithm. The essential
condition for performing the NMF approach was non-negative values,
therefore, the gene expression data was compressed into the range
from 0–1 in all distinct platforms to achieve data
normalization.
Statistical analyses
Statistical analyses were conducted with R software
3.6.1 (https://cran.r-project.org). The
difference in clinical characteristics between two subtypes were
compared using the χ2 test, and differences of TIDE
score, PD-L1 expression and TMB were compared using the
Wilcoxon rank-sum test. Survivals plot were drawn using the
Kaplan-Meier method and log-rank test for comparison. The
association between CRC subtypes and prognosis was analyzed with
univariate and multivariate Cox proportional hazards model in the R
‘survival’ package (v.2.41–3) (https://gitub.com/therneau/survival). P<0.05 was
considered to indicate a statistically significant difference.
Results
Identification of two CRC subtypes
with distinct prognoses
Using the univariate Cox proportional hazard model,
the association between the expression of 2,995 immune-related
genes and the prognosis of patients with CRC in TCGA cohort was
determined. Finally, 53 genes with P<0.01 (Table SIII) were included in the prognostic
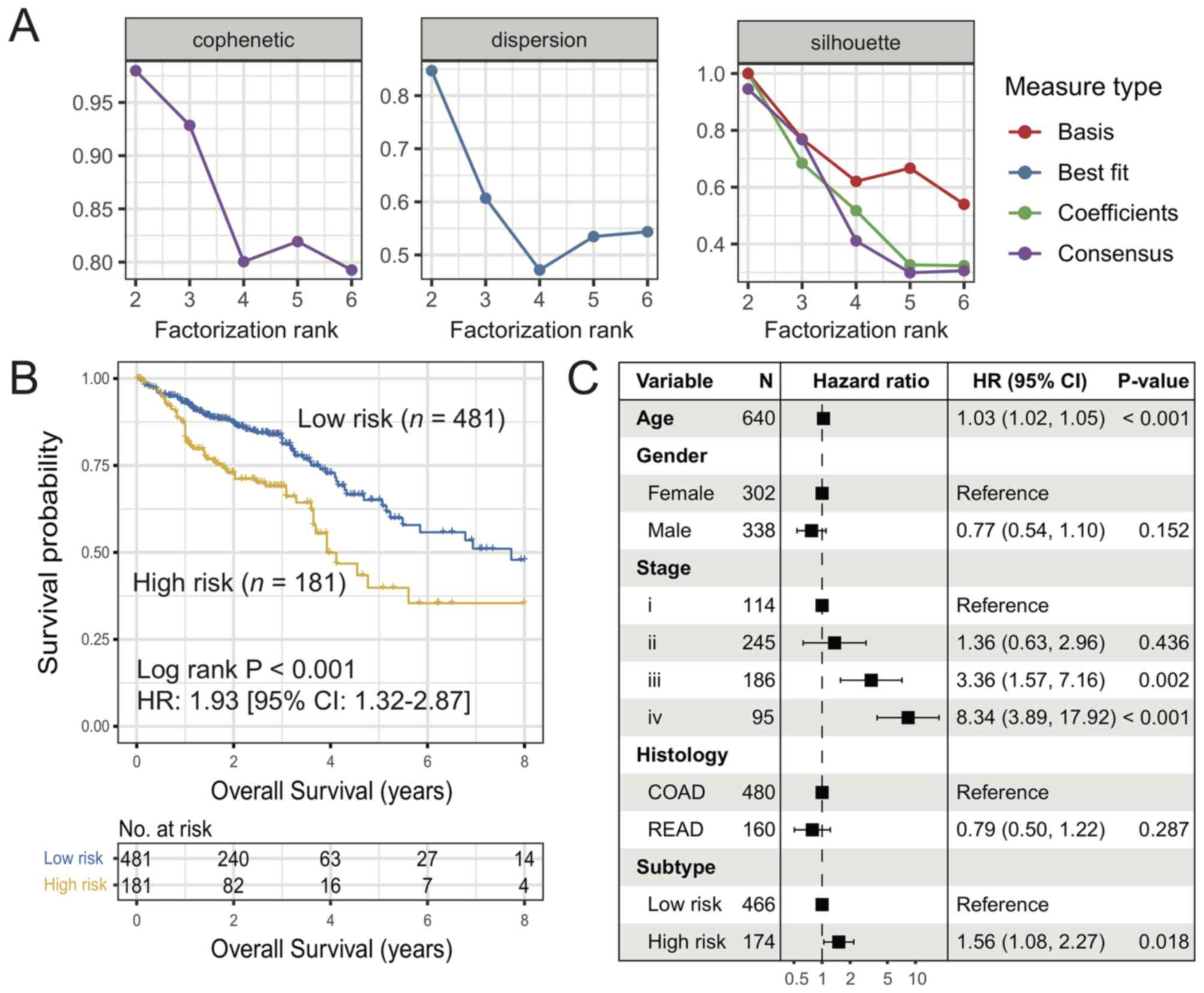
signature for molecular subtyping. NMF unsupervised clustering
analysis of these 53 immune genes was performed and the results
showed that the cophenetic, dispersion and silhouette coefficients
harbored the maximum value for the factorization rank of two
subtypes (Figs. 1A and S1). The survival analysis of these two
subtypes indicated that the overall survival rate of patients in
the high-risk subtype was lower compared with that of patients in
the low-risk subtype (HR, 1.93; 95% CI, 1.32–2.87; log-rank
P<0.001; Fig. 1B). Multivariate
Cox regression analysis adjusted for age, gender, stage and
histology remained statistically significant (HR, 1.56; 95% CI,
1.08–2.27; P=0.018; Fig. 1C).
