Introduction
Malignant melanoma is a highly metastatic skin
cancer with poor prognosis (1). The
incidence rates of melanoma have been growing in all regions of the
world (2), where ~287,723 cases of
cutaneous melanoma were newly diagnosed and about 60,712 deaths
were caused by melanoma in 2018 (3).
In the United States, the estimated number of new cases of melanoma
are 100,350 (60,190 men and 40,160 women), accounting for 3.33% of
all new cancer cases, which will result in 6,850 estimated deaths
in 2020 (4).
The advent of molecular targeted therapy and
immunotherapy has revolutionized the treatment strategy and
significantly improved the outcome of patients with melanoma
compared with 10 years ago, when the median survival of patients
was only about 6 months, and the 5-year survival rate was <5%
(5). Targeted therapy abolished the
abnormal activation of the MAPK pathway caused by hyperactive
mutations of the proto-oncogene BRAF (6). In total ~50% of patients with melanoma
harbor BRAF mutations, and 80–90% BRAF mutations
occur at the 600th codon known as BRAFV600E/K/R or BRAFV600 with
other amino acid substitutions (7,8). A few
BRAF kinase inhibitors (BRAFi) have been developed, of which
vemurafenib (PLX4030), dabrafenib and encorafenib targeting
BRAFV600E or BRAFV600K were approved for advanced melanoma by the
Food and Drug Administration (FDA) (9). Clinical trials have demonstrated that
vemurafenib produces as high as an 80% response rate in BRAFV600E
patients with melanoma (7,10,11). The
combinations of a BRAF inhibitor and a MEK inhibitor notably
increased the overall survival of BRAFV600E patients with melanoma
(12). Immunotherapy improves the
immune response to melanoma by inhibiting negative immunity
modulators (13). The immune
checkpoint blockade (ICB) approach targets cytotoxic T
lymphocyte-associated antigen 4 and programmed cell death protein 1
and its ligand programmed death ligand 1 which suppress antitumor
immunity (13). Compared with
conventional therapy, molecular targeted therapy and immunotherapy
provide multiple more effective treatment options; however, they
also present challenges that have yet to be addressed for improving
outcomes (13). Single-agent BRAF
inhibitor vemurafenib has a high response rate, but has much less
optimal durability of response (<6 months) (7). In addition, there are several common
side effects associated with vemurafenib including joint pain,
rash, photosensitivity dermatitis, fatigue, hair loss and itching
(7,14,15).
Though BRAFi-MEKi combinations demonstrated a more durable response
compared with single-agent BRAF inhibitors, there are also obvious
side effects including squamous cell carcinoma, keratoacanthoma,
liver enzyme abnormalities and pyrexia (14). ICB inhibitors (ICI) increase the
activity of immune response and cause immune-related adverse events
(irAEs) in multiple organs including skin, liver, gastrointestinal
tract, thyroid and lung (16–20).
Severe irAEs are life-threatening and can result in treatment
discontinuation (21,22). Therefore, lack of durability of
response to BRAF inhibitors, durable response occurring in only 1/3
patients receiving BRAFi/MEKi, resistance to BRAFi/MEKi and
systemic toxicity and intolerance of ICI treatment (7) pose pressing needs for developing
additional therapeutic regimens to achieve improved management for
advanced melanoma.
Previous studies reported that antioxidants are able
to inhibit cancer progression (23).
Antioxidants can inhibit the initiation of cancer by scavenging
free radicals, such as superoxides, hydroxyls and oxides of
nitrogen that cause DNA damage and mutations in tumor suppressor
genes (24–26). Antioxidants also scavenge the
reactive oxygen species, which are believed to promote cell
migration and invasion in metastasized cancers (27). Hence, antioxidants have been
advocated as a potent and safe supplement for cancer prevention.
Antioxidants can also repair normal tissue damage caused by free
radicals that are generated by radiotherapy and chemotherapy
(28–31). Hence, antioxidants have been widely
used to decrease the side effects of cancer therapy (31,32).
However, some research has demonstrated that antioxidants can
increase cancer risk (32,33). It has been reported that antioxidants
increase metastasis of melanoma in mice (34). Antioxidants may protect cancer cells
from oxidative stress, thus inhibiting apoptosis and promoting the
metastasis of melanoma cells (35).
Therefore, there is a heated debate on whether antioxidants can be
recommended to patients with cancer, especially for patients who
receive free-radical-producing radiotherapy or chemotherapy
(31,32). The contradictory results about the
effect of antioxidants on the progression of cancers warrants
further research on the working mechanisms of antioxidants in
cancers (36).
Coenzyme Q-10 (CoQ10) is used by the body system as
an endogenous antioxidant and it indicates the oxidative stress
level of cells (37). CoQ10 is
widely used as a dietary supplement because of its antioxidative
property, which has been reported to be beneficial in treating
hypertension and congestive heart failure and ameliorating the side
effects of chemotherapy (32,38,39).
Low blood level of CoQ10 was reported in patients with cancers of
breast, lung, prostate, colon, pancreas, kidney, head and neck, and
myeloma and lymphoma (32,40,41).
Studies have demonstrated that low plasma CoQ10 levels may be an
independent prognostic factor for the progression of melanoma and
breast cancer (42,43). However, a recent study reported a
completely contradictory finding: The serum level of CoQ10 were
found to be significantly higher in newly diagnosed and
non-intervened patients with breast cancer compared with the
healthy control group, suggesting that CoQ10 may offer a growth
advantage for breast cancer cells over normal cells (44). CoQ10 was reported to decrease the
effectiveness of radiation therapy against small-cell lung cancer
due to its antioxidant property that protects cancer cells from the
toxicity of free radicals produced by radiation (45). Several studies using CoQ10 as an
adjuvant therapy in human subjects reported that CoQ10 presented
favorable effects on achieving regression of tumor masses and
remission of distant metastasis of breast cancer (45,46).
However, all these studies have major design flaws, including the
absence of appropriate control groups, patient selection bias and
compounding factors such as receiving other supplements or standard
cancer treatment (45,46). Hence, it remains difficult to draw a
conclusion about any anticancer effect directly related to the
intake of CoQ10 (47). The National
Cancer Institute states that, as of April 2019, ‘No report of a
randomized clinical trial of coenzyme Q10 as a treatment
for cancer has been published in a peer-reviewed scientific
journal’ (48). In addition, to the
best of our knowledge very little research has been done on the
effect of CoQ10 on melanoma. Only one recent study demonstrated
that CoQ10 did not affect the viability of some BRAF V600E melanoma
cells, such as SK-MEL-28 (49).
β-carotene has been widely used as a pigment in
foods (fats and oil, and infant formula as a source of vitamin A),
cosmetics (an additive in cosmetics for tanning and sunscreen) and
drugs (such as a prescription drug for treating erythropoetic
protoporphyria) and it showed no mutagenicity or cytotoxicity
(50). β-carotene is an antioxidant
consisting of polyunsaturated hydrocarbons consisting of 40 carbons
and no oxygen (51). It has been
reported that β-carotene inhibits angiogenesis and activation of
transcription factors, such as c-fosc and activated transcription
factor 2 in mouse melanoma cells (52). An in vivo study demonstrated
that β-carotene inhibited lung metastasis induced by B16 melanoma
in mice (53). A large number of
epidemiological studies have reported an inverse relationship
between the blood level of β-carotene and lung cancer risk
(54,55). The incidence of non-melanocytic skin
cancer was inversely related to the serum level of β-carotene
(56). In addition, β-carotene was
found to be photoprotective against UV-induced carcinogenesis
(57). However, a study demonstrated
that β-carotene-supplemented semi-defined diets not only provided
no photoprotective effect, but also significantly exacerbated
UV-induced carcinogenesis (58). In
addition, smokers supplemented with β-carotene demonstrated a
significantly higher incidence of lung cancer compared with smokers
who were not taking β-carotene as a supplement (59,60).
Epidemiological studies have demonstrated an association between
higher incidence of lung cancer and β-carotene intake (50,61). The
effect of β-carotene on the initiation and development of cancers
may be divergent in different cancers (62). To the best of our knowledge no
research has been done on the effect of β-carotene on the
proliferation and invasiveness of human malignant melanoma cells.
To the best of our knowledge the effect of β-carotene on the
cytotoxicity of BRAF inhibitors has not been investigated
either.
Since cancer cells perform high-level metabolic
activity and suffer from more oxidative stress (63), antioxidants could potentially promote
the growth and progression of cancers by mopping up free radicals
from cancer cells. In fact, our previous research has demonstrated
that antioxidant vitamin C exerted a stimulatory effect at
physiological concentration on the growth and metastasis of human
malignant melanoma (64).
In the present study, we hypothesized that the
antioxidants CoQ-10 and β-carotene have an effect on the growth and
invasiveness of human malignant melanoma cells. In addition, in a
previous study our lab demonstrated that the BRAF kinase inhibitor
vemurafenib, an FDA-approved antimelanoma drug, increased the
oxidative stress in human malignant melanoma cells (64); thus antioxidants may interfere with
the cytotoxic effect of vemurafenib on melanoma cells by scavenging
free radicals. Hence, the present study aimed to determine the
effect of CoQ-10 and β-carotene on the growth, migration and
invasion and apoptosis induction of human malignant melanoma cell
lines, and also on the cytotoxicity of emurafenib on human
malignant melanoma cells. Τhe present study aimed to better
understand the biological effects and working mechanism of the
antioxidants CoQ-10 and β-carotene on malignant melanoma so that
clinicians can decide whether adding antioxidant supplements to the
cancer treatment regimen is a viable option.
Materials and methods
Chemicals
Vemurafenib (PLX4032; cat. no. S1267) was purchased
from Selleck Chemicals. CoQ10 (cat. no. C9538) and β-carotene (cat.
no. C9750) were purchased from Sigma-Aldrich; Merck KGaA.
Cells and culture conditions
SK-MEL-28 (PLX sensitive) and A2058 (PLX resistant)
human melanoma cell lines were purchased from the American Type
Culture Collection (ATCC). SK-MEL-28 and A2058 were cultured in
Eagle's Minimum Essential Medium (EMEM; Thermo Fisher Scientific
Inc.) and Dulbecco's Modified Eagle's medium (DMEM; Thermo Fisher
Scientific Inc.), respectively and were supplemented with 10% fetal
bovine serum (FBS; Thermo Fisher Scientific Inc.) and 0.1%
penicillin/streptomycin (Thermo Fisher Scientific Inc.). Cells were
grown at 37°C in a humidified atmosphere of 5% CO2.
