Introduction
Trifluridine (FTD)/tipiracil (TPI) are nucleoside
antineoplastic agents that are used in 1:0.5 molar ratio as a novel
oral treatment (1). FTD is an active
anticancer agent that possibly mediates its effect by inducing DNA
dysfunction through direct uptake into DNA after oral
administration. TPI specifically inhibits thymidine phosphorylase,
the enzyme that degrades FTD, increasing the bioavailability of FTD
(1–3). FTD/TPI has a different mechanism of
action from conventional antineoplastic agents such as
5-fluorouracil. Moreover, a preclinical study has shown the effect
of FTD/TPI on tumors with low susceptibility to pyrimidine
fluoride-based antineoplastic agents (4). Following a phase III trial comparing
FTD/TPI monotherapy and best supportive care (BSC) (5,6), FTD/TPI
was approved for patients with metastatic colorectal cancer (mCRC)
with refractory to conventional standard chemotherapy in Japan, the
US, and the Europe Union (7–9). One of the predictive factors of FTD/TPI
efficacy is chemotherapy-induced neutropenia (CIN), which is well
known as the most common adverse event of this drug (10). The predictive nature of CIN is
attributed to a dose-response relationship between FTD exposure and
neutropenia, in agreement with the findings of a dose-escalation
study that a higher rate of neutropenia at higher FTD and TPI doses
implies greater drug efficacy (10).
In addition, FTD/TPI plus bevacizumab (Bev) is an alternative
treatment option as a third- or later-line chemotherapy for
patients with mCRC, as this treatment is safe and leads to a higher
disease control rate (DCR) and longer progression-free survival
(PFS) and overall survival (OS), than FTD/TPI monotherapy.
Nevertheless, there are only a few phase I/II (11–13) or
randomized phase II trials (14)
investigating the efficacy of FTD/TPI + Bev. Moreover, because the
PFS following this salvage-line treatment is still low, predictors
of early treatment efficacy are important to help optimize
treatment strategies; however, the efficacy predictors of FTD/TPI +
Bev remain unclear. Therefore, this study aimed to evaluate the
clinical outcomes of FTD/TPI + Bev and to explore predictors of its
efficacy.
Materials and methods
Patients
This is a retrospective cohort study in a single
institute in Japan. Patients with mCRC who received FTD/TPI + Bev
at the Cancer Institute Hospital, Japanese Foundation for Cancer
Research, from January 2017 to August 2020 were enrolled. This
study was approved by the Institutional Review Board of the
Japanese Foundation for Cancer Research (Tokyo, Japan, registry
number 2020-1017). The protocol was described on the hospital
website, and subjects were provided the opportunity to opt-out;
therefore, no additional consent was required from patients. All
the data were readily available and not taken specifically for this
study. All methods were performed in accordance with the
Declaration of Helsinki.
Treatment schedule
FTD/TPI (35 mg/m2) was administered
orally twice daily, after breakfast and dinner, for 5 days a week
for 2 weeks, followed by a 14-day rest, and then Bev (5 mg/kg) was
administered via intravenous infusion for 30 min every 2 weeks.
This treatment cycle was repeated every 4 weeks until tumor
progression or unacceptable toxicity occurred or at the patient's
request. Dose reductions and treatment discontinuations were
performed owing to toxicity, disease progression, or based on the
physician's decisions (11).
Study endpoints
Tumor response was assessed by computed tomography
using the RECIST guidelines, v1.1. Complete response (CR) was
defined as the complete disappearance of all detectable evidence of
disease as determined using total body computed tomography. Partial
response (PR) was defined as a minimum of 30% decrease in the sum
of target lesion diameters. Stable disease (SD) was defined as
everything between a 30% decrease and a 20% growth in tumor size.
Progressive disease was defined as a minimum of 20% increase in the
sum of target lesion diameters. Objective response rate (ORR)
implied the proportion of patients who showed CR or PR to therapy,
and DCR indicated the proportion of patients who showed CR, PR, or
SD response to therapy. PFS was defined as the time from the first
day of treatment to either the first objective evidence of disease
progression or death from any cause. OS was defined as the time
from the first day of treatment until the time of death. Toxicity
was graded according to the Common Toxicity Criteria for Adverse
Events v4.0, both within the first cycle and at all periods of
treatment. Neutrophils were measured during the first cycle
treatment or just before the initiation of second cycle treatment,
which was defined as CIN within the first cycle of the treatment.
We also evaluated the relationship between clinical outcomes of
FTD/TPI + Bev and neutropenia within the first cycle.
Statistical analysis
PFS and OS were estimated using the Kaplan-Meier
method, and the statistical significance of the correlation between
the clinical outcome and clinical parameters was assessed using the
log-rank test. We compared the categorical characteristics by
conducting the Pearson's χ2 tests. Statistical tests
provided two-sided P values, with P<0.05 considered significant.
In the Cox proportional hazard analysis, factors with P<0.05 in
the univariate analysis were included in the multivariate analysis
(backward stepwise methods). Statistical analyses were conducted
using the EZR statistical software (Saitama Medical Center, Jichi
Medical University, Saitama, Japan) 1.41 based on R and R commander
(15).
