Introduction
According to the Global Cancer Statistics Report
2022, breast cancer has become the second most common malignancy in
the world and the leading cause of cancer incidence among women,
posing a notable threat to women's health (1). Invasive lobular carcinoma (ILC) is the
second most common histological type of breast cancer, accounting
for ~15% of all cases (2).
Triple-negative ILC (TN-ILC) accounts for 2–9% of ILC cases, with
the majority of cases exhibiting androgen receptor (AR) positivity
(3). Notably, ILC tends to
metastasize to the gastrointestinal tract, peritoneum, soft
meninges and ovaries more often than invasive ductal carcinoma
(4,5). However, gastric metastases are rare;
the reported incidence is 0.06–0.6% (6,7).
Reports in the literature of TN-ILC with gastric metastases at
initial diagnosis are uncommon, and gastric metastases can have
similarities to primary gastric cancer (5,8),
posing a diagnostic challenge.
In the present case report, a rare case of TN-ILC
with gastric metastasis upon initial presentation is described. The
imaging findings and histopathological evidence provide novel
insights into this uncommon metastatic pattern, contributing to the
limited body of knowledge on this clinical scenario.
Case report
Case presentation
A 68-year-old postmenopausal woman presenting with 1
week of chest distress was admitted to Nanjing Gaochun People's
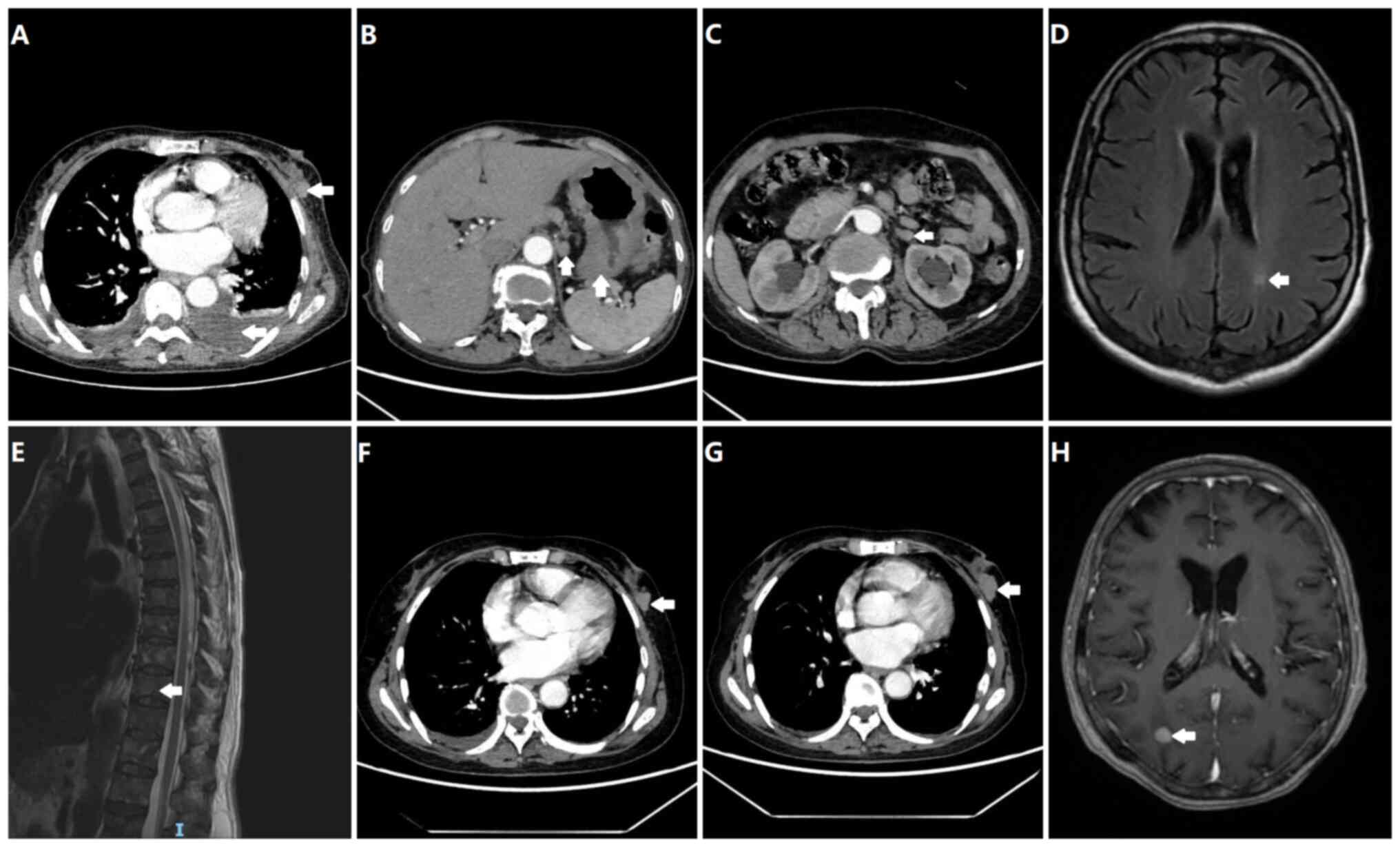
Hospital (Nanjing, China) in February 2024. Initial CT imaging
revealed a 4.0 cm irregular left breast mass (Breast Imaging
Reporting and Data System 5) (9)
with axillary lymphadenopathy, bilateral pleural effusions and
pericardial effusion (Fig. 1A).
Systemic evaluation including CTs and MRIs demonstrated extensive
metastases including gastric wall thickening (Fig. 1B), a left adrenal nodule (Fig. 1C), cerebral enhancing lesions
(Fig. 1D) and osteolytic bone
lesions (Fig. 1E).
Peripheral blood tests showed elevated tumor
markers: CEA 30.12 ng/ml (normal value, ≤5 ng/ml), CA125 321.1 U/ml
(normal value, <35 ng/ml) and CYFRA 21-1 117.5 ng/ml (normal
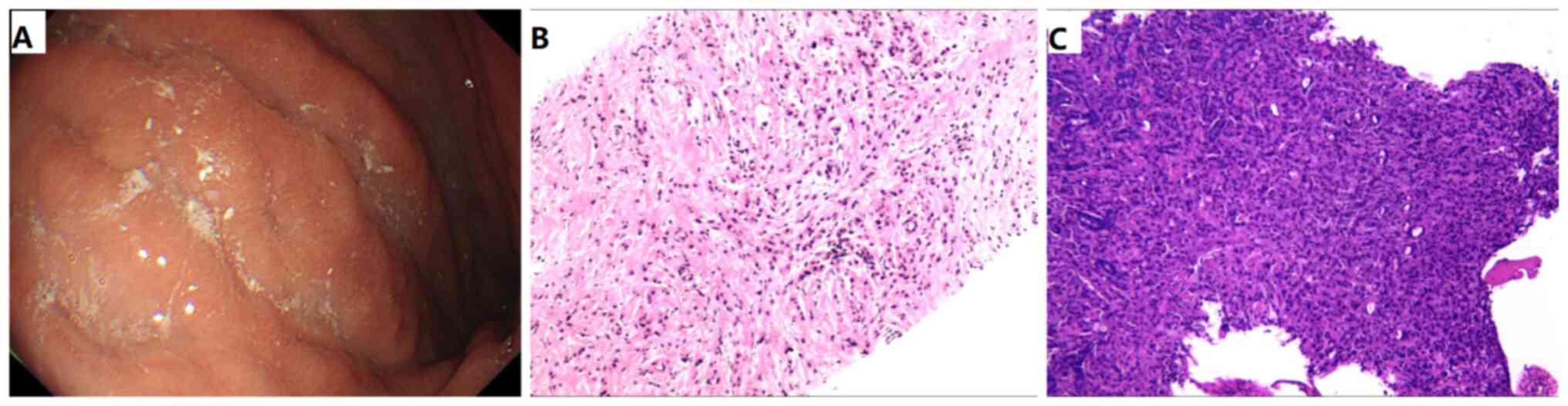
value, <3.3 ng/ml). Gastroscopy revealed superficial atrophic
gastritis, gastric fundus polyp and infiltrative lesion of the
gastric body, as shown in Fig. 2A.
