Introduction
Ovarian cancer (OC) presents a significant global
health challenge, with >300,000 new cases and 200,000 deaths
reported worldwide in 2020 (1).
Despite advancements in medical research, there are still no
effective tools for general population screening, which complicates
early detection. This challenge is reflected economically, as the
cost of treatment per patient with OC remains the highest among all
cancer types, with initial treatment costs in the first year
amounting to approximately USD 80,000, and potentially increasing
to USD 100,000 in the final year (2). Cost-effective strategies for early
detection and prevention of OC have thus been a significant focus
of research over the last decade.
This disease often remains undetected until the
advanced stages due to its elusive symptoms, leading to late
diagnoses and less effective treatments (3,4).
Currently, CA125 and HE4 are the only approved biomarkers for use
in epithelial OC (EOC); however, these markers are not sufficient
for early detection. To mitigate the limitations of single serum
biomarkers in EOC, multivariate index assays have been developed,
particularly for the pre-surgical evaluation of adnexal masses. The
Risk of Malignancy Algorithm, which integrates menopausal status,
CA125, and HE4 concentrations, is used to diagnose women with a
pelvic mass. Furthermore, microRNAs have shown remarkable potential
in EOC prediction, though further work is needed before they can be
utilized as reliable clinical biomarkers (5).
Among OC types, EOC is particularly known for its
invasive nature and predominance. However, it is important to note
that 10% of OC cases are non-epithelial, including germ cell
tumors, sex cord-stromal tumors, and some extremely rare tumors
such as small cell carcinomas. Germ cell tumors, for instance,
differ significantly from EOCs, with earlier age of incidence,
faster growth rates, unilateral localization in 95% of cases, and
generally better prognosis (6).
EOC encompasses a spectrum of histologic subtypes,
including serous, mucinous, endometrioid, clear cell, or
combinations of these subtypes (7).
These subtypes exhibit unique molecular profiles, contributing to
the differences in causes, epidemiology, treatments, and prognoses
(8). Specifically, Type I EOCs are
generally indolent and genetically stable tumors that typically
arise from precursor lesions such as endometriosis or borderline
tumors with low malignant potential. In contrast, Type II EOCs are
biologically aggressive tumors from their outset, with a tendency
to metastasize from small-volume primary lesions. High-grade serous
OC, following the Type II pathway, is often associated with p53 and
BRCA mutations (9).
Genetic and molecular pathway alterations play
significant roles in OC initiation and development. For instance,
serous OCs often exhibit BRCA1/2 and TP53 mutations
and is involved in the amplification of G1/S-specific cyclin-E or
defective homologous recombination DNA repair pathways (10), whereas non-serous OCs are associated
with mutations in genes involved in pathways such as AT-rich
interactive domain-containing protein, phosphatidylinositol
3-kinase (PI3K), K-Ras/B-Raf, Wnt, or protein phosphatase 2A
(11). Within this context, it is
critical to note that the PI3K pathway plays a pivotal role in
chemoresistance and preservation of genomic stability, as it is
implicated in numerous processes of DNA replication and cell cycle
regulation. Inhibition of the PI3K pathway may lead to genomic
instability and mitotic catastrophe through decreased activity of
the spindle assembly checkpoint protein Aurora kinase B,
consequently increasing the occurrence of lagging chromosomes
during prometaphase (12).
Moreover, emerging evidence suggests that high-grade serous OC,
closely connected to the fimbriated ends of the fallopian tubes,
may originate from the precursor lesions in the fallopian tubes
rather than from the ovary itself (3,11,13,14).
In addition to genetic factors, chronic inflammation
is emerging as a key risk factor in EOC development. Persistent
infections that affect the female reproductive organs can trigger a
pro-inflammatory response, exacerbate DNA damage, and contribute to
cancer initiation (15–17). In line with this, the prolonged
exposure of ovarian epithelial cells to inflammatory mediators,
such as pro-inflammatory cytokines, chemokines, and hormones, may
lead to DNA damage through oxidative stress and cause genetic and
epigenetic alterations (18).
However, the role of environmental factors in EOC initiation and
progression, particularly viral infections, is still being
investigated.
High-risk HPV (HR-HPV) plays a crucial role in the
development of cervical cancer and head and neck squamous cell
carcinoma (19,20). HR-HPV carries E6 and E7 oncoproteins
that can inactivate tumor suppressors such as p53, which may be
related to OC development (21,22).
Therefore, researchers have also been attracted to the potential
role of HPV in EOC. However, recent studies have yielded mixed
results regarding the presence of HPV in EOC, with some studies
confirming its presence, whereas others negating it. Notably, among
HR-HPV types, HPV 16 and/or 18 (HPV 16/18) are most frequently
associated with advanced-stage disease, while the others have not
been. Despite two meta-analyses that have explored the link between
HPV and EOC, a specific focus on HPV 16/18 in OC has yet to be
reported (23,24). To address this gap and provide an
updated perspective, emphasizing on HPV 16/18 investigation, this
meta-analysis was conducted to deepen our understanding of this
connection.
Materials and methods
Searching protocol and data
collection
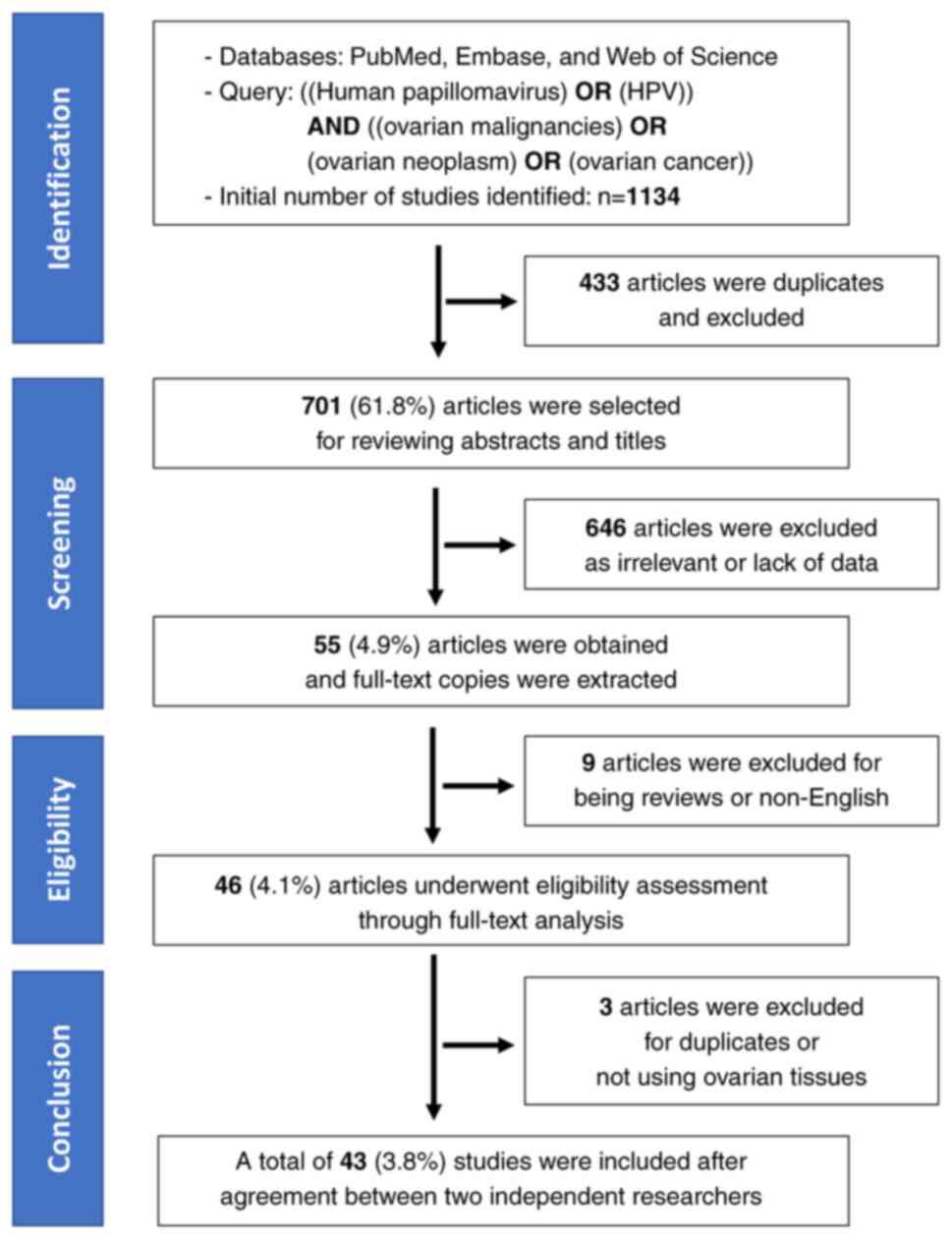
The meta-analysis followed the PRISMA criteria. Two
researchers, TML and HDNT, independently conducted a systematic
literature search covering the period from 1987 to August 2023.