Results
Patient characteristics
The characteristics of 94 patients with mCRC who
received FTD/TPI + Bev are summarized in Table I. The median age at the time of data
collection was 60 (range, 32–82) years. Of the 94 patients, 37 were
male (39.3%). The lung was the most frequent site of metastasis
(73.4%), followed by the liver (59.6%), lymph node (48.9%), and
peritoneum (42.6%) at the start of FTD/TPI + Bev. Fifty-seven
patients (60.5%) harbored RAS mutants in their tumor
tissues. There were no significant differences in clinical
characteristics between mCRC patients with and without grade 3 or 4
neutropenia within the first cycle of treatment (Table SI).
 | Table I.Patient demographics and clinical
characteristics (n=94). |
Table I.
Patient demographics and clinical
characteristics (n=94).
| Characteristic | Number of patients,
n (%) |
|---|
| Median age at
enrollment, years (range) | 60 (32–82) |
| Sex |
|
|
Male | 37 (39.3) |
|
Female | 57 (60.7) |
| ECOG PS |
|
| 0 | 64 (68.1) |
| 1 | 24 (25.5) |
| 2 | 6 (6.4) |
| Primary site |
|
|
Right-sided colon | 26 (27.7) |
|
Left-sided colon | 68 (72.3) |
| Metastatic
site |
|
|
Lung | 69 (73.4) |
|
Liver | 56 (59.6) |
| Lymph
node | 46 (48.9) |
|
Peritoneal | 40 (42.6) |
|
Other | 26 (27.7) |
| RAS status
in tissue |
|
|
Wild-type | 37 (39.4) |
|
Mutant | 57 (60.6) |
| Time from the start
of first-line chemotherapy, months |
|
|
<18 | 32 (34.0) |
|
≥18 | 60 (63.8) |
|
Unknown | 2 (2.2) |
| Number of prior
regimens |
|
| 1 | 0 (0.0) |
| 2 | 68 (72.3) |
| 3 | 22 (23.4) |
| 4 | 4 (4.3) |
| Prior regimens |
|
|
Fluoropyrimidine | 94 (100.0) |
|
Irinotecan | 94 (100.0) |
|
Oxaliplatin | 93 (98.9) |
|
Angiogenesis inhibitor | 94 (100.0) |
|
Anti-EGFR antibodies | 18 (19.1) |
| Number of
metastasis |
|
| 1 | 10 (10.6) |
|
>1 | 84 (89.4) |
Toxicity
