Introduction
Diffuse large B-cell lymphoma (DLBCL) is one of the
most common subtypes of Non-Hodgkin's lymphoma (NHL) in adults,
accounting for ~30% of NHLs (1).
DLBCL has significant heterogeneity in clinical manifestations,
biological characteristics, and prognosis (2–4).
Although >50% of patients with DLBCL may be cured by upfront
chemoimmunotherapy (2), ~40–50% of
patients relapse and/or the disease becomes refractory, and it is
estimated that one third of patients will eventually die of the
disease (5).
Given the notable heterogeneity within DLBCL, an
accurate and reliable prediction tool is essential to optimize the
treatment of patients. Since 1993, the international prognostic
index (IPI) has become a major clinical predictive tool for the
prognosis of patients with DLBCL (6). Based on the number of adverse
prognostic factors, four independent risk groups were identified,
and the 5-year overall survival (OS) rate was between 26–73%
(6). However, as rituximab
significantly improves the prognosis of patients with DLBCL, use of
the IPI in identifying high-risk groups is questionable (7,8).
In 2014, Zhou et al (9) proposed the National Comprehensive
Cancer Network (NCCN)-IPI based on IPI, which highlights the
prognostic effects of age, lactate dehydrogenase (LDH) level and
extranodal involvement site. Although previous studies have
reported that the NCCN-IPI has better risk stratification than the
IPI between low-risk and high-risk DLBCL (5-year OS, 96% vs. 33%
for NCCN-IPI; 5-year OS 90% vs. 54% for IPI), NCCN-IPI fails to
identify extremely high-risk populations (10–13). As
was the case with its predecessor, the prognostic factors of
NCCN-IPI mainly come from the clinical indicators of DLBCL
(14). However, the model does not
contain information obtained from standardized imaging
techniques.
Positron Emission Tomography-Computed Tomography
(PET/CT) has great value in the accurate staging, evaluation of
efficacy, determination of prognosis and guidance for the
subsequent treatment of malignant lymphoma (15–17).
High fluorodeoxyglucose (FDG) uptake is a surrogate indicator of
aggressive biological characteristics of malignant lymphoma
(18). The total metabolic tumor
volume (TMTV) assessed by PET/CT can be used as an index to measure
tumor volume and invasiveness (18).
Previous studies have demonstrated that TMTV has a greater
prognostic value than Ann Arbor stage and can be used as a
prognostic factor independent of IPI (19,20).
High TMTV is associated with poor progression-free survival (PFS)
(21). Analyses from the GOYA study
revealed that higher TMTV is significantly associated with poor
prognosis in patients independent of IPI (22). Notably, quantitative tumor imaging
indicators, such as TMTV have the potential to replace traditional
IPI factors that reflect tumor burden, such as extranodal diseases
and Ann Arbor stage (19,20).
Thus, in the era of immunochemotherapy, the present
study aimed to design a novel prognostic model of DLBCL composed of
standardized imaging techniques and clinical parameters, and to
assess its prognostic value in patients with DLBCL.
Patients and methods
Patients and data collection
This retrospective study included 169 patients
treated at Tianjin Medical University Cancer Institute and Hospital
between January 2011 and December 2017. The present study was
approved by the Institutional Review Board of the Tianjin Medical
University Cancer Institute and Hospital (Tianjin, China) and
written informed consent was obtained from all the patients. The
inclusion criteria were as follows: i) Age (>18 years),
regardless of sex; ii) CD20 positive patients with DLBCL who had
not received treatment in the past and iii) first-line treatment
options were rituximab, cyclophosphamide, doxorubicin, vincristine
and prednisone (RCHOP) or RCHOP-like regimens. Diagnosis of DLBCL
was confirmed by Dr. Meng and Dr. Zhai from the Department of
Pathology at The Tianjin Medical University Cancer Hospital
(Tianjin, China). The immunohistochemical markers CD10, BCL-6 and
multiple myeloma oncogene 1 were detected and patients were
subsequently divided into germinal-center B-cell-like (GCB) or
non-GCB subtypes, using Hans' algorithm (23). All patients were restaged according
to the Lugano classification system (24). Bulky disease was defined as a
measurable tumor mass ≥7.5 cm in diameter.
The IPI includes five risk factors: Age (>60
years), LDH above upper normal value, the involvement of
extra-lymph node tissues or organs >1, Eastern Cooperative
Oncology Group (ECOG) score ≥2 and disease stage III/IV (6). According to the number of poor
prognostic factors, IPI divided patients into four groups: Low-risk
group, low-intermediate risk group, intermediate-high risk group
and high-risk group. The NCCN-IPI relies on the same five poor
prognostic indicators as the IPI, but the patient's age, elevated
LDH levels and specific extranodal involvement are more heavily
weighted (9). Patients were also
divided into four groups by the NCCN-IPI (Table I).
 | Table I.Characteristics and scoring of the
different systems. |
Table I.
Characteristics and scoring of the
different systems.
| Characteristic | IPI | Score | NCCN-IPI | Score | M-PM | Score |
|---|
| Age, years | NA | 0 | >40 to ≤60 | 1 | NA | 0 |
|
| >60 | 1 | >60 to ≤75 | 2 | ≥65 | 1 |
|
| NA | 0 | >75 | 3 | NA | 0 |
| Ann Arbor
stage | III–IV | 1 | III–IV | 1 | NA | 0 |
| LDH,
normalized | >1 | 1 | >1 to ≤3 | 1 | >1 | 1 |
|
| NA | 0 | >3 | 2 | NA | 0 |
| Extranodal
disease | ≥2 | 1 | NA | 0 | NA | 0 |
| aDistinct extranodal disease | NA | 0 | Any | 1 | NA | 0 |
| Performance
status | ≥2 | 1 | ≥2 | 1 | ≥2 | 1 |
| COO | NA | 0 | NA | 0 | NA | 0 |
| TMTV,
cm3 | NA | 0 | NA | 0 | ≥300 | 1 |
| Maximum score | NA | 5 | NA | 8 | NA | 4 |
PET imaging
All patients underwent FDG PET/CT scanning prior to
chemotherapy. PET/CT studies were performed according to protocols
and manufacturer guidelines (25). A
total of two experienced nuclear medicine experts calculated the
quantitative parameters. The TMTV was obtained by summarizing the
metabolic volume of all lymph nodes and extra-lymph node lesions.
Bone marrow involvement was included in the volume measurement only
in the presence of focal uptake. The spleen was involved if the
focal or disseminated uptake was >150% of the liver
background.
