Thyroid cancer (TC) is the most common endocrine
malignant tumor, ranking ninth in incidence for both sexes and
representing the fifth most prevalent cancer in women (1). Most TCs are derived from follicular
cells and are classified into three main groups: a) differentiated
thyroid carcinoma (DTC) which includes papillary thyroid carcinoma
(PTC), follicular thyroid carcinoma (FTC) and Hürthle (oncocytic)
cell carcinoma (HCC); b) poorly differentiated thyroid carcinoma
(PDTC); and c) anaplastic thyroid carcinoma (ATC) (2).
PTC and FTC are the most common types of TC, have a
low overall mortality and are generally curable by surgery with or
without radioiodine treatment (3).
ATCs are rare undifferentiated cancers with no effective therapy,
having almost 100% disease-specific mortality (4–6). PDTCs
show limited evidence of follicular cell differentiation and are
morphologically and behaviorally intermediate between DTC and ATC
(2,7,8). PDTC
generally shows a poor response to radioiodine treatment and has an
overall 5-year survival rate of about 65%, thus necessitating more
effective therapies (2,8–10). Even
slight amounts of PDTC areas (≥10%) in a DTC affect the prognosis
significantly (11). Some HCCs are
also classified as PDTCs and have a worse prognosis than usual HCCs
(12,13).
Treatment of ATC must be carried out by a
multidisciplinary team generally requiring the combination of
surgery (as complete as possible), radiotherapy
(intensity-modulated radiotherapy) and conventional chemotherapy
using doxorubicin or taxanes (docetaxel or paclitaxel) usually with
cisplatin or carboplatin (4–6). Because these treatments are generally
not sufficient, newer therapies in development include single or
multi-tyrosine kinase inhibitors (MKIs), vascular disruptors, and
immunotherapy (6). Regarding MKIs,
the Food and Drug Administration have approved the combined
treatment with dabrafenib and trametinib for patients with locally
advanced or metastatic ATC and somatic BRAFV600E
mutation (14). Lenvatinib has
demonstrated an acceptable safety profile for Japanese patients
with unresectable thyroid tumors including ATC, regardless of
mutational status (15). Other
therapeutic options could include everolimus when somatic mutations
have been detected in the PI3K/mTOR pathway (16,17),
imatinib when overexpression of PDGF receptors are detected in
advanced ATC (18), and immune
checkpoint inhibitor (ICI) drugs targeting PD-1 or PD-L1 (6,19).
Programmed death ligand 1 (PD-L1), also designated
as CD274 or B7-H1, is expressed on activated lymphocytes, dendritic
cells, macrophages, healthy cells of different tissues and some
tumor cells (20,21). Programmed cell-death 1 (PD-1, CD279)
is a glycoprotein normally expressed by T lymphoid cells and
macrophages. The binding of PD-1 to its ligands PD-L1 and PD-L2
inhibits cytotoxic CD8+ T cell immune response and
facilitates the escape of the immune response to cells expressing
these ligands (20,21). Blockade of PD-L1 was effective in
inhibiting ATC in an in vivo model (BALB/c nude mice with
human ATC cells) (22). Using an
immunocompetent mouse model of orthotopic ATC, the combination of a
BRAFV600E inhibitor and anti-PD1/PD-L1 antibody
dramatically improved mouse survival with a tumor reduction along
with an increase in cytotoxic CD8+ T cells, NK cells and
M1-polarized tumor-associated macrophages (23). Additional studies in a mouse model of
orthotopic ATC confirmed that increased efficacy in reducing tumor
size and improving survival using an anti-PD1/PD-L1 checkpoint
inhibitor combined with an MKI (lenvatinib) was associated with a
modification of ATC microenvironment (24). Indoleamine 2,3-dioxygenase (IDO1) has
been associated with an altered tumor immune response; therefore
IDO1 inhibitors are being investigated in clinical trials in
combination with other ICIs (25).
A phase Ib proof-of-concept study of the anti-PD-1
antibody pembrolizumab in patients with advanced, PD-L1-positive
PTC or FTC evidenced antitumor activity in a minority of patients
treated (26). Another phase 2 trial
of pembrolizumab combined with chemoradiotherapy showed good
initial tolerance and effectiveness in locoregional disease control
but resulted in disappointing survival outcomes (27). A retrospective study of twelve ATC
patients, however, showed that in a subset of patients with ATC,
pembrolizumab may be an effective salvage therapy added to kinase
inhibitors (lenvatinib, dabrafenib + trametinib, trametinib alone)
at the time of progression of these drugs, encouraging the
incorporation of immunotherapy in patients with ATC (28). Another recent phase II clinical trial
to evaluate the efficacy and tolerability of a humanized monoclonal
antibody that binds PD-1 and blocks its interaction with PD-L1
(spartalizumab) was carried out in forty-two ATC patients (19). Interestingly, this study evidenced a
tumor response of 52.1% in the PD-L1-positive population and that
response was independent of BRAF mutational status (19). Several prospective studies are being
conducted using ICIs for the treatment of patients with ATC
(6), and an improvement in the
understanding of the immune microenvironment and the immune
biomarkers associated with these highly aggressive thyroid tumors
is highly relevant.
Thus, the aim of this study was to evaluate the
expression of PD-L1 and the tumor microenvironment in a series of
ATCs and PDTCs. We investigated the immunohistochemical expression
of PD-L1 in tumor cells, tumor-infiltrating lymphocytes (TILs) and
tumor associated macrophages (TAMs), along with the phenotypes of
TILs, TAMs and other cells.
We retrospectively analyzed the clinicopathological
data of a series of 26 patients who had undergone total or partial
thyroidectomy for ATC and/or PDTC at the Clinical University
Hospital of Santiago de Compostela (CHUS) and at the University
Hospital Complex of Ourense (CHOU), Spain. The inclusion criteria
included having a sufficient excess of tumor tissue fixed in
neutral, phosphate-buffered, 10% formalin and included in paraffin
blocks for additional immunohistochemical studies. Fifteen patients
had ATC and 11 patients had PDTC; PDTC areas coexisted with ATC in
two patients and these were also included in the study. The
patients consisted of 8 (30.7%) men and 18 (69.2%) women. The age
of patients ranged from 47 to 77 years with a mean age of
64.53±11.29 years (range 47–83) for ATC patients and 73.5±6.63
years (range 55–87) for PDTC patients (P=0.018). The patients were
followed from the time of histopathological diagnosis until death
or the moment of the last clinical follow-up, and clinical data
were retrieved from electronic medical records. The original
hematoxylin-eosin (H&E) slides from all cases were reviewed by
two expert thyroid pathologists (IA-N and JMC-T) and of each case,
a paraffin block containing sufficient representative tumor tissue
was selected for the additional immunohistochemical analyses of the
present study. Tumors were classified according to the criteria of
the latest World Health Organization (WHO) thyroid tumor
classification (2). All tissue
samples were provided by the Biobank of CHUS, integrated in the
Spanish National Biobank Network. The study was performed in
accordance with the declaration of Helsinki (and subsequent
ratifications) and approved by the Santiago-Lugo Medical Research
Ethics Committee (code: 2019/275). Written informed consent was
obtained.
Paraffin-embedded tumor tissue sections were stained
with H&E, and the immunohistochemical analyses were also
performed on 4µm-thick paraffin tissue sections with a
peroxidase-conjugated labeled dextran polymer (EnVision FLEX/HRP;
Dako), using 3,3′-diaminobenzidine as the chromogen (GC80611-2;
Dako). The primary antibodies and the conditions of use (clone,
concentration, antigenic recovery treatment and manufacturer) were
as follows: Thyroglobulin (TG) (code GA509, polyclonal,
ready-to-use, pH 6; Dako); calcitonin (code GA515, polyclonal,
ready-to-use, pH 6; Dako); PD-L1 (code GE006, clone 22C3, PD-L1 IHC
22C3 pharmDx, ready-to-use, pH 6; Dako), CD3 (code IR503,
polyclonal, ready-to-use, pH 9; Dako); CD4 (code IR649, clone 4B12,
ready-to-use, pH 9; Dako); CD8 (code IR623, clone C8/144B,
ready-to-use, pH 9; Dako); CD20 (code IR604, clone L26,
ready-to-use, pH 9; Dako); CD68 (code IR613, clone PGM1,
ready-to-use, pH 9; Dako); CD163 (code CM353AK, clone 10D6,
dilution 1:100, pH 9; Biocare Medical); S100 protein (code IR504,
polyclonal, ready-to-use, pH 9; Dako); p53 (code IR616, clone DO-7,
ready-to-use, pH 9; Dako); MLH1 (code IR079, clone E605,
ready-to-use, pH 9; Dako); MLH2 (code IR085, clone FE11,
ready-to-use, pH 9; Dako); MSH6 (code IR086, clone EP49,
ready-to-use, pH 9; Dako); and PMS2 (IR087, clone EP51,
ready-to-use, pH 9s; Dako). Non-tumorous thyroid tissue adjacent to
carcinoma (for thyroglobulin, MLH1, MSH2, MSH6 and PMS2), a
medullary thyroid carcinoma (for calcitonin), a lung adenocarcinoma
(for PD-L1), a colon cancer (for p53), and normal lymphoid tissue
of palatal tonsil (for CD3, CD4, CD8, CD20, CD68, CD163, and S100)
have been used as positive controls. Non-immune rabbit and mouse
serum samples were substituted for the primary antibodies as
negative control samples.