MTS assay
SK-MEL-28 and A2058 cells were seeded into 96-well
plates (3,000 cells/well) (Costar, Corning Inc.) and incubated for
12 h to allow the cells to attach. To test the effect of the CoQ10
on cell viability, the cells in the experimental groups were
treated with CoQ10 at final concentrations of 1, 5 and 10 µM,
respectively. The cells in control groups were treated with the
drug vehicle dimethyl sulfoxide (DMSO) (Fisher Bioreagents; Thermo
Fisher Scientific Inc.). To test the efficacy of CoQ10 on the
cytotoxicity of PLX4032 against melanoma cell proliferation, the
SK-MEL-28 and A2058 cells were treated with PLX4032 at 2 and 20 µM,
respectively, together with CoQ10 at 1, 5 and 10 µM. The cells in
the control groups were treated with the drug vehicle dimethyl
sulfoxide (DMSO) (Fisher Bioreagents; Thermo Fisher Scientific
Inc.). After incubation for 48 h, 10 µM MTS
(3-(4,5-dimethylthiazol-2-yl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H
tetrazolium) reagent (Promega Corporation) was added into each well
and incubated for 3 h at 37°C. The absorbance of solubilized dye
was measured by a microplate reader (BioTek Instruments Inc.) at
490 nm. Three independent experiments were performed and the
results were reported as means ± SD.
Wound healing assay
SK-MEL-28 and A2058 cells (2×105) were
seeded into 12-well plates and incubated for 24 h until they
reached ~90% confluence. Then the layer of cells was scraped with a
200 µl micropipette tip to create a wound. Plates were washed with
Hanks' Balanced Salt Solution (HBSS; Sigma-Aldrich; Merck KGaA) and
replaced with fresh serum free medium. The assay was performed in 8
groups: i) Group 1 was the control group, which was treated with
drug vehicle (DMSO); ii) groups 2, 3, and 4 were treated with CoQ10
or β-carotene at final concentrations of 1, 5 and 10 µM,
respectively; iii) group 5 was treated with 2 µM PLX4032 alone; and
iv) groups 6, 7, and 8 were treated with PLX4032 at a final
concentration of 2 µM and CoQ10 or β-carotene at final
concentrations of 1, 5 and 10 µM, respectively. The images of the
wounds were captured at 0 and 24 h under an inverted light
microscope (magnification, ×100) and the average wound distance was
calculated using ImageJ software v.1.53f (National Institutes of
Health).
Transwell cell invasion assay
Matrigel-precoated 24-well Transwell inserts (cat.
no. 354480; Corning Inc.) were used. A2058 (3×104) cells
were resuspended in 200 µl serum-free Eagle's minimum essential
medium in the upper chamber of a 24-well plate. Culture medium (700
µl) containing 20% fetal bovine serum was applied to the lower
chamber. The assay was performed in 8 groups: i) Group 1 was the
control group, which was treated with drug vehicle (DMSO); ii)
groups 2, 3, and 4 were treated with β-carotene at final
concentrations of 1, 5 and 10 µM, respectively; iii) groups 5, 6,
and 7 were treated with PLX4032 at a final concentration of 2 µM
and β-carotene at final concentrations of 1, 5, and 10 µM,
respectively; and iv) group 8 was treated with 2 µM PLX4032 alone.
After incubation for 18 h at 37°C in a 5% CO2 incubator,
the cells were fixed using 3% formaldehyde in PBS for 10 min at
room temperature and stained by Giemsa stain for 10 min at room
temperature. Non-migrated cells were scraped off using cotton swabs
and migrated cells were counted under the inverted light microscope
(magnification, ×100).
Apoptosis analysis
Apoptosis was examined using an Annexin
V-FITC-propidium iodide (PI) dual staining kit (BioLegend Inc.)
followed by flow cytometry analysis according to the manufacturer's
instructions. The assay was performed in 8 groups: i) Group 1 was
the control group which was treated with drug vehicle (DMSO); ii)
groups 2, 3, and 4 were treated with CoQ10 at final concentrations
of 1, 5 and 10 µM, respectively; iii) groups 5, 6, and 7 were
treated with PLX4032 at a final concentration of 2 µM and Coenzyme
Q10 at final concentrations of 1, 5 and 10 µM, respectively; and
iv) group 8 was treated with 2 µM PLX4032 alone. After 24 h, A2058
and SK-MEL-28 were harvested by trypsinization, washed with
ice-cold cell staining buffer (Biolegend Inc.), and then
resuspended in the binding buffer (BioLegend Inc.) at a density of
1×106 cells/ml. Cell suspension was stained with Annexin
V-FITC and PI and analyzed by the Accuri C6 Flow Cytometer System
(BD Biosciences). Both early and late stages of apoptotic cells
were counted using associated software CytExpert v.2.1 (Beckman
Coulter, Inc.).
Western blotting
After a 48 h treatment, A2058 cells were trypsinized
and washed 3 times with PBS and then lysed in a lysis buffer for 30
min at 4°C. The proteins were extracted in the supernatant after
centrifugation at 14,000 g for 20 min at 4°C and the concentration
of protein was detected using Bio-Rad protein assay reagent
(Bio-Rad Laboratories Inc.). After determining the concentrations
of proteins with the BCA assay, the proteins (20 µg/lane) were
mixed with a Laemmli sample buffer (Bio-Rad Laboratories Inc.) with
5% 2-Mercapto-ethanol (β-ME) (Sigma-Aldrich; Merck KGaA) at the
ratio of 1:1 and the mixture was boiled for 10 min before being
electrophoresed on an 4–12% SDS-PAGE gel (Bio-Rad Laboratories
Inc.). The protein was transferred to a nitrocellulose membrane at
350 mA for 1 h in the transfer buffer. The membrane was blocked
with 5% non-fat milk in TBST (0.1% Tween) for 2 h at room
temperature with shaking. The membrane was then rinsed 3 times with
TBST, and subsequently immunoblotted with primary antibodies for
rabbit anti-GAPDH (1:1,000; cat. no. 5174), anti-phospho-P44/42
MAPK (1:1,000 cat. no. 4370), anti-total P44/42 MAPK (1:1,000; cat.
no. 4695), anti-phospho-BRAF (1:1,000; cat. no. 2696) and
anti-total BRAF (1:1,000; cat. no. 14814) (all antibodies were from
Cell Signaling Technology Inc.) at 4°C overnight. Signals were
developed by incubating with the horse radish peroxidase
(HRP)-linked secondary antibody (1:1,000; cat. no. 32935; Cell
signaling Technology Inc.) for 2 h at room temperature. GAPDH was
used as the internal loading control. Subsequently, development was
performed using the ClarityTM Western ECL Substrate
(Bio-Rad Laboratories Inc.) for 5 min. The intensity of the signals
was determined by the FluorChemTM E system (Protein
Simple). ImageJ v.1.53f (National Institutes of Health) was used
for densitometry.
Statistical analysis
All values are represented as mean ± standard
deviation (SD) from at least three independent experiments, and
were subjected to one-way analysis of variance (ANOVA) and compared
by the post hoc Tukey's HSD test using SAS University edition (SAS
Institute Inc.). P<0.05 was considered to indicate a
statistically significant difference.
Results
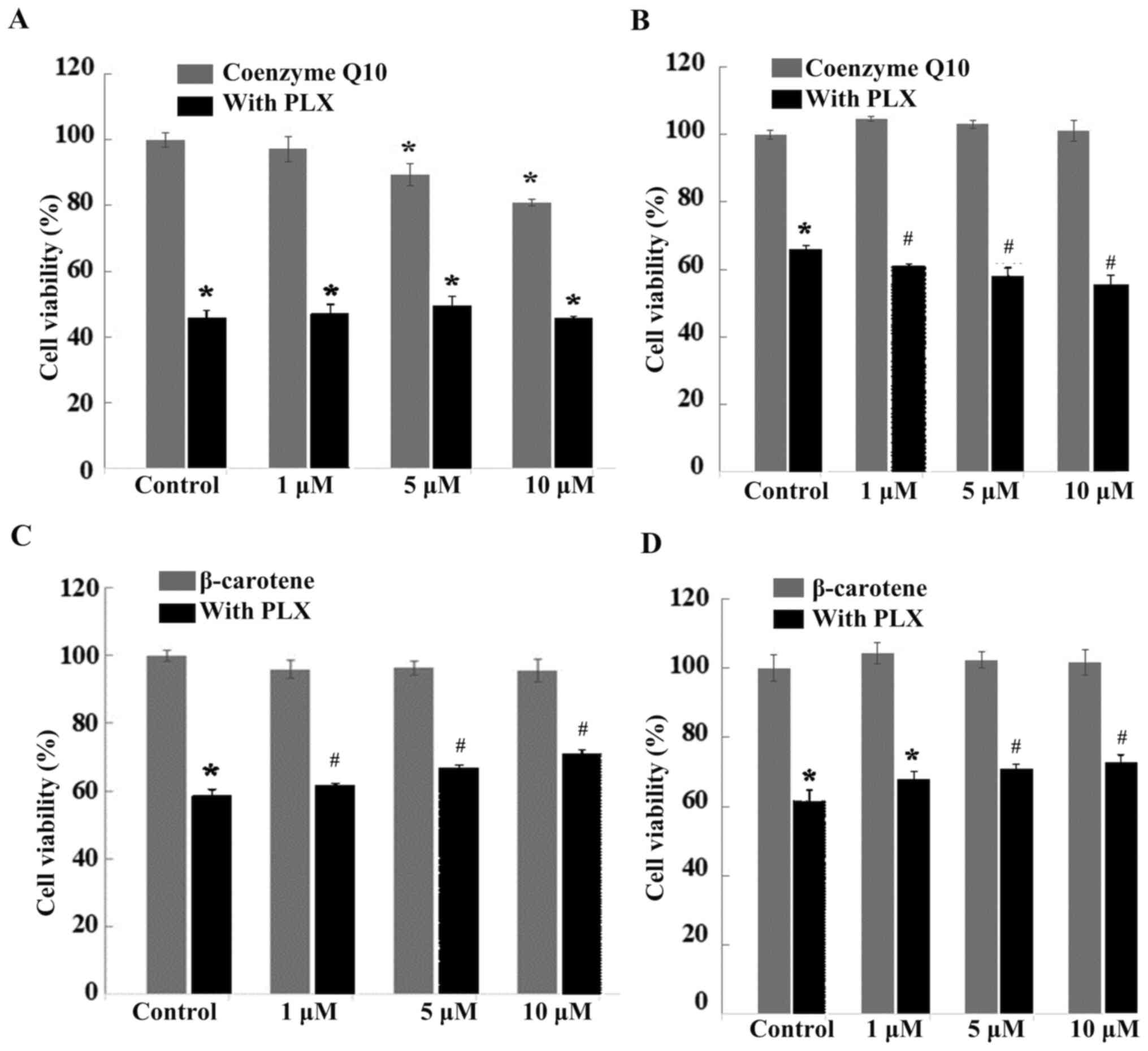
CoQ10 displays cytotoxicity against
the sensitive melanoma cell line and β-carotene alleviates the
cytotoxicity of PLX against melanoma cells
MTS assay was used to determine the cytotoxic effect
of CoQ10 and β-carotene in 2 malignant melanoma cell lines:
SK-MEL-28 and A2058. In the SK-MEL-28 cell line, which is
vemurafenib sensitive, CoQ10 decreased the cell viability and
displayed cytotoxicity at 5 and 10 µM, but did not affect the
cytotoxicity of PLX (Fig. 1A). In
A2058, which is a vemurafenib-resistant cell line, CoQ10 did not
display cytotoxicity (Fig. 1B).
