Introduction
Breast cancer (BC) is the most common type of
cancer, having the highest incidence and being the leading cause of
death from cancer in women worldwide. Globally, in 2018, more than
2 million cases of BC were newly diagnosed in women, with
>625,000 deaths due to this disease. It was also reported that,
in 2018, BC accounted for 31.6% of all newly diagnosed cancer cases
in women in Saudi Arabia (1).
Obesity poses a serious growing public health problem worldwide
(2). According to estimates by the
World Health Organization (WHO), in 2016, there were ~2 billion
overweight adults, of whom >650 million were considered obese
(3). In Saudi Arabia, the prevalence
of obesity is higher among women than men (4).
Obesity is one of the risk factors of cancer and may
be involved with ~20% of several types of cancer, including
colorectal, postmenopausal breast, endometrial, renal and prostate
cancers (5). Obesity has been
reported to be a risk factor in BC, especially in postmenopausal
women, and may associate with an increased incidence, a poor
prognosis and decreased survival rate (6–8).
Focusing on the molecular connection between BC and obesity could
provide an important tool for researchers to clarify the underlying
mechanisms, which may help identify novel prognostic biomarkers and
therapeutic targets for BC.
Long non-coding RNAs (lncRNAs) are a class of
untranslated regulatory RNA consisting of >200 nucleotides,
which are considered important cellular RNA types that play
critical regulatory roles in numerous biological processes,
including genomic imprinting, chromatin modeling and
post-transcriptional regulation (9);
they have also been associated with various human diseases,
including a variety of cancer types, such as breast, gastric and
colorectal cancers (10,11). Although numerous lncRNAs have
differential expression levels that may act as oncogenes or tumor
suppressors (12), their biological
functions and molecular mechanisms remain largely unknown (13).
Obesity involves profound epigenetic changes and
affects the expression level of obesity-associated lncRNAs, which
may be involved in cancer initiation and/or progression and affect
the outcome of cancer therapy (14).
Moreover, the expression levels of several lncRNAs, such as lncRNA
P5549 (P5549), lncRNA P19461 (P19461) and lncRNA
P3134 (P3134), are differentially expressed in obesity
(15). However, the contribution of
these lncRNAs to obesity in relation to BC is still unclear.
Although several mechanisms have been proposed (16), the molecular association between
obesity and BC is still not well understood and remains under
investigation (17). Moreover, the
role of lncRNAs in obesity-related cancer also remains unclear
(16). Therefore, the present study
was designed to evaluate the expression level of 29 selected
lncRNAs that have previously been linked to cancer or obesity
(Table I)(15,16,18–52) in
the whole blood of obese patients with BC compared with that in
non-obese patients with BC, using reverse
transcription-quantitative polymerase chain reaction (RT-qPCR).
Subsequently, the expression levels of significantly differentially
expressed lncRNAs were assayed in a larger cohort and the
associations with the baseline and clinicopathological
characteristics of the patients were assessed.
 | Table I.Selected lncRNAs associated with
different cancer types, BC or obesity. |
Table I.
Selected lncRNAs associated with
different cancer types, BC or obesity.
| lncRNA | Full name | Expression
status | Biological
functions | Associated
diseases | (Refs.) |
|---|
|
AC011891.5 | lncRNA
AC011891.5 | Upregulated | Positively
correlated with BMI | Obesity | (18) |
| ANRIL | lncRNA ANRIL | Upregulated | Homeostatic
regulator | Several cancer
types | (16) |
|
B4GALT1-AS1 | lncRNA
B4GALT1-AS1 | Upregulated | Promotes cancer
cell stemness and migration | Colon cancer | (19) |
| BCAR4 | BC anti-estrogen
resistance 4 | Upregulated | Induces cancer cell
proliferation and migration | BC | (20) |
| Blnc1 | lncRNA Blnc1 | Upregulated | Controls adipocyte
differentiation | Energy
homeostasis | (21,22) |
| CCAT1 | Colon
cancer-associated transcript 1 | Upregulated | Promotes cancer
cell proliferation, migration and invasion | Cancer cell | (23–25) |
| CCAT2 | Colon
cancer-associated transcript 2 | Upregulated | Promotes cancer
cell proliferation, migration and invasion | Several
carcinomas | (26) |
| H-19 | H19, imprinted
maternally expressed transcript | Upregulated | Inhibits adipocyte
differentiation and improves insulin sensitivity and mitochondrial
biogenesis | Obesity and
numerous cancer types, including BC | (16,27) |
| HOTAIR | HOX transcript
antisense RNA | Upregulated | Abdominal
preadipocyte differentiation | Several cancer
types | (16) |
|
LINC00968 | Long intergenic
non-protein coding RNA 968 | Upregulated | Positively
correlated with BMI | Obesity | (18) |
| LINCADL | lincRNA
adipogenesis- and lipogenesis-associated | Upregulated | Regulates adipocyte
differentiation and fatty acid synthesis | Obesity | (28) |
| MALAT-1 |
Metastasis-associated lung adenocarcinoma
transcript 1 | Upregulated | Promotes cancer
cell proliferation, migration and invasion, and plays a role in
tumorigenesis and/or metastasis | Various cancer
types | (29–31) |
| NEAT1 | Nuclear-enriched
abundant transcript 1 | Upregulated | Regulates
adipogenic differentiation | Obesity | (32,33) |
|
PANDAR-1 | Promoter of CDKN1A
antisense DNA damage-activated RNA 1 | Upregulated | Induces cancer cell
proliferation, invasion and activation of cell
epithelial-mesenchymal transition pathway | Gastric cancer | (34–36) |
| PCAT6 | Prostate
cancer-associated ncRNA transcript 6 | Upregulated | Promotes cancer
cell growth | Numerous cancer
types | (37–40) |
|
RP11-20G13.3 | LincRNA
RP11-20G13.3 | Upregulated | Attenuates
adipogenesis of preadipocytes | Obesity | (18) |
| ZFAS1 | Zinc finger
antisense 1 | Upregulated | Promotes cancer
cell proliferation and metastasis | Various cancer
types | (41,42) |
|
AP001429.1 | LncRNA
AP001429.1 | Upregulated | Negatively
correlated with BMI | Obesity | (43) |
| GAS5 | Growth
arrest-specific 5 | Downregulated | Inhibits cancer
cell proliferation and promotes apoptosis | Obesity and
numerous types of cancer | (44–47) |
| GYG2P1 | Glycogenin 2
pseudogene 1 | Downregulated | Negatively
associated with BMI, fasting insulin and triglycerides, and may
play a role in the pathogenetic mechanism | Obesity | (18) |
| MEG3 | Maternally
expressed gene 3 | Downregulated | Inhibits
adipogenesis | Obesity | (48) |
|
OLMALINC | Oligodendrocyte
maturation-associated lincRNA | Downregulated | Increases
expression of lipid metabolism genes | Obesity | (18) |
| P19461 | lncRNA P19461 | Downregulated | Negatively
correlated with BMI | Obesity | (15) |
| P21015 | lncRNA P21015 | Downregulated | Negatively
correlated with BMI | Obesity | (15) |
| P5549 | lncRNA P5549 | Downregulated | Negatively
correlated with BMI | Obesity | (15) |
|
RP11-529H2.1 | lincRNA
RP11-529H2.1 | Downregulated | Negatively
correlated with BMI | Obesity | (18) |
|
RP11-559N14.5 | lncRNA
RP11-559N14.5 | Downregulated | Involve in the AMPK
signaling pathway, adipocytokine signaling pathway and insulin
resistance | Obesity | (18) |
| SAR1 | lncRNA steroid
receptor RNA activator 1 | Downregulated | Regulates
adipogenesis and insulin sensitivity | Obesity | (49) |
| UCA1 | Urothelial
carcinoma-associated 1 | Downregulated | Promotes cancer
cell migration and invasion | Multiple cancer
types | (50–52) |
This study could lead to a better understanding of
the expression status of circulating lncRNAs and provide new
insights into the lncRNAs involved in the interaction between
obesity and BC, which could serve as a potential biomarker in BC
prognosis.
Materials and methods
Study subjects
The study included 69 BC female patients who
attended between October 2016 and September 2017 the Unit of
Mammography, Department of Radiography at King Abdulaziz University
Hospital (KAUH; Jeddah, Saudi Arabia), where they were diagnosed
with BC. No patient had yet undergone any treatment and patients
with recurrent BC were also excluded. Depending on the body mass
index (BMI) differentiation (53),
the BC patients were categorized as non-obese, which included lean
and overweight (BMI <30 kg/m2; n=33), and obese (BMI
≥30 kg/m2; n=36). All patients provided written informed
consent. The KAUH Unit of Biomedical Ethics Research Committee
approved the study (approval number, HA-02-J-008). The patient
information and sociodemographic characteristics were obtained
through a standard questionnaire by interview. A standard
well-established method was used to collect anthropometric data
following WHO recommendations (53).
The clinicopathological characteristics and clinical interpretation
were provided by the consultants, radiologist and pathologist, as
described previously (54,55).
Blood sample collection and
storage
According to the manufacturer's instruction, whole
blood samples were collected in PAXgene™ blood RNA tubes (Qiagen,
Inc.), and then stored at −80°C until being used for RNA
extraction.
