Introduction
Gastric cancer (GC) comprises >1,000,000 new
cases with an estimated 783,000 deaths reported worldwide in 2018,
which renders it the fifth most common malignancy and the third
primary cause of cancer-related mortality (1). GC also rates third in morbidity and
second in mortality in China (2).
The curative treatment for GC remains the complete excision of
primary tumors with proper lymphadenectomy, since the curative
effects of neoadjuvant therapy have been disappointing to date.
Even some GC patients with the same TNM stage have a different
prognosis and treatment outcome. Thus, researchers are focusing on
identifying the molecular biomarkers and development-related
targets of treatment. Treatment of the disease at an earlier stage
may be key to improving the prognosis of patients with GC.
Survivin has been depicted as the smallest member of
the ‘inhibitor of apoptosis’ family with a unique structure
(3). Survivin is frequently observed
to be overexpressed in malignancies when compared with normal
tissues (4). As regards its
functions, Survivin plays a regulatory role in cell division and
the inhibition of apoptosis, induces angiogenesis, and plays a
vital role in cancer progression (5). Survivin blocks apoptosis induced by a
variety of pro-apoptotic stimuli, including chemotherapy and
radiation, in numerous malignancies (6). In addition, an increased level of
Survivin is correlated with a poorer outcome in various
malignancies (4,7–10);
however, certain studies have indicated that an increased
expression of Survivin splice variants may represent a favorable
marker of survival in some malignancies (11,12).
Phosphatase and tensin homologue deleted on
chromosome 10 (PTEN), also known as mutated in multiple advanced
cancers (MMAC), was identified in 1997 by two independent research
groups as a candidate tumor suppressor gene that was located at the
human chromosome 10q23, a site frequently damaged in primary human
malignancies (13,14). The loss of PTEN function can occur
via a series of genetic or epigenetic abnormalities, such as point
chromosomal deletions, mutations, promoter hypermethylation and
post-translational modifications (15,16), and
may result in various human malignancies, including renal cancer
(17), pancreatic cancer (18), glioma (19), colorectal cancer (20), breast cancer (21), endometrial cancer (22), melanoma (23) and myeloid malignancies (24).
Although previous studies have reported enhanced
expression of Survivin and a decreased expression of PTEN in GC,
the level and correlation of Survivin and PTEN variations have not
yet been fully elucidated. Although some studies have depicted
their expression patterns in GC and analyzed the association of
these expression patterns with clinical characteristics and
prognosis (25,26), the outcomes have been controversial
or dubious due to the insufficiency of sample sizes (27,28).
Therefore, on the base of a relatively larger sample size, the
present study further investigated Survivin and PTEN expression in
GC in order to determine their expression levels, their effects on
patient survival and clinical significance in GC.
Materials and methods
GC patients and specimens
A total of 322 primary gastric adenocarcinoma
samples, 120 matched normal controls (situated 15 cm from the tumor
margin) and 45 metastatic lymph nodes, which had been selected from
the Tumor Hospital Affiliated to Xin Jiang Medical University
between January, 2009 and December, 2012, were included in this
study. Patient characteristics are shown in Table I. The study protocol was approved by
the Review Board of Xin Jiang Tumor Hospital of Xin Jiang Medical
University (approval no. 20090102, January 2, 2009) and all
procedures followed the principles of the Declaration of Helsinki.
All subjects provided written informed consent prior to
participation. All patients had undergone radical primary tumor
excision. All patients, apart from those with stage IV disease,
underwent radical surgery (D2) followed by standard chemotherapy.
None of the patients had received preoperative chemotherapy or
radiotherapy. All cases were staged in accordance with the
guidelines of the American Joint Committee on Cancer and the 2010
Cancer Staging manual of the Union for International Cancer Control
(25). The data on clinical
follow-up were obtained from the hospital record department. The
overall survival (OS) time was calculated from the date of primary
surgery to the date of death. The disease-free survival (DFS) time
was measured from the date of primary radical surgery to the date
of onset of local recurrence or distant metastasis. The patients
who died due to surgery or other causes were eliminated from this
study.
 | Table I.Survivin and PTEN expression in
gastric cancer and normal tissues. |
Table I.
Survivin and PTEN expression in
gastric cancer and normal tissues.
|
|
| Survivin |
| PTEN |
|
|---|
|
|
|
|
|
|
|
|---|
| Tissue | N | – | + | P-value | – | + | P-value |
|---|
| GC tissue | 322 | 90 (28) | 232 (72) |
<0.001a | 213 (66) | 109 (34) |
<0.001a |
| ANT | 120 | 114 (95) | 6 (5) |
<0.001b | 9 (7.5) | 111 (92.5) |
<0.001b |
| LNM | 45 | 9 (4.2) | 36 (13.1) | 0.208c | 34 (75.6) | 11 (24.4) | 0.102c |
Immunohistochemistry (IHC)
The streptavidin-biotin peroxidase complex (SP)
method was used for the IHC assay and was completed with a
commercially available SP-kit (SP-9000; OriGene Technologies,
Inc.). All tumor specimens that were embedded in paraffin were cut
into 4-µm sections and rehydrated in a gradient series of alcohols
following deparaffinization. The slides were boiled for antigen
retrieval in 10 mM sodium citrate buffer (pH 6.0) and quenched with
3% H2O2 for 15 min to block endogenous
peroxidase activity. Non-specific binding was prevented by
incubating the slides with 5% goat serum (OriGene Technologies,
Inc.) in PBS for 30 min at room temperature. The slides were
treated with rabbit polyclonal anti-human Survivin (cat. no.
