Introduction
Liver cancer (LC), the third leading cause of
cancer-associated mortality and the sixth most common cancer
worldwide in 2016, represents a global health problem (1). The majority of patients with LC are
diagnosed at advanced stages due to the insidious developmental
process (2). Curative therapies such
as resection or transplantation are not suitable for patients with
advanced stage LC, and advanced LCs are resistant to the majority
of standard chemotherapeutic regimens (3). Therefore, the overall survival (OS) of
patients with LC is dismal, with a five-year survival rate of
<15% in USA (3–5). Therefore, current research efforts are
directed towards the discovery of biomarkers for early diagnosis,
recognition of molecular subclasses of LC, correlation of molecular
signatures with radiological/histological features,
characterization of new therapeutic targets and personalization of
therapies based on an individual's tumor biology (6). Further investigations into the
mechanisms of carcinogenesis and development of LC are essential to
achieve these goals.
In the past few decades, intensive investigations
have focused on the role of protein-coding genes in the
pathogenesis of LC (7–10). However, only 2% of the human genome
is transcribed into protein-coding mRNAs, whereas 70–80% of the
genome is actively transcribed into non-coding RNAs (11,12).
Long non-coding RNAs (lncRNAs) are the non-coding RNAs, >200
nucleotides in length, without protein-coding ability (13). Accumulating evidence has suggested
that lncRNAs affect all essential processes in living cells,
including chromatin condensation, replication, transcription,
splicing, and translational and post-translational modification of
proteins and constituting the most abundant part of the transcribed
genome (14). In addition, a number
of lncRNAs have been discovered since the discovery and
characterization of the first lncRNA H19, in 1991 (15). In addition, current evidence has
identified lncRNAs as key regulators of cancer signaling networks
and characteristic cancer behaviors (16). Some lncRNAs, such as H19, HOX
transcript antisense intergenic RNA, metastasis associated lung
adenocarcinoma transcript 1 and lncRNA associated with
microvascular invasion in HCC, were suggested to be dysregulated in
LC and may serve as prognostic markers and therapeutic targets in
patients with LC (6,15,17–21).
However, the clinical significance and functional role of breast
cancer anti-estrogen resistance 4 (BCAR4) in LC have not yet been
reported.
The present study aimed to investigate the
expression levels of BCAR4 in LC cells and tissues. Furthermore,
the clinical significance of BCAR4 in LC was explored, and its
prognostic value was investigated, with the purpose of evaluating
the functional role of BCAR4 in LC cells.
Materials and methods
Collection of clinical specimens and
follow-up
Tumor tissues and paired normal adjacent tissues
were collected from 188 patients with LC (65 males and 35 females;
median age, 62.3 years; range, 39–86 years), who underwent surgical
resection between April 2011 and May 2014 at The Jiangxi Provincial
People's Hospital Affiliated with Nanchang University (Nanchang,
China). Adjacent tissues were obtained ≥2 cm away from the border
of tumor tissues. The final diagnosis of patients was confirmed by
pathology. None of the patients received preoperative chemotherapy,
radiotherapy or other anticancer treatments. The specimens were
collected immediately following surgical resection, and the
collected tissues were frozen in liquid nitrogen and stored at
−80°C until further use. The clinicopathological characteristics of
the patients analyzed in the present study included details of age,
sex, serum α-fetoprotein (AFP) level, alcoholism, hepatitis B virus
(HBV) infection, liver cirrhosis, differentiation grade (American
Joint Committee on Cancer) (22),
tumor size, encapsulation, number of tumors, lymph-vascular space
invasion (LVSI), and Tumor-Node-Metastasis (TNM) stage (American
Joint Committee on Cancer) (22).
Written informed consent was obtained from each patient and the
present study was approved by The Ethnic Committee of Jiangxi
Provincial People's Hospital Affiliated with Nanchang
University.
Follow-up was performed by telephone interview and
questionnaire every 3 months. The deadline of the follow-up was
June 2017. OS was defined as the time interval between the date of
diagnosis and the end of the follow-up, or the date at which the
patient succumbed to the disease. Progression-free survival (PFS)
was defined as the interval between the date of surgery and
recurrence; if recurrence was not diagnosed, the patients were
censored on the date of death or the last follow-up.
Cell culture and transfection
Liver cancer cell lines (HuH-6, Hep3B, HuH-7, HepG2,
and HuH-1) were purchased from The Cell Bank of Type Culture
Collection of the Chinese Academy of Sciences. HuH-6 and HuH-1 were
cultured in RPMI-1640 medium (Invitrogen; Thermo Fisher Scientific,
Inc.), whereas Hep3B, HuH-7 and HepG2 were cultured in DMEM
(Invitrogen; Thermo Fisher Scientific, Inc.) supplemented with 10%
FBS (Thermo Fisher Scientific, Inc.), 100 U/ml penicillin and 100
mg/ml streptomycin (Thermo Fisher Scientific, Inc.) in a humidified
atmosphere containing 5% CO2 at 37°C.
The BCAR4 expression vector (pcDNA3.1-BCAR4), a
negative control vector (pcDNA3.1-Vector), specific small
interfering RNAs (siRNAs) targeting BCAR4 (siBCAR4-1 and siBCAR4-2;
cat. no. A01002) and a scrambled negative control (siNC; cat. no.
A06001) were purchased from Shanghai GenePharma Co., Ltd,. The
overexpression and silencing of BCAR4 were conducted using
pcDNA3.1-BCAR4 (800 ng) and the siRNAs (siBCAR4-1 and siBCAR4-2; 50
nM), respectively. Transfection was performed using the
Lipofectamine® 2000 reagent (Thermo Fisher Scientific
Inc.) according to the manufacturer's instructions. Cells were
subjected to subsequent experimentation 48 h following
transfection.
