Introduction
Multiple primary malignant neoplasms (MPMN) are
defined as two or more primary malignancies occurring in the same
person, rather than metastasis. So far, numerous (1–6) of
MPMN have been reported, with a relatively large number of
diachronic MPMN and a smaller proportion of simultaneous MPMN. It
is rare to find three or more cases of simultaneous multiple
malignancies. Owing to continuous innovations in the treatment of
malignant tumors, the survival of some patients with cancer has
been prolonged. In addition, because of an increase in human
longevity and improvements in diagnostic technology, the incidence
of a number of types of malignant tumors is on the rise. The
present study reported the case of a 51-year-old woman with
right-sided invasive breast cancer, left-sided ductal carcinoma
in situ, endometrioid adenocarcinoma, cervical cancer and
ovarian cancer. Such cases of multiple concurrent primary tumors
are rare.
Case report
A 51-year-old woman with a history of mammary gland
involvement and no history of cancer or other diseases was admitted
to The Second Hospital of Jilin University (Jilin, China) for
vaginal bleeding. The approval number of this case are 2023138. Six
months before hospitalization, she had experienced vaginal bleeding
but did not pay attention to it. Gynecological examination revealed
a vaginal tumor 5–6 cm in diameter that appeared in the cervix and
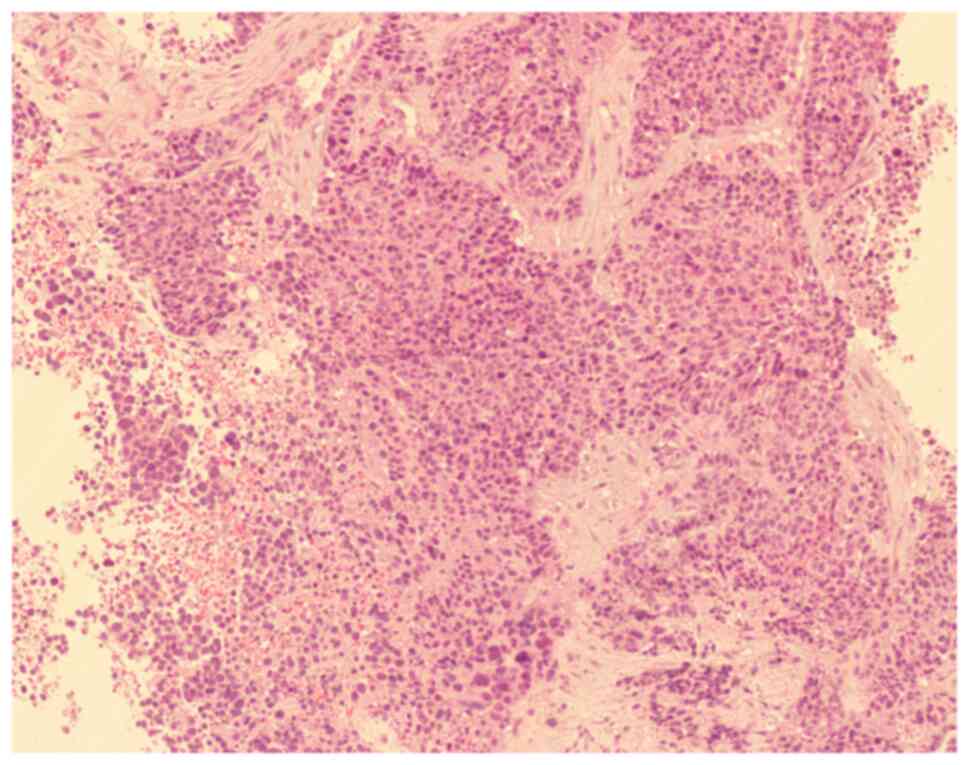
accumulated in the lower third of the vagina. Biopsy of the
cervical tumor showed a hypodifferentiated neuroendocrine carcinoma
