Breast cancer is one of the most common malignant
tumors among women worldwide and a leading cause of cancer-related
mortality, posing a notable threat to women's health. According to
the latest report from the International Agency for Research on
Cancer, breast cancer accounts for 11.6% of newly diagnosed cancer
cases globally, making it the second most prevalent cancer after
lung cancer (12.4%) (1). Despite
continuous advancements in the treatment of breast cancer, its
incidence continues to rise, and mortality rates vary markedly
across different regions (1). In
high-income countries, where early diagnosis and advanced treatment
options are widely available, the 5-year survival rate reaches
80–90%; however, in low-income countries, survival rates generally
remain <50% (2).
Breast cancer can be classified into different
subtypes based on molecular biological characteristics and
immunohistochemical markers, including hormone receptor-positive
(HR+) breast cancer, HER2+ breast cancer and
triple-negative breast cancer (TNBC), as well as rarer subtypes
such as basal-like breast cancer and normal-like breast cancer
(3). Increasing evidence suggests
that distinct molecular drivers, non-coding RNAs and tumor
microenvironmental factors contribute to subtype heterogeneity and
therapeutic response differences (4,5). Each
subtype differs notably in terms of incidence, distribution,
pathological features and response to treatment (6). For instance, recent advances in
immunotherapeutic strategies have shown varying efficacy across
molecular subtypes, particularly in TNBC, underscoring the
biological diversity of breast cancer (7). This classification forms the basis for
personalized treatment strategies and aids in optimizing treatment
plans and prognosis assessments.
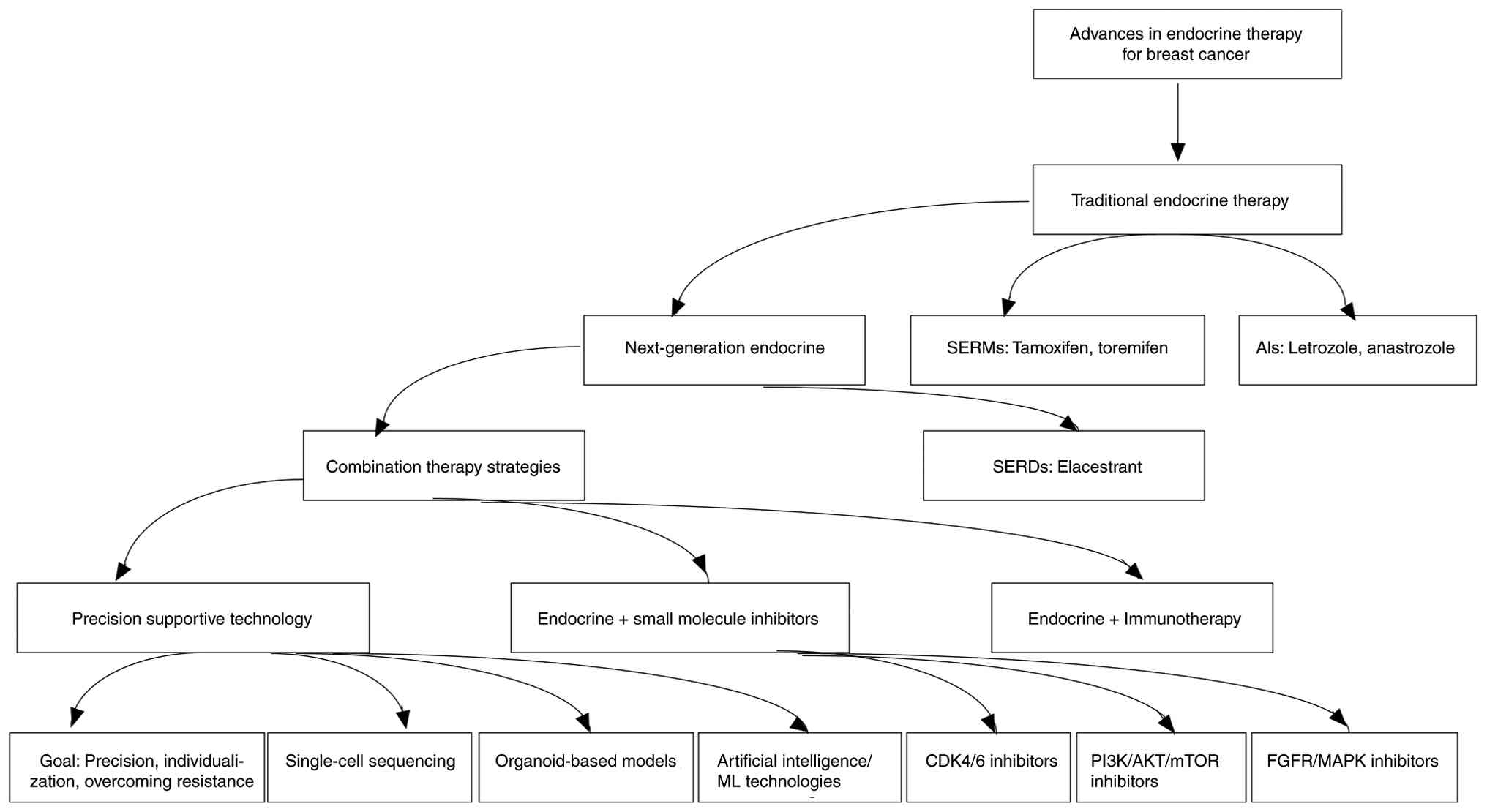
The main classes of endocrine therapy drugs for
breast cancer include selective ER modulators (SERMs), which
competitively bind to ERs to block the effects of estrogen. In
breast tissue, they act as ER antagonists, whereas in bone and
uterine tissue, they function as partial agonists. Tamoxifen, a
representative SERM drug, is a cornerstone treatment for both
premenopausal and postmenopausal patients with breast cancer
(3). Raloxifene, another SERM, is
primarily used for breast cancer prevention (12). Although SERMs have shown
considerable efficacy in the adjuvant and neoadjuvant treatment of
breast cancer, long-term use is associated with an increased risk
of endometrial cancer and osteoporosis (7,9,10,12–14).
Aromatase is a key enzyme responsible for converting
androstenedione to estradiol, representing the primary source of
estrogen synthesis in postmenopausal women. Aromatase inhibitors
(AIs) inhibit aromatase activity, thereby markedly reducing
circulating estrogen levels and suppressing the growth of breast
cancer (12). AIs are classified
into two categories: i) Non-steroidal AIs (such as letrozole and
anastrozole), which reversibly inhibit aromatase; and ii) steroidal
AIs (such as exemestane), which act irreversibly. AIs are widely
used in postmenopausal HR+ patients with breast cancer
and have demonstrated superior efficacy compared with tamoxifen,
making them the preferred first-line therapy (15).
Selective ER degraders (SERDs) bind to ERs and
induce their degradation, leading to the complete blockade of ER
signaling. Fulvestrant is the currently approved SERD and is
primarily used in HR+ patients with advanced breast
cancer who exhibit endocrine resistance. Due to their unique
mechanism of action, SERDs are considered breakthrough endocrine
agents, and next-generation oral SERDs (such as elacestrant) are
under clinical development (16).
Several next-generation oral SERDs have now progressed into
late-stage clinical development. Among these agents, elacestrant
currently has the most robust clinical evidence. In the randomized
phase III EMERALD trial, elacestrant demonstrated a notable
improvement in progression-free survival (PFS) compared with the
investigator's choice of standard endocrine monotherapy in patients
with ER+/HER2− metastatic breast cancer who
had previously received endocrine therapy in combination with a
CDK4/6 inhibitor. Notably, the magnitude of benefit was more
pronounced in tumors harboring ESR1 mutations, supporting the
biological rationale for ER degradation in this molecularly defined
subgroup (12). Subsequent updated
analyses presented at the San Antonio Breast Cancer Symposium
further indicated that patients with longer prior exposure to
CDK4/6 inhibitors derived greater clinical benefit, suggesting that
preserved endocrine sensitivity may identify a population
particularly suited to an oral SERD-based strategy (17). Taken together, these findings
support the integration of oral SERDs into contemporary treatment
algorithms for endocrine-resistant ER+/HER2−
metastatic breast cancer. In particular, they appear especially
relevant in the post-CDK4/6 inhibitor setting, where resistance is
associated with ESR1-driven reactivation of ER signaling and where
continued endocrine-based therapy remains clinically appropriate
(18).
Beyond randomized phase III data, emerging
real-world evidence has begun to provide complementary insights
into the effectiveness of next-generation oral SERDs in routine
oncology practice. Although the clinical adoption of elacestrant is
relatively recent and long-term data remain limited, retrospective
analyses derived from large US clinical-genomic and administrative
databases have suggested that treatment outcomes observed in
real-world settings are broadly consistent with those reported in
EMERALD, particularly in patients harboring ESR1 mutations
(19). A real-world study published
in Clinical Cancer Research evaluated elacestrant-treated patients
with ER+/HER2−, ESR1-mutant metastatic breast
cancer using integrated molecular and longitudinal clinical data,
supporting its clinical activity outside the constraints of a
randomized trial environment (19).
Additional database-driven analyses presented at scientific
meetings have reported real-world PFS estimates and treatment
patterns that align with phase III findings (20).
In recent years, notable progress has been made in
combining endocrine therapy with targeted therapies (such as CDK4/6
inhibitors and PI3K inhibitors). CDK4/6 inhibitors enhance the
effectiveness of endocrine therapy by inhibiting CDKs involved in
the cell cycle (21). PI3K
inhibitors target mutations in the PI3K pathway, improving the
overall response to endocrine therapy (22). These combination therapeutic
strategies have markedly prolonged PFS and overall survival (OS) of
patients, and represent a major focus of current research in the
field of HR+ breast cancer (Table I) (15,16,21,23,24).
The combination of AIs and CDK4/6 inhibitors has
markedly prolonged PFS, establishing a new standard of care for
HR+ breast cancer treatment (Tables I and II) (15,16,21,23–28).
Studies such as PALOMA-3 (25),
MONALEESA-3 (21) and MONALEESA-7
(26) have demonstrated that CDK4/6
inhibitors combined with endocrine therapy can notably extend PFS
and improve the objective response rate. However, the main adverse
effects associated with CDK4/6 inhibitors include neutropenia,
anemia, liver function abnormalities and fatigue. Therefore, close
clinical monitoring of these treatment-related toxicities is
essential.
In recent years, immunotherapy has made notable
progress in the treatment of TNBC (29), and the combination of endocrine
therapy and immunotherapy in breast cancer has become an emerging
research focus. Immune checkpoint inhibitors (ICIs), primarily
targeting the programmed cell death protein 1 (PD-1)/programmed
death-ligand 1 (PD-L1) axis, have established the clearest clinical
benefit in TNBC, where higher tumor immunogenicity and immune
infiltration make checkpoint blockade more actionable. In current
practice, pembrolizumab combined with chemotherapy is a key
ICI-based strategy in TNBC, supported by regulatory approvals and
phase III evidence in both early-stage and advanced settings, with
PD-L1 expression (such as CPS thresholds in metastatic disease)
serving as an important selection biomarker (30–33).