RNA extraction
Total RNA was isolated from the whole blood of 69
patients with BC using the PAXgene blood RNA kit (Qiagen, Inc.).
The quantity and quality of the extracted RNA were verified by
DeNovix DS-11 Spectrophotometer (DeNovix, Inc.). The RNA samples
were also separated in 1.2% agarose gel electrophoresis to check
the quality. The RNA samples were aliquoted and stored at −80°C
until being used for complementary DNA (cDNA) synthesis.
Complementary DNA (cDNA)
synthesis
Total RNA (400 ng) from each BC sample was reverse
transcribed to generate cDNA using a QuantiTect Reverse
Transcription (RT) kit (Qiagen, Inc.) following the manufacturer's
protocols. The cDNA was stored at −20°C until required.
Quantitative polymerase chain reaction
(qPCR)
The gene expression levels of 29 lncRNAs, selected
according to a suggested role in cancer or obesity as reported by
the literature, including by our previous study (43) (Table
I), were evaluated in the blood of obese and non-obese patients
with BC by qPCR. Each experiment was run in duplicate in 96-well
plates using a Bio-Rad IQ SYBR Green mix and the CFX Connect™
Real-Time PCR Detection system (both Bio-Rad Laboratories, Inc.),
according to the manufacturers' protocols and guidelines. The qPCR
reactions were carried out as follows: Initial cycle for 30 sec at
95°C; followed by 40 cycles of 15 sec at 98°C, and 30 sec at 60°C.
The amplification product was checked at the end of each cycle, and
the purity of amplification products was checked by the analysis of
melting curves. The lncRNA expression levels were normalized using
the housekeeping gene glyceraldehyde 3-phosphate dehydrogenase
(GAPDH) as an internal control for relative expression
quantification. The primer pairs of target lncRNAs and reference
genes were designed over two different exons using the Primer3 web
tool and assessed using the In-Silico PCR tool for human
genome assembly GRCh38 (hg38), provided by the University of
California, Santa Cruz Genome Browser (http://genome.ucsc.edu/index.html). The sequences of
the primers are presented in Table
II. The relative expression quantification was calculated using
the relative expression software tool (REST 2009) version 2.0.13
(56) and the comparative Cq method
(2−ΔΔCq) (57).
| Table II.PCR primer sequences for target
lncRNAs and reference genes. |
Table II.
PCR primer sequences for target
lncRNAs and reference genes.
| Gene symbol | Gene name | Gene type | Forward primer
(5′-3′) | Reverse primer
(5′-3′) |
|---|
| GAPDH |
Glyceraldehyde-3-phosphate
dehydrogenase | Reference |
TCACCAGGGCTGCTTTTAAC |
GATGATCTTGAGGCTGTTGTCA |
|
AP001429.1 | lncRNA
AP001429.1 | Non-coding |
AATATGACTGGGCCCTGCAA |
CCGTTGGCCATTTCGTGATT |
| P5549 | lncRNA P5549 | Non-coding |
CTTTTCCGGCTGAGGTGTTC |
TGAACCAGCCATCTCTCACA |
| P21015 | lncRNA P21015 | Non-coding |
ACCCCAGAAGTGACAAGAGG |
AGATAAACCGCTGCCTTGTG |
| P19461 | lncRNA P19461 | Non-coding |
CAGCCTCCTCCTGTGATGTA |
CGTTCTTCTTGTTTGGACCCA |
| Blnc1 | lncRNA Blnc1 | Non-coding |
CCTTCTCCAACCATCTGCCT |
CTCTTCCCTCTGCCTCTGAC |
| SRA1 | lncRNA steroid
receptor RNA activator 1 | Non-coding |
GGAGGATGTGCTGAGACCTT |
CAACTTTCCTCCAGCCCACT |
|
B4GALT1-AS1 | lncRNA
B4GALT1-AS1 | Non-coding |
CTAGCCCACCGTCTGTTTTGGCAG |
GGAAACTAGCCAACCT |
| LINCADL | lincRNA
adipogenesis-and lipogenesis-associated | Non-coding |
ATATGACCCAAGACCAGGCC |
TCACAGCGAATCACTCCCTT |
| ANRIL | lncRNA ANRIL | Non-coding |
ACGAAGCTCTACACACTTGAAG |
GGATCACAGACCATACTTGCAC |
|
RP11-20G13.3 | lincRNA
RP11-20G13.3 | Non-coding |
TCTGGAAGGAGTGTCGGTCT |
CGTGTTCACAGATTGGGAGA |
|
LINC00968 | long intergenic
non-protein coding RNA 968 | Non-coding |
ACCATCCCATTGAGAACCAA |
CGAAAGGCTGGAAGTGTCAT |
|
AC011891.5 | lncRNA
AC011891.5 | Non-coding |
CGAAAGGCTGGAAGTGTCAT |
TGACCCAATTCTGACATTTGC |
| GYG2P1 | Glycogenin 2
pseudogene 1 | Non-coding |
TCAGCCTCCCAAGTAGCTGT |
CAGCCTGTGTCTCCTCAGTG |
|
RP11-529H2.1 | lincRNA
RP11-529H2.1 | Non-coding |
AGGAGAATGGTGAAGGCAGA |
TGCCGAAGCAGTTTAATCCT |
|
OLMALINC | Oligodendrocyte
maturation-associated lincRNA | Non-coding |
AGACCCAGGACAGGAGGACT |
ATTGGCAAGATGTTCCTTGG |
| MALAT1 |
Metastasis-associated lung adenocarcinoma
transcript 1 | Non-coding |
GCAGGGAGAATTGCGTCATT |
TTCTTCGCCTTCCCGTACTT |
| PCAT6 | Prostate
cancer-associated ncRNA transcript 6 | Non-coding |
CTCCATCCTCATTCGGTCCA |
GAAGGGTGGTGGTAGAAGCA |
| UCA1 | Urothelial
carcinoma-associated 1 | Non-coding |
TTTGCCAGCCTCAGCTTAAT |
TTGTCCCCATTTTCCATCAT |
| MEG3 | Maternally
expressed 3 | Non-coding |
TCACCTGCTAGCAAACTGGA |
CATGCTCATTCCAGAAGCCC |
| CCAT2 | Colon
cancer-associated transcript 2 | Non-coding |
ATGAAGGCGTCGTCCAAATG |
TCAGGCAATTGGTCAGAGGT |
| BCAR4 | BC anti-estrogen
resistance 4 | Non-coding |
CGATGCTTGTCTTGCTCTGA |
CCGCTTTTTCGTATCACTCC |
| CCAT1 | Colon
cancer-associated transcript 1 | Non-coding |
TTGCTCACCTTACTGCCTGA |
CCTGCAACTAGACACTCCCA |
| PANDAR | Promoter of CDKN1A
antisense DNA damage-activated RNA 1 | Non-coding |
TTGTAGCTCCTCCCATGTCG |
AGGAACAGGCAATGGGATCA |
| HOTAIR | HOX transcript
antisense RNA | Non-coding |
GAGTTCCACAGACCAACACC |
AATCCGTTCCATTCCACTGC |
| NEAT1 | Nuclear-enriched
abundant transcript 1 | Non-coding |
CCAGTGTGAGTCCTAGCATTGC |
CCTGGAAACAGAACATTGGAGAAC |
| GAS5 | Growth
arrest-specific 5 | Non-coding |
CCCAAGGAAGGATGAGAATAGC |
CTGTCTAATGCCTGTGTGCC |
| H19 | H19 imprinted
maternally expressed transcript | Non-coding |
ATCCGGACACAAAACCCTCT |
AGAGCCGATTCCTGAGTCAG |
| ZFAS1 | ZNFX1 antisense
RNA1 | Non-coding |
AAGCCACGTGCAGACATCTAC |
CTACTTCCAACACCCGCATTCA |
| P3134 | lncRNA P3134 | Non-coding |
GTGGTGAGATCTCGGGGAAA |
GTGCCAGAATTTCCTCACCC |
Statistical analysis
GraphPad Prism version 8.0.1 (GraphPad Software) was
used to evaluate the statistical analyses of the obtained data
using an unpaired, two-tailed t-test to determine the significant
differences in the gene expression between groups. Moreover,
χ2 and Kruskal-Wallis tests (one-way ANOVA) with a
two-tailed P-value were used to test the distribution of
categorical baseline and clinicopathological characteristics
between obese and non-obese patients with BC. P≤0.05 was used to
indicate a statistically significant difference. Bonferroni's
correction was applied and the corrected P-value of ≤0.05 used for
multiple comparisons of AP001429.1 expression level and
patient baseline and clinicopathological characterizations. The
data are presented as the mean ± standard error of the mean (SEM).
Receiver operating characteristic (ROC) curves were generated to
evaluate the sensitivity and specificity of AP001429.1 as a
potential biomarker, using its gene expression values
(2−ΔCq) of obese and non-obese patients with BC in the
easyROC web-tool (ver.1.3.1; http://www.biosoft.hacettepe.edu.tr/easyROC/).