All immunostains were evaluated simultaneously by 2
investigators (IA-N and JMC-T) using a double-head optical
microscope (BX41TF; Olympus) until consensus was reached. Only
PD-L1 membranous staining of viable tumor cells was evaluated and
the tumor proportion score (TPS) represented the percentage of
PD-L1-positive tumor cells relative to all viable tumor cells. A
cutoff score ≥1% was used to define PD-L1 positivity. PD-L1
membranous staining was also scored in TILs and TAMs; stromal
immune cells distant from the tumor were excluded. Membranous
staining for CD4, CD8, and CD163, membranous/cytoplasmic staining
for CD3, CD20, CD68, and cytoplasmic/nuclear staining for S100 were
scored as 0 (negative), 1 (positive ≤10% of inflammatory cells), 2
(between 11 and 49%) and 3 (≥50%). Only nuclear staining was
considered positive for MLH1, MSH2, MSH6 and PMS2. For p53, diffuse
and strong nuclear staining (so-called ‘block staining’) and
complete loss of staining (‘null’ phenotype) were considered
positive (associated with mutations), while scattered, often weak
nuclear positivity was considered a negative (‘wild-type’) normal
p53 staining pattern.
The chi-square and Fisher's exact tests were, where
appropriate, used to investigate the association between
categorical variables. Student's t-test was used to evaluate the
statistical significance of the difference in the means between the
two groups. Survival analysis of differences between groups (ATC
vs. PDTC and PD-L1+ vs. PD-L1-) was performed using the
Kaplan-Meier method with the log-rank test. Differences with
P<0.05 were considered statistically significant. All
statistical analyses were performed using R statistical software
(version 4.0.3).
The main clinicopathological and immunohistochemical
characteristics of the study are shown in Tables I and II. In the ATC group (n=15), 60% of the
patients were women and 40% were men. Of the 15 ATC cases, 9 (60%)
tumors were morphologically subclassified as giant cell pattern, 3
(20%) as spindled cell pattern, and 3 (20%) as epithelial
(squamoid) cell pattern (Table I).
In the PDTC group (n=11), 81.8% of the patients were women and
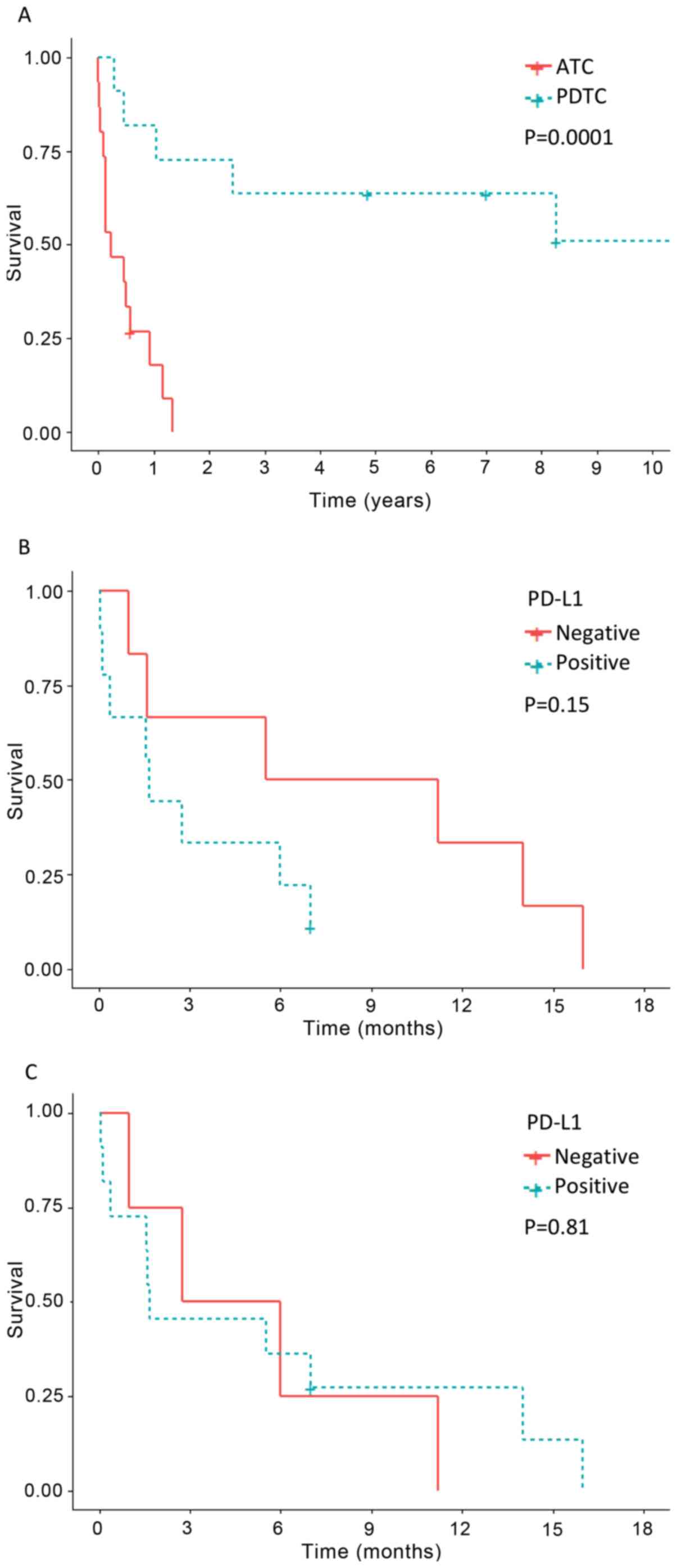
18.2% were men. Survival data appear in Table I and Fig.
1. Significant differences in survival were found when
comparing ATC and PDTC (P=0.0001); while 86.6% of patients with ATC
had died from the tumor after a mean follow-up of 5 months (range
0.1–16), only 54.5% of the patients with PDTC (without anaplastic
component) had died after a mean follow-up of 84.22 months (range
3.3–237) (Fig. 1).
The epithelial non-tumorous thyroid tissue adjacent
to PDTCs and ATCs showed positivity for thyroglobulin, MLH1, MSH2,
MSH6 and PMS2, but negativity for calcitonin, p53, PD-L1, CD3, CD4,
CD8, CD20, CD68 and S100 (Figs.
