Introduction
Invasive micropapillary carcinoma (IMPC), a rare
distinct histopathological subtype, is characterized
histopathologically by the presence of small morula-like clusters
of carcinoma cells displaying reverse polarity (so-called
inside-out pattern), wherein the apical pole of the neoplastic
cells faces the stroma side surrounded by clear stromal space
(1). This rare variant was
originally described in the breast in 1980 (2), and has been increasingly recognized as
a distinct histopathological subtype in a variety of organs,
including the salivary gland (3),
lung (4), stomach (5), colon (5), and urinary bladder (3–6).
Recognition of this variant is important because previous reports
demonstrated that IMPC shows significantly more frequent
lymphovascular invasion and lymph node metastasis (1,3–7). Although rare, IMPC in the pancreas has
been described (8,9), but only one case series of IMPC of the
pancreas has been reported (8).
Khayyata et al analyzed IMPC occurring in the
ampullo-pancreatobiliary region, and revealed that 2.6% of
pancreatic carcinomas have an IMPC component (>20% of the tumor)
and these patients show a poor prognosis (8). However, only limited information
regarding the clinicopathological features of IMPC is
available.
In order to differentiate IMPC from carcinoma with
retraction artifacts, several markers, such as epithelial membrane
antigen (EMA), mucin core protein 1 (MUC1), and sialyl-Lewis X,
have been suggested for identifying reverse polarity in the
neoplastic nests of IMPC (10–12).
MUC1 is a type I transmembrane glycoprotein that belongs to the
family of mucin proteins and is expressed in various epithelial
cells, EMA is also expressed in various epithelial cells. The
protein kinase C (PKC) isoforms are protein kinases involved in
multiple signal transduction cascades (13). In particular, the PKCζ isoform is
reported that it is required for growth, invasion and tumorigenesis
(14), and plays an important role
in the maintenance of cell polarity and is expressed in the apical
portion of epithelial cells (13,15).
However, there are no studies using PKCζ immunostaining to detect
reverse polarity in the neoplastic nests of IMPC.
The aim of the present study is to clarify the
clinicopathological features of IMPC of the pancreas. Moreover, we
examine the usefulness of PKCζ immunostaining to detect reverse
polarity in IMPC.
Materials and methods
Patients and samples
Two hundred fifty-five patients with pancreatic
carcinoma underwent surgery at the Department of Surgery of Kansai
Medical University (Osaka, Japan) between January 2006 and December
2015. Patients who had metastasis to other organs, those who died
of other causes or complications, and those who were macroscopic
surgical margin-positive were excluded. Finally, 242 patients were
included in this study.
All resected surgical specimens were reviewed by at
least two diagnostic pathologists. We selected patients with ductal
adenocarcinoma with an IMPC component and evaluated the extent of
IMPC component in the tumor. All patients were staged according to
the 8th Union for International Cancer Control TNM Classification
(16).
The study was conducted in accordance with the
Declaration of Helsinki, and the study protocol was approved by the
institutional review board of our hospital (protocol no. 2017272).
Informed and written consents were obtained from the patients and
their relatives for the use of these clinical materials for
research.
Immunohistochemistry
Formalin-fixed and paraffin-embedded blocks of the
resected specimens were cut into 4-µm-thick sections,
deparaffinized, and rehydrated. Immunohistochemical analyses were
performed using an autostainer (Discovery XT System; Roche
Diagnostics) according to the manufacturer's instructions. A mouse
monoclonal antibody against MUC1 (H23, prediluted, Roche,), a mouse
monoclonal antibody against EMA (E-29, prediluted; Agilent
Technologies, Inc.), and a rabbit polyclonal antibody against PKCζ
(ab59364, 1:30; Abcam plc) were used as primary antibodies. Normal
pancreatic ducts were used as a positive control.
Immunohistochemical stainings were assessed independently by
pathologists blinded to the patients' clinical features.