We reviewed the adverse events (AEs) of patients
with mCRC who received FTD/TPI + Bev. Grade 3 or 4 AEs in all
treatment periods occurred in 56 patients (59.6%). AE occurrences
in 94 patients with mCRC are summarized in Table II. There were no treatment-related
deaths. The most common grade 3 or 4 AEs were neutropenia (51.1%),
anemia (13.8%), and thrombocytopenia (6.4%), respectively. Febrile
neutropenia occurred in one patient (1.1%). Grade 3 or 4
neutropenia in the first cycle of treatment occurred in 26 patients
(27.7%). There were significant differences in the incidence of
leucopenia, anemia, thrombocytopenia, and hypertension between
patients with and without grade 3 or 4 CIN within the first cycle
of treatment (Table SII).
| Table II.Incidence of adverse events during
treatment period. |
Table II.
Incidence of adverse events during
treatment period.
| Adverse event | Any grade, n
(%) | Grade 3 or 4, n
(%) |
|---|
| Anemia | 45 (47.9) | 13 (13.8) |
| Neutropenia | 71 (75.5) | 48 (51.1) |
|
Thrombocytopenia | 18 (19.1) | 6 (6.4) |
| Anorexia | 20 (21.3) | 0 (0.0) |
| Vomiting | 15 (16.0) | 0 (0.0) |
| Nausea | 47 (50.0) | 0 (0.0) |
| Diarrhea | 16 (17.0) | 0 (0.0) |
| Febrile
neutropenia | 1 (1.1) | 1 (1.1) |
| Hypertension | 12 (12.8) | 0 (0.0) |
| Proteinuria | 33 (35.1) | 0 (0.0) |
Survival endpoints and factors
associated with survival
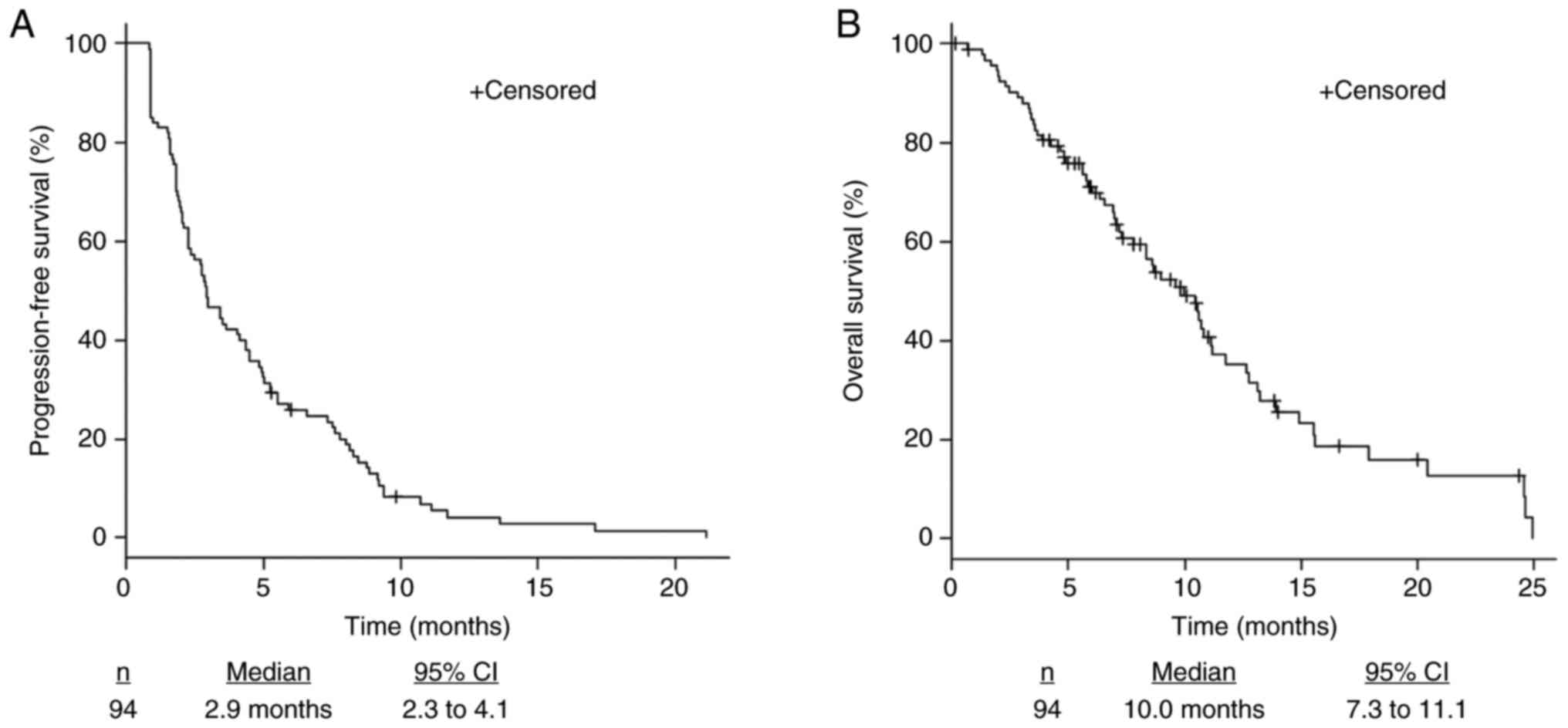
The median PFS was 2.9 months (2.3–4.1), and the
median OS was 10.0 months (7.3–11.1) (Fig. 1). The ORR and DCR were 0% and 44.7%,
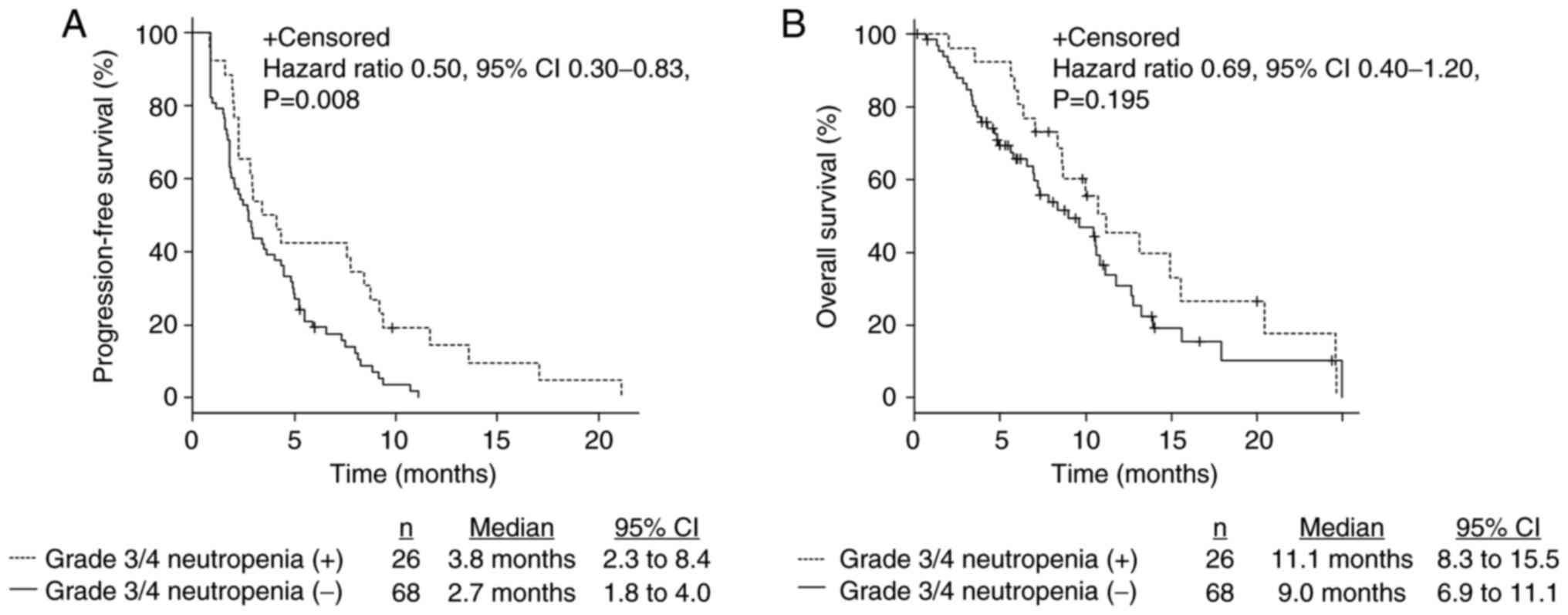
respectively (Table III). Patients
with grade 3 or 4 CIN within the first cycle of treatment had
significantly longer PFS (3.8 months [2.3–8.4] vs. 2.7 months
[1.8–4.0], P=0.008) (Fig. 2A) and
tended to have longer OS (11.1 months [8.3–15.5] vs. 9.0 months
[6.9–11.1], P=0.19 (Fig. 2B).