Immunohistochemical analysis of the left breast mass (Fig. 3) revealed estrogen receptor (ER)(−),
progesterone receptor (PR)(−), HER-2(1+), E-cadherin(−), Ki-67(+
with local areas reaching 30%), β-catenin(+), cytokeratin
(CK)5/6(−), CK14(−) and AR(++). Combined with the hematoxylin and
eosin (HE) staining results (Fig.
2B), these findings confirmed classic ILC with a
triple-negative molecular subtype. HE staining of the biopsy of the
gastric lesions showed an adenoid structure and indicated
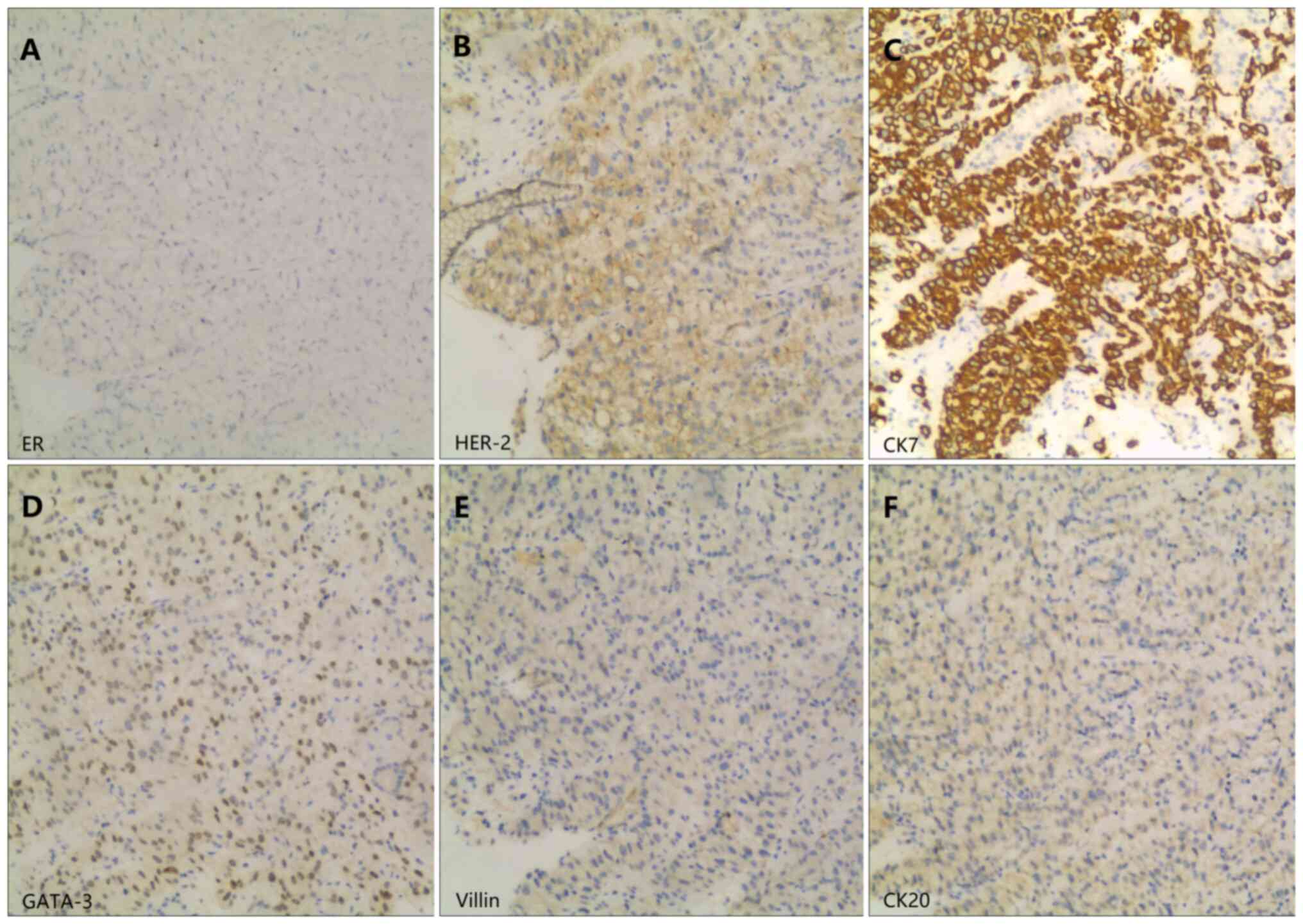
adenocarcinoma (Fig. 2C). The
gastric lesion (corpus ventriculi) exhibited ER(−), HER-2(1+), GATA
binding protein 3 (GATA-3)(+), CK7(++), CK20(−) and Villin(−),
confirming metastasis of the primary adenocarcinoma of the breast
(Fig. 4). The final diagnosis was
stage IV (cT2N3M1; TNM Staging System, the eighth AJCC staging
edition) (10) TN-ILC with
multisystem metastases involving gastric, cerebral, osseous,
adrenal, pleural and extensive lymph node sites. Unfortunately, due
to financial reasons, the patient did not undergo further BRCA1/2,
programmed death-ligand 1 and partner and localizer of BRCA2 gene
testing.