Results
General and clinicopathological
characterization of the studied patients
The study cohort consisted of 69 newly diagnosed
female patients with BC. The mean age ± SEM of the patients at the
time of diagnosis was 52.3±1.51 (age range, 29–80 years). Over half
(50.7%) were <50 years old, of which 29.0% were between 41 and
50 years old. The mean BMI ± SEM of the patients was 30.0±0.67
kg/m2; 52.2% of the patients were obese at the time of
diagnosis and 47.8% were not obese, with a mean BMI ± SEM of
33.9±0.74 and 25.8±0.51 kg/m2, respectively (Table III).
| Table III.Baseline characteristics of studied
patients with BC. |
Table III.
Baseline characteristics of studied
patients with BC.
| Parameters | Total | Non-obese BC | Obese BC |
|---|
| Number of patients,
n (%) | 69 (100.0) | 33 (47.8) | 36 (52.2) |
| Age,
yearsa | 52.3±1.51 | 46.5±1.55 | 57.5±2.20 |
| BMI,
kg/m2a | 30.0±0.67 | 25.8±0.51 | 33.9±0.74 |
| Waist
circumference, cma | 90.2±2.84 | 87.1±4.56 | 93.1±3.48 |
| Hip circumference,
cma | 104.5±2.94 | 101.8±4.51 | 106.9±3.84 |
| W/H
ratioa | 0.87±0.01 | 0.85±0.02 | 0.88±0.01 |
| Age of first
menstruation, yearsa | 13.36±0.16 | 13.22±0.23 | 13.49±0.23 |
| Age since
menopause, yearsa | 50.30±0.89 | 48.37±1.20 | 51.43±1.20 |
| Age of first
pregnancy, yearsa | 22.37±0.54 | 22.10±0.79 | 22.62±0.76 |
Overall, 84.1% of the patients were married with
three children or less, 46.4% had experienced a miscarriage and
81.1% were breastfeeding mothers. The mean age of first pregnancy
was 22.7±0.65 years. A total of 40 patients had reached menopause
at the time of diagnosis, with a mean age ± SEM 49.9±0.99 years,
while the first appearance of menstruation for most patients was at
a mean age ± SEM of 13.41±0.19 years, with only 5.8% experiencing
first menstruation when <12 years of age. Most patients did not
have any family history of BC or other cancer types, nor polycystic
fibrosis or diabetes mellitus. In total, 92.8% of the patients were
non-smokers, of which 33.3% performed physical activity. Moreover,
most of the patients (75.4%) did not have diet rich in fat, and a
few of the patients (18.8%) took omega-3 supplements (Table IV).
| Table IV.Distribution of general information
characteristics of the studied patients with BC. |
Table IV.
Distribution of general information
characteristics of the studied patients with BC.
| Categories | Total, n (%) | Non-obese BC, n
(%) | Obese BC, n
(%) | P-value |
|---|
| Patients | 69 (100) | 33 (47.8) | 36 (52.2) |
|
| Age of patients,
years |
|
|
| 0.004 |
|
≤40 | 15 (21.7) | 10 (66.7) | 5 (33.3) |
|
|
41-60 | 38 (55.1) | 21 (55.3) | 17 (44.7) |
|
|
>60 | 16 (23.2) | 2 (12.5) | 14 (87.5) |
|
| Marital status |
|
|
| 0.56 |
|
Single | 7 (10.1) | 2 (28.6) | 5 (71.4) |
|
|
Married | 58 (84.1) | 29 (50.0) | 29 (50.0) |
|
|
Divorced | 4 (5.8) | 2 (50.0) | 2 (50.0) |
|
| Education
level |
|
|
| 0.45 |
|
Illiterate | 19 (27.5) | 7 (36.8) | 12 (63.2) |
|
|
School | 25 (36.2) | 12 (48.0) | 13 (52.0) |
|
| First
and higher degree | 25 (36.2) | 14 (56.0) | 11 (44.0) |
|
| Nationality |
|
|
| 0.57 |
|
Saudi | 38 (55.1) | 17 (44.7) | 21 (55.3) |
|
|
Non-Saudi | 31 (44.9) | 16 (51.6) | 15 (48.4) |
|
| Age of first
menstruation, years |
|
|
| 0.53 |
|
<12 | 4 (5.8) | 3 (75.0) | 1 (25.0) |
|
|
12-15 | 61 (88.4) | 28 (45.9) | 33 (54.1) |
|
|
>15 | 4 (5.8) | 2 (50.0) | 2 (50.0) |
|
| Menopausal
status |
|
|
| 0.003 |
|
Postmenopausal | 40 (58.0) | 13 (32.5) | 27 (67.5) |
|
|
Premenopausal | 29 (42.0) | 20 (69.0) | 9 (31.0) |
|
| Age of menopause,
years |
|
|
| 0.44 |
|
<48 | 3 (7.5) | 0 (0.0) | 3 (100.0) |
|
|
48-55 | 32 (80.0) | 11 (34.4) | 21 (65.6) |
|
|
>55 | 5 (12.5) | 2 (40.0) | 3 (60.0) |
|
| Hormone replacement
therapy |
|
|
| 0.17 |
|
Yes | 2 (2.9) | 0 (0.0) | 2 (100.0) |
|
| No | 67 (97.1) | 33 (49.3) | 34 (50.7) |
|
| Number of
children |
|
|
| 0.14 |
|
None | 8 (11.6) | 2 (25.0) | 6 (75.0) |
|
| ≤3 | 31 (44.9) | 19 (61.3) | 12 (38.7) |
|
|
4-6 | 18 (26.1) | 6 (33.3) | 12 (66.7) |
|
|
>6 | 12 (17.4) | 6 (50.0) | 6 (50.0) |
|
| Number of
miscarriages |
|
|
| 0.48 |
|
None | 27 (39.1) | 14 (51.9) | 13 (48.1) |
|
| 1 or
2 | 24 (34.8) | 13 (54.2) | 11 (45.8) |
|
| ≥3 | 8 (11.6) | 2 (25.0) | 6 (75.0) |
|
| No
answer | 10 (14.5) | 4 (40.0) | 6 (60.0) |
|
| Age of pregnancy,
years |
|
|
| 0.79 |
|
≤20 | 22 (36.1) | 12 (54.5) | 10 (45.5) |
|
|
21-30 | 34 (55.7) | 16 (47.1) | 18 (52.9) |
|
|
>30 | 5 (8.2) | 3 (60.0) | 2 (40.0) |
|
| Breast feeding |
|
|
| 0.45 |
|
Never | 13 (18.8) | 5 (38.5) | 8 (61.5) |
|
|
Yes | 56 (81.2) | 28 (50.0) | 28 (50.0) |
|
| Family history of
BC |
|
|
| 0.89 |
|
Yes | 13 (18.8) | 6 (46.2) | 7 (53.8) |
|
| No | 56 (81.2) | 27 (48.2) | 29 (51.8) |
|
| Family history of
other cancer |
|
|
| 0.89 |
|
Yes | 13 (18.8) | 6 (46.2) | 7 (53.8) |
|
| No | 56 (81.2) | 27 (48.2) | 29 (51.8) |
|
| Polycystic fibrosis
status |
|
|
| 0.35 |
|
Yes | 9 (13.0) | 3 (33.3) | 6 (66.7) |
|
| No | 60 (87.0) | 30 (50.0) | 30 (50.0) |
|
| Diabetes mellitus
status |
|
|
| 0.92 |
|
Yes | 15 (21.7) | 7 (46.7) | 8 (53.3) |
|
| No | 54 (78.3) | 26 (48.1) | 28 (51.9) |
|
| Physical activities
performance |
|
|
| 0.31 |
|
Yes | 23 (33.3) | 13 (56.5) | 10 (43.5) |
|
| No | 46 (66.7) | 20 (43.5) | 26 (56.5) |
|
| Smoking status |
|
|
| 0.2 |
|
Yes | 5 (7.2) | 1 (20.0) | 4 (80.0) |
|
| No | 64 (92.8) | 32 (50.0) | 32 (50.0) |
|
| Omega-3
supplements |
|
|
| 0.17 |
|
Yes | 13 (18.8) | 4 (30.8) | 9 (69.2) |
|
| No | 56 (81.2) | 29 (51.8) | 27 (48.2) |
|
| Diet rich in
fat |
|
|
| 0.23 |
|
Yes | 17 (24.6) | 6 (35.3) | 11 (64.7) |
|
| No | 52 (75.4) | 27 (51.9) | 25 (48.1) |
|
Regarding the clinicopathological features (Table V), the majority of the patients
(76.8%) had invasive ductal carcinoma, 7.2% had invasive lobular
carcinoma and 10.1% were diagnosed with an invasive mixture of
ductal and lobular carcinoma. Approximately 56.5% of the patients
had grade II tumors, 53.6% had tumor size <2 cm, and 43.5% had
negative lymph node involvement. Based on the hormone receptor
phenotypes, 71.0% of the patients had a luminal BC subtype
(ER+/PR+/HER2−): 69.6%
ER+, 56.5% PR+ and 59.4% HER2−. By
contrast, HER2+ was only found in 34.8% of the patients.
Therefore, the ER+/PR+/HER2−
phenotype was the most abundant in the patient cohort.
| Table V.Distribution of clinicopathological
features of the studied patients with BC. |
Table V.