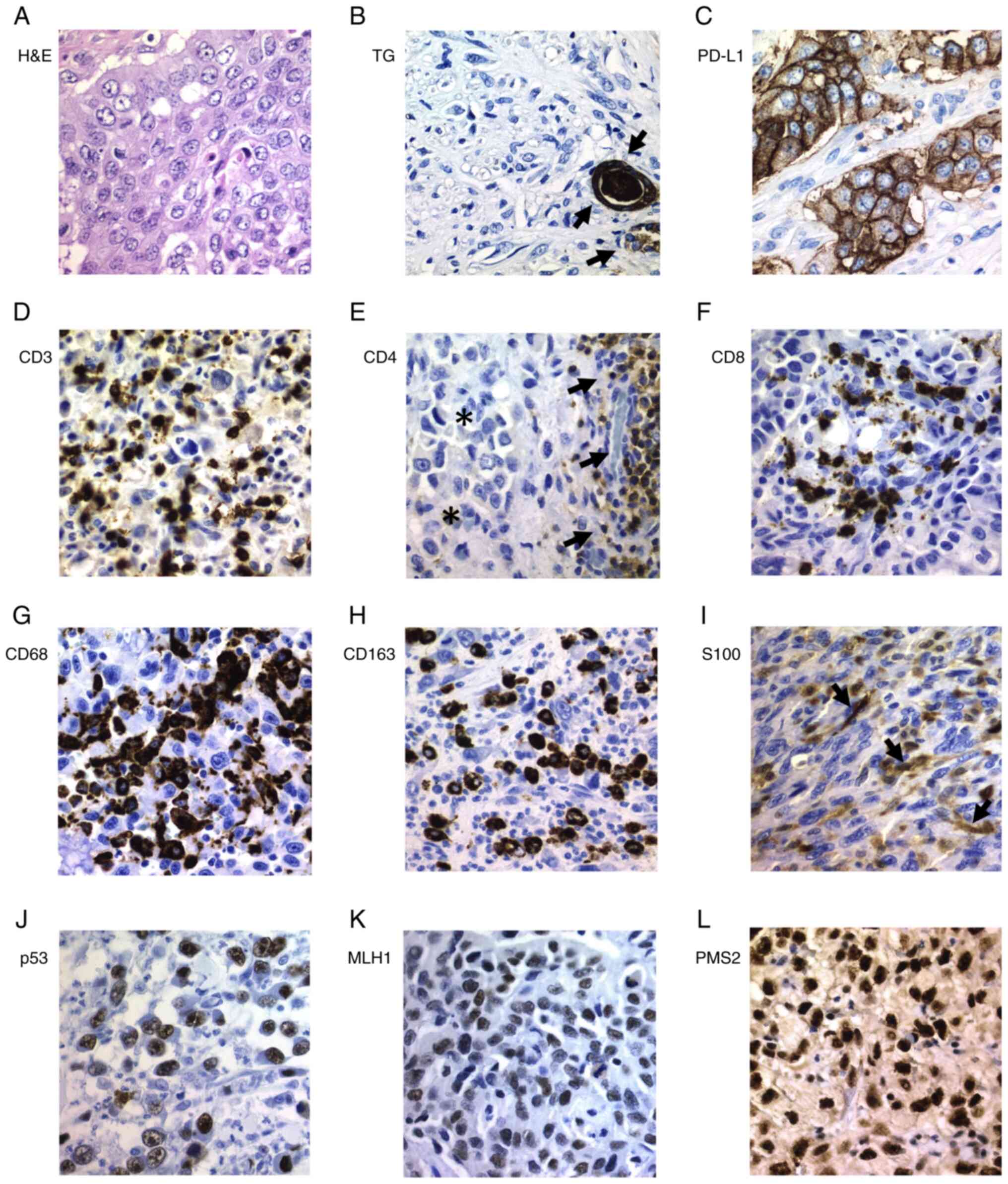
S1–S4). All ATC tumors were
negative for thyroglobulin (Fig. 2B)
and calcitonin while all PDTC tumors were positive for
thyroglobulin but negative for calcitonin. In the
immunohistochemical evaluation of PDTC areas present in the thyroid
tumors of two patients who had ATC, both tumor types were evaluated
independently as PDTCs and ATCs. Heterogeneous (focal or
multifocal) positivity for PD-L1 in tumor cells was detected in 60%
of ATC cases, in which the percentage of positive tumor cells
ranged from 15 to 90% (Tables I and
II). Positivity for PD-L1 was
detected in all cases of ATC with epithelial cell pattern and also
in different cases with other ATC patterns (Figs. 2–4).
PD-L1expression in ATC tumor cells was significantly higher than
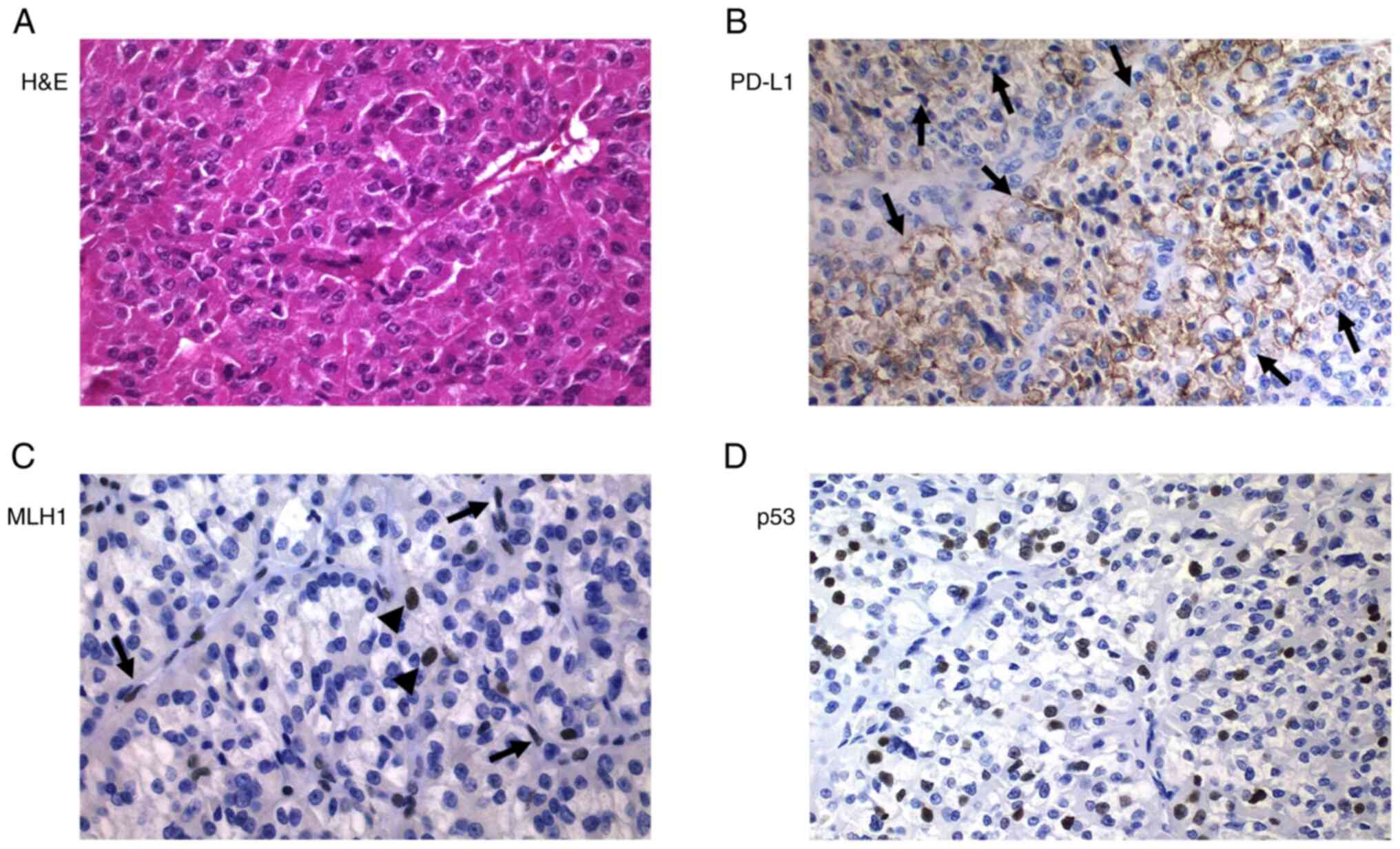
that in PDTC cases (60% vs. 7.7%, P=0.006) (Table II). The only case of PDTC with PD-L1
positive tumor cells (35%) was the one case of oncocytic cells, a
poorly differentiated Hürthle cell carcinoma (case 19) (Fig. 3). In the ATC group, a slightly higher
number of cases showed positivity for PD-L1 in TILs than in tumor
cells (73.3% vs. 60%), but neither PD-L1-positive TILs nor TAMs
were observed in the PDTC group (P=0.000) (Figs. 2–4).
Using TPS, PD-L1-positive ATC patients showed a trend for worse
survival than those with PD-L1-negative tumors (Fig. 1B), although the differences were not
significant (P=0.15). No difference in relation to survival was
found when comparing the expression of PD-L1 in ATC-TILs or TAMs
(P=0.81) (Fig. 1C).
Significant differences were found in the expression
of lymphocytic markers in ATC and PDTC (Tables I and II). All ATC cases showed CD3 and CD8
positive cells as well as a higher percentage of CD4 and CD20
positive cells, while no positivity for CD4 and CD20 was detected
in PDTC cases; when comparing the expression of all these lymphoid
markers in ATC and PDTC, the differences were significant (Table II). All ATCs showed a higher and
significant percentage of CD68, CD163 and S100 positive cells
compared to the group of PDTCs (Table
II) (Figs. 2,3 and 5).
While 11/15 (73.3%) of the ATCs showed an abnormal pattern of p53
protein expression, all PDTC cases except the poorly differentiated
Hürthle cell carcinoma case (7.7%) showed a p53 wild-type (i.e.,
normal) staining pattern (P=0.001). Expression of DNA mismatch
repair (MMR) proteins was detected in all cases except in one
single case with negativity for MLH1 and PMS2 in the ATC areas and
concomitant positivity for MLH1 in PDTC areas, as well as in
another case of PDTC (case 19) with a complete loss of nuclear MLH1
and PMS2 expression (Fig. 3).