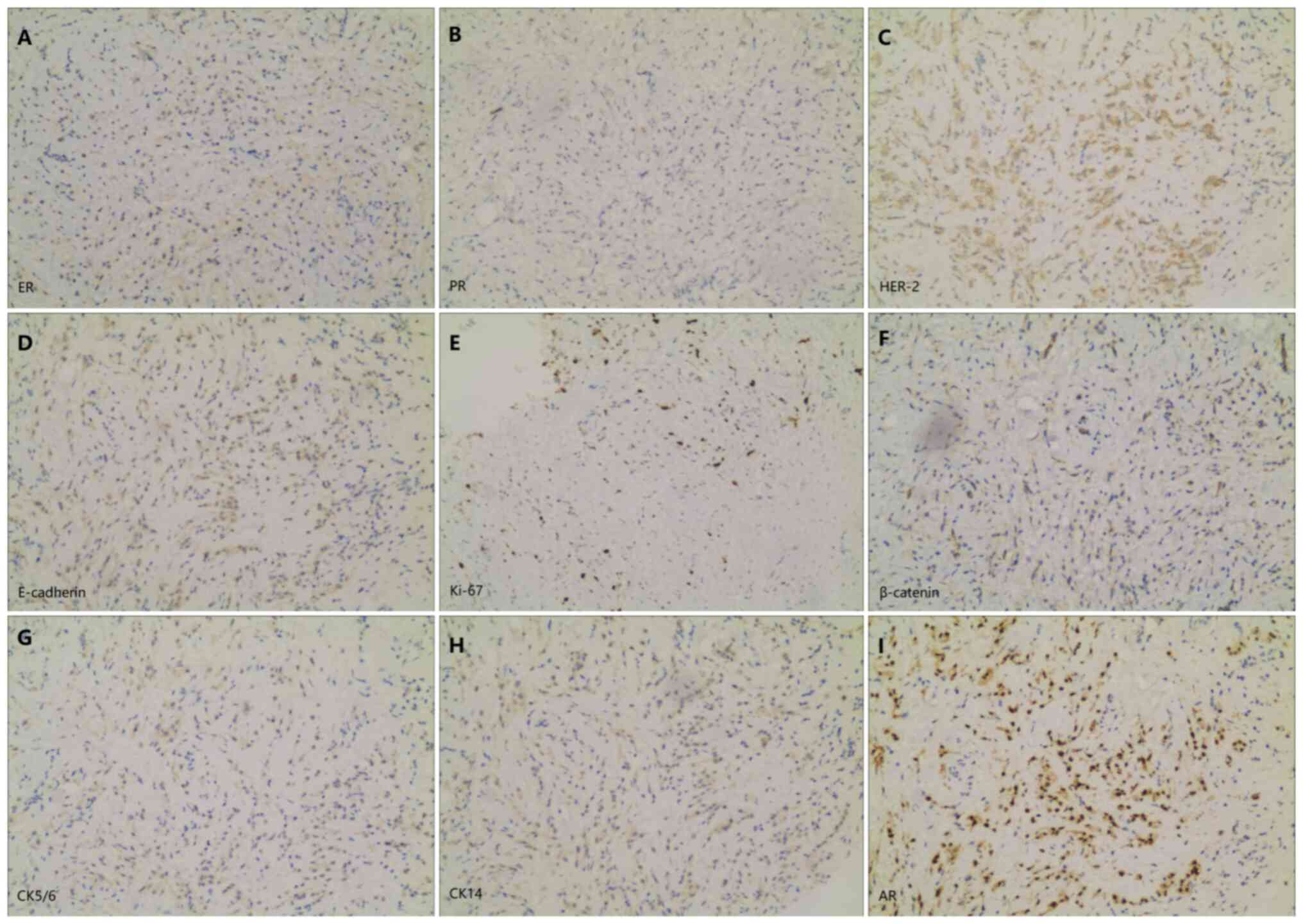 | Figure 3.Immunohistochemistry results of the
breast biopsy specimen (magnification, ×100). Staining for (A) ER,
(B) PR, (C) HER-2, (D) E-cadherin, (E) Ki-67, (F) β-catenin, (G)
CK5/6, (H) CK14 and (I) AR. ER, estrogen receptor; PR, progesterone
receptor; CK, cytokeratin; AR, androgen receptor. |
Following the confirmed diagnosis, the patient
underwent first-line chemotherapy with a TX regimen (paclitaxel 175
mg/m2 day 1 plus capecitabine 1,000 mg/m2
twice daily on days 1–14, every 21 days). The patient's disease was
stable after two cycles as assessed by the RECIST 1.1 criteria
(10) (Fig. 1F). After completing six cycles of
treatment, the patient started maintenance therapy with
single-agent capecitabine (1,000 mg/m2 twice daily for
14 consecutive days, repeated every 21 days) with regular imaging
monitoring.
Subsequent evaluation in February 2025 revealed
disease progression (Fig. 1G),
which led to a switch to second-line therapy. After initiation of
second-line utidelone monotherapy (30 mg/m2 on days 1–5,
every 3 weeks) in February 2025, follow-up imaging in May 2025
revealed new intracranial metastases accompanied by clinical
manifestations of dizziness. Following disease progression in May
2025 (Fig. 1H), the patient
underwent systemic therapy with toripalimab (240 mg on day 1, every
3 weeks) plus eribulin (1.4 mg/m2 on day 1–8, every 3
weeks), concurrent with local radiotherapy (stereotactic
radiotherapy of 27 Gy in 9 Gy fractions) for brain metastases. This
regimen remains ongoing as of July 2025.
Materials and methods
Gastroscopy and breast tissue biopsy specimens were
routinely fixed in 3.7% neutral formalin at room temperature for