with invasive squamous cell carcinoma nests in the local cells
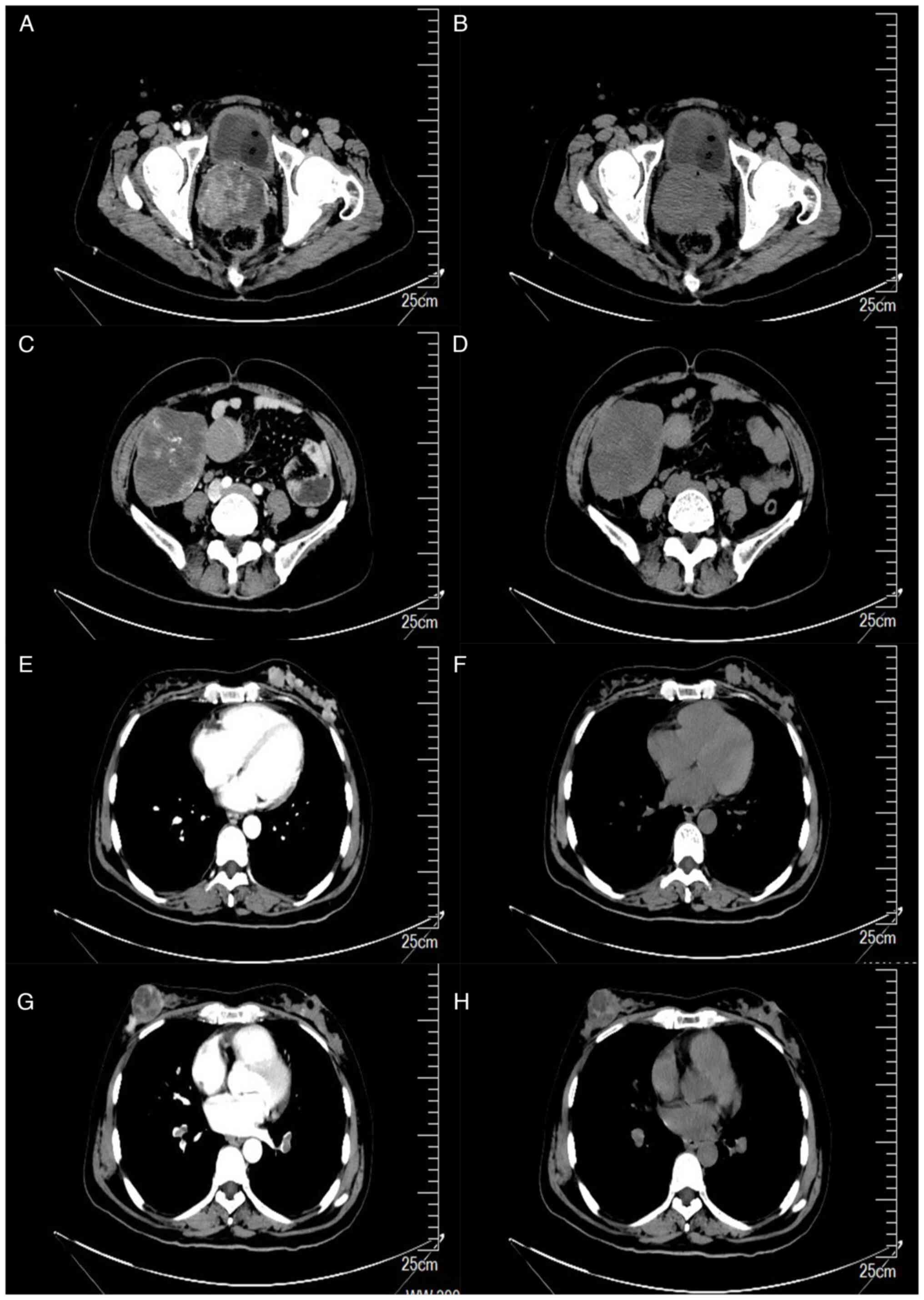
(Fig. 1). To clarify the stage and
further improve the examination, the brain was scanned using
functional magnetic resonance imaging (MRI). Chest, abdomen and
pelvis computed tomography (CT) with contrast were subsequently
performed, which revealed a cervical lump (Fig. 2A and B), right abdominal lump
(Fig. 2C and D), left breast lump
(Fig. 2E and F) and right breast
lump (Fig. 2G and H). Based on the
imaging findings, it was suspected that the lumps were malignant.
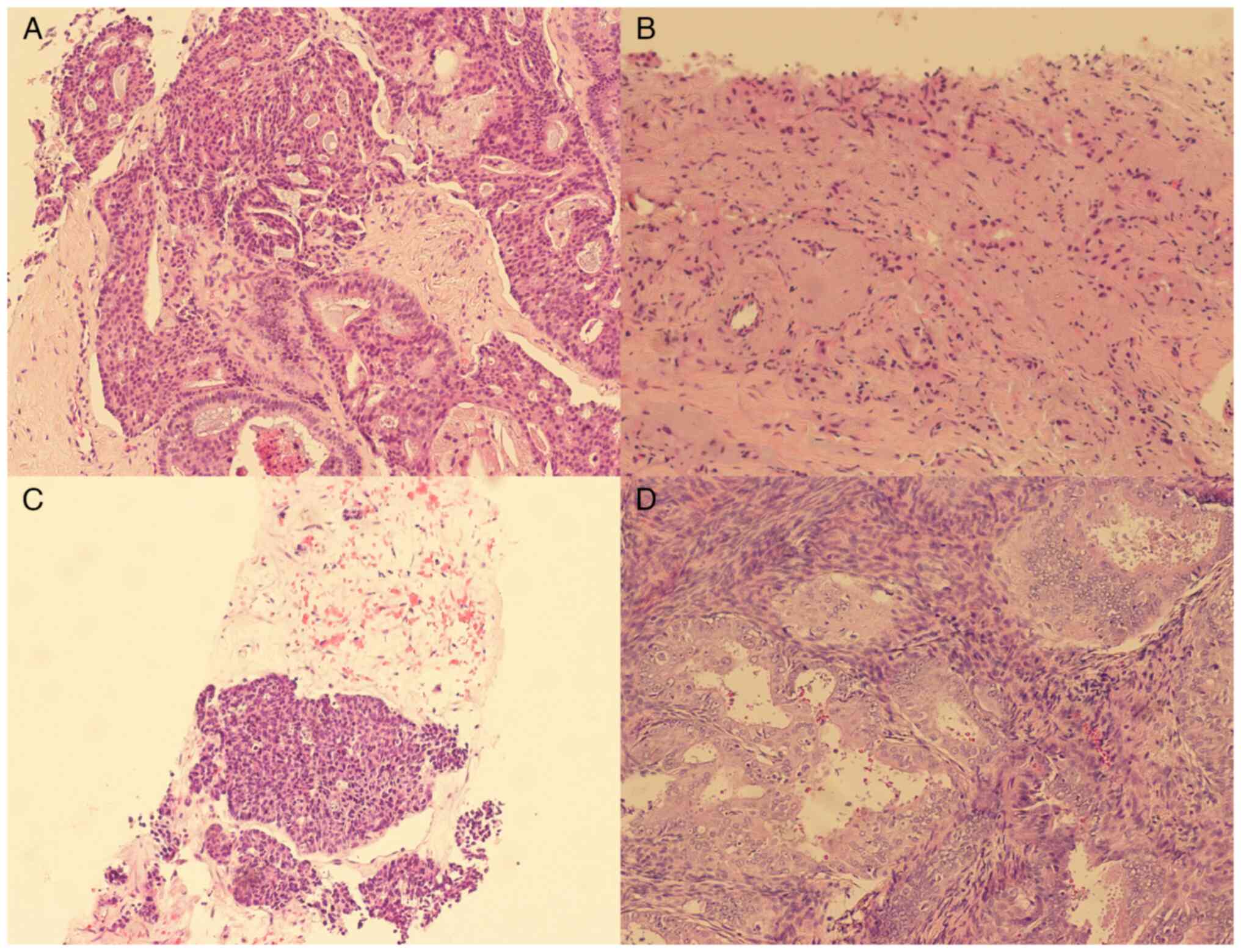
Therefore, a biopsy of the breast and ovarian masses was performed
to obtain pathological tissue. Low-grade ductal carcinoma in
situ was observed in the pathological tissue of the left breast
(Fig. 3A), invasive breast cancer
was observed in the pathological tissue of the right breast
(Fig. 3B) and invasive carcinoma
was observed in the pathological tissue of the right ovary with
localized areas of neuroendocrine differentiation (Fig. 3C). For H&E staining, the tumor
tissue sections were dewaxed and hydrated. The sections were
stained with hematoxylin and eosin staining, respectively.
Dehydrate with low to high levels of alcohol. Slices were
penetrated with xylene and covered with resin. HE-stained sections
were imaged using Leica DM4000B fluorescence microscope
(magnification: ×100).
Immunohistochemistry was performed on the cervical,
bilateral breast and right ovarian pathological biopsy tissues. For
immunohistochemical staining, tumor tissue was embedded in paraffin