Statistical analysis
Statistical analyses were performed using JMP 12
software (SAS Institute). Student's t-test was used to analyze
continuous variables, and χ2 and Fisher's exact
probability tests were used to analyze categorical variables.
P<0.05 was considered to indicate a statistically significant
difference. Cumulative survival rates were calculated using the
Kaplan-Meier method. Statistical differences in survival were
calculated using the log-rank test.
Results
Clinical characteristics
Table I summarizes
the clinicopathological features of patients in the present study.
This study included 101 women and 141 men. Fourteen patients had an
IMPC component (5.8%). In the IMPC group, 12 patients (85.7%) had
lymph node metastasis. There were no significant differences in
tumor location, T category, lymph node metastatic status,
preoperative serum carbohydrate antigen 19-9 (CA19-9) level, or
resection status between the IMPC and non-IMPC groups. Tumor size
in the IMPC group ranged from 20 to 65 mm (mean 37.3 mm; median
38.0 mm), and there was no significant difference compared to the
non-IMPC group (mean 35.5 mm; median 33.0 mm) (P=0.69).
 | Table I.Clinicopathological features of
pancreatic invasive ductal adenocarcinoma with and without IMPC
component. |
Table I.
Clinicopathological features of
pancreatic invasive ductal adenocarcinoma with and without IMPC
component.
| Variables | IMPC group (%) | No IMPC group
(%) | P-value |
|---|
| Sex |
|
| 0.0964 |
| Male | 5 (35.71) | 136 (59.65) |
|
|
Female | 9
(64.29) | 92 (40.35) |
|
| Age, years |
|
| 0.5183 |
| Mean | 66.50 | 68.19 |
|
|
Range | 53–82 | 36–86 |
|
| Location |
|
| 0.7755 |
| Ph | 10 (71.43) | 147 (64.47) |
|
| Pbt | 4