Statistical analysis
Statistical analysis was performed using SPSS 22
software (IBM Corp.). OS time refers to the time from random
assignment to mortality for any reason (lost follow-up is the last
follow-up time; patients who are still alive at the end of the
study are the end date of follow-up) (26). PFS refers to the time from the start
of randomization to the first tumor progression, relapse, mortality
or last contact (26). The
Kaplan-Meier method was used to calculate OS and PFS time, and the
log-rank test was used to determine statistically significant
differences between the two groups. Univariate and multivariate
analyses were performed according to the Cox regression model to
assess prognostic value. P≤0.05 was considered to indicate a
statistically significant difference.
Results
Clinical characteristics of
patients
The clinical characteristics of the 169 patients are
presented in Table II. The
patients' median follow-up time was 60 months. All patients
received induction chemotherapy containing R-CHOP or RCHOP-like
regimens, and 88.8 and 11.2% received RCHOP and R-mini-CHOP,
respectively. A total of 49 patients (29.0%) were >65 years old
and men have slightly more cases than women (53.3%). There were 25
patients (14.8%) with bulky disease (mass >7.5 cm). The
involvement of bone marrow occurred in 23 cases (13.6%). A total of
52 patients (30.8%) were diagnosed at stage I–II, while the
remaining 117 patients (69.2%) were diagnosed at stage III–IV. A
total of 99 patients (58.6%) had elevated LDH levels, and 28
patients (16.6%) had an ECOG performance status ≥2. Extranodal
involvement was present in 43 patients (25.4%). According to the
IPI, 56 patients (33.1%) and 35 patients (20.7%) had low or
low-intermediate IPI scores, respectively, whereas 44 patients
(26.1%) and 34 patients (20.1%) were categorized as
intermediate-high or high risk, respectively. According to the
NCCN-IPI, 42 cases (24.9%) were classified as low risk, 51 as
low-intermediate risk, 48 as intermediate-high and 28 cases as high
risk. Notably, fewer patients were classified as low risk by the
NCCN-IPI compared with the traditional IPI.
| Table II.Clinical characteristics of patients
(n=169). |
Table II.
Clinical characteristics of patients
(n=169).
| Characteristic | Number of patients,
n (%) |
|---|
| Age, years |
|
|
<65 | 120 (71.0) |
|
≥65 | 49 (29.0) |
| Sex |
|
|
Male | 90 (53.3) |
|
Female | 79 (46.7) |
| Presence of
B-symptoms |
|
| No | 118 (69.8) |
|
Yes | 51 (30.2) |
| Performance
status |
|
|
0–1 | 141 (83.4) |
| ≥2 | 28 (16.6) |
| Serum LDH |
|
|
Normal | 70 (41.4) |
|
Elevated | 99 (58.6) |
| Stage |
|
|
I–II | 52 (30.8) |
|
III–IV | 117 (69.2) |
| Extranodal
involvement |
|
|
<2 | 126 (74.6) |
| ≥2 | 43 (25.4) |
| BM involvement |
|
|
Absent | 146 (86.4) |
|
Present | 23 (13.6) |
| IPI |
|
| Low,
0–1 | 56 (33.1) |
|
Low-intermediate, 2 | 35 (20.7) |
|
High-intermediate, 3 | 44 (26.1) |
| High,
4–5 | 34 (20.1) |
| Subtype |
|
|
GCB | 72 (42.6) |
|
Non-GCB | 97 (57.4) |
| NCCN-IPI |
|
| Low,
0–1 | 42 (24.9) |
|
Low-intermediate, 2–3 | 51 (30.1) |
|
High-intermediate, 4–5 | 48 (28.4) |
| High,
≥6 | 28 (16.6) |
| Therapy |
|
|
RCHOP | 150 (88.8) |
|
RminiCHOP | 19 (11.2) |
| Bulky disease |
|
| No | 144 (85.2) |
|
Yes | 25 (14.8) |
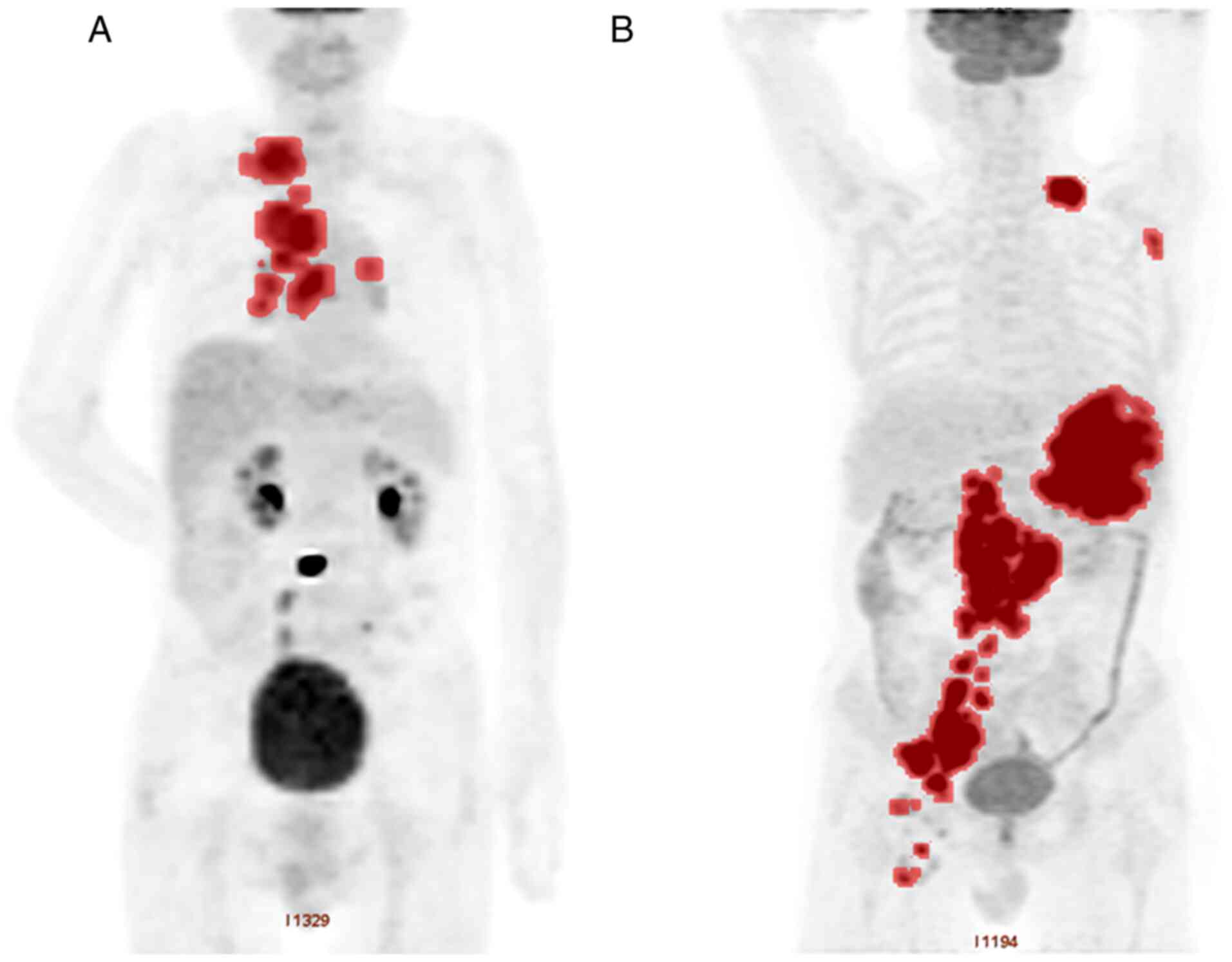
TMTV
The median TMTV of the entire population was 291.4
cm3 (50.3–1598.4 cm3; Fig. 1). The receiver operating curve (ROC)
analysis demonstrated that the best TMTV cut-off value for PFS and
OS estimation was 300 cm3 (data not shown). For PFS and
OS, the area under the curve (AUC) values were 0.701 and 0.724,
respectively (data not shown). The sensitivity and specificity of
the 300 cm3 cut-off for PFS were 75.1 and 67.3%,
respectively, while the sensitivity and specificity for OS were
76.6 and 66.7%, respectively (data not shown).