Early data from the I-SPY trial show that adding pembrolizumab to
taxane-based neoadjuvant therapy results in an estimated pathologic
complete response rate of 46 vs. 16% for HER2− patients,
60 vs. 20% for patients with TNBC and 34 vs. 13% for
ER−/PR+/HER2− patients (34). In HR+ breast cancer, the
efficacy of immunotherapy is relatively low, partly due to the low
level of immune infiltration and a strong immunosuppressive
microenvironment in these tumors (34). By contrast,
HR+/HER2− breast cancer generally exhibits
‘immune-cold’ features [low tumor-infiltrating lymphocytes (TILs)
and dominant immunosuppressive signaling], translating into modest
and heterogeneous activity of ICIs as monotherapy or in unselected
populations; nevertheless, ongoing trials are exploring rational
combinations-such as endocrine therapy plus CDK4/6 inhibition with
PD-1/PD-L1 blockade or other immunomodulators-to convert the tumor
microenvironment (TME) and potentially extend benefit to
biomarker-enriched HR+/HER2− subsets
(35,36). Currently, several clinical trials
are evaluating the combined efficacy of endocrine therapy and
immunotherapy (Table III)
(37–39). However, the discussion of predictive
biomarkers for endocrine-immunotherapy combinations remains
insufficient, particularly in HR+ breast cancer.
Identification of reliable biomarkers is critical for guiding
individualized treatment selection and improving therapeutic
efficacy.
First, tumor immune microenvironment-related
indicators may provide important predictive information. The level
of TILs and the composition of immune cell subsets-including
CD8+ cytotoxic T cells, regulatory T cells and
tumor-associated macrophages-have been associated with response to
immune checkpoint blockade in breast cancer (40,41).
Although HR+ tumors generally exhibit lower TIL levels
compared with TNBC, an immune-enriched subset of HR+
disease has been described, suggesting that quantitative and
functional immune profiling may refine patient selection (40).
Second, immune checkpoint-related biomarkers,
particularly PD-L1 expression, have been extensively investigated.
In metastatic TNBC, PD-L1 positivity determined by validated
companion diagnostic assays has demonstrated predictive value for
atezolizumab benefit (42).
However, in HR+ breast cancer, the predictive relevance
of PD-L1 remains controversial. Differences in antibody clones
(such as SP142 vs. 22C3), scoring systems (tumor cell vs. immune
cell vs. combined positive score) and assay platforms introduce
variability that limits cross-study comparability and clinical
interpretation (43).
Standardization of detection methodologies is therefore
essential.
Third, genomic-related biomarkers, including tumor
mutational burden (TMB) and microsatellite instability, may provide
complementary predictive value. High TMB has been associated with
improved response to ICIs across multiple tumor types (44). Although HR+ breast cancer
typically exhibits lower TMB compared with TNBC, a subset of tumors
with elevated mutational load or DNA repair deficiencies may
display enhanced immunogenicity. Integration of genomic instability
markers with endocrine resistance profiles may help identify
patients who could benefit from combination strategies.
Fourth, alterations in antigen presentation
machinery and interferon signaling pathways may influence immune
responsiveness. Deficiencies in major histocompatibility complex
expression or disruptions in interferon-γ signaling can impair
immune recognition, whereas tumors retaining intact antigen
presentation and active interferon-related gene signatures may
exhibit greater sensitivity to checkpoint blockade (45). These pathway-level biomarkers may
provide mechanistic stratification beyond single-marker
assessment.
Finally, circulating immune features and dynamic
circulating tumor DNA (ctDNA) monitoring represent promising early
predictive signals. Longitudinal ctDNA analysis has demonstrated
utility in monitoring treatment response and emerging resistance in
metastatic breast cancer (46). In
the context of endocrine-immunotherapy combinations, changes in
circulating immune cell subsets, cytokine profiles and ctDNA
mutation dynamics (including ESR1 mutation burden) may serve as
real-time indicators of therapeutic efficacy, although prospective
validation remains necessary.
Additionally, immunotherapy may serve an important
role in overcoming resistance to endocrine therapy. In breast
cancer with ER mutations or downregulation, immunotherapy can serve
as an alternative strategy and be combined with targeted therapies
(47). Overall, although multiple
candidate biomarkers have been proposed, robust validation in
HR+ breast cancer remains limited. Future research
should prioritize biomarker-driven stratification designs,
implement standardized detection methodologies and integrate
multi-omic approaches to establish clinically actionable predictive
models for endocrine-immunotherapy combinations.
Although endocrine therapy has markedly improved the
survival of patients with HR+ breast cancer, some
patients experience resistance and limited efficacy. Resistance can
be classified into primary resistance (present before treatment)
and acquired resistance (developed over time after treatment), both
of which are key challenges limiting the long-term effectiveness of
endocrine therapy (11).
Patients with primary resistance show limited
response to endocrine therapy, primarily due to mechanisms such as
the loss of ER signaling pathways and molecular heterogeneity
(48,49). Acquired resistance is a major
challenge, particularly in patients undergoing long-term treatment
or experiencing disease progression. Current research on resistance
mechanisms focuses on the following aspects: i) Mutations in the ER
gene (ESR1) are a key mechanism of acquired resistance (50); common mutation sites, such as Y537S
and D538G, lead to ER activation that is independent of estrogen,
thereby conferring resistance to AIs (51–53);
ii) activation of alternative signaling pathways: Aberrant
activation of pathways such as PI3K/AKT/mTOR, fibroblast growth
factor receptor and MAPK can promote tumor growth independently of
ER signaling, contributing to resistance (51,52,54);
iii) changes in the TME: The presence of an immunosuppressive
microenvironment and the secretion of pro-inflammatory cytokines
may mediate resistance through non-ER-dependent pathways (52); and iv) compensatory estrogen
synthesis: After AI treatment, tumors may increase local estrogen
production through alternative pathways, thereby counteracting the
therapeutic effects (55). For
patients with rapidly progressing breast cancer, the efficacy of
endocrine therapy is often limited, and numerous patients
eventually require a switch to chemotherapy.
Age and menopausal status substantially influence
endocrine responsiveness and resistance patterns in HR+
breast cancer. In premenopausal women, persistent ovarian estrogen
production necessitates ovarian function suppression (OFS) combined
with tamoxifen or an AI. The SOFT and TEXT trials demonstrated that
the addition of OFS markedly improves disease outcomes compared
with tamoxifen alone, with exemestane plus OFS providing further
benefit in selected higher-risk populations, including younger
patients (particularly those aged <35 years), lymph node
positivity (especially 4 or more positive lymph nodes), a high
Ki-67 proliferation index (>20%), tumor grade 3, or the presence
of lymphovascular invasion (56,57).
However, incomplete ovarian suppression may represent a clinically
relevant source of functional resistance, particularly in younger
women with high ovarian reserve, as suboptimal estradiol
suppression during AI plus OFS therapy has been associated with
inferior outcomes (58). In the
metastatic setting, the MONALEESA-7 trial established that adding
ribociclib to endocrine therapy plus OFS markedly improves OS in
premenopausal patients, reinforcing the importance of combined
endocrine-targeted approaches in this subgroup (59).
By contrast, elderly patients represent a
biologically and clinically heterogeneous population (60). Although HR+ tumors are
more prevalent in older women, treatment decisions are frequently
influenced by comorbidities, frailty, polypharmacy and tolerability
considerations (61). Older
individuals remain underrepresented in randomized trials.
Observational analyses have suggested higher rates of dose
modification and treatment discontinuation with CDK4/6
inhibitor-based regimens in elderly populations, underscoring the
need for careful treatment individualization (62). Collectively, these age-specific
differences highlight the importance of tailoring endocrine
strategies across the lifespan, balancing efficacy with safety and
patient-centered factors.
Beyond CDH1 loss, ILC frequently harbors alterations
in phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit
a (PIK3CA), AKT1, T-box 3 and forkhead box A1, and may exhibit a
luminal A-like transcriptional profile with relatively low
proliferation indices, although substantial molecular heterogeneity
exists (67). Clinically, ILC
demonstrates distinctive metastatic patterns compared with invasive
ductal carcinoma (IDC), with a higher propensity for metastasis to
the peritoneum, gastrointestinal tract, ovaries and leptomeninges
(64,68).
Due to its distinct molecular landscape, metastatic
behavior and potential therapeutic nuances, greater attention to
ILC and other rare HR+ subtypes is warranted. Future
clinical trials incorporating histology-specific stratification,
molecular profiling and prospective validation will be critical to
refining precision endocrine therapy strategies for these
understudied populations.
Single-cell sequencing technology provides powerful
tools for revealing breast cancer heterogeneity and its endocrine
therapy response mechanisms by analyzing the genome, transcriptome
and epigenome features of individual cells at high resolution
(71–73).
Traditional population-based sequencing methods
typically analyze tumor tissues as a whole, making it difficult to
capture the differences between cell subpopulations within the
tumor. Single-cell sequencing, by individually analyzing each cell
in tumor samples, reveals the molecular differences and functional
characteristics between tumor cell subpopulations. scRNA-seq can
differentiate various subpopulations of cells in breast cancer,
revealing some subgroups that are highly sensitive or resistant to
endocrine therapy (72,74–76).
Additionally, by analyzing the spatiotemporal distribution of gene
mutations and expression patterns, single-cell sequencing can
reconstruct the evolutionary trajectory of breast cancer from the
initial clone to the late-stage resistant clone, providing clues
for studying resistance mechanisms (77).
Resistance to endocrine therapy is a major challenge
that limits its efficacy. Single-cell sequencing provides the
following key insights for studying resistance: i) Cell
heterogeneity in ESR1 mutations: ESR1 mutations represent a
well-established mechanism of secondary endocrine resistance in
HR+ breast cancer. Single-cell analyses have been
proposed as a powerful tool to dissect clonal architecture;
however, to date, no studies have directly applied single-cell
sequencing to precisely quantify the intratumoral frequency of
individual ESR1-mutant clones and to monitor their clonal expansion
dynamics. Instead, analyses of ctDNA have demonstrated the
coexistence of multiple ESR1-mutant clones exhibiting distinct
evolutionary behaviors (78).
Furthermore, ESR1 mutations are typically rare in primary tumors
but occur at markedly higher frequencies in metastatic lesions
(79). Consistent with these
findings, RNA-seq-based analyses have also identified
resistance-associated ESR1 mutations in early-stage primary breast
cancers (80); and ii) interactions
of signaling pathways: scRNA-seq and epigenomic analyses have
revealed that specific endocrine-resistant breast cancer cell
subpopulations exhibit aberrant activation of alternative signaling
pathways, particularly the PI3K/AKT/mTOR axis, suggesting potential
therapeutic targets to overcome resistance (72,81,82).