(28.57) | 81
(35.53) |
|
| T category |
|
| 1.0000 |
| 1+2 | 9
(64.29) | 146 (64.04) |
|
| 3+4 | 5
(35.71) | 82
(35.96) |
|
| Tumor size, mm |
|
| 0.6858 |
| Mean | 37.07 | 35.53 |
|
|
Range | 20–65 | 9–100 |
|
| Lymph node
metastasis |
|
| 0.3618 |
|
Negative | 2
(14.29) | 64
(28.07) |
|
|
Positive | 12 (85.71) | 164 (71.93) |
|
| R0/1 |
|
| 0.1879 |
| 0 | 9
(64.29) | 181 (79.39) |
|
| 1 | 5
(35.71) | 47
(20.61) |
|
| Serum CA19-9,
U/ml |
|
| 0.5447 |
|
<37 | 5
(35.71) | 63
(27.63) |
|
|
37< | 9
(64.29) | 165 (72.97) |
|
Histopathological characteristics
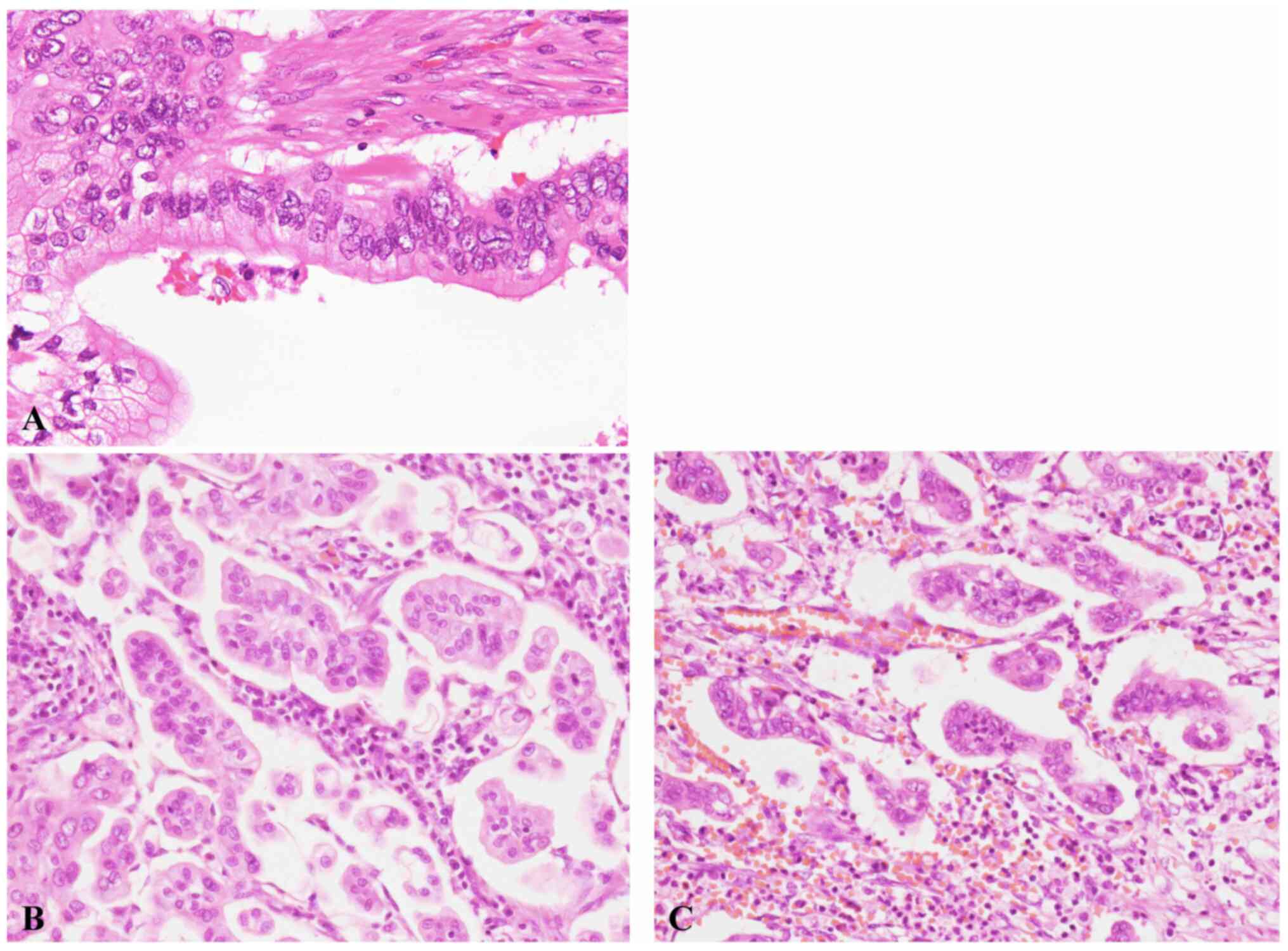
The characteristic histopathological features of
ductal adenocarcinoma and IMPC are shown in Fig. 1A and B. The neoplastic cells showed a
typical inside-out pattern surrounded by clear stromal space.
Table II summarizes the
clinicopathological characteristics of patients with pancreatic
ductal adenocarcinoma with IMPC component. The extent of IMPC
component ranged from 5 to 20% (Table
II). IMPC component accounted for 5% of the tumor in 10
patients, 10% in 2 patients, and 20% in 2 patients. All patients
had lymphovascular and perineural invasion, and the IMPC component
was usually present at the edge of the tumor. Neutrophilic
infiltration of the IMPC component was noted in 12 patients
(85.7%), and abundant neutrophilic infiltration was observed in 7
patients (50%). Neutrophils were present around and within the
tumor nests in the IMPC component (Fig.
1C). In most of these patients, neutrophilic infiltration was
much less frequent in the conventional adenocarcinoma region. No
neutrophilic infiltration was noted in 2 patients (cases 1 and
13).
| Table II.Cases of IMPC component. |
Table II.