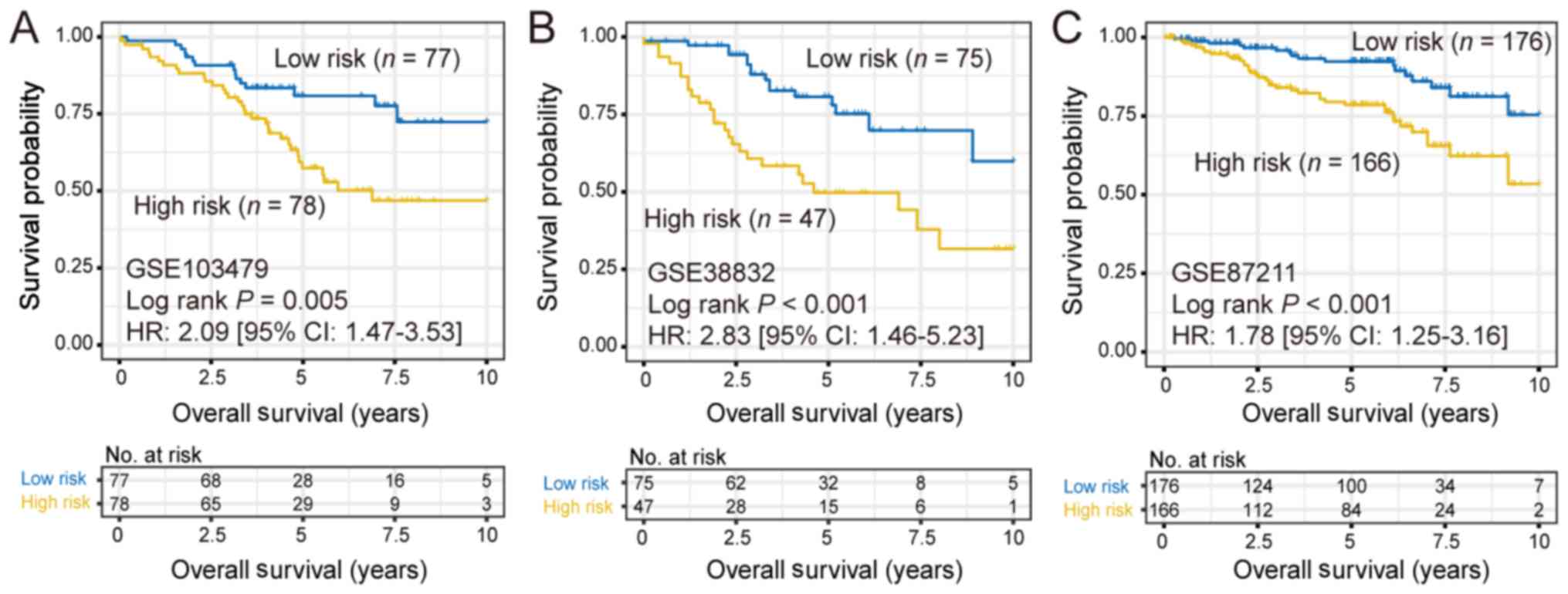
In order to verify whether the aforementioned
subtyping approach would discover the same subtypes in other CRC
cohorts, the same clustering approach was applied to analyze 3
independent CRC cohorts, including GSE103479 (n=155), GSE38832
(n=122) and GSE87211 (n=342). Consistently, two different subtypes
were identified in all 3 additional cohorts and the high-risk
subtype also exhibited a significantly poorer prognosis [GSE103479:
HR, 2.09 (95% CI, 1.47–3.53; log-rank P=0.005); GSE38832: HR, 1.78
(95% CI, 1.25–3.16; log-rank P<0.001) and GSE87211: HR, 1.78
(95% CI, 1.25–3.16; log-rank P<0.001); Fig. 2].