RAB-0536; NeoMarkers, Inc.) antibody (1:100) (ready to use) or
mouse monoclonal anti-human PTEN (cat. no. 17A; NeoMarkers, Inc.)
antibody (ready to use, 1:50) at room temperature for 2 h, followed
by incubation with biotinylated goat anti-rabbit IgG (HRP;
1:10,000; cat. no. ab6721) and streptavidin-peroxidase (cat. no.
TS-060-HR; Thermo Fisher Scientific, Inc.) for 1 h at room
temperature. Diaminobenzidine was used for visualizing the
peroxidase binding at room temperature for 1 h. The slides were
counterstained lightly with hematoxylin at room temperature for 1 h
and visualized under an light microscope (magnification, ×100). PBS
was employed as a negative control in the IHC assay.
Evaluation of IHC staining
A tumor cell cytoplasm that stained brown under a
light microscope was considered as positive staining. The cells
were scored grossly based on the intensity of staining and the
percentage of positive tumor cells (26). The intensity of staining (I) was
scored as follows: The absence of staining as 0 points; weak
staining as 1 point; and moderate to strong staining as 2 points.
The percentage of positive tumor cells (P) was divided into three
grades as follows: None or <10% of tumor cells with positive
staining as 0 points; 10–50% as 1 point; and >50% as 2 points.
The total score was calculated as (I) × (P) and the outcome was
graded as 0, 1+, 2+ or 3+. All stained slides were scored
independently by two individual pathologists. The evaluation was
performed twice, with the evaluator having no knowledge of the
patient's diagnosis or prognosis. A total of two pathologists
jointly examined the cases and came to an agreement towards any
inconsistent results of the samples.
Statistical analysis
The SPSS software package (version 18.0 SPSS Inc.)
was used for correlation analysis between categorical variables.
The difference in the clinical features between the positive and
negative groups was assessed using the Chi-squared or Fisher's
exact tests. The patient OS and DFS were calculated using the
Kaplan-Meier method. Univeriate and multivariate analysis was
performed to analyze the factors that were determined to be
significant for OS by the Cox proportional hazards model. All
experiment were performed in triplicate. P<0.05 was considered
to indicate a statistically significant difference.
Results
General data of the samples
Among the 322 cases examined, there were 206 (63.9%)
males and 116 (36.1%) females, with a mean age of 62 years (range,
25 to 87 years). A total of 296 (91.9%) cases were categorized as
differentiated type and 26 (8.1%) as undifferentiated type
(including mucinous adenocarcinoma and signet-ring cell
carcinoma;). The invasion depth was T1 in 14 (4.3%), T2 in 54
(16.8%), T3 in 133 (41.3%) and T4 in 121 (37.6%) patients. As
regards TNM staging, 31 patients had stage I disease, 78 had stage
II, 159 had stage III and 54 had stage IV disease. In total, 212
cases exhibited regional lymph node metastasis. The follow-up data
were complete in 292 cases and the median duration of follow-up was
38 months (range, 8–110 months) after primary surgery. A total of
30 patients were lost during follow-up. The follow-up rate was
90.67%.
Expression of Survivin or PTEN in GC,
normal tissues and metastatic lymph nodes
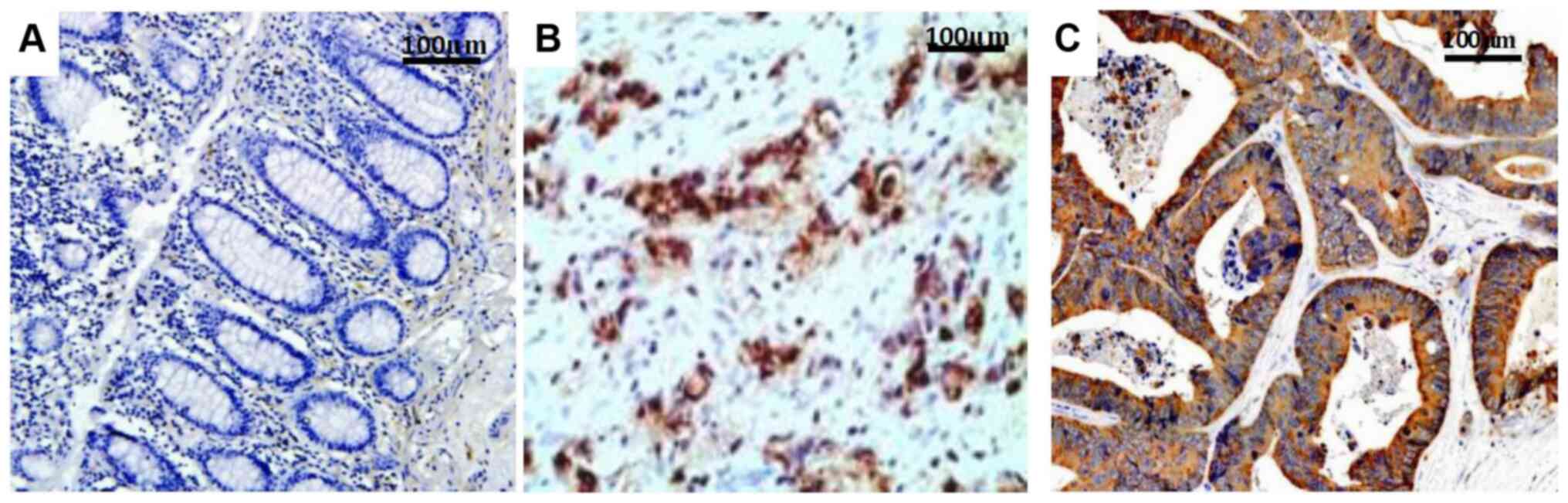
Survivin expression was located mainly in the
cytoplasm and cell membrane, with minimal expression in the nucleus
(Fig. 1), while PTEN expression was
observed in both the cytoplasm and nucleus (Fig. 2). The Survivin expression rates in
the GC, normal tissues and metastatic lymph nodes were 72%
(232/322), 5% (6/120) and 80% (36/45), respectively (Fig. 1), while the PTEN expression rates
were 34% (109/322), 92.5% (111/120) and 24.4% (11/45), respectively
(Table I). The primary GC tissues
and metastatic lymph nodes expressed significantly increased levels
of Survivin and decreased levels of PTEN compared with the normal
mucosal tissues (P<0.001). However, the difference in Survivin
or PTEN expression between the GC tissues and metastatic lymph
nodes was not statistically significant (P=0.208 for Survivin and
P=0.102 for PTEN), although Survivin expression was slightly
increased and PTEN expression was slightly decreased in the
metastatic lymph nodes compared with in the cancerous tissues.