However, CoQ10 increased the cytotoxicity of PLX at 1, 5 and 10 µM
(Fig. 1B). In both SK-MEL-28 and
A2058 cell lines, β-carotene did not display cytotoxicity (Fig. 1C and D). However, β-carotene
alleviated the cytotoxicity of PLX in both cell lines (Fig. 1C and D).
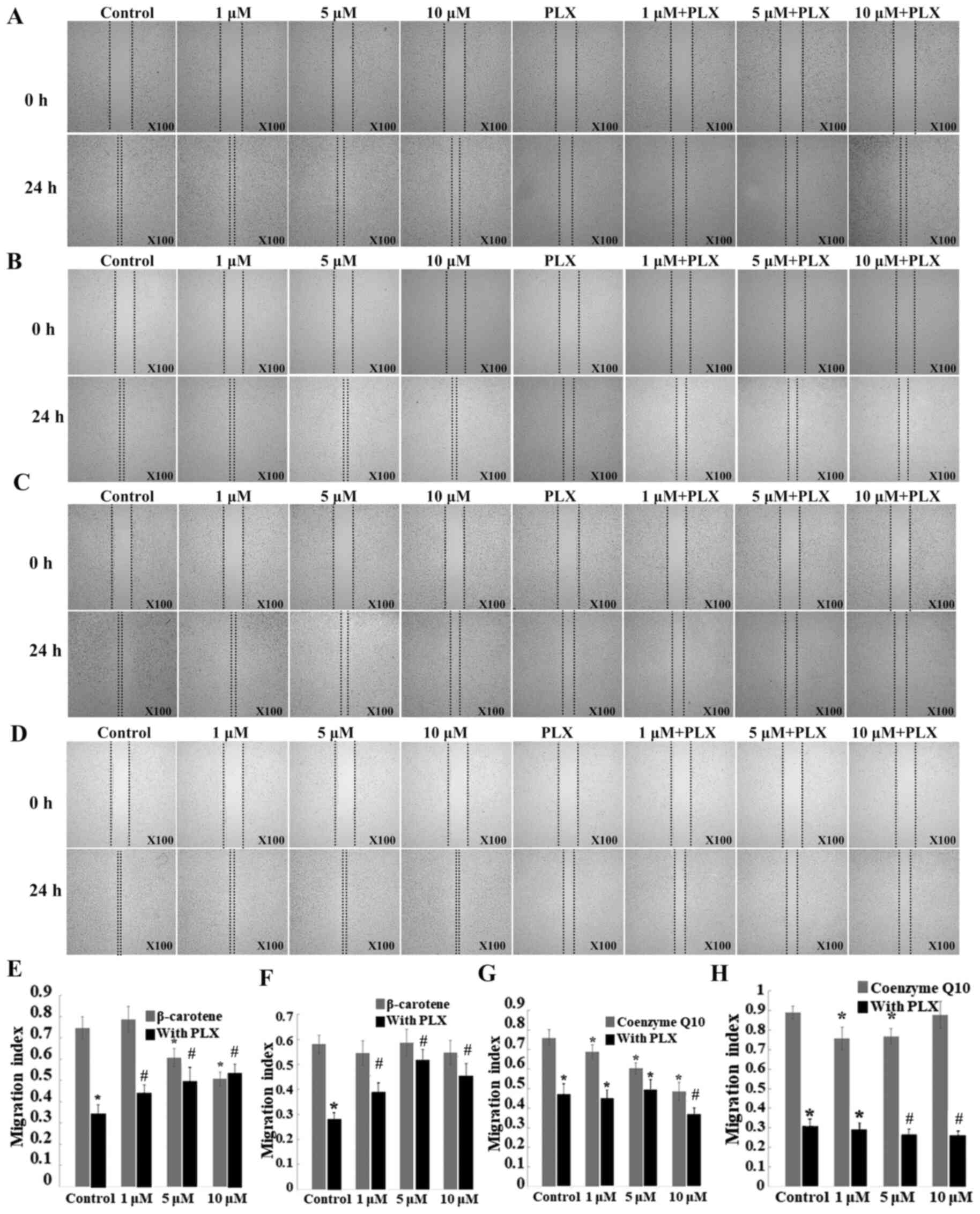
CoQ10 and β-carotene both inhibit cell
migration, but display different effects on the inhibition of
migration of melanoma cells caused by PLX4032
SK-MEL-28 and A2058 migration was examined using the
wound healing assay. β-carotene inhibited the migration of
SK-MEL-28 cells (Fig. 2A and E), but
showed no effect on A2058 cells (Fig. 2B
and F). Notably, β-carotene alleviated the inhibitory effect of
PLX on the migration of both SK-MEL-28 (Fig. 2A and E) and A2058 cells (Fig. 2B and F). CoQ10 inhibited the
migration of both SK-MEL-28 (Fig. 2C and
G) and A2058 (Fig. 2D and H)
cells. In contrast to β-carotene, CoQ10 at 10 µM enhanced the
inhibition of SK-MEL-28 cell migration by PLX (Fig. 2C and G), and CoQ10 at 5 and 10 µM
enhanced the inhibition of A2058 cell migration by PLX (Fig. 2D and H).
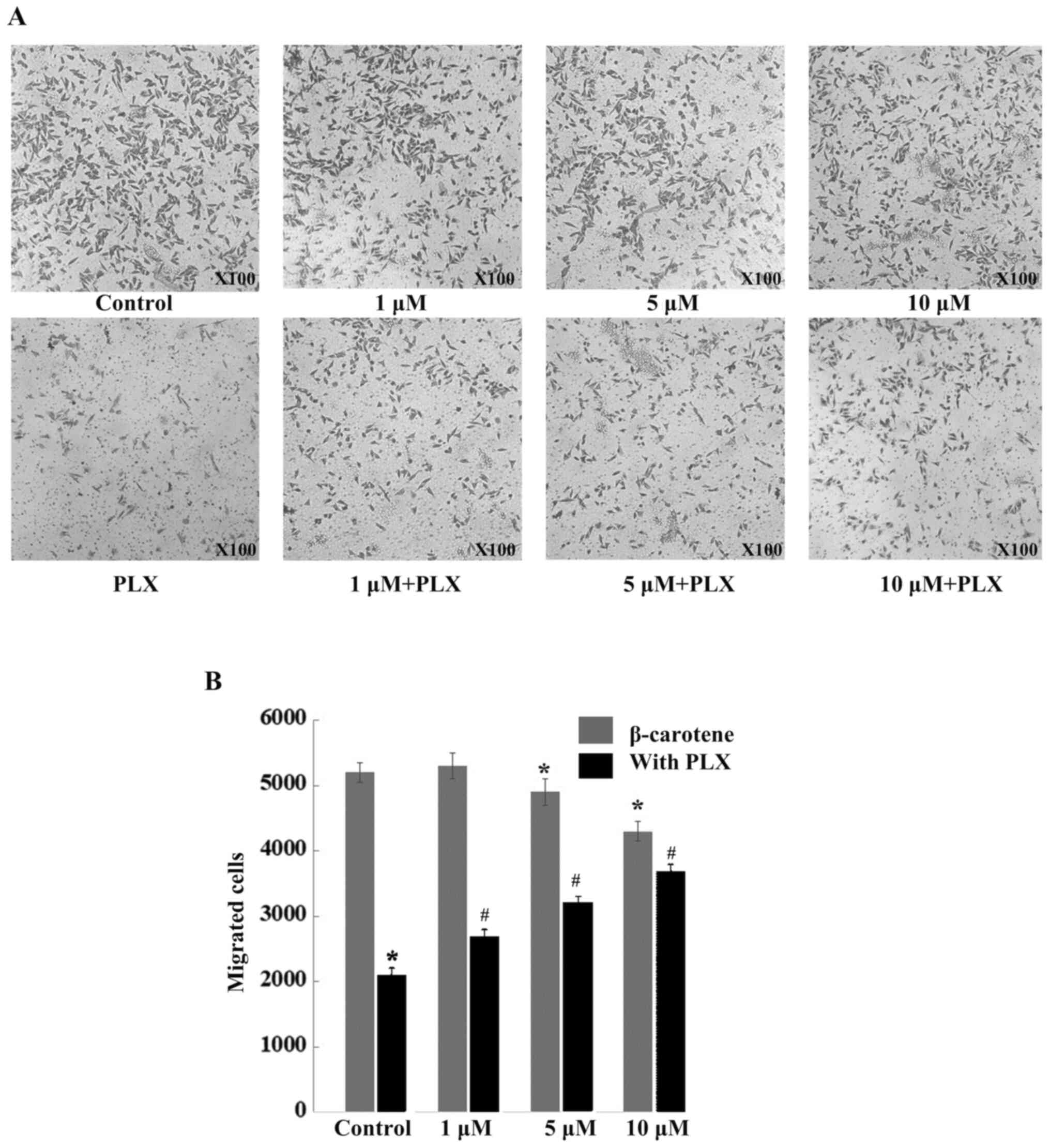
β-carotene inhibits cell invasion, but
alleviates the inhibitory effect of PLX on cell invasion
Since it was reported that β-carotene inhibited lung
metastasis of murine melanoma in vivo (53) and inhibited migration and invasion of
human hepatocarcinoma cells in vitro (65), based on these findings the present
study examined the effects of β-carotene on the invasive ability of
A2058 human melanoma cells and on the inhibitory effect of PLX4032
on cell invasion using a Matrigel-coated Transwell cell invasion
assay. β-carotene alone at 5 and 10 µM significantly decreased
A2058 cell invasion across the cell-permeable microporous membrane
by 6 and 17%, respectively (Fig. 3A and
B). Notably, β-carotene alleviated the inhibitory effect of PLX
on A2058 melanoma cell invasion in a dose-dependent manner
(Fig. 3A and B).