wax and a section of 4-µm thickness was cut using a microtome
(HM355s, Thermo Scientific). The slices are dewaxed and hydrated.
Heat-induced antigen repair was performed with 10 mM sodium citrate
buffer (PH 6.0). The activity of endogenous peroxidase was blocked
by incubation with 3% H2O2 for 10 min. Penetration was performed in
0.1% Triton X-100. The tissue sections were incubating by PBS-T
(QuickBlock™ Blocking Buffer, Beyotime, Shanghai, China) containing
10% goat serum (Beyotime, Shanghai, China) at room temperature for
25 min to block non-specific binding. Primary antibody (Catalogue
number, supplier are listed in Table
I) is incubated overnight at 4°C. Add horseradish peroxidase
(HRP) labeled goat anti mouse/rabbit IgG, 1:50, (Beyotime, A0216,
A0208, Shanghai, China) to slices, and incubation for 30 min at
room temperature. Add Diaminobenzidine (DAB) (DAB Horseradish
Peroxidase Color Development Kit, Beyotime, P0203, Shanghai, China)
to each section and the color was developed 30 sec to 5 min away
from light. The staining effect was observed under a microscope,
and the staining was terminated with distilled water. Double dye
with hematoxylin for 30 sec at room temperature. Photographs are
taken under an optical microscope. Immunostained sections were
imaged using Leica DM4000B fluorescence microscope (magnification:
×100). Immunohistochemistry of cervical tissue was as follows
(Fig. S1): CK(AE1/AE3) (+), CK5/6
(partial +), p63 (partial +), P40 (partial +), Pl6 (+), Ki67
(90%+), CgA (−), Syn (weak +), CD56 (partial +).