Single-cell sequencing has emerged as a powerful
translational tool in breast cancer research, offering new
perspectives for clinical application in endocrine therapy: i)
Precision treatment guidance: By characterizing intratumoral
heterogeneity and identifying subpopulations with distinct
endocrine sensitivity, single-cell profiling may help predict
therapeutic response and support individualized treatment planning
(72,75,81);
ii) monitoring resistant clones: Integrating single-cell and ctDNA
analyses enables real-time tracking of resistant ESR1-mutant or
ligand-independent clones, thereby informing adaptive combination
strategies (85,86); and iii) drug development: scRNA-seq
and epigenomic analyses have uncovered novel molecular targets-such
as atypical ER co-regulators and downstream signaling
effectors-that are being explored for the next generation of
endocrine therapies (87).
Despite its substantial translational promise,
several technical and practical barriers currently limit the
routine clinical implementation of single-cell sequencing. First,
the overall cost of single-cell workflows-including tissue
processing, library preparation, sequencing depth requirements and
computational infrastructure-remains high, which constrains
scalability and clinical adoption in routine oncology practice
(88). Moreover, reimbursement
pathways for clinical-grade single-cell assays are not yet well
established in most healthcare systems. Second, single-cell
sequencing requires high-quality biological material, typically
fresh or optimally preserved tissue samples. Factors such as low
tumor cellularity, ischemia time, necrosis and dissociation-induced
transcriptional artifacts may notably compromise data reliability
and downstream biological interpretation (89,90).
These pre-analytical variables are particularly relevant in
clinical breast cancer specimens, where tissue availability may be
limited. Third, variability in experimental workflows-including
cell dissociation protocols, chemistry platforms, sequencing depth
and computational preprocessing-introduces substantial batch
effects, thereby limiting reproducibility and cross-cohort
comparability (91,92). Although computational integration
methods have improved correction strategies, complete elimination
of batch-driven bias remains challenging. Fourth, bioinformatic
analysis pipelines for single-cell data are complex and
computationally intensive, requiring advanced statistical modeling
and multi-layered annotation frameworks. Currently, there is no
universally accepted clinical interpretation standard for
translating high-dimensional cellular states into actionable
therapeutic decisions, particularly in the context of endocrine
resistance (89,93).
To advance clinical-grade implementation, the
development of high-quality reference atlases, harmonized
quality-control (QC) standards and consensus reporting systems will
be essential to ensure reproducibility, cross-platform
comparability and clinically meaningful interpretation (90,94).
In recent years, organoid technology has gradually
emerged in breast cancer research, providing a new platform for
personalized treatment. Organoids are three-dimensional cell
structures cultivated from patient tumor tissue that retain the
molecular and genetic characteristics of the original tumor,
including the complexity and heterogeneity of the TME (95,96).
This technology overcomes the limitations of traditional
two-dimensional cell cultures and animal models in simulating human
tumor biological behavior (96,97),
bringing revolutionary breakthroughs to the forefront of breast
cancer endocrine therapy research.
First, organoid models provide more accurate tools
for drug screening in endocrine therapy for breast cancer (98). ER+ subtypes account for
the majority of breast cancer patients, and selecting anti-estrogen
drugs (such as tamoxifen) and AIs (such as letrozole) are the main
strategies for endocrine therapy. However, due to individual
differences, patients often show notable variations in drug
responses. Organoid models can be directly cultivated from patient
tumor tissue to create personalized models that simulate the drug
response in the body of the patient (99). Studies have shown that testing
endocrine drugs in patient with breast cancer-derived organoids can
accurately predict clinical treatment outcomes for patients
(76,100). This ‘in vitro testing-in
vivo verification’ approach helps quickly identify the most
effective treatment plans, providing support for clinical
decision-making (76).
Additionally, organoids provide a platform for the development of
combination therapy strategies (76). By studying the combined use of
endocrine drugs and CDK4/6 inhibitors in organoids, the synergistic
effects of drugs can be assessed (101). These research findings not only
accelerate the development of new drugs but also improve treatment
precision.
Second, endocrine therapy resistance has always been
a major challenge in breast cancer treatment. Traditional research
methods struggle to fully capture the dynamic process of resistance
development, but organoid technology offers a new perspective
(97). Patient-derived breast
cancer organoids retain tumor heterogeneity and genetic mutation
characteristics, simulating molecular changes during treatment over
long-term cultures (96,98,102).
Research shows that organoids can capture the dynamic evolution of
ESR1 gene mutations during endocrine therapy, which is an important
mechanism of tamoxifen and fulvestrant resistance (103). Furthermore, by integrating
organoid models with scRNA-seq, researchers can comprehensively
analyze resistance-related cell subpopulations and gene expression
changes (104). Studies using
organoids have found that under prolonged drug exposure, some
breast cancer cells can escape immune suppression by upregulating
the PI3K/AKT signaling pathway (97,102).
This finding provides a basis for developing combination therapies
to block the PI3K pathway (105).
At the same time, organoid models also serve an important role in
studying strategies to reverse endocrine therapy resistance
(97). For example, combining
anti-estrogen drugs with epigenetic modulators in organoids showed
notable resistance reversal effects (104).
Lastly, another important application of organoid
models is exploring the role of the tumor immune microenvironment
in breast cancer treatment. The influence of the immune
microenvironment on endocrine therapy for breast cancer is
increasingly being recognized (96,106).
By establishing co-culture systems of organoids and immune cells,
the dynamic interactions between tumor cells and immune cells can
be simulated (97,107). At the same time, organoids provide
opportunities to analyze the roles of CAFs and immune cells in the
TME (106,108). Researchers found that by
introducing CAFs into organoids, they could induce resistance to
endocrine therapy in tumor cells through the secretion of TGF-β
(108). These findings provide
important clues for targeted regulation of the immune
microenvironment.
Although organoid technology holds great potential,
its widespread application in personalized breast cancer treatment
still faces challenges. The success rate and growth efficiency of
organoid cultures from different patient sources vary, which may be
influenced by the quality of tumor samples and culture conditions
(96). Importantly, notable
inter-laboratory variability exists in organoid culture protocols.
Differences in growth factor supplementation (such as EGF,
R-spondin and Noggin), media composition and passaging strategies
may influence clonal selection and phenotypic stability, thereby
compromising reproducibility and cross-study comparability
(109,110).
Moreover, most current organoid systems rely on
extracellular matrix (ECM) components such as Matrigel, which
possess undefined biochemical composition and substantial
batch-to-batch variability. These inconsistencies can affect
organoid architecture, differentiation status and drug response
profiles, limiting standardization and clinical translation
(111,112).
Although organoids are highly valuable for drug
testing, scalability for high-throughput screening (HTS) remains
constrained. Compared with conventional two-dimensional cell
systems, organoid cultures require more complex handling procedures
and longer expansion times, which restrict their integration into
rapid and large-scale screening pipelines (113). In addition, the time required for
successful organoid establishment and expansion-often several
weeks-may limit their utility in real-time clinical
decision-making, particularly in aggressive breast cancer cases
where rapid therapeutic selection is required (99). Organoid platforms are also
associated with substantial cost, technical complexity and
infrastructure demands, including specialized culture systems,
continuous growth factor supplementation and advanced imaging or
molecular profiling capabilities, which may hinder routine clinical
implementation (110).
Furthermore, traditional epithelial-only organoid models often lack
immune and stromal components, and therefore cannot fully
recapitulate tumor-immune or tumor-stroma interactions. While
co-culture systems incorporating immune cells or CAFs, as well as
air-liquid interface platforms, can enhance biological fidelity,
they substantially increase technical complexity and
standardization challenge (114).
Therefore, further optimization of standardized
culture methods is needed, as well as the development of defined
ECM alternatives, scalable automation platforms and consensus QC
standards before organoid models can be fully integrated into
precision oncology workflows. In terms of application prospects,
organoid models are expected to become a core technology for
personalized treatment (107,109). By integrating organoids into
clinical diagnostic and treatment processes, personalized organoid
models can be rapidly established from patient-derived tumor tissue
to screen the most suitable treatment plans and predict potential
resistance during treatment (107). At the same time, combining
organoids with CRISPR/Cas9 technology will enable in-depth
exploration of gene editing potential in breast cancer treatment
(96,97). As the technology continues to
mature, organoid models will serve an increasingly important role
in breast cancer basic research, drug development and clinical
translation (96,107).
HTS technology serves a key role in the development
of new drugs and target exploration for endocrine therapy in breast
cancer. By rapidly and on a large scale assessing the impact of
compounds on specific biological targets, HTS provides an efficient
means of discovering potential therapeutic drugs and new treatment
targets (96,106).
The emergence of endocrine therapy resistance and
side effects in breast cancer has driven researchers to
continuously seek new therapeutic drugs. HTS, implemented on
automated robotic platforms and miniaturized microplate formats
(such as 384- and 1,536-well plates), enables rapid testing of
large compound libraries-ranging from thousands to tens of
thousands of compounds per run-against cellular phenotypes. Using
cell-based viability, proliferation and apoptosis assays or
high-content imaging readouts, HTS accelerates the identification
of chemical modulators of breast cancer cell proliferation and
death and thereby expedites early-stage drug discovery (115). For instance, Sun et al
(116) used HTS to identify novel
coactivator binding inhibitors of ERα that at low micromolar
concentrations suppress estrogen signaling and inhibit
estrogen-stimulated reporter gene expression (117) These compounds, after further
optimization and validation, are expected to develop into new
endocrine therapy drugs.
In addition to new drug development, HTS also
serves an important role in discovering new treatment targets for
breast cancer. By systematically screening molecules that regulate
breast cancer cell proliferation, differentiation and
apoptosis-using approaches such as high-throughput small-molecule
screening and large-scale functional genomics (RNA
interference/CRISPR) screens-researchers have identified candidate
therapeutic targets that provide a rationale for the development of
targeted treatment strategies (117–119). Recent HTS research, employing
automated robotic platforms and high-content readouts, has been
used to identify small-molecule modulators of the PI3K/AKT/mTOR
signaling axis; several studies report HTS-derived hits that
inhibit PI3K/AKT/mTOR activity and demonstrate antitumor efficacy
in cellular and/or in vivo models (120,121). The PI3K/AKT/mTOR signaling axis
serves a central role in breast cancer development and progression,
and its aberrant activation has been strongly associated with
resistance to endocrine therapies (122). Clinical and translational studies
demonstrate that inhibition of this pathway by mTOR inhibitors
(such as everolimus), PI3Kα inhibitors (such as alpelisib) or AKT
inhibitors (such as capivasertib) can restore sensitivity or
provide clinical benefit (123,124). In addition, HTS has been used to
discover and optimize small-molecule modulators of PI3K/AKT/mTOR,
offering new therapeutic candidates to overcome endocrine
resistance (125).
