Introduction
Malignant wounds (MWs) are lesions caused by
malignant tumors infiltrating or damaging the skin (1–3). MWs
are often accompanied by ulcerations, necrosis, hemorrhage, and
inflammation (1,2). It is estimated that 5–7% of cancer
patients experience MWs, especially patients with breast cancer,
soft tissue sarcoma (STS), head and neck cancer, and melanoma
(1,2). Previous studies mainly enrolled
patients with limited life expectancy due to unresectable advanced
or metastatic breast and skin cancers (4,5).
Some studies reported an incidence of 3–4% for MW in patients with
STS (6–9).
MWs are often infected because necrotic tissue
provides a suitable environment for bacterial growth. Patients
frequently report symptoms as malodorous wounds, exudation, pain,
and bleeding. These symptoms lead to impaired mobility, emotional
distress, and a poor quality of life (3–5).
Fromantin et al proposed that MWs in patients with breast
cancer had polymicrobial colonization predominated by
Staphylococcus aureus and Pseudomonas aeruginosa
(4). Biofilms were present in the
wounds of 35% of the patients, and the concentration of bacteria
correlated with the emergence of odor and pain. Few studies have
focused on the bacteriological investigation of MWs in patients
with STS (10–12). Lutchminarian et al reported
that the most common pathogen in MW from STS was Staphylococcus
aureus (33%), followed by β-hemolytic Streptococcus
(17%), and Pseudomonas aeruginosa (17%) (13). These infections sometimes lead to
severe clinical problems, such as sepsis and surgical site
infection (SSI) (10,12). Elfallal et al reported a
case of life-threatening sepsis from severe necrotic wound in a
patient with giant angiolipoma of the back (14). Immediate tumor excision with
hemostasis was required. This supports the need for early diagnosis
and treatment of concurrent sepsis. The effectiveness of
sensitivity-guided perioperative antibacterial prophylaxis remains
unclear. Data on perioperative improvement of clinical symptoms and
laboratory data are lacking.
MWs have some oncologic features in STS; thus, it is
important to manage both oncologic and infectious problems. In
previous reports, patients with MWs from STS were older (mean age:
65–73 years), and presented with higher grade, higher stage, and
higher proportion of metastases (20–33%) compared to those without
MWs (15–18). When the lesions are large, possibly
requiring skin reconstruction, limb salvage was sometimes
difficult, leading to a high rate of amputation (13–33%) (15–18).
Although resection of the tumor can control the symptoms associated
with MWs, previous studies reported high rates of surgical site
infection (SSI) as much as 26–42% (15,18).
Hoshi et al reported 42% incidence of postoperative (SSI),
and Candida species was the most common isolate, followed by
Pseudomonas aeruginosa and Enterococcus species
(18).
Therefore, this study aimed to perform
microbiological analyses in a series of STS patients with MWs. We
specifically investigated the bacterial profile in MWs and the
effectiveness of sensitivity-guided perioperative antibacterial
prophylaxis. Lastly, we investigated the incidence of sepsis and
the changes in laboratory values after treatment.
Materials and methods
Study design and setting
We retrospectively evaluated the medical records of
patients who presented with MWs at Okayama University Hospital
(Okayama, Japan) between April 2006 and April 2020.
Study population
Patients who had pathologically confirmed MW and
underwent surgical resection for STS in the extremity were included
in the study. The exclusion criteria were as follows: (a) only
conservative management done; (b) follow-up less than two years
post-surgery; (c) development of MW during the clinical course.
Finally, seven patients (four males, three females) were included
in this study (Table I). Their
median age at the start of treatment was 59 years (range, 30–78).
Histological diagnosis was established according to the WHO
Classification (19). Myxoid
liposarcoma was diagnosed in two patients, and myxofibrosarcoma,
undifferentiated pleomorphic sarcoma (UPS), fibrosarcoma,
angiosarcoma, leiomyosarcoma, and malignant peripheral nerve sheath
tumor (MPNST) was diagnosed in one patient each. The median tumor
size was 10 cm (range: 6–31) and was superficial in 5 patients and
deep in 2 patients. The grade was determined using the French
Fédération Nationale des Centres de Lutte Contre Le Cancer (FNCLCC)
grading system; grade 2 cancer was observed in three patients and
grade 3 in four patients (20).
The American Joint Committee on Cancer (AJCC) stages were IIIA in
four patients and IV in three patients. The locations of the tumor
were as follows: the thigh (4),
each upper arm (1), lower leg
(1), and abdomen (1). No patient had a treatment history of
hypertension, diabetes mellitus (DM), renal disorder, liver
disorder, or respiratory disorder. The median follow-up period was
53 months (range: 4–152 months).
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Case | Sex | Age, years | Histology | Size, cm | Location | FNCLCC | AJCC | Margin | Reconstruction | Metastases | Outcome |
|---|
| 1 | Female | 75 | Myxoid
liposarcoma | 17 | Thigh | 2 | IV | R0 | Skin graft | Lymph node | NED |
| 2 | Female | 42 | Myxoid
liposarcoma | 31 | Thigh | 2 | IV | R0 (hip
disarticulation) |
| Lung | DOD |
| 3 | Male | 76 | Undifferentiated
sarcoma | 8 | Thigh | 3 | IIIA | Initial surgery; R0
Recurrence; R0 (hip disarticulation) | Latissimus dorsi
flap + skin graft | Lung Soft tissue
(follow up period) | DOD |
| 4 | Female | 59 | Fibrosarcoma | 9 | Thigh | 3 | IIIA | R0 | Gastrocnemius
muscle flap + skin graft |
| DOA |
| 5 | Male | 55 | Angiosarcoma | 10 | Lower leg | 3 | IV | R0
(Amputation) |
| Lymph node Bone
Lung (follow-up period) | DOD |
| 6 | Male | 78 |
Myxofibrosarcoma | 10 | Upper arm | 2 | IIIA | R0 | Latissimus dorsi
flap | Lymph node
(follow-up period) | NED |
| 7 | Male | 30 | Malignant
peripheral nerve sheath tumor | 6 | Abdomen | 3 | IIIA | R0 |
|
| CDF |
Microbiological sampling and
testing
Preoperative microbiological samples were obtained
from the necrotic zone of the wound. Detection of aerobic,
facultative anaerobic, and strict anaerobic bacteria was carried
out using a quantitative method. We investigated the incidence of
SSI based on the definition provided by the Centers for Disease
Control (CDC) (Table SI)
(21).