Reverse transcription-quantitative PCR
assay (RT-qPCR)
Total RNA from the tissue samples and the
transfected cells were extracted using the TRIzol reagent
(Invitrogen; Thermo Fisher Scientific, Inc.) according to the
manufacturer's protocol. The concentration and purity of RNA were
determined by measuring its optical density (OD) using a NanoDrop
2000 spectrophotometer (1.8<A260/280<2.0; Thermo Fisher
Scientific, Inc.). Total RNA (1 µg) was reverse transcribed in a
final volume of 20 µl, under standard conditions (37°C for 15 min,
then 85°C for 5 sec), using PrimeScript RT Reagent kit (Takara
Biotechnology Co., Ltd.). qPCR was performed using an ABI PRISM
7000 Fluorescent Quantitative PCR system (Applied Biosystems;
Thermo Fisher Scientific, Inc.) according to the manufacturer's
protocols. Briefly, reactions were loaded onto a 96-well plate in
triplicate and the thermocycling conditions used were: 95°C For 5
min; followed by 40 cycles of denaturation at 95°C for 30 sec, 1
min of annealing at 60°C and extension at 60°C for 1 min. The
average value of triplicate samples was used to calculate the
relative expression of BCAR4 using the 2−ΔΔCq method
(23). The experiments were repeated
at least three times. The primer sequences were as follows: BCAR4
forward, 5′-TACAACCACTGCACTACCTG-3′ and reverse,
5′-TGGAATGCTTGAAGGCTGCT-3′; and GAPDH, forward,
5′-CGCTCTCTGCTCCTCCTGTTC-3′ and reverse,
5′-ATCCGTTGACTCCGACCTTCAC-3′. GAPDH was used as the internal
control.
MTT and colony-formation assays
A Cell Proliferation Reagent kit I (MTT) (Roche
Diagnostics) was used to assess cell proliferation. Transfected
cells (2×103 per well) were plated in each well of a
96-well plate, dimethyl sulfoxide was used to dissolve the purple
formazan, and the optical density was assessed at specific time
points (0, 24, 48, 72, and 96 h) at a wavelength of 490 nm,
according to the manufacturer's protocol.
For the colony-formation assay, each well in a
6-well culture plate was seeded with 1×103 cells and
cultured for 7 days in DMEM (Invitrogen; Thermo Fisher Scientific,
Inc.) supplemented with 10% FBS, 100 U/ml penicillin and 100 mg/ml
streptomycin (all Thermo Fisher Scientific, Inc.). Subsequently,
the adherent cells were washed with PBS, fixed with 10%
paraformaldehyde for 10 min at room temperature and stained with 1%
crystal violet for 5 min at room temperature. Images of culture
plates were captured using a light microscope (magnification, ×40),
and the number of colonies was counted. Triplicate wells were
measured in each treatment group.
Transwell migration and invasion
assays
After 48 h of transfection, cells (1×105)
were resuspended in fresh medium (200 µl) and added to the upper
side of a Transwell chamber (8-µm pore size; BD Biosciences),
uncoated (for the Transwell migration assay) or coated (for the
Matrigel invasion assay) with 50 µl Matrigel (BD Biosciences).
Medium (700 µl) containing 20% FBS was added to the lower chamber.
After 24 h of incubation, the cells remaining on the upper membrane
were removed using cotton wool. The migrated/invaded cells on the
bottom side of the chamber were fixed with 4% paraformaldehyde for
30 min at room temperature and stained with Giemsa (Beijing
Zhongsheng Ruitai Technology Co., Ltd.; 1:10 dilution) for 30 min
at room temperature. Cell numbers were counted in 5 random fields
of each chamber under the light microscope (magnification,
×40).
Statistical analysis
All statistical analyses were performed using SPSS
version 20.0 (IBM Corp.). The χ2 test and Student's