The immunohistochemical expression of PD-L1 is
sometimes a prerequisite for the establishment of checkpoint
inhibitor therapy and has prognostic value in several types of
malignant tumors (21,29). Based on the encouraging results of
trials involving immunotherapy in the management of ATC (25), we have investigated PD-L1 expression
and tumor microenvironment (TME) in a series of 15 ATCs and 13
PDTCs.
Thyroid carcinogenesis arises and progresses
gradually as a result of the accumulation of various genetic and
epigenetic alterations (2,30,31).
There are early driver mutations shared by more than one category
of thyroid tumors (31,32) and DTCs have a relatively low level of
somatic mutations compared to cancers from other sites (33,34). The
rate of mutations, however, is higher in the PDTC group than in the
DTC group (35,36) and is much higher in the ATCs
(37,38). This model of tumor progression is
also supported, as in cases 6 and 15 of our series, by the
coexistence of differentiated and less-differentiated areas in some
thyroid tumors (39,40). The existence of cases of patients
with DTC whose tumor recurrence and/or metastasis included a PDTC
and/or an ATC (41) also supports
this model; the possibility of two independent tumors, however,
cannot be excluded. The mean age of patients with TC increases in
relation with the loss of tumor differentiation (2), further supporting the sequential model
of carcinogenesis. The older mean and median age of the 13 patients
with PDTC in our series contrasted with the findings of other
studies (42,43), but this could be attributed to biases
due to pathological diagnostic criteria and/or the limited number
of cases. The tumors in our series were classified according to the
WHO (2), applying the Turin criteria
(and algorithm) (7), which by
definition exclude PTCs. Other groups, such as the Memorial Sloan
Kettering Cancer Center (MSKCC) group, consider PDTC to be any
carcinoma with follicular cell differentiation that shows fresh
tumor necrosis and/or presence of ≥5 mitoses/10 high power
microscopic fields (×400), thus also including PTC-derived cases
(42,44). Given that PTC is more common in young
adults, the exclusion of PTCs with a BRAF-like signature
from the group of PDTCs in our series could explain the differences
(31,32). These different diagnostic criteria
(PDTC-Turin vs. PDTC-MSKCC), do, in fact, explain the variations in
the prevalence of ‘early’ genomic alterations in PDTC (RAS
mutations vs. BRAFV600E mutations, respectively)
(36,45).
In our series we found immunohistochemical
positivity for PD-L1 in tumor cells (TPS) of more than half of the
ATCs (60%) but in only one case of PDTC (7.7%). Similarly, PD-L1
expression was detected in TILs and TAMs from the ATC group (73.3%)
but not in the PDTC group, probably related to the higher
mutational load of ATCs (37,38). A
few studies reported the expression of PD-L1 in TCs. PD-L1
immunoexpression was found in 6.1 to 82.5% of PTCs (46,47),
including cases of papillary thyroid microcarcinoma (48) and cases with simultaneous chronic
thyroiditis and BRAF mutation (29,49). In
PTCs a significant association between PD-L1 expression and
BRAFV600E mutation has been reported in several
studies (48,49). Positivity for PD-L1 (clone E1L3N) and
IDO1 was detected in 7/28 (25%) and 2/28 (7.1%) respectively of a
series of PDTCs (50). Positivity
for PD-L1 using different antibodies (clones SP142, 5H1, E1L3N,
SP142, E1L3N, 22C3, 22C3, SP263 and SP263 respectively) was
detected in 2/9 (22.2%) (47), 3/13
(23.1%) (51), 14/49 (28.6%)
(52), 6/8 (75%) (53), 13/16 (81.2%) (54), 1/1 (100%) (55), 1/1 (100%) (56), 1/1 (100%) (22), 1/1 (100%) (57), 10/10 (100%) (28) of the ATCs but in none of the 6 (0%)
PDTCs studied by Ahn et al (47). Mutation load or tumor mutational
burden (TMB) represents the amount of somatic coding, base
substitution and indel mutations per megabase of genome studied in
each tumor, and high TMB is considered a new biomarker of
sensitivity to ICIs (34). It has
been postulated that a greater number of mutations would imply more
neoantigens and consequently more targets for activated immune
cells, which is why these tumors are good candidates for immune
checkpoint inhibitor therapy (21,58–60). In
human carcinogenesis, high TMB is mainly related to germline or
somatic alterations in the DNA MMR complex (61–63),
related to defects in genes involved in the recognition and removal
of errors during lagging- and leading-strand DNA replication such
as POLD1 and POLE genes, respectively (64–66),
and/or related to loss of function mutations in the TP53
gene (67), and other alterations
(68,69). ATCs are tumors with a high mutational
load (37), usually accompanied by
mutations of the TP53 gene (31,37),
which in our series was detected in 73.3% of ATCs. In the tumor of
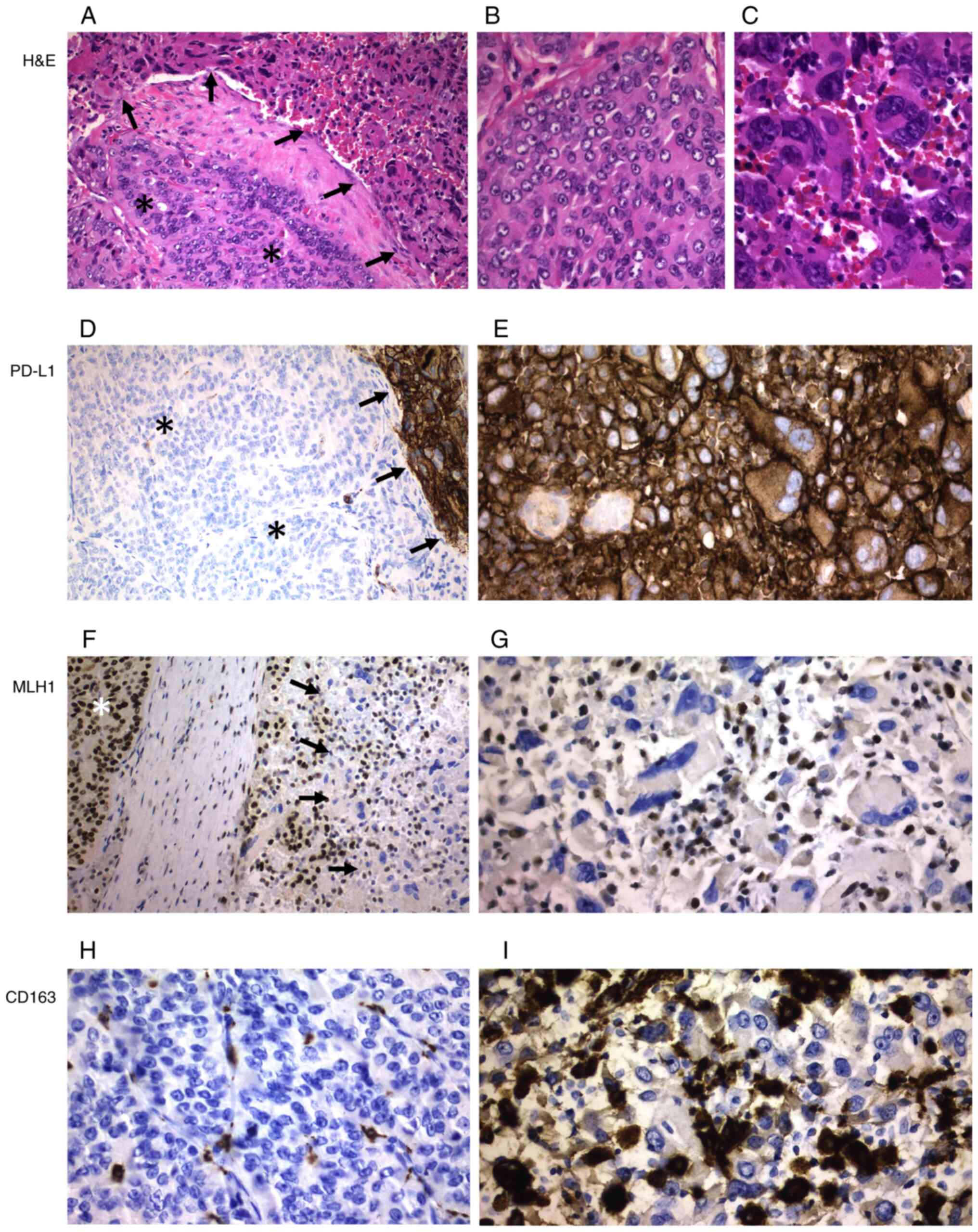
one of the patients in our series (case 15) (Fig. 5), the ATC areas showed the highest
positivity for PD-L1, positivity for p53 and loss of expression of
MLH1 and PMS2, while the areas of PDTC showed negativity for PD-L1,
a wild type pattern for p53 and conservation of the protein
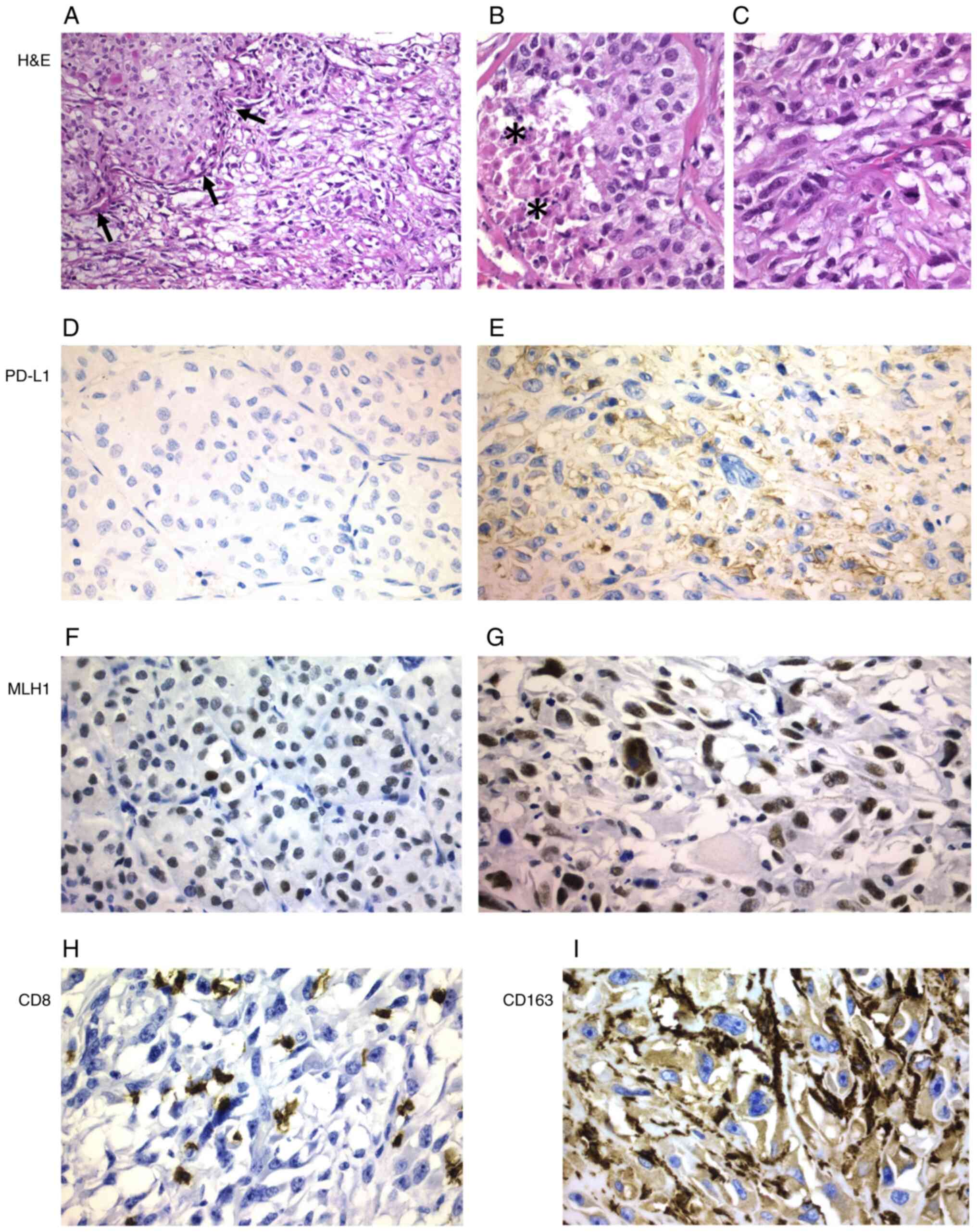
expression of the MMR genes. On the other hand, in the other tumor
combining anaplastic and poorly differentiated areas (case 6)
(Fig. 4), the expression of PD-L1