Clinical investigation
We investigated the symptoms of the wound (e.g.,
bleeding, odor/exudate, and pain) and clinical condition (fever) on
presentation and after surgery. Fever was defined as a temperature
higher than or equal to 37.5°C. Pain was quantified using a
10-point numeric rating scale (NRS). The symptoms were documented
at baseline, one, and two weeks postoperatively. Bleeding was
reported in five patients, foul odor in three patients, and exudate
in five (Table II). These
symptoms disappeared after surgery. All but one patient had pain at
the MW site during the initial presentation, with an average NRS of
4.4 (range: 0–10). It decreased after surgery; the average NRS were
1.4 (range: 0–10, P=0.14) and 0.6 (range: 0–3, P=0.04) after one
and two weeks of surgery, respectively. During the last follow-up,
all but one patient had pain at the surgical site. Two patients
presented with fever, which defervesced one week after surgery.
| Table II.Characteristics of the malignant
wound. |
Table II.
Characteristics of the malignant
wound.
| Case | Bleeding | Odor | Exudate | Awareness of the
tumor | Duration of the
malignant wound |
|---|
| 1 | - | + | + | 24 months | 12 months |
| 2 | + | + | + | 36 months | 3 days |
| 3 | + | - | + | 4 months | 3 days |
| 4 | + | - | + | 36 months | 4 months |
| 5 | + | - | - | 7 months | 4 months |
| 6 | - | + | + | 13 months | 11 days |
| 7 | + | - | - | 4 months | 1 day |
We investigated the presence of sepsis at the
initial presentation. The diagnosis for sepsis was defined based on
the Japanese Clinical Practice Guidelines for Management of Sepsis
and Septic Shock 2020 (J-SSCG 2020) (22). By this definition, suspected
infection can be rapidly identified in the presence of two or more
quick Sequential Organ Failure Assessment (qSOFA) score: A
respiratory rate (≥22/min), altered mentation (Glasgow Coma Score
≤14), and a systolic blood pressure (≤100 mmHg) (23–25).
Next, the diagnosis of sepsis was confirmed when the SOFA score was
≥2 points higher in the presence of a clear infection or suspected
infection (Table III). Septic
shock was defined as persistent hypotension requiring vasopressors
to maintain a mean arterial pressure of ≥65 mmHg and a serum
lactate level >2 mmol/l (18 mg/dl) despite adequate volume
resuscitation (22). One patient
met the diagnostic criteria for sepsis (case 2).
| Table III.Sequential Organ Failure Assessment
score. |
Table III.
Sequential Organ Failure Assessment
score.
|
| Assessment
score |
|---|
|
|
|
|---|
| Variables | 0 | 1 | 2 | 3 | 4 |
|---|
| Respiration |
|
|
|
|
|
|
PaO2/FIO2
(mm Hg) | ≥400 | <400 | <300 | <200 | <100 |
| Coagulation |
|
|
|
|
|
|
Platelets
(×103/l) | ≥150 | <150 | <100 | <50 | <20 |
| Liver |
|
|
|
|
|
|
Bilirubin (mg/dl) | <1.2 | 1.2-1.9 | 2.0-5.9 | 6.0-11.9 | ≥12.0 |
| Cardiovascular |
|
|
|
|
|
| Mean
arterial pressure (mmHg) | ≥70 | <70 | Dopamine ≤5 or
dobutamine (any) | Dopamine >5 or
norepinephrine ≤0.1 | Dopamine >15 or
norepinephrine >0.1 |
| Nervous system |
|
|
|
|
|
| Glasgow
Coma Score | 15 | 13-14 | 10-12 | 6-9 | <6 |
| Renal |
|
|
|
|
|
|
Creatinine (mg/dl) | <1.2 | 1.2-1.9 | 2.0-3.4 | 3.5-4.9 | >5.0 |
| Urine
output (ml/d) |
|
|
| <500 | <200 |
Laboratory investigation
The following laboratory parameters were documented
at baseline and 2–6 weeks after surgery: white blood cell (WBC)
count, serum C-reactive protein (CRP), hemoglobin (Hgb), blood urea
nitrogen (BUN), creatinine (Cr), albumin (Alb), alanine
aminotransferase (ALT), aspartate aminotransferase (AST), and total
bilirubin (T-bil). Anemia was defined as hemoglobin (Hgb) <12.0
g/dl in non-pregnant women and <13.0 g/dl in men based on the
World Health Organization (WHO) criteria (26).
Treatment
Five patients initially underwent limb-sparing
surgery, amputation was performed for one patient, and
disarticulation was performed for one patient. Surgical excision
margins were estimated based on the AJCC residual tumor
classification (R classification) (27). These surgical margins were
classified as follows: R0 margin, free of malignancy; R1 margin,
microscopic tumor cells present at the inked border of the
specimen; and R2 margin, grossly positive margins. Surgical margins
were estimated as R0 in all patients. Soft tissue coverage was
required in four patients: two free flaps (latissimus dorsi flap),
one medial gastrocnemius muscle flap and skin graft, and one skin
graft. Since all patients achieved R0 resection, radiation therapy
was not performed for any of the patients. No patients received
pre- or postoperative chemotherapy.
Statistical analysis
The Mann-Whitney U test was used to analyze
continuous parameters, while Fisher's exact test was used for
categorical parameters. We used the BellCurve for Excel (Social
Survey Research Information Co., Ltd.) for all the analyses. The
overall survival (OS) was calculated from the date of diagnosis to
the date of death or the last follow-up visit. Survival rates were
estimated using the Kaplan-Meier method. A P-value of <0.05 was
considered statistically significant.
Results
Microbiological analyses
Microbiological sampling from the wound was
performed prior to surgery for five patients and 11 different
bacterial strains were identified in them (Table IV). The average number of
bacterial strains isolated per wound was 2.6 (1 aerobic, 1.6
anaerobic species). The aerobic bacteria identified included
Pseudomonas aeruginosa, Alcaligenes faecalis, Acinetobacter
baumannii complex, Stenotrophomonas maltophilia, and
Bacillus cereus (all of these were isolated in one patient).
The facultative anaerobic bacteria were methicillin-sensitive
Staphylococcus aureus (MSSA; three patients),
Enterococcus faecalis, Enterobacter cloacae, Streptococcus
dysgalactiae, and Proteus vulgaris (all isolated from
all wounds). The strict anaerobic bacterial species was
Peptostreptococcus asaccharolyticus (one patient).
Preoperative blood culture performed in one patient was negative.
Antibiotics were selected and administered for four patients (cases
1–4) based on the preoperative antibiotic sensitivity test
(Table IV).
| Table IV.Microbiological analyses and
antibiotics. |
Table IV.