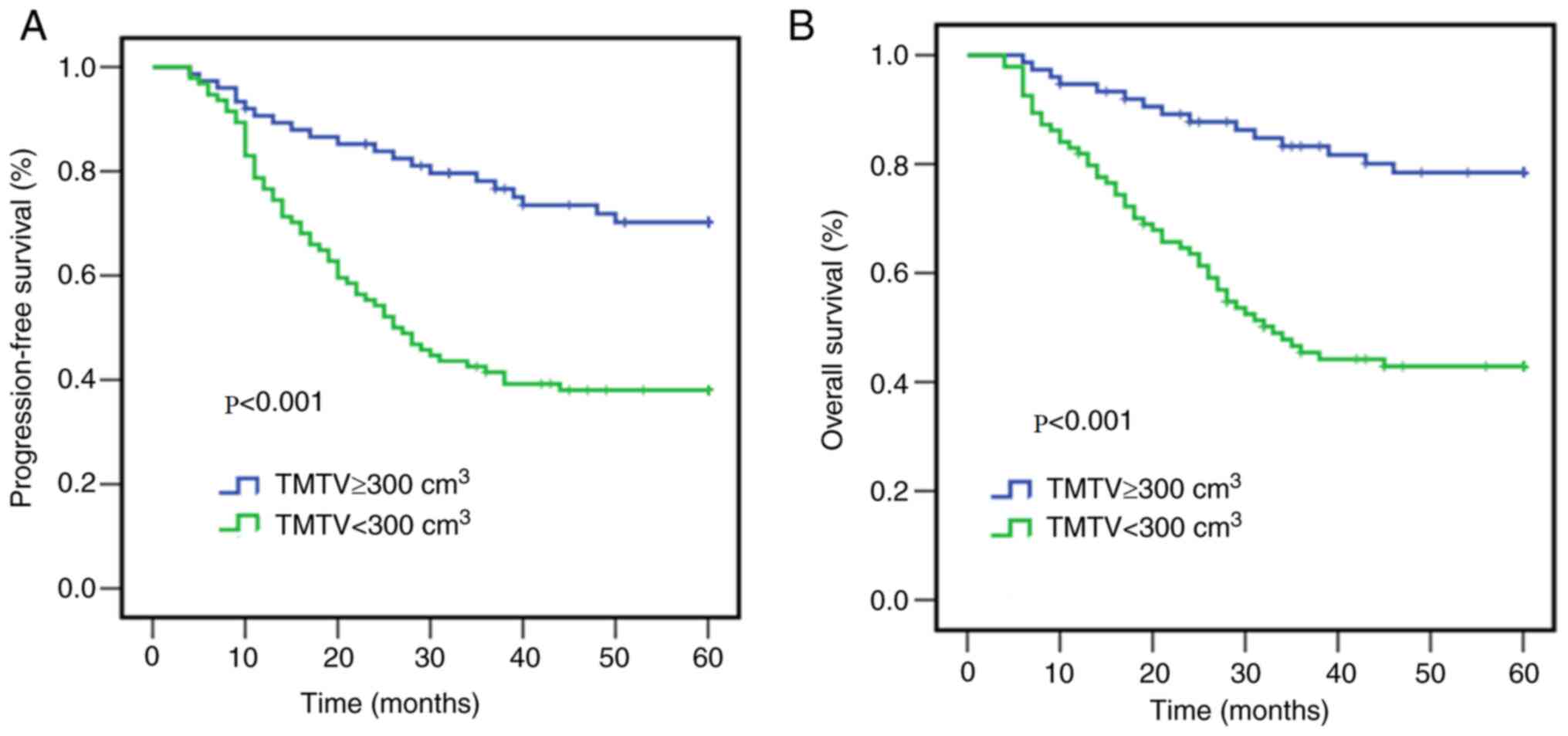
The critical value of the ROC curve was used for
Kaplan-Meier survival analysis. The results demonstrated that TMTV
was a reliable predictor of OS at the univariable level (Table III). As presented in Fig. 2, the 5-year PFS rate of patients with
high TMTV (≥300 cm3, n=94, 55.6%) was 38.3%, while that
of patients with low TMTV (<300 cm3, n=75, 44.4%) was
72% (P<0.001). The 5-year OS rate of patients with high TMTV was
44.7%, while that of patients with low TMTV was 80% (P<0.001).
In addition, significant differences were observed in OS between
patients with TMTV values above and below 300 cm3 at the
multivariate level [hazard ratio (HR), 4.21; 95% confidence
interval (CI), 2.71–7.32; P<0.001; Table III].
| Table III.Multivariate analysis of variables
for overall survival. |
Table III.