Prediction of response to ICB therapy
in the two CRC subtypes
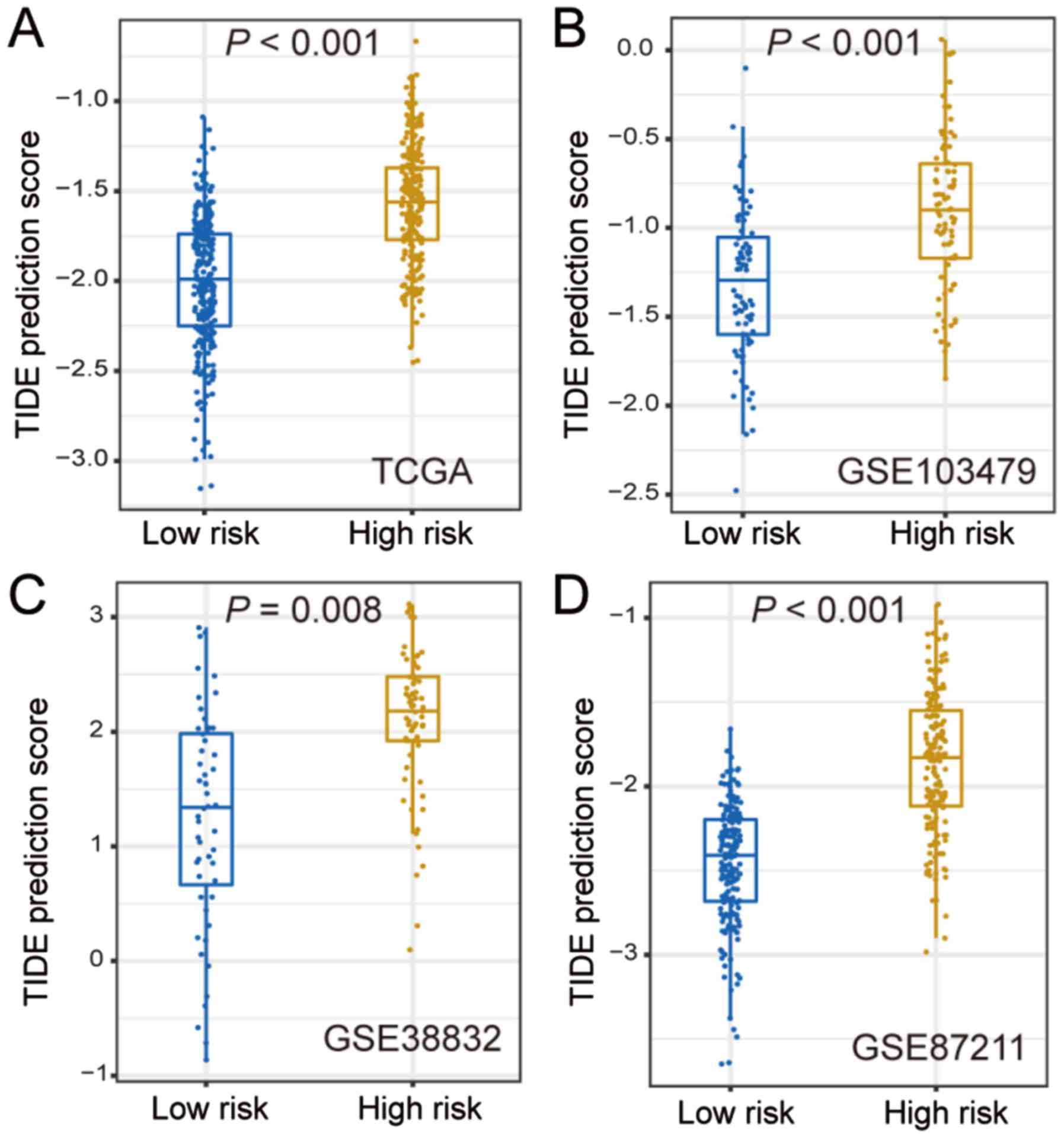
Since the two CRC subtypes were identified by the
application of 53 immune-related genes, it was hypothesized that
these two subtypes may have distinct responses to ICB therapy.
Thus, the TIDE algorithm was used to predict the potentially
different responses to ICB therapy. In TCGA cohort, the TIDE
prediction score was significantly lower in the low-risk subtype
compared with that in the high-risk group (P<0.001; Fig. 3A), which was further validated in the
three other independent cohorts (GSE103479, GSE38832 and GSE87211;
all P<0.01; Fig. 3B-D). These
findings revealed that the patients of the low-risk subtype may be
more sensitive to ICB treatment.
Differences in ICI response markers
between the two CRC subtypes
PD-L1 expression, TIL and TMB are highly important
clinical factors, due to their vital roles in immunotherapy
responses. Therefore, the differences in these 3 factors were
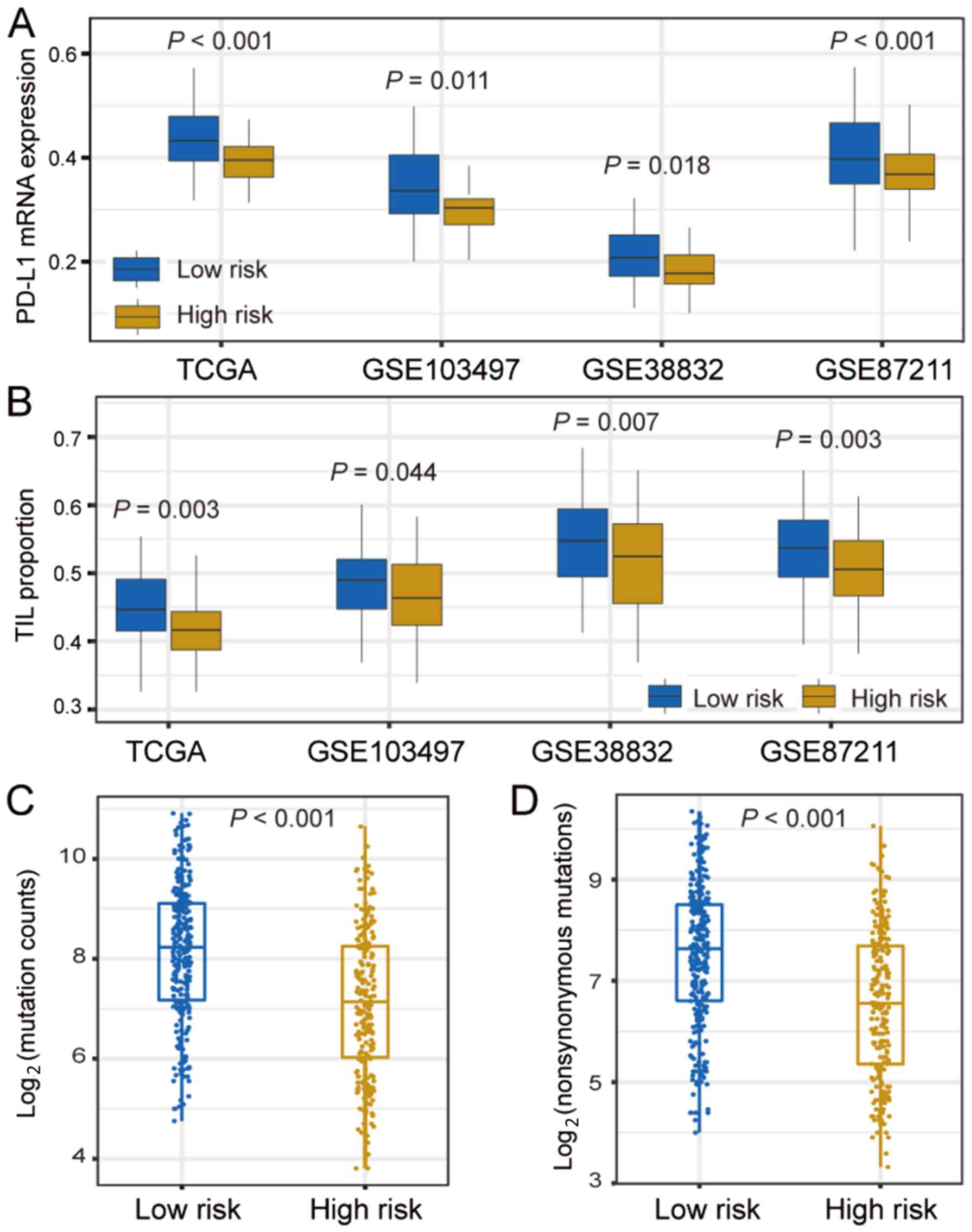
compared between the two CRC subtypes. PD-L1 expression was
significantly higher in the low-risk subtype compared with that in
the high-risk subtype in TCGA cohort (P<0.001), which was
further validated in three other independent cohorts (GSE103479,
GSE38832 and GSE87211; all P<0.05; Fig. 4A).
Results showed that the TIL proportion was
significantly higher in the patients of the low-risk subtype