t-test were performed to examine the associations between BCAR4
expression level and clinical characteristics. Paired and unpaired
Student's t-test were used to compare the difference between paired
and independent samples, respectively. A one-way ANOVA with a
post-hoc Dunnett's test was used to detect differences between
multiple groups. The survival curves were plotted using the
Kaplan-Meier method and a log-rank test was used to evaluate the
differences between the survival curves. Hazard ratio (HR) and 95%
confidence interval (95% CI) values were calculated using a Cox
proportional hazard regression model to evaluate the association
between BCAR4 expression and OS/PFS. Variables with a value of
P<0.05 in univariate analysis were subjected to multivariate
analysis on the basis of Cox regression analyses. P<0.05 was
considered to indicate a statistically significant difference.
Results
BCAR4 is overexpressed in LC and is
associated with cancer progression
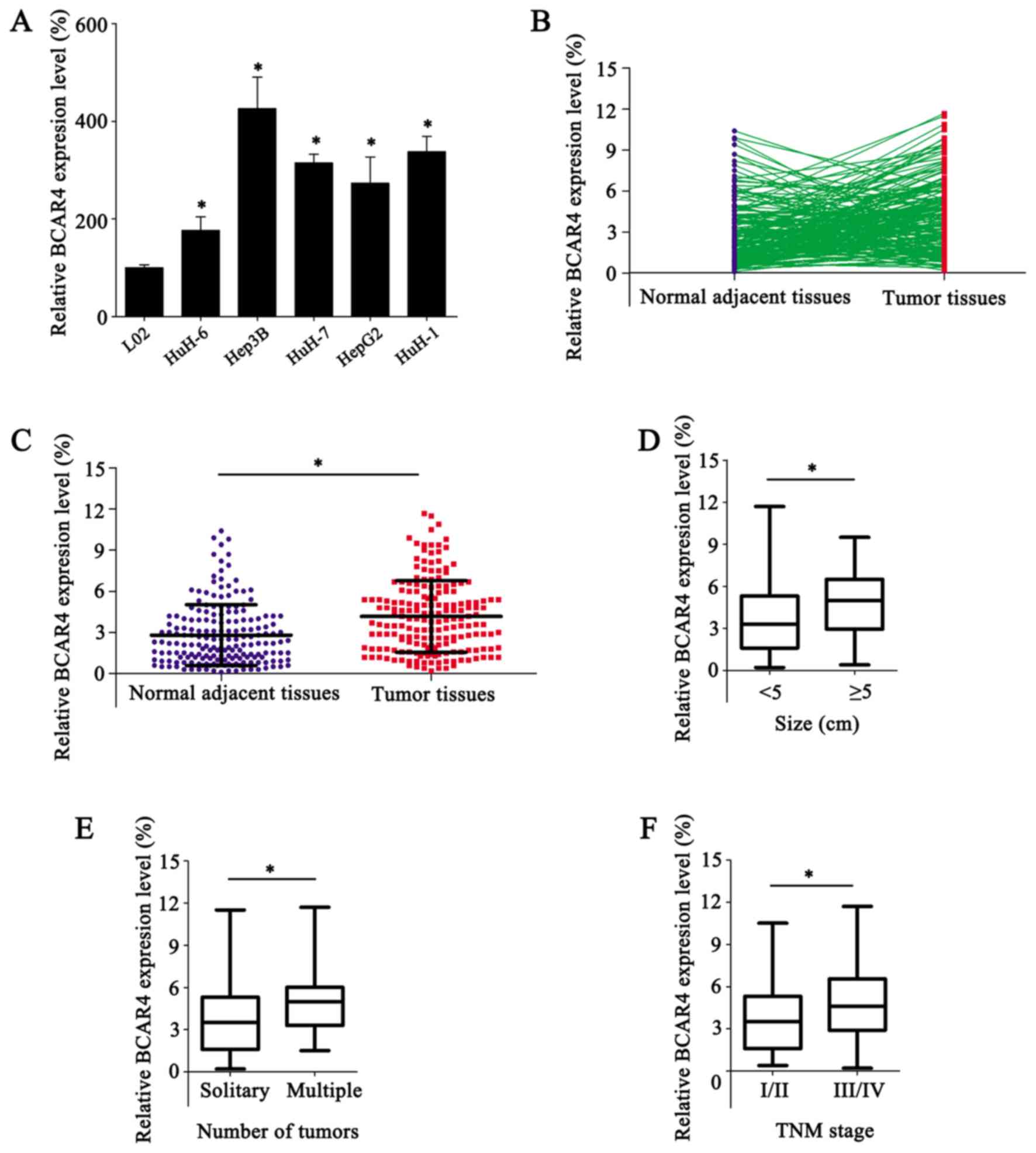
Determining the expression levels of lncRNAs is a
pivotal aspect in analyzing their potential role in cancer. In
order to investigate the functional role of BCAR4 in LC, its
expression levels in five LC cell lines (HuH-6, Hep3B, HuH-7, HepG2
and HuH-1) were measured by RT-qPCR. BCAR4 displayed varying
expression levels in LC cells; Hep3B cells exhibited the highest
expression level of the 4 LC cell lines, while HepG2 cells
expressed the lowest levels, and the difference in expression
between the aforementioned cell lines was significant (Fig. 1A). The expression of BCAR4 was
detected in 188 LC tissues and paired normal adjacent tissues
(Fig. 1B). LC tissues exhibited
significantly higher levels of BCAR4 expression compared with the
paired normal adjacent tissues (P<0.05; Fig. 1C). Additionally, patients with tumor
sizes ≥5 cm, multiple tumors and advanced TNM stages (III/IV)
showed significantly higher expression levels of BCAR4 compared
with those with tumor size <5 cm (P<0.05; Fig. 1D), solitary tumors (P<0.05;
Fig. 1E) and less advanced TNM
stages (I/II) (P<0.05; Fig. 1F),
respectively.
In order to determine the clinical significance of
BCAR4 in LC, patients were divided into a low-BCAR4 expression
group (n=100) and a high-BCAR4 expression group (n=88). The average
BCAR4 expression level was used as the cut-off value. The
association between BCAR4 expression levels and the
clinicopathological characteristics of LC was statistically
analyzed. Higher levels of BCAR4 expression were associated with
the presence of multiple tumors and advanced TNM stages (III/IV)
(Table I). Overall, high BCAR4
expression is associated with the clinical progression of LC.
 | Table I.Association between BCAR4 expression
and clinicopathological characteristics of hepatocellular
carcinoma. |
Table I.
Association between BCAR4 expression
and clinicopathological characteristics of hepatocellular
carcinoma.
|
| No. of
patients |
|
|---|
|
|
|
|
|---|
| Parameters | Low BCAR4
expression, n=100 | High BCAR4
expression, n=88 | P-value |
|---|
| Age, years |
|
| 0.970 |
|
<55 | 52 | 46 |
|
|
≥55 | 48 | 42 |
|
| Sex |
|
| 0.137 |
|
Male | 65 | 66 |
|
|
Female | 35 | 22 |
|
| AFP, ng/ml |
|
| 0.862 |
|
<20 | 51 | 46 |
|
|
≥20 | 49 | 42 |
|
| Alcoholism |
|
| 0.586 |
|
Negative | 46 | 37 |
|
|
Positive | 54 | 51 |
|
| HBV |
|
| 0.974 |
|
Negative | 18 | 16 |
|
|
Positive | 82 | 72 |
|
| Liver
cirrhosis |
|
| 0.505 |
|
Present | 44 | 43 |
|
|
Absent | 56 | 45 |
|
| Differentiation
grade |
|
| 0.320 |
| Well +
moderate | 62 | 58 |
|
|
Poor | 38 | 30 |