Searches were conducted in PubMed (on October 6, 2023), Embase (on
October 8, 2023), and Web of Science (on October 8, 2023), using
the following search terms with detailed Boolean logic: ((Human
papillomavirus) OR (HPV)) AND ((ovarian malignancies) OR (ovarian
neoplasm) OR (ovarian cancer)).
The initial search yielded 364 records in PubMed,
420 in Embase, and 350 in Web of Science, totaling 1,134 records.
To ensure reproducibility, the search process was independently
verified by both researchers. After eliminating duplicates, all
abstracts (n=701) were independently reviewed to exclude studies
irrelevant to the topic or lacking sufficient data on the
association between HPV and OC. Subsequently, 646 papers were
excluded based on abstract reviews. Full-text copies of potentially
relevant papers were obtained and independently reviewed (n=55). In
total, 43 papers met the inclusion criteria for the meta-analysis
(25–67). Data from these identified studies
were extracted independently, and any disagreements regarding
inclusion or exclusion were resolved through discussion. Recorded
data included the first author's details, publication country,
publication year, detection method, histological type, specimen
type, sample size, HPV genotype, and number of HPV-positive and
HPV-negative OCs, as well as HPV-positive and HPV-negative ovarian
benign tumors or normal ovaries.
To be eligible for inclusion in this meta-analysis,
studies must meet the following criteria: (1) they were observational studies
published between 1987 and August 2023 and provided data on the
association between HPV and OC, (2)
ovarian tissues were used in the study to identify HPV genotypes,
and (3) they were written in
English and published as full, peer-reviewed articles. The
exclusion criteria were as follows: (1) studies not meeting the inclusion
criteria and (2) studies conducted
solely on animals.
Statistical analysis
In this analysis, the pooled prevalence was
estimated using both fixed- and random-effect models, based on the
data from the included studies (68). Forest plots were used to display the
prevalence for all the studies sorted by their publication year
(69). The prevalence derived from
individual studies and pooled proportions were presented with 95%
confidence intervals (CIs). In addition, for case-control studies,
the pooled odds ratio (OR) was computed for the presence of HPV in
OC cases, along with the corresponding 95% CI. Both random- and
fixed-effect models were employed for this analysis. The overall
heterogeneity among the included studies was assessed using the
I2 statistic, with I2 values >50% and/or
P-value <0.05 indicating significant heterogeneity (70,71).
To explore the potential sources of heterogeneity, subgroup
analysis was conducted using meta-regression. This analysis
included variables of geographic region.
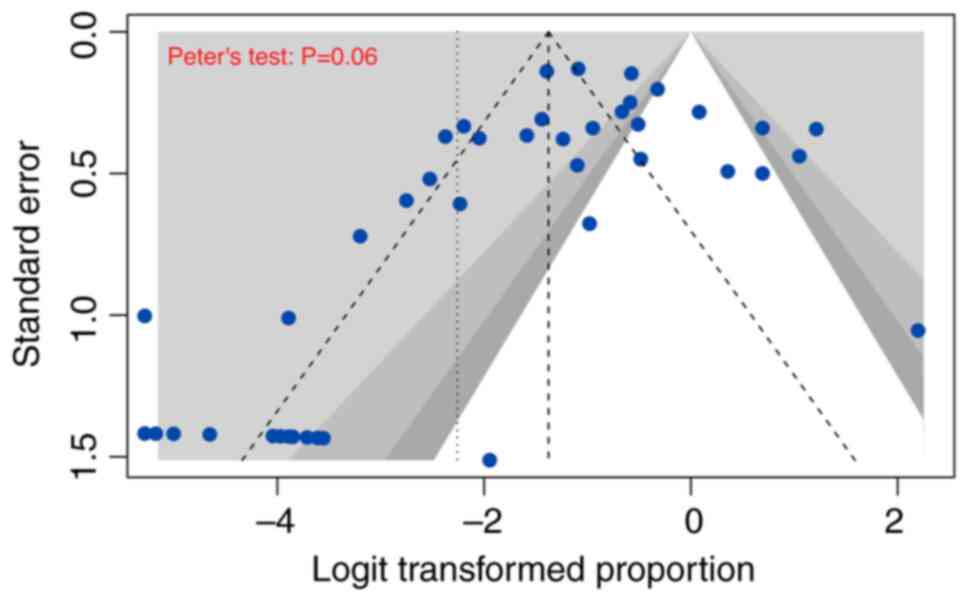
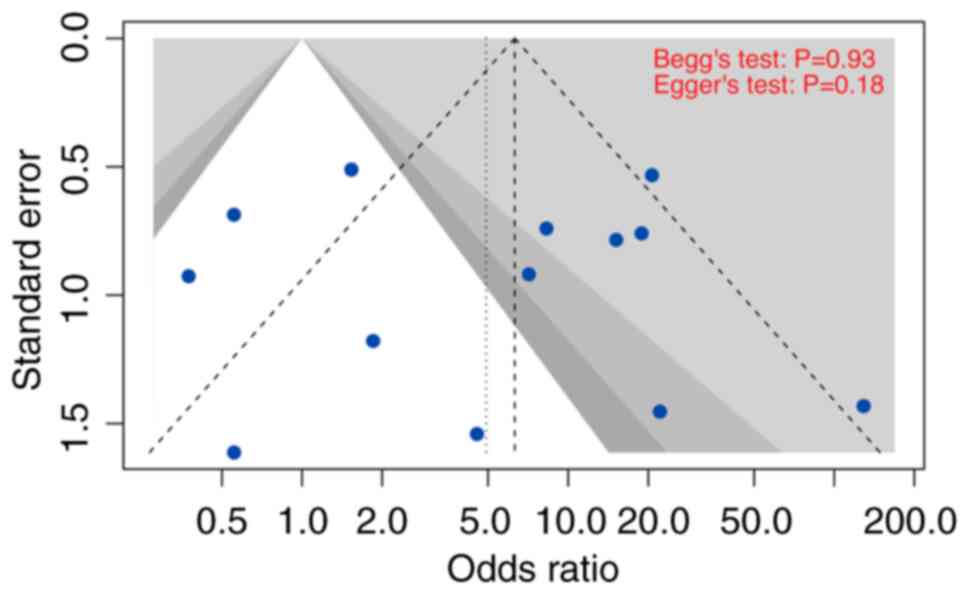
To evaluate publication bias, a funnel plot, which
illustrated the association between the logarithm of HPV prevalence
and standard error, was generated (68,72).
In the comparative (case-control) meta-analysis, potential
asymmetry was examined using two methods: Egger's regression test
and the Begg and Mazumdar adjusted rank correlation test (73,74).
For the proportional meta-analysis, Peter's test, which is based on
precision-effect estimates with standard errors, was employed
(75). Statistical significance was
defined as P-values <0.05.
Analyses were conducted using R v4.3.1 (R Core Team
2023) with packages including ‘meta,’ ‘metasens,’ and ‘metafor’
(69,72,76–78).
Results
Study description
This meta-analysis included 43 studies to
investigate the prevalence of HPV in OC tumor tissue. The study
selection process is illustrated in Fig. 1, and details of the additional study
are available in Table I.
 | Table I.Overview of the included studies. |
Table I.