Microbiological analyses and
antibiotics.
| A, Initial
presentation |
|---|
|
|---|
| Case | Sampling | Bacterial
strain | Antibiotics |
|---|
| 1 | Wound | Pseudomonas
aeruginosa Enterococcus faecalis Alcaligenes faecalis | Levofloxacin
hydrate |
| 2 | Wound |
Methicillin-sensitive Staphylococcus
aureus Streptococcus dysgalactiae | Clindamycin +
Cefazolin sodium → Cefazoplan |
|
| Blood | Negative |
|
| 3 | Wound |
Methicillin-sensitive Staphylococcus
aureus Bacillus cereus | Cefazolin
sodium |
| 4 | Wound |
Methicillin-sensitive Staphylococcus
aureus Proteus vulgaris | Cefazolin
sodium |
| 6 | Wound | Enterobacter
cloacae Acinetobacter baumannii complex Stenotrophomonas
maltophilia Peptostreptococcus asaccharolyticus | Cefazolin
sodium |
|
| B, Surgical site
infection |
|
| Case |
Sampling | Bacterial
strain |
Antibiotics |
|
| 1 | Wound | Pseudomonas
aeruginosa Enterococcus faecalis | - |
| 2 | Wound |
Methicillin-sensitive Staphylococcus
aureus | Meropenem |
| 3 | Initial
surgery |
|
|
|
| Wound,
blood, urine | Pseudomonas
aeruginosa | Meropenem |
|
| Recurrence |
|
|
|
|
Wound | Pseudomonas
aeruginosa | Meropenem |
|
|
Blood | Negative |
|
Surgical Site Infection
Surgical site infection (SSI) occurred in three
patients (43%), including two patients with superficial incisional
SSI and one with deep incisional SSI. It was observed in 3/5
patients with exudate, but none in those without exudate. All three
patients had received preoperative sensitivity-guided perioperative
antibacterial prophylaxis. The bacterial isolates from MWs and
surgical sites were identical in two of three patients (MSSA and
Pseudomonas aeruginosa) and in one other patient
(Pseudomonas aeruginosa). One patient (case 1) had
levofloxacin-sensitive Pseudomonas aeruginosa and
Alcaligenes faecalis cultured from the wound at the initial
presentation, and was given levofloxacin hydrate preoperatively.
Five days after resection and skin graft, Pseudomonas
aeruginosa was cultured from the exudate of the grafted skin.
Saline washing was performed and the wound healed without delay. In
another patient (case 2), MSSA and Streptococcus
dysgalactiae were isolated from the wound at the initial
presentation. Pus was observed in the separated wound after one
month of the hip disarticulation, from which MSSA was cultured.
Irrigation, debridement, and intravenous meropenem resolved the
deep incisional infection. In another patient (case 3), MSSA and
Bacillus cereus were cultured from the wound at the initial
presentation. Resection following reconstruction with free flap and
skin graft was performed and cefazolin sodium, to which MSSA was
sensitive, was given one day prior to surgery up to four days
postoperatively. Fever continued after surgery, and Pseudomonas
aeruginosa was isolated from the exudate of the grafted skin,
in blood, and urine. The wound improved after saline washing and
meropenem administration. The patient developed MWs from the
recurrence 2.5 years later, for which hip disarticulation was
performed. Pus was observed from the separated wound one month
after surgery, and Pseudomonas aeruginosa was cultured from
the wound. Irrigation and debridement were performed and meropenem
was administered, which cured the deep incisional infection.
Laboratory investigation
The values of the laboratory tests for each patient
are shown in Table SII. Four
patients presented with elevated WBC count (average; 10169/µl,
range: 5820-14820/µl), which decreased to the normal value within
three weeks after surgery for all patients (Fig. 1A). Five patients presented with
elevated CRP (average; 8.4 mg/dl, range: 0.11-27.7 mg/dl), which
decreased to the normal value in three patients and was less than 1