Cases of IMPC component.
| Case | Sex | Age | IMPC component,
% | Tumor size, mm | N0/1 | ly or v | R0/1 | Overall survival,
months | Dead/Alive |
|---|
| 1 | M | 74 | 5 | 45 | 1 | 1 | 1 | 5 | Dead |
| 2 | F | 63 | 5 | 20 | 1 | 1 | 0 | 65 | Alive |
| 3 | F | 66 | 5 | 35 | 1 | 1 | 1 | 62 | Dead |
| 4 | F | 71 | 5 | 38 | 1 | 1 | 1 | 36 | Alive |
| 5 | M | 65 | 5 | 24 | 1 | 1 | 0 | 30 | Alive |
| 6 | F | 65 | 5 | 30 | 1 | 1 | 1 | 25 | Dead |
| 7 | F | 70 | 5 | 40 | 1 | 1 | 0 | 7 | Dead |
| 8 | F | 72 | 5 | 45 | 1 | 1 | 0 | 8 | Dead |
| 9 | M | 63 | 5 | 42 | 1 | 1 | 0 | 75 | Alive |
| 10 | F | 53 | 5 | 30 | 1 | 1 | 0 | 54 | Alive |
| 11 | F | 82 | 10 | 65 | 0 | 1 | 0 | 14 | Alive |
| 12 | M | 56 | 10 | 32 | 0 | 1 | 0 | 39 | Dead |
| 13 | M | 64 | 20 | 38 | 1 | 1 | 0 | 26 | Dead |
| 14 | F | 67 | 20 | 35 | 1 | 1 | 1 | 7 | Dead |
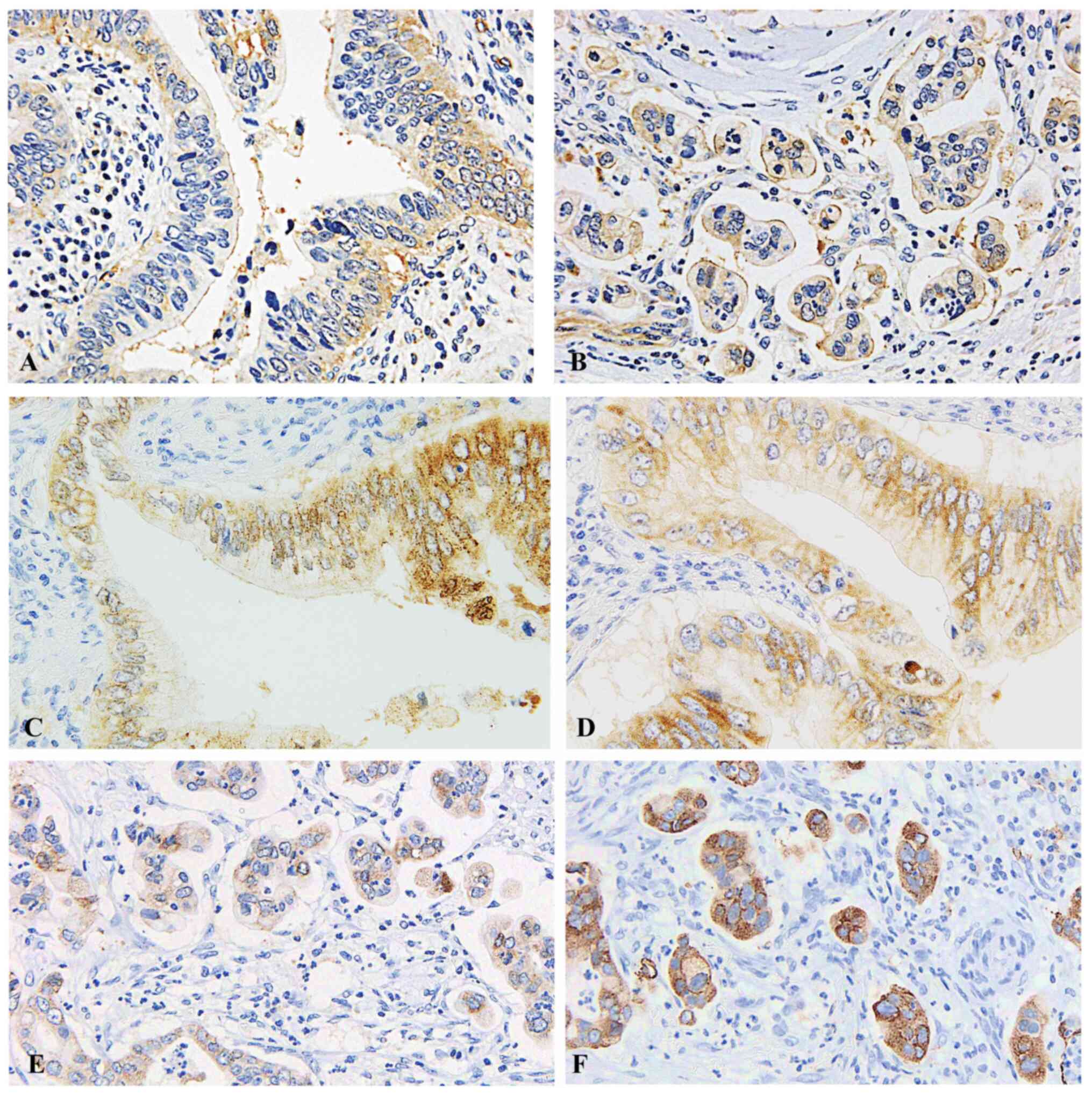