Among the 236 tissues with positive Survivin expression, there were
75 cases with weak staining (32.3%), 97 cases with moderate
staining (41.8%) and 64 with strong staining (27.6%). Among the 109
tissues with positive PTEN expression, 44 exhibited weak staining
(40.4%), 35 demonstrated moderate staining (32.1%) and 30 displayed
strong staining (27.5%).
Association between the expression of
Survivin or PTEN and clinical factors
The expression of Survivin was significantly
associated with gross type, depth of invasion, distant metastasis,
TNM stage and vascular invasion, while PTEN expression was
predominantly associated with age, tumor size, invasion depth, TNM
stage and lymphatic invasion in patients with GC (P<0.05;
Table II). The expression of both
was associated with postoperative metastasis and metastatic site
(P=0.007 and P=0.011 for Survivin, and P=0.002 and P=0.005 for
PTEN) (Table III). Correlation
analysis also revealed a negative correlation between Survivin and
PTEN expression (P=0.001, r=−0.531, Table IV); the higher the expression of
Survivin, the lower the expression of PTEN.
| Table II.The correlation between Survivin and
PTEN expression and clinicopathological factors. |
Table II.
The correlation between Survivin and
PTEN expression and clinicopathological factors.
|
|
| PTEN
expression | Survivin
expression |
|---|
|
|
|
|
|
|---|
| Clinicopathological
factors | N=322 | (−) n (%) | (+) n (%) | P-value | (−) n (%) | (+) n (%) | P-value |
|---|
| Age | ≤60 | 34 (36.6) | 109 (47.6) | 0.071 | 102 (49) | 41 (36) | 0.024a |
|
| >60 | 59 (63.4) | 120 (52.4) |
| 106 (51) | 73 (64) |
|
| Sex | Male | 58 (62.4) | 148 (64.6) | 0.701 | 131 (63) | 75 (65.8) | 0.616 |
|
| Female | 35 (37.6) | 81 (35.4) | 0.846 | 77 (37) | 39 (34.2) |
|
| Race | Han | 89 (95.7) | 218 (95.2) |
| 196 (94.2) | 111 (97.4) | 0.201 |
|
| Uyghur | 4 (4.3) | 11 (4.8) |
| 12 (5.8) | 3 (2.6) |
|
| Blood type | A | 32 (34.4) | 80 (34.8) | 0.404 | 75 (36.1) | 37 (32.5) | 0.813 |
|
| B | 37 (39.8) | 78 (34.1) |
| 71 (34.1) | 44 (38.6) |
|
|
| AB | 4 (4.3) | 22 (9.6) |
| 18 (8.7) | 8 (7) |
|
|
| O | 20 (21.5) | 49 (21.4) |
| 44 (21.2) | 25 (21.9) |
|
| Tumor size | ≤4 | 16 (17.2) | 38 (16.6) | 0.973 | 33 (15.9) | 21 (18.4) | 0.012a |
|
| 4-8 | 65 (69.9) | 163 (71.2) |
| 157 (75.5) | 71 (62.3) |
|
|
| >8 | 12 (12.9) | 28 (12.2) |
| 18 (8.7) | 22 (19.3) |
|
| Gross type | Fungus | 35 (37.6) | 93 (40.6) | 0.022a | 88 (42.3) | 40 (35.1) | 0.193 |
|
| Ulcerous | 38 (40.9) | 113 (49.3) |
| 97 (46.6) | 54 (47.4) |
|
|
| Invasive | 18 (21.4) | 23 (10.0) |
| 23 (11.1) | 20 (17.5) |
|
| Histology | Well | 18 (19.4) | 35 (15.3) | 0.883 | 27 (13) | 26 (22.8) | 0.208 |
|
| Moderate | 58 (62.4) | 147 (64.2) |
| 142 (68.3) | 63 (55.3) |
|
|
| Poor | 8 (8.6) | 16 (7) |
| 14 (6.7) | 10 (8.8) |
|
|
| Papillary
adenocarcinoma | 3 (3.2) | 11 (4.8) |
| 9 (4.3) | 5 (4.4) |
|
|
| Mucinous
adenocarcinoma | 5 (5.4) | 17 (7.4) |
| 13 (6.3) | 9 (7.9) |
|
|
| Signet ring | 1 (1.1) | 3 (1.3) |
| 3 (1.4) | 1 (0.9) |
|
| Tumor site | Antrum | 27 (29) | 77 (33.6) | 0.668 | 67 (32.2) | 37 (32.5) | 0.884 |
|
| Body | 28 (30.1) | 69 (30.1) |
| 61 (29.3) | 36 (31.6) |
|
|
| GEJ | 38 (40.9) | 83 (36.2) |
| 80 (38.5) | 41 (36) |
|
| Infiltration
depth | T1 | 5 (5.4) | 9 (3.9) |
<0.001a | 5 (2.4) | 9 (7.9) | 0.001a |
|
| T2 | 28 (30.1) | 26 (11.4) |
| 28 (13.5) | 26 (22.8) |
|
|
| T3 | 44 (47.3) | 89 (38.9) |
| 83 (39.9) | 50 (43.9) |
|
|
| T4 | 16 (17.2) | 105 (45.9) |
| 92 (44.2) | 29 (25.4) |
|
| LN metastasis | None | 37 (39.8) | 73 (31.9) | 0.206 | 60 (28.8) | 50 (43.9) | 0.025a |
|
| ≤7 | 39 (41.9) | 121 (52.8) |
| 117 (56.3) | 43 (37.7) |
|
|
| >7 | 17 (18.3) | 35 (15.3) |
| 31 (14.9) | 21 (18.4) |
|
| Distant
metastasis | No | 86 (92.5) | 182 (79.5) | 0.005a | 169 (81.3) | 99 (86.8) | 0.199 |
|
| Yes | 7 (7.5) | 47 (20.5) |
| 39 (18.8) | 15 (13.2) |
|
| TNM staging | I | 22 (23.7) | 9 (3.9) |
<0.001a | 7 (3.4) | 24 (21.1) |
<0.001a |
|
| II | 15 (16.1) | 63 (27.5) |
| 53 (25.5) | 25 (21.9) |
|
|
| III | 49 (52.7) | 110 (48) |
| 109 (52.4) | 50 (43.9) |
|
|
| IV | 7 (7.5) | 47 (20.5) |
| 39 (18.8) | 15 (13.2) |
|
| Vascular
invasion | No | 75 (84.3) | 214 (91.8) | 0.045 | 195 (86.7) | 77 (79.4) | 0.098 |
|
| Yes | 14 (14.8) | 19 (8.2) |
| 30 (13.3) | 20 (20.6) |
|
| Lymphatic
invasion | No | 101 (88.6) | 171 (82.2) | 0.130 | 201 (87.4) | 71 (77.2) | 0.022 |
|
| Yes | 13 (11.4) | 37 (17.8) |
| 29 (12.6) | 21 (22.8) |
|
| CEA | ≤3.5 | 18 (20) | 58 (27.9) | 0.152 | 52 (27.4) | 24 (22.2) | 0.327 |
|
| >3.5 | 72 (80) | 150 (72.1) |
| 138 (72.6) | 84 (77.8) |
|
| Table III.Correlation between Survivin or PTEN
expression and related factors of prognosis. |
Table III.
Correlation between Survivin or PTEN
expression and related factors of prognosis.
|
| Survivin | PTEN |
|---|
|
|
|
|
|---|
| Prognostic
factors | −N (%) | +N (%) | P-value | −N (%) | +N (%) | P-value |
|---|
| Local
recurrence |
| No | 74 (88.1) | 195 (90.3) | 0.577 | 184 (88.5) | 105 (92.1) | 0.303 |
|
Yes | 10 (11.9) | 21 (9.7) |
| 24 (11.5) | 9 (7.9) |
|
| Postoperative
metastasis |
| No | 62 (72.1) | 100 (54.9) | 0.007 | 90 (53.3) | 72 (72.7) | 0.002 |
|
Yes | 24 (27.9) | 82 (45.1) |
| 79 (46.7) | 27 (27.3) |
|
| Metastatic
site |
| No | 61 (70.9) | 100 (54.9) | 0.011 | 89 (52.7) | 72 (72.7) | 0.005 |
|
Single | 13 (5.1) | 59 (32.4) |
| 55 (32.5) | 17 (17.2) |
|
| PD | 12 (14) | 23 (12.7) |
| 25 (14.8) | 10 (10.1) |
|
| Median DFS | 61 | 31 | <0.001 | 31 | 70 | <0.001 |
| Median OS | 73 | 39 | <0.001 | 37 | 71 | <0.001 |
| Table IV.Relation between Survivin and PTEN
expression. |
Table IV.
Relation between Survivin and PTEN
expression.