mg/dl in the other two patients after surgery (Fig. 1B). Four patients presented with low
Hgb, which was diagnosed as anemia (average; 11.4 g/dl, range:
8.2-14.4 g/dl) (Fig. 1C). Four
patients received RBC transfusions. The value of Hgb improved in
three patients, though new asymptomatic anemia was seen in two
patients after surgery. Two patients presented with elevated levels
of BUN (average; 18.4 mg/dl, range: 9.7-43.5 mg/dl), which improved
to within normal limits within one week after surgery in both the
patients (Fig. 1D). Cr was within
the normal range (average; 0.77 mg/dl, range: 0.53-0.96 mg/dl) in
all patients during the first presentation and after surgery
(Fig. 1E). Six patients presented
with low Alb levels (average; 3.2 g/dl, range: 1.6-3.9 g/dl), which
improved in three patients after surgery (Fig. 1F). ALT was within the normal range
(average; 19 g/dl, range: 6–38 g/dl) during the first presentation,
and one patient had transient elevation after surgery (Fig. 1G). All but one patient presented
with elevated AST (average; 23 g/dl, range: 11–56 g/dl), which
improved within five weeks after surgery (Fig. 1H). Two patients had transient
elevation after surgery. All but one patient presented with
elevated T-bil (average; 0.98 mg/dl, range: 0.47-2.3 mg/dl), which
improved to the normal value one week after surgery (Fig. 1I), and significantly decreased two
weeks after surgery (P=0.04).
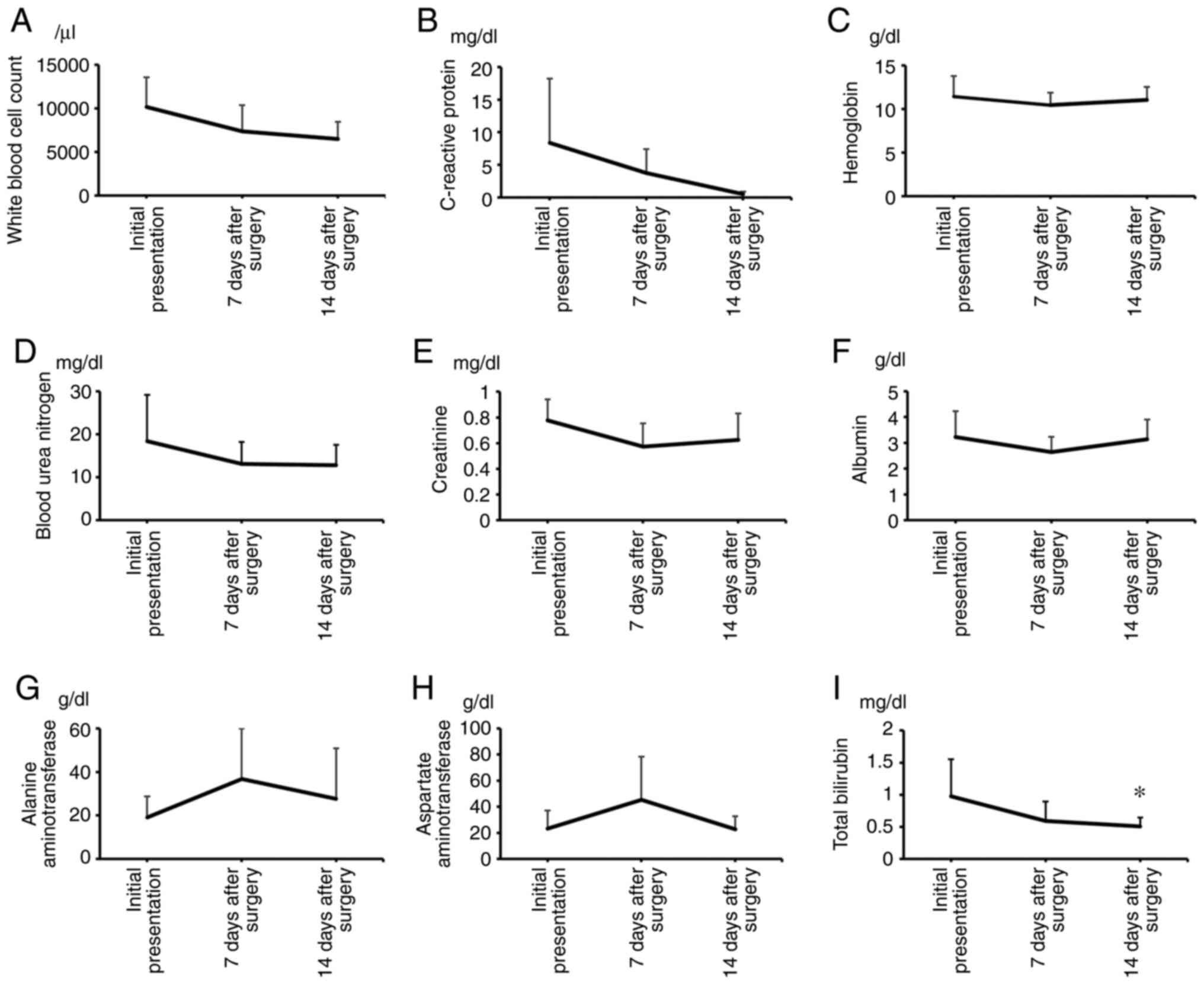 | Figure 1.Laboratory results. The levels of
WBC, CRP, Hgb, BUN, Cr, Alb, ALT, AST and T-bil were investigated
at the initial presentation and after surgery (2–6 weeks). (A) A
total of four patients presented with elevated WBC count (average
10169/µl), which decreased to the normal range within three weeks
after surgery in all patients. (B) A total of five patients
presented with elevated CRP (average 8.4 mg/dl), which decreased
over time. (C) Four patients presented with low Hgb and were
diagnosed as having anemia (average 11.4 g/dl). The level of Hgb
improved in three patients. (D) Two patients presented with
elevated BUN (average 18.4 mg/dl), which normalized within one week
after surgery. (E) Cr was within the normal range (average 0.77
mg/dl) in all patients during the first presentation and after
surgery. (F) Six patients presented with low Alb (average 3.2
g/dl), which improved in three patients after surgery. (G) ALT was
within the normal value (average 19 g/dl), and one patient
experienced transient elevation after surgery. (H) All patients,
except for one, presented with elevated AST (average 23 g/dl),
which improved within five weeks after surgery. (I) All patients,
except for one, presented with elevated T-bil (average 0.98 mg/dl),
which improved to within normal limits one week after surgery, and
significantly decreased two weeks after surgery. *P=0.04. Alb,
albumin; ALT, alanine aminotransferase; AST, aspartate
aminotransferase; BUN, blood urea nitrogen; Cr, creatinine; CRP,
C-reactive protein; Hgb, hemoglobin; T-bil, total bilirubin; WBC,
white blood cell. |
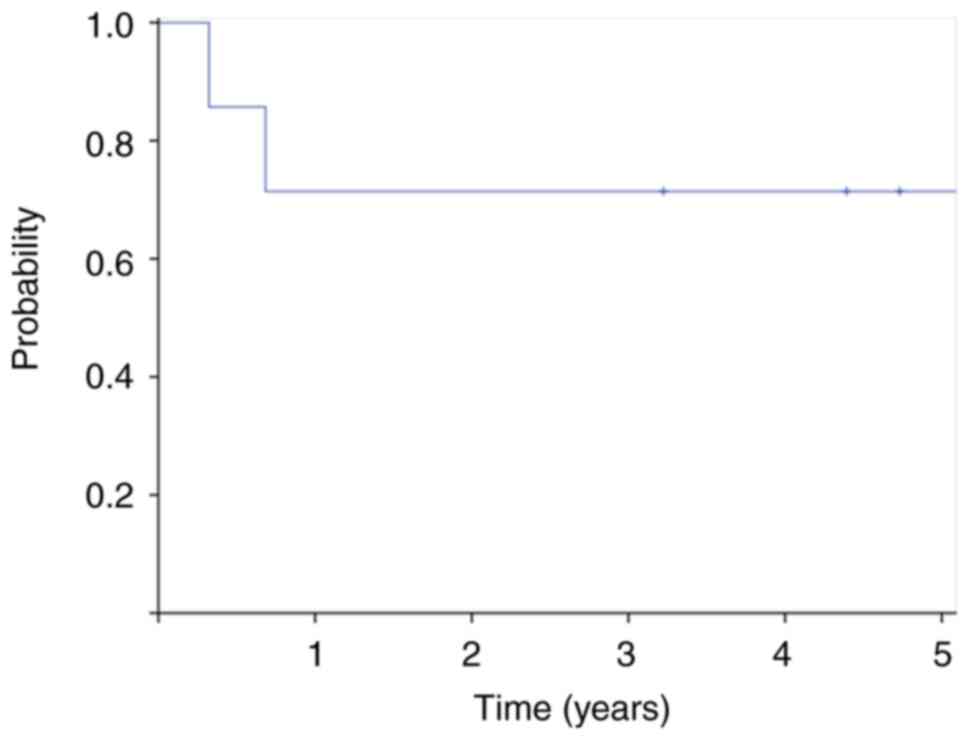
Prognosis
Among the seven patients, one experienced local
recurrence after 4 months, and underwent re-excision of the
recurrent lesion. Three patients had distant metastases at
presentation: lymph node metastasis in two patients, lung
metastasis in one patient, and bone metastasis in one patient. Two
patients developed distant metastases during the follow-up period,
including lymph node metastasis in one patient, lung metastasis in
one patient, and soft tissue in one patient. Four patients died
before the last follow-up. The 5-year OS rate was 71% (Fig. 2).