Mechanistically, the PI3K/AKT/mTOR pathway
functions as a central regulator of tumor cell proliferation,
survival, metabolism and anti-apoptotic signaling. Upon activation
by receptor tyrosine kinases or ER-associated signaling, PI3K
generates PIP3, leading to AKT activation and downstream
phosphorylation of multiple substrates that promote cell-cycle
progression, protein synthesis and metabolic reprogramming while
inhibiting pro-apoptotic factors (126,127). Oncogenic alterations such as
activating mutations in PIK3CA, loss of the tumor suppressor PTEN
or aberrant AKT activation result in constitutive pathway
activation in breast cancer (125,128). Persistent PI3K/AKT/mTOR signaling
can promote ligand-independent ER activation and enhance
estrogen-independent transcriptional programs, thereby driving
resistance to endocrine therapies (127,129). This mechanistic framework provides
the biological rationale for combining endocrine therapy with mTOR
inhibitors, PI3Kα inhibitors or AKT inhibitors, aiming to suppress
compensatory survival signaling and restore endocrine sensitivity
(123).
With ongoing technological advances, HTS is
evolving toward greater throughput and improved precision (130). The incorporation of microfluidic
technologies-including droplet-based and arrayed microfluidic
platforms-enables assays to be performed in drastically reduced
volumes, increasing screening throughput and assay sensitivity
(131). Concurrently, artificial
intelligence and machine-learning (ML) methods have been integrated
into HTS workflows to accelerate data processing, deconvolute
complex readouts, prioritize true hits and predict compound-target
relationships (132). Finally, the
convergence of HTS with physiologically relevant patient-derived
models (such as organoids and other 3D culture systems) points to a
future in which HTS can be used for personalized drug screening
tailored to individual tumor characteristics, thereby facilitating
precision oncology (133).
Previous studies have applied artificial
intelligence and ML methods to breast cancer metabolomics and
transcriptomics data to improve diagnostic and predictive
capabilities (134,135). For example, Alakwaa et al
(133) used a deep learning-based
framework together with other ML algorithms to classify
ER+ vs. ER− breast cancers from metabolomics
data, achieving an area under the curve of 0.93. Similarly, in
predicting response to neoadjuvant endocrine therapy, gene
expression-based classifiers have been developed with high
accuracy. These advances support three promising applications in
endocrine therapy: i) Treatment response prediction; ii) analysis
of resistance mechanisms; and iii) designing more personalized
therapeutic strategies (136).
Artificial intelligence and ML approaches offer
powerful tools to dissect complex, high-dimensional molecular
datasets to uncover resistance-associated mechanisms. Indeed,
recent reviews have documented the application of artificial
intelligence in tumor drug resistance to identify resistance
biomarkers, infer signaling dependencies and stratify patient
subsets based on predicted resistance risk (141,142). In breast cancer specifically, ML
models have been deployed to integrate genomic, transcriptomic,
proteomic and clinical data to predict resistance to endocrine
agents and to prioritize candidate regulators or pathways
underlying resistance (143).
Taken together, integrating mechanistic insights (such as
PI3K/AKT/mTOR activation) with ML-driven discovery pipelines could
facilitate more precise resistance stratification and the rational
design of combination strategies to overcome endocrine
resistance.
Beyond outcome prediction, artificial intelligence
techniques also hold promise for designing personalized therapeutic
strategies tailored to individual patients. Through reinforcement
learning (RL), artificial intelligence agents can simulate the
longitudinal effects of alternative treatment regimens, iteratively
optimize policy and recommend adaptive therapeutic plans that
adjust dynamically in response to disease evolution (144,145). For example, in non-breast cancer
settings, simulated trials applying RL have been used to compare
survival outcomes under different regimens; for instance, in
relapsed extensive-stage small cell lung cancer, Bozcuk and Artaç
(146) developed an RL-based
simulated clinical trial comparing irinotecan plus ifosfamide with
topotecan, illustrating the feasibility of this approach for
evaluating alternative therapeutic strategies in silico.
More recently, deep RL frameworks have been proposed to infer
personalized adaptive therapy strategies by modeling tumor dynamics
and treatment response trajectories (147).
In parallel, artificial intelligence can accelerate
the identification of synergistic drug combinations that potentiate
endocrine therapy. Although direct artificial intelligence-driven
evaluations of combinations such as CDK4/6 inhibitors plus
endocrine agents in resistant breast cancer remain scarce, clinical
evidence already supports the efficacy of such combinations in
HR+/HER2− settings (148,149). With sufficiently large molecular
and treatment response datasets, artificial intelligence models
could, in principle, prioritize optimal combination regimens or
novel targeted therapies for patient subgroups with endocrine
resistance.
In summary, artificial intelligence and ML
approaches not only enhance predictive accuracy but also open
avenues toward adaptive, treatment-tailored strategies in endocrine
therapy for breast cancer. As computational models mature and more
multi-omic or longitudinal treatment datasets become available,
these methodologies are expected to accelerate precision medicine
and the discovery of novel therapeutic targets.
However, despite these promising advances,
important methodological challenges remain regarding model
interpretability and external validation. Numerous artificial
intelligence/ML models-particularly deep learning
frameworks-function as ‘black-box’ systems, generating highly
accurate predictions without transparent explanation of how
specific variables contribute to decision-making. In the context of
oncology, where treatment decisions directly affect patient
survival and safety, limited interpretability may reduce clinician
trust and hinder clinical adoption (150,151). To enhance transparency and
clinical credibility, interpretable artificial intelligence
strategies should be incorporated into predictive pipelines. These
include feature attribution methods (such as SHapley Additive
exPlanations values), variable importance reporting, biologically
constrained modeling frameworks and pathway-informed architectures
that align model outputs with known molecular mechanisms (152). Such approaches allow clinicians to
understand which genomic, transcriptomic or clinical features drive
predictions, thereby improving explainability and supporting
hypothesis generation.
In addition, a number of existing artificial
intelligence models in endocrine therapy research are trained on
retrospective datasets derived from single institutions or publicly
available cohorts (such as The Cancer Genome Atlas), which may
introduce selection bias and limit generalizability. Without
validation in independent external cohorts, model performance may
be overestimated due to overfitting or dataset-specific artifacts
(153). Therefore, future studies
should prioritize multi-center external validation, prospective
clinical evaluation and adherence to standardized reporting
frameworks such as TRIPOD-AI or CONSORT-AI to reduce bias, enhance
reproducibility and improve translational reliability (154,155). Strengthening interpretability,
transparency and rigorous validation will be essential for
translating artificial intelligence-driven endocrine therapy
prediction tools from computational research settings into routine
clinical oncology practice.
In recent years, combination strategies involving
CDK4/6 inhibitors, PI3K/AKT/mTOR pathway inhibitors and ICIs have
become a central focus of research, demonstrating promising
potential to prolong PFS and overcome specific mechanisms of
resistance. Concurrently, technological innovations-such as
scRNA-seq, patient-derived organoids, HTS and artificial
intelligence-have accelerated investigations into resistance
biology and facilitated the design of personalized therapeutic
strategies. Despite these advances, the intrinsic heterogeneity of
breast cancer and the multifactorial nature of endocrine resistance
continue to create substantial research gaps. Future directions are
expected to emphasize the integration of multi-omics, computational
modeling and precision oncology, with a focus on incorporating
novel immunotherapies, biomarker-driven stratification and rational
optimization of targeted drug combinations.
However, several limitations of the present review
should be acknowledged. First, as a narrative synthesis of rapidly
evolving literature, the review may not capture all emerging
clinical trial data or newly reported therapeutic strategies.
Second, many of the discussed approaches-particularly novel
immunotherapy combinations and biomarker-driven strategies-remain
under active investigation and their long-term clinical benefits
require further validation in large-scale prospective studies.
Additionally, variations in study design, patient populations and
biomarker assessment methodologies across the cited studies may
introduce heterogeneity that limits direct comparisons.
Ultimately, progress will depend on the synergistic
convergence of technological innovation and clinical translation.
By coupling drug discovery, mechanistic insight and immune
modulation strategies, it will be possible to develop more precise,
durable and patient-tailored treatment paradigms for breast cancer,
thereby addressing the current limitations in endocrine
therapy.
Not applicable.
The present study was supported by the Soft Science Special
Project of Gansu Basic Research Plan (grant no. 24JRZA019), the
Lanzhou City Science and Technology Program Project (grant no.
2022-5-101) and the Major Health Science and Technology Innovation
Project of Gansu Province (grant no. GSWSZD2025-13).
Not applicable.
YMD, SHW and HYQ designed the study. QL, YXQ and
TTL were responsible for data collection and integration. YMD, LHS,
QL, YXQ, TTL, SHW and HYQ performed data analysis and
interpretation of the results, and drafted the manuscript. Data
authentication is not applicable. All authors reviewed and approved
the final version of the manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
During the preparation of this work, an artificial
intelligence tool (ChatGPT, developed by OpenAI; version GPT-4) was
used to improve the readability and language of the manuscript, and
subsequently, the authors revised and edited the content produced
by the artificial intelligence tool as necessary, taking full
responsibility for the ultimate content of the present
manuscript.
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Kim J, Harper A, McCormack V, Sung H,
Houssami N, Morgan E, Mutebi M, Garvey G, Soerjomataram I and
Fidler-Benaoudia MM: Global patterns and trends in breast cancer
incidence and mortality across 185 countries. Nat Med.
31:1154–1162. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gradishar WJ, Moran MS, Abraham J,
Abramson V, Aft R, Agnese D, Allison KH, Anderson B, Bailey J,
Burstein HJ, et al: Breast cancer, version 3.2024, NCCN clinical
practice guidelines in oncology. J Natl Compr Canc Netw.
22:331–357. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pourhanifeh MH, Farrokhi-Kebria H,
Mostanadi P, Farkhondeh T and Samarghandian S: Anticancer
properties of baicalin against breast cancer and other
gynecological cancers: Therapeutic opportunities based on
underlying mechanisms. Curr Mol Pharmacol. 17:e187614292630632024.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hussain MS, Agrawal M, Shaikh NK, Saraswat
N, Bahl G, Maqbool Bhat M, Khurana N, Bisht AS, Tufail M and Kumar
R: Beyond the genome: Deciphering the role of MALAT1 in breast
cancer progression. Curr Genomics. 25:343–357. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lumachi F, Luisetto G, Basso SM, Basso U,
Brunello A and Camozzi V: Endocrine therapy of breast cancer. Curr
Med Chem. 18:513–522. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Araghi M, Gharebakhshi F, Faramarzi F,
Mafi A, Mousavi T, Alimohammadi M and Soleimantabar H: Efficacy and
safety of pembrolizumab monotherapy or combined therapy in patients
with metastatic Triple-negative breast cancer: A Systematic review
and Meta-analysis of randomized controlled trials. Curr Gene Ther.