|
| PTEN |
|
|
|---|
|
|
|
|
|
|---|
| Factor | + | – | P-value | r |
|---|
| Survivin |
| + | 44 | 185 | <0.001 | −0.531 |
| − | 70 | 23 |
|
|
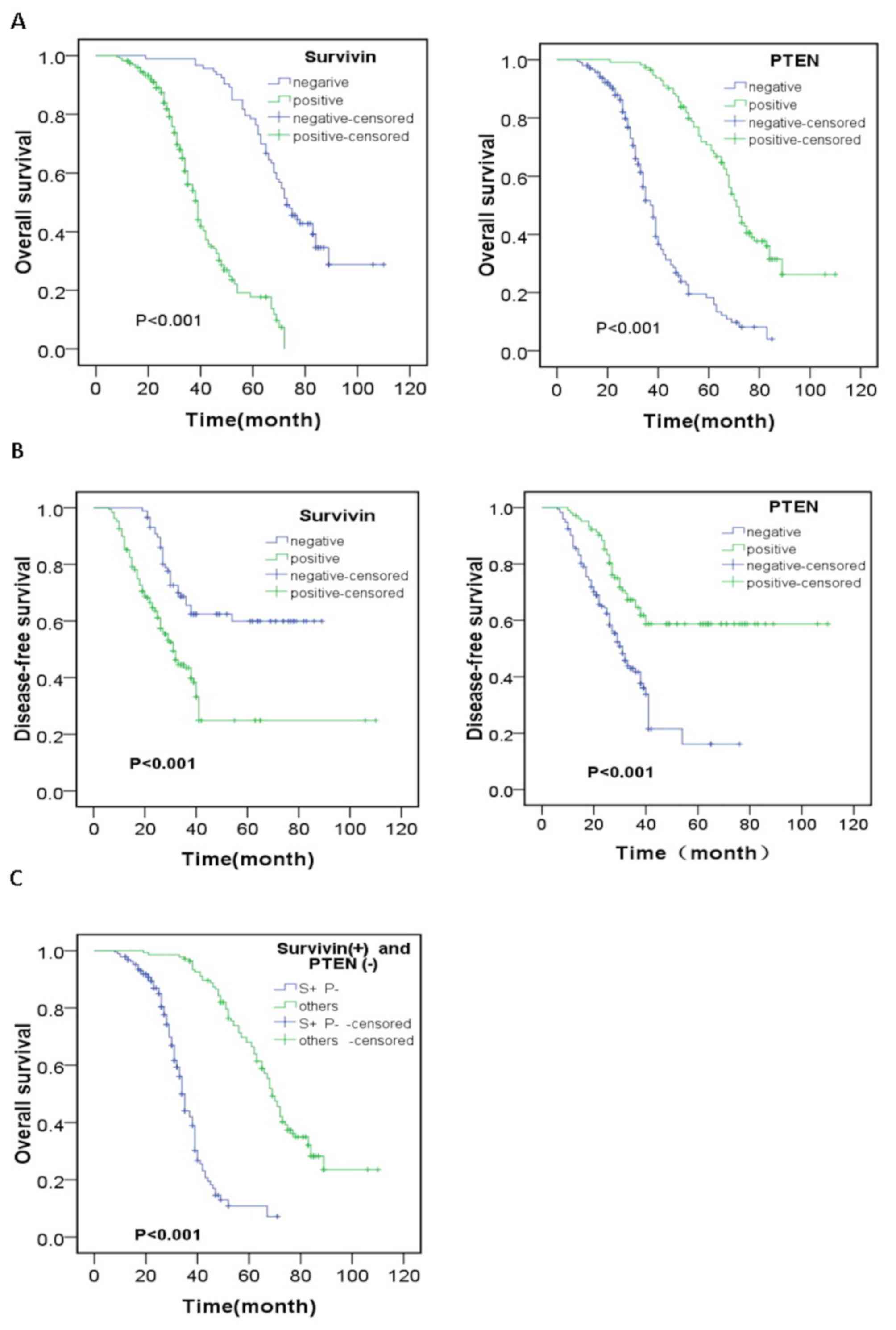
Survival analysis
The results of survival analysis by the Kaplan-Meier
method are presented in Fig. 3. The
1-, 3- and 5-year survival rates of all patients were 91.9, 53.8
and 27.7%, respectively. A statistically significant difference was
observed in OS or DFS between the Survivin- or PTEN-positive and
-negative patients (P<0.001 and P=0.001). The patients who were
Survivin+ or PTEN− had lower OS and DFS
compared with those who were Survivin− or
PTEN+. Multivariate analysis using the Cox model was
performed to analyze relevant prognostic factors in GC patients.
The survival rate of the patients was significantly associated with
invasion depth, advanced TNM stage, postoperative metastasis, tumor
size and the Survivin and PTEN expression level (P<0.05;
Table V). The OS and DFS of the
patients who were simultaneously Survivin+ and
PTEN− were the lowest compared to the others (patients
with Survivin+ and PTEN+ or Survivin- and PTEN- or Survivin- and
PTEN+) (P=0.001 and P=0.001).
| Table V.Cox regression model for univariate
and multivariate analyses of prognostic factors in gastric
cancer. |
Table V.
Cox regression model for univariate
and multivariate analyses of prognostic factors in gastric
cancer.
| Prognostic
factor | Univariate HR (95%
CI) | P-value | Multivariate HR
(95% CI) | P-value |
|---|
| Age | 0.824
(0.619-1.097) | 0.184 | 1.436
(0.600-3.435) | 0.416 |
| Sex | 0.995
(0.742-1.334) | 0.975 | 1.108
(0.786-1.562) | 0.557 |
| Ethnicity | 0.580
(0.314-1.069) | 0.081 | 1.623
(0.728-4.121) | 0.473 |
| Blood type | 0.805
(0.543-1.193) | 0.28 | 0.814
(0.522-1.269) | 0.363 |
| Tumor site | 1.066
(0.900-1.264) | 0.459 | 0.723
(0.329-1.847) | 0.513 |
| Histological
type | 0.799
(0.629-1.016) | 0.067 | 0.831
(0.603-1.145) | 0.258 |
| Gross type | 1.109
(0.706-1.743) | 0.652 | 0.780
(0.465-1.309) | 0.347 |
| Tumor size | 0.994