Overview of the included studies.
|
|
|
| No. of
patients |
|---|
|
|
|
|
|
|---|
| Variable 1 | Variable 2 | No. of included
studies | Serous POS | Serous total | Case POS | Case total | Control POS | Control total |
|---|
| Country | Africa | 2 | 6 | 53 | 18 | 170 | 0 | 0 |
|
| Asia | 21 | 45 | 563 | 426 | 1,691 | 32 | 677 |
|
| Europe | 13 | 35 | 425 | 102 | 763 | 47 | 252 |
|
| North America | 7 | 0 | 30 | 9 | 130 | 0 | 35 |
| Method | PCR | 36 | 58 | 947 | 483 | 2,498 | 68 | 871 |
|
| IHC | 1 | 3 | 26 | 3 | 31 | 0 | 18 |
|
| PCR/IHC | 1 | 9 | 53 | 9 | 53 | 0 | 0 |
|
| ISH | 2 | 15 | 24 | 41 | 90 | 11 | 62 |
|
| PCR/ISH | 2 | 1 | 6 | 17 | 31 | 0 | 8 |
|
| PCR/Southern
blot | 1 | 0 | 15 | 2 | 51 | 0 | 5 |
| Sample type | FFPE | 29 | 46 | 768 | 466 | 2,218 | 77 | 805 |
|
| FFPE, frozen
tissue | 1 | 7 | 14 | 10 | 17 | 0 | 0 |
|
| Frozen tissue | 9 | 27 | 132 | 69 | 287 | 2 | 137 |
|
| Fresh tissue | 4 | 6 | 157 | 10 | 232 | 0 | 22 |
The analysis included a total of 2,754 patients from
43 selected studies (Tables I and
SI). Of these studies, 21 were
conducted in Asia, and the remaining 22 were carried out in other
regions (Europe=13, North America=7, and Africa=2). Among the
selected papers, 19 of 43 were case-control studies that involved
normal ovarian or benign ovarian tumor tissues in the control
group. These studies used formalin-fixed paraffin-embedded samples
(n=30), frozen sections (n=11), and fresh tissues (n=4). These
studies (n=36) predominantly used HPV detection methods based on
polymerase chain reaction. Furthermore, 17 of 43 selected studies
focused specifically only on the detection of HPV 16/18 in the
analysis.
Prevalence of HPV in OC and
subgroups
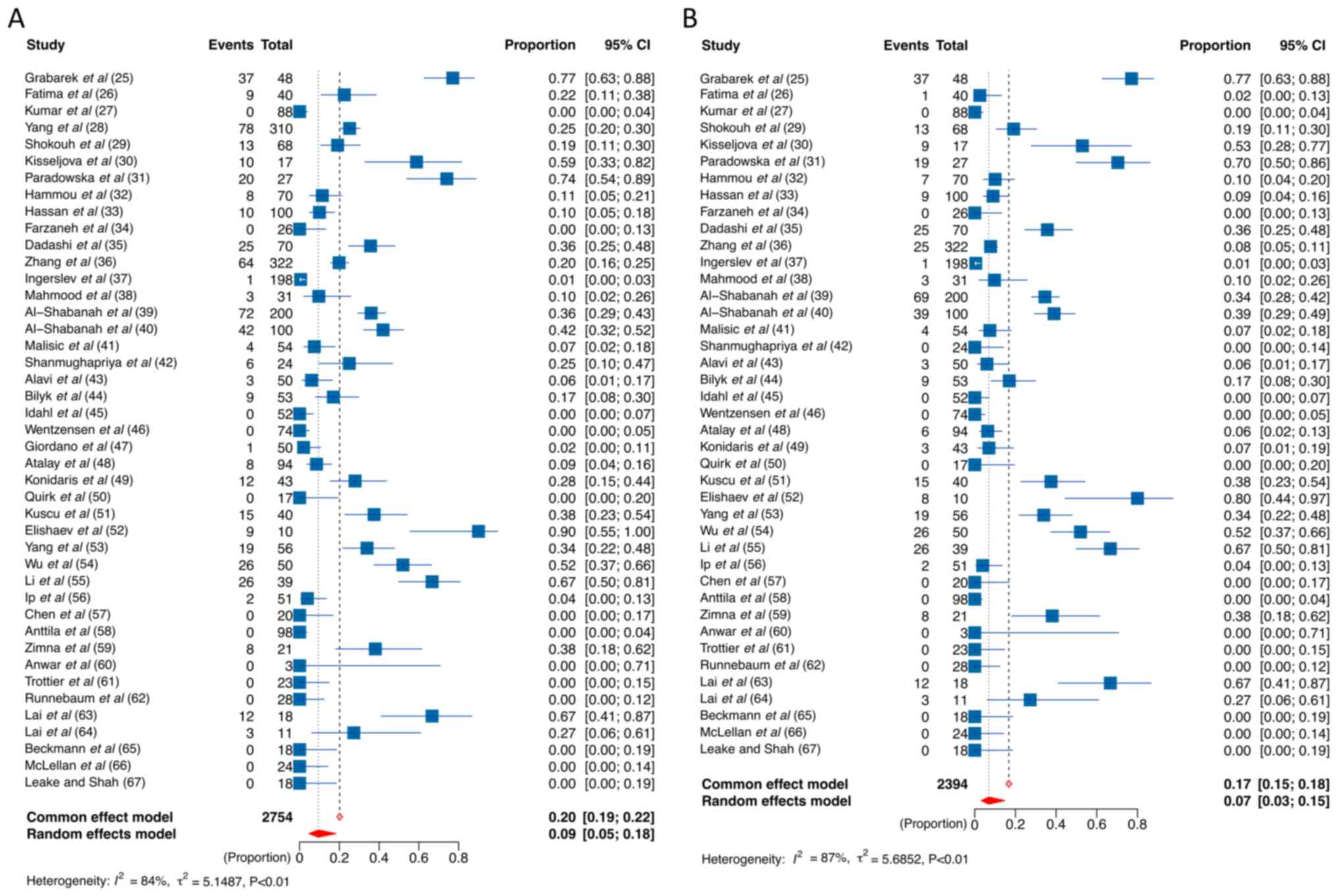
Forest plots of the 43 studies (Fig. 2) show the prevalence of HPV in OC.
The pooled prevalence of all HPV genotypes and HPV 16/18 in OC were
20 and 17% (fixed-effect model) and 10 and 7% (random-effect
model), respectively. To gain deeper insights into the relationship
between HPV and OC, we conducted more subgroup meta-regression
analyses, including histologic types and ethnic groups.
Regarding histopathological types, serous OC, on the
one hand, exhibited a significantly higher prevalence of HPV 16/18
positivity, approximately doubling that of non-serous OC (4% vs.
2%) as indicated by a random-effect model (Table II). On the other hand, positivity
prevalence for all HPV genotypes was 6 and 5% in serous and
non-serous OC, respectively (Table
II).
| Table II.HPV prevalence in selected studies
and subgroups. |
Table II.
HPV prevalence in selected studies
and subgroups.
|
|
| No. of
patients | Pooled HPV
prevalence |
|
|
|---|
|
|
|
|
|
|
|
|---|
| Variable | No. of included
studies | Summed events | Summed total | Fixed effect model
(95% CI) | Random effects
model (95% CI) | I2 | P-value (Cochrane
Q-test) |
|---|
| Ovarian cancer (all
cases) |
|
|
|
|
|
|
|
| HPV
16/18 | 41 | 401 | 2,394 | 0.17
(0.15–0.18) | 0.07
(0.03–0.15) | 86.8 | <0.0001 |
| All
genotypes | 43 | 555 | 2,754 | 0.20
(0.19–0.22) | 0.10
(0.05–0.18) | 83.8 | <0.0001 |
| Ovarian cancer by
pathological types |
|
|
|
|
|
|
|
| HPV
16/18 |
|
|
|
|
|
|
|
|
Serous | 25 | 75 | 791 | 0.09
(0.08–0.12) | 0.04
(0.01–0.13) | 72.9 | <0.0001 |
|
Non-serous | 23 | 38 | 434 | 0.09
(0.06–0.12) | 0.02
(0.01–0.12) | 12.5 | <0.0001 |
| HPV
(all genotypes) |
|
|
|
|
|
|
|
|
Serous | 26 | 86 | 791 | 0.11
(0.09–0.13) | 0.06
(0.02–0.16) | 74.5 | <0.0001 |
|
Non-serous | 24 | 47 | 459 | 0.10
(0.08–0.13) | 0.05
(0.01–0.16) | 24.0 | <0.0001 |
| Subgroup by
region |
|
|
|
|
|
|
|
| HPV
16/18 |
|
|
|
|
|
|
|
|
Asia | 20 | 287 | 1,381 | 0.21
(0.19–0.23) | 0.14
(0.07–0.26) | 88.6 | <0.0001 |
|
Europe | 12 | 90 | 713 | 0.13
(0.10–0.15) | 0.05
(0.01–0.26) | 88.5 | <0.0001 |
| HPV
(all genotypes) |
|
|
|
|
|
|
|
|
Asia | 21 | 426 | 1,691 | 0.25
(0.23–0.27) | 0.20
(0.12–0.32) | 83.3 | <0.0001 |
|
Europe | 13 | 102 | 763 | 0.13
(0.11–0.16) | 0.05
(0.01–0.26) | 88.0 | <0.0001 |
When considering the effect of regional factors on
HPV prevalence, variations in HPV status were observed across
geographic regions. Although the test for subgroup difference using
a meta-regression model did not yield statistical significance,
Asian countries showed a considerably higher HPV prevalence in OC
than European countries. Specifically, the prevalence of HPV across
all genotypes in Asian countries was 20% compared with 5% in
European countries. Moreover, the HPV 16/18 positivity was 14% in
Asian countries compared with 5% in European countries (Table II; Figs. S1 and S2).