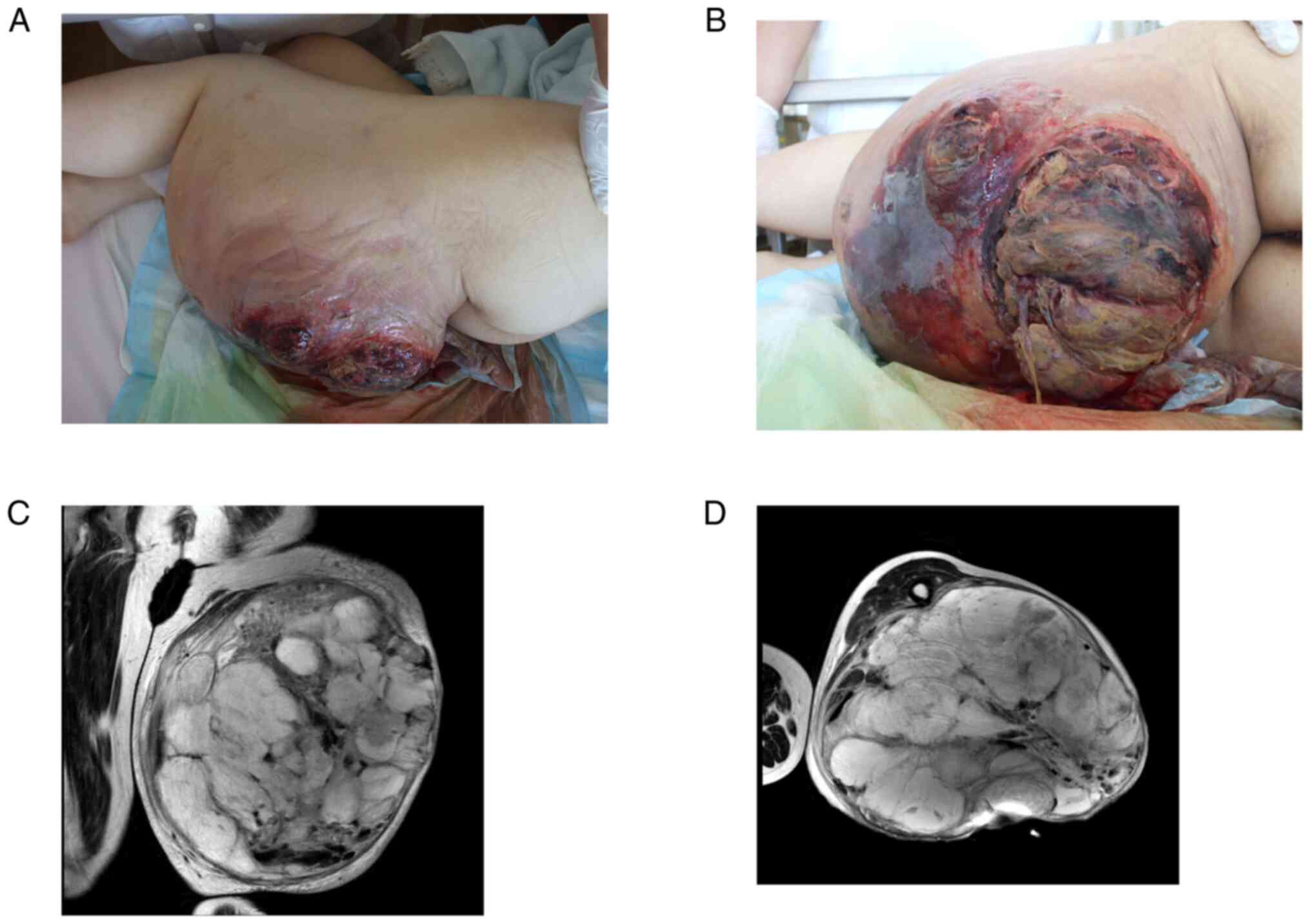
Case 1
The patient was a 42-year-old woman with MW from a
myxoid liposarcoma in the thigh. She was quickly transported to the
hospital because of pain and fatigue. She had a large tumor in her
left thigh with bleeding, odor, and exudate on the overlying skin
(Fig. 3A and B), and was referred
to our institution. MRI revealed a mass with high intensity on
T2-weighted images (Fig. 3C and
D). CT revealed multiple lesions in both lungs. Although the
patient was conscious (Glasgow Coma Score of 15), she was pale and
had abnormal vital signs: fever (39°C), low systolic blood pressure
(89 mmHg), tachycardia (123/min), and hyperpnea (38/min). She also
had low oxygen saturation (96%). Laboratory examination showed
elevation of WBC (14820/µl), CRP (27.7 mg/dl), BUN (43.5 mg/dl),
AST (56 U/l), and T-bil (2.3 mg/dl), low value of Hgb (8.2g/dl) and
Alb (1.6 g/dl), and normal levels of ALT and Cr. Infection was
suspected in the presence a qSOFA score of 2 at presentation. The
patient received red blood cell (RBC) transfusions and infusion. A
diagnosis of sepsis was confirmed by a SOFA score of 2. Culture
from the wound revealed MSSA and Streptococcus dysgalactiae,
for which clindamycin and cefazolin sodium were given. Improvement
was seen in both clinical status and abnormal laboratory values.
Needle biopsy revealed myxoid liposarcoma. Hip disarticulation was
performed four days later, and all abnormal values of laboratory
examinations improved after surgery. Antibiotics were changed to
cefazolin after surgery, which was given for seven days.
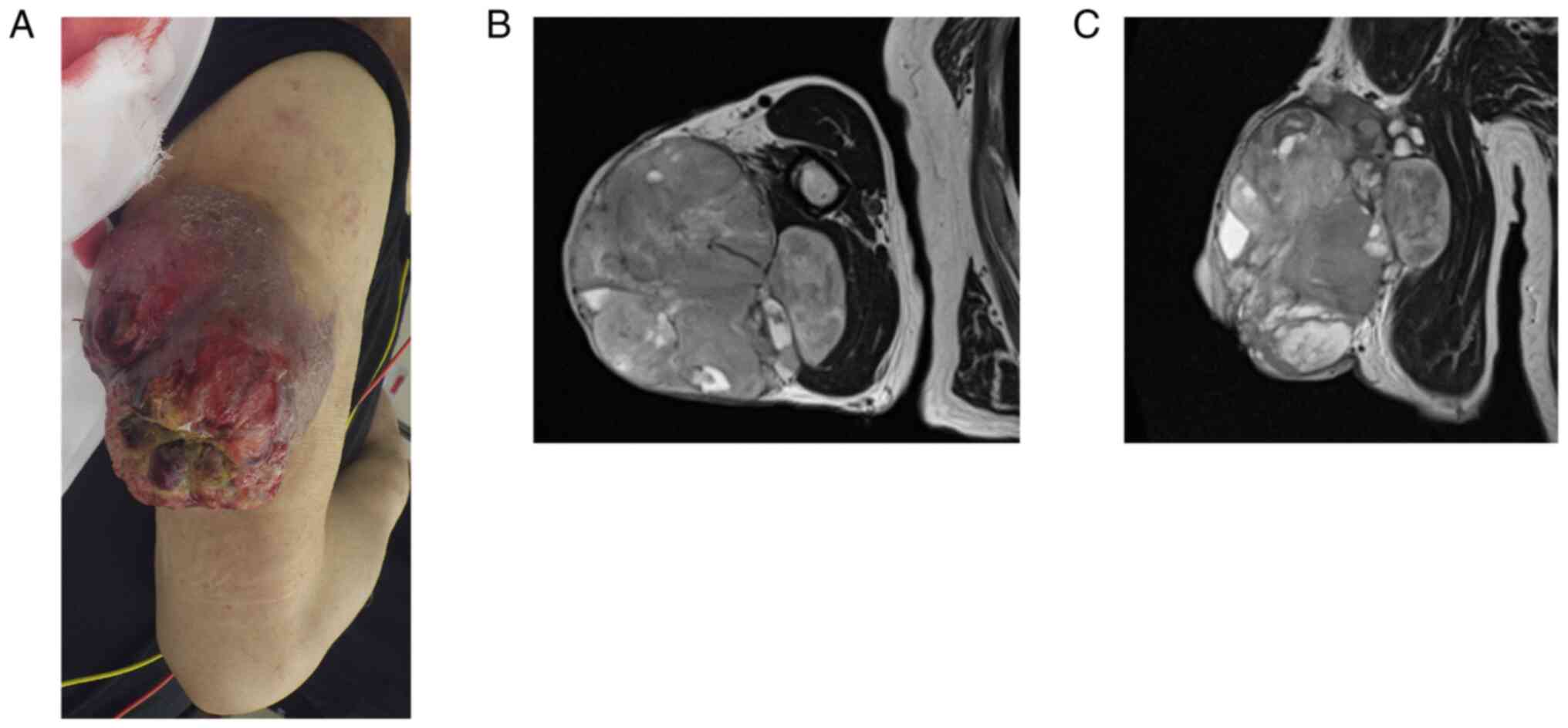
Case 6
The patient was a 78-year-old man who was referred
to our institution for further examination of MW from a
myxofibrosarcoma in the upper arm. He had a large tumor in his
right upper arm with odor and exudate on the wounded overlying skin
(Fig. 4A). MRI revealed a mass
with high intensity on T2-weighted images (Fig. 4B and C). Laboratory examination
showed elevation of, CRP (15.1 mg/dl), low value of Hgb (9.5 g/dl)
and Alb (2.5 g/dl). Culture from the wound revealed polymicrobial
etiology: Enterobacter cloacae, Acinetobacter baumannii
complex, Stenotrophomonas maltophilia, and
Peptostreptococcus asaccharolyticus. Wide resection and free
flap (latissimus dorsi flap) were performed. Cefazolin sodium was
given for 7 days postoperatively. Improvement was seen in abnormal
laboratory values after surgery. Lymph node metastasis was
documented four years later, which was excised, and the patient had
remained disease-free at the last follow up.
Discussion
Fromantin et al identified polymicrobial
flora composed of 54 different bacterial types in the
microbiological analyses of MWs of breast cancer. The study
reported that the average number of bacteria per patient was 3.6
aerobic species and 1.7 anaerobic species, with a predominance of
Staphylococcus aureus, Pseudomonas aeruginosa, Corynebacterium
striatum, and Proteus mirabilis (4). Lutchminarian et al reported
that the most common pathogen in the wound was Staphylococcus
aureus (33%), followed by β-hemolytic Streptococcus
(17%) and Pseudomonas aeruginosa (17%) in patients with MWs
of STS (13). Similar to these
reports, we found that MSSA was the most commonly isolated species,
followed by Pseudomonas aeruginosa and Enterococcus
faecalis. Moreover, we first showed that MWs of STS were
polymicrobial in etiology, with an average number of bacteria per
patient was 2.6, including 1 aerobic species and 1.6 anaerobic
species.
We found that SSI occurred in three of the seven
patients (43%). This high rate of SSI is in line with a previous
report in which SSI was found to be in as many as 26–42% of
patients with MWs (15,18). There are numerous reports
investigating the risk factors associated with SSI (28–30).