(0.741-1.203) | 0.054 | 1.426
(1.091-1.862) | 0.009a |
| Lymphatic
invasion | 1.241
(0.934-2.623) | 0.042a | 0.582
(0.124-1.690) | 0.164 |
| Vascular
invasion | 2.251
(1.283-3.421) | 0.084 | 1.324
(0.452-4.378) | 0.87 |
| Invasion depth | 1.852
(1.532-2.237) | 0.001a | 1.383
(1.130-1.693) | 0.002a |
| LN metastasis | 1.527
(1.267-1.840) | 0.021a | 0.589
(0.402-0.970) | 0.098 |
| Distant
metastasis | 2.726
(1.959-3.792) | 0.002a | 0.460
(0.218-0.973) | 0.102 |
| TNM Staging | 2.089
(1.746-2.499) | 0.001a | 1.988
(1.581-2.502) | 0.001a |
| Local
recurrence | 1.227
(0.786-1.918) | 0.368 | 0.824
(0.481-1.411) | 0.481 |
| Postoperative
metastasis | 2.933
(2.178-3.950) | 0.001a | 1.561
(1.100-2.215) | 0.013a |
| Metastatic
site | 1.616
(1.359-1.927) | 0.001a | 0.672
(0.429-1.054) | 0.083 |
| PTEN | 0.219
(0.158-0.304) | 0.001a | 0.228
(0.157-0.332) | 0.001a |
| Survivin | 5.889
(4.020-8.626) | 0.001a | 4.514
(2.964-6.876) | 0.001a |
| CEA | 0.774
(0.555-1.080) | 0.14 | 0.933
(0.558-1.546) | 0.231 |
Discussion
Survivin is observed in a number of human
malignancies but is almost undetectable in normal tissues. Survivin
expression is associated with a diminished apoptotic index, a
poorer survival rate and an increased recurrence risk in the
majority of tumors (29–31). Data on the expression of Survivin in
different gastric tissues are limited, particularly in large sample
analyses. Bury et al (32)
reported that the Survivin expression rate was 73.17% in GC
patients and Gu et al (25)
found that Survivin was expressed at a rate of 62.9% (44/70) in GC
tissues and 0% (0/20) in adjacent normal tissues; both studies had
small sample sizes. In the present study, the expression rate of
Survivin was 72% in malignant tissues, 5% in adjacent normal
tissues and 80% in metastatic lymph nodes. Survivin expression was
increased in malignant tissues and the expression in metastatic
lymph nodes was the highest. These findings suggested that the
upregulation of Survivin may be closely associated with malignant
transformation and the invasive behavior of GC.