|
| Tumor size, cm |
|
| 0.089 |
|
<5 | 73 | 54 |
|
| ≥5 | 27 | 34 |
|
| Encapsulation |
|
| 0.784 |
| No | 48 | 44 |
|
|
Complete | 52 | 44 |
|
| Number of
tumors |
|
| 0.029 |
|
Solitary | 81 | 59 |
|
|
Multiple | 19 | 29 |
|
| LVSI |
|
| 0.122 |
|
Present | 41 | 46 |
|
|
Absent | 59 | 42 |
|
| TNM stage |
|
| 0.020 |
|
I/II | 75 | 52 |
|
|
III/IV | 25 | 36 |
|
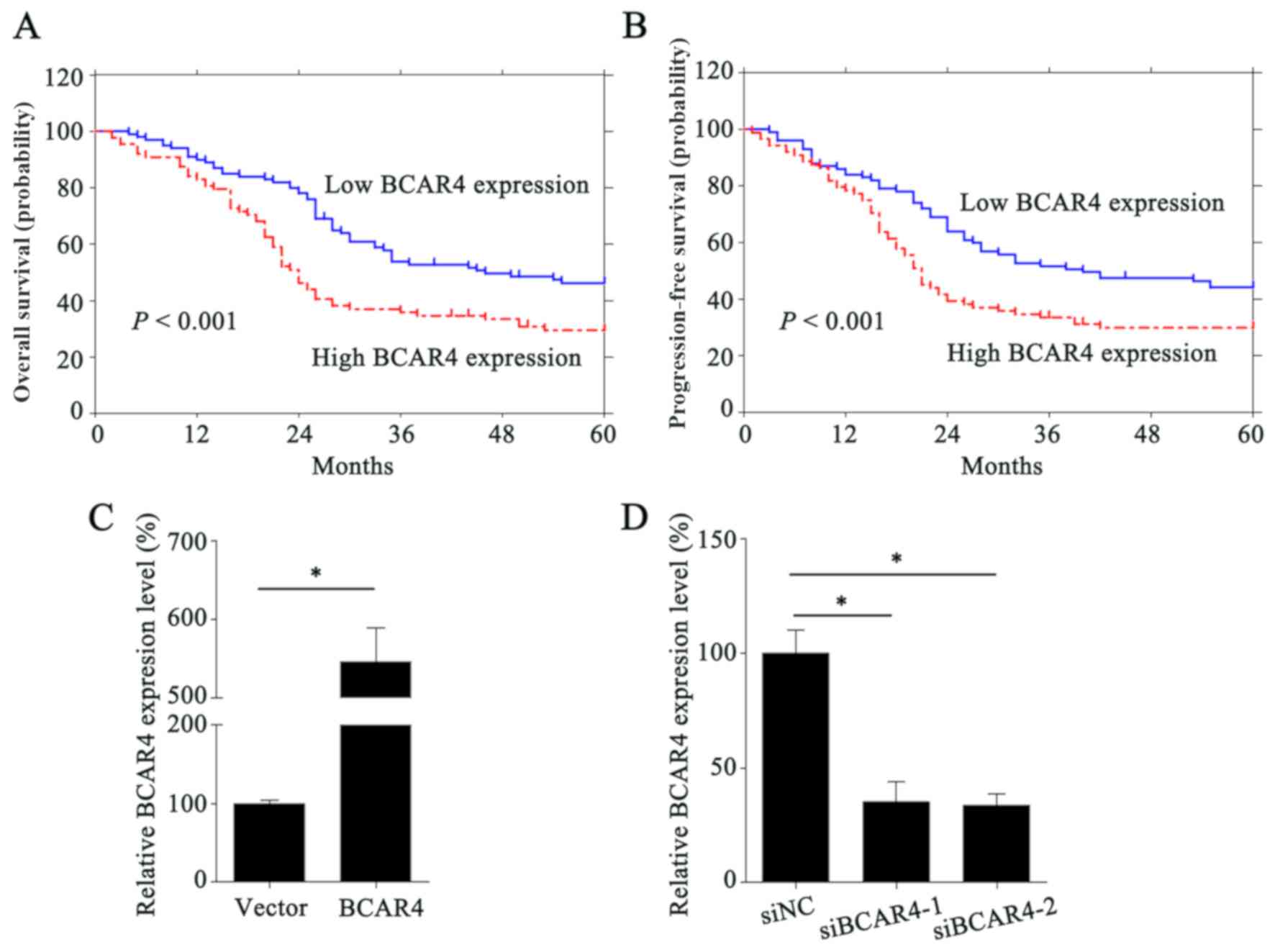
High BCAR4 expression predicts poor
prognosis in LC
A lack of prognostic markers with adequate
efficiency and efficacy complicates individualized therapeutic
regimens in clinical practice. The present study evaluated the
prognostic value of high BCAR4 expression in LC. Patients with high
BCAR4 expression exhibited poorer OS time (P<0.01; Fig. 2A) and PFS time (P<0.01; Fig. 2B) compared with patients with low
BCAR4 expression.
Univariate analysis and multivariate analysis were
performed to identify the risk factors of poor OS. Five parameters
(tumor size ≥5 cm, multiple tumors, presence of LVSI, TNM stages
III/IV and high BCAR4 expression) were shown to be risk factors of
poor OS and PFS in the univariate analysis (Table II). Further analysis of these
factors using multivariate analysis found that the presence of LVSI
(P=0.001; HR, 1.943; 95% CI, 1.319–2.862), TNM stages III/IV
(P<0.001; HR, 3.418; 95% CI, 2.156–5.420) and high BCAR4
expression (P=0.002; HR, 1.126; 95% CI, 1.046–1.212,) were
independent risk factors of poor OS (Table III). In addition, the presence of
LVSI (P<0.001; HR, 2.009; 95% CI, 1.372–2.941), TNM stage III/IV
(P<0.001; HR, 3.253; 95% CI, 2.061–5.137) and high BCAR4
expression (P=0.007; HR, 1.105; 95% CI, 1.027–1.189) were also
demonstrated to be independent risk factors of poor PFS (Table III). Collectively, high BCAR4
expression predicts poor prognosis and serves as an independent
risk factor of poor OS and PFS in LC.
| Table II.Univariate analysis of
clinicopathological features, OS and PFS of hepatocellular
carcinoma patients. |
Table II.
Univariate analysis of
clinicopathological features, OS and PFS of hepatocellular
carcinoma patients.
|
| OS | PFS |
|---|
|
|
|
|
|---|
| Parameters | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years (≥55 vs.
<55) | 1.373 | 0.950–1.984 | 0.092 | 1.332 | 0.925–1.918 | 0.124 |
| Sex (male vs.
female) | 1.011 | 0.679–1.505 | 0.959 | 1.061 | 0.718–1.568 | 0.767 |
| AFP, ng/ml (<20
vs. ≥20) | 1.127 | 0.780–1.628 | 0.523 | 1.148 | 0.798–1.652 | 0.458 |
| Alcoholism
(negative vs. positive) | 1.179 | 0.813–1.710 | 0.386 | 1.197 | 0.827–1.732 | 0.341 |
| HBV (negative vs.
positive) | 1.045 | 0.639–1.711 | 0.860 | 0.957 | 0.596–1.535 | 0.855 |
| Liver cirrhosis
(present vs. absent) | 1.082 | 0.749–1.563 | 0.674 | 1.074 | 0.746–1.547 | 0.699 |
| Differentiation
grade (poor vs. well + moderate) | 0.865 | 0.58–1.271 | 0.461 | 0.833 | 0.568–1.222 | 0.350 |
| Tumor size, cm (≥5
vs. <5) | 1.623 | 1.109–2.374 | 0.013 | 1.587 | 1.087–2.316 | 0.017 |
| Encapsulation (no
vs. complete) | 1.257 | 0.870–1.817 | 0.224 | 1.287 | 0.893–1.855 | 0.177 |
| No. of tumors
(multiple vs. solitary) | 1.986 | 1.333–2.957 | 0.001 | 1.934 | 1.301–2.876 | 0.001 |
| LVSI (present vs.
absent) | 2.036 | 1.401–2.959 | <0.001 | 2.087 | 1.441–3.023 | <0.001 |
| TNM stage (III/IV
vs. I/II) | 3.333 | 2.289–4.853 | <0.001 | 3.165 | 2.181–4.593 | <0.001 |
| BCAR4 (high vs.
low) | 1.157 | 1.076–1.244 | <0.001 | 1.138 | 1.059–1.223 | <0.001 |
| Table III.Multivariate analysis of
clinicopathologic features and OS and PFS of patients with
hepatocellular carcinoma. |
Table III.