Immunohistochemical findings
PKCζ was expressed in the apical pole of the
neoplastic cells in conventional ductal adenocarcinoma (Fig. 2A). PKCζ was detected in the
stroma-facing surface of the neoplastic cell clusters of IMPC in
all patients with IMPC component, indicating reverse polarity
(Fig. 2B). Detection of reverse
polarity by PKCζ was clearer than detection by MUC1 or EMA
(Fig. 2E and F). As reference, MUC1
and EMA were expressed in the apical pole of the neoplastic cells
in conventional ductal adenocarcinoma (Fig. 2C and D).
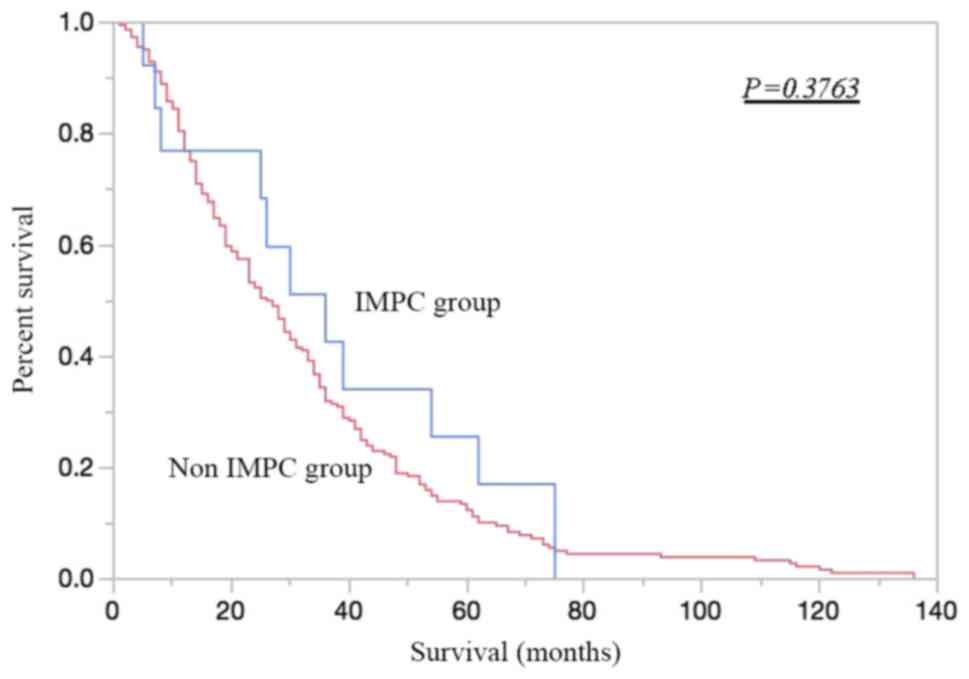
Clinical outcome
The follow-up period ranged from 5 to 75 months for
14 patients with IMPC component. Six patients (42.9%) are still
alive (14-75 months). The Kaplan-Meier curve showed no significant
difference in overall survival between the IMPC and non-IMPC groups
(P=0.38) (Fig. 3).