compared with that in the high-risk group in TCGA cohort (P=0.003).
This association was also corroborated in the three additional
validation cohorts (GSE103479, GSE38832 and GSE87211; all
P<0.05; Fig. 4B). The differences
in the infiltration of 22 immune cells between the two identified
CRC subtypes in the TCGA cohort are shown in Fig. S2. The results demonstrated that the
low-risk subtype has significantly higher specific immune cells
infiltration (e.g., CD4 T cells, plasma cells, natural killer cells
and dendritic cells), which was consistent with the aforementioned
results.
Patients with higher TMB often have a higher number
of neoantigen; therefore, these patients could obtain a stronger
immune response (34,35). It was found that patients in the
low-risk subgroup had significantly higher TMB compared with
patients in the high-risk group (P<0.001; Fig. 4C). TMB is closely associated with
genomic instability. DNA damage repair (DDR)-related genes, such as
BRCA1/2, TP53 and POLE, and clinical factors were
therefore considered in the multivariate logistic regression model.
Following adjustment of these confounding factors, the association
between the low-risk subtype and higher TMB remained notably
significant (OR, 2.95; 95% CI, 1.89–4.67; P<0.001; Fig. S3). Neoantigens are generated mainly
owing to non-synonymous mutations. It was found that the low-risk
subtype harbored a significantly higher non-synonymous mutation
load compared with the high-risk group (P<0.001; Fig. 4D).