Multivariate analysis of
clinicopathologic features and OS and PFS of patients with
hepatocellular carcinoma.
|
| OS | PFS |
|---|
|
|
|
|
|---|
| Parameters | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Tumor size, cm (≥5
vs. <5) | 0.889 | 0.554–1.427 | 0.626 | 0.889 | 0.556–1.421 | 0.622 |
| No. of tumors
(multiple vs. solitary) | 0.836 | 0.491–1.423 | 0.509 | 0.857 | 0.506–1.450 | 0.564 |
| LVSI (present vs.
absent) | 1.943 | 1.319–2.862 | 0.001 | 2.009 | 1.372–2.941 | <0.001 |
| TNM stage (III/IV
vs. I/II) | 3.418 | 2.156–5.420 | <0.001 | 3.253 | 2.061–5.137 | <0.001 |
| BCAR4 (high vs.
low) | 1.126 | 1.046–1.212 | 0.002 | 1.105 | 1.027–1.189 | 0.007 |
BCAR4 promotes proliferation,
migration and invasion in LC
HuH-6 and Hep3B cells had the lowest and highest
BCAR4 expression levels among the 5 LC cell lines used in this
study, respectively (Fig. 1A). BCAR4
was ectopically overexpressed in HuH-6 cells (Fig. 2C) and silenced in Hep3B cells
(Fig. 2D) for the functional assays.
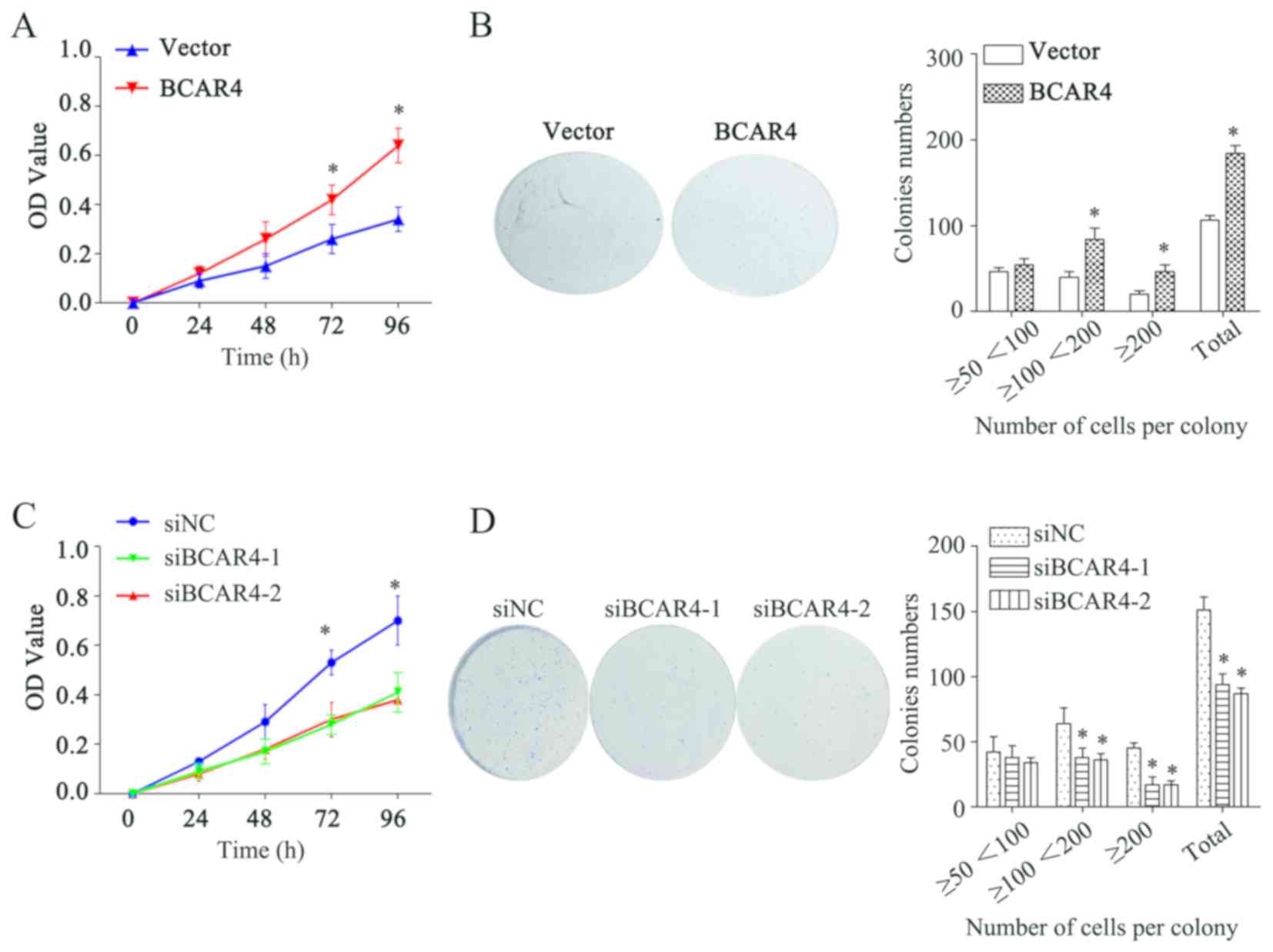
The proliferative abilities of LC cells with BCAR4 overexpression
and knockdown were evaluated using MTT and colony-formation assays.
Overexpression of BCAR4 resulted in increased OD values after 72
and 96 h (P<0.05; Fig. 3A) and
number of colonies (P<0.05; Fig.