Distribution of clinicopathological
features of the studied patients with BC.
| Categories | Total, n (%) | Non-obese BC, n
(%) | Obese BC, n
(%) | P-value |
|---|
| Patients | 69 (100) | 33 (47.8) | 36 (52.2) |
|
| Hormone receptor
phenotype |
|
|
| 0.28 |
|
Luminal | 49 (71.0) | 25 (51.0) | 24 (49.0) |
|
|
HER2-enriched | 10 (14.5) | 5 (50.0) | 5 (50.0) |
|
| Triple
negative/basal like | 6 (8.7) | 1 (16.7) | 5 (83.3) |
|
|
Unknown | 4 (5.8) | 2 (50.0) | 2 (50.0) |
|
| ER status |
|
|
| 0.53 |
|
ER− | 17 (24.6) | 7 (41.2) | 10 (58.8) |
|
|
ER+ | 48 (69.6) | 24 (50.0) | 24 (50.0) |
|
|
Unknown | 4 (5.8) | 2 (50.0) | 2 (50.0) |
|
| PR status |
|
|
| 0.08 |
|
PR− | 26 (37.7) | 9 (34.6) | 17 (65.4) |
|
|
PR+ | 39 (56.5) | 22 (56.4) | 17 (43.6) |
|
|
Unknown | 4 (5.8) | 2 (50.0) | 2 (50.0) |
|
| HER2 status |
|
|
| 0.19 |
|
HER2− | 41 (59.4) | 17 (41.5) | 24 (58.5) |
|
|
HER2+ | 24 (34.8) | 14 (58.3) | 10 (41.7) |
|
|
Unknown | 4 (5.8) | 2 (50.0) | 2 (50.0) |
|
| Lymph node
involvement |
|
|
| 0.67 |
|
Negative | 30 (43.5) | 12 (40.0) | 18 (60.0) |
|
|
Positive | 15 (21.7) | 7 (46.7) | 8 (53.3) |
|
|
Unknown | 24 (34.8) | 14 (58.3) | 10 (41.7) |
|
| Size of tumor,
cm |
|
|
| 0.69 |
|
<2 | 37 (53.6) | 17 (45.9) | 20 (54.1) |
|
|
2-5 | 22 (31.9) | 9 (40.9) | 13 (59.1) |
|
|
>5 | 3 (4.3) | 2 (66.7) | 1 (33.3) |
|
|
Unknown | 7 (10.1) | 5 (71.4) | 2 (28.6) |
|
| Tumor grade |
|
|
| 0.37 |
| I | 8 (11.6) | 4 (50.0) | 4 (50.0) |
|
| II | 39 (56.5) | 16 (41.0) | 23 (59.0) |
|
|
III | 18 (26.1) | 11 (61.1) | 7 (38.9) |
|
|
Unknown | 4 (5.8) | 2 (50.0) | 2 (50.0) |
|
| Histotype |
|
|
| 0.32 |
|
DCIS | 53 (76.8) | 23 (43.4) | 30 (56.6) |
|
|
LCIS | 5 (7.2) | 3 (60.0) | 2 (40.0) |
|
| Mixture
of ductal and lobular | 7 (10.1) | 5 (71.4) | 2 (28.6) |
|
|
Unknown | 4 (5.8) | 2 (50.0) | 2 (50.0) |
|
| Vascular
invasion |
|
|
| 0.28 |
|
Negative | 42 (60.9) | 19 (45.2) | 23 (54.8) |
|
|
Positive | 11 (15.9) | 3 (27.3) | 8 (72.7) |
|
|
Unknown | 16 (23.2) | 11 (68.8) | 5 (31.3) |
|
| Margin |
|
|
| 0.40 |
|
Negative | 41 (59.4) | 17 (41.5) | 24 (58.5) |
|
|
Positive | 1 (3.6) | 0 (0.0) | 1 (100.0) |
|
|
Unknown | 27 (39.1) | 16 (59.3) | 11 (40.7) |
|
The non-obese and obese BC groups were significantly
different in terms of age and menopausal status (P=0.003); however,
the results did not show any significant differences with regard to
other general and clinicopathological characteristics (Tables IV and V).
Screening of lncRNAs in a selected
cohort of obese versus non-obese BC patients
The gene expression levels of the 29 selected
lncRNAs were initially measured in a selected cohort of BC
patients, based on the greatest BMI differentiation: 6 obese
patients with the highest BMI and 6 non-obese BC patients with the
lowest BMI were selected from the overall BC patient cohort. The
amplification products for lncRNAs and GAPDH were specific and pure
in all samples as assessed by melting curve analysis and across the
threshold within 30 cycles.
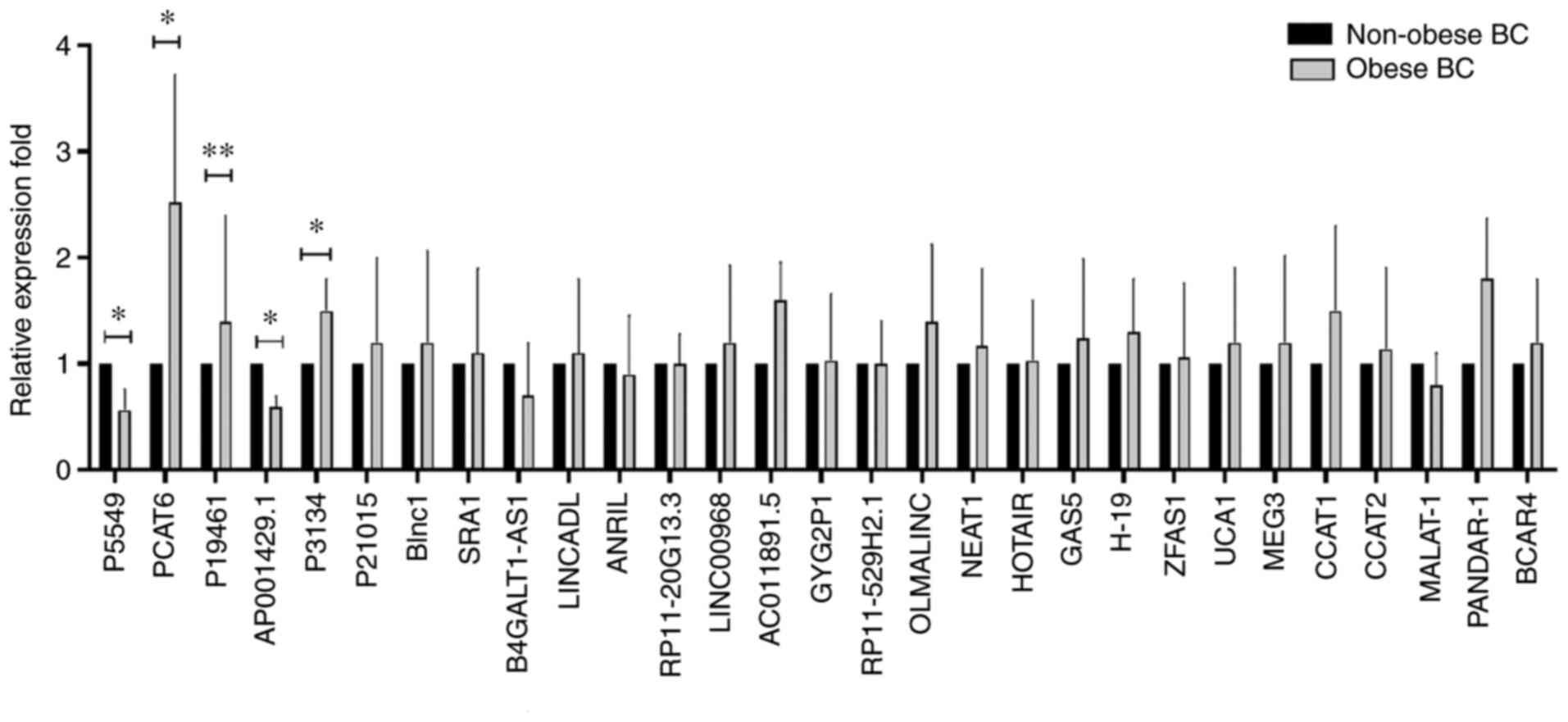
The expression level of lncRNAs in a selected cohort
of obese compared with non-obese patients with BC is shown in
Fig. 1. Among all selected lncRNAs,
P5549, P19461, PCAT6, AP001429.1 and P3134 were
significantly differentially expressed. The expression levels of
circulating PCAT6, P19461 and P3134 were
significantly upregulated [fold-change (FC), 2.526 and P≤0.02; FC,
1.361 and P≤0.008; and FC, 1.5 and P=0.05, respectively], whereas
P5549 and AP001429.1 showed a significant decrease in
expression within the same group of obese BC patients (FC, 0.56 and
P=0.05; and FC, 0.6 and P=0.02, respectively). The rest of the
studied lncRNAs did not show any significant differences in
expression between the groups (Fig.
1).