Unfortunately, owing to the limited number of
studies from other regions (only two studies from Africa and seven
from North America), a meta-regression could not be conducted.
Nonetheless, these figures remain notably higher than the HPV
prevalence in the control group, which stands at 3 and 2% for all
HPV genotypes and HPV 16/18, respectively, as determined by the
random-effect model (Table
SII).
HPV status in the case-control
analysis
In our case-control analysis, 19 studies, including
1,071 OC samples in contrast to 906 samples of normal or benign
ovarian tissues, were obtained. The study by Li et al
(55) was excluded from our
analysis because it used blood as a control sample instead of
ovarian tissues. The control groups in the selected studies ranged
from women without ovarian diseases [Shokouh et al (29); Paradowska et al (31); Zhang et al (36); Shanmughapriya et al (42); Alavi et al (43); Konidaris et al (49); Ip et al (56); Trottier et al (61); Lai et al (63); Leake et al (67)], benign ovarian tumors [Grabarek
et al (25); Farzaneh et
al (34); Dadashi et al
(35); Mahmood et al
(38); Idahl et al (45); Kuscu et al (51); Quirk et al (50); Wu et al (54)], or adjacent normal ovarian tissues
[Al-Shabanah et al (40)].
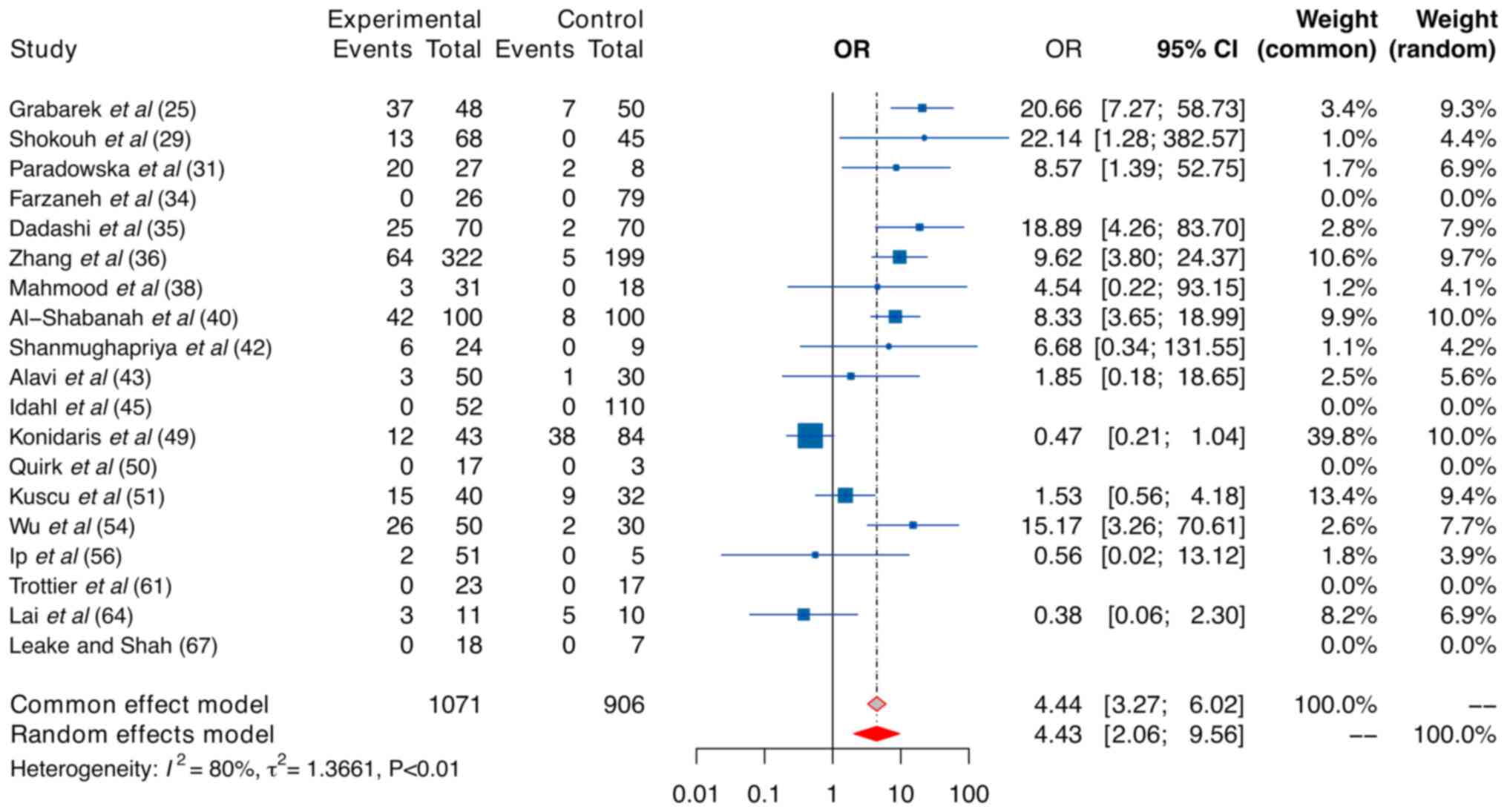
The findings of our case-control analysis regarding
all HPV genotypes are presented in Fig.
3. In our investigation, a significant risk associated with OC
was found in the context of HPV infection, reflected in fixed- and
random-effect size ORs of 4.44 (95% CI, 3.27–6.02) and 4.43 (95%
CI, 2.06–9.56), respectively. Importantly, owing to the high level
of heterogeneity indicated by a sample I2 of 80% and
P-value of <0.01, the random model should be considered a more
appropriate choice for our case-control analysis. In addition, our
analysis using the random-effect model revealed that the pooled
proportion of all HPV genotypes in the case group was 18%.