Immunohistochemistry of the left breast tissues was as follows
(Fig. S2): ER (+), PR (partial +),
CK5/6 (−), HER 2 (2+), Ki67 (10%+), P16 (+), P40 (−), Syn (−), CK
(AEl/AE3) (+). Immunohistochemistry of the right breast tissue was
as follows (Fig. S3): INSMl
(partial +), CgA (−), Nkx2. 2 (−), CK7 (−), CK8/18 (+), nut (−),
BRG 1 (+), ER (partial +), PR (−), GATA3 (little +), INI-1 (+).
Immunohistochemistry of the right ovarian tissue was as follows
(Fig. S4): TTF I 1 (+), Ki67 (95%
positive), P53 (−).
 | Table I.Primary antibodies. |
Table I.
Primary antibodies.
| Antibody | Company | Cat. no. | Dilution |
|---|
| Anti-Cytokeratin
AE1/AE3 | Sigma-Aldrich; Merck
KGaA | MAB3412 | 1:500 |
| Anti-CK5/6 | Uni-science | PA6040 | 1:100 |
| Anti-p63 Rabbit
Monoclonal | Sigma-Aldrich; Merck
KGaA | SAB56000289 | 1:50 |
| NCF4/p40-phox Rabbit
mAb | ABclonal | A0935 | 1:200 |
| Anti-ARPC5/p16
ARC | Abcam | ab51243 | 1:50 |
| Anti-CGA | Sigma-Aldrich; Merck
KGaA | HPA029698 | 1:250 |
| Anti-NCAM1
antibody | Abcam | ab133345 | 1:500 |
| Anti-Desmuslin/SYN
antibody | Abcam | ab204369 | 1:1000 |
| Ki67 Rabbit mAb | ABclonal | A20018 | 1:250 |
| ERp44 (D17A6)
XP® Rabbit mAb | Cell Signaling | 3798 | 1:500 |
| ERp44 (D17A6)
XP® Rabbit mAb | Cell Signaling | 8757 | 1:500 |
| Anti-INSM1 | Abcam | ab305104 | 1:100 |
| NKX2-1 Rabbit
mAb | ABclonal | A22247 | 1:1000 |
| Anti-Cytokeratin 7
antibody | Abcam | ab181598 | 1:5000 |
| Aiti-CK8/18
antibody | Uni-science | PA7148 | 1:1000 |
| NUT (C52B1) Rabbit
mAb | Cell Signaling | 3625 | 1:3000 |
| Anti-BRG1 | Abcam | ab110641 | 1:100 |
| Anti-GATA3 | Abcam | ab199428 | 1:500 |
| INI-1 (MRQ-27) Mouse
monoclonal | Sigma-Aldrich; Merck
KGaA | 272M-1 | 1:200 |
| Anti-TTF1 | Abcam | ab76013 | 1:250 |
| p53 Rabbit pAb | ABclonal | A0263 | 1:50 |
Due to the large cervical lump and persistent
vaginal bleeding, our treatment team decided to perform external
beam radiation therapy (EBRT) to shrink the tumor for surgery. EBRT
was started on February 18, 2022 and finished on March 21, 2022.
The whole uterus, adnexa and lymphatic drainage area were treated
with 50 Gy in 25 fractions, 1.8 Gy per day, 5 days per week, to the
planning target volume. Positive pelvic lymph nodes were treated
with 60 Gy in 25 fractions, 2.4 Gy per day, 5 days per week,
delivered to the planning target volume. In addition, combined
chemotherapy, including albumin, paclitaxel, carboplatin and
bevacizumab, was administered for three cycles during and after
radiotherapy. Gynecological surgery was performed on June 12, 2022,
during which the entire uterus and bilateral adnexa were removed.
The postoperative pathological findings were as follows: Cervical
tissue infiltrated by multiple foam cells, consistent with
manifestation after neoadjuvant therapy and, surprisingly,
localized cancerous tissue was observed in the endometrium, a
highly differentiated endometrioid carcinoma with a maximum
diameter of ~5 mm (Fig. 3D). A
small number of heterotypic cell nests were observed in the right
ovary, consistent with poorly differentiated carcinomas. The
patient then underwent three cycles of chemotherapy and radical
breast cancer surgery according to the original protocol. She is
currently in a good general condition and intends to continue
adjuvant treatment for breast cancer.
Literature review
MPMN refers to the occurrence of two or more primary
malignant tumors in a single patient. It occurs around the age of
50 years, which is similar to the age at which the incidence of
malignant tumors is high. It is widely considered that the reasons
for the increasing incidence of multiple cancers are multifaceted,
such as the increased health awareness of individuals, improved
clinical treatment techniques, genetic defects, environmental
problems, adverse effects of treatment for the first primary
cancer, decreased immune levels due to tumors or treatments and
increased life expectancy. With the improvement of the Chinese
economy, the realization of early tumor diagnosis and the rapid
development of tumor treatment technology, an increasing number of
patients with tumors have significantly longer survival times than
previously and the incidence of multiple cancers has increased.