Functional annotation of the low-risk
subtype
In order to verify whether the two CRC subtypes had
distinct functionalities, differential analysis and GSEA pathway
analysis of genome-wide gene expression data were performed on the
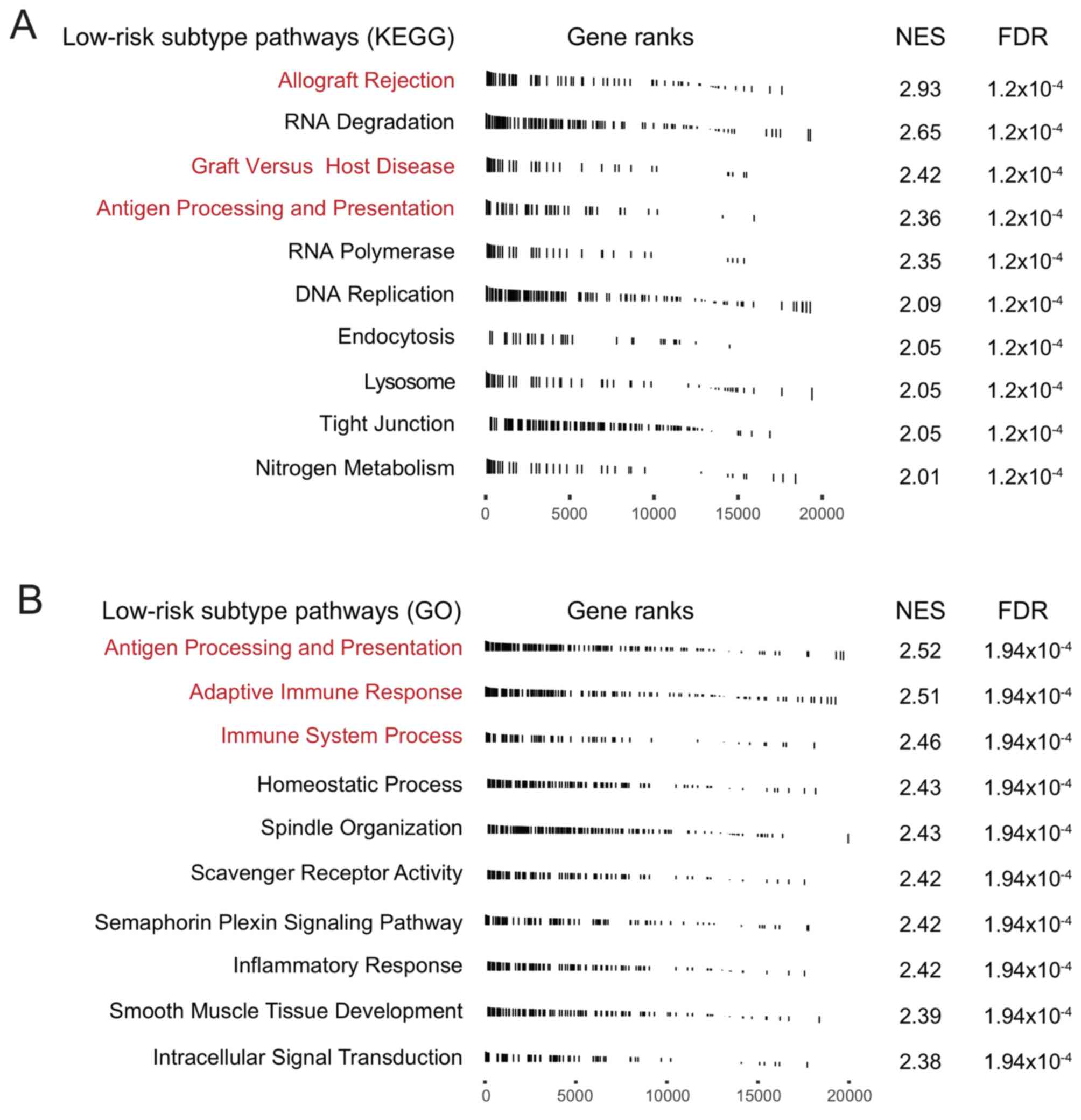
two CRC subtypes in TCGA CRC cohort. Analysis of differentially
expressed genes in the KEGG pathway demonstrated that signaling
pathways associated with immune response activation, such as
‘allograft rejection’, ‘graft versus host disease’, and ‘antigen
processing and presentation’ were significantly enriched in the
low-risk subtype (Fig. 5A). GO
analysis also revealed the enrichment of ‘antigen processing and
presentation’ signaling in the low-risk subtype. Both the ‘adaptive
immune response’ and ‘immune system process’ pathways were also
significantly enriched in low-risk patients (Fig. 5B). These results suggested that
patients in the low-risk subgroup had a better immune response.
Discussion
The present study identified two clinically distinct
subtypes of CRC, with markedly different clinical outcomes and
immune infiltration patterns, by using immune-related signatures on
TCGA cohort. For responses to ICI therapy in the two CRC subtypes,
the TIDE algorithm demonstrated a low score in patients of the
low-risk subtype compared with that in patients of the high-risk
subtype. Furthermore, higher PD-L1 expression, TIL proportion and
TMB were remarkably enriched in the low-risk subtype. Finally, GSEA
pathway analysis indicated immune response activation-, and
‘antigen processing and presentation’-related pathways to be
significantly enriched in the low-risk subtype. Overall, the
present study suggests that patients in the low-risk group have the
potential to respond better to ICI treatment.
The NMF algorithm is a useful tool to perform
clustering or subtyping, and extract genomic signatures; previous
studies have shown its utility in distinct research directions,
such as identification of image pattern, signal processing and text
mining (36–38). The TIDE prediction score is a better
predictor of ICI therapy compared with PD-L1 expression and TMB.
The algorithm uses gene expression signatures to model two major
mechanisms of tumor immune evasion: The induction of T-cell
dysfunction in tumors with high infiltration of cytotoxic T
lymphocytes (CTLs) and the prevention of T-cell infiltration in
tumors with a low CTL level (25).
In the present study, patients of the low-risk subtype harbored a
significantly lower TIDE prediction score compared with patients of
the high-risk subtype in TCGA and validation cohorts, suggesting
that this subtype has potential for an improved response to
ICI.
To date, only PD-L1 expression is confirmed by the
FDA as an official criterion for ICI therapy (18). Based on the results from the
KEYNOTE-001 clinical trial (18),
high PD-L1 expression is now an essential condition for the use of
pembrolizumab in NSCLC. The present study also demonstrated
markedly higher PD-L1 expression in the low-risk CRC subtype
compared with that in the high-risk subtype in TCGA and validation
cohorts. TMB is emerging as a potential biomarker to predict the
response to ICI therapy. Three clinical trials, including
KEYNOTE-001, CHECKMATE-026 and CHECKMATE-227, demonstrated that
patients with higher TMB responded more effectively to ICI
(39,40). A recent study reported that high TMB
was positively associated with the response to PD-1/PD-L1
inhibitors (such as pembrolizumab) in metastatic CRC, and may serve
as a biomarker to predict associated immune therapy effects
(41). The present study discovered
that TMB in the low-risk CRC subtype was significantly higher
compared with that in the high-risk subtype in TCGA cohort.