The association between the expression of Survivin
and invasion depth or metastatic lymph node in GC remains unclear.
Lins et al (27), reported
that Survivin expression was not associated with the depth of
invasion, lymph node metastasis or differentiation. However, Gu
et al (25) demonstrated that
Survivin expression was associated with tumor differentiation,
depth of invasion and lymph node metastasis. The data of the
present study also indicated that the expression of Survivin was
associated with gross type, invasion depth, distant metastasis, TNM
stage, vascular invasion, postoperative metastasis and metastatic
site. Wang et al (33),
concluded that a positive Survivin expression in the nuclei was
associated with prognosis, although its positive expression in the
cytoplasm was not associated with prognosis in GC. Chen et
al (34), found that the
upregulation of Survivin was associated with a worse survival rate
in GC in 11 studies compared with the normal group. The results of
the present study also supported the hypothesis that patients with
positive Survivin expression exhibit shorter OS and DFS compared
with those with negative Survivin expression.
There is increasing evidence to indicate that PTEN
is a pivotal element that participates in the process of cancer
development and progression (35),
and that it is a prognostic and predictive biomarker in cancer
(36). Li et al (37) reported positive expression of PTEN in
41.2% (47/114) of cases, while a reduction or loss of PTEN
expression was detected in over half of GC cases (58.7%, 67/114).
Zhu et al (38), found that
the percentage of PTEN expression in GC samples (48%, 77/159) was
significantly lower compared with that in adjacent normal tissue
(75%, 113/151). The present study demonstrated that PTEN expression
in GC (34%) and metastatic lymph nodes (24.4%) was downregulated
compared with in normal tissues (92.5%). PTEN expression in
metastatic lymph nodes was lower compared with that in GC tissues,
although the difference did not reach statistical significance.
Therefore, the loss or diminished expression of PTEN in malignant
tissues of the stomach may be a major general event in the
progression of GC.
Reports on the associations between PTEN expression
and clinicopathological factors are inconsistent. Bai et al
(39) demonstrated that age,
differentiation, TNM classification, depth of invasion and distant
metastasis were negatively associated with the expression of
nuclear PTEN. Furthermore, the lower level of nuclear PTEN
expression was also associated with a good prognosis. Li et
al (37) found that the loss of
PTEN expression was associated with distant metastasis and advanced
clinical stage, but not with prognosis. The data of the present
study demonstrated that PTEN expression was associated with age,
tumor size, invasion depth, TNM stage, lymph node metastasis,
lymphatic invasion, postoperative metastasis and metastatic site.
Patients with positive PTEN expression had higher OS compared with
those with negative PTEN expression. Therefore, low expression of
PTEN may be a critical biomarker for GC progression and may be
closely associated with cancer invasiveness and metastasis.
The correlation analysis in the present study
demonstrated a negative correlation between Survivin and PTEN
expression. Lu et al (40),
demonstrated that the expression of PTEN was negatively correlated
with the expression of Survivin in cervical intraepithelial
neoplasia and cervical squamous cell carcinoma. Wu et al
(41), found that PTEN
overexpression suppressed the growth of bladder cancer cells and
significantly induced apoptosis via the downregulation of Survivin
and caspase cascade activation. As previously demonstrated,
following treatment with aspirin, Hep-2 cells exhibited a
significant upregulation of PTEN and the inhibition of nuclear
factor (NF)-κB and Survivin, the downstream targets of the
PTEN/protein kinase B (AKT) signaling pathway, suggesting that the
anticancer molecular mechanism of aspirin may be associated with
the inhibition of tumor invasion and the induction of apoptosis by
regulating the activity of the PTEN/AKT/NF-κB/Survivin signaling
pathway (42). The aforementioned
findings suggest that there may be an association between Survivin
and PTEN.