The more accepted diagnostic criteria for multiple
cancers are those proposed by Warren and Gates (7): i) Each tumor should be histologically
malignant; ii) each tumor has unique pathological features; iii)
tumors occur at different sites/organs or in different locations in
the same organ and iv) patients with mutual metastases or
recurrence are excluded. Multiple carcinomas are classified as
concurrent or heterochronic multiple carcinomas according to the
time of occurrence. Concurrent multiple carcinomas are those that
occur within 6 months and multiple heterochronic carcinomas are
those that occur for more than 6 months. Metastases can occur
within the same organ or between different organs and multiple
cancers exhibit this feature. Therefore, in the process of tumor
diagnosis and treatment, metastases and multiple cancers should be
identified based on a combination of various tumor characteristics,
imaging and pathologies to reduce missed diagnoses of multiple
cancers.
Coyte et al (8) found that the prevalence of multiple
cancers is associated with the epidemiological characteristics of
the tumor in a country or region. For example, in Japan the most
common type of primary MPMN is gastrointestinal malignancy,
followed by breast cancer (9). It
is reported that the incidence of multiple cancers in patients with
primary head and neck squamous cell carcinoma can account for
10–40% (10). Adjei Boakye et
al (11) reported that the
incidence of secondary primary carcinoma after treatment for
squamous carcinoma of the head and neck ranged from 5–36%. Song
et al (12) found that the
incidence of second primary carcinoma of the oral cavity associated
with radiotherapy for nasopharyngeal carcinoma was 0.3–11% and that
the tissue type was mostly squamous cell carcinoma. When the first
cancer is breast cancer, there are more reports of a second primary
cancer occurring in the thyroid (13). A study conducted at the Cancer
Hospital of the Chinese Academy of Medical Sciences showed that the
most frequent cancers with cervical cancer as the primary cancer
were esophageal cancer, followed by bronchial lung cancer, stomach
cancer, uterine body malignancy, rectal cancer and breast cancer.
In addition, the wide application of radiotherapy for cervical
cancer and its treatment effects have been improving and an
increasing number of patients are surviving for a long time.
Therefore, radiation cancer, a serious long-term complication of
radiation therapy, has been identified. Radiation carcinomas
account for 23% of repeat carcinomas and 82.2% of repeat carcinomas
within the radiated area of cervical cancer (14).
Several factors contribute to the development of
multiple cancer types. Therefore, primary prevention of diseases,
such as smoking cessation, exercise and good sleep, should be
performed. Attention should be paid to secondary prevention
strategies including early detection, diagnosis and treatment. In
addition, cancer patients have a higher tendency to develop
multiple types of cancer. According to statistics, it is estimated
that 5–15% of patients develop secondary primary cancer. Therefore,
attention should be paid not only to the diagnosis of multiple
cancers before the treatment of malignant tumors, but also to
regular and comprehensive reviews after treatment. If this can be
done, we can avoid missed and mis-diagnoses, which can delay
treatment. Clinicians should consider the most common organs
involved in multiple cancers. Follow-up reviews of patients with
breast cancer should focus on the thyroid and ovaries; patients
with nasopharyngeal cancer should pay attention to tongue changes.
Patients with cervical cancer can undergo regular esophagoscopy
during the review. In all patients with cancer, the possibility
that the lung lesion may be a secondary primary cancer should be
considered.
Among the theories on multiple cancer risk factors,
one is the ‘regional carcinogenesis theory’, in which researchers
consider that the esophagus and gastrointestinal tract are the
channels for food, the lungs are the channels for breathing and the
urinary system is the channel for waste excretion. After tumor
treatment, they continue to receive stimulation from carcinogens,
leading to the development of multiple carcinogens (15). Considering that regional
carcinogenesis is a continuous and progressive process, it is
important to follow patients with relevant tumors for life. In
addition, in the clinical treatment process, combined immunotherapy
can be considered to reduce toxicity, increase effectiveness, avoid
the harm caused by traditional treatments, such as radiotherapy and
chemotherapy, and can also enhance the immune ability of patients,
control disease development, improve clinical efficacy and prolong
and improve the quality of life and survival of patients.
Multiple cancers not only aggravate the condition of
cancer patients but also make treatment difficult. Prognosis also
differs depending on the location of multiple cancers and treatment
methods. Although multiple cancers are difficult to treat, early
detection, diagnosis and selection of appropriate treatment methods
can still enable long-term survival in some patients. Therefore,
once multiple cancers are considered, multidisciplinary
consultations should be actively conducted to consider the specific
conditions of each patient and to formulate individualized
treatment plans to obtain the best treatment and prognosis.
Discussion
The occurrence and reporting of multiple cancers
associated with breast cancer is common. Previous case reports
(16–21) have identified a number of types of
multiple cancers associated with breast cancer, including skin
cancer, gastrointestinal cancer, colon cancer, hematologic tumors,
sarcomas, lung cancer, gynecologic tumors, thyroid cancer and
urinary malignancies (16). There
is a close association between breast cancer and gynecological
tumors, especially ovarian cancer, because they share similar risk
factors such as early menarche, advanced age without childbearing,
obesity and high-fat diet (22,23).