was limited to the ATC areas without detecting alterations related
to p53 or the MMR genes in any of the different tumor areas.
Interestingly, the only PDTC case with PD-L1 expression (case 19)
(Fig. 3), also showed positivity for
p53, but loss of MLH1 and PMS2 expression, fitting with the
proposed hypermutator role of the MLH mismatch-repair genes
reported in ATCs (37). In
colorectal cancer, a significantly higher expression of PD-L1 was
detected in tumors exhibiting MMR deficiency and BRAF
mutation (40); this also agrees
with the data from our series since BRAF mutation is
commonly an early event in the progression from conventional
(BRAF-like) PTC to ATC. BRAFV600E mutation
does not participate, however, in the development of the PDTC
defined by the Turin criteria (31).
Our study evidenced significant differences in TME
between the ATC and PDTC groups (Table
II). Similar to our data, a recent study using fluorescence
multiplex immunohistochemistry found significant differences
between ATC and advanced DTC in relation to PD-L1 expression and
lymphoid infiltration (70). We
found an exclusive presence of CD3+ CD8+
(cytotoxic) T lymphoid population and S100+ dendritic
cells infiltrating the tumor cells, with a minority of helper
(CD4+) T lymphocytes at the interface of the
tumor/normal thyroid tissue in all ATCs but in only one case (case
19) of PDTC. The role of TILs in PTC is controversial since its
association with both a favorable (71) and an unfavorable (72,73)
prognosis has been described. More specifically, a protumorigenic
role of FoxP3+ regulatory T cells (Treg) in DTC has been
demonstrated while CD8+ T cells develop an antitumor
function (73,74). In fact, exhausted PD-1+
CD8+ T lymphocytes appeared to be a marker of bad
prognosis and immunosuppression in DTC (73,74). In
PTCs, S100+ dendritic cells were more numerous when
compared to normal thyroid tissue (75), and CD1a+ dendritic cell
density was associated with better disease-free survival (71). Significant differences between ATCs
and PDTCs were also observed in our series in relation to tumor
infiltration by TAMs using a histiocytic pan-marker (CD68) as well
as CD163, a member of a scavenger receptor cysteine-rich
superfamily restricted to the monocyte/macrophage lineage
(histiocytic differentiation). Our data confirmed previous
observations indicating the over-representation of pro-tumor TAMs
in ATC and in advanced DTCs (71).
Our images also strongly support the existence of a very dense
network of interconnected CD163+ macrophages in direct
contact with intermingled cancer cells that may trap cells in the
tumor stroma (76), where they
correlate with poorer survival (71). Compared with type 1 inflammatory
macrophages, type 2 suppressor macrophages (CD163+)
promote invasiveness of human TC cell lines (77) and have also been associated with a
worse prognosis in cancers of other locations (78,79). Our
findings are consistent with a relationship between high TMB of
ATC, expression of neoantigens and changes in the immune system
(PD-L1 expression and changes in TME).
In a recent meta-analysis the association of PD-L1
and disease-free survival (DFS) remained strong in PTC when
compared with dedifferentiated thyroid carcinomas (ATC and PDTC) in
which a significant association with PD-L1 was not confirmed
(20). In another PDTC series, PD-L1
expression was significantly associated with tumor size and
multifocality as well as with a non-significant trend towards older
age, metastasis, an increased number of CD8+ T cells and
decreased disease-free and overall survival (50). In our series we found a significantly
higher expression of PD-L1 in TILs and TAMs in ATC group when
compared to the same expression in the PDTC group (P=0.0001). We
also found a trend towards worse survival in ATC with PD-L1
expression in tumor cells, but the figures did not reach
statistical significance, probably due to the limited number of
cases (Fig. 1B). No trend, however,
was evidenced when evaluating PD-L1 expression in TILs and TAMs. A
meta-analysis of non-medullary TC comprising 721 positive studies
showed an association between PD-L1 expression and disease
recurrence (49). PD-L1
up-regulation has recently been associated with poor
disease-specific survival in patients with ATC or advanced DTC
(43). This association between
PD-L1 expression and a poor prognosis has also been confirmed in
other tumors from different locations such as head and neck
(80), breast (81), kidney (81,82),
urothelial carcinoma (83),
non-small cell lung cancer (84),
colorectal cancer (85), and other
solid tumors (81,86).
Although this study has several limitations such as
its retrospective nature and the limited number of the sample,
which could lead to selection biases, there are invaluable data in
relation to immunotherapy. In fact, we can conclude that PD-L1
expression and tumor infiltration by CD3+CD8+
T lymphocytes, S100+ dendritic cells and
CD68+CD163+ macrophages is common in ATC but
rare in PDTC. Our findings also suggest that microsatellite
instability may also play a role in both TME as well as in the
identification of immunotherapy candidates among PDTC patients.
Not applicable.
The present study was supported in part by grant no.
ISCIII-PI19/01316 from Instituto de Salud Carlos III, State
Research Agency and Ministry of Science and Innovation (Spain),
with the participation of European FEDER funds.