Multivariate analysis of variables
for overall survival.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variable (risk
factor) | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age, years (65 vs.
≥65) | 3.32
(1.52–6.13) | <0.001 | 2.14
(1.20–4.41) | 0.002 |
| aB-symptoms, Yes vs. No | 1.54
(1.16–3.26) | 0.019 | 2.24
(1.38–4.36) | 0.016 |
| Cell of origin, GCB
vs. Non-GCB | NS |
| NS |
|
| Serum LDH, normal
vs. elevated | 3.29
(1.79–9.12) | <0.001 | 4.21
(2.12–14.54) | <0.001 |
| ECOG PS, 0–1 vs.
2–4 | 2.65
(2.16–5.72) | 0.011 | 3.32
(2.45–6.62) | 0.025 |
| Ann Arbor stage,
I-11 vs. III–IV | 3.11
(1.88–5.22) | 0.015 | NS |
|
| Number of
extranodal sites, 0–1 vs. ≥2 | 1.89
(1.16–5.51) | 0.013 | NS |
|
| TMTV,
cm3 (≥300 vs. <300) | 3.13
(2.43–6.76) | <0.001 | 4.21
(2.71–7.32) | <0.001 |
| Bone marrow
involvement, Yes vs. No | 2.37
(1.27–5.43) | 0.024 | NS |
|
| bBulky mass, Yes vs. No | 1.37
(1.19–4.21) | 0.033 | NS |
|
Univariate and multivariate
analyses
As presented in Table
III, the following prognostic factors were assessed in the
univariate and multivariable analyses: Age (<65 years vs. ≥65
years), disease stage (I–II vs. III–IV), ECOG performance status
(0–1 vs. 2–4), B-symptoms (yes vs. no), LDH level (normal vs.
elevated), the number of extranodal sites involved (0–1 vs. ≥2),
cell of origin (GCB vs. Non-GCB), bulky disease (yes vs. no), bone
marrow involvement (yes vs. no) and TMTV (≥300 cm3 vs.
<300 cm3). Univariate analysis demonstrated that age
≥65 years (P<0.001), B-symptoms (P=0.019), elevated LDH levels
(P<0.001), ECOG performance status 2–4 (P=0.011), advanced stage
(P=0.015), number of extranodal sites >1 (P=0.013), bulky
disease (P=0.033), bone marrow involvement (P=0.024) and TMTV ≥300
cm3 (P<0.001) were all associated with poor
prognosis. However, multivariate analysis demonstrated that only
age ≥65 years (HR, 2.14; 95% CI, 1.20–4.41; P=0.002), B-symptoms
(HR, 2.24; 95% CI, 1.38–4.36; P=0.016), elevated serum LDH levels
(HR, 4.21; 95% CI, 2.12–14.54; P<0.001), ECOG performance status
2–4 (HR, 3.32; 95% CI, 2.45–6.62; P=0.025) and TMTV ≥300
cm3 (HR, 4.21; 95% CI, 2.71–7.32; P<0.001) were
considered independent prognostic factors.
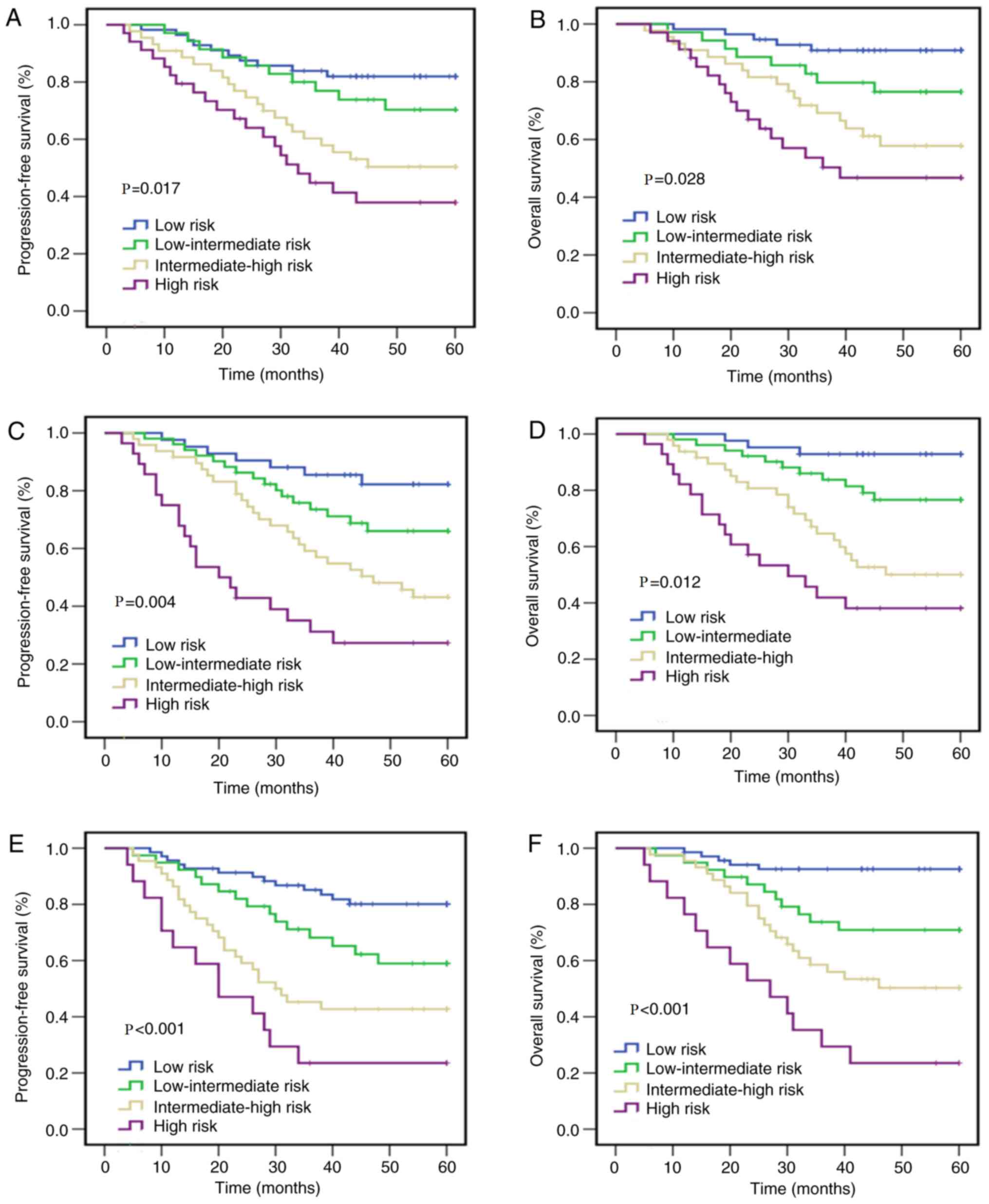
Comparison of the M-PM with existing
prognostic indexes
In the rituximab era, the M-PM model presented here
combined metabolic parameters and clinical characteristics into a
new integrative prognostic factor (Table
I). According to the number of IPI risk factors, patients were
distributed into four different risk groups. However, the IPI
failed to effectively differentiate between the intermediate-high
group and the high-risk group. As presented in Fig. 3, the 5-year PFS rate of patients at
high risk was 41.2% and the OS rate was 50.8%, whereas those at
intermediate-high risk had a 5-year PFS rate of 52.3% and an OS
rate of 60.4% (P=0.017 for PFS; P=0.028 for OS). The NCCN-IPI also
divided patients into four different risk groups. Each group had
significantly different 5-year OS and PFS rates, and the index had
a better discriminative ability compared with IPI. According to the
NCCN-IPI, the 5-year PFS rate of patients at intermediate-high risk
was 45.8% and the 5-year OS rate was 54.3%, while the 5-year PFS
rate of patients at high risk was 28.6% and the 5-year OS rate was
39.4% (P=0.004 for PFS; P=0.012 for OS) (Table IV and Fig. 3).