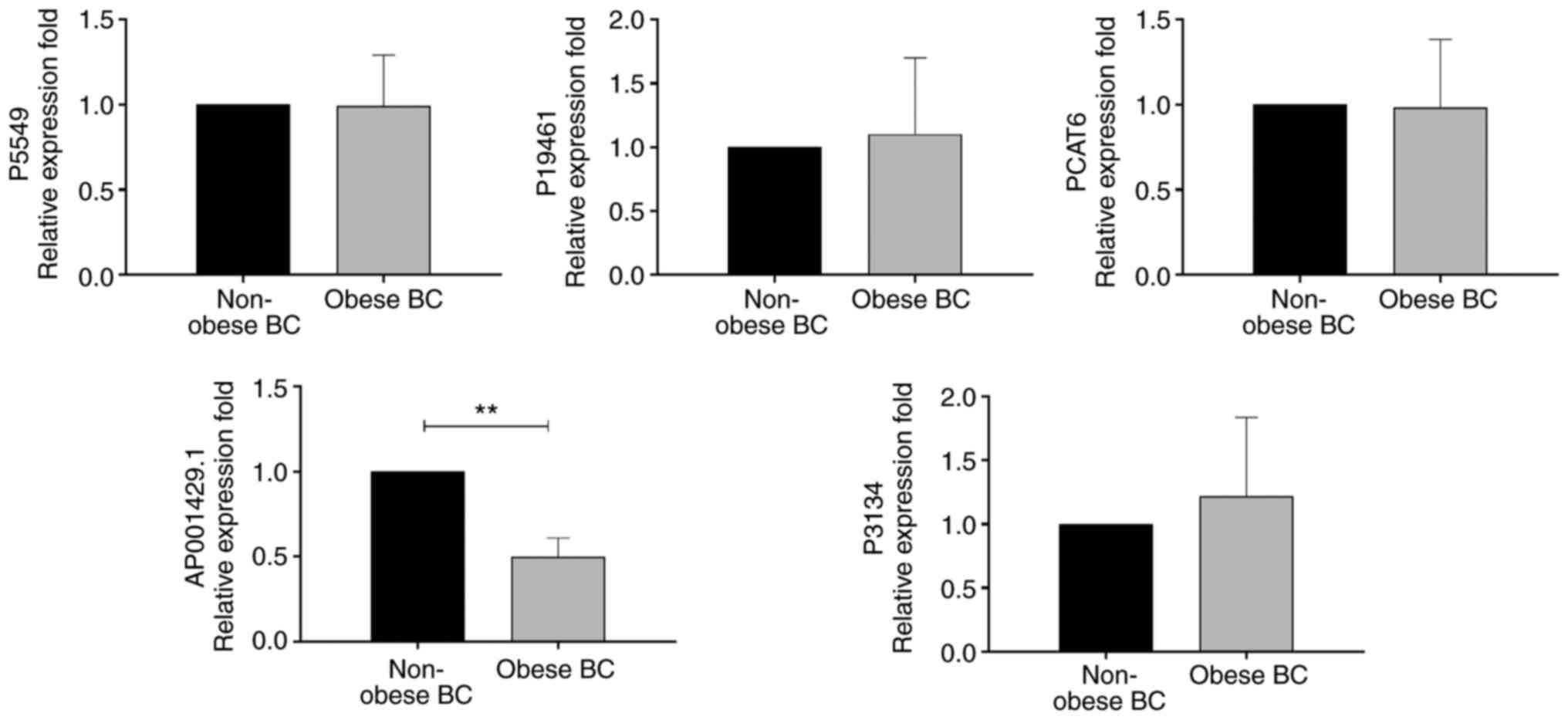
Evaluation of lncRNA expression in a
larger cohort of obese and non-obese BC patients
The gene expression levels of the significantly
differentially expressed identified lncRNAs, (P5549, P19461,
P3134, PCAT6 and AP001429.1) were evaluated in a larger
cohort consisting of the study population of 36 obese and 33
non-obese BC patients, as shown in Fig.
2. Among these evaluated lncRNAs, AP001429.1 was
significantly downregulated in obese compared with non-obese
patients with BC (FC, 0.5; P=0.002). By contrast, P5549 (FC,
1.0; P=0.97), P19461 (FC, 1.1; P=0.56), P3134 (FC,
1.2; P=0.12) and PCAT6 (FC, 1.0; P=0.94) were not found to
exhibit any significant differences in expression within the larger
group of patients (Fig. 2).
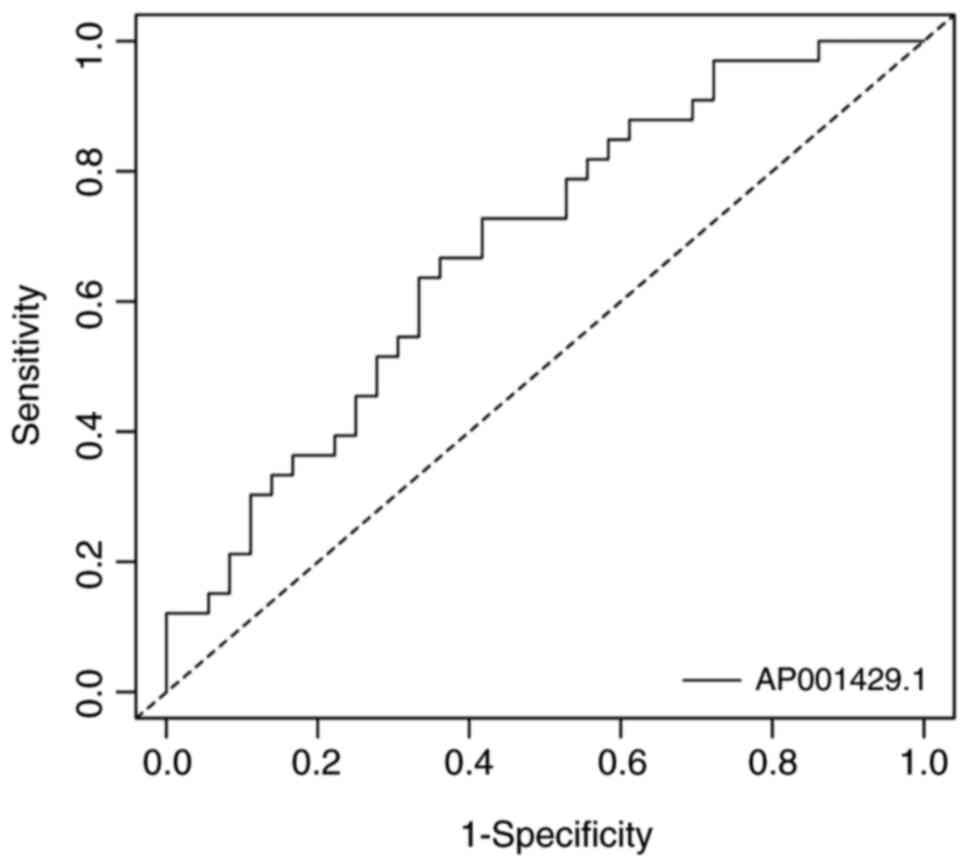
To evaluate AP001429.1 as a potential
biomarker, a ROC curve was generated using the gene expression
values of AP001429.1 in obese and non-obese BC patients. In
the ROC curve analysis (Fig. 3 and
Table SI), the area under the ROC
curve was 0.684 (nearly 0.7), indicating that AP001429.1 expression
enabled weak but significant differentiation of patients with BC
based on obesity status (P=0.004) (58). Therefore, AP001429.1 may act
as a potential biomarker in obese patients with BC.
Association between AP001429.1
expression level and patient baseline characteristics
Differential expression patterns in
AP001429.1 were observed when assessing the association with
patient baseline features (Table
SII). Significant differences in AP001429.1 expression
with regard to patient baseline characteristics were assessed by
Bonferroni's correction (P≤0.05) and are presented in Fig. 4. Significant decreases in
AP001429.1 expression were detected in obese patients with
BC who were at middle-aged (FC, 0.4; P=0.03), married (FC, 0.4;
P=0.006), Saudi national (FC, 0.5; P=0.02) and patients who had low
education level (FC, 0.2; P<0.0003). AP001429.1 also
showed significant downregulation in relation to premenopausal
obese BC patients (FC, 0.3; P=0.002), in those who were
breastfeeding their children (FC, 0.4; P<0.001) and in those who
experienced their first menstruation event between 12 and 15 years
old (FC, 0.5; P=0.01) or had their first pregnancy aged between 21
and 30 (FC, 0.4; P=0.03). Moreover, the non-smoking obese BC
patients, those who did not take omega-3 supplements and those who
performed physical activity also showed a significantly decreased
expression level of AP001429.1 (FC, 0.6 and P=0.01; FC, 0.5
and P=0.02; and FC, 0.2 and P<0.001, respectively). Furthermore,
AP001429.1 showed significant downregulation in relation to
diabetic obese patients with BC, as well as those who did not have
hormone replacement therapy, those who did not have any family
history of BC, other cancer types or polycystic fibrosis (FC, 0.2
and P<0.001; FC, 0.5 and P=0.01; FC, 0.4 and P=0.004; and FC,
0.5 and P=0.01, respectively). Moreover, the significantly
decreased expression of AP001429.1 was also detected in
obese patients with BC who had 4 to 6 children (FC, 0.2; P=0.03)
and those who had miscarriages once or twice (FC, 0.4; P=0.03)
(Fig. 4).