All data generated or analyzed during this study are
included in this published article.
SCG, IAN, GRC, JGG and JMCT designed the study. SCG,
GRC and JGG collected the clinical data. JMCT and GRC are
responsible for confirming the authenticity of the data. SAS and
MSA performed the staining. IAN and JMCT evaluated the
immunohistochemical data. FGS performed the statistical analysis.
SCG, IAN and JMCT wrote the manuscript draft. SCG, SAS, MSA, GRC,
JGG, FGS, IAN and JMCT contributed to critical revision of the
manuscript for important intellectual content. JMCT obtained
financial support. All authors have read and approved the final
manuscript.
The study was approved by the Santiago-Lugo Medical
Research Ethics Committee (Santiago de Compostela, Spain; approval
no. 2019/275) and written informed consent was obtained.
Not applicable.
SCG, ORCID 0000-0002-2678-7230; SAS, ORCID
0000-0003-3576-1953; MSA, ORCID 0000-0003-0098-4161; GRC, ORCID
0000-0002-2015-7369; JGG, ORCID 0000-0002-5372-2467; FGS, ORCID
0000-0002-9681-1662; IAN, ORCID 0000-0003-1247-2331; and JMCT,
ORCID 0000-0002-5516-8914.
The authors declare that they have no competing
interests.
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lloyd RV, Osamura RY, Klöppel G and Rosai
J: WHO Classification of Tumours of Endocrine Organs. IARC; Lyon:
2017
|
|
3
|
Luster M, Aktolun C, Amendoeira I,
Barczyński M, Bible KC, Duntas LH, Elisei R, Handkiewicz-Junak D,
Hoffmann M, Jarząb B, et al: European Perspective on 2015 American
Thyroid Association Management Guidelines for adult patients with
thyroid nodules and differentiated thyroid cancer: Proceedings of
an Interactive International Symposium. Thyroid. 29:7–26. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Smallridge RC, Ain KB, Asa SL, Bible KC,
Brierley JD, Burman KD, Kebebew E, Lee NY, Nikiforov YE, Rosenthal
MS, et al: American Thyroid Association guidelines for management
of patients with anaplastic thyroid cancer. Thyroid. 22:1104–1139.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Haddad RI, Nasr C, Bischoff L, Busaidy NL,
Byrd D, Callender G, Dickson P, Duh QY, Ehya H, Goldner W, et al:
NCCN Guidelines Insights: Thyroid Carcinoma, Version 2.2018. J Natl
Compr Canc Netw. 16:1429–1440. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
De Leo S, Trevisan M and Fugazzola L:
Recent advances in the management of anaplastic thyroid cancer.
Thyroid Res. 13:172020. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Volante M, Collini P, Nikiforov YE,
Sakamoto A, Kakudo K, Katoh R, Lloyd RV, LiVolsi VA, Papotti M,
Sobrinho-Simoes M, et al: Poorly differentiated thyroid carcinoma:
The Turin proposal for the use of uniform diagnostic criteria and
an algorithmic diagnostic approach. Am J Surg Pathol. 31:1256–1264.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Xu B and Ghossein R: Poorly differentiated
thyroid carcinoma. Semin Diagn Pathol. 37:243–247. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Akaishi J, Kondo T, Sugino K, Ogimi Y,
Masaki C, Hames KY, Yabuta T, Tomoda C, Suzuki A, Matsuzu K, et al:
Prognostic impact of the Turin criteria in poorly differentiated
thyroid carcinoma. World J Surg. 43:2235–2244. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Walczyk A, Kopczyński J, Gąsior-Perczak D,
Pałyga I, Kowalik A, Chrapek M, Hejnold M, Góźdź S and Kowalska A:
Histopathology and immunohistochemistry as prognostic factors for
poorly differentiated thyroid cancer in a series of Polish
patients. PLoS One. 15:e02292642020. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dettmer M, Schmitt A, Steinert H,
Haldemann A, Meili A, Moch H, Komminoth P and Perren A: Poorly
differentiated thyroid carcinomas: How much poorly differentiated
is needed? Am J Surg Pathol. 35:1866–1872. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dettmer M, Schmitt A, Steinert H, Moch H,
Komminoth P and Perren A: Poorly differentiated oncocytic thyroid
carcinoma-diagnostic implications and outcome. Histopathology.
60:1045–1051. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bai S, Baloch ZW, Samulski TD, Montone KT
and LiVolsi VA: Poorly differentiated oncocytic (Hürthle cell)
follicular carcinoma: An institutional experience. Endocr Pathol.
26:164–169. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang JR, Zafereo ME, Dadu R, Ferrarotto R,
Busaidy NL, Lu C, Ahmed S, Gule-Monroe MK, Williams MD, Sturgis EM,
et al: Complete Surgical resection following neoadjuvant dabrafenib
plus trametinib in BRAF600E-mutated anaplastic thyroid
carcinoma. Thyroid. 29:1036–1043. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Takahashi S, Tahara M, Ito K, Tori M,
Kiyota N, Yoshida K, Sakata Y and Yoshida A: Safety and
effectiveness of lenvatinib in 594 patients with unresectable
thyroid cancer in an all-case post-marketing observational study in
Japan. Adv Ther. 37:3850–3862. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hanna GJ, Busaidy NL, Chau NG, Wirth LJ,
Barletta JA, Calles A, Haddad RI, Kraft S, Cabanillas ME,
Rabinowits G, et al: Genomic correlates of response to everolimus
in aggressive radioiodine-refractory thyroid cancer: A phase II
study. Clin Cancer Res. 24:1546–1553. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Harris EJ, Hanna GJ, Chau N, Rabinowits G,
Haddad R, Margalit DN, Schoenfeld J, Tishler RB, Barletta JA, Nehs
M, et al: Everolimus in anaplastic thyroid cancer: A case series.
Front Oncol. 9:1062019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ha HT, Lee JS, Urba S, Koenig RJ, Sisson
J, Giordano T and Worden FP: A phase II study of imatinib in
patients with advanced anaplastic thyroid cancer. Thyroid.
20:975–980. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Capdevila J, Wirth LJ, Ernst T, Ponce Aix
S, Lin CC, Ramlau R, Butler MO, Delord JP, Gelderblom H, Ascierto
PA, et al: PD-1 Blockade in Anaplastic Thyroid Carcinoma. J Clin
Oncol. 38:2620–2627. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Guan J, Lim KS, Mekhail T and Chang CC:
Programmed death ligand-1 (PD-L1) expression in the programmed
death receptor-1 (PD-1)/PD-L1 blockade: A key player against
various cancers. Arch Pathol Lab Med. 141:851–861. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
You W, Shang B, Sun J, Liu X, Su L and
Jiang S: Mechanistic insight of predictive biomarkers for antitumor
PD-1/PD-L1 blockade: A paradigm shift towards immunome evaluation
(Review). Oncol Rep. 44:424–437. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cantara S, Bertelli E, Occhini R, Regoli
M, Brilli L, Pacini F, Castagna MG and Toti P: Blockade of the
programmed death ligand 1 (PD-L1) as potential therapy for
anaplastic thyroid cancer. Endocrine. 64:122–129. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gunda V, Gigliotti B, Ndishabandi D, Ashry
T, McCarthy M, Zhou Z, Amin S, Freeman GJ, Alessandrini A and
Parangi S: Combinations of BRAF inhibitor and anti-PD-1/PD-L1
antibody improve survival and tumour immunity in an immunocompetent
model of orthotopic murine anaplastic thyroid cancer. Br J Cancer.
119:1223–1232. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gunda V, Gigliotti B, Ashry T, Ndishabandi
D, McCarthy M, Zhou Z, Amin S, Lee KE, Stork T, Wirth L, et al:
Anti-PD-1/PD-L1 therapy augments lenvatinib's efficacy by favorably
altering the immune microenvironment of murine anaplastic thyroid
cancer. Int J Cancer. 144:2266–2278. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Moretti S, Menicali E, Nucci N, Guzzetti
M, Morelli S and Puxeddu E: Therapy of endocrine disease
Immunotherapy of advanced thyroid cancer: From bench to bedside.