In addition, some genetic syndromes, such as Lynch syndrome, Cowden
syndrome and mutations in the BRCA1 and BRCA2 genes, increase the
risk of developing breast, ovarian and endometrial cancers
(21,24). Therefore, gynecological examinations
should be considered when patients are diagnosed with breast
cancer. During follow-up after treatment, attention should be paid
to the examination of the ovary and uterus to exclude lesions.
In the present case, pathological tissues were
obtained from patients with cervical cancer, bilateral breast
cancer, ovarian cancer and endometrial cancer and hematoxylin and
eosin staining performed (H&E staining). Cervical malignancies,
bilateral breast malignancies and endometrial malignancies are
significantly different histologically, which meet the inclusion
criteria of Warren and Gates and can be defined as MPMN. To further
confirm the origin of these cancerous tissues, immunohistochemical
testing was performed on these tissues. P16, CK (AE1/AE3), CD56
were positive, confirming that cervical cancer was primary.
Bilateral breast cancer histological morphology is different;
estrogen (ER) and progesterone receptors are positive in left
breast cancer; ER and insulinoma-associated-1 receptors are
positive in right breast cancer. These features confirm that
bilateral breast cancers are primary and that bilateral breast
cancers do not metastasize to each other. Endometrial cancer is
found after surgery and its histological morphology shows that it
is endometrioid carcinoma. Although there is no immunohistochemical
support, the diagnosis was confirmed as primary endometrial cancer
by three experienced pathologists. Here, cancerous tissue of the
ovaries is poorly differentiated and immunohistochemistry is not
specific. Ovarian cancer with neuroendocrinization is relatively
rare and there are few relevant descriptions in the literature. In
a previously reported case, a patient had peritoneal recurrence of
high-grade serous ovarian carcinoma with tumor cell components
expressing neuroendocrine markers but lacking the morphological
features of neuroendocrine differentiation (25). A case of simultaneous ovarian
neuroendocrine and endometrial serous carcinoma has also been
reported, but the ovarian tumor was confirmed to be metastatic from
the endometrial serous carcinoma by gene sequencing (26). Schultheis et al (27) showed that ovarian metastases could
be confirmed to originate from endometrial cancer by genetic
testing of pathological tissues of co-occurring endometrial and
ovarian cancers and found that the vast majority shared common
ancestral clones. Karpathiou et al (26) argued that caution should be
exercised when interpreting immunostaining results in poorly
differentiated carcinoma because the expression of neuroendocrine
markers does not necessarily indicate a tumor of neuroendocrine
cell origin. Instead, it represents a form of tumor progression. In
addition, the clinical manifestations of ovarian metastases and
primary cancers differ. The classic criteria for ovarian metastasis
in endometrial cancer include bilateral multinodular small ovarian
involvement, large endometrial tumors with deep muscularity and
vascular invasion and tubal lumen involvement. By contrast, primary
ovarian cancers are unilateral, large and have different
morphological types. In the present study, the ovarian biopsy
pathology of the patient showed a low-grade carcinoma with local
neuroendocrine differentiation. The clinical manifestation was a
large-volume unilateral tumor. The patient also had cervical
neuroendocrine carcinoma and endometrial cancer. Therefore, poorly
differentiated ovarian carcinomas can be primary or metastatic. The
source of ovarian cancer cannot be identified by pathology and
immunohistochemistry alone and it needs to be confirmed by gene
sequencing if it is to be further confirmed. In addition, genetic
testing can determine whether a patient has genetic syndromes.
Unfortunately, due to the poor financial status of the patient,
this examination was not performed. The absence of genetic testing
is a limitation in this case, but this patient has no family
history of hereditary tumor syndromes, which can basically rule out
genetic factors. In addition, the lack of MRI scans before breast
cancer surgery was also a limitation in the present case.
The patient had multiple primary cancers
simultaneously, with multiple and complex pathological types,
making the choice of a treatment plan more difficult. Due to the
large cervical cancer mass with lymphocytic metastasis,
hypodifferentiated ovarian and bilateral breast cancer without
axillary lymph node metastasis, it was decided to perform
neoadjuvant chemoradiotherapy to shrink the gynecological tumor for
surgery and simultaneously treat the bilateral breast cancer at the
same time. Considering the pathological type of the patient, the
decision was made after multidisciplinary consultation and
discussion of albumin, paclitaxel and carboplatin combined with
bevacizumab chemotherapy and concurrent pelvic radiotherapy.
Following neoadjuvant therapy, gynecological surgery was performed
and she was diagnosed with endometrial cancer. The original
chemotherapy regimen is also applicable to endometrial cancer.
Subsequently, three cycles of chemotherapy and radical mastectomy
were performed. Currently, the patient has been reviewed regularly
and no metastasis or recurrence has been observed.