CoQ10 and β-carotene inhibit the
apoptosis induced by PLX in melanoma cells
To determine whether CoQ10 and β-carotene induce
apoptosis and affect apoptosis induced by PLX, SK-MEL-28 and A2058
cells were treated with CoQ10 or β-carotene alone, PLX alone, the
combination of PLX and CoQ10, or a combination of PLX and
β-carotene. CoQ10 at 10 µM inhibited the apoptosis induced by PLX
in A2058 (Fig. 4A and B) and
SK-MEL-28 cells (Fig. 4C and D).
Notably, CoQ10 alone inhibited the apoptosis in SK-MEL-28 cells
(Fig. 4C and D). Similarly,
β-carotene at 10 µM protected A2058 (Fig. 4E and F) and SK-MEL-28 (Fig. 4G and H) from apoptosis induced by
PLX. However, β-carotene alone did not inhibit the apoptosis in
SK-MEL-28 cells (Fig. 4G and H).
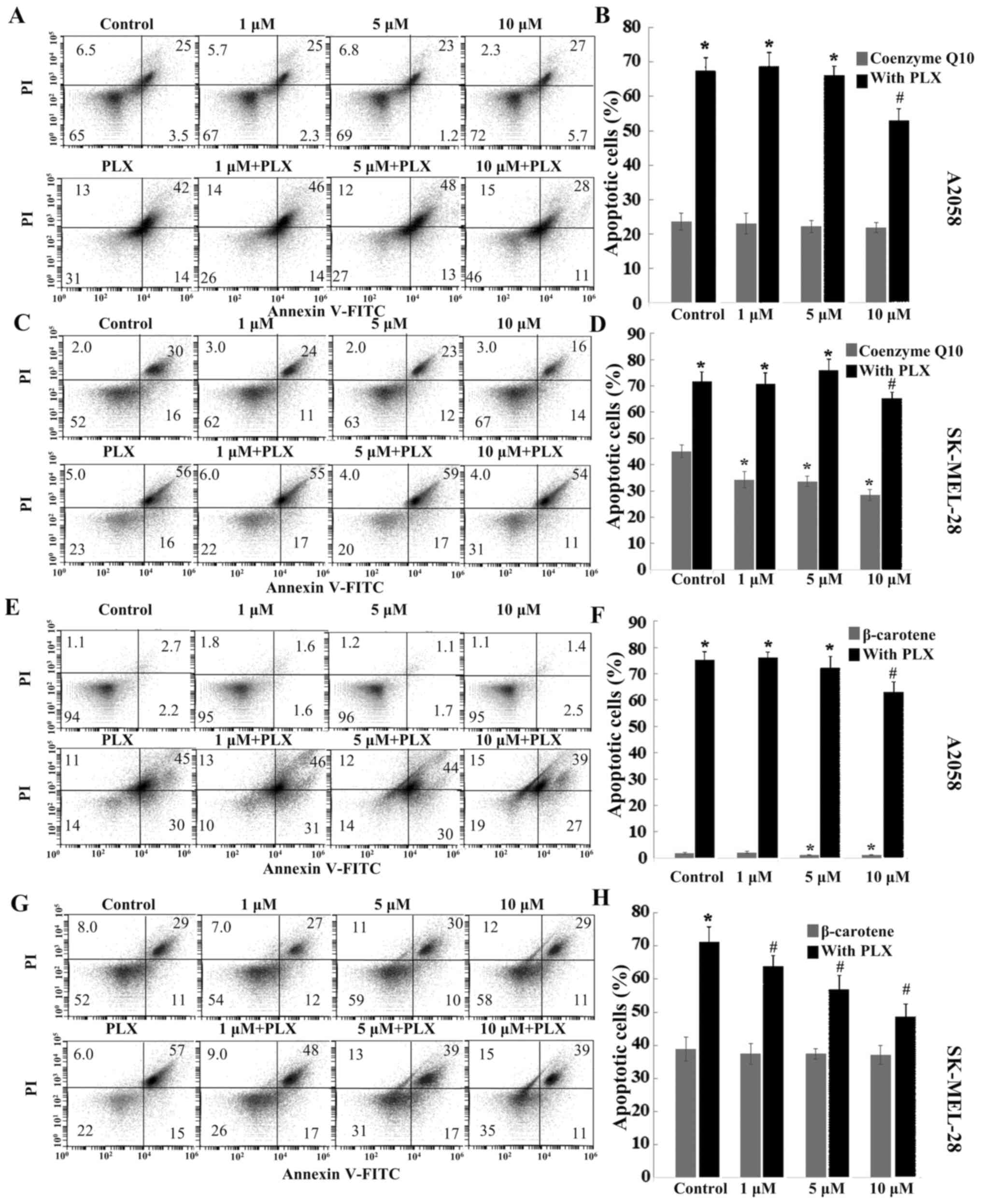 | Figure 4.CoQ10 and β-carotene protect cells
from apoptosis induced by PLX. (A) Apoptosis of A2058 cell treated
with coenzyme Q10 alone, PLX alone, a combination of PLX with
coenzyme Q10, or DMSO vehicle; (B) Quantification of apoptosis
rate. (C) Apoptosis of SK-MEL-28 cells treated with coenzyme Q10
alone, PLX alone, a combination of PLX with coenzyme Q10, or DMSO
vehicle. (D) Quantification of apoptosis rate of panel C. (E)
Apoptosis of A2058 cell treated with β-carotene alone, PLX alone, a
combination of PLX with β-carotene, or DMSO vehicle. (F)
Quantification of apoptosis rate of panel E. (G) Apoptosis of
SK-MEL-28 cells treated with β-carotene alone, PLX alone, a
combination of PLX with β-carotene, or DMSO vehicle. (H)
Quantification of apoptosis rate shown in panel G. *P<0.05,
control group vs. treatment group; #P<0.05, PLX alone
group vs. combined treatment groups (PLX and CoQ10 group or PLX and
β-carotene group). PLX, vemurafenib; PI, propidium iodide. |
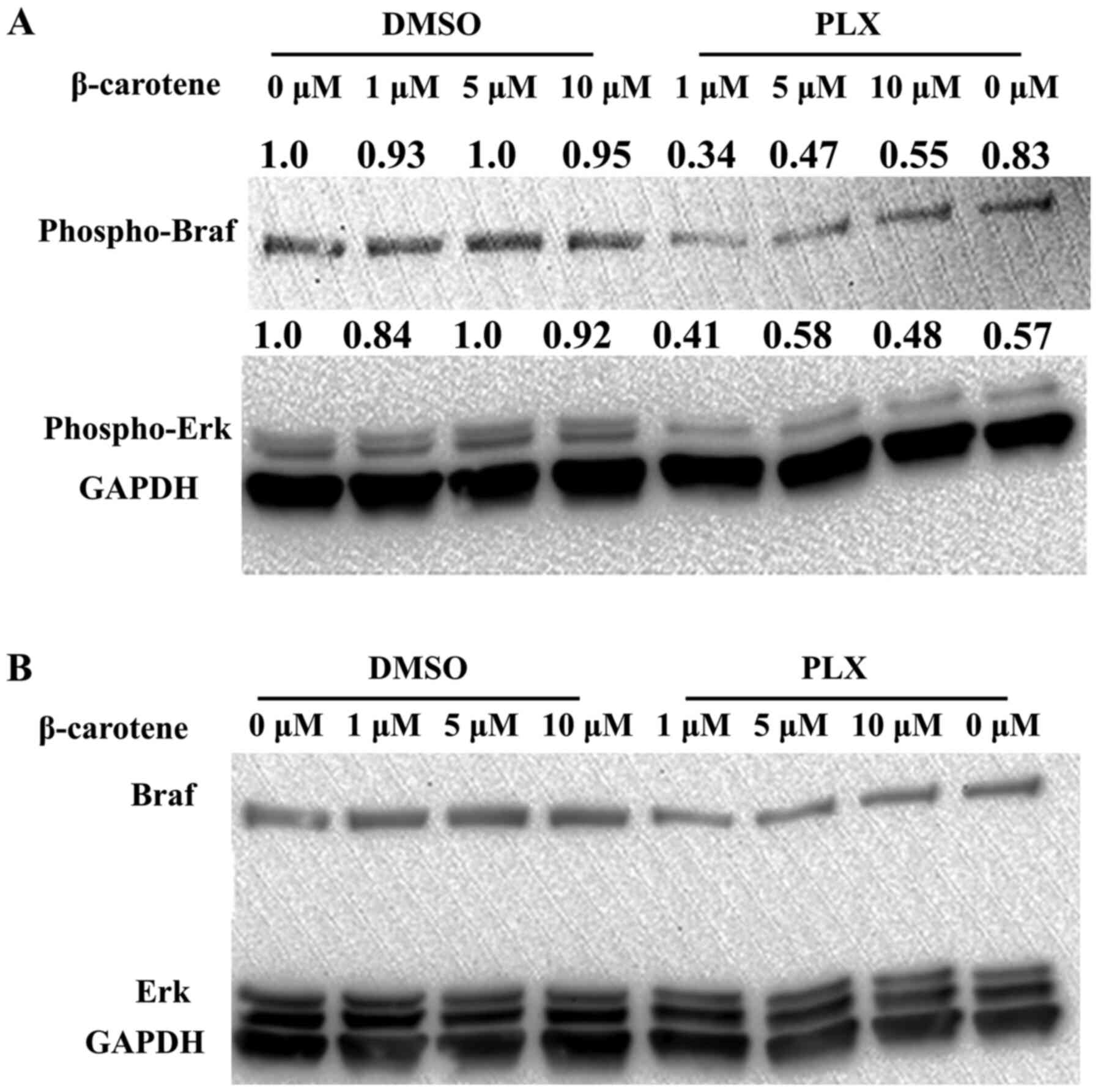
β-carotene works synergistically with
PLX to suppress the Ras-Raf-Mek-Erk pathway
Since the inhibitory effect of CoQ10 on the
signaling pathway has been more established, the present study
examined the effect of β-carotene on the Ras-Raf-Mek-Erk signaling
pathway. Ras-Raf-Mek-Erk is an important intracellular cell growth
signaling pathway and serves critical roles in cancer initiation
and development (66). β-carotene
was found in the present study to inhibit cell migration and
migration/invasion, which are regulated by the Ras-Raf-Mek-Erk
pathway (Fig. 5). In addition,
β-carotene affects the cytotoxicity of veramufenib (Fig. 5), which is a BRAF inhibitor. Based on
these findings the present study investigated the effect of
β-carotene on activation of the Ras-Raf-Mek-Erk signaling pathway.