25:72–88. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Johnston SJ and Cheung KL: Endocrine
therapy for breast cancer: A model of hormonal manipulation. Oncol
Ther. 6:141–156. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Goldhirsch A, Wood WC, Coates AS, Gelber
RD, Thürlimann B and Senn HJ; Panel members, : Strategies for
subtypes-dealing with the diversity of breast cancer: Highlights of
the St. Gallen international expert consensus on the primary
therapy of early breast cancer 2011. Ann Oncol. 22:1736–1747. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cheang MC, Chia SK, Voduc D, Gao D, Leung
S, Snider J, Watson M, Davies S, Bernard PS, Parker JS, et al: Ki67
index, HER2 status, and prognosis of patients with luminal B breast
cancer. J Natl Cancer Inst. 101:736–750. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Torun V, Degerli E and Cansaran-Duman D:
Revealing the molecular signatures of miR-185-5p on breast cancer
cells using proteomic analysis. Protein Pept Lett. 31:681–695.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Early Breast Cancer Trialists' and
Collaborative Group (EBCTCG), . Davies C, Godwin J, Gray R, Clarke
M, Cutter D, Darby S, McGale P, Pan HC, Taylor C, et al: Relevance
of breast cancer hormone receptors and other factors to the
efficacy of adjuvant tamoxifen: Patient-level meta-analysis of
randomised trials. Lancet. 378:771–784. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Howell A, Cuzick J, Baum M, Buzdar A,
Dowsett M, Forbes JF, Hoctin-Boes G, Houghton J, Locker GY and
Tobias JS; ATAC Trialists' Group, : Results of the ATAC (Arimidex,
Tamoxifen, Alone or in Combination) trial after completion of 5
years' adjuvant treatment for breast cancer. Lancet. 365:60–62.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bidard FC, Kaklamani VG, Neven P, Streich
G, Montero AJ, Forget F, Mouret-Reynier MA, Sohn JH, Taylor D,
Harnden KK, et al: Elacestrant (oral selective estrogen receptor
degrader) versus standard endocrine therapy for estrogen
receptor-positive, human epidermal growth factor receptor
2-negative advanced breast cancer: Results from the randomized
phase III EMERALD trial. J Clin Oncol. 40:3246–3256. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Johnston SRD, Toi M, O'Shaughnessy J,
Rastogi P, Campone M, Neven P, Huang CS, Huober J, Jaliffe GG,
Cicin I, et al: Abemaciclib plus endocrine therapy for hormone
receptor-positive, HER2-negative, node-positive, high-risk early
breast cancer (monarchE): Results from a preplanned interim
analysis of a randomised, open-label, phase 3 trial. Lancet Oncol.
24:77–90. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mayer EL, Dueck AC, Martin M, Rubovszky G,
Burstein HJ, Bellet-Ezquerra M, Miller KD, Zdenkowski N, Winer EP,
Pfeiler G, et al: Palbociclib with adjuvant endocrine therapy in
early breast cancer (PALLAS): Interim Analysis of a multicentre,
open-label, randomised, phase 3 study. Lancet Oncol. 22:212–222.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bardia ABF, Neven P, Streich G, Montero
AJ, Forget F, Mouret-Reynier MA, Sohn JH, Taylor D, Harnden KK,
Khong H, et al: Abstract GS3-01: GS3-01 EMERALD phase 3 trial of
elacestrant versus standard of care endocrine therapy in patients
with ER+/HER2-metastatic breast cancer: Updated results by duration
of prior CDK4/6i in metastatic setting. Cancer Res. 83 (Suppl
5):GS3–01. 2023. View Article : Google Scholar
|
|
18
|
Moore GR and Labatut AE: Updates in
endocrine-resistant metastatic breast cancer and Treatment-related
adverse event management. Curr Breast Cancer Rep. 17:532025.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rugo HS, Kaklamani V, Mcarthur H, Wander
SA, Gradishar W, Mahtani R, Pegram M, Lustberg M, Swallow E,
Maitland J, et al: Real-world outcomes of elacestrant in ER+,
HER2-, ESR1-mutant metastatic breast cancer. Clin Cancer Res.
32:179–187. 2026. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Swallow E, Maitland J, Sarathy K, Sears E,
Nagarwala Y, Depalantino J, Kruep E, Pelletier C, Kloss S and
Wasserman T: Elacestrant real-world progression-free survival
(rwPFS) of adult patients with ER+/HER2-, advanced breast cancer: A
retrospective analysis using insurance claims in the United States.
Clin Cancer Res. 31:31008. 2025. View Article : Google Scholar
|
|
21
|
Neven P, Fasching PA, Chia S, Jerusalem G,
De Laurentiis M, Im SA, Petrakova K, Bianchi GV, Martín M, Nusch A,
et al: Updated overall survival from the MONALEESA-3 trial in
postmenopausal women with HR+/HER2-advanced breast cancer receiving
first-line ribociclib plus fulvestrant. Breast Cancer Res.
25:1032023. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Baselga J, Cortés J, Kim SB, Im SA, Hegg
R, Im YH, Roman L, Pedrini JL, Pienkowski T, Knott A, et al:
Pertuzumab plus trastuzumab plus docetaxel for metastatic breast
cancer. N Engl J Med. 366:109–119. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sledge GW Jr, Toi M, Neven P, Sohn J,
Inoue K, Pivot X, Burdaeva O, Okera M, Masuda N, Kaufman PA, et al:
The effect of abemaciclib plus fulvestrant on overall survival in
hormone Receptor-Positive, ERBB2-Negative breast cancer that
progressed on endocrine Therapy-MONARCH 2: A randomized clinical
trial. JAMA Oncol. 6:116–124. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Robertson JFR, Shao Z, Noguchi S,
Bondarenko I, Panasci L, Singh S, Subramaniam S and Ellis MJ:
Fulvestrant versus anastrozole in endocrine Therapy-naïve women
with hormone receptor-Positive advanced breast cancer: Final
overall survival in the phase III FALCON trial. J Clin Oncol.
43:1539–1545. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cristofanilli M, Rugo HS, Im SA, Slamon
DJ, Harbeck N, Bondarenko I, Masuda N, Colleoni M, DeMichele A, Loi
S, et al: Overall survival with palbociclib and fulvestrant in
women with HR+/HER2-ABC: Updated exploratory analyses of PALOMA-3,
a Double-blind, Phase III randomized study. Clin Cancer Res.
28:3433–3442. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Slamon D, Lipatov O, Nowecki Z, McAndrew
N, Kukielka-Budny B, Stroyakovskiy D, Yardley DA, Huang CS,
Fasching PA, Crown J, et al: Ribociclib plus endocrine therapy in
early breast cancer. N Engl J Med. 390:1080–1091. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Rugo HS, Im SA, Joy AA, Shparyk Y, Walshe
JM, Sleckman B, Loi S, Theall KP, Kim S, Huang X, et al: Effect of
palbociclib plus endocrine therapy on time to chemotherapy across
subgroups of patients with hormone receptor-positive/human
epidermal growth factor receptor 2-negative advanced breast cancer:
Post hoc analyses from PALOMA-2 and PALOMA-3. Breast. 66:324–331.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bardia A, Hurvitz SA, DeMichele A, Clark
AS, Zelnak A, Yardley DA, Karuturi M, Sanft T, Blau S, Hart L, et
al: Phase I/II trial of exemestane, ribociclib, and everolimus in
women with HR+/HER2-Advanced breast cancer after progression on
CDK4/6 Inhibitors (TRINITI-1). Clin Cancer Res. 27:4177–4185. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mayer EL, Ren Y, Wagle N, Mahtani R, Ma C,
DeMichele A, Cristofanilli M, Meisel J, Miller KD, Abdou Y, et al:
PACE: A randomized phase II study of fulvestrant, palbociclib, and
avelumab after progression on Cyclin-Dependent kinase 4/6 inhibitor
and aromatase inhibitor for hormone Receptor-Positive/Human
epidermal growth factor Receptor-negative metastatic breast cancer.
J Clin Oncol. 42:2050–2060. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Shah M, Osgood CL, Amatya AK, Fiero MH,
Pierce WF, Nair A, Herz J, Robertson KJ, Mixter BD, Tang S, et al:
FDA approval summary: Pembrolizumab for neoadjuvant and adjuvant
treatment of patients with High-risk early-stage triple-negative
breast cancer. Clin Cancer Res. 28:5249–5253. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Schmid P, Oliveira M, O'Shaughnessy J,
Cristofanilli M, Graff SL, Im SA, Loi S, Saji S, Wang S, Cescon DW,
et al: TROPION-Breast05: A randomized phase III study of Dato-DXd
with or without durvalumab versus chemotherapy plus pembrolizumab
in patients with PD-L1-high locally recurrent inoperable or
metastatic triple-negative breast cancer. Ther Adv Med Oncol.
17:175883592513279922025. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Im SA, Cortes J, Cescon DW, Yusof MM,
Iwata H, Masuda N, Takano T, Huang CS, Chung CF, Tsugawa K, et al:
Results from the randomized KEYNOTE-355 study of pembrolizumab plus
chemotherapy for Asian patients with advanced TNBC. NPJ Breast
Cancer. 10:792024. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Cortes J, Rugo HS, Cescon DW, Im SA, Yusof
MM, Gallardo C, Lipatov O, Barrios CH, Perez-Garcia J, Iwata H, et
al: Pembrolizumab plus chemotherapy in advanced Triple-negative
breast cancer. N Engl J Med. 387:217–226. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Burstein HJ, Somerfield MR, Barton DL,
Dorris A, Fallowfield LJ, Jain D, Johnston SRD, Korde LA, Litton
JK, Macrae ER, et al: Endocrine treatment and targeted therapy for
hormone Receptor-Positive, human epidermal growth factor receptor
2-Negative metastatic breast cancer: ASCO guideline update. J Clin
Oncol. 39:3959–3977. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Di Grazia G, Dri A, Grieco A, Martinelli
C, Palleschi M, Martorana F, Barchiesi G, Arpino G, De Angelis C,
De Laurentiis M, et al: Unlocking the potential of immune
checkpoint inhibitors in HR+/HER2-breast cancer: A systematic
review. Cancers (Basel). 17:29402025. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Heater NK, Warrior S and Lu J: Current and
future immunotherapy for breast cancer. J Hematol Oncol.
17:1312024. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Jerusalem G, Prat A, Salgado R, Reinisch
M, Saura C, Ruiz-Borrego M, Nikolinakos P, Ades F, Filian J, Huang
N, et al: Neoadjuvant nivolumab + palbociclib + anastrozole for
oestrogen receptor-positive/human epidermal growth factor receptor
2-negative primary breast cancer: Results from CheckMate 7A8.