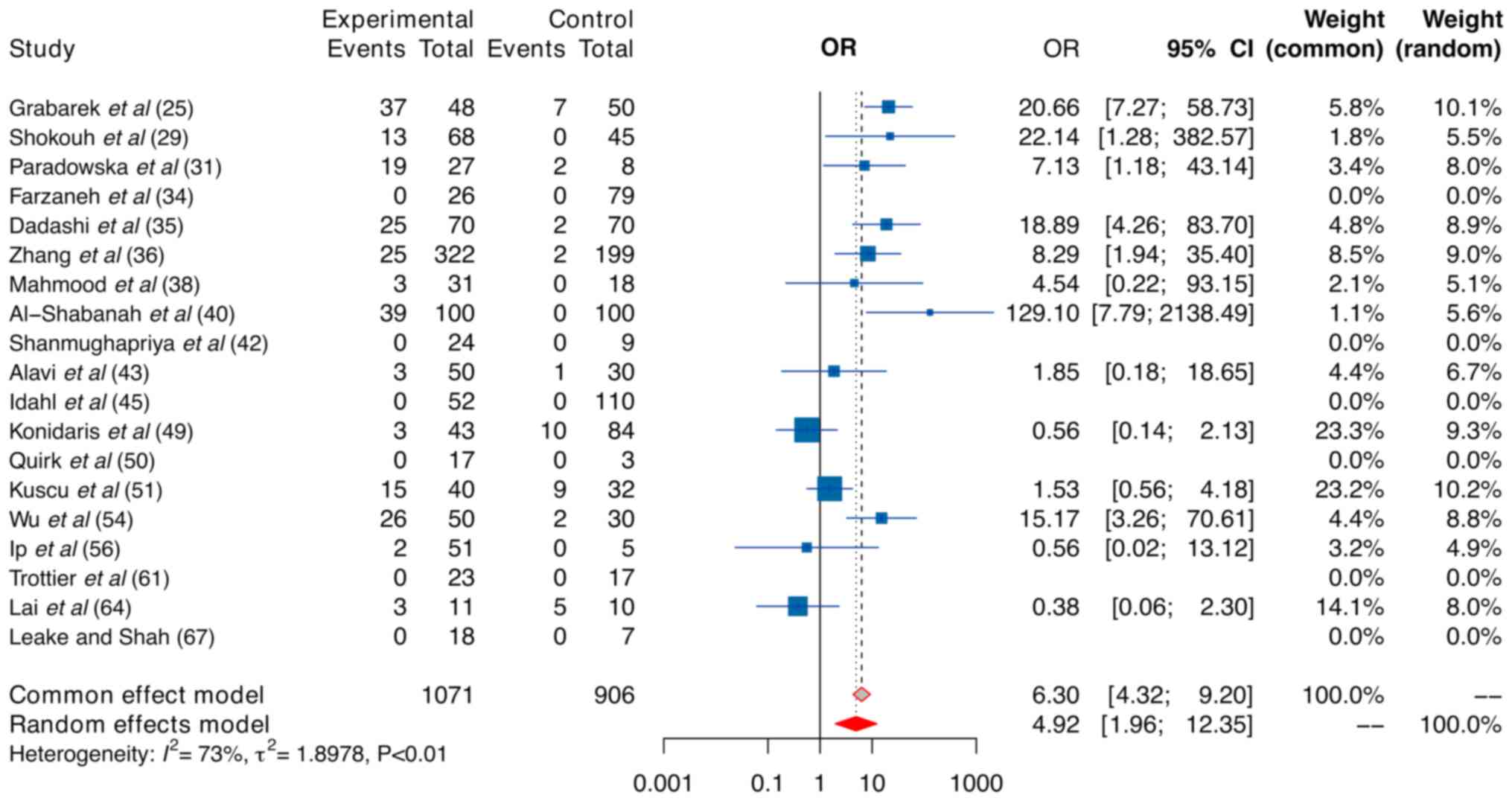
In light of exploring the sources of heterogeneity,
a subgroup analysis was conducted by considering HPV 16/18 and
different regions. When examining the subgroup related to HPV
16/18, HPV 16/18 was strongly linked to a heightened risk. Both the
fixed- and random-effect models produced ORs of 6.30 and 4.92
(Fig. 4), respectively, which were
higher than those of all HPV genotypes (4.44 and 4.43),
respectively. As anticipated, the pooled prevalence of HPV 16/18 in
the case group was considerably high, reaching 13% when using the
random-effect model.
As heterogeneity persisted after subgrouping by HPV
16/18 (I2=73%, P-value <0.01), further subgrouping by
regions was conducted. Due to the limited sample size from North
America and Africa, patients were categorized into Asian (n=12
studies) and non-Asian (n=8 studies) groups. Heterogeneity
decreased to less than 67% in Asian subgroups (Table III). HPV infection, particularly
HPV 16/18, emerged as a more substantial risk factor for OC among
Asian women compared to those from other regions (Asia vs.
non-Asia: 4.75 vs. 4.13 for all HPV genotypes, and 5.12 vs. 4.40
for HPV 16/18). Despite the observed trend, the test for
differences was not statistically significant.
| Table III.Regional subgroup analysis: Asian vs.
non-Asian countries. |
Table III.
Regional subgroup analysis: Asian vs.
non-Asian countries.
|
|
| Case group | Control group |
|
|
|
|
|---|
|
|
|
|
| Random effects
model OR (95% CI) | P-value
(meta-regression) | I2 | P-value (Cochrane
Q-test) |
|---|
| Subgroups | No. of studies | Summed events | Summed total | Summed events | Summed total |
|---|
| HPV (all
genotypes) |
|
|
|
|
|
|
|
|
|
|
Asia | 12 | 202 | 422 | 32 | 176 | 4.75
(2.15–10.49) | 0.91 | 60.2 | 0.0051 |
|
Non-Asia | 7 | 69 | 228 | 47 | 279 | 4.13
(0.42–40.90) |
| 94.2 | <0.0001 |
| HPV 16/18 |
|
|
|
|
|
|
|
|
|
|
Asia | 12 | 154 | 843 | 21 | 627 | 5.12
(1.74–15.06) | 0.90 | 66.9 | 0.0013 |
|
Non-Asia | 7 | 59 | 228 | 19 | 279 | 4.40
(0.52–37.19) |
| 88.5 | 0.0002 |
Publication bias
In our meta-analysis, publication bias was assessed
using funnel plots and tests for asymmetry (Figs. 5 and 6; Tables
SIII and SIV). Accordingly,
the selected studies that were used to investigate the prevalence
of all HPV genotypes and HPV 16/18 in OC displayed no substantial
indications of significant asymmetry. Moreover, the results from
Begg's, Egger's, and Peter's tests collectively confirmed the
absence of significant publication bias.
Discussion
HR-HPV is a well-known etiological factor in
anogenital and oropharyngeal cancers (79–82).
Recently, interest in the prevalence of HPV, particularly HPV
16/18, and its potential role in OC has grown. HPV may reach EOC
through: (1) anatomical continuity
with endocervical glands, where the endometrium and fallopian tubes
extend from the endocervical glands, allowing infection to spread.
The fallopian tube's fimbriae are close to the ovarian surface
(27); 2) sperm-mediated
transmission, where sperm facilitate this by absorbing HPV DNA and
transmitting the virus to reproductive system cells, and also serve
as virus carriers during their passage through the endocervical
canal, potentially reaching the ovarian cortex after ovulation
(83).
In the context of HPV infection, integration into
the human genome produces oncoproteins such as E6 and E7, crucial
in initiating cancer, including EOC. E6 degrades p53, suppressing
viral DNA synthesis and enhancing telomerase activity to evade
senescence (21), while E7 disrupts
retinoblastoma protein function, overriding p21-mediated growth
arrest and increasing p16 for cell immortalization (22,84).
Remarkably, over half of EOCs exhibit p53 and RB pathway mutations,
with serous carcinomas representing 40% of cases (85). HPV infection leads to the emergence
of HPV-related lesions over time. Interestingly, the precursor
lesions for EOC, including serous tubal intraepithelial carcinoma
and p53 signature, are widely accepted to originate within the
fallopian tubes at the fimbriated end because of their proximity to
these structures (10). Naturally,
while some lesions transition into a quiescent state, others
continue to proliferate, contributing to cancer development through
genomic instability, telomere maintenance, and immune cell
responses (10,11,13).
Given these considerations, HPV prevalence in OC may
exhibit a substantial effect, akin to what has been observed in
cervical cancer. In line with this, our meta-analysis, which
consolidated data from 43 studies involving a total of 2,754
patients, unveiled a significant correlation between the prevalence
of HPV (specifically HPV 16/18) and the risk of OC.
In our proportional meta-analysis, the overall
pooled HPV prevalence was approximately 20% for all genotypes and
17% for the high-risk genotypes HPV 16/18 using a fixed-effect
model. However, when employing the random-effect model, lower
prevalence, with all HPV genotypes at 10% and HPV 16/18 at 7%, was
obtained. In studies designed as case-control investigations, a
higher pooled prevalence of HPV for all genotypes was found at 17%
and HPV 16/18 at 13% using the random-effect model. Owing to the
substantial heterogeneity across the studies, the random-effect
model was considered more appropriate.
In addition, our meta-analysis considered variations
in HPV prevalence among different regions. Asian countries
exhibited higher HPV prevalence in OC than European countries. This
regional disparity may be due to differences in healthcare
practices, genetic factors, or environmental influences. The
limited number of studies from Africa and North America prevented a
comprehensive regional analysis, highlighting the need for more
research in these regions to understand the disparities better.
This study further substantiated the role of HPV in
OC risk through a comparative analysis. Accordingly, HPV 16/18
demonstrated a stronger association with OC than all HPV genotypes,
particularly in Asian countries (with respective ORs of 5.12 (95%
CI, 1.74–15.06) and 4.75 (95% CI, 2.15–10.49)). This finding
emphasized the importance of recognizing specific HPV genotypes
that may carry a higher risk for OC development and the role of
geographical and host genetic factors in influencing susceptibility
to HPV infection.