A2058 cells, which harbor a BRAF activating mutation and are
melanoma resistant, were treated with β-carotene alone, PLX alone,
the combination of PLX and β-carotene, and DMSO vehicle. After 48 h
incubation, western blotting demonstrated that β-carotene had no
effect on BRAF or ERK expression (Fig.
5A and B), indicating that β-carotene alone did not have an
effect on the activation of this pathway. However, β-carotene at a
physiological concentration (1 µM) synergistically worked with PLX
to suppress the activation of BRAF and the downstream Erk1/2
(Fig. 5A and B).
Discussion
Antioxidants are molecules that scavenge free
radicals including ROS, and thus, relieve the oxidative stress of
cells (67). An insufficient level
of antioxidants causes increased oxidative stress that is closely
involved in aging and numerous diseases including cancers (67). Specifically, antioxidants affect
tumor initiation and development through quenching carcinogen
activation, reducing DNA oxidation, switching of growth-related
signal transduction pathways, inducing cell cycle arrest and
inhibiting cell migration and invasion (68). Hence, it is generally believed that
taking antioxidant supplementation is beneficial for the prevention
and treatment of cancers (69).
Numerous research articles advocated antioxidants as cancer
fighters (70–72) and reported that high doses of dietary
antioxidants often inhibit the growth of cancer cells without
affecting the growth of normal cells (71,72). A
population-based prospective cohort study demonstrated that the use
of antioxidants vitamin E and C in the first six months of
diagnosis significantly reduced the mortality and recurrence of
invasive breast cancer (73).
Antioxidants have been used as beneficial adjuncts to the
conventional cancer therapy in clinical studies (74,75).
However, increasing evidence has demonstrated that antioxidants are
not necessarily beneficial in combating cancers. For example, it
has been reported that antioxidants stimulated cell growth in
parotid acinar cells (76). In
addition, the use of antioxidants vitamin E and β-carotene
concurrently with radiotherapy in head and neck cancer patients
significantly increased recurrence and cancer-specific mortality
(25). Hence, whether the use of
antioxidants in cancer prevention and treatment is recommendable
and whether antioxidants exert a synergistic or antagonistic effect
with chemotherapy deserves close scrutiny. The present study
examined the effects of two antioxidants, CoQ10 and β-carotene, on
the viability, migration, invasion, apoptosis, and intracellular
signaling of human malignant melanoma cells. As our previous study
demonstrated that vemurafenib increased the oxidative stress in
human malignant melanoma cells (33), the present study hypothesized that
CoQ10 and β-carotene can affect the cytotoxicity of vemurafenib by
modulating oxidative stress and its downstream effects. The present
study used a venurafenib-resistant melanoma cell line (A2058) to
examine whether the combination of antioxidants with vemurafenib
can produce stronger cytotoxicity against resistant cell lines.
CoQ10 is a free radical-scavenging antioxidant due
to its capacity to act as both a two-electron carrier and a
one-electron carrier (68). Since no
large-scale strictly-controlled clinical trials of coenzyme Q10 in
cancer treatment have been done, the association between coenzyme
Q10 and cancers is not well understood (47). However, the American Cancer Society
has concluded that ‘CoQ10 may reduce the effectiveness
of chemo and radiation therapy, so most oncologists would recommend
avoiding it during cancer treatment’ (77). Research has demonstrated that an
imbalance in the antioxidant system can be detected in melanoma
cells and in a percentage of normal melanocytes from patients with
melanoma (78), and low plasma level
of CoQ10 may be a prognostic factor for melanoma progression
(42). Due to the low concentration
of coenzyme Q10 in melanoma cell lines, and in sera of patients
with melanoma, CoQ10 was used in combination with an optimized dose
of recombinant interferon α-2b in a 3-year trial, which
demonstrated that this combination significantly reduced the
recurrence rate (79). A recent
study reported that the mean of maximum plasma concentration in a
group of healthy volunteers who received 100 mg (Bid) of CoQ10 was
1501 µg/l (1.8 µM) (80). It is also
known that 300 mg per day is a common dosage of commercial products
of coenzyme Q10 (81). Published
research used coenzyme Q10 at concentrations from 5–60 µM (64,82,83). The
present study used CoQ10 at concentrations of 1, 5 and 10 µM that
are achievable in the plasma of CoQ10 supplement-consuming
individuals.
Hong et al (49) reported that coenzyme Q10 did not
suppress the BRAF V600E melanoma cell line. However, by examining
the effect of coenzyme Q10 on the viability of two human malignant
melanoma cell lines in the present study, it was found that CoQ10
significantly reduced the viability of SK-MEL-28 cells, which is a
PLX-sensitive melanoma cell line. In the present study for the
A2058 cell line, which is a PLX-resistant cell line, CoQ10 alone
did not display cytotoxicity. However, it increased the
cytotoxicity of the FDA-approved Braf inhibitor vemurafenib. The
findings of the present study support the notion that CoQ10 can
potentially be a good adjunct to targeted chemotherapy or
immunotherapy against melanoma.
The present study also demonstrated that CoQ10
significantly reduced the migration of both SK-MEL-28 and A2058
cells. To the best of our knowledge, the present study is the first
to have reported the inhibitory effect of CoQ10 on the migration of
cancer cells. It has been previously reported that a functional
dietary supplement containing CoQ10 branched-chain amino acids and
L-carnitine completely inhibited the metastasis of melanoma to the
lung (84). In addition, exogenous
CoQ10 reduced matrix metalloproteinases 2 (MMP-2) activity in a
breast cancer cell line (MCF-7), suggesting the importance of
coenzyme Q10 on cell invasion effector molecules (85). Hence, CoQ10 may inhibit metastasis of
melanoma by directly inhibiting cell migration and reducing MMP-2
activity that helps melanoma cells break through the intracellular
matrix facilitating metastasis.
The present study also examined the effect of CoQ10
on the induction of apoptosis that serves vital roles in tumor
survival and progression. The present study demonstrated that CoQ10
significantly reduced the percentage of apoptotic cells. In
addition, CoQ10 alleviated the apoptosis induced by vemurafenib in
both A2058 and SK-MEL-28 cells. This finding is in concert with
previous reports that demonstrated that CoQ10 protects cells from
undergoing apoptosis induced by cytotoxic chemicals in both
cancerous (86) and non-cancerous
cells (87). Therefore, apoptosis
induction is not a mechanism by which CoQ10 exerts its cytotoxic
effect against melanoma cell lines. In addition, in the present
study CoQ10 potentially mitigated the cytotoxic effect of
chemotherapeutic agents that kill cancer cells primarily through
inducing apoptosis.
The association of β-carotene with cancers is a hot
focus of research. A trial demonstrated that neither β-carotene nor
vitamin A supplement had any beneficial effect in preventing cancer
including melanoma (61). Instead,
increased risk of lung and prostate cancers was found in
participants who consumed β-carotene and had lung irritation from
cigarette smoking or asbestos exposure (88). Another study demonstrated that in
addition to lung cancer, the incidence of gastric cancers was also
significantly increased in individuals who took 20–30mg β-carotene
a day (89). However, other studies
have reported some anticancer activities of β-carotene. For
example, β-carotene at a low physiological concentration inhibited
cell viability and induced apoptosis in human breast cancer MCF-7
cell line (90,91). β-carotene also inhibited lung
metastasis induced by melanoma cells in mice (53). In addition, β-carotene inhibited
angiogenesis and the activation of transcription factors in mouse
melanoma cells (52). The present
study aimed to further characterize the effect of β-carotene on
human malignant melanoma cells. In the present study, β-carotene
did not exhibit inhibitory or promoting effects on the viability of
SK-MEL-28 and A2058 melanoma cells. However, in both cell lines,
β-carotene mitigated the cytotoxic effect of vemurafenib,
suggesting that the intake of β-carotene may decrease the
therapeutic effect of vemurafenib. β-carotene significantly reduced
cell migration and invasion, which was indicated by the ability of
cells to move across the microporous membrane as seen in the
transwell cell migration/invasion assay (Fig. 3). These findings are consistent with
a published work, which reported that β-carotene inhibited the
migration of human umbilical vein endothelial cells by
downregulating the expression of MMP-2 and MMP-9, and by
upregulating the expression of tissue inhibitors of
metalloproteinase (TIMP)-1 and TIMP-2 (52). The present study supports the notion
that β-carotene may inhibit the metastasis of melanoma, which is in
concert with a previous report that demonstrated that β-carotene
inhibited the metastasis of mouse melanoma cells to the lung
(53). However, as in the present
study β-carotene significantly alleviated the inhibition of cell
migration caused by vemurafenib in both the SK-MEL-28 and A2058
cell lines, which raises a concern that β-carotene may suppress the
anti-metastatic effect of vemurafenib.