6–24 h, followed by conventional procedures including dehydration
and paraffin embedding. The specimens were then cut into 3-µm-thick
sections and stained with HE for light microscopy examination.
Hematoxylin staining was performed for 5 min and eosin staining for
3 min at room temperature. Immunohistochemistry was performed using
the EnVision method. The staining process included dewaxing and
hydration of the paraffin sections which involved a descending
alcohol series, then PBS washing for 5 min for three times. Antigen
retrieval was performed using citrate buffer (pH 6.0; cat. no.
G1202; Wuhan Servicebio Technology Co., Ltd.) at 95°C for 20 min.
Endogenous peroxidase blocking was achieved by incubating with 0.3%
H2O2 for 15 min. Non-specific binding was
blocked with 5% normal goat serum (cat. no. ab7481; Abcam) for 30
min at room temperature. The primary antibodies used included: ER
(cat. no. ZA0102), PR (cat. no. ZA-0255), HER-2 (cat. no. ZM-0065),
E-cadherin (cat. no. ZA-0565), Ki-67 (cat. no. ZM-0166), CK5/6
(cat. no. ZM-0313), CK14 (cat. no. ZA-0540), AR (cat. no. ZA-0554),
GATA-3 (cat. no. ZA-0661), CK7 (cat. no. ZM-0071), CK20 (cat. no.
ZA-0574) and Villin (cat. no. ZM-0261), all from Beijing Zhongshan
Golden Bridge Biotechnology Co., Ltd. (OriGene Technologies, Inc.)
and supplied at a ready to use dilution. The primary antibodies
were applied at 37°C for 1 h. Following this, secondary universal
antibodies (rabbit/mouse IgG; 1:200; cat. no. SAP-9100; Beijing
Zhongshan Golden Bridge Biotechnology Co., Ltd.; OriGene
Technologies, Inc.) combined with diluted biotin (100 µl) were
applied at 37°C for an additional 30 min. The specimens underwent
chromogenic reactions and re-staining before being sealed.