Meanwhile, the non-synonymous mutation load was also markedly
enriched in the low-risk CRC subgroup. Studies have reported that
mutations of BRCA1/2, POLE and TP53 genes also
indicate high TMB, due to the loss of DDR (42–44).
Thus, multivariate analysis was conducted following the adjustment
of these factors (i.e., mutations of BRCA1/2, POLE and
TP53), and the association of low-risk subtype with higher
TMB remained statistically significant. Several studies have
revealed that TILs play crucial roles in the tumor-immune
microenvironment, immune response and prognosis of CRC (44–47). In
the present study, results from the CIBERSORT algorithm showed that
the low-risk CRC subtype harbored a significantly higher TIL
proportion compared with the high-risk group in TCGA and
independent validation cohorts. Thus, TMB, TIL proportion and
non-synonymous mutations load may contribute to the response to ICI
in patients of the low-risk CRC subtype.
The present study has several limitations. Firstly,
the gene expression data from the four validation cohorts were from
different platforms, which may create bias in the analyses.
Secondly, the results associated with the CRC mutation data derived
from TCGA cohort were not sufficiently validated, owing to the
unavailability of mutation data from the other cohorts. Thirdly,
the number of CRC samples with a gene expression profile is
currently insufficient to perform molecular subtyping, and thus the
results could not be validated using biological experiments such as
histochemical staining.
In summary, two clinically distinct CRC subtypes
were identified that have significantly different survival outcomes
and immune microenvironments. The low-risk CRC subtype may indicate
improved response to ICI therapy, due to higher PD-L1 expression,
TIL proportion and TMB. Thus, this molecular classification study
and integrated multi-omic analysis of CRC may lead to a novel
therapeutic approach for improving the prognosis of patients in the
low-risk CRC subtype.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
XZ and GC designed the study; GC developed the
methodology and acquired the related data; GC, LW, TD, YC and CC
performed the data analysis and interpretation; GC and XZ drafted
and revised the manuscript; XZ supervised the study. All authors
read and approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CRC
|
colorectal cancer
|
|
ICI
|
immune checkpoint inhibitor
|
|
TCGA
|
The Cancer Genome Atlas
|
|
NMF
|
non-negative matrix factorization
|
|
TIDE
|
tumor immune dysfunction and
exclusion
|
|
GSEA
|
gene set enrichment analysis
|
|
PD-L1
|
programmed death-ligand 1
|
|
TILs
|
tumor-infiltrating lymphocytes
|
|
TMB
|
tumor mutation burden
|
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kamal Y, Schmit SL, Hoehn HJ, Amos CI and
Frost HR: Transcriptomic differences between primary colorectal
adenocarcinomas and distant metastases reveal metastatic colorectal
cancer subtypes. Cancer Res. 79:4227–4241. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rashid M, Vishwakarma RK, Deeb AM, Hussein
MA and Aziz MA: Molecular classification of colorectal cancer using
the gene expression profile of tumor samples. Exp Biol Med
(Maywood). 244:1005–1016. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Abdul Aziz NA, Mokhtar NM, Harun R, Mollah
MM, Mohamed Rose I, Sagap I, Mohd Tamil A, Wan Ngah WZ and Jamal R:
A 19-Gene expression signature as a predictor of survival in
colorectal cancer. BMC Med Genomics. 9:582016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen H, Sun X, Ge W, Qian Y, Bai R and
Zheng S: A seven-gene signature predicts overall survival of
patients with colorectal cancer. Oncotarget. 8:95054–95065. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Borghaei H, Paz-Ares L, Horn L, Spigel DR,
Steins M, Ready NE, Chow LQ, Vokes EE, Felip E, Holgado E, et al:
Nivolumab versus docetaxel in advanced nonsquamous non-small-cell
lung cancer. N Engl J Med. 373:1627–1639. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Brahmer J, Reckamp KL, Baas P, Crinò L,
Eberhardt WE, Poddubskaya E, Antonia S, Pluzanski A, Vokes EE,
Holgado E, et al: Nivolumab versus docetaxel in advanced
squamous-cell non-small-cell lung cancer. N Engl J Med.
373:123–135. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wolchok JD, Chiarion-Sileni V, Gonzalez R,
Rutkowski P, Grob JJ, Cowey CL, Lao CD, Wagstaff J, Schadendorf D,
Ferrucci PF, et al: Overall survival with combined nivolumab and
ipilimumab in advanced melanoma. N Engl J Med. 377:1345–1356. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hodi FS, O'Day SJ, McDermott DF, Weber RW,
Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel
JC, et al: Improved survival with ipilimumab in patients with
metastatic melanoma. N Engl J Med. 363:711–723. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cohen EEW, Soulières D, Le Tourneau C,
Dinis J, Licitra L, Ahn MJ, Soria A, Machiels JP, Mach N, Mehra R,
et al: Pembrolizumab versus methotrexate, docetaxel, or cetuximab
for recurrent or metastatic head-and-neck squamous cell carcinoma
(KEYNOTE-040): A randomised, open-label, phase 3 study. Lancet.