| Table IV.5-year overall survival rates and
distribution of patients in the risk groups using IPI, NCCN-IPI and
M-PM scores. |
Table IV.
5-year overall survival rates and
distribution of patients in the risk groups using IPI, NCCN-IPI and
M-PM scores.
|
| IPI | NCCN-IPI | M-PM |
|---|
|
|
|
|
|
|---|
| Risk level | Score (%) | 5-year PFS, % | 5-year OS, % | Score (%) | 5-year PFS, % | 5-year OS, % | Score (%) | 5-year PFS, % | 5-year OS, % |
|---|
| Low | 0–1 (33.1) | 82.1 | 90.8 | 0–1 (24.9) | 83.3 | 93.8% | 0–1 (40.8) | 81.2 | 92.4 |
|
Low-intermediate | 2 (20.7) | 71.4 | 78.4 | 2–3 (30.1) | 68.6 | 76.5% | 2 (23.1) | 61.5 | 70.6 |
|
Intermediate-high | 3 (26.1) | 52.3 | 60.4 | 4–5 (28.4) | 45.8 | 54.3% | 3 (26.0) | 43.2 | 52.3 |
| High | 4–5 (20.1) | 41.2 | 50.8 | 6–8 (16.6) | 28.6 | 39.4% | 4 (10.1) | 23.5 | 24.5 |
Patients were also divided into four different risk
groups by the M-PM, namely the low risk, low-intermediate risk,
intermediate-high risk and high risk groups. The groups had a
median follow-up time of 61, 58, 59 and 60 months, respectively. As
presented in Table IV, the 5-year
PFS rates of the four groups were 81.2, 61.5, 43.2 and 23.5%,
respectively, while the 5-year OS rates were 92.4, 70.6, 52.3 and
24.5%, respectively (P<0.001 for PFS and OS; Fig. 3). The M-PM identified a group with
even worse outcomes, with a 5-year OS rate of only 24.5%, which
neither the NCCN-IPI or the IPI identified. Thus, it was concluded
that the predictive value of the M-PM was significantly stronger
compared with the IPI and the NCCN-IPI for predicting high risk
DLBCL (P<0.01). This high-risk group in the M-PM only
represented a small number of patients (10.1%), which was lower
than that identified by the NCCN-IPI (16.6%) and the IPI (20.1%)
(Table IV).
Discussion
DLBCL is a disease with biological heterogeneity,
which is reflected in the different curative effects and survival
of patients (2–4). The IPI is the most recognized and
widely used prognostic evaluation model in DLBCL (6). In the rituximab era, the cure rate of
DLBCL has improved, and the value of IPI's prognostic risk
stratification has weakened, particularly among intermediate-high
risk and high-risk groups (8,27). In
addition, NCCN-IPI and other prognostic evaluation systems cannot
sufficiently distinguish high risk patients with a short survival
time (28,29). Thus, it remains critical to develop a
more accurate prognostic model for DLBCL.
Common prognostic indexes of lymphoma include age,
ECOG score and increased LDH levels, which are associated with a
short survival time in DLBCL (6). In
the original IPI model, the age limit was set to 60 years, which
represented the demarcation point for myeloablative therapy and
stem cell transplantation at the time (30). Currently, this restriction is no
longer in place (30). With the
extensive application of growth factors and rituximab, an
increasing number of elderly patients have received sufficient
immunochemotherapy (30). Thus, in
the novel prediction model presented here, the age limit was
altered to 65 years. The results of the present study confirmed
that age (≥65 years) is a key prognostic indicator. Notably, age
(<65 years) is also commonly used as an age node for
dose-intensified immunochemotherapy or hematopoietic stem cell
transplantation in mantle cell lymphomas (30).
Disease stage is a crude substitute for total tumor
burden, which is illustrated by bulky stage I disease vs. stage IV
lesions, with extensive but small extranodal lesions (31). FDG-PET/CT uses quantitative
indicators of metabolically active tissues, such as TMTV, as
indicators of tumor volume (31). In
previous studies, the prognosis of patients with DLBCL was often
stratified based on interim PET-CT parameters, such as the
Deauville score (32,33). The prognostic model presented here is
based on baseline PET-CT parameters and clinical markers, and can
predict the prognosis of patients earlier. The Maximum Standardized
Uptake Value (SUVmax) is the most common metabolic parameter used
in the clinic (34–37). However, measurement of SUVmax can
only detect the most obvious metabolic activity of a tumor at a
single site, and is unable to reflect the metabolic activity of the
whole tumor, the size and volume of the tumor (34). Furthermore, several factors affect
the accuracy of SUVmax, such as uptake interval, injection dose,
injection leakage, tumor size and heterogeneity, blood sugar and
hormone levels (34,35). Thus, the prognostic value of SUVmax
in DLBCL remains controversial (36,37).