Diaminobenzidine (DAB) served as the chromogenic substrate.
Following DAB visualization, nuclei were counterstained with
hematoxylin for 5 min at room temperature. A BX53 Olympus standard
light microscope equipped with an image acquisition system was used
to analyze the sections.
Discussion
ILC represents the predominant breast cancer
histological subtype that metastasizes to the gastrointestinal
tract (4). Existing literature
reports gastric metastasis incidence rates of 0.06% among patients
with breast cancer, but some studies suggest that this percentage
may be slightly higher, at ~6% (6,7). Of
note, gastric metastases typically appear several years after the
diagnosis of the primary breast tumor (11,12).
Notably, >90% of breast cancer cases with gastric metastases are
documented to be ER positive (13).
The present case represents a rare clinical presentation of TN-ILC
with synchronous gastric metastasis at initial diagnosis.
Gastric metastases typically present with
non-specific gastrointestinal symptoms including abdominal pain
(the most common symptom), nausea, dyspepsia, anorexia and bleeding
(14). Notably, 20–30% of cases
remain asymptomatic and are incidentally detected during
evaluations, which significantly increases the diagnostic
difficulty (15). Endoscopic
features of gastric metastases typically show poor specificity,
with the classic ‘linitis plastica’ pattern being the most commonly
observed (16). Other endoscopic
findings may include localized ulcerative or polypoid lesions,
submucosal nodularity or mass formation, increased mucosal
fragility, fold thickening, diffuse infiltration patterns and
external compression deformities. The diagnostic sensitivity of
superficial biopsies remains suboptimal due to the characteristic
submucosal and muscular infiltrative pattern, similar to that of
primary gastric malignancies. Current evidence suggests that ~30%
of gastric metastases may be missed during initial endoscopic
evaluation, primarily due to inadequate sampling depth (17). This diagnostic challenge is further
corroborated by autopsy studies revealing an 11.6% incidence of
gastric metastases among patients with breast cancer (18), strongly suggesting clinical
under-detection of this metastatic pattern. In the present study,
the complete absence of gastrointestinal symptoms and the
non-specific radiological finding of gastric wall thickening in the
patient posed significant diagnostic difficulties. The endoscopic
appearance of infiltrative lesions in the gastric body was
indistinguishable from primary gastric carcinoma. Ultimately, a
comprehensive histopathological evaluation by immunohistochemical
analysis was required to confirm the diagnosis.
Immunohistochemical analysis is the most important
method for distinguishing primary gastric cancer from metastatic
gastric cancer. While ~80% of breast cancer metastases to the
stomach retain ER and PR expression, it is noteworthy that 32 and
12% of primary gastric carcinomas may demonstrate ER and PR
positivity, respectively, which limits the specificity of these
markers when used alone (19,20).
HER-2, an established oncogenic driver in breast cancer, typically
shows negative expression in ILC (21) and exhibits marked heterogeneity in
gastric cancer, thereby diminishing its diagnostic utility for
identifying metastatic lesions (14). CK7/20 provides a clearer
distinction, with CK7(+)/CK20(−) expression strongly suggesting a
breast, lung, thyroid or gynecological origin, whereas primary
gastric malignancies often show a CK7(+)/CK20(+) co-expression
pattern (22). Of particular value
is GATA-3, a zinc finger transcription factor that plays a key role
in breast epithelial differentiation. GATA-3 is expressed in all
ILC cases (23), whereas its
expression in primary gastric adenocarcinoma is <5% (24). In addition, Villin, a cytoskeletal
protein that is consistently expressed in the gastrointestinal
epithelium but is absent in breast tissue, further improves
diagnostic specificity (25). In
the present case of triple-negative breast cancer
[ER(−)/PR(−)/HER-2(−)], the combined immunohistochemical profile of
CK7(+)/CK20(−)/GATA-3(+)/Villin(−) provided conclusive evidence for
metastatic breast carcinoma, resolving the initial diagnostic
challenge posed by morphological similarities to primary gastric
cancer.