According to the international consensus on orthopedic infection by
the Musculoskeletal Infection Society, the risk of developing SSI
is influenced by several factors, such as malignancy, malnutrition,
preoperative anemia, age (>75 years), and a history of diabetes
mellitus (DM) (28). In a
systematic review, risk factors associated with SSI among surgical
patients include high body mass index, National Nosocomial
Infections Surveillance risk index (contamination class, American
Society of Anesthesiologists class, and operative time), and a
history of DM (30). In this
study, patients with MWs had multiple accompanying factors,
including malignancy (100%), contaminated or dirty wound (100%),
malnutrition with low albumin (86%), and anemia (57%), which would
lead to a high SSI rate. Hoshi et al reported that
Candida species were detected most commonly, followed by
Pseudomonas aeruginosa and Enterococcus species from
the infected surgical site (18).
In this study, we found Pseudomonas aeruginosa in two
patients and MSSA in one patient from the infected surgical site.
We compared the bacterium both in the preoperative wound and the
surgical site and found that two of the three patients with SSI had
identical isolates on both sites. These three patients had received
perioperative prophylaxis. However, it was unclear whether the
perioperative antibiotic prophylaxis could be attributed in
preventing SSI in patients with MWs. The limited efficacy of
systemic antibiotic injections may be due to the necrotic tissue,
avascular environment of MWs, and the biofilm (31). Once bacteria adhere to the surface
of the tissue or prosthetic materials, they form microcolonies
(31–33). Next, they produce an extracellular
polymeric matrix and encase themselves in the matrix (33). Bacteria that form biofilms and
colonize or infect medical devices or wounds are particularly
difficult to treat as biofilms are highly resistant to antibiotics
(32–34). Several pharmaceutical interventions
for reducing the microbial concentration in the wound have been
investigated in patients with MWs to avoid wound contamination of
potentially colonized bacterium (32–34).
Recently, the use of metronidazole, which is deemed effective in
eliminating anaerobes, has been shown to be effective in improving
odor in 83–95% of patients (35,36).
In a multicenter, open-label, phase III study conducted among
patients with unresectable breast cancer, head and neck cancer,
skin cancer, and STS, Watanabe et al reported that 95% of
the patients experienced relief with respect to severity of odor by
using topical metronidazole 0.75% gel (36). Mohs' paste has also been shown to
be effective for controlling MWs from various malignant tumors,
including STS (6–8). It is mainly composed of zinc chloride
and was originally developed for curative treatment via repeated
fixation and excision until there is complete removal of the tumor
(6). Hoshi et al reported
success in the combined treatment using Mohs' paste and neoadjuvant
chemotherapy for undifferentiated pleomorphic sarcoma arising in
the right chest wall (9). Systemic
chemotherapy and Mohs' paste led to significant shrinkage of the
tumor and received wide resection and reconstruction with a rectus
abdominis musculocutaneous flap. In this study, we did not utilize
these agents prior to surgery. As patients with MWs frequently
require soft tissue coverage for large defects after resection, it
is necessary to adjust the schedule of plastic surgery, as it is
not possible to remove it immediately. The pharmacologic agents may
be considered for control of both tumor and the infection when
surgery cannot be performed immediately (33). The efficacy of these agents for
reducing SSI should be further investigated using randomized
controlled trials in the future.