In conclusion, Survivin and PTEN exhibit a negative
association in GC, which may indicate that Survivin fuctions as an
oncogene while PTEN plays the role of tumor suppressor gene in GC
occurrence. PTEN and Survivin expression are likely important
molecular events in gastric tumorigenesis and may be used as
molecular markers of GC progression and reliable prognostic
indicators of GC. The patient's odds of recurrence, metastasis and
survival may be predicted preliminarily by detecting the Survivin
and PTEN expression in GC tissue before treatment. The major
limitation of the present study is that there wasn't the chance to
perform the experiments in vitro and in vivo for
further functional corroboration of the two genes, which is the
main emphasis of future research.
Acknowledgements
Not applicable.
Funding
The present study was funded by the Natural Science
Fund of the Xin Jiang Uyghur Autonomous Region (grant no.
2019D01C253).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author upon reasonable
request.
Authors' contributions
AY and HW conceived and designed the present study.
RT acquired and analyzed the data and drafted the initial
manuscript. DR assisted with the collection of the
clinicopathological materials and the overall statistics. AR and ZZ
helped perform the IHC experiment. All authors have read and
approved the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Review Board
of Xin Jiang Tumor Hospital of Xin Jiang Medical University
(Urumqi, China; approval no. 20090102), and performed in accordance
with The Declaration of Helsinki. All subjects provided written
informed consent prior to participation.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global Cancer Statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Macdonald JS, Smalley SR, Benedetti J,
Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA,
Gunderson LL, Jessup JM and Martenson JA: Chemoradiotherapy after
surgery compared with surgery alone for adenocarcinoma of the
stomach or gastroesophageal junction. N Engl J Med. 345:725–730.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ambrosini G, Adida C and Altieri DC: A
novel anti-apoptosis gene, survivin, expressed in cancer and
lymphoma. Nat Med. 3:917–921. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Margulis V, Lotan Y and Shariat SF:
Survivin: A promising biomarker for detection and prognosis of
bladder cancer. World J Urol. 26:59–65. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pennati M, Folini M and Zaffaroni N:
Targeting survivin in cancer therapy. Expert Opin Ther Targets.
12:463–476. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kato J, Kuwabara Y, Mitani M, Shinoda N,
Sato A, Toyama T, Mitsui A, Nishiwaki T, Moriyama S, Kudo J and
Fujii Y: Expression of survivin in esophageal cancer: Correlation
with the prognosis and response to chemotherapy. Int J Cancer.
95:92–95. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang LQ, Wang J, Jiang F, Xu L, Liu FY
and Yin R: Prognostic value of survivin in patients with non-small
cell lung carcinoma: A systematic review with meta-analysis. PLoS
One. 7:e341002012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Krieg A, Werner TA, Verde PE, Stoecklein
NH and Knoefel WT: Prognostic and clinicopathological significance
of survivin in colorectal cancer: A meta analysis. PLoS One.
8:e653382013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hingorani P, Dickman P, Garcia-Filion P,
White-Collins A, Kolb EA and Azorsa DO: BIRC5 expression is a poor
prognostic marker in Ewing sarcoma. Pediatr Blood Cancer. 60:35–40.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Carter BZ, Qiu Y, Huang X, Diao L, Zhang
N, Coombes KR, Mak DH, Konopleva M, Cortes J, Kantarjian HM, et al:
Survivin is highly expressed in CD34(+)38(−) leukemic
stem/progenitor cells and predicts poor clinical outcomes in AML.
Blood. 120:173–180. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Vallböhmer D, Drebber U, Schneider PM,
Baldus S, Bollschweiler E, Brabender J, Warnecke-Eberz U, Mönig S,
Hölscher AH and Metzger R: Survivin expression in gastric cancer:
Association with histomorphological response to neoadjuvant therapy
and prognosis. J Surg Oncol. 99:409–413. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jamieson NB, Carter CR, McKay CJ and Oien
KA: Tissue biomarkers for prognosis in pancreatic ductal
adenocarcinoma: A systematic review and meta-analysis. Clin Cancer
Res. 17:3316–3331. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Steck PA, Pershouse MA, Jasser SA, Yung
WK, Lin H, Ligon AH, Langford LA, Baumgard ML, Hattier T, Davis T,
et al: Identification of a candidate tumour suppressor gene, MMAC1,
at chromosome 10q23.3 that is mutated in multiple advanced cancers.
Nat Genet. 15:356–362. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ngeow J, Sesock K and Eng C: Clinical
implications for germline PTEN spectrum disorders. Endocrinol Metab
Clin North Am. 46:503–517. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Correia NC, Girio A, Antunes I, Martins LR
and Barata JT: The multiple layers of non-genetic regulation of
PTEN tumour suppressor activity. Eur J Cancer. 50:216–225. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bermúdez Brito M, Goulielmaki E and
Papakonstanti EA: Focus on PTEN regulation. Front Oncol. 5:1662015.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Que WC, Qiu HQ, Cheng Y, Liu MB and Wu CY:
PTEN in kidney cancer: A review and meta-analysis. Clin Chim Acta.
480:92–98. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hill R, Calvopina JH, Kim C, Wang Y,
Dawson DW, Donahue TR, Dry S and Wu H: PTEN loss accelerates
KrasG12D-induced pancreatic cancer development. Cancer Res.
70:7114–7124. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Han F, Hu R, Yang H, Liu J, Sui J, Xiang
X, Wang F, Chu L and Song S: PTEN gene mutations correlate to poor
prognosis in glioma patients: A meta-analysis. Onco Targets Ther.