β-carotene was reported to induce apoptosis by
decreasing the expression of the anti-apoptotic proteins Bcl-2 and
Poly (ADP-ribose) polymerase and the survival protein NF-κB in
breast cancer cells (90). Contrary
to the aforementioned study, the present study demonstrated that
β-carotene did not induce apoptosis in human malignant melanoma
cell lines, suggesting that the apoptosis induction of β-carotene
may be specific to particular types of cancers. In addition,
similar to the effect of β-carotene on the inhibitory effect of
vemurafenib on cell viability and cell migration/invasion,
β-carotene protected cells from apoptosis induction in both the
SK-MEL-28 and A2058 cells induced by vemurafenib in the present
study. This finding also suggests that β-carotene may decrease the
antimelanoma effect of vemurafenib.
Ras-Raf-Mek-Erk is a vital cell-signaling pathway
that regulates cell cycle entry and drives cell proliferation.
Since A2058 cells harbor BRAF activating mutations (92), the present study examined the effect
of β-carotene on the activation of the Ras-Raf-Mek-Erk signaling
pathway. The present study revealed that β-carotene alone did not
have effect on the activation of this pathway, however, β-carotene
at physiological concentration (1 µM) synergistically worked with
vemurafenib to suppress the activation of BRAF and the downstream
Erk1/2. This result is consistent with another study which
demonstrated that β-carotene inhibited Erk1/2 in breast cancer
MCF-7 cells (90). It has been
reported that CoQ10 inhibited activation of Ras-Raf-Mek-Erk
signaling pathway in various cell types, such as fibroblasts and
endothelial cells (93–95). Since the inhibitory effect of CoQ10
on the signaling pathway has been more established, the present
study examined the effect of CoQ10 on the Ras-Raf-Mek-Erk signaling
pathway.
It has been reported that CD8+
tumor-infiltrating lymphocytes (TILs) contributes to the
development of BRAFi resistance (96). The prolonged exposure to BRAFi causes
melanoma cells to become non-proliferative and non-differentiated
cells that are less responsive to TILs (97). Since no study has demonstrated to the
best of our knowledge that CoQ10 or β-carotene regulate the antigen
recognizing activities of TILs, the effect of antioxidants on
CD8+ T cell-mediated BRAFi resistance were not
investigated in the present study.
Antioxidants serve a significant role in the
antiinflammatory mechanism (67). As
oxidative stress leads to inflammatory response, antioxidants can
reduce inflammation by alleviating the oxidative stress (98). Antioxidants, such as CoQ10, suppress
inflammation, ameliorate the autoimmune response and modulate
immune cells including Th17 (99).
It was recently reported that antioxidants can improve adoptive T
cell transfer immunotherapy against tumors by regulating
CD8+ T memory stem cell formation (100). Hence, the effect of CoQ10 on
immunotherapy warrants further study.
The present study had a limitation that it was an
in vitro study. In vitro assays can contribute to
knowledge of direct effects of CoQ10 and β-carotene on melanoma
cells and to elucidate the working mechanisms. However, the actual
biological effects of CoQ10 and β-carotene need to verified in
animal models. Numerous previous studies using coenzyme Q10 as an
adjuvant therapy in human subjects had major flaws, including
taking other supplements that confounded the effect of consumption
of CoQ10 or β-carotene (101,102).
Nevertheless, the synergistic effect of CoQ10 and vemurafenib and
the antagonist effect of β-carotene and vemurafenib need to be
examined in mouse xenograft models in future studies. In addition,
since the cardiocytotoxicity of combination of BRAFi/MEKi has
become a growing problem in the treatment of metastatic melanoma
(103), and CoQ10 is protective
against cardiotoxicity and improves tolerability of cancer
therapeutics (47), the effect of
the combination of CoQ10 and BRAFi/MEKi on melanoma should be the
aim of future studies. In summary, in the present study regardless
of displaying its ability to protect melanoma cells from apoptosis
induction, CoQ10 demonstrated an inhibitory effect on cell
proliferation and migration/invasion when used individually or in
combination with vemurafenib. The cytotoxic effects of CoQ10 make
it a good candidate adjunct for existing standard therapies for
melanoma. In contrast, β-carotene suppressed the anti-melanoma
effects (antiproliferative effect, antiinvasive effect and
apoptosis-inducing effect) of vemurafenib, suggesting that caution
should be taken when β-carotene is used concurrently with
anti-melanoma BRAF inhibitors including vemurafenib.
Acknowledgements
Not applicable.
Funding
The current study was supported by a grant from the
Zhejiang International Science and Technology Cooperation Center
Fund provided by Wenzhou Kean University.
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YY designed and directed the project. CH performed
the experiments. YH and PL performed the experiments. CH wrote the
manuscript. YY revised the manuscript for important intellectual
content. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sandru A, Voinea S, Panaitescu E and
Blidaru A: Survival rates of patients with metastatic malignant
melanoma. J Med Life. 7:572–576. 2014.PubMed/NCBI
|
|
2
|
Karimkhani C, Green AC, Nijsten T,
Weinstock MA, Dellavalle RP, Naghavi M and Fitzmaurice C: The
global burden of melanoma: Results from the global burden of
disease study 2015. Br J Dermatol. 177:134–140. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schadendorf D, van Akkooi ACJ, Berking C,
Griewank KG, Gutzmer R, Hauschild A, Stang A, Roesch A and Ugurel
S: Melanoma. Lancet. 392:971–984. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2020. CA Cancer J Clin. 70:7–30. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Boniol M, Autier P, Boyle P and Gandini S:
Cutaneous melanoma attributable to sunbed use: Systematic review
and meta-analysis. BMJ. 345:e47572012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liu F, Yang X, Geng M and Huang M:
Targeting ERK, an Achilles' Heel of the MAPK pathway, in cancer
therapy. Acta Pharm Sin B. 8:552–562. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chapman PB, Hauschild A, Robert C, Haanen
JB, Ascierto P, Larkin J, Dummer R, Garbe C, Testori A, Maio M, et
al: Improved survival with vemurafenib in melanoma with BRAF V600E
mutation. N Engl J Med. 364:2507–2516. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Menzies AM, Haydu LE, Visintin L, Carlino
MS, Howle JR, Thompson JF, Kefford RF, Scolyer RA and Long GV:
Distinguishing clinicopathologic features of patients with V600E
and V600K BRAF-mutant metastatic melanoma. Clin Cancer Res.
18:3242–3249. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sanchez JN, Wang T and Cohen MS: BRAF and
MEK Inhibitors: Use and resistance in BRAF-mutated cancers. Drugs.
78:549–566. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Livingstone E, Zimmer L, Piel S and
Schadendorf D: PLX4032: Does it keep its promise for metastatic
melanoma treatment? Expert Opin Investig Drugs. 19:1439–1449. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bradish JR, Montironi R, Lopez-Beltran A,
Post KM, MacLennan GT and Cheng L: Towards personalized therapy for
patients with malignant melanoma: Molecular insights into the
biology of BRAF mutations. Future Oncol. 9:245–253. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hamid O, Cowey CL, Offner M, Faries M and
Carvajal RD: Efficacy, Safety, and tolerability of approved
combination BRAF and MEK inhibitor regimens for BRAF-mutant
melanoma. Cancers (Basel). 11:16422019. View Article : Google Scholar
|
|
13
|
Barrueto L, Caminero F, Cash L, Makris C,
Lamichhane P and Deshmukh RR: Resistance to checkpoint inhibition
in cancer immunotherapy. Transl Oncol. 13:1007382020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Flaherty KT, Infante JR, Daud A, Gonzalez
R, Kefford RF, Sosman J, Hamid O, Schuchter L, Cebon J, Ibrahim N,
et al: Combined BRAF and MEK inhibition in melanoma with BRAF V600
mutations. N Engl J Med. 367:1694–1703. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Flaherty KT, Puzanov I, Kim KB, Ribas A,
McArthur GA, Sosman JA, O'Dwyer PJ, Lee RJ, Grippo JF, Nolop K and
Chapman PB: Inhibition of mutated, activated BRAF in metastatic
melanoma. N Engl J Med. 363:809–819. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chang CY, Park H, Malone DC, Wang CY,
Wilson DL, Yeh YM, Van Boemmel-Wegmann S and Lo-Ciganic WH: Immune
checkpoint inhibitors and immune-related adverse events in patients
with advanced melanoma: A systematic review and network
meta-analysis. JAMA Netw Open. 3:e2016112020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wolchok JD, Chiarion-Sileni V, Gonzalez R,
Rutkowski P, Grob JJ, Cowey CL, Lao CD, Wagstaff J, Schadendorf D,
Ferrucci PF, et al: Overall survival with combined nivolumab and
ipilimumab in advanced melanoma. N Engl J Med. 377:1345–1356. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ascierto PA, Del Vecchio M, Robert C,
Mackiewicz A, Chiarion-Sileni V, Arance A, Lebbé C, Bastholt L,
Hamid O, Rutkowski P, et al: Ipilimumab 10 mg/kg versus ipilimumab
3 mg/kg in patients with unresectable or metastatic melanoma: A
randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol.
18:611–622. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hodi FS, Chesney J, Pavlick AC, Robert C,
Grossmann KF, McDermott DF, Linette GP, Meyer N, Giguere JK,
Agarwala SS, et al: Combined nivolumab and ipilimumab versus
ipilimumab alone in patients with advanced melanoma: 2-year overall
survival outcomes in a multicentre, randomised, controlled, phase 2
trial. Lancet Oncol. 17:1558–1568. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Robert C, Schachter J, Long GV, Arance A,
Grob JJ, Mortier L, Daud A, Carlino MS, McNeil C, Lotem M, et al:
Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med.