In comparison to two existing meta-analyses, Cherif
et al (23) analyzed 29
studies involving 2,280 OC cases and reported a pooled HPV
proportion of 15.9% (95% CI, 11–22), while Ibragimova et al
(24) included 14 case-control
studies with 1,163 ovarian tumor samples and 738 normal ovarian
tissue samples, showing a relative risk of 2.68 (95% CI,
1.97–3.64). Despite similarities in search strategy with the
previous study (23), our study's
larger and more recent dataset (43 studies vs. 29 studies, 2,754
patients vs. 2,280 patients) allows for more comprehensive subgroup
analyses, revealing significant variations in HPV 16/18 prevalence
across histologic types and ethnic groups. This approach offers a
deeper understanding of HPV's impact on OC, addressing gaps in
previous research. We observed a similar OC risk related to HPV
infection with a random-effects size OR of 4.43, but a lower pooled
prevalence of HPV (10%). However, the HPV proportion in
case-control studies was comparable (17% vs. 15.9%). In the case of
HPV 16/18, these two meta-analyses calculated the proportion among
HPV-positive studies, which differed from our approach of
calculating HPV 16/18 prevalence across all studies. Our approach
not only allows us to better demonstrate the predominance of HPV
16/18 among HPV genotypes in OC but also to mitigate the potential
bias that arises from certain studies focusing solely on HPV 16/18,
which can inflate the proportion of these two genotypes. As
expected, this study effectively highlighted the association of HPV
16/18 in OC. Although the prevalence of HPV 16/18 (7%) was lower
than that of all HPV genotypes (10%), the OR for HPV 16/18 was
higher than that for all HPV genotypes (4.92 vs. 4.43).
The prevalence of HPV 16/18 in OC (7.0%) was lower
than that of HPV 16/18 in women with uterine cervical lesions.
According to the latest data from the ICO/IARC Information Centre
on HPV and Cancer (2023), the worldwide incidence rates of HPV are
3.9, 25.8, 51.9, and 69.4% in normal cytology, low-grade lesions,
high-grade lesions, and cervical cancer, respectively (86). This difference may arise from
variations in sample type, as our data exclusively assessed the
presence of HPV in OC tissue.
Publication bias is a potential concern in
meta-analyses. However, the lack of significant asymmetry in the
funnel plot and the results of Begg's, Egger's, and Peter's tests
suggest that publication bias is not a significant issue in this
study, thereby strengthening the credibility of the findings.
This study has several limitations. Firstly, the
data availability was limited to regions outside Asia and Europe,
which may restrict the comprehensiveness of our meta-analysis.
Secondly, we only included studies published in English,
potentially excluding important findings from non-English
literature. Moreover, the absence of data on high-grade serous OC,
especially in case-control studies, highlights a significant
knowledge gap regarding HPV's role in this particular subtype.
Additionally, further research, including well-designed and
multi-ethnic epidemiological studies or prospective cohort studies,
can provide stronger evidence of the causal relationship and
underlying mechanisms between HPV and ovarian cancer.
In conclusion, this meta-analysis provides evidence
of a significant association between HPV infection and OC risk,
particularly in Asian countries. The high prevalence of HPV,
particularly HPV 16/18, in OC cases highlights the imperative need
for further in-depth research to elucidate the underlying
mechanisms governing this association. Furthermore, a comprehensive
understanding of the role and intricate interplay between HPV
infections and this cancer can be crucial for early detection and
prevention efforts.
Supplementary Material
Supporting Data
Supporting Data
Acknowledgements
Not applicable.
Funding
This research was supported by a grant of the Korea Health
Technology R&D Project through the Korea Health Industry
Development Institute, funded by the Ministry of Health &
Welfare, Republic of Korea (grant no. HI23C0515), and the National
Research Foundation of Korea (grant no. NRF-2021R1A5A202161).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
IS, GOC and HSH contributed to conception and
design. IS, TML and HDTN were involved in the acquisition and
analysis of data. HSH, GOC, IS, JC and NJYP were involved in the
interpretation of data. IS, TML and HDTN were involved in
visualization. TML wrote the original draft. GOC, IS, HSH, HDTN, JC
and NJYP revised the manuscript critically for important
intellectual content. IS and GOC confirm the authenticity of all
the raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
HPV
|
human papillomavirus
|
|
OC
|
ovarian cancer
|
|
EOC
|
epithelial ovarian cancer
|
|
HR-HPV
|
high-risk human papillomavirus
|
|
OR
|
odds ratio
|
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ghose A, Bolina A, Mahajan I, Raza SA,
Clarke M, Pal A, Sanchez E, Rallis KS and Boussios S: Hereditary
ovarian cancer: Towards a cost-effective prevention strategy. Int J
Environ Res Public Health. 19:120572022. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lõhmussaar K, Kopper O, Korving J, Begthel
H, Vreuls CPH, van Es JH and Clevers H: Assessing the origin of
high-grade serous ovarian cancer using CRISPR-modification of mouse
organoids. Nat Commun. 11:26602020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Maringe C, Walters S, Butler J, Coleman
MP, Hacker N, Hanna L, Mosgaard BJ, Nordin A, Rosen B, Engholm G,
et al: Stage at diagnosis and ovarian cancer survival: Evidence
from the international cancer benchmarking partnership. Gynecol
Oncol. 127:75–82. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ghose A, McCann L, Makker S, Mukherjee U,
Gullapalli SVN, Erekkath J, Shih S, Mahajan I, Sanchez E, Uccello
M, et al: Diagnostic biomarkers in ovarian cancer: Advances beyond
CA125 and HE4. Ther Adv Med Oncol. 16:175883592412332252024.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Saani I, Raj N, Sood R, Ansari S,
Mandviwala HA, Sanchez E and Boussios S: Clinical challenges in the
management of malignant ovarian germ cell tumours. Int J Environ
Res Public Health. 20:60892023. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Singh N: WHO classification of tumors of
the ovary. In: Encyclopedia of Pathology. Van Krieken JHJM:
Springer International Publishing; Cham: pp. 1–4. 2022
|
|
8
|
Matulonis UA, Sood AK, Fallowfield L,
Howitt BE, Sehouli J and Karlan BY: Ovarian cancer. Nat Rev Dis
Primers. 2:160612016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pavlidis N, Rassy E, Vermorken JB, Assi T,
Kattan J, Boussios S and Smith-Gagen J: The outcome of patients
with serous papillary peritoneal cancer, fallopian tube cancer, and
epithelial ovarian cancer by treatment eras: 27 years data from the
SEER registry. Cancer Epidemiol. 75:1020452021. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kindelberger DW, Lee Y, Miron A, Hirsch
MS, Feltmate C, Medeiros F, Callahan MJ, Garner EO, Gordon RW,
Birch C, et al: Intraepithelial carcinoma of the fimbria and pelvic
serous carcinoma: Evidence for a causal relationship. Am J Surg
Pathol. 31:161–169. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shih IM, Wang Y and Wang TL: The origin of
ovarian cancer species and precancerous landscape. Am J Pathol.
191:26–39. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Aliyuda F, Moschetta M, Ghose A, Sofia
Rallis K, Sheriff M, Sanchez E, Rassy E and Boussios S: Advances in
ovarian cancer treatment beyond PARP Inhibitors. Curr Cancer Drug
Targets. 23:433–446. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lee Y, Miron A, Drapkin R, Nucci MR,
Medeiros F, Saleemuddin A, Garber J, Birch C, Mou H, Gordon RW, et
al: A candidate precursor to serous carcinoma that originates in
the distal fallopian tube. J Pathol. 211:26–35. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Colvin EK and Howell VM: Why the dual
origins of high grade serous ovarian cancer matter. Nat Commun.
11:12002020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Greten FR and Grivennikov SI: Inflammation
and cancer: Triggers, mechanisms, and consequences. Immunity.
51:27–41. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Łaniewski P, Ilhan ZE and Herbst-Kralovetz
MM: The microbiome and gynaecological cancer development,
prevention and therapy. Nat Rev Urol. 17:232–250. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chambers LM, Bussies P, Vargas R, Esakov
E, Tewari S, Reizes O and Michener C: The microbiome and
gynecologic cancer: Current evidence and future opportunities. Curr
Oncol Rep. 23:922021. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jia D, Nagaoka Y, Katsumata M and Orsulic
S: Inflammation is a key contributor to ovarian cancer cell
seeding. Sci Rep. 8:123942018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sabatini ME and Chiocca S: Human
papillomavirus as a driver of head and neck cancers. Br J Cancer.