Association between AP001429.1
expression level and patient clinicopathological
characteristics
Associations in the expression levels of
AP001429.1 in obese patients with BC compared with that in
non-obese patients with BC were assessed with regard to patient
clinicopathological characteristics (Table SIII). Significant differences in
AP001429.1 expression with regard to patient
clinicopathological characteristics were assessed by Bonferroni's
correction (P≤0.05) and are presented in Fig. 5. AP001429.1 exhibited a
significantly lower expression level in obese patients compared
with that in non-obese patients with BC; however, the significantly
decreased expression was detected with regard to negative HER2
status (FC, 0.4; P=0.02), negative E-cadherin expression (FC, 0.1;
P<0.001), negative vascular invasion (FC, 0.4; P=0.004),
negative margin invasion (FC, 0.5; P=0.02) and LCIS (FC, 0.2;
P<0.001) BC patients. By contrast, a high expression level of
AP001429.1 was only detected in relation to positive
E-cadherin expression (FC, 5.3; P=0.04) within the obese patients
with BC (Fig. 5).
Discussion
lncRNA, as a class of untranslated regulatory RNA,
is considered an important type of cellular RNA that plays a
critical regulatory role in a number of biological processes in
normal development, as well as in tumorigenesis and tumor
progression processes (59). lncRNA
is regarded as a key regulator of diseases with tissue specificity
(60). lncRNA controls the flux of
genetic information modulating various cellular processes, such as
modulation of chromosome structure, transcription, splicing, mRNA
stability and availability, post-translational modifications
(61) and epigenetic mechanisms
(62). Obesity involves profound
epigenetic changes and affects the expression of obesity-associated
lncRNAs that may be involved in cancer initiation and/or
progression and affect cancer therapy. To the best of our
knowledge, the approach of the present study comparing differences
between obese and non-obese patients with BC has so far not been
applied. Previous studies investigated healthy non-obese versus
obese patients (15,16,44,63,64) as
well as healthy control cases versus patients with BC (65–68).
Therefore, in the present study, lncRNA expression levels were
evaluated in whole blood taken from BC patients by liquid biopsy,
with obese patients being compared with non-obese patients, aiming
to determine the expression status of lncRNAs in obese patients
with BC and their associations with the general and
clinicopathological attributes of the patients.
AP001429.1 is also known as novel transcript
sense intronic lncRNA to tetratricopeptide repeat domain 3; it is
located on the long arm of chromosome 21 (21q22.13) and is 530
nucleotides in length (69). Very
limited information is available on the expression and biological
functions of AP001429.1; however, its mRNA expression has
been detected in a number of normal human tissues and cells,
including whole blood, brain, cerebellum, endometrium, heart, ovary
and testis (69). Furthermore,
according to the RNAcentral resource (70) and the LncBase database (71), AP001429.1 is targeted by
several miRNAs; notably, a number of AP001429.1-targeted
miRNAs are downregulated and reported to have roles as tumor
suppressors in BC, such as miR-124-3p (72), miR-196b-5p (73), the miR-34-5p family (74,75),
miR-449b-5p (76),
miR-940 (77) and
miR-99a-3p (78,79). In addition, miR-196a-5p and
miR-449a were upregulated and reported to be involved in
oncogenesis in BC (80,81), suggesting that AP001429.1 may
function as a potential tumor suppressor in BC by targeting those
miRNAs. The present study showed that AP001429.1 was
significantly downregulated in obese patients with BC compared with
non-obese patients with BC. A significant decrease in
AP001429.1 expression was detected in obese patients with BC
who were middle-aged, premenopausal, married, had 4 to 6 children
and who breastfed their newborn. Moreover, in the BC patient
cohort, non-smoking status, performance of a physical activity,
diabetes, the absence of hormone replacement therapy and the
absence of a family history of cancer or polycystic fibrosis, was
also associated with a significant decrease in the expression level
of AP001429.1 (Fig. 3 and
Table SII). Moreover, a significant
association was also detected with regard to certain molecular and
histological characteristic, including negative HER2 status,
negative E-cadherin expression, negative vascular and margin
invasion, and LCIS. Obese patients with BC also exhibited
downregulation of AP001429.1 compared with non-obese
patients with BC (Fig. 4 and
Table SIII). The exact reasoning
behind the significant associations with regard to these parameters
is not clear.
Numerous lncRNAs have been detected as
differentially expressed in different cells and tissues associated
with cancer and/or obesity (82).
Moreover, the differential expression of lncRNAs may contribute to
the initiation, development, invasion and metastasis of various
types of cancer, including BC, as well as obesity development,
brown adipocyte differentiation and the function of adipose tissue
(83), through both activation and
inhibition of the expression of other genes (84) that could affect various
cancer-related physiological processes (85). Therefore, lncRNAs may serve as BC
prognostic and diagnostic biomarkers as well as being useful as
therapeutic targets for BC treatments. Despite the existence of
studies considering lncRNAs in BC, there is still an urgent need
for more studies focusing on the role of lncRNAs in BC with obesity
in order to provide a better understanding of their involvement and
offer new insights into the role of lncRNAs in obesity-related
BC.
In conclusion, the present results demonstrated the
downregulation of AP001429.1 in obese patients with BC,
suggesting that obesity may have a role in inhibiting the
expression of AP001429.1, which could be considered as a
potential tumor suppressor of BC. This information may help improve
our understanding and provide an important research tool with
regard to the molecular associations between obesity and BC.
Therefore, the expression of AP001429.1 could serve as a
potential biomarker for BC prognosis and a target for therapy.
Further study is needed to confirm these findings and elucidate the
underlying mechanism for the effects of AP001429.1 with
regard to connections between obesity and BC.
The current study has certain limitations, including
the small sample size, which needs to be increased to confirm and
validate the findings. Further control cross-sectional studies
using healthy obese and non-obese patients with an increase in
sample size will be conducted in the near future. Finally, further
investigation is required to elucidate the expression profile and
functional role of AP001429.1 in BC tissue.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
This project was funded by the Deanship of
Scientific Research (DSR) at King Abdulaziz University (KAU)
Jeddah, Kingdom of Saudi Arabia (grant no. G: 638/130/1438).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MAH, HC, KAAS and ALAM designed and coordinated the
experiments. KAAS obtained the ethical approval, patients' consent
and blood samples. MAH performed the experiments and analyzed the
data. HC contributed to laboratory facilitates and project funding.
MAH wrote the original manuscript draft. KAAS and HC edited the
manuscript. HC, MAH and KAAS confirm the authenticity of all the
raw data. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Unit of Biomedical
Ethics Research Committee, KAUH (approval no. HA-02-J-008). All
patients signed a consent form to engage in this study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare no that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Smith KB and Smith MS: Obesity statistics.
Prim Care. 43:121–135. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
WHO, . Obesity and overweight. https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweightDecember
15–2020
|
|
4
|
Memish ZA, El Bcheraoui C, Tuffaha M,
Robinson M, Daoud F, Jaber S, Mikhitarian S, Al Saeedi M, AlMazroa
MA, Mokdad AH and Al Rabeeah AA: Obesity and associated
factors-Kingdom of Saudi Arabia, 2013. Prev Chronic Dis.
11:E1742014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
De Pergola G and Silvestris F: Obesity as
a major risk factor for cancer. J Obes. 2013:2915462013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Argolo DF, Hudis CA and Iyengar NM: The
impact of obesity on breast cancer. Curr Oncol Rep. 20:472018.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Iyengar NM, Hudis CA and Dannenberg AJ:
Obesity and cancer: Local and systemic mechanisms. Annu Rev Med.
66:297–309. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chan DS and Norat T: Obesity and breast
cancer: Not only a risk factor of the disease. Curr Treat Options
Oncol. 16:222015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang J, Zhang X, Chen W, Hu X, Li J and
Liu C: Regulatory roles of long noncoding RNAs implicated in cancer
hallmarks. Int J Cancer. 146:906–916. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhao H, Shi J, Zhang Y, Xie A, Yu L, Zhang
C, Lei J, Xu H, Leng Z, Li T, et al: LncTarD: A manually-curated
database of experimentally-supported functional lncRNA-target
regulations in human diseases. Nucleic Acids Res. 48:D118–D126.
2019.PubMed/NCBI
|
|
11
|
Li Z, Zhao W, Wang M and Zhou X: The Role
of Long Noncoding RNAs in Gene Expression Regulation. Gene
Expression Profiling in Cancer IntechOpen London, UK: 2019,
View Article : Google Scholar
|
|
12
|
Zhuang C, Ma Q, Zhuang C, Ye J, Zhang F
and Gui Y: LncRNA GClnc1 promotes proliferation and invasion of
bladder cancer through activation of MYC. FASEB J. 33:11045–11059.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li Y, Yang X, Kang X and Liu S: The
regulatory roles of long noncoding RNAs in the biological behavior
of pancreatic cancer. Saudi J Gastroenterol. 25:145–151. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rohde K, Keller M, la Cour Poulsen L,
Blüher M, Kovacs P and Böttcher Y: Genetics and epigenetics in
obesity. Metabolism. 92:37–50. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sun J, Ruan Y, Wang M, Chen R, Yu N, Sun
L, Liu T and Chen H: Differentially expressed circulating LncRNAs
and mRNA identified by microarray analysis in obese patients. Sci
Rep. 6:354212016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yau MY, Xu L, Huang CL and Wong CM: Long
non-coding RNAs in obesity-induced cancer. Noncoding RNA.