We found that patients with MWs of STS had various
symptoms. They had bleeding (71%), exudated (71%), or developed an
odor (43%) at the initial presentation. However, these symptoms
disappeared after surgery. All except for one patient experienced
pain at the site of the MWs on initial presentation, with an
average NRS of 4.4. The NRS decreased after surgery, with an
average of 1.4 (P=0.14) and 0.6 (P=0.04) one and two weeks after
surgery, respectively., All but one patient had pain at the
surgical site at the last follow-up. Two patients presented with
fever, which improved one week after surgery. Regarding laboratory
results, the patients had elevated CRP level (71%), anemia (57%),
malnutrition with low albumin (86%), and renal or liver
disturbances (14–29%). These abnormal laboratory values could have
been due to the complex effect of both the tumor and infection. We
found that these abnormal laboratory values were reversible, as
most of them improved after surgery. Then, we think the tumor with
MWs should be excised completely if possible.
In this study, one patient was diagnosed with sepsis
and required emergency treatment. Although she had poor general
condition at the first presentation to the hospital, RBC
transfusion and infusion could improve the hemodynamics. In case of
MWs at the first presentation, the microbiological condition is
sometimes underrecognized or underestimated because physicians tend
to focus on investigating the oncological condition of the patient
(9). However, physicians should
consider that MWs can potentially turn into a life-threatening
condition when complicated by sepsis. Clinical parameters, such as
vital signs, laboratory results, bacterial culture from the wound
should be examined promptly to manage the patients adequately.
We found some studies which highlight the
oncological implications of MWs of STS (15–18).
In these previous reports, patients with MWs of STS presented with
high proportion of metastases (20–33%) and had a poor prognosis
with a 5-year OS of 15–26% (15–18).
Potter et al compared the oncological outcomes between the
MWs group and the non-MWs group and found that patients with MWs
from STS presented with a higher rate of metastases (33% in the MWs
group and 9% in the non-MWs group; P=0.003) and had a poor
prognosis (5-year OS of 20% in the MWs group and 63% in the non-MWs
group; P<0.0001) (16).
Similarly, Parry et al reported that prognosis of patients
with MWs was poor compared to that of without MWs (5-year OS of 15%
in the MWs group and 66% in the non-MWs group; P<0.0001)
(17). They also reported that MW
was associated with poor prognosis as an independent risk factor.
In line with previous reports (15–18),
three out of seven patients in our study had distant metastases
during presentation. All patients had high-grade sarcoma and a
relatively large tumor size (>5 cm), and three patients died
because of the disease before the last follow-up, with a 5-year OS
rate of 71%. However, limb salvage may be difficult for bulky
tumors, which often increases the risk of amputation (20–33%). In
previous reports, 48–60% of patients required plastic surgery,
including skin graft or flap in limb-sparing surgery (15–18).
In the current study, five patients initially underwent
limb-sparing surgery, and four patients required skin graft or
flap.
This study has some limitations. First, it has a
small sample size of only seven patients. MW occur in 3–4% STS.
Therefore, it was difficult to include enough cases for this study.
Second, we did not investigate the biofilms in the MWs. Since, this
is a retrospective study, we had not investigated the biofilms in
this series of the patients. Third, due to the retrospective study
we had not investigated the preoperative microbiological samples
from the necrotic zone of the wound in all patients. However, we
showed that the MWs of STS had a polymicrobial etiology with an
average number of bacteria per patient was 2.6, and predominance of
Staphylococcus aureus and Pseudomonas aeruginosa,
consistence with previous reports. Fourth, we could not determine
the effectiveness of selected antibiotics in preventing SSI in
patients with MWs, since not all patients received perioperative
prophylaxis. Their effectiveness in preventing SSI needs to be
investigated in the future. Despite these limitations, this is the
first report investigating perioperative clinical symptoms,
laboratory examination, and the bacterial landscape in patients
with MWs of STS.
In conclusion, MW is composed of high-grade sarcoma
and polymicrobial colonization. Physicians should consider that MWs
can possibly lead to life-threatening conditions when complicated
by sepsis; therefore, clinical and laboratory examinations should
be performed promptly to manage patients adequately. Although
patients presented with various symptoms and showed abnormal values
in laboratory examination, they might improve after surgical
resection. The effectiveness of the selected antibiotics based on
the results of the preoperative culture in preventing SSI needs to
be investigated in the future in patients with MWs.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
EN, TK, and TO designed the study. EN, TF and TK
treated the patients. EN, HK and TI collected and analyzed data. EN
and TK confirmed the authenticity of all the raw data. All authors
have read and approved the final manuscript.
Ethics approval statement and consent to
participate
This retrospective chart review study involving
human participants was in accordance with the ethical standards of
the institutional and national research committee and with the 1964
Helsinki Declaration and its later amendments or comparable ethical
standards. The Human Investigation Committee (IRB) of Okayama
University Hospital approved this study (approval no. K2104-020).
Patients provided written informed consent for their participation
in this study.
Patient consent for publication
Written informed consent was obtained from each
participant included in this study.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Alexander S: Malignant fungating wounds:
Epidemiology, aetiology, presentation and assessment. J Wound Care.
18:273–274. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Alvarez O, Kalinski C, Nusbaum J,
Hernandez L, Pappous E, Kyriannis C, Parker R, Chrzanowski G and
Comfort CP: Incorporating wound healing strategies to improve
palliation (symptom management) in patients with chronic wounds. J
Palliat Med. 10:1161–1189. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Vardhan M, Flaminio Z, Sapru S, Tilley CP,
Fu MR, Comfort C, Li X and Saxena D: The microbiome, malignant
fungating wounds, and palliative care. Front Cell Infect Microbiol.
9:3732019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fromantin I, Seyer D, Watson S, Rollot F,
Elard J, Escande MC, De Rycke Y, Kriegel I and Larreta Garde V:
Bacterial floras and biofilms of malignant wounds associated with
breast cancers. J Clin Microbiol. 51:3368–3373. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Finlayson K, Teleni L and McCarthy AL:
Topical opioids and antimicrobials for the management of pain,
infection, and infection-related odors in malignant wounds: A
systematic review. Oncol Nurs Forum. 44:626–632. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mohs FE, Sevringhaus EL and Schmidt ER:
Conservative amputation of gangrenous parts by chemosurgery. Ann
Surg. 114:274–282. 1941. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mohs FE: Chemosurgical treatment of cancer
of the extremities and trunk; a microscopically controlled method
of excision. Arch Surg (1920). 57:818–832. 1948. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nemoto K, Okamoto M, Kito M, Aoki K,
Suzuki S, Takazawa A, Yoshimura Y and Kato H: Combined treatment
using Mohs' paste and neoadjuvant chemotherapy for giant gluteal
soft tissue sarcoma with malignant fungating wound: A case report.
J Surg Case Rep. 2019:rjz1372019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hoshi M, Iwai T, Oebisu N and Nakamura H:
Successful pre-operative local control of skin exposure by sarcoma
using combination of systemic chemotherapy and Mohs' chemosurgery.