Furthermore, there were no complete nor partial response. The DCR
in patients with grade 3 or 4 CIN within the first cycle of
treatment was higher than in patients without grade 3 or 4 CIN
(61.5 and 38.2%, P=0.07; Table
III).
| Table III.Summary of antitumor response. |
Table III.
Summary of antitumor response.
| Variable | Total number of
patients (n=94) | Patients with grade
3 or 4 neutropenia within the first cycle of treatment (n=26) | Patients without
grade 3 or 4 neutropenia within the first cycle of treatment
(n=68) | P-value |
|---|
| Best overall
response, n (%) |
|
|
|
|
|
Complete response | 0 (0.0) | 0 (0.0) | 0 (0.0) | – |
| Partial
response | 0 (0.0) | 0 (0.0) | 0 (0.0) | – |
| Stable
disease | 42 (44.7) | 16 (61.5) | 26 (38.2) | – |
|
Progressive disease | 45 (47.9) | 10 (38.5) | 35 (51.5) | – |
| Not
evaluated | 7 (7.4) | 0 (0.0) | 7 (10.3) | – |
| Disease control
rate, % | 42 (44.7) | 16 (61.5) | 26 (38.2) | 0.07 |
Univariate and multivariate analyses
of predictors of clinical outcomes
In the univariate Cox proportional hazard analysis,
liver metastasis, lymph node metastasis, and grade 3 or 4 CIN
within the first cycle of treatment were predictive factors for
PFS. PS and liver metastasis were predictive factors for OS
(Tables IV and V). Moreover, liver and lymph node
metastases were independent predictive factors for a shorter PFS,
while CIN was an independent predictive factor for a longer PFS
(liver metastasis: HR 1.82, 95% CI 1.17–2.83, P=0.007; lymph node
metastasis: HR 2.23, 95% CI 1.40–3.54, P=0.0007; grade 3 or 4 CIN
within the first cycle of treatment: HR 0.51, 95% CI 0.3–0.86,
P=0.01) in the multivariate analysis. Furthermore, liver metastasis
and performance status were independent predictive factors for a
shorter OS (liver metastasis: HR 2.31, 95% CI 1.34–3.98, P=0.002;
PS: HR 2.26, 95% CI 1.29–3.97, P=0.004) in the multivariate
analysis (Tables IV and V).
| Table IV.Univariate Cox regression analyses
for PFS and OS in patients with metastatic colorectal cancer. |
Table IV.
Univariate Cox regression analyses
for PFS and OS in patients with metastatic colorectal cancer.
| A, PFS |
|---|
|
|---|
| Variable | HR | Lower 95% CI | Upper 95% CI | P-value |
|---|
| Sex (female vs.
male) | 1.16 | 0.75 | 1.79 | 0.4950 |
| ECOG PS (0 vs. 1 or
2) | 1.42 | 0.89 | 2.26 | 0.1340 |
| Age, years (<65
vs. ≥65) | 0.91 | 0.59 | 1.39 | 0.6532 |
| Primary tumor
location (left vs. right) | 0.83 | 0.52 | 1.34 | 0.4615 |
| Liver metastasis
(negative vs. positive) | 1.53 | 0.99 | 2.36 | 0.0515 |
| Lung metastasis
(negative vs. positive) | 0.91 | 0.56 | 1.47 | 0.6975 |
| Peritoneal
metastasis (negative vs. positive) | 1.05 | 0.68 | 1.59 | 0.8289 |
| Lymph node
metastasis (negative vs. positive) | 2.22 | 1.40 | 3.51 | 0.0006c |
| Tissue RAS
mutation (negative vs. positive) | 0.68 | 0.44 | 1.05 | 0.0826 |
| Time from the start
of first-line chemotherapy, months (<18 vs. ≥18) | 0.65 | 0.42 | 1.02 | 0.0586 |
| Grade 3 or 4
neutropenia within the first cycle of treatment (negative vs.
positive) | 0.50 | 0.30 | 0.84 | 0.0080b |
| Treatment regimen
(bevacizumab vs. other) | 0.78 | 0.51 | 1.20 | 0.2623 |
|
| B, OS |
|
|
Variable | HR | Lower 95%
CI | Upper 95%
CI | P-value |
|
| Sex (female vs.
male) | 1.04 | 0.62 | 1.75 | 0.8573 |
| ECOG PS (0 vs. 1 or
2) | 1.83 | 1.07 | 3.12 | 0.0273a |
| Age, years (<65
vs. ≥65) | 0.81 | 0.47 | 1.37 | 0.4292 |
| Primary tumor
location (left vs. right) | 1.01 | 0.58 | 1.77 | 0.9616 |
| Liver metastasis
(negative vs. positive) | 1.95 | 1.15 | 3.30 | 0.0126a |
| Lung metastasis
(negative vs. positive) | 0.81 | 0.46 | 1.42 | 0.4567 |
| Peritoneal
metastasis (negative vs. positive) | 1.11 | 0.66 | 1.85 | 0.6868 |
| Lymph node
metastasis (negative vs. positive) | 1.16 | 0.70 | 1.91 | 0.5673 |
| Tissue RAS
mutation (negative vs. positive) | 1.13 | 0.67 | 1.89 | 0.6407 |
| Time from the start
of first-line chemotherapy, months (<18 vs. ≥18) | 0.91 | 0.54 | 1.52 | 0.7077 |
| Grade 3 or 4
neutropenia within the first cycle of treatment (negative vs.
positive) | 0.70 | 0.40 | 1.20 | 0.1950 |
| Treatment regimen
(bevacizumab vs. other) | 1.37 | 0.81 | 2.33 | 0.2423 |
| Table V.Multivariate Cox regression analyses
for PFS and OS in patients with metastatic colorectal cancer. |
Table V.