9:3485–3492. 2016.PubMed/NCBI
|
|
20
|
Yazdani Y, Farazmandfar T, Azadeh H and
Zekavatian Z: The prognostic effect of PTEN expression status in
colorectal cancer development and evaluation of factors affecting
it: Mir-21 and promoter methylation. J Biomed Sci. 23:92016.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Golmohammadi R, Rakhshani MH, Moslem AR
and Pejhan A: Prognostic role of PTEN gene expression and length of
survival of breast cancer patients in the north east of Iran. Asian
Pac J Cancer Prev. 17:305–309. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang HM, Fan TT, Li W and Li XX:
Expressions and significances of ttf-1 and PTEN in early
endometrial cancer. Eur Rev Med Pharmacol Sci. 21 (Suppl
3):S20–S26. 2017.
|
|
23
|
Giles KM, Rosenbaum BE, Berger M, Izsak A,
Li Y, Illa Bochaca I, Vega-Saenz de Miera E, Wang J, Darvishian F,
Zhong H and Osman I: Revisiting the clinical and biologic relevance
of partial PTEN loss in melanoma. J Investig Dermatol. 139:430–438.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Morotti A, Panuzzo C, Crivellaro S, Carra
G, Torti D, Guerrasio A and Saglio G: The role of PTEN inmyeloid
malignancies. Hematol. Rep. 7:58442015.
|
|
25
|
Gu Y, Jin S, Wang F, Hua Y, Yang L, Shu Y,
Zhang Z and Guo R: Clinicopathological significance of PI3K, Akt
and survivin expression in gastric cancer. Biomed Pharmacother.
68:471–475. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yusup A, Huji B, Fang C, Wang F, Dadihan
T, Wang HJ and Upur H: Expression of trefoil factors and TWIST1 in
colorectal cancer and their correlation with metastatic potential
and prognosis. World J Gastroenterol. 23:110–120. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lins RR, Oshima CT, Oliveira LA, Silva MS,
Mader AM and Waisberg J: Expression of E-cadherin and WNT pathway
proteins Betacatenin, APC, TCF-4 and Survivin in gastric
adenocarcinoma: Clinical and pathological implication. Arq Bras Cir
Dig. 29:227–231. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Deng H, Wu RL, Zhou HY, Huang X, Chen Y
and Liu LJ: Significance of Survivin and PTEN expression in full
lymph node-examined gastric cancer. World J Gastroenterol.
12:1013–1017. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Contis J, Lykoudis PM, Goula K, Karandrea
D and Kondi-Pafiti A: Survivin expression as an independent
predictor of overall survival in pancreatic adenocarcinoma. J
Cancer Res Ther. 14 (Suppl):S719–S723. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Xia H, Chen S, Huang H and Ma H: Survivin
over-expression is correlated with a poor prognosis in esophageal
cancer patients. Clin Chim Acta. 446:82–85. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Li S, Wang L, Meng Y, Chang Y, Xu J and
Zhang Q: Increased levels of LAPTM4B, VEGF and survivin are
correlated with tumor progression and poor prognosis in breast
cancer patients. Oncotarget. 8:41282–41293. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Bury J, Szumiło J, Dąbrowski A, Ciechański
A, Śliwińska J and Wallner G: Vascular endothelial growth factor
and survivin immunostaining in gastric adenocarcinoma. Pol Przegl
Chir. 84:341–347. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang ZN, Xu HM, Jiang L, Zhou X, Lu C and
Zhang X: Expression of survivin in primary and metastatic gastric
cancer cells obtained by laser capture microdissection. World J
Gastroenterol. 10:3094–3098. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Chen J, Li T, Liu Q, Jiao H, Yang W, Liu X
and Huo Z: Clinical and prognostic significance of HIF-1a, PTEN,
CD44v6, and survivin for gastric cancer: A meta-analysis. PLoS One.
9:e918422014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Milella M, Falcone I, Conciatori F, Cesta
Incani U, Del Curatolo A, Inzerilli N, Nuzzo CM, Vaccaro V, Vari S,
Cognetti F and Ciuffreda L: PTEN: Multiple functions in human
malignant tumors. Front Oncol. 5:242015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Bazzichetto C, Conciatori F, Pallocca M,
Falcone I, Fanciulli M, Cognetti F, Milella M and Ciuffreda L: PTEN
as a prognostic/predictive biomarker in cancer: An unfulfilled
promise? Cancers (Basel). 11:4352019. View Article : Google Scholar
|
|
37
|
Li Y, Cui J, Zhang CH, Yang DJ, Chen JH,
Zan WH, Li B, Li Z and He YL: High-expression of DJ-1 and loss of
PTEN associated with tumor metastasis and correlated with poor
prognosis of gastric carcinoma. Int J Med Sci. 10:1689–1697. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Zhu X, Qin X, Fei M, Hou W, Greshock J,
Bachman KE, Kang J and Qin Y: Loss and reduced expression of PTEN
correlate with advanced-stage gastric carcinoma. Exp Ther Med.
5:57–64. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Bai ZG, Ye YJ, Shen DH, Lu YY, Zhang ZT
and Wang S: PTEN expression and suppression of proliferation are
associated with Cdx2 overexpression in gastric cancer cells. Int J
Oncol. 42:1682–1691. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Lu D, Qian J, Yin X, Xiao Q, Wang C and
Zeng Y: Expression of PTEN and survivin in cervical cancer:
Promising biological markers for early diagnosis and prognostic
evaluation. Brit J Biomed Sci. 69:143–146. 2012. View Article : Google Scholar
|
|
41
|
Wu ZX, Song TB, Li DM, Zhang XT and Wu XL:
Overexpression of PTEN suppresses growth and induces apoptosis by
inhibiting the expression of survivin in bladder cancer cells.
Tumour Biol. 28:9–15. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Jin M, Li C, Zhang Q, Xing S, Kan X and
Wang J: Effects of aspirin on proliferation, invasion and apoptosis
of Hep-2 cells via the PTEN/AKT/NF-κB/survivin signaling pathway.
Oncol Lett. 15:8454–8460. 2018.PubMed/NCBI
|