The discovery of gastric metastasis typically
implies advanced disease. Notably, 90–94% of patients with breast
cancer diagnosed with gastric metastasis also have other distant
metastases (26). This aggressive
clinical presentation portends a poor prognosis, with a median
survival time of ~10 months (17)
and 3-year survival rates of 79.1% (6). Current evidence suggests that while a
mastectomy may confer survival benefits in carefully selected
patients with solitary metastases, the majority of cases derive no
significant survival advantage from surgical intervention compared
with systemic therapy alone (27).
Based on these considerations, we recommend that treatment
strategies for patients with breast cancer and gastric metastases
should prioritize systemic therapies, with individualized regimens
incorporating tumor burden, biomarker profiles (including hormone
receptor and HER-2 status) and patient performance status. Local
interventions should be reserved for two specific clinical
scenarios: i) As consolidative therapy following favorable response
to systemic treatment; or ii) for palliation of refractory local
symptoms including pain or obstructive complications.
In the present study, the simultaneous discovery of
the primary TN-ILC and its gastric metastasis serves as a notable
clinical alert, emphasizing the need for heightened suspicion of
unusual metastatic sites even at initial presentation in patients
with this aggressive subtype. Multiple biopsies of the suspicious
area and immunohistochemistry can improve the diagnostic accuracy
of gastric metastases in breast cancer.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
LZ conceptualized the case report, wrote the
manuscript and performed additional data analysis. YX and MW were
involved in the treatment and follow-up in this case. MW critically
revised the manuscript, provided supervision and approved the final
manuscript for publication. All authors have read and approved the
final version of the manuscript. LZ and MW confirm the authenticity
of all the raw data.
Ethics approval and consent to
participate
Ethics approval was not required for the present
study in accordance with our local and institutional requirements.
The present study was conducted in accordance with local
legislation and institutional requirements. The participant
provided written informed consent to participate in the present
study.
Patient consent for publication
Written informed consent for publication of this
article was obtained from the participant.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Leon-Ferre RA and Goetz MP: Advances in
systemic therapies for triple negative breast cancer. BMJ.
381:e0716742023. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lin NU, Claus E, Sohl J, Razzak AR,
Arnaout A and Winer EP: Sites of distant recurrence and clinical
outcomes in patients with metastatic triple-negative breast cancer:
High incidence of central nervous system metastases. Cancer.
113:2638–2645. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Caparica R, Lambertini M and de Azambuja
E: How I treat metastatic triple-negative breast cancer. ESMO Open.
4 (Suppl 2):e0005042019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kioleoglou Z, Georgaki E, Koufopoulos N,
Kostek O, Volakakis N, Dimitriadou A and Kokkali S:
Gastrointestinal metastases from lobular breast carcinoma: A
literature review. Cureus. 16:e658522024.PubMed/NCBI
|
|
6
|
Hong J, Kim Y, Cho J, Lim SW, Park SE, Kim
HK, Lee H, Cho SY, Kim JY, Ahn JS, et al: Clinical features and
prognosis of breast cancer with gastric metastasis. Oncol Lett.
17:1833–1841. 2019.PubMed/NCBI
|
|
7
|
Ito A, Nakatsubo M, Yoshino R, Yoshida N
and Kitada M: Two cases of breast cancer with gastric metastasis.
Cureus. 15:e434342023.PubMed/NCBI
|
|
8
|
Dilawar H, Ahmed A, Habib S, Iqbal J,
Abdul Rehman T, Hadi I, Nisa N and Fatima S: Gastric metastasis
from invasive lobular breast cancer, resembling primary gastric
cancer. J Nucl Med Technol. 52:68–70. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mercado CL: BI-RADS update. Radiol Clin
North Am. 52:481–487. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: The eighth edition AJCC cancer staging manual:
Continuing to build a bridge from a population-based to a more
‘personalized’ approach to cancer staging. CA Cancer J Clin.