122:306–314. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Demarco M, Hyun N, Carter-Pokras O,
Raine-Bennett TR, Cheung L, Chen X, Hammer A, Campos N, Kinney W,
Gage JC, et al: A study of type-specific HPV natural history and
implications for contemporary cervical cancer screening programs.
EClinicalMedicine. 22:1002932020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Scheffner M, Werness BA, Huibregtse JM,
Levine AJ and Howley PM: The E6 oncoprotein encoded by human
papillomavirus types 16 and 18 promotes the degradation of p53.
Cell. 63:1129–1136. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fischer M, Uxa S, Stanko C, Magin TM and
Engeland K: Human papilloma virus E7 oncoprotein abrogates the
p53-p21-DREAM pathway. Sci Rep. 7:26032017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cherif S, Amine A, Thies S, Taube ET,
Braicu EI, Sehouli J and Kaufmann AM: Prevalence of human
papillomavirus detection in ovarian cancer: A meta-analysis. Eur J
Clin Microbiol Infect Dis. 40:1791–1802. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ibragimova MK, Kokorina EV, Tsyganov MM,
Churuksaeva ON and Litviakov NV: Human papillomavirus and ovarian
cancer (review of literature and meta-analysis). Infect Genet Evol.
95:1050862021. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Grabarek BO, Ossowski P, Czarniecka J,
Ożóg M, Prucnal J, Dziuba I, Ostenda A, Dziobek K, Boroń D, Peszek
W, et al: Detection and genotyping of human papillomavirus
(HPV16/18), Epstein-barr virus (EBV), and human cytomegalovirus
(HCMV) in endometrial endometroid and ovarian cancers. Pathogens.
12:3972023. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fatima B, Masud R, Sultana N, Javed A and
Justin S: Detection of human papillomavirus in archival bladder and
ovarian cancer samples. Clin Epidemiology Glob Health.
22:1013392023. View Article : Google Scholar
|
|
27
|
Kumar P, Ranmale S, Tongaonkar H, Mehta S
and Mania-Pramanik J: Human papillomavirus infection: Is it
associated with epithelial ovarian cancer? Indian J Med Microbiol.
39:311–314. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yang X, You Q, Yao G, Geng J, Ma R and
Meng H: Evaluation of p16 in epithelial ovarian cancer for a
10-year study in northeast China: Significance of HPV in
correlation with PD-L1 expression. Cancer Manag Res. 12:6747–6753.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Shokouh MR, Safaei A, Moattari A and
Sarvari J: Association of human papilloma virus and Epstein-barr
virus with ovarian cancer in Shiraz, southwestern Iran. Iran J
Pathol. 15:292–298. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kisseljova N, Zhordania K, Fedorova M,
Katargin A, Valeeva A, Pajanidi J, Pavlova L, Khvan O and
Vinokurova S: Detection of human papillomavirus prevalence in
ovarian cancer by different test systems. Intervirology.
62:198–204. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Paradowska E, Jabłońska A, Studzińska M,
Wilczyński M and Wilczyński JR: Detection and genotyping of CMV and
HPV in tumors and fallopian tubes from epithelial ovarian cancer
patients. Sci Rep. 9:199352019. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hammou RA, Benhessou M, Bouziyane A,
Hassou N, Benhchekroun MN, Bessi H and Ennaji MM: Oncogenic human
papillomavirus involvement in epithelial ovarian carcinoma among
women in Morocco. Bioinformation. 15:55–60. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hassan ZK, Hafez MM, Kamel MM and Zekri
ARN: Human Papillomavirus genotypes and methylation of CADM1, PAX1,
MAL and ADCYAP1 genes in epithelial ovarian cancer patients. Asian
Pac J Cancer Prev. 18:169–176. 2017.PubMed/NCBI
|
|
34
|
Farzaneh F, Nadji SA, Khosravi D, Hosseini
MS, Hashemi Bahremani M, Chehrazi M, Bagheri G, Sigaroodi A and
Haghighatian Z: Lack of HPV in benign and malignant epithelial
ovarian tumors in Iran. Asian Pac J Cancer Prev. 18:1233–1236.
2017.PubMed/NCBI
|
|
35
|
Dadashi M, Eslami G, Faghihloo E,
Pourmohammad A, Hosseini J, Taheripanah R and Arab-Mazar Z:
Detection of human papilloma virus type 16 in epithelial ovarian
tumors samples. Arch Clin Infect Dis. 12:e396662017.
|
|
36
|
Zhang PP, Zhou L, Cao JS, Li YP, Zeng Z,
Sun N, Shen L, Zhu HY, Ruan Y, Zha WT, et al: Possible epithelial
ovarian cancer association with HPV18 or HPV33 infection. Asian Pac
J Cancer Prev. 17:2959–2964. 2016.PubMed/NCBI
|
|
37
|
Ingerslev K, Hogdall E, Skovrider-Ruminski
W, Schnack TH, Karlsen MA, Nedergaard L, Hogdall C and Blaakær J:
High-risk HPV is not associated with epithelial ovarian cancer in a
Caucasian population. Infect Agent Cancer. 11:392016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Mahmood FM, Kadhim HS and Mousa Al Khuzaee
LR: Detection of human papillomavirus-16 E6-oncoprotein in
epithelial ovarian tumors samples of Iraqi patients. Jundishapur J
Microbiol. 7:e119452014.PubMed/NCBI
|
|
39
|
Al-Shabanah OA, Hafez MM, Hassan ZK,
Sayed-Ahmed MM, Abozeed WN, Alsheikh A and Al-Rejaie SS:
Methylation of SFRPs and APC genes in ovarian cancer infected with
high risk human papillomavirus. Asian Pac J Cancer Prev.
15:2719–2725. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Al-Shabanah OA, Hafez MM, Hassan ZK,
Sayed-Ahmed MM, Abozeed WN, Al-Rejaie SS and Alsheikh AA: Human
papillomavirus genotyping and integration in ovarian cancer Saudi
patients. Virol J. 10:3432013. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Malisic E, Jankovic R and Jakovljevic K:
Detection and genotyping of human papillomaviruses and their role
in the development of ovarian carcinomas. Arch Gynecol Obstet.
286:723–728. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Shanmughapriya S, SenthilKumar G,
Vinodhini K, Das BC, Vasanthi N and Natarajaseenivasan K: Viral and
bacterial aetiologies of epithelial ovarian cancer. Eur J Clin
Microbiol Infect Dis. 31:2311–2317. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Alavi G, Sharifi N, Sadeghian A, Rezaei A
and Shidaee H: Failure to demonstrate the role of high risk human
papilloma virus in epithelial ovarian cancer. Iran J Pathol.
7:151–156. 2012.
|
|
44
|
Bilyk OO, Pande NT and Buchynska LG:
Analysis of P53, P16INK4A, PRB and Cyclin D1 expression and human
papillomavirus in primary ovarian serous carcinomas. Exp Oncol.
33:150–156. 2011.PubMed/NCBI
|
|
45
|
Idahl A, Lundin E, Elgh F, Jurstrand M,
Møller JK, Marklund I, Lindgren P and Ottander U: Chlamydia
trachomatis, Mycoplasma genitalium, Neisseria gonorrhoeae, human
papillomavirus, and polyomavirus are not detectable in human tissue
with epithelial ovarian cancer, borderline tumor, or benign
conditions. Am J Obstet Gynecol. 202:71.e1–e6. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Wentzensen N, du Bois A, Kommoss S,
Pfisterer J, Von Knebel Doeberitz M, Schmidt D and Kommoss F: No
metastatic cervical adenocarcinomas in a series of
p16INK4a-positive mucinous or endometrioid advanced ovarian
carcinomas: An analysis of the AGO ovarian cancer study group. Int
J Gynecol Pathol. 27:18–23. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Giordano G, D'Adda T, Gnetti L, Froio E,
Merisio C and Melpignano M: Role of human papillomavirus in the
development of epithelial ovarian neoplasms in Italian women. J
Obstet Gynaecol. 34:210–217. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Atalay F, Taskiran C, Taner MZ, Pak I, Or
M and Tuncer S: Detection of human papillomavirus DNA and
genotyping in patients with epithelial ovarian carcinoma. J Obstet
Gynaecol. 33:823–828. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Konidaris S, Kouskouni EE, Panoskaltsis T,
Kreatsas G, Patsouris ES, Sarivalassis A, Nonni A and Lazaris AC:
Human papillomavirus infection in malignant and benign
gynaecological conditions: A study in Greek women. Health Care
Women Int. 28:182–191. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Quirk JT, Kupinski JM and DiCioccio RA:
Analysis of ovarian tumors for the presence of human papillomavirus
DNA. J Obstet Gynaecol. 32:202–205. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Kuscu E, Ozdemir BH, Erkanli S and Haberal
A: HPV and p53 expression in epithelial ovarian carcinoma. Eur J
Gynaecol Oncol. 26:642–645. 2005.PubMed/NCBI
|
|
52
|
Elishaev E, Gilks CB, Miller D, Srodon M,
Kurman RJ and Ronnett BM: Synchronous and metachronous endocervical
and ovarian neoplasms: Evidence supporting interpretation of the
ovarian neoplasms as metastatic endocervical adenocarcinomas
simulating primary ovarian surface epithelial neoplasms. Am J Surg
Pathol. 29:281–294. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Yang HJ, Liu VW, Tsang PC, Yip AM, Ng TY,
Cheung AN and Ngan HY: Comparison of human papillomavirus DNA
levels in gynecological cancers: Implication for cancer
development. Tumor Biol. 24:310–316. 2003. View Article : Google Scholar
|
|
54
|
Wu QJ, Guo M, Lu ZM, Li T, Qiao HZ and Ke
Y: Detection of human papillomavirus-16 in ovarian malignancy. Br J
Cancer. 89:672–675. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Li T, Lu ZM, Guo M, Wu QJ, Chen KN, Xing
HP, Mei Q and Ke Y: p53 codon 72 polymorphism (C/G) and the risk of
human papillomavirus-associated carcinomas in China. Cancer.