4:192018.PubMed/NCBI
|
|
17
|
Zeng J, Sauter ER and Li B: FABP4: A new
player in obesity-associated breast cancer. Trends Mol Med.
26:437–440. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liu Y, Ji Y, Li M, Wang M, Yi X, Yin C,
Wang S, Zhang M, Zhao Z and Xiao Y: Integrated analysis of long
noncoding RNA and mRNA expression profile in children with obesity
by microarray analysis. Sci Rep. 8:87502018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhang Y, Fang ZX, Guo X, Dong H, Zhou K,
Huang Z and Xiao Z: lncRNA B4GALT1-AS1 promotes colon cancer cell
stemness and migration by recruiting YAP to the nucleus and
enhancing YAP transcriptional activity. J Cell Physiol.
234:18524–18534. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ouyang S, Zhou X, Chen Z, Wang M, Zheng X
and Xie M: LncRNA BCAR4, targeting to miR-665/STAT3 signaling,
maintains cancer stem cells stemness and promotes tumorigenicity in
colorectal cancer. Cancer Cell Int. 19:722019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mi L, Zhao XY, Li S, Yang G and Lin JD:
Conserved function of the long noncoding RNA Blnc1 in brown
adipocyte differentiation. Mol Metab. 6:101–110. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sun L and Lin JD: Function and mechanism
of long noncoding RNAs in adipocyte biology. Diabetes. 68:887–896.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Li GH, Ma ZH and Wang X: Long non-coding
RNA CCAT1 is a prognostic biomarker for the progression of oral
squamous cell carcinoma via miR-181a-mediated Wnt/β-catenin
signaling pathway. Cell Cycle. 18:2902–2913. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hu M, Zhang Q, Tian XH, Wang JL, Niu YX
and Li G: lncRNA CCAT1 is a biomarker for the proliferation and
drug resistance of esophageal cancer via the miR-143/PLK1/BUBR1
axis. Mol Carcinog. 58:2207–2217. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Li Y, Zhu G, Ma Y and Qu H: lncRNA CCAT1
contributes to the growth and invasion of gastric cancer via
targeting miR-219-1. J Cell Biochem. 120:19457–19468. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cai Y, He J and Zhang D: Long noncoding
RNA CCAT2 promotes breast tumor growth by regulating the Wnt
signaling pathway. Onco Targets Ther. 8:2657–2664. 2015.PubMed/NCBI
|
|
27
|
Schmidt E, Dhaouadi I, Gaziano I, Oliverio
M, Klemm P, Awazawa M, Mitterer G, Fernandez-Rebollo E, Pradas-Juni
M, Wagner W, et al: LincRNA H19 protects from dietary obesity by
constraining expression of monoallelic genes in brown fat. Nat
Commun. 9:36222018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhang X, Xue CY, Line J, Ferguson JF,
Weiner A, Liu W, Han Y, Hinkle C, Li W, Jiang H, et al:
Interrogation of nonconserved human adipose lincRNAs identifies a
regulatory role of linc-ADAL in adipocyte metabolism. Sci Transl
Med. 10:eaar59872018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kong X, Wang J, Cao Y, Zhang H, Lu X, Wang
Y, Bo C, Wang T, Li S, Tian K, et al: The long noncoding RNA
MALAT-1 functions as a competing endogenous RNA to regulate MSL2
expression by sponging miR-338-3p in myasthenia gravis. J Cell
Biochem. 120:5542–5550. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Han X, Xu Z, Tian G, Tang Z, Gao J, Wei Y
and Xu X: Suppression of the long non-coding RNA MALAT-1 impairs
the growth and migration of human tongue squamous cell carcinoma
SCC4 cells. Arch Med Sci. 15:992–1000. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tripathi V, Ellis JD, Shen Z, Song DY, Pan
Q, Watt AT, Freier SM, Bennett CF, Sharma A, Bubulya PA, et al: The
nuclear-retained noncoding RNA MALAT1 regulates alternative
splicing by modulating SR splicing factor phosphorylation. Mol
Cell. 39:925–938. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Gernapudi R, Wolfson B, Zhang Y, Yao Y,
Yang P, Asahara H and Zhou Q: MicroRNA 140 promotes expression of
long noncoding RNA NEAT1 in adipogenesis. Mol Cell Biol. 36:30–38.
2015.PubMed/NCBI
|
|
33
|
Cooper DR, Carter G, Li P, Patel R, Watson
JE and Patel NA: Long non-coding RNA NEAT1 associates with SRp40 to
temporally regulate PPARγ2 splicing during adipogenesis in 3T3-L1
cells. Genes (Basel). 5:1050–1063. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Li Y, Su X and Pan H: Inhibition of lncRNA
PANDAR reduces cell proliferation, cell invasion and suppresses EMT
pathway in breast cancer. Cancer Biomark. 25:185–192. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Liu J, Ben Q, Lu E, He X, Yang X, Ma J,
Zhang W, Wang Z, Liu T, Zhang J and Wang H: Long noncoding RNA
PANDAR blocks CDKN1A gene transcription by competitive interaction
with p53 protein in gastric cancer. Cell Death Dis. 9:1682018.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wang H, Fang L, Jiang J, Kuang Y, Wang B,
Shang X, Han P, Li Y, Liu M, Zhang Z and Li P: The
cisplatin-induced lncRNA PANDAR dictates the chemoresistance of
ovarian cancer via regulating SFRS2-mediated p53 phosphorylation.
Cell Death Dis. 9:11032018. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Xin Y, He X, Zhao W, Zhan M, Li Y, Xiao J,
He K and Lu L: LncRNA PCAT6 increased cholangiocarcinoma cell
proliferation and invasion via modulating miR-330-5p. Am J Transl
Res. 11:6185–6195. 2019.PubMed/NCBI
|
|
38
|
Wu H, Zou Q, He H, Liang Y, Lei M, Zhou Q,
Fan D and Shen L: Long non-coding RNA PCAT6 targets miR-204 to
modulate the chemoresistance of colorectal cancer cells to
5-fluorouracil-based treatment through HMGA2 signaling. Cancer Med.
8:2484–2495. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Huang WM, Su G, Huang XX, Zou A, Wu J,
Yang Y, Zhu Y, Liang S, Li D, Ma F and Guo L: Long noncoding RNA
PCAT6 inhibits colon cancer cell apoptosis by regulating
anti-apoptotic protein ARC expression via EZH2. Cell Cycle.
18:69–83. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Dong F, Ruan S, Wang J, Xia Y, Le K, Xiao
X, Hu T and Wang Q: M2 macrophage-induced lncRNA PCAT6 facilitates
tumorigenesis and angiogenesis of triple-negative breast cancer
through modulation of VEGFR2. Cell Death Dis. 11:7282020.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Tong H, Zhuang X, Cai J, Ding Y, Si Y,
Zhang H and Shen M: Long noncoding RNA ZFAS1 promotes progression
of papillary thyroid carcinoma by sponging miR-590-3p and
upregulating HMGA2 expression. Onco Targets Ther. 12:7501–7512.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Dong D, Mu Z, Wei N, Sun M, Wang W, Xin N,
Shao Y and Zhao C: Long non-coding RNA ZFAS1 promotes proliferation
and metastasis of clear cell renal cell carcinoma via targeting
miR-10a/SKA1 pathway. Biomed Pharmacother. 111:917–925. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Hassan MA, Al-Sakkaf K, Shait Mohammed MR,
Dallol A, Al-Maghrabi J, Aldahlawi A, Ashoor S, Maamra M, Ragoussis
J, Wu W, et al: Integration of transcriptome and metabolome
provides unique insights to pathways associated with obese breast
cancer patients. Front Oncol. 10:8042020. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Mansoori Y, Tabei MB, Askari A, Izadi P,
Daraei A, Bastami M, Naghizadeh MM, Nariman-Saleh-Fam Z, Mansoori B
and Tavakkoly-Bazzaz J: Expression levels of breast cancer-related
GAS5 and LSINCT5 lncRNAs in cancer-free breast tissue: Molecular
associations with age at menarche and obesity. Breast J.
24:876–882. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Ni W, Yao S, Zhou Y, Liu Y, Huang P, Zhou
A, Liu J, Che L and Li J: Long noncoding RNA GAS5 inhibits
progression of colorectal cancer by interacting with and triggering
YAP phosphorylation and degradation and is negatively regulated by
the m6A reader YTHDF3. Mol Cancer. 18:1432019.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Ji J, Dai X, Yeung SJ and He X: The role
of long non-coding RNA GAS5 in cancers. Cancer Manag Res.
11:2729–2737. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Sun M, Jin FY, Xia R, Kong R, Li JH, Xu
TP, Liu YW, Zhang EB, Liu XH and De W: Decreased expression of long
noncoding RNA GAS5 indicates a poor prognosis and promotes cell
proliferation in gastric cancer. BMC Cancer. 14:3192014. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Li Z, Jin C, Chen S, Zheng Y, Huang Y, Jia
L, Ge W and Zhou Y: Long non-coding RNA MEG3 inhibits adipogenesis
and promotes osteogenesis of human adipose-derived mesenchymal stem
cells via miR-140-5p. Mol Cell Biochem. 433:51–60. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Xu B, Gerin I, Miao H, Vu-Phan D, Johnson
CN, Xu R, Chen XW, Cawthorn WP, MacDougald OA and Koenig RJ:
Multiple roles for the non-coding RNA SRA in regulation of
adipogenesis and insulin sensitivity. PLoS One. 5:e141992010.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Gong P, Qiao F, Wu H, Cui H, Li Y, Zheng
Y, Zhou M and Fan H: LncRNA UCA1 promotes tumor metastasis by
inducing miR-203/ZEB2 axis in gastric cancer. Cell Death Dis.