Eur J Endocrinol. 183:R41–R55. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mehnert JM, Varga A, Brose MS, Aggarwal
RR, Lin CC, Prawira A, de Braud F, Tamura K, Doi T, Piha-Paul SA,
et al: Safety and antitumor activity of the anti-PD-1 antibody
pembrolizumab in patients with advanced, PD-L1-positive papillary
or follicular thyroid cancer. BMC Cancer. 19:1962019. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Chintakuntlawar AV, Yin J, Foote RL,
Kasperbauer JL, Rivera M, Asmus E, Garces NI, Janus JR, Liu M, Ma
DJ, et al: A phase 2 study of pembrolizumab combined with
chemoradiotherapy as initial treatment for anaplastic thyroid
cancer. Thyroid. 29:1615–1622. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Iyer PC, Dadu R, Gule-Monroe M, Busaidy
NL, Ferrarotto R, Habra MA, Zafereo M, Williams MD, Gunn GB, Grosu
H, et al: Salvage pembrolizumab added to kinase inhibitor therapy
for the treatment of anaplastic thyroid carcinoma. J Immunother
Cancer. 6:682018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Girolami I, Pantanowitz L, Mete O,
Brunelli M, Marletta S, Colato C, Trimboli P, Crescenzi A,
Bongiovanni M, Barbareschi M and Eccher A: Programmed Death-Ligand
1 (PD-L1) is a potential biomarker of disease-free survival in
papillary thyroid carcinoma: A systematic review and meta-analysis
of PD-L1 immunoexpression in follicular epithelial derived thyroid
carcinoma. Endocr Pathol. 31:291–300. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bangaraiahgari R, Panchangam RB,
Puthenveetil P, Mayilvaganan S, Bangaraiahgari R, Banala RR,
Karunakaran P and Md R: Is there adenoma-carcinoma sequence between
benign adenoma and papillary cancer of thyroid: A genomic linkage
study. Ann Med Surg (Lond). 60:695–700. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Volante M, Lam AK, Papotti M and Tallini
G: Molecular pathology of poorly differentiated and anaplastic
thyroid cancer: What do pathologists need to know. Endocr Pathol.
32:63–76. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Soares P, Póvoa AA, Melo M, Vinagre J,
Máximo V, Eloy C, Cameselle-Teijeiro JM and Sobrinho-Simões M:
Molecular pathology of Non-familial follicular epithelial-derived
thyroid cancer in adults: From RAS/BRAF-like tumor designations to
molecular risk stratification. Endocr Pathol. 32:44–62. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Jung SH, Kim MS, Jung CK, Park HC, Kim SY,
Liu J, Bae JS, Lee SH, Kim TM, Lee SH and Chung YJ: Mutational
burdens and evolutionary ages of thyroid follicular adenoma are
comparable to those of follicular carcinoma. Oncotarget.
7:69638–69648. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Chalmers ZR, Connelly CF, Fabrizio D, Gay
L, Ali SM, Ennis R, Schrock A, Campbell B, Shlien A, Chmielecki J,
et al: Analysis of 100,000 human cancer genomes reveals the
landscape of tumor mutational burden. Genome Med. 9:342017.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Cancer Genome Atlas Research Network, .
Integrated genomic characterization of papillary thyroid carcinoma.
Cell. 159:676–690. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Landa I, Ibrahimpasic T, Boucai L, Sinha
R, Knauf JA, Shah RH, Dogan S, Ricarte-Filho JC, Krishnamoorthy GP,
Xu B, et al: Genomic and transcriptomic hallmarks of poorly
differentiated and anaplastic thyroid cancers. J Clin Invest.
126:1052–1066. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kunstman JW, Juhlin CC, Goh G, Brown TC,
Stenman A, Healy JM, Rubinstein JC, Choi M, Kiss N, Nelson-Williams
C, et al: Characterization of the mutational landscape of
anaplastic thyroid cancer via whole-exome sequencing. Hum Mol
Genet. 24:2318–2329. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Riesco-Eizaguirre G and Santisteban P:
Endocrine Tumours: Advances in the molecular pathogenesis of
thyroid cancer: Lessons from the cancer genome. Eur J Endocrinol.
175:R203–R217. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Capdevila J, Mayor R, Mancuso FM, Iglesias
C, Caratù G, Matos I, Zafón C, Hernando J, Petit A, Nuciforo P, et
al: Early evolutionary divergence between papillary and anaplastic
thyroid cancers. Ann Oncol. 29:1454–1460. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Ragazzi M, Torricelli F, Donati B,
Ciarrocchi A, de Biase D, Tallini G, Zanetti E, Bisagni A, Kuhn E,
Giordano D, et al: Coexisting well-differentiated and anaplastic
thyroid carcinoma in the same primary resection specimen:
Immunophenotypic and genetic comparison of the two components in a
consecutive series of 13 cases and a review of the literature.
Virchows Arch. 478:265–281. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Cameselle-Teijeiro JM, Rodríguez-Pérez I,
Celestino R, Eloy C, Piso-Neira M, Abdulkader-Nallib I, Soares P
and Sobrinho-Simões M: Hobnail variant of papillary thyroid
carcinoma: Clinicopathologic and molecular evidence of progression
to undifferentiated carcinoma in 2 cases. Am J Surg Pathol.
41:854–860. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ibrahimpasic T, Ghossein R, Shah JP and
Ganly I: Poorly Differentiated carcinoma of the thyroid gland:
Current status and future prospects. Thyroid. 29:311–321. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Yoo SK, Song YS, Lee EK, Hwang J, Kim HH,
Jung G, Kim YA, Kim SJ, Cho SW, Won JK, et al: Integrative analysis
of genomic and transcriptomic characteristics associated with
progression of aggressive thyroid cancer. Nat Commun. 10:27642019.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Hiltzik D, Carlson DL, Tuttle RM, Chuai S,
Ishill N, Shaha A, Shah JP, Singh B and Ghossein RA: Poorly
differentiated thyroid carcinomas defined on the basis of mitosis
and necrosis: A clinicopathologic study of 58 patients. Cancer.
106:1286–1295. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Gerber TS, Schad A, Hartmann N, Springer
E, Zechner U and Musholt TJ: Targeted next-generation sequencing of
cancer genes in poorly differentiated thyroid cancer. Endocr
Connect. 7:47–55. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Cunha LL, Marcello MA, Morari EC, Nonogaki
S, Conte FF, Gerhard R, Soares FA, Vassallo J and Ward LS:
Differentiated thyroid carcinomas may elude the immune system by
B7H1 upregulation. Endocr Relat Cancer. 20:103–110. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Ahn S, Kim TH, Kim SW, Ki CS, Jang HW, Kim
JS, Kim JH, Choe JH, Shin JH, Hahn SY, et al: Comprehensive
screening for PD-L1 expression in thyroid cancer. Endocr Relat
Cancer. 24:97–106. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Chowdhury S, Veyhl J, Jessa F, Polyakova
O, Alenzi A, MacMillan C, Ralhan R and Walfish PG: Programmed
death-ligand 1 overexpression is a prognostic marker for aggressive
papillary thyroid cancer and its variants. Oncotarget.
7:32318–32328. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Aghajani M, Graham S, McCafferty C,
Shaheed CA, Roberts T, DeSouza P, Yang T and Niles N:
Clinicopathologic and prognostic significance of programmed cell
death ligand 1 expression in patients with non-medullary thyroid
cancer: A systematic review and meta-analysis. Thyroid. 28:349–361.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Rosenbaum MW, Gigliotti BJ, Pai SI,
Parangi S, Wachtel H, Mino-Kenudson M, Gunda V and Faquin WC: PD-L1
and IDO1 are expressed in poorly differentiated thyroid carcinoma.
Endocr Pathol. 29:59–67. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Wu H, Sun Y, Ye H, Yang S, Lee SL and de
las Morenas A: Anaplastic thyroid cancer: Outcome and the
mutation/expression profiles of potential targets. Pathol Oncol
Res. 21:695–701. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Zwaenepoel K, Jacobs J, De Meulenaere A,
Silence K, Smits E, Siozopoulou V, Hauben E, Rolfo C, Rottey S and
Pauwels P: CD70 and PD-L1 in anaplastic thyroid cancer-promising
targets for immunotherapy. Histopathology. 71:357–365. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Bastman JJ, Serracino HS, Zhu Y, Koenig
MR, Mateescu V, Sams SB, Davies KD, Raeburn CD, McIntyre RC Jr,
Haugen BR and French JD: Tumor-Infiltrating T cells and the PD-1
checkpoint pathway in advanced differentiated and anaplastic
thyroid cancer. J Clin Endocrinol Metab. 101:2863–2873. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Chintakuntlawar AV, Rumilla KM, Smith CY,
Jenkins SM, Foote RL, Kasperbauer JL, Morris JC, Ryder M, Alsidawi
S, Hilger C and Bible KC: Expression of PD-1 and PD-L1 in
anaplastic thyroid cancer patients treated with multimodal therapy:
Results from a retrospective study. J Clin Endocrinol Metab.