Discussion
In the present study, we demonstrated that the
frequency of IMPC in pancreatic ductal adenocarcinoma patients is
5.8%, although the extent of the IMPC component was less than 20%
in all of the patients with IMPC component, and the presence of
IMPC component (less than 20%) did not indicate a worse prognosis.
Moreover, we also clearly showed that PKCζ is a useful
immunohistochemical marker for detecting reverse polarity of IMPC
and this is the first report for usefulness.
The clinicopathological significance of IMPC has
been reported in several organs, including the breast (1,7) and
urinary bladder (6). However,
probably due to lack of recognition of this entity in the pancreas,
only one case series of IMPC (8) and
one case report of pure IMPC (9) in
the pancreas have been described in the English literature.
Khayyata et al reported IMPC in the pancreas for the first
time (8). They defined IMPC as
invasive micropapillary architecture in more than 20% of the tumor,
and the incidence of pancreatic IMPC was 2.6%. All IMPC components
were located in the pancreas head, and the characteristic
histopathological finding was abundant infiltration of neutrophils
around the tumor nests of IMPC. In the present series, we examined
pancreatic ductal adenocarcinoma with IMPC component regardless of
the extent, because the clinicopathological features of pancreatic
ductal adenocarcinoma with less than 20% IMPC component have not
been clarified. The frequency of pancreatic IMPC (5.8%) in this
study was higher than the results of the previous report (2.6%)
(8), although we included cases
where the extent of IMPC component was less than 20%. Neutrophilic
infiltration was observed in 85.7% of patients in the present
series, which may be a characteristic feature of pancreatic IMPCs,
because this has rarely been described in IMPCs occurring in other
organs (1,3–7).
Moreover, this study revealed that pancreatic IMPC can develop in
the pancreas body and tail (4/14 patients).
Most IMPCs found in various organs have a
conventional carcinoma component, and pure IMPC is rare. Even in
the breast, where IMPC most frequently develops, pure IMPC accounts
for approximately 0.9–2% of carcinomas (1,17). The
amount of micropapillary carcinoma component required for diagnosis
of IMPC has not been established yet, although the clinical
significance of the extent of IMPC component has been discussed
(1). Chen et al analyzed the
association of the amount of IMPC component and the
clinicopathological parameters, and they concluded that the
presence of IMPC component suggested higher incidence of lymph node
metastasis. However, there was no significant association between
the amount of IMPC component and lymph node and distant metastases,
although a trend was noted (18).
Khayyata et al reported that the prognosis of pancreatic
IMPC (all patients had >20% IMPC component) was poor, similar to
that of poorly differentiated pancreatic adenocarcinoma (8). In the present series, there was no
significant difference in overall survival between the IMPC and
non-IMPC groups (P=0.38). The results of the previous report
(8) and the present study do not
correspond to the above-mentioned clinical significance of the
presence of IMPC component in the breast (18). In this study, the limitation is that
the number of target patients is small. Therefore, additional large
studies are needed to clarify the clinical significance of the
amount of IMPC component in pancreatic ductal adenocarcinoma.
The PKC family is composed of 12 members, and is
grouped into three subclasses: Classical, novel, and atypical
(13). PKCζ is an atypical PKC.