372:2521–2532. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Larkin J, Chiarion-Sileni V, Gonzalez R,
Grob JJ, Rutkowski P, Lao CD, Cowey CL, Schadendorf D, Wagstaff J,
Dummer R, et al: Five-year survival with combined nivolumab and
ipilimumab in advanced melanoma. N Engl J Med. 381:1535–1546. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Dummer R, Ascierto PA, Nathan P, Robert C
and Schadendorf D: Rationale for immune checkpoint inhibitors plus
targeted therapy in metastatic melanoma: A review. JAMA Oncol. Sep
24–2020.doi: 10.1001/jamaoncol.2020.4401 (Epub ahead of print).
View Article : Google Scholar
|
|
23
|
Godic A, Poljsak B, Adamic M and Dahmane
R: The role of antioxidants in skin cancer prevention and
treatment. Oxid Med Cell Longev. 2014:8604792014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ahmad R, Wani A and Ahsan H: Role of
antioxidants in pathophysiology. J Med Erudite. 2:9–15. 2013.
|
|
25
|
Bairati I, Meyer F, Gélinas M, Fortin A,
Nabid A, Brochet F, Mercier JP, Têtu B, Harel F, Mâsse B, et al: A
randomized trial of antioxidant vitamins to prevent second primary
cancers in head and neck cancer patients. J Natl Cancer Inst.
97:481–488. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Devasagayam TP, Tilak JC, Boloor KK, Sane
KS, Ghaskadbi SS and Lele RD: Free radicals and antioxidants in
human health: Current status and future prospects. J Assoc
Physicians India. 52:794–804. 2004.PubMed/NCBI
|
|
27
|
Ma J, Zhang Q, Chen S, Fang B, Yang Q,
Chen C, Miele L, Sarkar FH, Xia J and Wang Z: Mitochondrial
dysfunction promotes breast cancer cell migration and invasion
through HIF1alpha accumulation via increased production of reactive
oxygen species. PLoS One. 8:e694852013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kvam E and Tyrrell RM: The role of melanin
in the induction of oxidative DNA base damage by ultraviolet A
irradiation of DNA or melanoma cells. J Invest Dermatol.
113:209–213. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sun L, Guo Y, Zhang Y and Zhuang Y:
Antioxidant and Anti-tyrosinase activities of phenolic extracts
from rape bee pollen and inhibitory melanogenesis by cAMP/MITF/TYR
pathway in B16 mouse melanoma cells. Front Pharmacol. 8:1042017.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Umemura T, Naoi M, Takahashi T, Fukui Y,
Yasue T, Ohashi M and Nagatsu T: Cytotoxic effect of
1-methyl-4-phenylpyridinium ion on human melanoma cell lines,
HMV–II and SK-MEL-44, is dependent on the melanin contents and
caused by inhibition of mitochondrial electron transport. Biochem
Med Metab Biol. 44:51–58. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Oliveira S, Coelho P, Prudêncio C, Vieira
M, Soares R, Guerreiro SG and Fernandes R: Melanoma and obesity:
Should antioxidant vitamins be addressed? Life Sci. 165:83–90.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sarangarajan R, Meera S, Rukkumani R,
Sankar P and Anuradha G: Antioxidants: Friend or foe? Asian Pac J
Trop Med. 10:1111–1116. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yang G, Yan Y, Ma Y and Yang Y: Vitamin C
at high concentrations induces cytotoxicity in malignant melanoma
but promotes tumor growth at low concentrations. Mol Carcinog.
56:1965–1976. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Le Gal K, Ibrahim MX, Wiel C, Sayin VI,
Akula MK, Karlsson C, Dalin MG, Akyürek LM, Lindahl P, Nilsson J
and Bergo MO: Antioxidants can increase melanoma metastasis in
mice. Sci Transl Med. 7:308re3082015. View Article : Google Scholar
|
|
35
|
Piskounova E, Agathocleous M, Murphy MM,
Hu Z, Huddlestun SE, Zhao Z, Leitch AM, Johnson TM, DeBerardinis RJ
and Morrison SJ: Oxidative stress inhibits distant metastasis by
human melanoma cells. Nature. 527:186–191. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Poljsak B and Milisav I: The role of
antioxidants in cancer, friends or foes? Curr Pharm Des.
24:5234–5244. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Yamamoto Y and Yamashita S: Plasma ratio
of ubiquinol and ubiquinone as a marker of oxidative stress. Mol
Aspects Med. 18 (Suppl):S79–S84. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Saha SP and Whayne TF Jr: Coenzyme Q-10 in
human health: Supporting evidence? South Med J. 109:17–21. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Overvad K, Diamant B, Holm L, Holmer G,
Mortensen SA and Stender S: Coenzyme Q10 in health and disease. Eur
J Clin Nutr. 53:764–770. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Folkers K, Osterborg A, Nylander M, Morita
M and Mellstedt H: Activities of vitamin Q10 in animal models and a
serious deficiency in patients with cancer. Biochem Biophys Res
Commun. 234:296–299. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Folkers K: The potential of coenzyme Q10
(NSC-140865) in cancer treatment. Cancer Chemother Rep. 2(4):
19–22. 1974.
|
|
42
|
Rusciani L, Proietti I, Rusciani A,
Paradisi A, Sbordoni G, Alfano C, Panunzi S, De Gaetano A and Lippa
S: Low plasma coenzyme Q10 levels as an independent prognostic
factor for melanoma progression. J Am Acad Dermatol. 54:234–241.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Jolliet P, Simon N, Barré J, Pons JY,
Boukef M, Paniel BJ and Tillement JP: Plasma coenzyme Q10
concentrations in breast cancer: Prognosis and therapeutic
consequences. Int J Clin Pharmacol Ther. 36:506–509.
1998.PubMed/NCBI
|
|
44
|
El-Attar E, Kamel A, Karmouty A, Wehida N,
Nassra R, El Nemr M and Kandil NS: Assessment of serum CoQ10 levels
and other antioxidant markers in breast cancer. Asian Pac J Cancer
Prev. 21:465–471. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Lund EL, Quistorff B, Spang-Thomsen M and
Kristjansen PE: Effect of radiation therapy on small-cell lung
cancer is reduced by ubiquinone intake. Folia Microbiol (Praha).
43:505–506. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Lockwood K, Moesgaard S and Folkers K:
Partial and complete regression of breast cancer in patients in
relation to dosage of coenzyme Q10. Biochem Biophys Res Commun.
199:1504–1508. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Roffe L, Schmidt K and Ernst E: Efficacy
of coenzyme Q10 for improved tolerability of cancer treatments: A
systematic review. J Clin Oncol. 22:4418–4424. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Coenzyme Q10 (PDQ(R)): Health Professional
Version. PDQ Cancer Information Summaries Bethesda, MD: 2002
|
|
49
|
Hong SK, Starenki D, Wu PK and Park JI:
Suppression of B-RafV600E melanoma cell survival by targeting
mitochondria using triphenyl-phosphonium-conjugated nitroxide or
ubiquinone. Cancer Biol Ther. 18:106–114. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Diplock AT: Safety of antioxidant vitamins
and beta-carotene. Am J Clin Nutr. 62 (Suppl 6):1510S–1516S. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Fiedor J and Burda K: Potential role of
carotenoids as antioxidants in human health and disease. Nutrients.
6:466–488. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Guruvayoorappan C and Kuttan G:
Beta-carotene inhibits tumor-specific angiogenesis by altering the
cytokine profile and inhibits the nuclear translocation of
transcription factors in B16F-10 melanoma cells. Integr Cancer
Ther. 6:258–270. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Pradeep CR and Kuttan G: Effect of
beta-carotene on the inhibition of lung metastasis in mice.
Phytomedicine. 10:159–164. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
IARC Working Group on the Evaluation of
Cancer-Preventive Agents, . IARC Handbooks of Cancer Prevention.
Carotenoids; Lyon; 1998
|
|
55
|
Mayne ST, Handelman GJ and Beecher G:
Beta-carotene and lung cancer promotion in heavy smokers-a
plausible relationship? J Natl Cancer Inst. 88:1513–1515. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Stryker WS, Stampfer MJ, Stein EA, Kaplan
L, Louis TA, Sober A and Willett WC: Diet, plasma levels of
beta-carotene and alpha-tocopherol, and risk of malignant melanoma.
Am J Epidemiol. 131:597–611. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Epstein JH: Effects of beta-carotene on
ultraviolet induced cancer formation in the hairless mouse skin.
Photochem Photobiol. 25:211–213. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Black HS: Radical interception by
carotenoids and effects on UV carcinogenesis. Nutr Cancer.
31:212–217. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Alpha-Tocopherol, Beta Carotene Cancer
Prevention Study Group: The effect of vitamin E and beta carotene
on the incidence of lung cancer and other cancers in male smokers.
N Engl J Med. 330:1029–1035. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Middha P, Weinstein SJ, Mannisto S,
Albanes D and Mondul AM: β-carotene supplementation and lung cancer
incidence in the alpha-tocopherol, beta-carotene cancer prevention
study: The role of tar and nicotine. Nicotine Tob Res.
21:1045–1050. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Zhang YP, Chu RX and Liu H: Vitamin A
intake and risk of melanoma: A meta-analysis. PLoS One.
9:e1025272014. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Chen HY, Huang SM, Yang CM and Hu ML:
Diverse effects of β-carotene on secretion and expression of VEGF
in human hepatocarcinoma and prostate tumor cells. Molecules.
17:3981–3988. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Jang M, Kim SS and Lee J: Cancer cell
metabolism: Implications for therapeutic targets. Exp Mol Med.
45:e452013. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Wang HM, Yang HL, Thiyagarajan V, Huang
TH, Huang PJ, Chen SC, Liu JY, Hsu LS, Chang HW and Hseu YC:
Coenzyme Q0 enhances ultraviolet b-induced apoptosis in human
estrogen receptor-positive breast (MCF-7) cancer cells. Integr
Cancer Ther. 16:385–396. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Chen HY, Yang CM, Chen JY, Yueh TC and Hu
ML: Multicarotenoids at physiological levels inhibit metastasis in
human hepatocarcinoma SK-Hep-1 cells. Nutr Cancer. 67:676–686.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
McCubrey JA, Steelman LS, Chappell WH,
Abrams SL, Wong EW, Chang F, Lehmann B, Terrian DM, Milella M,
Tafuri A, et al: Roles of the Raf/MEK/ERK pathway in cell growth,
malignant transformation and drug resistance. Biochim Biophys Acta.