TMTV and TLG reflect tumor volume and tumor activity (38). Our previous study demonstrated that
TMTV is a more robust predictor of survival than TLG (39). Thus, TMTV was incorporated into the
novel prognostic model presented here.
Previous studies have reported that TMTV has a
strong predictive value for newly treated patients with DLBCL
(40,41). Higher TMTV is significantly
associated with worse PFS and OS in patients with DLBCL (19,20,42,43).
Previous studies have also demonstrated that TMTV measured on
18F-FDG PET/CT can be used as an important index in determining the
prognosis of DLBCL (19,43). However, there is still insufficient
consensus on the calculation of TMTV. Currently, the two most
common methods are based on the fixed threshold of SUV 2.5 (MTV
2.5) and the use of 41% SUVmax isocontour (MTV 41) (41,44).
These methods are based on the principle of the fixed threshold to
calculate the metabolism of local tumors (41,44). The
European Association of Nuclear Medicine recommends a SUVmax
threshold of 41%, which has been used in patients with DLBCL with
good interobserver repeatability (40). Given that the patients included in
these studies had different ethnicities and research methods,
different cut-off values were used (20,40,45). The
results of the present study demonstrated that TMTV ≥300
cm3 was significantly associated with poor
prognosis.
High TMTV was significantly associated with advanced
tumor stage and bulky disease (9,14,46).
High TMTV often represents a large tumor load and it may eventually
replace the traditional IPI factors reflecting tumor load, such as
extranodal diseases and Ann Arbor stage (9,14,46).
Thus, it would be useful to add indicators associated with tumor
metabolic characteristics to the current prognostic model in the
form of quantitative PET indicators.
Some studies have included the functional parameters
of PET into the prognostic evaluation model of DLBCL (32,47,48).
However, most prognostic models are based on the results of interim
PET-CT indicators (32,47). The present study predominantly used
baseline TMTV and clinical indicators to predict the prognosis of
DLBCL. To the best of our knowledge, the M-PM presented here is the
first prognostic model to combine PET metabolic parameters and
clinical characteristics in the rituximab era. According to the
M-PM, there were 40.8, 33.1, 26.0 and 10.1% of patients with a low,
low-intermediate, intermediate-high, and high risk,
respectively.
Patients with low or intermediate risk can be cured
by the RCHOP regimen (49); however,
an unmet clinical requirement for patients at high risk remains.
The M-PM can effectively identify this group of exceedingly
high-risk patients. Future clinical trials should aim to maximize
disease control and survival in high risk patients and develop
promising targeted drugs.
The present study was not without limitations.
First, it was a single-center, retrospective study with a moderate
sample size, so there may have been some statistical errors.
Secondly, the calculation of TMTV is time-consuming and the current
calculation method is not uniform. In addition, transplantation and
CAR-T may also affect the overall survival of patients. In our
studies, patients who relapsed or refractory did not receive CAR-T
cell therapy and allogeneic hematopoietic stem cell
transplantation. A total of four patients received autologous
hematopoietic stem cell transplantation, of which two patients
relapsed 2 years after transplantation. However, a small sample
size will not affect the final outcome. In the context of modern
treatment, the model presented here should be verified in
prospective trials. Furthermore, the present study failed to
predict time to next therapy using the novel model. Thus, further
studies are required to confirm the results presented here.
In conclusion, the present study proposed a novel
modified prognostic model for newly diagnosed DLBCL, which consists
of clinical parameters, biological parameters, and standardized
imaging techniques. The results confirmed that in the rituximab
era, the predictive value of the M-PM is more accurate than that of
the IPI and the NCCN-IPI, particularly in the high risk DLBCL
group. Furthermore, the M-PM can identify the high-risk population
with a 5-year OS rate <30%. Taken together, these results
suggest that M-PM may be applied to prospective clinical trials.
The prognostic model presented here requires verification through
large-scale and multi-center trials. In addition, whether M-PM will
retain its strong risk stratification ability in the context of
targeted treatment and novel biomarkers also warrants further
investigation.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Natural
Science Foundation of China (grant no. 81402575).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author upon reasonable
request.
Authors' contributions
HZ and WX designed the present study. PZ and LZ
analyzed the experimental data and drafted the initial manuscript.
LL, ZQ, LQ and SZ helped perform some experiments, obtained the
data and revised the manuscript for important intellectual content.
All authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board of Tianjin Medical University Cancer Institute and
Hospital (Tianjin, China). Written informed consent was obtained
from all the patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jaffe ES: The 2008 WHO classification of
lymphomas: Implications for clinical practice and translational
research. Hematology Am Soc Hematol Educ Program. 523–531. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sehn LH and Gascoyne RD: Diffuse large
B-cell lymphoma: Optimizing outcome in the context of clinical and
biologic heterogeneity. Blood. 125:22–32. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chapuy B, Stewart C, Dunford AJ, Kim J,
Kamburov A, Redd RA, Lawrence MS, Roemer MGM, Li AJ, Ziepert M, et
al: Molecular subtypes of diffuse large B cell lymphoma are
associated with distinct pathogenic mechanisms and outcomes. Nat
Med. 24:679–690. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schmitz R, Wright GW, Huang DW, Johnson
CA, Phelan JD, Wang JQ, Roulland S, Kasbekar M, Young RM, Shaffer
AL, et al: Genetics and pathogenesis of diffuse large B-cell
lymphoma. N Engl J Med. 378:1396–1407. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cunningham D, Hawkes EA, Jack A, Qian W,
Smith P, Mouncey P, Pocock C, Ardeshna KM, Radford JA, McMillan A,
et al: Rituximab plus cyclophosphamide, doxorubicin, vincristine,
and prednisolone in patients with newly diagnosed diffuse large
B-cell non-Hodgkin lymphoma: A phase 3 comparison of dose
intensification with 14-day versus 21-day cycles. Lancet.
381:1817–1826. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
International Non-Hodgkin's Lymphoma
Prognostic Factors Project, . A predictive model for aggressive
non-Hodgkin's lymphoma. N Engl J Med. 329:987–994. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bari A, Marcheselli L, Sacchi S,
Marcheselli R, Pozzi S, Ferri P, Balleari E, Musto P, Neri S, Aloe
Spiriti MA and Cox MC: Prognostic models for diffuse large B-cell
lymphoma in the rituximab era: A never-ending story. Ann Oncol.