393:156–167. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bellmunt J, de Wit R, Vaughn DJ, Fradet Y,
Lee JL, Fong L, Vogelzang NJ, Climent MA, Petrylak DP, Choueiri TK,
et al: Pembrolizumab as second-line therapy for advanced urothelial
carcinoma. N Engl J Med. 376:1015–1026. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Motzer RJ, Escudier B, McDermott DF,
George S, Hammers HJ, Srinivas S, Tykodi SS, Sosman JA, Procopio G,
Plimack ER, et al: Nivolumab versus everolimus in advanced
renal-cell carcinoma. N Engl J Med. 373:1803–1813. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Overman MJ, McDermott R, Leach JL, Lonardi
S, Lenz HJ, Morse MA, Desai J, Hill A, Axelson M, Moss RA, et al:
Nivolumab in patients with metastatic DNA mismatch repair-deficient
or microsatellite instability-high colorectal cancer (CheckMate
142): An open-label, multicentre, phase 2 study. Lancet Oncol.
18:1182–1191. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Overman MJ, Lonardi S, Wong KYM, Lenz HJ,
Gelsomino F, Aglietta M, Morse MA, Van Cutsem E, McDermott R, Hill
A, et al: Durable clinical benefit with nivolumab plus ipilimumab
in DNA mismatch repair-deficient/microsatellite instability-high
metastatic colorectal cancer. J Clin Oncol. 36:773–779. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Motzer RJ, Rini BI, McDermott DF, Arén
Frontera O, Hammers HJ, Carducci MA, Salman P, Escudier B,
Beuselinck B, Amin A, et al: Nivolumab plus ipilimumab versus
sunitinib in first-line treatment for advanced renal cell
carcinoma: Extended follow-up of efficacy and safety results from a
randomised, controlled, phase 3 trial. Lancet Oncol. 20:1370–1385.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Larkin J, Chiarion-Sileni V, Gonzalez R,
Grob JJ, Cowey CL, Lao CD, Schadendorf D, Dummer R, Smylie M,
Rutkowski P, et al: Combined nivolumab and ipilimumab or
monotherapy in untreated melanoma. N Engl J Med. 373:23–34. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Asaoka Y, Ijichi H and Koike K: PD-1
blockade in tumors with mismatch-repair deficiency. N Engl J Med.
373:19792015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Garon EB, Rizvi NA, Hui R, Leighl N,
Balmanoukian AS, Eder JP, Patnaik A, Aggarwal C, Gubens M, Horn L,
et al: Pembrolizumab for the treatment of non-small-cell lung
cancer. N Engl J Med. 372:2018–2028. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Van Allen EM, Miao D, Schilling B, Shukla
SA, Blank C, Zimmer L, Sucker A, Hillen U, Foppen MHG, Goldinger
SM, et al: Genomic correlates of response to CTLA-4 blockade in
metastatic melanoma. Science. 350:207–211. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bremnes RM, Busund LT, Kilvaer TL,
Andersen S, Richardsen E, Paulsen EE, Hald S, Khanehkenari MR,
Cooper WA, Kao SC and Dønnem T: The role of tumor-infiltrating
lymphocytes in development, progression, and prognosis of non-small
cell lung cancer. J Thorac Oncol. 11:789–800. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rooney MS, Shukla SA, Wu CJ, Getz G and
Hacohen N: Molecular and genetic properties of tumors associated
with local immune cytolytic activity. Cell. 160:48–61. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hu Y, Gaedcke J, Emons G, Beissbarth T,
Grade M, Jo P, Yeager M, Chanock SJ, Wolff H, Camps J, et al:
Colorectal cancer susceptibility loci as predictive markers of
rectal cancer prognosis after surgery. Genes Chromosomes Cancer.
57:140–149. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tripathi MK, Deane NG, Zhu J, An H, Mima
S, Wang X, Padmanabhan S, Shi Z, Prodduturi N, Ciombor KK, et al:
Nuclear factor of activated T-cell activity is associated with
metastatic capacity in colon cancer. Cancer Res. 74:6947–6957.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Allen WL, Dunne PD, McDade S, Scanlon E,
Loughrey M, Coleman H, McCann C, McLaughlin K, Nemeth Z, Syed N, et
al: Transcriptional subtyping and CD8 immunohistochemistry
identifies poor prognosis stage II/III colorectal cancer patients
who benefit from adjuvant chemotherapy. JCO Precis Oncol.
2018:2018.
|
|
25
|
Thorsson V, Gibbs DL, Brown SD, Wolf D,
Bortone DS, Ou Yang TH, Porta-Pardo E, Gao GF, Plaisier CL, Eddy
JA, et al: The immune landscape of cancer. Immunity.
48:812–830.e14. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Gaujoux R and Seoighe C: A flexible R
package for nonnegative matrix factorization. BMC Bioinformatics.
11:3672010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gao Y and Church G: Improving molecular
cancer class discovery through sparse non-negative matrix
factorization. Bioinformatics. 21:3970–3975. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Devarajan K: Nonnegative matrix
factorization: An analytical and interpretive tool in computational
biology. PLoS Comput Biol. 4:e10000292008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Jiang P, Gu S, Pan D, Fu J, Sahu A, Hu X,
Li Z, Traugh N, Bu X, Li B, et al: Signatures of T cell dysfunction
and exclusion predict cancer immunotherapy response. Nat Med.