1773:1263–1284. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Lobo V, Patil A, Phatak A and Chandra N:
Free radicals, antioxidants and functional foods: Impact on human
health. Pharmacogn Rev. 4:118–126. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Bowman BA and Russell RM: Present
Knowledge in Nutrition. ILSI Press; Washington D.C.: 2006
|
|
69
|
Hajhashemi V, Vaseghi G, Pourfarzam M and
Abdollahi A: Are antioxidants helpful for disease prevention? Res
Pharm Sci. 5:1–8. 2010.PubMed/NCBI
|
|
70
|
Salganik RI: The benefits and hazards of
antioxidants: Controlling apoptosis and other protective mechanisms
in cancer patients and the human population. J Am Coll Nutr. 20
(Suppl 5):464S–475S. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Prasad KN, Kumar A, Kochupillai V and Cole
WC: High doses of multiple antioxidant vitamins: Essential
ingredients in improving the efficacy of standard cancer therapy. J
Am Coll Nutr. 18:13–25. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Prasad KN, Cole WC, Kumar B and Prasad KC:
Scientific rationale for using high-dose multiple micronutrients as
an adjunct to standard and experimental cancer therapies. J Am Coll
Nutr. 20 (5 Suppl):450S–463S; discussion 473S-475S. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Nechuta S, Lu W, Chen Z, Zheng Y, Gu K,
Cai H, Zheng W and Shu XO: Vitamin supplement use during breast
cancer treatment and survival: A prospective cohort study. Cancer
Epidemiol Biomarkers Prev. 20:262–271. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Lecumberri E, Dupertuis YM, Miralbell R
and Pichard C: Green tea polyphenol epigallocatechin-3-gallate
(EGCG) as adjuvant in cancer therapy. Clin Nutr. 32:894–903. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Seely D, Wu P, Fritz H, Kennedy DA, Tsui
T, Seely AJ and Mills E: Melatonin as adjuvant cancer care with and
without chemotherapy: A systematic review and meta-analysis of
randomized trials. Integr Cancer Ther. 11:293–303. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Prasad KN and Kumar R: Effect of
individual and multiple antioxidant vitamins on growth and
morphology of human nontumorigenic and tumorigenic parotid acinar
cells in culture. Nutr Cancer. 26:11–19. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Jaber S and Polster BM: Idebenone and
neuroprotection: Antioxidant, pro-oxidant, or electron carrier? J
Bioenerg Biomembr. 47:111–118. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Picardo M, Grammatico P, Roccella F,
Roccella M, Grandinetti M, Del Porto G and Passi S: Imbalance in
the antioxidant pool in melanoma cells and normal melanocytes from
patients with melanoma. J Invest Dermatol. 107:322–326. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Rusciani L, Proietti I, Paradisi A,
Rusciani A, Guerriero G, Mammone A, De Gaetano A and Lippa S:
Recombinant interferon alpha-2b and coenzyme Q10 as a postsurgical
adjuvant therapy for melanoma: A 3-year trial with recombinant
interferon-alpha and 5-year follow-up. Melanoma Res. 17:177–183.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Martucci A, Reurean-Pintilei D and Manole
A: Bioavailability and sustained plasma concentrations of CoQ10 in
healthy volunteers by a novel oral timed-release preparation.
Nutrients. 11:5272019. View Article : Google Scholar
|
|
81
|
Lee BJ, Tseng YF, Yen CH and Lin PT:
Effects of coenzyme Q10 supplementation (300 mg/day) on
antioxidation and anti-inflammation in coronary artery disease
patients during statins therapy: A randomized, placebo-controlled
trial. Nutr J. 12:1422013. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Frontinan-Rubio J, Santiago-Mora RM,
Nieva-Velasco CM, Ferrín G, Martínez-González A, Gómez MV, Moreno
M, Ariza J, Lozano E, Arjona-Gutiérrez J, et al: Regulation of the
oxidative balance with coenzyme Q10 sensitizes human glioblastoma
cells to radiation and temozolomide. Radiother Oncol. 128:236–244.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Abdulhasan MK, Li Q, Dai J, Abu-Soud HM,
Puscheck EE and Rappolee DA: CoQ10 increases mitochondrial mass and
polarization, ATP and Oct4 potency levels, and bovine oocyte MII
during IVM while decreasing AMPK activity and oocyte death. J
Assist Reprod Genet. 34:1595–1607. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Awa H, Futamura A, Higashiguchi T, Ito A,
Mori N, Murai M, Ohara H, Chihara T and Kaneko T: Effects of
combined treatment with branched-chain amino acids, citric acid,
L-carnitine, coenzyme Q10, zinc, and various vitamins in
tumor-bearing mice. Biol Pharm Bull. 40:266–271. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Bahar M, Khaghani S, Pasalar P, Paknejad
M, Khorramizadeh MR, Mirmiranpour H and Nejad SG: Exogenous
coenzyme Q10 modulates MMP-2 activity in MCF-7 cell line as a
breast cancer cellular model. Nutr J. 9:622010. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Qi XF, Kim DH, Yoon YS, Kim SK, Cai DQ,
Teng YC, Shim KY and Lee KJ: Involvement of oxidative stress in
simvastatin-induced apoptosis of murine CT26 colon carcinoma cells.
Toxicol Lett. 199:277–287. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Ashkani-Esfahani S, Bagheri F, Emami Y,
Esmaeilzadeh E, Azarpira N, Hassanabadi N, Keshtkar M, Farjam M,
Koohi-Hosseinabadi O and Noorafshan A: Protective effects of
Co-Enzyme Q10 on thioacetamide-induced acute liver damage and its
correlation with behavioral, biochemical, and pathological factors.
Iran Red Crescent Med J. 18:e291662016. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Omenn GS, Goodman GE, Thornquist MD,
Balmes J, Cullen MR, Glass A, Keogh JP, Meyskens FL Jr, Valanis B,
Williams JH Jr, et al: Risk factors for lung cancer and for
intervention effects in CARET, the beta-carotene and retinol
efficacy trial. J Natl Cancer Inst. 88:1550–1559. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Druesne-Pecollo N, Latino-Martel P, Norat
T, Barrandon E, Bertrais S, Galan P and Hercberg S: Beta-carotene
supplementation and cancer risk: A systematic review and
metaanalysis of randomized controlled trials. Int J Cancer.
127:172–184. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Sowmya Shree G, Yogendra Prasad K, Arpitha
HS, Deepika UR, Nawneet Kumar K, Mondal P and Ganesan P: β-carotene
at physiologically attainable concentration induces apoptosis and
down-regulates cell survival and antioxidant markers in human
breast cancer (MCF-7) cells. Mol Cell Biochem. 436:1–12. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Shultz TD, Chew BP, Seaman WR and Luedecke
LO: Inhibitory effect of conjugated dienoic derivatives of linoleic
acid and beta-carotene on the in vitro growth of human cancer
cells. Cancer Lett. 63:125–133. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Mebratu Y and Tesfaigzi Y: How ERK1/2
activation controls cell proliferation and cell death: Is
subcellular localization the answer? Cell Cycle. 8:1168–1175. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Choi JS, Park SY, Yi EY, Kim YJ and Jeong
JW: Coenzyme Q10 decreases basic fibroblast growth factor
(bFGF)-induced angiogenesis by blocking ERK activation. Oncol Res.
19:455–461. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Zhao Q, Ma YM, Jing L, Zheng TX, Jiang HF,
Li PA and Zhang JZ: Coenzyme Q10 protects astrocytes from
ultraviolet B-induced damage through inhibition of ERK 1/2 pathway
overexpression. Neurochem Res. 44:1755–1763. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Shin JY, Choi JW, Kim DG, Zhou ZQ, Shin
YK, Seo JH, Song HJ, Choi BM, Bae GS and Park SJ: Protective
effects of Coenzyme Q10 against acute pancreatitis. Int
Immunopharmacol. 88:1069002020. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Atay C, Kwak T, Lavilla-Alonso S,
Donthireddy L, Richards A, Moberg V, Pilon-Thomas S, Schell M,
Messina JL, Rebecca VW, et al: BRAF targeting sensitizes resistant
melanoma to cytotoxic T cells. Clin Cancer Res. 25:2783–2794. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Pieper N, Zaremba A, Leonardelli S,
Harbers FN, Schwamborn M, Lübcke S, Schrörs B, Baingo J, Schramm A,
Haferkamp S, et al: Evolution of melanoma cross-resistance to
CD8+ T cells and MAPK inhibition in the course of BRAFi
treatment. Oncoimmunology. 7:e14501272018. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Tan BL, Norhaizan ME, Liew WP and Sulaiman
Rahman H: Antioxidant and oxidative stress: A mutual interplay in
age-related diseases. Front Pharmacol. 9:11622018. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Jhun J, Lee SH, Byun JK, Jeong JH, Kim EK,
Lee J, Jung YO, Shin D, Park SH and Cho ML: Coenzyme Q10 suppresses
Th17 cells and osteoclast differentiation and ameliorates
experimental autoimmune arthritis mice. Immunol Lett. 166:92–102.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Pilipow K, Scamardella E, Puccio S, Gautam
S, De Paoli F, Mazza EM, De Simone G, Polletti S, Buccilli M, Zanon
V, et al: Antioxidant metabolism regulates CD8+ T memory
stem cell formation and antitumor immunity. JCI Insight.
3:e1222992018. View Article : Google Scholar
|
|
101
|
Molyneux SL, Young JM, Florkowski CM,
Lever M and George PM: Coenzyme Q10: Is there a clinical role and a
case for measurement? Clin Biochem Rev. 29:71–82. 2008.PubMed/NCBI
|
|
102
|
Toti E, Chen CO, Palmery M, Villaño
Valencia D and Peluso I: Non-provitamin A and provitamin A
carotenoids as immunomodulators: Recommended dietary allowance,
therapeutic index, or personalized nutrition? Oxid Med Cell Longev.
2018:46378612018. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Bronte E, Bronte G, Novo G, Rinaldi G,
Bronte F, Passiglia F and Russo A: Cardiotoxicity mechanisms of the
combination of BRAF-inhibitors and MEK-inhibitors. Pharmacol Ther.
192:65–73. 2018. View Article : Google Scholar : PubMed/NCBI
|