102:1943–1950. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Kollipara R, Schneider B, Radovich M, Babu
S and Kiel PJ: Exceptional response with immunotherapy in a patient
with anaplastic thyroid cancer. Oncologist. 22:1149–1151. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Aghajani MJ, Cooper A, McGuire H, Jeffries
T, Saab J, Ismail K, de Souza P, Bray V, Fazekas de St Groth B,
Niles N and Roberts TL: Pembrolizumab for anaplastic thyroid
cancer: A case study. Cancer Immunol Immunother. 68:1921–1934.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Stenman A, Hellgren LS, Jatta K, Hysek M,
Zemmler M, Altena R, Nilsson IL, Bränström R, Zedenius J and Juhlin
CC: Metastatic anaplastic thyroid carcinoma in complete remission:
Morphological, molecular, and clinical work-up of a rare case.
Endocr Pathol. 31:77–83. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Snyder A, Makarov V, Merghoub T, Yuan J,
Zaretsky JM, Desrichard A, Walsh LA, Postow MA, Wong P, Ho TS, et
al: Genetic basis for clinical response to CTLA-4 blockade in
melanoma. N Engl J Med. 371:2189–2199. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Le DT, Uram JN, Wang H, Bartlett BR,
Kemberling H, Eyring AD, Skora AD, Luber BS, Azad NS, Laheru D, et
al: PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl
J Med. 372:2509–2520. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Mehnert JM, Panda A, Zhong H, Hirshfield
K, Damare S, Lane K, Sokol L, Stein MN, Rodriguez-Rodriquez L,
Kaufman HL, et al: Immune activation and response to pembrolizumab
in POLE-mutant endometrial cancer. J Clin Invest. 126:2334–2340.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Duval A and Hamelin R: Mutations at coding
repeat sequences in mismatch repair-deficient human cancers: Toward
a new concept of target genes for instability. Cancer Res.
62:2447–2454. 2002.PubMed/NCBI
|
|
62
|
Peltomäki P: Role of DNA mismatch repair
defects in the pathogenesis of human cancer. J Clin Oncol.
21:1174–1179. 2003. View Article : Google Scholar
|
|
63
|
Mensenkamp AR, Vogelaar IP, van
Zelst-Stams WA, Goossens M, Ouchene H, Hendriks-Cornelissen SJ,
Kwint MP, Hoogerbrugge N, Nagtegaal ID and Ligtenberg MJ: Somatic
mutations in MLH1 and MSH2 are a frequent cause of mismatch-repair
deficiency in Lynch syndrome-like tumors. Gastroenterology.
146:643–646 e8. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Briggs S and Tomlinson I: Germline and
somatic polymerase ε and δ mutations define a new class of
hypermutated colorectal and endometrial cancers. J Pathol.
230:148–153. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Church DN, Briggs SE, Palles C, Domingo E,
Kearsey SJ, Grimes JM, Gorman M, Martin L, Howarth KM, Hodgson SV,
et al: DNA polymerase epsilon and δ exonuclease domain mutations in
endometrial cancer. Hum Mol Genet. 22:2820–2828. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Domingo E, Freeman-Mills L, Rayner E,
Glaire M, Briggs S, Vermeulen L, Fessler E, Medema JP, Boot A,
Morreau H, et al: Somatic POLE proofreading domain mutation, immune
response, and prognosis in colorectal cancer: A retrospective,
pooled biomarker study. Lancet Gastroenterol Hepatol. 1:207–216.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Petitjean A, Mathe E, Kato S, Ishioka C,
Tavtigian SV, Hainaut P and Olivier M: Impact of mutant p53
functional properties on TP53 mutation patterns and tumor
phenotype: Lessons from recent developments in the IARC TP53
database. Hum Mutat. 28:622–629. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Lawrence MS, Stojanov P, Polak P, Kryukov
GV, Cibulskis K, Sivachenko A, Carter SL, Stewart C, Mermel CH,
Roberts SA, et al: Mutational heterogeneity in cancer and the
search for new cancer-associated genes. Nature. 499:214–218. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Poulos RC, Wong YT, Ryan R, Pang H and
Wong JWH: Analysis of 7,815 cancer exomes reveals associations
between mutational processes and somatic driver mutations. PLoS
Genet. 14:e10077792018. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Ahn J, Jin M, Song E, Ryu YM, Song DE, Kim
SY, Kim TY, Kim WB, Shong YK, Jeon MJ and Kim WG: Immune profiling
of advanced thyroid cancers using fluorescent multiplex
immunohistochemistry. Thyroid. 31:61–67. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Ferrari SM, Fallahi P, Galdiero MR,
Ruffilli I, Elia G, Ragusa F, Paparo SR, Patrizio A, Mazzi V,
Varricchi G, et al: Immune and inflammatory cells in thyroid cancer
microenvironment. Int J Mol Sci. 20:44132019. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
French JD, Weber ZJ, Fretwell DL, Said S,
Klopper JP and Haugen BR: Tumor-associated lymphocytes and
increased FoxP3+ regulatory T cell frequency correlate with more
aggressive papillary thyroid cancer. J Clin Endocrinol Metab.
95:2325–2333. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
French JD, Kotnis GR, Said S, Raeburn CD,
McIntyre RC Jr, Klopper JP and Haugen BR: Programmed death-1+ T
cells and regulatory T cells are enriched in tumor-involved lymph
nodes and associated with aggressive features in papillary thyroid
cancer. J Clin Endocrinol Metab. 97:E934–E943. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Severson JJ, Serracino HS, Mateescu V,
Raeburn CD, McIntyre RC Jr, Sams SB, Haugen BR and French JD:
PD-1+Tim-3+ CD8+ T lymphocytes display varied degrees of functional
exhaustion in patients with regionally metastatic differentiated
thyroid cancer. Cancer Immunol Res. 3:620–630. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Hilly O, Koren R, Raz R, Rath-Wolfson L,
Mizrachi A, Hamzany Y, Bachar G and Shpitzer T: The role of
s100-positive dendritic cells in the prognosis of papillary thyroid
carcinoma. Am J Clin Pathol. 139:87–92. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Caillou B, Talbot M, Weyemi U,
Pioche-Durieu C, Al Ghuzlan A, Bidart JM, Chouaib S, Schlumberger M
and Dupuy C: Tumor-associated macrophages (TAMs) form an
interconnected cellular supportive network in anaplastic thyroid
carcinoma. PLoS One. 6:e225672011. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Fang W, Ye L, Shen L, Cai J, Huang F, Wei
Q, Fei X, Chen X, Guan H, Wang W, et al: Tumor-associated
macrophages promote the metastatic potential of thyroid papillary
cancer by releasing CXCL8. Carcinogenesis. 35:1780–1787. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Zhang M, He Y, Sun X, Li Q, Wang W, Zhao A
and Di W: A high M1/M2 ratio of tumor-associated macrophages is
associated with extended survival in ovarian cancer patients. J
Ovarian Res. 7:192014. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Yuan A, Hsiao YJ, Chen HY, Chen HW, Ho CC,
Chen YY, Liu YC, Hong TH, Yu SL, Chen JJ and Yang PC: Opposite
effects of M1 and M2 macrophage subtypes on lung cancer
progression. Sci Rep. 5:142732015. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Li J, Wang P and Xu Y: Prognostic value of
programmed cell death ligand 1 expression in patients with head and
neck cancer: A systematic review and meta-analysis. PLoS One.
12:e01795362017. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Wang Q, Liu F and Liu L: Prognostic
significance of PD-L1 in solid tumor: An updated meta-analysis.
Medicine (Baltimore). 96:e63692017. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Xu F, Xu L, Wang Q, An G, Feng G and Liu
F: Clinicopathological and prognostic value of programmed death
ligand-1 (PD-L1) in renal cell carcinoma: A meta-analysis. Int J
Clin Exp Med. 8:14595–14603. 2015.PubMed/NCBI
|
|
83
|
Powles T, Walker J, Andrew Williams J and
Bellmunt J: The evolving role of PD-L1 testing in patients with
metastatic urothelial carcinoma. Cancer Treat Rev. 82:1019252020.
View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Pan ZK, Ye F, Wu X, An HX and Wu JX:
Clinicopathological and prognostic significance of programmed cell
death ligand1 (PD-L1) expression in patients with non-small cell
lung cancer: A meta-analysis. J Thorac Dis. 7:462–470.
2015.PubMed/NCBI
|
|
85
|
Siraj AK, Parvathareddy SK,
Annaiyappanaidu P, Haqawi W, Al-Rasheed M, AlManea HM, AlHussaini
HF, Al-Dayel F and Al-Kuraya KS: PD-L1 expression is associated
with deficient mismatch repair and poor prognosis in middle eastern
colorectal cancers. J Pers Med. 11:732021. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Walter D, Herrmann E, Schnitzbauer AA,
Zeuzem S, Hansmann ML, Peveling-Oberhag J and Hartmann S: PD-L1
expression in extrahepatic cholangiocarcinoma. Histopathology.
71:383–392. 2017. View Article : Google Scholar : PubMed/NCBI
|