3B) in HuH-6 cells compared with the empty vector control;
whereas BCAR4 knockdown significantly decreased the OD value
(P<0.05; Fig. 3C) and the colony
number (P<0.05; Fig. 3D) in Hep3B
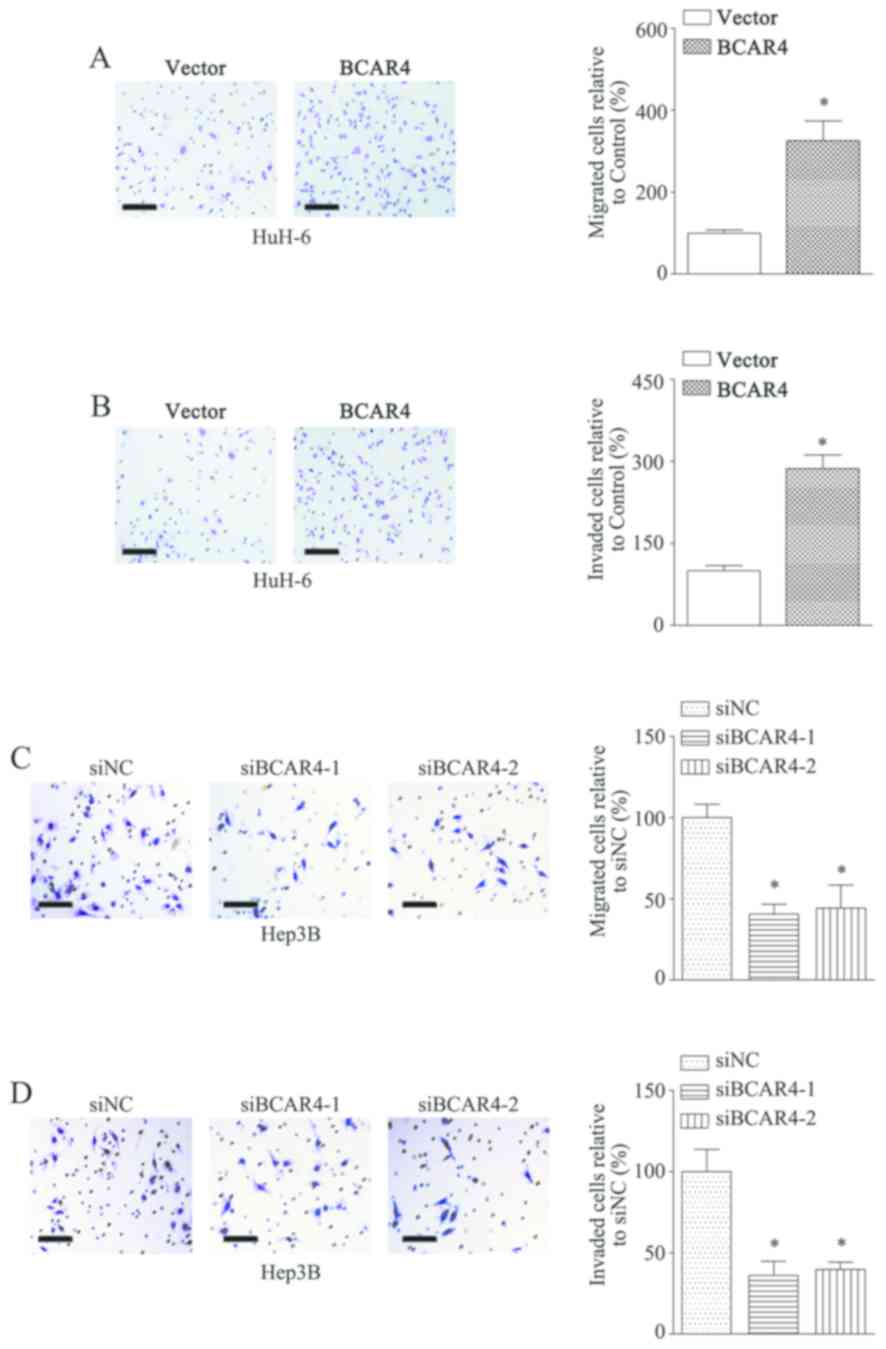
cells compared with siNC transfected cells. Moreover,
overexpression of BCAR4 in HuH-6 cells significantly promoted
migration (P<0.05; Fig. 4A) and
invasion (P<0.05; Fig. 4B)
compared with the empty vector control. Knockdown of BCAR4 in Hep3B
cells resulted in reduced migration (P<0.05; Fig. 4C) and invasion (P<0.05; Fig. 4D) compared with cells transfected
with siNC. Overall, these results suggest that BCAR4 promotes the
proliferation, migration and invasion of LC cells.
Discussion
Several canonical signaling pathways have been
indicated to mediate lncRNA-regulated behaviors in LC, such as Wnt
signaling (24,25) and STAT3 signaling (26–29). In
addition, lncRNAs are involved in the determination and maintenance
of hepatic cancer stem cell characteristics (30,31) and
the regulation of epithelial-to-mesenchymal transition (32–34).
Furthermore, one study evaluated lncRNAs alone and in combination
as candidate biomarkers for LC diagnosis, with reported
sensitivities ranging from 91.4 to 92.7% and specificity ranging
from 82.1 to 88.6% (18). lncRNAs
have been considered as potential early diagnostic biomarkers in LC
(35,36). Additionally, some studies suggested
that lncRNAs may be potential therapeutic targets in LC, owing to
their tissue-specific expression patterns (19,37–39).
Therefore, lncRNAs serve pivotal roles in LC biology and may shed
new light on the early diagnosis and therapy for patients with
LC.
In 2006, BCAR4 expression was first found to
positively correlate with tamoxifen resistance, and ectopic
expression of BCAR4 was shown to induce anti-estrogen resistance
and anchorage-independent transformation of breast cancer (40); and this result was confirmed by
additional studies (41–43). Further investigations performed by
Godinho et al (44) found
that BCAR4-positive breast tumors were driven by homologue
2/homologue 3 signaling. Therefore, BCAR4 was regarded as a
suitable target for treating anti-estrogen-resistant breast cancer
(42,43). In addition, the oncogenic role of
BCAR4 has been defined in osteosarcoma (45), colorectal cancer (46), non-small cell lung cancer (47), chondrosarcoma (48), gastric cancer (49) and glioma (50). Studies have revealed that BCAR4
promotes cancer progression through a number of mechanisms, such as
increasing the metastatic behaviors of cells, proliferation,
chemoresistance and epithelial-to-mesenchymal transition (45,47–50).
Several signaling pathways, such as Wnt signaling and mTOR
signaling, have been shown to mediate the functional role of BCAR4
in accelerating cancer progression (48,51). The
prognostic value of BCAR4 upregulation was reported in
osteosarcoma, gastric cancer and colorectal cancer (45,46,49).
These findings lay a foundation for utilizing BCAR4 as a prognostic
marker and therapeutic target in different types of cancer.
However, the detailed mechanisms underlying the oncogenic functions
of BCAR4 in LC are yet to be elucidated. Besides, the samples used
in the present study were collected from a single medical center
and the population size was limited; thus, more samples from
multiple sources need to be analyzed to validate the present
results.