Atypical PKCs play an important role in maintaining cell polarity
because they are present in the tight junctions, which physically
separate the apical and basolateral portions of the cell (13). PKCζ has also been reported to play a
role in the reorientation of polarity and lumen formation
(inside-out pattern) in Madin-Darby canine kidney cells (18). Accordingly, we speculated that PKCζ
could be used as a marker of reverse polarity in IMPC. We
demonstrated that PKCζ was expressed in the apical pole of the
neoplastic cells in conventional adenocarcinoma; in contrast, its
expression was noted in the stroma-facing surface of the neoplastic
cell clusters in the IMPC component, clearly showing reverse
polarity in IMPC. Several markers for demonstrating reverse
polarity in IMPC, including EMA, MUC1, and sialyl-Lewis X, have
been reported (10,11). However, immunostaining and evaluation
of these markers is not always easy due to the background
cytoplasmic staining, as shown in Fig.
2E and F. Staining with PKCζ was clearer than with EMA and
MUC1, and reverse polarity was easier to determine in all cases.
The present study demonstrated the usefulness of PKCζ, an apical
marker, to detect reverse polarity in IMPC; therefore, PKCζ must be
added as an immunohistochemical marker for detecting reverse
polarity, and this marker may be available for IMPC occurring in
other organs.
In summary, the present study demonstrated that IMPC
component (less than 20%) did not suggest a worse prognosis
(P=0.38) and there were no significant differences in tumor
location, T category, lymph node metastatic status, preoperative
CA19-9 level, or resection status between the IMPC and non-IMPC
groups. Moreover, immunostaining for PKCζ is useful for
demonstrating reverse polarity of neoplastic cells of IMPC.
Acknowledgements
This abstract was presented at The 50th Annual
Congress of the Korean Association of HBP Surgery on April 4, 2019
in Seoul, South Korea, and was published as Abstract no. BP OP 2-6.
The authors would like to thank Dr Tatsuma Sakaguchi (Department of
Surgery, Kansai Medical University, Osaka, Japan) for conference
presentation.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
HR and MI were responsible for the conception and
design of the study. HR and YE performed immunohistochemical
analyses. HR, MI, YE, HY, TY, HK, SH, SY, MK, YM, KT and SS were
involved in the acquisition, analysis and interpretation of data.
HR and MI confirm the authenticity of all raw data. HR and MI
drafted the manuscript and prepared figures. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Declaration of Helsinki, and the study protocol was approved by
the Kansai Medical University Hospital Ethics Review Committee
(protocol no. 2017272). Informed and written consents were obtained
from the patients and their relatives for the use of these clinical
materials for research.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
IMPC
|
invasive micropapillary carcinoma
|
|
EMA
|
epithelial membrane antigen
|
|
MUC1
|
mucin core protein
|
|
PKC
|
protein kinase C
|
|
CA19-9
|
carbohydrate antigen 19-9
|
References
|
1
|
Yang YL, Liu BB, Zhang X and Fu L:
Invasive micropapillary carcinoma of the breast: An update. Arch
Pathol Lab Med. 140:799–805. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fisher ER, Palekar AS, Redmond C, Barton B
and Fisher B: Pathologic findings from the National surgical
adjuvant breast project (protocol no. 4). VI. Invasive papillary
cancer. Am J Clin Pathol. 73:313–322. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nagao T, Gaffey TA, Visscher DW, Kay PA,
Minato H, Serizawa H and Lewis JE: Invasive micropapillary salivary
duct carcinoma: A distinct histologic variant with biologic
significance. Am J Surg Pathol. 28:319–326. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cakir E, Yilmaz A, Demirag F, Oguztuzun S,
Sahin S, Yazici UE and Aydin M: Prognostic significance of
micropapillary pattern in lung adenocarcinoma and expression of
apoptosis-related markers: Caspase-3, bcl-2, and p53. APMIS.