67:93–99. 2017.PubMed/NCBI
|
|
11
|
Ayadi S, Monastiri S, Safta AB, Hammami M,
Samaali I, Kammoun M, Blel A, Aloui R, Zaimi Y and Mouelhi L:
Gastric metastasis and peritoneal carcinosis revealing primary
breast cancer: an unusual presentation. Future Sci OA.
10:FSO9702024. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
McLemore EC, Pockaj BA, Reynolds C, Gray
RJ, Hernandez JL, Grant CS and Donohue JH: Breast cancer:
Presentation and intervention in women with gastrointestinal
metastasis and carcinomatosis. Ann Surg Oncol. 12:886–894. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhao Q, Zhang D and Wang X: Case report:
Gastric metastasis of breast cancer. Front Oncol. 14:14308812024.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cheng M, Jia Z, Zhang G, Wang Y, Li S,
Yang S, Li C and Geng C: Gastric metastasis from breast cancer:
Five cases and a single-institutional review. J Int Med Res.
52:30006052412339882024. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kim GH, Ahn JY, Jung HY, Park YS, Kim MJ,
Choi KD, Lee JH, Choi KS, Kim DH, Lim H, et al: Clinical and
endoscopic features of metastatic tumors in the stomach. Gut Liver.
9:615–622. 2015.PubMed/NCBI
|
|
16
|
Zhang B, Copur-Dahi N, Kalmaz D and Boland
BS: Gastrointestinal manifestations of breast cancer metastasis.
Dig Dis Sci. 59:2344–2346. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Taal BG, Peterse H and Boot H: Clinical
presentation, endoscopic features, and treatment of gastric
metastases from breast carcinoma. Cancer. 89:2214–2221. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cormier WJ, Gaffey TA, Welch JM, Welch JS
and Edmonson JH: Linitis plastica caused by metastatic lobular
carcinoma of the breast. Mayo Clin Proc. 55:747–753.
1980.PubMed/NCBI
|
|
19
|
Briki R, Cherif O, Bannour B, Hidar S,
Boughizane S and Khairi H: Uncommon metastases of invasive lobular
breast cancer to the endometrium: A report of two cases and review
of the literature. Pan Afr Med J. 30:2682018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Arpino G, Bardou VJ, Clark GM and Elledge
RM: Infiltrating lobular carcinoma of the breast: Tumor
characteristics and clinical outcome. Breast Cancer Res.
6:R149–R156. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
Almubarak MM, Laé M, Cacheux W, de Cremoux
P, Pierga JY, Reyal F, Bennett SP, Falcou MC, Salmon RJ, Baranger B
and Mariani P: Gastric metastasis of breast cancer: A single centre
retrospective study. Dig Liver Dis. 43:823–827. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Dum D, Menz A, Völkel C, De Wispelaere N,
Hinsch A, Gorbokon N, Lennartz M, Luebke AM, Hube-Magg C, Kluth M,
et al: Cytokeratin 7 and cytokeratin 20 expression in cancer: A
tissue microarray study on 15,424 cancers. Exp Mol Pathol.
126:1047622022. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liu H, Shi J, Wilkerson ML and Lin F:
Immunohistochemical evaluation of GATA3 expression in tumors and
normal tissues: A useful immunomarker for breast and urothelial
carcinomas. Am J Clin Pathol. 138:57–64. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang S, Li W, Li S, Liu X, Zhang L, Hao C,
Meng W, Zhao W and Tong Z: Clinicopathological features and
prognosis of gastrointestinal metastases from breast carcinoma: A
clinicopathological study of 22 patients. Int J Surg Pathol.
31:1075–1084. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Dum D, Lennartz M, Menz A, Kluth M,
Hube-Magg C, Weidemann S, Fraune C, Luebke AM, Hornsteiner L,
Bernreuther C, et al: Villin expression in human tumors: A tissue
microarray study on 14,398 tumors. Expert Rev Mol Diagn.
22:665–675. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yoo KC, Kim DH, Park S, Yun H, Ryu DH, Lee
J and Son SM: Gastric Metastasis mimicking early gastric cancer
from invasive ductal carcinoma of the breast: Case report and
literature review. Medicina (Kaunas). 60:9802024. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ueno T: Surgical management of metastatic
breast cancer: A mini review. Front Oncol. 12:9105442022.
View Article : Google Scholar : PubMed/NCBI
|