Multivariate Cox regression analyses
for PFS and OS in patients with metastatic colorectal cancer.
| A, PFS |
|---|
|
|---|
| Variable | HR | Lower 95% CI | Upper 95% CI | P-value |
|---|
| Liver metastasis
(negative vs. positive) | 1.82 | 1.17 | 2.83 | 0.0079b |
| Lymph node
metastasis (negative vs. positive) | 2.23 | 1.40 | 3.54 | 0.0007c |
| Grade 3 or 4
neutropenia within the first cycle of treatment (negative vs.
positive) | 0.51 | 0.30 | 0.86 | 0.0118a |
|
| B, OS |
|
|
Variable | HR | Lower 95%
CI | Upper 95%
CI | P-value |
|
| ECOG PS (0 vs. 1 or
2) | 2.26 | 1.29 | 3.97 | 0.0043b |
| Liver metastasis
(negative vs. positive) | 2.31 | 1.34 | 3.98 | 0.0027b |
Previous reports of clinical
outcomes
A summary of previous prospective and retrospective
reports of FTD/TPI + Bev for patients with mCRC receiving
salvage-line therapy is presented in Table VI (11,14,16–20). In
these reports, the median PFS time was 3.7–6.8 months and the
median OS time was 8.6–14.4 months. In addition, grade 3 or 4
neutropenia occurred in 38.9–72.0% of all cases. The clinical
outcomes of the present study were comparable to previous reports
(11,14,16–20). A
summary of previous prospective and retrospective reports of
FTD/TPI monotherapy for patients with mCRC is presented in Table SIII (5,6,21–28). In
these reports, the median PFS time was 2.0–2.5 months and the
median OS time was 5.3–9.0 months. Furthermore, grade 3 or 4
neutropenia occurred in 14.3–50.0% of all cases.
| Table VI.Previous reports of clinical outcomes
in patients with metastatic colorectal cancer treated with
trifluridine/tipiracil plus bevacizumab as a late-line
treatment. |
Table VI.
Previous reports of clinical outcomes
in patients with metastatic colorectal cancer treated with
trifluridine/tipiracil plus bevacizumab as a late-line
treatment.
| Author, year
(ref.) | Number of
patients | RR, % | DCR, % | PFS, months | OS, months | Grade 3 or 4
neutropenia in all treatment periods, % |
|---|
| Kuboki et
al, 2017 (11) | 21 | 0.0 | 64.0 | 3.7 | 11.4 | 72.0 |
| Kotani et
al, 2019 (17) | 60 | 5.0 | 53.3 | 3.7 | 8.6 | 50.0 |
| Matsuhashi et
al, 2019 (18) | 17 | 0.0 | 70.1 | 6.8 | 14.1 | 41.2 |
| Pfeiffer et
al, 2020 (14) | 46 | 2.2 | 67.4 | 4.6 | 9.4 | 67.4 |
| Fujii et al,
2020 (19) | 21 | 0.0 | 76.1 | 5.6 (TTF) | 14.4 | 52.4 |
| Shibutani et
al, 2020 (20) | 36 | 8.3 | 58.3 | – | – | 38.9 |
| Nose et al,
2020 (16) | 32 | – | – | 4.7 | 11.7 | 53.1 |
| Data in present
study | 94 | 0.0 | 44.7 | 2.9 | 10.0 | 51.1 |
Discussion
In the present study, we explored the clinical
outcomes of FTD/TPI + Bev and the predictive factors of its
efficacy. To our knowledge, this is the first study to demonstrate
that CIN within the first cycle of treatment is an indicator for
the efficacy of FTD/TPI + Bev in multivariate analysis of a large
number of cases. FTD/TPI + Bev showed enhanced activity against
colorectal cancer xenografts compared with FTD/TPI alone (29). Moreover, clinical data from the phase
I/II C-TASK FORCE study and the phase II study conducted by
Pfeiffer et al (11,14) showed that treatment with FTD/TPI +
Bev induced promising antitumor activity with manageable toxicity
in advanced mCRC refractory or intolerant to standard therapies. A
summary of previous prospective and retrospective reports of
FTD/TPI + Bev for patients with mCRC receiving salvage-line therapy
is shown in Table VI (11,14,16–20). The
clinical outcomes such as PFS, OS, and DCR in patients treated with
the FTD/TPI + Bev are better than those in patients treated with
the FTD/TPI monotherapy (Tables VI
and SIII) (5,6,11,14,16–28).
Furthermore, the clinical outcomes of FTD/TPI + Bev of this study
were comparable to previous reports. Thus, FTD/TPI + Bev may be a
more effective regimen than FTD/TPI monotherapy. On the other hand,
the incidence of grade 3 or 4 CIN of FTD/TPI + Bev is higher than
FTD/TPI monotherapy (Tables VI and
SIII) (5,6,11,14,16–28). CIN
was an independent predictive factor for the efficacy of FTD/TPI
monotherapy, as reported previously (11,30–32). As
mentioned before, pharmacokinetics and pharmacodynamics analysis in
the RECOURSE trial suggests a dose-response relationship between
FTD exposure and CIN, in agreement with the findings of the
dose-escalation studies that a higher rate of CIN at higher doses
of FTD/TPI leads to greater efficacy of the drug (10). Furthermore, results of a randomized
phase II trial comparing FTD/TPI + Bev with FTD/TPI monotherapy
showed that grade 3 or higher neutropenia in the FTD/TPI + Bev
group was 67 vs. 38% in the FTD/TPI monotherapy group and PFS in
the FTD/TPI + Bev group is significantly longer than that in the
FTD/TPI monotherapy group (14).