Breast. 72:1035802023. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Rugo HS, Delord JP, Im SA, Ott PA,
Piha-Paul SA, Bedard PL, Sachdev J, Le Tourneau C, van Brummelen
EMJ, Varga A, et al: Safety and antitumor activity of pembrolizumab
in patients with estrogen Receptor-Positive/Human epidermal growth
factor receptor 2-Negative advanced breast cancer. Clin Cancer Res.
24:2804–2811. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Dirix LY, Takacs I, Jerusalem G,
Nikolinakos P, Arkenau HT, Forero-Torres A, Boccia R, Lippman ME,
Somer R, Smakal M, et al: Avelumab, an anti-PD-L1 antibody, in
patients with locally advanced or metastatic breast cancer: A phase
1b JAVELIN Solid tumor study. Breast Cancer Res Treat. 167:671–686.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Denkert C, von Minckwitz G, Darb-Esfahani
S, Lederer B, Heppner BI, Weber KE, Budczies J, Huober J, Klauschen
F, Furlanetto J, et al: Tumour-infiltrating lymphocytes and
prognosis in different subtypes of breast cancer: A pooled analysis
of 3771 patients treated with neoadjuvant therapy. Lancet Oncol.
19:40–50. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Salgado R, Denkert C, Demaria S, Sirtaine
N, Klauschen F, Pruneri G, Wienert S, Van den Eynden G, Baehner FL,
Penault-Llorca F, et al: The evaluation of tumor-infiltrating
lymphocytes (TILs) in breast cancer: Recommendations by an
International TILs Working Group 2014. Ann Oncol. 26:259–271. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Schmid P, Adams S, Rugo HS, Schneeweiss A,
Barrios CH, Iwata H, Diéras V, Hegg R, Im SA, Shaw Wright G, et al:
Atezolizumab and Nab-Paclitaxel in advanced Triple-negative breast
cancer. N Engl J Med. 379:2108–2121. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Rugo HS, Loi S, Adams S, Schmid P,
Schneeweiss A, Barrios CH, Iwata H, Diéras V, Winer EP, Kockx MM,
et al: PD-L1 immunohistochemistry assay comparison in atezolizumab
plus nab-Paclitaxel-Treated advanced Triple-negative breast cancer.
J Natl Cancer Inst. 113:1733–1743. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Marabelle A, Fakih M, Lopez J, Shah M,
Shapira-Frommer R, Nakagawa K, Chung HC, Kindler HL, Lopez-Martin
JA, Miller WH Jr, et al: Association of tumour mutational burden
with outcomes in patients with advanced solid tumours treated with
pembrolizumab: Prospective biomarker analysis of the multicohort,
open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 21:1353–1365.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Spranger S and Gajewski TF: Impact of
oncogenic pathways on evasion of antitumour immune responses. Nat
Rev Cancer. 18:139–147. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Dawson SJ, Tsui DW, Murtaza M, Biggs H,
Rueda OM, Chin SF, Dunning MJ, Gale D, Forshew T, Mahler-Araujo B,
et al: Analysis of circulating tumor DNA to monitor metastatic
breast cancer. N Engl J Med. 368:1199–1209. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Brufsky AM and Dickler MN: Estrogen
Receptor-positive breast cancer: Exploiting signaling pathways
implicated in endocrine resistance. Oncologist. 23:528–539. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Hanker AB, Sudhan DR and Arteaga CL:
Overcoming endocrine resistance in breast cancer. Cancer Cell.
37:496–513. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Belachew EB and Sewasew DT: Molecular
mechanisms of endocrine resistance in Estrogen-positive breast
cancer. Front Endocrinol (Lausanne). 12:5995862021. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Jeselsohn R, Buchwalter G, De Angelis C,
Brown M and Schiff R: ESR1 mutations-a mechanism for acquired
endocrine resistance in breast cancer. Nat Rev Clin Oncol.
12:573–583. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Fribbens C, O'Leary B, Kilburn L, Hrebien
S, Garcia-Murillas I, Beaney M, Cristofanilli M, Andre F, Loi S,
Loibl S, et al: Plasma ESR1 mutations and the treatment of estrogen
Receptor-positive advanced breast cancer. J Clin Oncol.
34:2961–2968. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Wagner J, Rapsomaniki MA, Chevrier S,
Anzeneder T, Langwieder C, Dykgers A, Rees M, Ramaswamy A, Muenst
S, Soysal SD, et al: A Single-cell atlas of the tumor and immune
ecosystem of human breast cancer. Cell. 177:1330–1345.e18. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Ye J, Baer JM, Faget DV, Morikis VA, Ren
Q, Melam A, Delgado AP, Luo X, Bagchi SM, Belle JI, et al:
Senescent CAFs mediate immunosuppression and drive breast cancer
progression. Cancer Discov. 14:1302–1323. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Chandarlapaty S, Chen D, He W, Sung P,
Samoila A, You D, Bhatt T, Patel P, Voi M, Gnant M, et al:
Prevalence of ESR1 mutations in cell-free DNA and outcomes in
metastatic breast cancer: A secondary analysis of the BOLERO-2
clinical trial. JAMA Oncol. 2:1310–1315. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Magnani L, Frige G, Gadaleta RM, Corleone
G, Fabris S, Kempe MH, Verschure PJ, Barozzi I, Vircillo V, Hong
SP, et al: Acquired CYP19A1 amplification is an early specific
mechanism of aromatase inhibitor resistance in ERα metastatic
breast cancer. Nat Genet. 49:444–4450. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Pagani O, Regan MM, Walley BA, Fleming GF,
Colleoni M, Láng I, Gomez HL, Tondini C, Burstein HJ, Perez EA, et
al: Adjuvant exemestane with ovarian suppression in premenopausal
breast cancer. N Engl J Med. 371:107–118. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Francis PA, Pagani O, Fleming GF, Walley
BA, Colleoni M, Láng I, Gómez HL, Tondini C, Ciruelos E, Burstein
HJ, et al: Tailoring adjuvant endocrine therapy for premenopausal
breast cancer. N Engl J Med. 379:122–137. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Bellet M, Gray KP, Francis PA, Láng I,
Ciruelos E, Lluch A, Climent MA, Catalán G, Avella A, Bohn U, et
al: Twelve-Month estrogen levels in premenopausal women with
hormone Receptor-Positive breast cancer receiving adjuvant
triptorelin plus exemestane or tamoxifen in the suppression of
ovarian function trial (SOFT): The SOFT-EST substudy. J Clin Oncol.
34:1584–1593. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Tripathy D, Im S, Colleoni M, Franke F,
Bardia A, Harbeck N, Hurvitz SA, Chow L, Sohn J, Lee KS, et al:
Ribociclib plus endocrine therapy for premenopausal women with
hormone-receptor-positive, advanced breast cancer (MONALEESA-7): A
randomised phase 3 trial. Lancet Oncol. 19:904–915. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Lung Cancer Specialty Committee of Chinese
Elderly Health Care Association, Lung Cancer Specialty Committee of
Beijing Cancer Society, . Consensus of Chinese experts on medical
treatment of advanced lung cancer in the elderly (2022 edition).
Chin J Lung Cancer. 25:363–384. 2022.(In Chinese).
|
|
61
|
Breast Committee of Chinese Research
Hospital Association and Geriatric Oncology Sub-Committee of
Chinese Geriatric Society, Consensus Expert Group on Diagnosis,
Treatment of Elderly Breast Cancer in China, . Consensus on the
diagnosis and treatment of breast carcinoma in elderly Chinese
patients (2023 edition). Chin Res Hosp. 10:1–8. 2023.(In
Chinese).
|
|
62
|
Harbeck N, Brufsky A, Grace Rose C,
Korytowsky B, Chen C, Tantakoun K, Jazexhi E, Nguyen DHV, Bartlett
M, Samjoo IA and Pluard T: Real-world effectiveness and safety of
CDK4/6i in elderly and BIPOC patients with
HR+/HER2-advanced/metastatic breast cancer: An updated systematic
literature review. Front Oncol. 15:15770752025. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Jenkins S, Kachur ME, Rechache K, Wells JM
and Lipkowitz S: Rare breast cancer subtypes. Curr Oncol Rep.
23:542021. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Petrausch U and Pestalozzi BC: Distinct
clinical and prognostic features of invasive lobular breast cancer.
Breast Dis. 30:39–44. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Berx G and Van Roy F: The
E-cadherin/catenin complex: An important gatekeeper in breast
cancer tumorigenesis and malignant progression. Breast Cancer Res.
3:289–293. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
66
|
Cancer Genome Atlas Network, .
Comprehensive molecular portraits of human breast tumours. Nature.
490:61–70. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Ciriello G, Gatza ML, Beck AH, Wilkerson
MD, Rhie SK, Pastore A, Zhang H, McLellan M, Yau C, Kandoth C, et
al: Comprehensive molecular portraits of invasive lobular breast
cancer. Cell. 163:506–519. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Borst MJ and Ingold JA: Metastatic
patterns of invasive lobular versus invasive ductal carcinoma of
the breast. Surgery. 114:637–641. 1993.PubMed/NCBI
|
|
69
|
Metzger Filho O, Giobbie-Hurder A, Mallon
E, Gusterson B, Viale G, Winer EP, Thürlimann B, Gelber RD,
Colleoni M, Ejlertsen B, et al: Relative effectiveness of letrozole
compared with tamoxifen for patients with lobular carcinoma in the
BIG 1–98 trial. J Clin Oncol. 33:2772–2779. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Early Breast Cancer Trialists' and
Collaborative Group (EBCTCG), . Aromatase inhibitors versus
tamoxifen in early breast cancer: Patient-level meta-analysis of
the randomised trials. Lancet. 386:1341–1352. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Kumegawa K, Takahashi Y, Saeki S, Yang L,
Nakadai T, Osako T, Mori S, Noda T, Ohno S, Ueno T and Maruyama R:
GRHL2 motif is associated with intratumor heterogeneity of
cis-regulatory elements in luminal breast cancer. NPJ Breast
Cancer. 8:702022. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Fang K, Ohihoin AG, Liu T, Choppavarapu L,
Nosirov B, Wang Q, Yu XZ, Kamaraju S, Leone G and Jin VX:
Integrated single-cell analysis reveals distinct
epigenetic-regulated cancer cell states and a heterogeneity-guided
core signature in Tamoxifen-resistant breast cancer. Genome Med.
16:1342024. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Nolan E, Lindeman GJ and Visvader JE:
Deciphering breast cancer: From biology to the clinic. Cell.