The present study verified the upregulation of BCAR4
in LC, and its association with LC progression. Statistical
analysis demonstrated that high BCAR4 expression indicated poor OS
and PFS times. Furthermore, Cox regression analyses revealed high
BCAR4 expression as an independent risk factor of poor OS and PFS.
Furthermore, in vitro assays validated the effects of BCAR4
in promoting LC proliferation, migration and invasion. The present
study indicates the potential of BCAR4 as a prognostic biomarker in
LC.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZZ and AW designed the study and revised the
manuscript. JM, ZZ AW and HL performed the experiments. JM and HL
drafted the manuscript. JM and CL performed statistical analysis of
the data and conducted follow-up of the patients. All authors
approved the final manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from each
patient and the present study was approved by The Ethnic Committee
of Jiangxi Provincial People's Hospital Affiliated with Nanchang
University.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2016. CA Cancer J Clin. 66:7–30. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ayoub WS, Steggerda J, Yang JD, Kuo A,
Sundaram V and Lu SC: Current status of hepatocellular carcinoma
detection: Screening strategies and novel biomarkers. Ther Adv Med
Oncol. 11:17588359198691202019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Altekruse SF, McGlynn KA and Reichman ME:
Hepatocellular carcinoma incidence, mortality, and survival trends
in the United States from 1975 to 2005. J Clin Oncol. 27:1485–1491.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Alqahtani A, Khan Z, Alloghbi A, Said
Ahmed TS, Ashraf M and Hammouda DM: Hepatocellular carcinoma:
Molecular mechanisms and targeted therapies. Medicina (Kaunas).
55:E5262019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Golabi P, Fazel S, Otgonsuren M, Sayiner
M, Locklear CT and Younossi ZM: Mortality assessment of patients
with hepatocellular carcinoma according to underlying disease and
treatment modalities. Medicine (Baltimore). 96:e59042017.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dhanasekaran R, Venkatesh SK, Torbenson MS
and Roberts LR: Clinical implications of basic research in
hepatocellular carcinoma. J Hepatol. 64:736–745. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cheng H, Sun G, Chen H and Li Y, Han Z and
Li Y, Zhang P, Yang L and Li Y: Trends in the treatment of advanced
hepatocellular carcinoma: Immune checkpoint blockade immunotherapy
and related combination therapies. Am J Cancer Res. 9:1536–1545.
2019.PubMed/NCBI
|
|
8
|
Kumari R, Sahu MK, Tripathy A, Uthansingh
K and Behera M: Hepatocellular carcinoma treatment: Hurdles,
advances and prospects. Hepat Oncol. 5:HEP082018. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Neureiter D, Stintzing S, Kiesslich T and
Ocker M: Hepatocellular carcinoma: Therapeutic advances in
signaling, epigenetic and immune targets. World J Gastroenterol.
25:3136–3150. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Villanueva A: Hepatocellular carcinoma. N
Engl J Med. 380:1450–1462. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sana J, Faltejskova P, Svoboda M and Slaby
O: Novel classes of non-coding RNAs and cancer. J Transl Med.
10:1032012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
ENCODE Project Consortium, . An integrated
encyclopedia of DNA elements in the human genome. Nature.
489:57–74. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kopp F and Mendell JT: Functional
classification and experimental dissection of long noncoding RNAs.
Cell. 172:393–407. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Huang B and Zhang R: Regulatory non-coding
RNAs: Revolutionizing the RNA world. Mol Biol Rep. 41:3915–3923.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Smekalova EM, Kotelevtsev YV, Leboeuf D,
Shcherbinina EY, Fefilova AS, Zatsepin TS and Koteliansky V: lncRNA
in the liver: Prospects for fundamental research and therapy by RNA
interference. Biochimie. 131:159–172. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bartonicek N, Maag JL and Dinger ME: Long
noncoding RNAs in cancer: Mechanisms of action and technological
advancements. Mol Cancer. 15:432016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Niu ZS, Niu XJ and Wang WH: Long
non-coding RNAs in hepatocellular carcinoma: Potential roles and
clinical implications. World J Gastroenterol. 23:5860–5874. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Klingenberg M, Matsuda A, Diederichs S and
Patel T: Non-coding RNA in hepatocellular carcinoma: Mechanisms,
biomarkers and therapeutic targets. J Hepatol. 67:603–618. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shibata C, Otsuka M, Kishikawa T, Ohno M,
Yoshikawa T, Takata A and Koike K: Diagnostic and therapeutic
application of noncoding RNAs for hepatocellular carcinoma. World J
Hepatol. 7:1–6. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sun J, Bie B, Zhang S, Yang J and Li Z:
Long non-coding RNAs: Critical players in hepatocellular carcinoma.
Int J Mol Sci. 15:20434–20448. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Shi L, Peng F, Tao Y, Fan X and Li N:
Roles of long noncoding RNAs in hepatocellular carcinoma. Virus
Res. 223:131–139. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Amin MB: American Joint Committee on
Cancer Staging Manual. 8th. Springer; New York, NY: pp. 103–111.
2017, PubMed/NCBI
|
|
23
|
Schmittgen TD and Livak KJ: Analyzing
real-time PCR data by the comparative C(T) method. Nat Protoc.
3:1101–1108. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yuan SX, Wang J, Yang F, Tao QF, Zhang J,
Wang LL, Yang Y, Liu H, Wang ZG, Xu QG, et al: Long noncoding RNA
DANCR increases stemness features of hepatocellular carcinoma by
derepression of CTNNB1. Hepatology. 63:499–511. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhu P, Wang Y, Huang G, Ye B, Liu B, Wu J,
Du Y, He L and Fan Z: lnc-β-Catm elicits EZH2-dependent β-catenin
stabilization and sustains liver CSC self-renewal. Nat Struct Mol
Biol. 23:631–639. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yuan JH, Yang F, Wang F, Ma JZ, Guo YJ,
Tao QF, Liu F, Pan W, Wang TT, Zhou CC, et al: A long noncoding RNA
activated by TGF-β promotes the invasion-metastasis cascade in
hepatocellular carcinoma. Cancer Cell. 25:666–681. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zheng Q, Lin Z, Li X, Xin X, Wu M, An J,
Gui X, Li T, Pu H, Li H and Lu D: Inflammatory cytokine IL6
cooperates with CUDR to aggravate hepatocyte-like stem cells
malignant transformation through NF-kB signaling. Sci Rep.