24:1550–1558. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Newman AM, Liu CL, Green MR, Gentles AJ,
Feng W, Xu Y, Hoang CD, Diehn M and Alizadeh AA: Robust enumeration
of cell subsets from tissue expression profiles. Nat Methods.
12:453–457. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Love MI, Huber W and Anders S: Moderated
estimation of fold change and dispersion for RNA-seq data with
DESeq2. Genome Biol. 15:5502014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ritchie ME, Phipson B, Wu D, Hu Y, Law CW,
Shi W and Smyth GK: limma powers differential expression analyses
for RNA-sequencing and microarray studies. Nucleic Acids Res.
43:e472015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Liberzon A, Subramanian A, Pinchback R,
Thorvaldsdottir H, Tamayo P and Mesirov JP: Molecular signatures
database (MSigDB) 3.0. Bioinformatics. 27:1739–1740. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Schrock AB, Ouyang C, Sandhu J, Sokol E,
Jin D, Ross JS, Miller VA, Lim D, Amanam I, Chao J, et al: Tumor
mutational burden is predictive of response to immune checkpoint
inhibitors in MSI-high metastatic colorectal cancer. Ann Oncol.
30:1096–1103. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Birkbak NJ, Kochupurakkal B, Izarzugaza
JM, Eklund AC, Li Y, Liu J, Szallasi Z, Matulonis UA, Richardson
AL, Iglehart JD and Wang ZC: Tumor mutation burden forecasts
outcome in ovarian cancer with BRCA1 or BRCA2 mutations. PLoS One.
8:e800232013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zeng Z, Vo AH, Mao C, Clare SE, Khan SA
and Luo Y: Cancer classification and pathway discovery using
non-negative matrix factorization. J Biomed Inform. 96:1032472019.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Yang Z and Michailidis G: A non-negative
matrix factorization method for detecting modules in heterogeneous
omics multi-modal data. Bioinformatics. 32:1–8. 2016.PubMed/NCBI
|
|
38
|
Eng SWM, Aeschlimann FA, van Veenendaal M,
Berard RA, Rosenberg AM, Morris Q and Yeung RSM; ReACCh-Out
Research Consortium, : Patterns of joint involvement in juvenile
idiopathic arthritis and prediction of disease course: A
prospective study with multilayer non-negative matrix
factorization. PLoS medicine. 16:e10027502019. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Carbone DP, Reck M, Paz-Ares L, Creelan B,
Horn L, Steins M, Felip E, van den Heuvel MM, Ciuleanu TE, Badin F,
et al: First-line nivolumab in stage IV or recurrent non-small-cell
lung cancer. N Engl J Med. 376:2415–2426. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Hellmann MD, Ciuleanu TE, Pluzanski A, Lee
JS, Otterson GA, Audigier-Valette C, Minenza E, Linardou H, Burgers
S, Salman P, et al: Nivolumab plus ipilimumab in lung cancer with a
high tumor mutational burden. N Engl J Med. 378:2093–2104. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yarchoan M, Hopkins A and Jaffee EM: Tumor
mutational burden and response rate to PD-1 inhibition. N Engl J
Med. 377:2500–2501. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Billingsley CC, Cohn DE, Mutch DG,
Stephens JA, Suarez AA and Goodfellow PJ: Polymerase ε (POLE)
mutations in endometrial cancer: Clinical outcomes and implications
for Lynch syndrome testing. Cancer. 121:386–394. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Gridelli C, Ardizzoni A, Barberis M,
Cappuzzo F, Casaluce F, Danesi R, Troncone G and De Marinis F:
Predictive biomarkers of immunotherapy for non-small cell lung
cancer: Results from an Experts Panel Meeting of the Italian
Association of Thoracic Oncology. Transl Lung Cancer Res.
6:373–386. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kudryavtseva AV, Lukyanova EN, Kalinin DV,
Zaretsky AR, Pokrovsky AV, Golovyuk AL, Fedorova MS, Pudova EA,
Kharitonov SL, Pavlov VS, et al: Mutational load in carotid body
tumor. BMC Med Genomics. 12 (Suppl 2):S392019. View Article : Google Scholar
|
|
45
|
Narayanan S, Kawaguchi T, Peng X, Qi Q,
Liu S, Yan L and Takabe K: Tumor infiltrating lymphocytes and
macrophages improve survival in microsatellite unstable colorectal
cancer. Sci Rep. 9:134552019. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Mirjolet C, Charon-Barra C, Ladoire S,
Arbez-Gindre F, Bertaut A, Ghiringhelli F, Leroux A, Peiffert D,
Borg C, Bosset JF and Créhange G: Tumor lymphocyte immune response
to preoperative radiotherapy in locally advanced rectal cancer: The
LYMPHOREC study. Oncoimmunology. 7:e13964022018. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Glaire MA, Domingo E, Sveen A, Bruun J,
Nesbakken A, Nicholson G, Novelli M, Lawson K, Oukrif D, Kildal W,
et al: Tumour-infiltrating CD8(+) lymphocytes and colorectal cancer
recurrence by tumour and nodal stage. Br J Cancer. 121:474–482.
2019. View Article : Google Scholar : PubMed/NCBI
|