9:11582018. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Bian Z, Jin L, Zhang J, Yin Y, Quan C, Hu
Y, Feng Y, Liu H, Fei B, Mao Y, et al: LncRNA-UCA1 enhances cell
proliferation and 5-fluorouracil resistance in colorectal cancer by
inhibiting miR-204-5p. Sci Rep. 6:238922016. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Yao F, Wang Q and Wu Q: The prognostic
value and mechanisms of lncRNA UCA1 in human cancer. Cancer Manag
Res. 11:7685–7696. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
de Onis M and Habicht JP: Anthropometric
reference data for international use: Recommendations from a world
health organization expert committee. Am J Clin Nutr. 64:650–658.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Al-Maghrabi J, Al-Sakkaf K, Qureshi IA,
Butt NS, Damnhory L, Elshal M, Al-Maghrabi B, Aldahlawi A, Ashoor
S, Brown B, et al: AMPK expression patterns are significantly
associated with poor prognosis in breast cancer patients. Ann Diagn
Pathol. 29:62–67. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Khabaz MN, Al-Sakkaf K, Qureshi IA, Butt
NS, Damnhory L, Elshal M, Al-Maghrabi B, Aldahlawi A, Ashoor S,
Brown B, et al: Expression of p-AMPK is associated with hormone
receptor phenotypes and lymph node metastasis in breast cancer. Int
J Clin Exp Patho. 10:7044–7051. 2017.
|
|
56
|
Pfaffl MW, Horgan GW and Dempfle L:
Relative expression software tool (REST) for group-wise comparison
and statistical analysis of relative expression results in
real-time PCR. Nucleic Acids Res. 30:e362002. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Mandrekar JN: Receiver operating
characteristic curve in diagnostic test assessment. J Thorac Oncol.
5:1315–1316. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Soudyab M, Iranpour M and Ghafouri-Fard S:
The role of long non-coding RNAs in breast cancer. Arch Iran Med.
19:508–517. 2016.PubMed/NCBI
|
|
60
|
Zhu Y, Mao D, Gao W, Han G and Hu H:
Analysis of lncRNA expression in patients with eosinophilic and
neutrophilic asthma focusing on LNC_000127. Front Genet.
10:1412019. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Fernandes JCR, Acuña SM, Aoki JI,
Floeter-Winter LM and Muxel SM: Long non-coding RNAs in the
regulation of gene expression: Physiology and disease. Noncoding
RNA. 5:172019.PubMed/NCBI
|
|
62
|
Wei JW, Huang K, Yang C and Kang CS:
Non-coding RNAs as regulators in epigenetics (Review). Oncol Rep.
37:3–9. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Ghafouri-Fard S and Taheri M: The
expression profile and role of non-coding RNAs in obesity. Eur J
Pharmacol. 892:1738092021. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Butler AE, Hayat S, Dargham SR, Malek JA,
Abdullah SA, Mahmoud YA, Sathyapalan T and Atkin SL: Long
non-coding RNA expression in non-obese women with polycystic ovary
syndrome and weight-matched controls. Reprod Biomed Online.
41:579–583. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Liang Y, Song X, Li Y, Chen B, Zhao W,
Wang L, Zhang H, Liu Y, Han D, Zhang N, et al: LncRNA BCRT1
promotes breast cancer progression by targeting miR-1303/PTBP3
axis. Mol Cancer. 19:852020. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Sun Z and Liu J and Liu J: The expression
of lncRNA-MALAT1 in breast cancer patients and its influences on
prognosis. Cell Mol Biol (Noisy-le-grand). 66:72–78. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Lv D, Xu K, Jin X, Li J, Shi Y, Zhang M,
Jin X, Li Y, Xu J and Li X: LncSpA: LncRNA spatial atlas of
expression across normal and cancer tissues. Cancer Res.
80:2067–2071. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Mohebi M, Ghafouri-Fard S, Modarressi MH,
Dashti S, Zekri A, Kholghi-Oskooei V and Taheri M: Expression
analysis of vimentin and the related lncRNA network in breast
cancer. Exp Mol Pathol. 115:1044392020. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Stelzer G, Rosen N, Plaschkes I, Zimmerman
S, Twik M, Fishilevich S, Stein TI, Nudel R, Lieder I, Mazor Y, et
al: The genecards suite: From gene data mining to disease genome
sequence analyses. Curr Protoc Bioinformatics. 54:1.30.1–1.30.33.
2016.PubMed/NCBI
|
|
70
|
The Rnacentral Consortium, Petrov AI, Kay
SJE, Kalvari I, Howe KL, Gray KA, Bruford EA, Kersey PJ, Cochrane
G, Finn RD, et al: RNAcentral: A comprehensive database of
non-coding RNA sequences. Nucleic Acids Res. 45:D128–D134. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Paraskevopoulou MD, Vlachos IS, Karagkouni
D, Georgakilas G, Kanellos I, Vergoulis T, Zagganas K, Tsanakas P,
Floros E, Dalamagas T and Hatzigeorgiou AG: DIANA-LncBase v2:
Indexing microRNA targets on non-coding transcripts. Nucleic Acids
Res. 44:D231–D238. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Wang Y, Chen L, Wu Z, Wang M, Jin F, Wang
N, Hu X, Liu Z, Zhang CY, Zen K, et al: miR-124-3p functions as a
tumor suppressor in breast cancer by targeting CBL. BMC Cancer.
16:8262016. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Zhu X, Rao X, Yao W and Zou X:
Downregulation of MiR-196b-5p impedes cell proliferation and
metastasis in breast cancer through regulating COL1A1. Am J Transl
Res. 10:3122–3132. 2018.PubMed/NCBI
|
|
74
|
Wang B, Li D, Kovalchuk I, Apel IJ,
Chinnaiyan AM, Wóycicki RK, Cantor CR and Kovalchuk O: miR-34a
directly targets tRNAiMet precursors and affects
cellular proliferation, cell cycle, and apoptosis. Proc Natl Acad
Sci USA. 115:7392–7397. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Zhang L, Wang L, Dong D, Wang Z, Ji W, Yu
M, Zhang F, Niu R and Zhou Y: MiR-34b/c-5p and the neurokinin-1
receptor regulate breast cancer cell proliferation and apoptosis.
Cell Prolif. 52:e125272019. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Jiang J, Yang X, He X, Ma W, Wang J, Zhou
Q, Li M and Yu S: MicroRNA-449b-5p suppresses the growth and
invasion of breast cancer cells via inhibiting CREPT-mediated
Wnt/β-catenin signaling. Chem Biol Interact. 302:74–82. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Hou L, Chen M, Yang H, Xing T, Li J, Li G,
Zhang L, Deng S, Hu J, Zhao X and Jiang J: MiR-940 inhibited cell
growth and migration in triple-negative breast cancer. Med Sci
Monit. 22:3666–3672. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Hu Y, Zhu Q and Tang L: MiR-99a antitumor
activity in human breast cancer cells through targeting of mTOR
expression. PLoS One. 9:e920992014. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Wang X, Li Y, Qi W, Zhang N, Sun M, Huo Q,
Cai C, Lv S and Yang Q: MicroRNA-99a inhibits tumor aggressive
phenotypes through regulating HOXA1 in breast cancer cells.
Oncotarget. 6:32737–32747. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Wang YW, Zhang W and Ma R: Bioinformatic
identification of chemoresistance-associated microRNAs in breast
cancer based on microarray data. Oncol Rep. 39:1003–1010.
2018.PubMed/NCBI
|
|
81
|
Shi W, Bruce J, Lee M, Yue S, Rowe M,
Pintilie M, Kogo R, Bissey PA, Fyles A, Yip KW and Liu FF: MiR-449a
promotes breast cancer progression by targeting CRIP2. Oncotarget.
7:18906–18918. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Dahariya S, Paddibhatla I, Kumar S,
Raghuwanshi S, Pallepati A and Gutti RK: Long non-coding RNA:
Classification, biogenesis and functions in blood cells. Mol
Immunol. 112:82–92. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Xu S, Chen P and Sun L: Regulatory
networks of non-coding RNAs in brown/beige adipogenesis. Biosci
Rep. 35:e002622015. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Jiang MC, Ni JJ, Cui WY, Wang BY and Zhuo
W: Emerging roles of lncRNA in cancer and therapeutic
opportunities. Am J Cancer Res. 9:1354–1366. 2019.PubMed/NCBI
|
|
85
|
Lo PK, Wolfson B, Zhou X, Duru N,
Gernapudi R and Zhou Q: Noncoding RNAs in breast cancer. Brief
Funct Genomics. 15:200–221. 2016. View Article : Google Scholar : PubMed/NCBI
|