6:368432016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang X, Sun W, Shen W, Xia M, Chen C,
Xiang D, Ning B, Cui X, Li H, Li X, et al: Long non-coding RNA DILC
regulates liver cancer stem cells via IL-6/STAT3 axis. J Hepatol.
64:1283–1294. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lv L, Chen G, Zhou J, Li J and Gong J:
WT1-AS promotes cell apoptosis in hepatocellular carcinoma through
down-regulating of WT1. J Exp Clin Cancer Res. 34:1192015.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wang F, Yuan JH, Wang SB, Yang F, Yuan SX,
Ye C, Yang N, Zhou WP, Li WL, Li W and Sun SH: Oncofetal long
noncoding RNA PVT1 promotes proliferation and stem cell-like
property of hepatocellular carcinoma cells by stabilizing NOP2.
Hepatology. 60:1278–1290. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Guo W and Liu S, Cheng Y, Lu L, Shi J, Xu
G, Li N, Cheng K, Wu M, Cheng S and Liu S: ICAM-1-related noncoding
RNA in cancer stem cells maintains ICAM-1 expression in
hepatocellular carcinoma. Clin Cancer Res. 22:2041–2050. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yang F, Huo XS, Yuan SX, Zhang L, Zhou WP,
Wang F and Sun SH: Repression of the long noncoding RNA-LET by
histone deacetylase 3 contributes to hypoxia-mediated metastasis.
Mol Cell. 49:1083–1096. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang TH, Yu CC, Lin YS, Chen TC, Yeh CT,
Liang KH, Shieh TM, Chen CY and Hsueh C: Long noncoding RNA
CPS1-IT1 suppresses the metastasis of hepatocellular carcinoma by
regulating HIF-1α activity and inhibiting epithelial-mesenchymal
transition. Oncotarget. 7:43588–43603. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Panzitt K, Tschernatsch MM, Guelly C,
Moustafa T, Stradner M, Strohmaier HM, Buck CR, Denk H, Schroeder
R, Trauner M and Zatloukal K: Characterization of HULC, a novel
gene with striking up-regulation in hepatocellular carcinoma, as
noncoding RNA. Gastroenterology. 132:330–342. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Bao H and Su H: Long Noncoding RNAs Act as
novel biomarkers for hepatocellular carcinoma: Progress and
prospects. Biomed Res Int. 2017:60494802017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zheng C, Hao H, Chen L and Shao J: Long
noncoding RNAs as novel serum biomarkers for the diagnosis of
hepatocellular carcinoma: A systematic review and meta-analysis.
Clin Transl Oncol. 19:961–968. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
George J and Patel T: Noncoding RNA as
therapeutic targets for hepatocellular carcinoma. Semin Liver Dis.
35:63–74. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ma L, Chua MS, Andrisani O and So S:
Epigenetics in hepatocellular carcinoma: An update and future
therapy perspectives. World J Gastroenterol. 20:333–345. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Parasramka MA, Maji S, Matsuda A, Yan IK
and Patel T: Long non-coding RNAs as novel targets for therapy in
hepatocellular carcinoma. Pharmacol Ther. 161:67–78. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Meijer D, van Agthoven T, Bosma PT, Nooter
K and Dorssers LC: Functional screen for genes responsible for
tamoxifen resistance in human breast cancer cells. Mol Cancer Res.
4:379–386. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
van Agthoven T, Godinho MF, Wulfkuhle JD,
Petricoin EF 3rd and Dorssers LC: Protein pathway activation
mapping reveals molecular networks associated with antiestrogen
resistance in breast cancer cell lines. Int J Cancer.
131:1998–2007. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Godinho MF, Wulfkuhle JD, Look MP,
Sieuwerts AM, Sleijfer S, Foekens JA, Petricoin EF 3rd, Dorssers LC
and van Agthoven T: BCAR4 induces antioestrogen resistance but
sensitises breast cancer to lapatinib. Br J Cancer. 107:947–955.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Godinho M, Meijer D, Setyono-Han B,
Dorssers LC and van Agthoven T: Characterization of BCAR4, a novel
oncogene causing endocrine resistance in human breast cancer cells.
J Cell Physiol. 226:1741–1749. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Godinho MF, Sieuwerts AM, Look MP, Meijer
D, Foekens JA, Dorssers LC and van Agthoven T: Relevance of BCAR4
in tamoxifen resistance and tumour aggressiveness of human breast
cancer. Br J Cancer. 103:1284–1291. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Ju L, Zhou YM and Yang GS: Up-regulation
of long non-coding RNA BCAR4 predicts a poor prognosis in patients
with osteosarcoma, and promotes cell invasion and metastasis. Eur
Rev Med Pharmacol Sci. 20:4445–4451. 2016.PubMed/NCBI
|
|
46
|
Li Q, Dai Y, Wang F and Hou S:
Differentially expressed long non-coding RNAs and the prognostic
potential in colorectal cancer. Neoplasma. 63:977–983. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Li N, Gao WJ and Liu NS: LncRNA BCAR4
promotes proliferation, invasion and metastasis of non-small cell
lung cancer cells by affecting epithelial-mesenchymal transition.
Eur Rev Med Pharmacol Sci. 21:2075–2086. 2017.PubMed/NCBI
|
|
48
|
Shui X, Zhou C, Lin W, Yu Y, Feng Y and
Kong J: Long non-coding RNA BCAR4 promotes chondrosarcoma cell
proliferation and migration through activation of mTOR signaling
pathway. Exp Biol Med (Maywood). 242:1044–1050. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Wang L, Chunyan Q, Zhou Y, He Q, Ma Y, Ga
Y and Wang X: BCAR4 increase cisplatin resistance and predicted
poor survival in gastric cancer patients. Eur Rev Med Pharmacol
Sci. 21:4064–4070. 2017.PubMed/NCBI
|
|
50
|
Yang H, Yan L, Sun K, Sun X, Zhang X, Cai
K and Song T: LncRNA BCAR4 increases viability, invasion and
migration non-small cell lung cancer cells by targeting
glioma-associated oncogene 2(GLI2). Oncol Res. 27:359–369. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Ouyang S, Zheng X, Zhou X, Chen Z, Yang X
and Xie M: LncRNA BCAR4 promotes colon cancer progression via
activating Wnt/betaβ-catenin signaling. Oncotarget. 8:92815–92826.
2017. View Article : Google Scholar : PubMed/NCBI
|