In summary, MPMN is common. The reasons for its
occurrence are multifaceted and include genetic, physical and
environmental factors, cancer inducers caused by chemotherapy or
radiotherapy, or decreased immune function (28). Patients with MPMN have obvious
genetic factors and genetic abnormalities may be the cause of
multiple cancers (29). Abnormal
DNA mismatch repair is also associated with MPMN (29–31).
MPMN can occur at any age but is more likely to occur in
middle-aged and elderly individuals. The incidence of MPMN is
higher in men than in women (32).
When a patient is suspected of having an MPMN, a comprehensive
physical examination should be performed to detect and treat other
potential cancers in a timely manner. The principle of treatment
for multiple cancers is to develop an individualized treatment plan
based on the specific situation of the patient, including
comprehensive treatments such as surgery, radiotherapy,
chemotherapy and targeted therapy.
Currently, there is no standard treatment protocol
for multiple cancers. Most literature on multiple cancers is
presented in the form of case reports that can be used by
oncologists to learn from each other. There remain a number of
forms of multiple cancers or successful cases that are not widely
known. A multi-cancer website could be established for oncologists,
in order to deepen the understanding of multiple cancers and learn
from each other's experience in treatment, so that multi-cancer can
be diagnosed and treated early and prognosis improved.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was supported by funding from Health
Commission of Jilin Province (A project to improve the ability to
diagnose and treat gynecological oncology; grant no. 3D517EC03427),
Health Commission of Jilin Province (CBCT bone registration was
used to analyze the effect of volume rotation intensity modulation
on target dose; grant no. 2020SCZT012), Health Commission of Jilin
Province (Dose-effect analysis of Zeiss intraoperative radiotherapy
machine irradiating primary cultured vertebral metastases; grant
no. 2019SCZT029).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
JG and LH drafted the manuscript and conceived the
study. LZ, CX, MJ and GZ were responsible for collection and
analysis of case data and literature. JG provided financial
support. MJ and GZ confirmed the authenticity of all the raw data.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of this case report and its
accompanying images
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Awad BI, Melibari B, Safadi N, Al-Garni M
and Al-Hakami HA: Triple head and neck carcinoma: Case report and
literature review. Cureus. 12:e70822020.PubMed/NCBI
|
|
2
|
Huang XY, Huang ZL, Huang J, Wang ZG and
Zheng Q: A case of multiple primary malignancies and investigation
of family history. Oncol Lett. 4:931–934. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tzortzatos G, Wersäll O, Danielsson KG,
Lindblom A, Tham E and Mints M: Familial cancer among consecutive
uterine cancer patients in Sweden. Hered Cancer Clin Pract.
12:142014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sun JJ, Yang TB, Yang YH, Liu WF and Song
JX: Synchronous double primary malignancies of the liver and
kidney: A case report. Oncol Lett. 11:2057–2060. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pu X, Xu T, Ge C, He Y, Yang X and Chang
P: A case of durvalumab-treated double primary cancers of the colon
and lung. Ann Palliat Med. 9:3614–3622. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhao J, Tan Y, Wu Y, Zhao W, Wu J, Ji M,
Shi L, Jiang J and Wu C: A rare case of eight multiple primary
malignant neoplasms in a female patient: A case report and review
of the literature. Oncol Lett. 9:587–590. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Warren S and Gates O: Multiple primary
malignant tumors. A survey of the literature and a statistical
study. Am J Cancer. 16:1358–1414. 1932.
|
|
8
|
Coyte A, Morrison DS and McLoone P: Second
primary cancer risk-the impact of applying different definitions of
multiple primaries: Results from a retrospective population-based
cancer registry study. BMC Cancer. 14:2722014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Arpaci E, Tokluoglu S, Yetigyigit T and
Alkis N: Multiple primary malignancies-a retrospective analysis at
a single center in Turkey. Asian Pac J Cancer Prev. 14:769–773.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Licciardello J, Spitz MR and Hong WK:
Multiple primary cancer in patients with cancer of the head and
neck: Second cancer of the head and neck, esophagus, and lung. Int
J Radiat Oncol Biol Phys. 17:467–476. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Adjei Boakye E, Buchanan P, Hinyard L,
Osazuwa-Peters N, Schootman M and Piccirillo JF: Incidence and risk
of second primary malignant neoplasm after a first head and neck
squamous cell carcinoma. JAMA Otolaryngol Head Neck Surg.
144:727–737. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Song M, Zhuang SM, Chen SW, Zhang Q, Yang
AK, Wang LP and Guo ZM: Survival study and treatment strategy for
second primary tumors in the oral cavity in patients with
nasopharyngeal carcinoma after definitive radiation. Head Neck.