119:574–580. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Guzinska-Ustymowicz K, Niewiarowska K and
Pryczynicz A: Invasive micropapillary carcinoma: A distinct type of
adenocarcinomas in the gastrointestinal tract. World J
Gastroenterol. 20:4597–4606. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Comperat E, Roupret M, Yaxley J, Reynolds
J, Varinot J, Ouzaïd I, Cussenot O and Samaratunga H:
Micropapillary urothelial carcinoma of the urinary bladder: A
clinicopathological analysis of 72 cases. Pathology. 42:650–654.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Umeda T, Ishida M, Murata S, Mori T, Kawai
Y, Itoi N, Tomida K, Tanaka A, Sakai S, Kitamura M, et al:
Immunohistochemical analyses of CD44 variant isoforms in invasive
micropapillary carcinoma of the breast: Comparison with a
concurrent conventional invasive carcinoma of no special type
component. Breast Cancer. 23:869–875. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Khayyata S, Basturk O and Adsay NV:
Invasive micropapillary carcinomas of the ampullo-pancreatobiliary
region and their association with tumor-infiltrating neutrophils.
Mod Pathol. 18:1504–1511. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kitagawa H, Nakamura M, Tani T, Tajima H,
Nakagawara H, Ohnishi I, Takamura H, Kayahara M, Ohta T, Zen Y, et
al: A pure invasive micropapillary carcinoma of the pancreatic
head: Long disease-free survival after pancreatoduodenectomy and
adjuvant chemotherapy with gemcitabine. Pancreas. 35:190–192. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Acs G, Esposito NN, Rakosy Z, Laronga C
and Zhang PJ: Invasive ductal carcinomas of the breast showing
partial reversed cell polarity are associated with lymphatic tumor
spread and may represent part of a spectrum of invasive
micropapillary carcinoma. Am J Surg Pathol. 34:1637–1646. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nassar H, Pansare V, Zhang H, Che M, Sakr
W, Ali-Fehmi R, Grignon D, Sarkar F, Cheng J and Adsay V:
Pathogenesis of invasive micropapillary carcinoma: Role of MUC1
glycoprotein. Mod Pathol. 17:1045–1050. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wei J, Cui L, Liu F, Fan Y, Lang R, Gu F,
Guo X, Tang P and Fu L: E-selectin and Sialyl Lewis X expression is
associated with lymph node metastasis of invasive micropapillary
carcinoma of the breast. Int J Surg Pathol. 18:193–200. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rosse C, Linch M, Kermorgant S, Cameron
AJ, Boeckeler K and Parker PJ: PKC and the control of localized
signal dynamics. Nat Rev Mol Cell Biol. 11:103–112. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Butler AM, Scotti Buzhardt ML, Li S, Smith
KE, Fields AP and Murray NR: Protein kinase C zeta regulates human
pancreatic cancer cell transformed growth and invasion through a
STAT3-dependent mechanism. PLoS One. 8:e720612013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Whyte J, Thornton L, McNally S, McCarthy
S, Lanigan F, Gallagher WM, Stein T and Martin F: PKCzeta regulates
cell polarisation and proliferation restriction during mammary
acinus formation. J Cell Sci. 123:3316–3328. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Brierley J, Gospodarowicz MK and Wittekind
C: TNM classification of malignant tumours. John Wiley & Sons,
Inc.; Chichester, Hoboken, NJ: 2017
|
|
17
|
Guo X, Chen L, Lang R, Fan Y, Zhang X and
Fu L: Invasive micropapillary carcinoma of the breast: Association
of pathologic features with lymph node metastasis. Am J Clin
Pathol. 126:740–746. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chen L, Fan Y, Lang RG, Guo XJ, Sun YL,
Cui LF, Liu FF, Wei J, Zhang XM and Fu L: Breast carcinoma with
micropapillary features: Clinicopathologic study and long-term
follow-up of 100 cases. Int J Surg Pathol. 16:155–163. 2008.
View Article : Google Scholar : PubMed/NCBI
|