186:1708–1728. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Azizi E, Carr AJ, Plitas G, Cornish AE,
Konopacki C, Prabhakaran S, Nainys J, Wu K, Kiseliovas V, Setty M,
et al: Single-Cell map of diverse immune phenotypes in the breast
tumor microenvironment. Cell. 174:1293–1308.e36. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Wu SZ, Al-Eryani G, Roden DL, Junankar S,
Harvey K, Andersson A, Thennavan A, Wang C, Torpy JR, Bartonicek N,
et al: A single-cell and spatially resolved atlas of human breast
cancers. Nat Genet. 53:1334–1347. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Sachs N, de Ligt J, Kopper O, Gogola E,
Bounova G, Weeber F, Balgobind AV, Wind K, Gracanin A, Begthel H,
et al: A living biobank of breast cancer organoids captures disease
heterogeneity. Cell. 172:373–386.e10. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Liu YM, Ge JY, Chen YF, Liu T, Chen L, Liu
CC, Ma D, Chen YY, Cai YW, Xu YY, et al: Combined Single-Cell and
spatial transcriptomics reveal the metabolic evolvement of breast
cancer during early dissemination. Adv Sci (Weinh).
10:e22053952023. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Spoerke JM, Gendreau S, Walter K, Qiu J,
Wilson TR, Savage H, Aimi J, Derynck MK, Chen M, Chan IT, et al:
Heterogeneity and clinical significance of ESR1 mutations in
ER-positive metastatic breast cancer patients receiving
fulvestrant. Nat Commun. 7:115792016. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Wang P, Bahreini A, Gyanchandani R, Lucas
PC, Hartmaier RJ, Watters RJ, Jonnalagadda AR, Trejo Bittar HE,
Berg A, Hamilton RL, et al: Sensitive detection of Mono- and
polyclonal ESR1 mutations in primary tumors, metastatic lesions,
and cell-free DNA of breast cancer patients. Clin Cancer Res.
22:1130–1137. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Dahlgren M, George AM, Brueffer C,
Gladchuk S, Chen Y, Vallon-Christersson J, Hegardt C, Häkkinen J,
Rydén L, Malmberg M, et al: Preexisting somatic mutations of
estrogen receptor alpha (ESR1) in Early-Stage primary breast
cancer. JNCI Cancer Spectr. 5:pkab0282021. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Kim H, Whitman AA, Wisniewska K, Kakati
RT, Garcia-Recio S, Calhoun BC, Franco HL, Perou CM and Spanheimer
PM: Tamoxifen response at Single-cell resolution in estrogen
receptor-positive primary human breast tumors. Clin Cancer Res.
29:4894–4907. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Dini A, Barker H, Piki E, Sharma S,
Raivola J, Murumägi A and Ungureanu D: A multiplex single-cell
RNA-Seq pharmacotranscriptomics pipeline for drug discovery. Nat
Chem Biol. 21:432–442. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Yuan J, Yang L, Li Z, Zhang H, Wang Q,
Huang J, Wang B, Mohan CD, Sethi G and Wang G: The role of the
tumor microenvironment in endocrine therapy resistance in hormone
receptor-positive breast cancer. Front Endocrinol (Lausanne).
14:12612832023. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Bartoschek M, Oskolkov N, Bocci M, Lövrot
J, Larsson C, Sommarin M, Madsen CD, Lindgren D, Pekar G, Karlsson
G, et al: Spatially and functionally distinct subclasses of breast
cancer-associated fibroblasts revealed by single cell RNA
sequencing. Nat Commun. 9:51502018. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Fribbens C, Garcia Murillas I, Beaney M,
Hrebien S, O'Leary B, Kilburn L, Howarth K, Epstein M, Green E,
Rosenfeld N, et al: Tracking evolution of aromatase inhibitor
resistance with circulating tumour DNA analysis in metastatic
breast cancer. Ann Oncol. 29:145–153. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Caldwell BA, Wu Y, Wang J and Li L:
Altered DNA methylation underlies monocyte dysregulation and immune
exhaustion memory in sepsis. Cell Rep. 43:1138942024. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Xiong S, Song K, Xiang H and Luo G:
Dual-target inhibitors based on ERα: Novel therapeutic approaches
for endocrine resistant breast cancer. Eur J Med Chem.
270:1163932024. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Svensson V, da Veiga Beltrame E and
Pachter L: A curated database reveals trends in Single-cell
transcriptomics. Nat Methods. 17:795–799. 2020.
|
|
89
|
Luecken MD and Theis FJ: Current best
practices in single-cell RNA-seq analysis: A tutorial. Mol Syst
Biol. 15:e87462019. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Regev A, Teichmann SA, Lander ES, Amit I,
Benoist C, Birney E, Bodenmiller B, Campbell P, Carninci P,
Clatworthy M, et al: The human cell atlas. Elife. 6:e270412017.
View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Stuart T, Butler A, Hoffman P, Hafemeister
C, Papalexi E, Mauck WM III, Hao Y, Stoeckius M, Smibert P and
Satija R: Comprehensive integration of single-cell data. Cell.
177:1888–1902.e21. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Tran HTN, Ang KS, Chevrier M, Zhang X, Lee
NYS, Goh M and Chen J: A benchmark of batch-effect correction
methods for single-cell RNA-seq data. Genome Biol. 21:122020.
View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Kiselev VY, Andrews TS and Hemberg M:
Challenges in unsupervised clustering of single-cell RNA-seq data.
Nat Rev Genet. 20:273–282. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Hicks SC, Townes FW, Teng M and Irizarry
RA: Missing data and technical variability in single-cell
RNA-sequencing experiments. Biostatistics. 19:562–578. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Sachs N and Clevers H: Organoid cultures
for the analysis of cancer phenotypes. Curr Opin Genet Dev.
24:68–73. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Dhimolea E, de Matos Simoes R, Kansara D,
Weng X, Sharma S, Awate P, Liu Z, Gao D, Mitsiades N, Schwab JH, et
al: Pleiotropic mechanisms drive endocrine resistance in the
Three-dimensional bone microenvironment. Cancer Res. 81:371–383.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Rosenbluth JM, Schackmann RCJ, Gray GK,
Selfors LM, Li CM, Boedicker M, Kuiken HJ, Richardson A, Brock J,
Garber J, et al: Organoid cultures from normal and cancer-prone
human breast tissues preserve complex epithelial lineages. Nat
Commun. 11:17112020. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Wu H, Wang W, Zhang Y, Chen Y, Shan C, Li
J, Jia Y, Li C, Du C, Cai Y, et al: Establishment of
patient-derived organoids for guiding personalized therapies in
breast cancer patients. Int J Cancer. 155:324–338. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Vlachogiannis G, Hedayat S, Vatsiou A,
Jamin Y, Fernández-Mateos J, Khan K, Lampis A, Eason K, Huntingford
I, Burke R, et al: Patient-derived organoids model treatment
response of metastatic gastrointestinal cancers. Science.
359:920–926. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Pan B, Li X, Zhao D, Li N, Wang K, Li M
and Zhao Z: Optimizing individualized treatment strategy based on
breast cancer organoid model. Clin Transl Med. 11:e3802021.
View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Chen P, Zhang X, Ding R, Yang L, Lyu X,
Zeng J, Lei JH, Wang L, Bi J, Shao N, et al: Patient-Derived
organoids can guide Personalized-therapies for patients with
advanced breast cancer. Adv Sci (Weinh). 8:e21011762021. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Bruna A, Rueda OM, Greenwood W, Batra AS,
Callari M, Batra RN, Pogrebniak K, Sandoval J, Cassidy JW,
Tufegdzic-Vidakovic A, et al: A biobank of breast cancer explants
with preserved Intra-tumor heterogeneity to screen anticancer
compounds. Cell. 167:260–274.e22. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Ma S, Tang T, Probst G, Konradi A, Jin C,
Li F, Gutkind JS, Fu XD and Guan KL: Transcriptional repression of
estrogen receptor alpha by YAP reveals the Hippo pathway as
therapeutic target for ER+ breast cancer. Nat Commun. 13:10612022.
View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Guillen KP, Fujita M, Butterfield AJ,
Scherer SD, Bailey MH, Chu Z, DeRose YS, Zhao L, Cortes-Sanchez E,
Yang CH, et al: A human breast cancer-derived xenograft and
organoid platform for drug discovery and precision oncology. Nat
Cancer. 3:232–250. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Önder CE, Ziegler TJ, Becker R, Brucker
SY, Hartkopf AD, Engler T and Koch A: Advancing cancer therapy
predictions with Patient-derived organoid models of metastatic
breast cancer. Cancers (Basel). 15:36022023. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Guan D, Liu X, Shi Q, He B, Zheng C and
Meng X: Breast cancer organoids and their applications for
precision cancer immunotherapy. World J Surg Oncol. 21:3432023.
View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Ma X, Wang Q, Li G, Li H, Xu S and Pang D:
Cancer organoids: A platform in basic and translational research.
Genes Dis. 11:614–632. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Yin S, Xi R, Wu A, Wang S, Li Y, Wang C,
Tang L, Xia Y, Yang D, Li J, et al: Patient-derived tumor-like cell
clusters for drug testing in cancer therapy. Sci Transl Med.
12:eaaz17232020. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Lancaster MA and Knoblich JA:
Organogenesis in a dish: Modeling development and disease using
organoid technologies. Science. 345:12471252014. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Drost J and Clevers H: Organoids in cancer
research. Nat Rev Cancer. 18:407–418. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Huch M, Gehart H, van Boxtel R, Hamer K,
Blokzijl F, Verstegen MM, Ellis E, van Wenum M, Fuchs SA, de Ligt
J, et al: Long-term culture of genome-stable bipotent stem cells
from adult human liver. Cell. 160:299–312. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Gjorevski N, Sachs N, Manfrin A, Giger S,
Bragina ME, Ordóñez-Morán P, Clevers H and Lutolf MP: Designer
matrices for intestinal stem cell and organoid culture. Nature.
539:560–564. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Fatehullah A, Tan SH and Barker N:
Organoids as an in vitro model of human development and disease.
Nat Cell Biol. 18:246–254. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Neal JT, Li X, Zhu J, Giangarra V,
Grzeskowiak CL, Ju J, Liu IH, Chiou SH, Salahudeen AA, Smith AR, et
al: Organoid modeling of the tumor immune microenvironment. Cell.
175:1972–1988.e16. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Szymański P, Markowicz M and
Mikiciuk-Olasik E: Adaptation of high-throughput screening in drug
discovery-toxicological screening tests. Int J Mol Sci. 13:427–452.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Sun A, Moore TW, Gunther JR, Kim MS,
Rhoden E, Du Y, Fu H, Snyder JP and Katzenellenbogen JA:
Discovering small-molecule estrogen receptor α/coactivator binding
inhibitors: High-throughput screening, ligand development, and
models for enhanced potency. ChemMedChem. 6:654–666. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Gligorich KM, Vaden RM, Shelton DN, Wang
G, Matsen CB, Looper RE, Sigman MS and Welm BE: Development of a
screen to identify selective small molecules active against
patient-derived metastatic and chemoresistant breast cancer cells.