34:1551–1555. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sadetzki S, Calderon-Margalit R, Peretz C,
Novikov I, Barchana M and Papa MZ: Second primary breast and
thyroid cancers (Israel). Cancer Causes Control. 14:367–375. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Weibo Y; Zihao Y, Guozhen X and Yimin H:
Radiation Oncology. 4th Edition. Beijing: Chinese Union Medical
University Press, Beijing, China; pp. 13742008, (In Chinese).
|
|
15
|
Mukaiyama Y, Suzuki M, Morikawa T, Mori Y,
Takeshima Y, Fujimura T, Fukuhara H, Nakagawa T, Nishimatsu H, Kume
H and Homma Y: Multiple primary malignant neoplasms of the glottis,
renal pelvis, urinary bladder, oral floor, prostate, and esophagus
in a Japanese male patient: A case report. World J Surg Oncol.
12:2942014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
De Luca A, Frusone F, Vergine M, Cocchiara
R, La Torre G, Ballesio L, Monti M and Amabile MI: Breast cancer
and multiple primary malignant tumors: Case report and review of
the literature. In Vivo. 33:1313–1324. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Asaad A, Barron M, Rasheed N, Idaewor P
and Saad Abdalla Al-Zawi A: The rare diagnosis of synchronous
breast and colonic cancers: A case report and review of literature.
Cureus. 13:e133142021.PubMed/NCBI
|
|
18
|
Mellemkjaer L, Friis S, Olsen JH, Scélo G,
Hemminki K, Tracey E, Andersen A, Brewster DH, Pukkala E, McBride
ML, et al: Risk of second cancer among women with breast cancer.
Int J Cancer. 118:2285–2292. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim JY and Song HS: Metachronous double
primary cancer after treatment of breast cancer. Cancer Res Treat.
47:64–71. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Fukuda H, Tanaka A, Hirashima Y and Ito I:
Lambert-eaton myasthenic syndrome associated with synchronous
double cancer: A combination of small cell carcinoma of the cervix
and breast carcinoma. Intern Med. 57:2409–2411. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nomura H, Ikki A, Fusegi A, Omi M, Aoki Y,
Netsu S, Tanigawa T, Matoda M, Okamoto S, Omatsu K, et al: Clinical
and pathological outcomes of risk-reducing salpingo-oophorectomy
for Japanese women with hereditary breast and ovarian cancer. Int J
Clin Oncol. 26:2331–2337. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fruscalzo A, Damante G, Calcagno A, Di
Loreto C and Marchesoni D: Four primary malignancies successively
occurred in a BRCA2 mutation carrier: A case report. Cancer Invest.
24:611–614. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Filippakis GM, Lagoudianakis EE,
Genetzakis M, Antonakis P, Papadima A, Boussiotou A, Katergiannakis
V and Manouras A: Squamous cell carcinoma arising in a mature
cystic teratoma of the ovary with synchronous invasive lobular
breast cancer: Case report. Eur J Gynaecol Oncol. 27:537–540.
2006.PubMed/NCBI
|
|
24
|
Sakellakis M, Peroukides S, Iconomou G,
Boumpoucheropoulos S and Kalofonos H: Multiple primary
malignancies: A report of two cases. Chin J Cancer Res. 26:215–218.
2014.PubMed/NCBI
|
|
25
|
Taube ET, Denkert C, Pietzner K, Dietel M,
Sehouli J and Darb-Esfahani S: Prognostic impact of neuroendocrine
differentiation in high-grade serous ovarian carcinoma. Virchows
Arch. 466:333–342. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Karpathiou G, Matias-Guiu X, Mobarki M,
Vermesch C, Stachowicz ML, Chauleur C and Peoc'h M: Ovarian
neuroendocrine carcinoma of metastatic origin: Clues for diagnosis.
Hum Pathol. 85:309–312. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Schultheis AM, Ng CK, De Filippo MR,
Piscuoglio S, Macedo GS, Gatius S, Perez Mies B, Soslow RA, Lim RS,
Viale A, et al: Massively parallel sequencing-based clonality
analysis of synchronous endometrioid endometrial and ovarian
carcinomas. J Natl Cancer Inst. 108:djv4272016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Vogt A, Schmid S, Heinimann K, Frick H,
Herrmann C, Cerny T and Omlin A: Multiple primary tumours:
Challenges and approaches, a review. ESMO Open. 2:e0001722017.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Copur MS and Manapuram S: Multiple primary
tumors over a lifetime. Oncology (Williston Park).
33:6293842019.PubMed/NCBI
|
|
30
|
Bateman AC: DNA mismatch repair proteins:
Scientific update and practical guide. J Clin Pathol. 74:264–268.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sharma R, Lewis S and Wlodarski MW: DNA
repair syndromes and cancer: Insights into genetics and phenotype
patterns. Front Pediatr. 8:5700842020. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhai C, Cai Y, Lou F, Liu Z, Xie J, Zhou
X, Wang Z, Fang Y, Pan H and Han W: Multiple primary malignant
tumors-a clinical analysis of 15,321 patients with malignancies at
a single center in China. J Cancer. 9:2795–2801. 2018. View Article : Google Scholar : PubMed/NCBI
|