95:2571–2576. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Ip SM, Wong LC, Xu CM, Cheung AN, Tsang PC
and Ngan HY: Detection of human papillomavirus DNA in malignant
lesions from Chinese women with carcinomas of the upper genital
tract. Gynecol Oncol. 87:104–111. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Chen TR, Chan PJ, Seraj IM and King A:
Absence of human papillomavirus E6-E7 transforming genes from HPV
16 and 18 in malignant ovarian carcinoma. Gynecol Oncol.
72:180–182. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Anttila M, Syrjänen S, Ji H, Saarikoski S
and Syrjänen K: Failure to demonstrate human papillomavirus DNA in
epithelial ovarian cancer by general primer PCR. Gynecol Oncol.
72:337–341. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Zimna K, Poreba E, Kedzia W,
Gozdzicka-Józefiak A and Kezia H: Human papillomavirus (HPV) in
upper genital tract carcinomas of women. Eur J Gynaecol Oncol.
18:415–417. 1997.PubMed/NCBI
|
|
60
|
Anwar K, Nakakuki K, Imai H, Shiraishi T
and Inuzuka M: Infection of human papillomavirus (HPV) and p53
over-expression in human female genital tract carcinoma. J Pak Med
Assoc. 46:220–224. 1996.PubMed/NCBI
|
|
61
|
Trottier AM, Provencher D, Mes-Masson AM,
Vauclair R and Coutlée F: Absence of human papillomavirus sequences
in ovarian pathologies. J Clin Microbiol. 33:1011–1013. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Runnebaum IB, Maier S, Tong XW, Rosenthal
HE, Möbus VJ, Kieback DG and Kreienberg R: Human papillomavirus
integration is not associated with advanced epithelial ovarian
cancer in German patients. Cancer Epidemiol Biomarkers Prev.
4:573–575. 1995.PubMed/NCBI
|
|
63
|
Lai CH, Wang CY, Lin CY and Pao CC:
Detection of human papillomavirus RNA in ovarian and endometrial
carcinomas by reverse transcription/polymerase chain reaction.
Gynecol Obstet Invest. 38:276–280. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Lai CH, Hsueh S, Lin CY, Huang MY, You GB,
Chang HC and Pao CC: Human papillomavirus in benign and malignant
ovarian and endometrial tissues. Int J Gynecol Pathol. 11:210–215.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Beckmann AM, Sherman KJ, Saran L and Weiss
NS: Genital-type human papillomavirus infection is not associated
with surface epithelial ovarian carcinoma. Gynecol Oncol.
43:247–251. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
McLellan R, Buscema J, Guerrero E, Shah
KV, Woodruff JD and Currie JL: Investigation of ovarian neoplasia
of low malignant potential for human papillomavirus. Gynecol Oncol.
38:383–385. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Leake JF, Woodruff JD, Searle C, Daniel R,
Shah KV and Currie JL: Human papillomavirus and epithelial ovarian
neoplasia. Gynecol Oncol. 34:263–273. 1989. View Article : Google Scholar
|
|
68
|
Nikolakopoulou A, Mavridis D and Salanti
G: Demystifying fixed and random effects meta-analysis. BMJ Ment
Health. 17:53–57. 2014.
|
|
69
|
Schwarzer G: meta: An R package for
meta-analysis. R News. 7:40–45. 2007.
|
|
70
|
Higgins JP and Green S: Cochrane handbook
for systematic reviews of interventions. In: Cochrane Handbook for
Systematic Reviews of Interventions. Wiley; 2019
|
|
71
|
Paule RC and Mandel J: Consensus values
and weighting factors. J Res Natl Bur Stand (1977). 87:377–385.
1982. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Balduzzi S, Rücker G and Schwarzer G: How
to perform a meta-analysis with R: A practical tutorial. Evid Based
Ment Health. 22:153–160. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Sterne JA, Sutton AJ, Ioannidis JP, Terrin
N, Jones DR, Lau J, Carpenter J, Rücker G, Harbord RM, Schmid CH,
et al: Recommendations for examining and interpreting funnel plot
asymmetry in meta-analyses of randomised controlled trials. BMJ.
343:d40022011. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Begg CB and Mazumdar M: Operating
characteristics of a rank correlation test for publication bias.
Biometrics. 50:1088–1101. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Peters JL, Sutton AJ, Jones DR, Abrams KR
and Rushton L: Comparison of two methods to detect publication bias
in meta-analysis. JAMA. 295:676–680. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Viechtbauer W: Conducting meta-analyses in
R with the metafor package. J Stat Soft. 36:1–48. 2010. View Article : Google Scholar
|
|
77
|
R Core Team, . R: A language and
environment for statistical computing. R Foundation for Statistical
Computing; Vienna: 2023
|
|
78
|
Schwarzer G, Carpenter JR and Rücker G:
metasens: Statistical methods for sensitivity analysis in
meta-analysis. R package version 1.5–2. https://CRAN.R-project.org/package=metasens
|
|
79
|
Halec G, Alemany L, Quiros B, Clavero O,
Höfler D, Alejo M, Quint W, Pawlita M, Bosch FX and de Sanjose S:
Biological relevance of human papillomaviruses in vulvar cancer.
Mod Pathol. 30:549–562. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Lechner M, Liu J, Masterson L and Fenton
TR: HPV-associated oropharyngeal cancer: Epidemiology, molecular
biology and clinical management. Nat Rev Clin Oncol. 19:306–327.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Bjørge T, Engeland A, Luostarinen T, Mork
J, Gislefoss RE, Jellum E, Koskela P, Lehtinen M, Pukkala E,
Thoresen SO and Dillner J: Human papillomavirus infection as a risk
factor for anal and perianal skin cancer in a prospective study. Br
J Cancer. 87:61–64. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Cohen PA, Jhingran A, Oaknin A and Denny
L: Cervical cancer. Lancet. 393:169–182. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Chan PJ, Seraj IM, Kalugdan TH and King A:
Evidence for ease of transmission of human papillomavirus DNA from
sperm to cells of the uterus and embryo. J Assist Reprod Genet.
13:516–519. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Dyson N, Howley PM, Münger K and Harlow E:
The human papilloma virus-16 E7 oncoprotein is able to bind to the
retinoblastoma gene product. Science. 243:934–937. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Hashiguchi Y, Tsuda H, Yamamoto K, Inoue
T, Ishiko O and Ogita S: Combined analysis of p53 and RB pathways
in epithelial ovarian cancer. Hum Pathol. 32:988–996. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Bruni L, Albero G, Serrano B, Mena M,
Collado J, Gómez D, Muñoz J, Bosch F and de Sanjosé S: ICO/IARC
Information Centre on HPV and Cancer (HPV Information Centre).
Human papillomavirus and related diseases in the world. Summary
Report 10 March 2023. https://hpvcentre.net/statistics/reports/XWX.pdfOctober
8–2023
|