Breast Cancer Res. 15:R582013. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
He C, Han S, Chang Y, Wu M, Zhao Y, Chen C
and Chu X: CRISPR screen in cancer: Status quo and future
perspectives. Am J Cancer Res. 11:1031–1050. 2021.PubMed/NCBI
|
|
119
|
Zhong L, Li Y, Xiong L, Wang W, Wu M, Yuan
T, Yang W, Tian C, Miao Z, Wang T and Yang S: Small molecules in
targeted cancer therapy: Advances, challenges, and future
perspectives. Signal Transduct Target Ther. 6:2012021. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Tuijnenburg P, Aan de Kerk DJ, Jansen MH,
Morris B, Lieftink C, Beijersbergen RL, van Leeuwen EMM and
Kuijpers TW: High-throughput compound screen reveals mTOR
inhibitors as potential therapeutics to reduce (auto)antibody
production by human plasma cells. Eur J Immunol. 50:73–85. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Yu K, Toral-Barza L, Shi C, Zhang WG,
Lucas J, Shor B, Kim J, Verheijen J, Curran K, Malwitz DJ, et al:
Biochemical, cellular, and in vivo activity of novel
ATP-competitive and selective inhibitors of the mammalian target of
rapamycin. Cancer Res. 69:6232–6240. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Baselga J, Campone M, Piccart M, Burris HA
III, Rugo HS, Sahmoud T, Noguchi S, Gnant M, Pritchard KI, Lebrun
F, et al: Everolimus in postmenopausal hormone-receptor-positive
advanced breast cancer. N Engl J Med. 366:520–529. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
123
|
André F, Ciruelos E, Rubovszky G, Campone
M, Loibl S, Rugo HS, Iwata H, Conte P, Mayer IA, Kaufman B, et al:
Alpelisib for PIK3CA-mutated, hormone receptor-positive advanced
breast cancer. N Engl J Med. 380:1929–1940. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Turner NC, Oliveira M, Howell SJ, Dalenc
F, Cortes J, Gomez Moreno HL, Hu X, Jhaveri K, Krivorotko P, Loibl
S, et al: Capivasertib in hormone receptor-positive advanced breast
cancer. N Engl J Med. 388:2058–2070. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Wang J, Gong GQ, Zhou Y, Lee WJ, Buchanan
CM, Denny WA, Rewcastle GW, Kendall JD, Dickson JMJ, Flanagan JU,
et al: High-throughput screening campaigns against a PI3Kα isoform
bearing the H1047R mutation identified potential inhibitors with
novel scaffolds. Acta Pharmacol Sin. 39:1816–1822. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Courtney KD, Corcoran RB and Engelman JA:
The PI3K pathway as drug target in human cancer. J Clin Oncol.
28:1075–1083. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Miller TW, Balko JM and Arteaga CL:
Phosphatidylinositol 3-kinase and antiestrogen resistance in breast
cancer. J Clin Oncol. 29:4452–4461. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Stemke-Hale K, Gonzalez-Angulo AM, Lluch
A, Neve RM, Kuo WL, Davies M, Carey M, Hu Z, Guan Y, Sahin A, et
al: An integrative genomic and proteomic analysis of PIK3CA, PTEN,
and AKT mutations in breast cancer. Cancer Res. 68:6084–6091. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Razavi P, Chang MT, Xu G, Bandlamudi C,
Ross DS, Vasan N, Cai Y, Bielski CM, Donoghue MTA, Jonsson P, et
al: The genomic landscape of endocrine-resistant advanced breast
cancers. Nat Genet. 50:1426–1431. 2018.PubMed/NCBI
|
|
130
|
Kwon KK, Lee J, Kim H, Lee DH and Lee SG:
Advancing high-throughput screening systems for synthetic biology
and biofoundry. Curr Opin Systems Biol. 37:1004872024. View Article : Google Scholar
|
|
131
|
De Stefano P, Bianchi E and Dubini G: The
impact of microfluidics in high-throughput drug-screening
applications. Biomicrofluidics. 16:0315012022. View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Serrano DR, Luciano FC, Anaya BJ, Ongoren
B, Kara A, Molina G, Ramirez BI, Sánchez-Guirales SA, Simon JA,
Tomietto G, et al: Artificial intelligence (AI) applications in
drug discovery and drug delivery: Revolutionizing personalized
medicine. Pharmaceutics. 16:13282024. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Alakwaa FM, Chaudhary K and Garmire LX:
Deep learning accurately predicts estrogen receptor status in
breast cancer metabolomics data. J Proteome Res. 17:337–347. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Jiang YZ, Ma D, Jin X, Xiao Y, Yu Y, Shi
J, Zhou YF, Fu T, Lin CJ, Dai LJ, et al: Integrated multiomic
profiling of breast cancer in the Chinese population reveals
patient stratification and therapeutic vulnerabilities. Nat Cancer.
5:673–690. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Zhang H, Yang F, Xu Y, Zhao S, Jiang YZ,
Shao ZM and Xiao Y: Multimodal integration using a machine learning
approach facilitates risk stratification in HR+/HER2-breast cancer.
Cell Rep Med. 6:1019242025. View Article : Google Scholar : PubMed/NCBI
|
|
136
|
Turnbull AK, Arthur LM, Renshaw L,
Larionov AA, Kay C, Dunbier AK, Thomas JS, Dowsett M, Sims AH and
Dixon JM: Accurate prediction and validation of response to
endocrine therapy in breast cancer. J Clin Oncol. 33:2270–2278.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
137
|
Sgroi DC, Treuner K, Zhang Y, Piper T,
Salunga R, Ahmed I, Doos L, Thornber S, Taylor KJ, Brachtel E, et
al: Correlative studies of the breast cancer index (HOXB13/IL17BR)
and ER, PR, AR, AR/ER ratio and Ki67 for prediction of extended
endocrine therapy benefit: A Trans-aTTom study. Breast Cancer Res.
24:902022. View Article : Google Scholar : PubMed/NCBI
|
|
138
|
Mosly D, Turnbull A, Sims A, Ward C and
Langdon S: Predictive markers of endocrine response in breast
cancer. World J Exp Med. 8:1–7. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
139
|
Sammut SJ, Crispin-Ortuzar M, Chin SF,
Provenzano E, Bardwell HA, Ma W, Cope W, Dariush A, Dawson SJ,
Abraham JE, et al: Multi-omic machine learning predictor of breast
cancer therapy response. Nature. 601:623–629. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Wu X, Li Y, Chen J, Chen J, Zhang W, Lu X,
Zhong X, Zhu M, Yi Y and Bu H: Multimodal recurrence risk
prediction model for HR+/HER2-early breast cancer following
adjuvant chemo-endocrine therapy: Integrating pathology image and
clinicalpathological features. Breast Cancer Res. 27:272025.
View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Gu JY, Zhang JF, Zeng SL, Zhang WY, Xia
RP, Wang XX, Zhou Q, Guo SX, Wang HZ and Chen ZS: Artificial
intelligence in tumor drug resistance: Mechanisms and treatment
prospects. Intelligent Oncol. 1:73–88. 2025. View Article : Google Scholar
|
|
142
|
Mao Y, Shangguan D, Huang Q, Xiao L, Cao
D, Zhou H and Wang YK: Emerging artificial intelligence-driven
precision therapies in tumor drug resistance: Recent advances,
opportunities, and challenges. Mol Cancer. 24:1232025. View Article : Google Scholar : PubMed/NCBI
|
|
143
|
Saha S, Mahapatra S, Khanra S, Mishra B,
Swain B, Malhotra D, Saha S, Panda VK, Kumari K, Jena S, et al:
Decoding breast cancer treatment resistance through genetic,
epigenetic, and immune-regulatory mechanisms: From molecular
insights to translational perspectives. Cancer Drug Resist.
8:362025.PubMed/NCBI
|
|
144
|
Eckardt JN, Wendt K, Bornhäuser M and
Middeke JM: Reinforcement learning for precision oncology. Cancers
(Basel). 13:46242021. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Jayaraman P, Desman J, Sabounchi M,
Nadkarni GN and Sakhuja A: A primer on reinforcement learning in
medicine for clinicians. NPJ Digit Med. 7:3372024. View Article : Google Scholar : PubMed/NCBI
|
|
146
|
Bozcuk HŞ and Artaç M: A simulated trial
with reinforcement learning for the efficacy of Irinotecan and
Ifosfamide versus Topotecan in relapsed, extensive stage small cell
lung cancer. BMC Cancer. 24:12072024. View Article : Google Scholar : PubMed/NCBI
|
|
147
|
Lu Y, Chu Q, Li Z, Wang M, Gatenby R and
Zhang Q: Deep reinforcement learning identifies personalized
intermittent androgen deprivation therapy for prostate cancer.
Brief Bioinform. 25:bbae0712024. View Article : Google Scholar : PubMed/NCBI
|
|
148
|
Zhao M, Hanson KA, Zhang Y, Zhou A and
Cha-Silva AS: Place in therapy of Cyclin-dependent Kinase 4/6
inhibitors in breast cancer: A targeted literature review. Target
Oncol. 18:327–358. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Kappel C, Elliott MJ, Kumar V, Nadler MB,
Desnoyers A and Amir E: Comparative overall survival of CDK4/6
inhibitors in combination with endocrine therapy in advanced breast
cancer. Sci Rep. 14:31292024. View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Rudin C: Stop explaining black box machine
learning models for high stakes decisions and use interpretable
models instead. Nat Mach Intell. 1:206–215. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
151
|
Topol EJ: High-performance medicine: The
convergence of human and artificial intelligence. Nat Med.
25:44–56. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
152
|
Lundberg SM and Lee SI: A unified approach
to interpreting model predictions. Adv Neural Inf Process Syst.
30:4768–4777. 2017.PubMed/NCBI
|
|
153
|
Beam AL and Kohane IS: Big data and
machine learning in health care. JAMA. 319:1317–1318. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
154
|
Collins GS, Reitsma JB, Altman DG and
Moons KG: Transparent reporting of a multivariable prediction model
for individual prognosis or diagnosis (TRIPOD): The TRIPOD
statement. BMJ. 350:g75942015. View Article : Google Scholar : PubMed/NCBI
|
|
155
|
Liu X, Cruz Rivera S, Moher D, Calvert MJ
and Denniston AK; SPIRIT-AI; CONSORT-AI Working Group, : Reporting
guidelines for clinical trial reports for interventions involving
artificial intelligence: The CONSORT-AI extension. Lancet Digit
Health. 2:e537–e548. 2020. View Article : Google Scholar : PubMed/NCBI
|