This is because anti-angiogenic drugs can normalize tumor
vasculature, alleviate hypoxia, increase drug delivery, and elevate
antitumor immune cells; because tumors are accompanied by abnormal
vascular structure, tumor interstitial fluid pressure increases
owing to vascular leakage, accompanied by hypoxia (33). In addition, a meta-analysis showed
that Bev was associated with an increased risk of high-grade
neutropenia, as inhibition of the VEGF receptor blocks
hematopoietic stem cell cycle, differentiation, and recovery after
bone marrow suppression (34).
According to the above hypothesis, the clinical outcome of FTD/TPI
+ Bev was better than that of FTD/TPI monotherapy. Furthermore, it
was similar to the results of several second-line clinical trials
(35,36) that investigated a combination therapy
consisting of a chemotherapy and anti-VEGF antibody for patients
with mCRC. We did not discuss the results of first-line clinical
trials in this manuscript. Nevertheless, this study was limited by
the relatively small number of patients and its retrospective
nature. Despite these limitations, the results of this study
provide important and novel insights into the clinical use of
FTD/TPI + Bev in salvage-line chemotherapy. For mCRC patients
without neutropenia after the initiation of FTD/TPI + Bev, we
should consider early image evaluation and treatment changes (e.g.,
regorafenib) or BSC. In conclusion, the clinical outcomes of
FTD/TPI + Bev were comparable to previous reports that showed it to
be more effective than FTD/TPI monotherapy. Grade 3 or 4 CIN within
the first cycle of treatment is an early predictive marker of the
chemotherapeutic efficacy of FTD/TPI + Bev. This could be a useful
biomarker for optimizing treatment decisions in daily clinical
practice.
Supplementary Material
Supporting Data
Acknowledgements
The authors of the present study would like to thank
Ms Yukie Naito and Ms Yuki Horiike (Cancer Institute Hospital,
Japanese Foundation for Cancer Research) for providing data
management.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
DK, HO and ES conceptualized and designed the
present study. DK, HO, ES, AO, TW, KYo, TS, IN, MO, DT, KC and KYa
acquired and analyzed the data. DK, HO, ES and AO interpreted the
data. DK and HO drafted the initial manuscript and performed
statistical analysis. ES, AO, TW, KYo, TS, IN, MO, DT, KC and KYa
critically revised the manuscript for important intellectual
content. ES and KYa supervised the study. DK, HO and ES confirmed
the authenticity of all the raw data. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board of the Japanese Foundation for Cancer Research (Tokyo,
Japan; approval no. 2020-1017). The protocol is described on the
hospital website, and subjects were provided the opportunity to
opt-out; therefore, no additional consent was required from
patients. All experiments were performed in accordance with the
Declaration of Helsinki.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
BSC
|
best supportive care
|
|
CIN
|
chemotherapy-induced neutropenia
|
|
CR
|
complete response
|
|
DCR
|
disease control rate
|
|
ORR
|
objective response rate
|
|
OS
|
overall survival
|
|
PFS
|
progression-free survival
|
|
PR
|
partial response
|
|
SD
|
stable disease
|
References
|
1
|
Tanaka N, Sakamoto K, Okabe H, Fujioka A,
Yamamura K, Nakagawa F, Nagase H, Yokogawa T, Oguchi K, Ishida K,
et al: Repeated oral dosing of TAS-102 confers high trifluridine
incorporation into DNA and sustained antitumor activity in mouse
models. Oncol Rep. 32:2319–3226. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Heidelberger C, Parsons DG and Remy DC:
Syntheses of 5-trifluoromethyluracil and
5-trifluoromethyl-2′-deoxyuridine. J Med Chem. 7:1–5. 1964.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fujiwara Y, Oki T and Heidelberger C:
Fluorinated pyrimidines. XXXVII. Effects of
5-trifluoromethyl-2′-deoxyuridine on the synthesis of
deoxyribonucleic acid of mammalian cells in culture. Mol Pharmacol.
6:273–280. 1970.PubMed/NCBI
|
|
4
|
Emura T, Suzuki N, Fujioka A, Ohshimo H
and Fukushima M: A novel combination antimetabolite, TAS-102,
exhibits antitumor activity in FU-resistant human cancer cells
through a mechanism involving FTD incorporation in DNA. Int J
Oncol. 25:571–578. 2004.PubMed/NCBI
|
|
5
|
Mayer RJ, Van Cutsem E, Falcone A, Yoshino
T, Garcia-Carbonero R, Mizunuma N, Yamazaki K, Shimada Y, Tabernero
J, Komatsu Y, et al: Randomized trial of TAS-102 for refractory
metastatic colorectal cancer. N Engl J Med. 372:1909–1919. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Xu J, Kim TW, Shen L, Sriuranpong V, Pan
H, Xu R, Guo W, Han SW, Liu T, Park YS, et al: Results of a
randomized, double-blind, placebo-controlled, phase iii trial of
trifluridine/tipiracil (TAS-102) monotherapy in Asian patients with
previously treated metastatic colorectal cancer: The TERRA study. J
Clin Oncol. 36:350–358. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hashiguchi Y, Muro K, Saito Y, Ito Y,
Ajioka Y, Hamaguchi T, Hasegawa K, Hotta K, Ishida H, Ishiguro M,
et al: Japanese Society for Cancer of the Colon and Rectum (JSCCR)
guidelines 2019 for the treatment of colorectal cancer. Int J Clin
Oncol. 25:1–42. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Benson AB, Venook AP, Al-Hawary MM, Arain
MA, Chen YJ, Ciombor KK, Cohen S, Cooper HS, Deming D, Farkas L, et
al: Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines
in Oncology. J Natl Compr Canc Netw. 19:329–359. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Van Cutsem E, Cervantes A, Adam R, Sobrero
A, Van Krieken JH, Aderka D, Aranda Aguilar E, Bardelli A, Benson
A, Bodoky G, et al: ESMO consensus guidelines for the management of
patients with metastatic colorectal cancer. Ann Oncol.