21:1486–1491. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ziepert M, Hasenclever D, Kuhnt E, Glass
B, Schmitz N, Pfreundschuh M and Loeffler M: Standard International
prognostic index remains a valid predictor of outcome for patients
with aggressive CD20+ B-cell lymphoma in the rituximab
era. J Clin Oncol. 28:2373–2380. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhou Z, Sehn LH, Rademaker AW, Gordon LI,
Lacasce AS, Crosby-Thompson A, Vanderplas A, Zelenetz AD, Abel GA,
Rodriguez MA, et al: An enhanced International Prognostic Index
(NCCN-IPI) for patients with diffuse large B-cell lymphoma treated
in the rituximab era. Blood. 123:837–842. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Adams HJ and Kwee TC: Prognostic value of
interim FDG-PET in R-CHOP-treated diffuse large B-cell lymphoma:
Systematic review and meta-analysis. Crit Rev Oncol Hematol.
106:55–63. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nakaya A, Fujita S, Satake A, Nakanishi T,
Azuma Y, Tsubokura Y, Hotta M, Yoshimura H, Ishii K, Ito T and
Nomura S: Enhanced international prognostic index in Japanese
patients with diffuse large B-cell lymphoma. Leuk Res Rep. 6:24–26.
2016.PubMed/NCBI
|
|
12
|
Prochazka KT, Melchardt T, Posch F,
Schlick K, Deutsch A, Beham-Schmid C, Weiss L, Gary T, Neureiter D,
Klieser E, et al: NCCN-IPI score-independent prognostic potential
of pretreatment uric acid levels for clinical outcome of diffuse
large B-cell lymphoma patients. Br J Cancer. 115:1264–1272. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Montalbán C, Díaz-López A, Dlouhy I,
Rovira J, Lopez-Guillermo A, Alonso S, Martín A, Sancho JM, García
O, Sánchez JM, et al: Validation of the NCCN-IPI for diffuse large
B-cell lymphoma (DLBCL): The addition of
β2-microglobulin yields a more accurate GELTAMO-IPI. Br
J Haematol. 176:918–928. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dybkaer K, Bøgsted M, Falgreen S, Bødker
JS, Kjeldsen MK, Schmitz A, Bilgrau AE, Xu-Monette ZY, Li L,
Bergkvist KS, et al: Diffuse large B-cell lymphoma classification
system that associates normal B-cell subset phenotypes with
prognosis. J Clin Oncol. 33:1379–1388. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cheson BD, Pfistner B, Juweid ME, Gascoyne
RD, Specht L, Horning SJ, Coiffier B, Fisher RI, Hagenbeek A, Zucca
E, et al: Revised response criteria for malignant lymphoma. J Clin
Oncol. 25:579–586. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Schot BW, Zijlstra JM, Sluiter WJ, van
Imhoff GW, Pruim J, Vaalburg W and Vellenga E: Early FDG-PET
assessment in combination with clinical risk scores determines
prognosis in recurring lymphoma. Blood. 109:486–491. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Culpin RE, Sieniawski M, Angus B, Menon
GK, Proctor SJ, Milne P, McCabe K and Mainou-Fowler T: Prognostic
significance of immunohistochemistry-based markers and algorithms
in immunochemotherapy-treated diffuse large B cell lymphoma
patients. Histopathology. 63:788–801. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wight JC, Chong G, Grigg AP and Hawkes EA:
Prognostication of diffuse large B-cell lymphoma in the molecular
era: Moving beyond the IPI. Blood Rev. 32:400–415. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim J, Hong J, Kim SG, Hwang KH, Kim M,
Ahn HK, Sym SJ, Park J, Cho EK, Shin DB and Lee JH: Prognostic
value of metabolic tumor volume estimated by (18) F-FDG positron
emission tomography/computed tomography in patients with diffuse
large B-cell lymphoma of stage II or III disease. Nucl Med Mol
Imaging. 48:187–195. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sasanelli M, Meignan M, Haioun C,
Berriolo-Riedinger A, Casasnovas RO, Biggi A, Gallamini A, Siegel
BA, Cashen AF, Véra P, et al: Pretherapy metabolic tumour volume is
an independent predictor of outcome in patients with diffuse large
B-cell lymphoma. Eur J Nucl Med Mol Imaging. 41:2017–2022. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tout M, Casasnovas O, Meignan M, Lamy T,
Morschhauser F, Salles G, Gyan E, Haioun C, Mercier M, Feugier P,
et al: Rituximab exposure is influenced by baseline metabolic tumor
volume and predicts outcome of DLBCL patients: A Lymphoma Study
Association report. Blood. 129:2616–2623. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Vitolo U, Trněný M, Belada D, Burke JM,
Carella AM, Chua N, Abrisqueta P, Demeter J, Flinn I, Hong X, et
al: Obinutuzumab or rituximab plus cyclophosphamide, doxorubicin,
vincristine, and prednisone in previously untreated diffuse large
B-cell lymphoma. J Clin Oncol. 35:3529–3537. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hans CP, Weisenburger DD, Greiner TC,
Gascoyne RD, Delabie J, Ott G, Müller-Hermelink HK, Campo E,
Braziel RM, Jaffe ES, et al: Confirmation of the molecular
classification of diffuse large B-cell lymphoma by
immunohistochemistry using a tissue microarray. Blood. 103:275–282.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cheson BD, Fisher RI, Barrington SF,
Cavalli F, Schwartz LH, Zucca E, Lister TA; Alliance, Australasian
Leukaemia and Lymphoma Group; Eastern Cooperative Oncology Group;
European Mantle Cell Lymphoma Consortium, ; et al: Recommendations
for initial evaluation, staging, and response assessment of Hodgkin
and non-Hodgkin lymphoma: The Lugano classification. J Clin Oncol.
32:3059–3068. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhu L, Bian H, Yang L, Liu J, Chen W, Li
X, Wang J, Song X, Dai D, Ye Z, et al:
18Fluorodeoxyglucose-positron emission
tomography/computed tomography features of suspected solitary
pulmonary lesions in breast cancer patients following previous
curative treatment. Thorac Cancer. 10:1086–1095. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhao P, Li L, Zhou S, Qiu L, Qian Z, Liu
X, Meng B and Zhang H: CD5 expression correlates with inferior
survival and enhances the negative effect of p53 overexpression in
diffuse large B-cell lymphoma. Hematol Oncol. 37:360–367. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sehn LH, Berry B, Chhanabhai M, Fitzgerald
C, Gill K, Hoskins P, Klasa R, Savage KJ, Shenkier T, Sutherland J,
et al: The revised International Prognostic Index (R-IPI) is a
better predictor of outcome than the standard IPI for patients with
diffuse large B-cell lymphoma treated with R-CHOP. Blood.