World J Surg Oncol. 18:362020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bower M, Stein R, Evans TR, Hedley A, Pert
P and Coombes RC: A double-blind study of the efficacy of
metronidazole gel in the treatment of malodorous fungating tumours.
Eur J Cance. 28A:888–889. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kalinski C, Schnepf M, Laboy D, Hernandez
L, Nusbaum J, McGrinder B, Comfort C and Alvarez OM: Effectiveness
of a topical formulation containing metronidazole for wound odor
and exudate control. Wounds. 17:84–90. 2005.
|
|
12
|
Ashford R, Plant G, Maher J and Teare L:
Double-blind trial of metronidazole in malodorous ulcerating
tumours. Lancet. 1:1232–1233. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lutchminarian K and Clarke DL: The
microbiology of ulcerative skin cancers: Does the presence of
pathogenic bacteria increase the risk of postoperative
complications? S Afr J Surg. 59:25a–25e. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Elfallal AH, Laimon YN and Emile SH: Giant
angiolipoma of the back complicated with ulceration and sepsis:
Unusual presentation of a rare benign tumour. Ann R Coll Surg Engl.
101:e91–e93. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Okajima K, Kobayashi H, Okuma T, Arai S,
Zhang L, Hirai T, Ishibashi Y, Ikegami M, Shinoda Y, Akiyama T, et
al: Prognosis and surgical outcome of soft tissue sarcoma with
malignant fungating wounds. Jpn J Clin Oncol. 51:78–84. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Potter BK, Adams SC, Qadir R, Pitcher JD
and Temple HT: Fungating soft-tissue sarcomas. Treatment
implications and prognostic importance of malignant ulceration. J
Bone Joint Surg Am. 91:567–574. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Parry M, Evans S, Sugath S, Wafa H, Jeys L
and Grimer R: Fungation in soft tissue sarcomas is associated with
poor survival. Int Orthop. 41:2613–2618. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hoshi M, Oebisu N, Iwai T, Ieguchi M and
Nakamura H: Clinical course of soft tissue sarcomas presenting as
malignant wounds. J Orthop Sci. 24:1088–1093. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fletcher CD, Bridge JA, Hogendoorn P and
Mertens F: WHO Classification of Tumours of soft tissue and bone.
4th edition. IARC Press; Lion: 2013
|
|
20
|
Guillou L, Coindre JM, Bonichon F, Nguyen
BB, Terrier P, Collin F, Vilain MO, Mandard AM, Le Doussal V,
Leroux A, et al: Comparative study of the National cancer institute
and french federation of cancer centers sarcoma group grading
systems in a population of 410 adult patients with soft tissue
sarcoma. J Clin Oncol. 15:350–362. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mangram AJ, Horan TC, Pearson ML, Silver
LC and Jarvis WR: Guideline for prevention of surgical site
infection, 1999. Hospital infection control practices advisory
committee. Infect Control Hosp Epidemiol. 20:250–278. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Egi M, Ogura H, Yatabe T, Atagi K, Inoue
S, Iba T, Kakihana Y, Kawasaki T, Kushimoto S, Kuroda Y, et al: The
Japanese clinical practice guidelines for management of sepsis and
septic shock 2020 (J-SSCG 2020). J Intensive Care. 9:532021.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rhodes A, Evans LE, Alhazzani W, Levy MM,
Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally
ME, et al: Surviving sepsis campaign: International guidelines for
management of sepsis and septic shock: 2016. Crit Care Med.
45:486–552. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Seymour CW, Liu VX, Iwashyna TJ,
Brunkhorst FM, Rea TD, Scherag A, Rubenfeld G, Kahn JM,
Shankar-Hari M, Singer M, et al: Assessment of Clinical criteria
for sepsis: For the Third International consensus definitions for
sepsis and septic shock (Sepsis-3). JAMA. 315:762–774. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pandharipande PP, Sanders N, Jacques P,
Ely EW and Shintani A: Calculating SOFA scores when arterial blood
gasses are not available: Validating
SpO2/FIO2 ratios for imputing
PaO2/FIO2 ratios in the SOFA scores. Crit
Care Med. 34:A12006. View Article : Google Scholar
|
|
26
|
Pasricha SR, Colman K, Centeno-Tablante E,
Garcia-Casal MN and Peña-Rosas JP: Revisiting WHO haemoglobin
thresholds to define anaemia in clinical medicine and public
health. Lancet Haematol. 5:e60–e62. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wittekind C, Compton C, Quirke P,
Nagtegaal I, Merkel S, Hermanek P and Sobin LH: A uniform residual
tumor (R) classification: Integration of the R classification and
the circumferential margin status. Cancer. 115:3483–3488. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zainul-Abidin S, Amanatullah DF, Anderson
MB, Austin M, Barretto JM, Battenberg A, Bedard NA, Bell K, Blevins
K, Callaghan JJ, et al: General assembly, prevention, host related
general: Proceedings of International consensus on orthopedic
infections. J Arthroplasty. 34:S13–S35. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chauveaux D: Preventing surgical-site
infections: Measures other than antibiotics. Orthop Traumatol Surg
Res. 101 (Suppl 1):S77–S83. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Korol E, Johnston K, Waser N, Sifakis F,
Jafri HS, Lo M and Kyaw MH: A systematic review of risk factors
associated with surgical site infections among surgical patients.
PLoS One. 8:e837432013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ramasubbu DA, Smith V, Hayden F and Cronin
P: Systemic antibiotics for treating malignant wounds. Cochrane
Database Syst Rev. Aug 24–2017.(Epu. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Schierle CF, De la Garza M, Mustoe TA and
Galiano RD: Staphylococcal biofilms impair wound healing by
delaying reepithelialization in a murine cutaneous wound model.
Wound Repair Regen. 17:354–359. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Salisbury AM, Woo K, Sarkar S, Schultz G,
Malone M, Mayer DO and Percival SL: Tolerance of biofilms to
antimicrobials and significance to antibiotic resistance in wounds.
Surg Technol Int. 33:59–66. 2018.PubMed/NCBI
|
|
34
|
Hughes G and Webber MA: Novel approaches
to the treatment of bacterial biofilm infections. Br J Pharmacol.
174:2237–2246. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Villela-Castro DL, Santos VLCG and Woo K:
Polyhexanide versus metronidazole for odor management in malignant
(fungating) wounds: A double-blinded, randomized, clinical trial. J
Wound Ostomy Continence Nurs. 45:413–418. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Watanabe K, Shimo A, Tsugawa K, Tokuda Y,
Yamauchi H, Miyai E, Takemura K, Ikoma A and Nakamura S: Safe and
effective deodorization of malodorous fungating tumors using
topical metronidazole 0.75% gel (GK567): A multicenter, open-label,
phase III study (RDT.07.SRE.27013). Support Care Cancer.
24:2583–2590. 2016. View Article : Google Scholar : PubMed/NCBI
|