27:1386–1422. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yoshino T, Cleary JM, Van Cutsem E, Mayer
RJ, Ohtsu A, Shinozaki E, Falcone A, Yamazaki K, Nishina T,
Garcia-Carbonero R, et al: Neutropenia and survival outcomes in
metastatic colorectal cancer patients treated with
trifluridine/tipiracil in the RECOURSE and J003 trials. Ann Oncol.
31:88–95. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kuboki Y, Nishina T, Shinozaki E, Yamazaki
K, Shitara K, Okamoto W, Kajiwara T, Matsumoto T, Tsushima T,
Mochizuki N, et al: TAS-102 plus bevacizumab for patients with
metastatic colorectal cancer refractory to standard therapies
(C-TASK FORCE): An investigator-initiated, open-label, single-arm,
multicentre, phase 1/2 study. Lancet Oncol. 18:1172–1181. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Satake H, Kato T, Oba K, Kotaka M, Kagawa
Y, Yasui H, Nakamura M, Watanabe T, Matsumoto T, Kii T, et al:
Phase Ib/II Study of biweekly TAS-102 in combination with
bevacizumab for patients with metastatic colorectal cancer
refractory to standard therapies (BiTS Study). Oncologist.
25:e1855–e1863. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Van Cutsem E, Danielewicz I, Saunders MP,
Pfeiffer P, Argilés G, Borg C, Glynne-Jones R, Punt CJA, Van de
Wouw AJ, Fedyanin M, et al: Trifluridine/tipiracil plus bevacizumab
in patients with untreated metastatic colorectal cancer ineligible
for intensive therapy: The randomized TASCO1 study. Ann Oncol.
31:1160–1168. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pfeiffer P, Yilmaz M, Möller S, Zitnjak D,
Krogh M, Petersen LN, Poulsen LØ, Winther SB, Thomsen KG and
Qvortrup C: TAS-102 with or without bevacizumab in patients with
chemorefractory metastatic colorectal cancer: An
investigator-initiated, open-label, randomised, phase 2 trial.
Lancet Oncol. 21:412–420. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kanda Y: Investigation of the freely
available easy-to-use software ‘EZR’ for medical statistics. Bone
Marrow Transplant. 48:452–458. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Nose Y, Kagawa Y, Hata T, Mori R, Kawai K,
Naito A, Sakamoto T, Murakami K, Katsura Y, Ohmura Y, et al:
Neutropenia is an indicator of outcomes in metastatic colorectal
cancer patients treated with FTD/TPI plus bevacizumab: A
retrospective study. Cancer Chemother Pharmacol. 86:427–433. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kotani D, Kuboki Y, Horasawa S, Kaneko A,
Nakamura Y, Kawazoe A, Bando H, Taniguchi H, Shitara K, Kojima T,
et al: Retrospective cohort study of trifluridine/tipiracil
(TAS-102) plus bevacizumab versus trifluridine/tipiracil
monotherapy for metastatic colorectal cancer. BMC Cancer.
19:12532019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Matsuhashi N, Takahashi T, Fujii H,
Suetsugu T, Fukada M, Iwata Y, Tokumaru Y, Imai T, Mori R,
Tanahashi T, et al: Combination chemotherapy with TAS-102 plus
bevacizumab in salvage-line treatment of metastatic colorectal
cancer: A single-center, retrospective study examining the
prognostic value of the modified Glasgow Prognostic Score in
salvage-line therapy of metastatic colorectal cancer. Mol Clin
Oncol. 11:390–396. 2019.PubMed/NCBI
|
|
19
|
Fujii H, Matsuhashi N, Kitahora M,
Takahashi T, Hirose C, Iihara H, Yamada Y, Watanabe D, Ishihara T,
Suzuki A and Yoshida K: Bevacizumab in combination with TAS-102
improves clinical outcomes in patients with refractory metastatic
colorectal cancer: A retrospective study. Oncologist. 25:e469–e476.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Shibutani M, Nagahara H, Fukuoka T, Iseki
Y, Wang EN, Okazaki Y, Kashiwagi S, Maeda K, Hirakawa K and Ohira
M: Combining bevacizumab with trifluridine/thymidine phosphorylase
inhibitor improves the survival outcomes regardless of the usage
history of bevacizumab in front-line treatment of patients with
metastatic colorectal cancer. Anticancer Res. 40:4157–4163. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yoshino T, Mizunuma N, Yamazaki K, Nishina
T, Komatsu Y, Baba H, Tsuji A, Yamaguchi K, Muro K, Sugimoto N, et
al: TAS-102 monotherapy for pretreated metastatic colorectal
cancer: A double-blind, randomised, placebo-controlled phase 2
trial. Lancet Oncol. 13:993–1001. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Arita S, Shirakawa T, Matsushita Y,
Shimokawa HK, Hirano G, Makiyama A, Shibata Y, Tamura S, Esaki T,
Mitsugi K, et al: Efficacy and safety of TAS-102 in clinical
practice of salvage chemotherapy for metastatic colorectal cancer.