109:1857–1861. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
McMillan DC: Systemic inflammation,
nutritional status and survival in patients with cancer. Curr Opin
Clin Nutr Metab Care. 12:223–226. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Li X, Zhang Y, Zhao W, Liu Z, Shen Y, Li J
and Shen Z: The Glasgow Prognostic Score as a significant predictor
of diffuse large B cell lymphoma treated with R-CHOP in China. Ann
Hematol. 94:57–63. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Dreyling M, Campo E, Hermine O, Jerkeman
M, Le Gouill S, Rule S, Shpilberg O, Walewski J and Ladetto M; ESMO
Guidelines Committee, : Newly diagnosed and relapsed mantle cell
lymphoma: ESMO Clinical Practice Guidelines for diagnosis,
treatment and follow-up. Ann Oncol. 28 (Suppl 4):iv62–iv71. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
El-Galaly TC, Villa D, Gormsen LC, Baech
J, Lo A and Cheah CY: FDG-PET/CT in the management of lymphomas:
Current status and future directions. J Intern Med. 284:358–376.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sun H, Yu Z, Ma N, Zhou J, Tian R, Zhao M
and Wang T: Risk stratification of diffuse large B-cell lymphoma
with interim PET/CT by combining deauville scores and international
prognostic index. Cancer Manag Res. 11:9449–9457. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yim SK, Yhim HY, Han YH, Jeon SY, Lee NR,
Song EK, Jeong HJ, Kim HS and Kwak JY: Early risk stratification
for diffuse large B-cell lymphoma integrating interim Deauville
score and International Prognostic Index. Ann Hematol.
98:2739–2748. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kostakoglu L and Chauvie S: Metabolic
tumor volume metrics in lymphoma. Semin Nucl Med. 48:50–66. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Akamatsu G, Ikari Y, Nishida H, Nishio T,
Ohnishi A, Maebatake A, Sasaki M and Senda M: Influence of
statistical fluctuation on reproducibility and accuracy of SUVmax
and SUVpeak: A Phantom Study. J Nucl Med Technol. 43:222–226. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Park S, Moon SH, Park LC, Hwang DW, Ji JH,
Maeng CH, Cho SH, Ahn HK, Lee JY, Kim SJ, et al: The impact of
baseline and interim PET/CT parameters on clinical outcome in
patients with diffuse large B cell lymphoma. Am J Hematol.
87:937–940. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Gallicchio R, Mansueto G, Simeon V,
Nardelli A, Guariglia R, Capacchione D, Soscia E, Pedicini P,
Gattozzi D, Musto P and Storto G: F-18 FDG PET/CT quantization
parameters as predictors of outcome in patients with diffuse large
B-cell lymphoma. Eur J Haematol. 92:382–389. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kim TM, Paeng JC, Chun IK, Keam B, Jeon
YK, Lee SH, Kim DW, Lee DS, Kim CW, Chung JK, et al: Total lesion
glycolysis in positron emission tomography is a better predictor of
outcome than the International Prognostic Index for patients with
diffuse large B cell lymphoma. Cancer. 119:1195–1202. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Zhao P, Zhu L, Song Z, Wang X, Ma W, Zhu
X, Qiu L, Li L, Zhou S, Qian Z, et al: Combination of baseline
total metabolic tumor volume measured on FDG-PET/CT and
β2-microglobulin have a robust predictive value in patients with
primary breast lymphoma. Hematol Oncol. 38:493–500. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Cottereau AS, Lanic H, Mareschal S,
Meignan M, Vera P, Tilly H, Jardin F and Becker S: Molecular
profile and FDG-PET/CT total metabolic tumor volume improve risk
classification at diagnosis for patients with diffuse large B-cell
lymphoma. Clin Cancer Res. 22:3801–3809. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Mikhaeel NG, Smith D, Dunn JT, Phillips M,
Møller H, Fields PA, Wrench D and Barrington SF: Combination of
baseline metabolic tumour volume and early response on PET/CT
improves progression-free survival prediction in DLBCL. Eur J Nucl
Med Mol Imaging. 43:1209–1219. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Song MK, Chung JS, Shin HJ, Lee SM, Lee
SE, Lee HS, Lee GW, Kim SJ, Lee SM and Chung DS: Clinical
significance of metabolic tumor volume by PET/CT in stages II and
III of diffuse large B cell lymphoma without extranodal site
involvement. Ann Hematol. 91:697–703. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Xie M, Zhai W, Cheng S, Zhang H, Xie Y and
He W: Predictive value of F-18 FDG PET/CT quantization parameters
for progression-free survival in patients with diffuse large B-cell
lymphoma. Hematology. 21:99–105. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Meignan M, Sasanelli M, Casasnovas RO,
Luminari S, Fioroni F, Coriani C, Masset H, Itti E, Gobbi PG, Merli
F and Versari A: Metabolic tumour volumes measured at staging in
lymphoma: Methodological evaluation on phantom experiments and
patients. Eur J Nucl Med Mol Imaging. 41:1113–1122. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Ilyas H, Mikhaeel NG, Dunn JT, Rahman F,
Møller H, Smith D and Barrington SF: Defining the optimal method
for measuring baseline metabolic tumour volume in diffuse large B
cell lymphoma. Eur J Nucl Med Mol Imaging. 45:1142–1154. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Gulec SA, Suthar RR, Barot TC and
Pennington K: The prognostic value of functional tumor volume and
total lesion glycolysis in patients with colorectal cancer liver
metastases undergoing 90Y selective internal radiation therapy plus
chemotherapy. Eur J Nucl Med Mol Imaging. 38:1289–1295. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Yang DH, Ahn JS, Byun BH, Min JJ, Kweon
SS, Chae YS, Sohn SK, Lee SW, Kim HW, Jung SH, et al: Interim
PET/CT-based prognostic model for the treatment of diffuse large B
cell lymphoma in the post-rituximab era. Ann Hematol. 92:471–479.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Zhang YY, Song L, Zhao MX and Hu K: A
better prediction of progression-free survival in diffuse large
B-cell lymphoma by a prognostic model consisting of baseline TLG
and % ∆SUVmax. Cancer Med. 8:5137–147. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Friedberg JW and Fisher RI: Diffuse large
B-cell lymphoma. Hematol Oncol Clin North Am. 22941–952. (ix)2008.
View Article : Google Scholar : PubMed/NCBI
|