Anticancer Res. 36:1959–1966. 2016.PubMed/NCBI
|
|
23
|
Masuishi T, Taniguchi H, Hamauchi S,
Komori A, Kito Y, Narita Y, Tsushima T, Ishihara M, Todaka A,
Tanaka T, et al: Regorafenib versus trifluridine/tipiracil for
refractory metastatic colorectal cancer: A retrospective
comparison. Clin Colorectal Cancer. 16:e15–e22. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kotani D, Shitara K, Kawazoe A, Fukuoka S,
Kuboki Y, Bando H, Okamoto W, Kojima T, Doi T, Ohtsu A, et al:
Safety and efficacy of trifluridine/tipiracil monotherapy in
clinical practice for patients with metastatic colorectal cancer:
Experience at a single institution. Clin Colorectal Cancer.
15:e109–e115. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sueda T, Sakai D, Kudo T, Sugiura T,
Takahashi H, Haraguchi N, Nishimura J, Hata T, Hayashi T, Mizushima
T, et al: Efficacy and safety of regorafenib or TAS-102 in patients
with metastatic colorectal cancer refractory to standard therapies.
Anticancer Res. 36:4299–4306. 2016.PubMed/NCBI
|
|
26
|
Kwakman JJM, Vink G, Vestjens JH,
Beerepoot LV, de Groot JW, Jansen RL, Opdam FL, Boot H, Creemers
GJ, van Rooijen JM, et al: Feasibility and effectiveness of
trifluridine/tipiracil in metastatic colorectal cancer: Real-life
data from the netherlands. Int J Clin Oncol. 23:482–489. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cremolini C, Rossini D, Martinelli E,
Pietrantonio F, Lonardi S, Noventa S, Tamburini E, Frassineti GL,
Mosconi S, Nichetti F, et al: Trifluridine/tipiracil (TAS-102) in
refractory metastatic colorectal cancer: A multicenter register in
the frame of the Italian compassionate use program. Oncologist.
23:1178–1187. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Moriwaki T, Fukuoka S, Taniguchi H,
Takashima A, Kumekawa Y, Kajiwara T, Yamazaki K, Esaki T, Makiyama
C, Denda T, et al: Propensity score analysis of regorafenib versus
trifluridine/tipiracil in patients with metastatic colorectal
cancer refractory to standard chemotherapy (REGOTAS): A Japanese
Society for Cancer of the Colon and Rectum multicenter
observational study. Oncologist. 23:7–15. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Tsukihara H, Nakagawa F, Sakamoto K,
Ishida K, Tanaka N, Okabe H, Uchida J, Matsuo K and Takechi T:
Efficacy of combination chemotherapy using a novel oral
chemotherapeutic agent, TAS-102, together with bevacizumab,
cetuximab, or panitumumab on human colorectal cancer xenografts.
Oncol Rep. 33:2135–2142. 2015.PubMed/NCBI
|
|
30
|
Kasi PM, Kotani D, Cecchini M, Shitara K,
Ohtsu A, Ramanathan RK, Hochster HS, Grothey A and Yoshino T:
Chemotherapy induced neutropenia at 1-month mark is a predictor of
overall survival in patients receiving TAS-102 for refractory
metastatic colorectal cancer: A cohort study. BMC Cancer.
16:4672016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hamauchi S, Yamazaki K, Masuishi T, Kito
Y, Komori A, Tsushima T, Narita Y, Todaka A, Ishihara M, Yokota T,
et al: Neutropenia as a predictive factor in metastatic colorectal
cancer treated with TAS-102. Clin Colorectal Cancer. 16:51–57.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Makihara K, Fukui R, Uchiyama H, Shigeoka
Y and Toyokawa A: Decreased percentage of neutrophil is a predict
factor for the efficacy of trifluridine and tipiracil hydrochloride
for pretreated metastatic colorectal cancer. J Gastrointest Oncol.
10:878–885. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
De Bock K, Mazzone M and Carmeliet P:
Anti-angiogenic therapy, hypoxia, and metastasis: Risky liaisons,
or not? Nat Rev Clin Oncol. 8:393–404. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Schutz FA, Jardim DL, Je Y and Choueiri
TK: Haematologic toxicities associated with the addition of
bevacizumab in cancer patients. Eur J Cancer. 47:1161–1174. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hurwitz H, Fehrenbacher L, Novotny W,
Cartwright T, Hainsworth J, Heim W, Berlin J, Baron A, Griffing S,
Holmgren E, et al: Bevacizumab plus irinotecan, fluorouracil, and
leucovorin for metastatic colorectal cancer. N Engl J Med.
350:2335–2342. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Bennouna J, Sastre J, Arnold D, Österlund
P, Greil R, Van Cutsem E, von Moos R, Viéitez JM, Bouché O, Borg C,
et al: Continuation of bevacizumab after first progression in
metastatic colorectal cancer (ML18147): A randomised phase 3 trial.
Lancet Oncol. 14:29–37. 2013. View Article : Google Scholar : PubMed/NCBI
|