Introduction
Matrix metalloproteinases (MMPs) and their tissue
inhibitors (TIMPs) are controllers of extracellular matrix
turnover. Both MMP and TIMP expressions are found to be altered in
benign and malignant tumors, as well as during invasion and
metastasis which require the breakdown and removal of extracellular
matrix (1).
The presence of MMPs in ovarian cancer and their
contribution to the invasive phenotype of these tumors have been
documented in both in vitro and clinical studies.
Immunochemistry and Western blot analysis have shown higher
activated MMP-2 in epithelial ovarian carcinomas than in benign
tumors (2,3). High levels of MMP-9 have been found in
human ovarian carcinoma xenografts and overexpression of MMP-7 in
ovarian cancer cell lines and cancer surgical specimens (3,4).
MT1-MMP has been shown to regulate cell proliferation, cell
mobility, invasiveness and differentiation (5). The expression of TIMP-1 was higher in
malignant and borderline tumors than in benign tumors and strong
TIMP-2 immunostaining has been found in serous ovarian carcinomas
(6,7).
About 15 studies have been published on the
prognostic value of MMP-2, MMP-7, MMP-9, MT1-MMP, TIMP-1 or TIMP-2
in ovarian cancers, but the results remain controversial. Most of
these MMPs and TIMPs have been shown to be overexpressed in tumors,
peritoneal implants or metastatic lesions, and associated with poor
outcome (2,8-13). On
the other hand, a strong MMP-2, MMP-9 or MMP-7 signal in cancer
cells has been found to predict better survival (14–16).
However, most of the previous studies evaluated MMPs and TIMPs
separately in ovarian neoplasms, and little is known of their
concomitant expression in epithelial ovarian cancers. We therefore,
used a translational approach to analyze the epithelial and stromal
expressions of MMP-2, MMP-7, MMP-9, MT1-MMP, TIMP-1 and TIMP-2 in
advanced epithelial ovarian cancers and to assess their prognostic
value.
Materials and methods
Patients and tumors
Ovarian tissue samples were obtained from all the
patients who underwent surgery consecutively for FIGO stage III and
IV epithelial ovarian cancer in the Gynecology Department of Tenon
Hospital, Paris, from 2001 to 2006.
All the tumors were reviewed to confirm histological
diagnosis. Histological typing followed the FIGO recommendations
(17). Epidemiological
characteristics, recurrence and survival were recorded for all
patients. The study was approved by the Ethics Committee of the
College National des Gynécologues et Obstétriciens Français.
Tissue microarray (TMA) and
immunohistochemistry
Formalin-fixed, paraffin-embedded tumor samples were
used to construct a TMA, as previously described (18). Briefly, after selection of a
representative tumor region from each tumor block, tissue cylinders
were punched with the use of a custom-made precision instrument
(Beecher Instruments, Silver Spring, MD) and transferred to a 25 ×
35 mm paraffin block under microscopic control. TMA blocks were cut
into 4 μm sections and transferred to glass slides (19). Separate sections from the TMA blocks
were used for immunohistochemical analysis, using the Ventana Nexes
automated immunohistochemistry system (Ventana Medical Systems,
Tucson, AZ).
Purified mouse monoclonal or rabbit polyclonal
antibodies against human MMP-2, -7, -9, MT1-MMP, TIMP-1, and -2
were used as primary antibodies at various concentrations: MMP-2
(mouse; clone 42-5D11; Calbiochem, San Diego, CA; 5 μg/ml), MMP-7
(mouse; clone ID2; Lab Vision Corp., Fremont, CA; 1.3 μg/ml), MMP-9
(mouse; clone 56-2A4; Calbiochem; 20 μg/ml), MT1-MMP (rabbit; Lab
Vision Corp.; 8 μg/ml), TIMP-1 (mouse; clone 102D1; Lab Vision
Corp.; 8 μg/ml), and TIMP-2 (mouse; clone 3A4; Lab Vision Corp.; 4
μg/ml).
Prior to the primary antibody staining an antigen
retrieval step was used combined with a high temperature
antigen-unmasking technique (Dako Target Retrieval Solution,
Glostrup, Denmark; 100°C, 30 min). For MMP-7, antigen unmasking was
achieved with proteinase K, 4 min. The automated procedure is based
on an indirect biotin-avidin system with a universal biotinylated
immunoglobulin as secondary antibody, diaminobenzidine as
substrate, and hematoxylin as counterstain. Except for MT1-MMP, a
Ventana amplification kit was used in addition to the automated
procedure (Ventana Medical Systems).
Positive controls for MMP-2, MMP-7, MMP-9, MT1-MMP,
TIMP-1 and TIMP-2 were sections of endometrial cancers which had
been strongly stained in a previous study (20). For negative control, the primary
antibody was replaced by an irrelevant non-immune mouse antibody of
the same immunoglobulin G subtype.
Semiquantitative analysis
The TMA was analyzed by light microscopy by use of a
×10 objective. Immunostaining results were scored by JLB and AC
independently, using the HSCORE (21). The HSCORE was produced by
multiplying the percentage of stained tumor cells (0–100%) with the
intensity score. The intensity of staining was scored on a 4-point
scale: 0, no staining; 1, weak; 2, moderate; 3, intense. Thus, each
score ranged 0–300. For each tumor specimen, the HSCORE of a given
MMP or TIMP was assessed in epithelial and stromal cells.
Discordance between the two examiners never exceeded 5%.
Statistical analysis
Continuous variables were compared with Student’s
t-test and categorical variables were compared with the
χ2 test or Fisher’s exact test, as appropriate. P-values
<0.05 were considered statistically significant. Because of
multiple comparisons in MMP and TIMP expressions, Bonferroni
correction was used to determine the significance levels of
two-tailed P-values (22). This was
achieved by dividing the common P-value border 0.05 by the number
of comparisons.
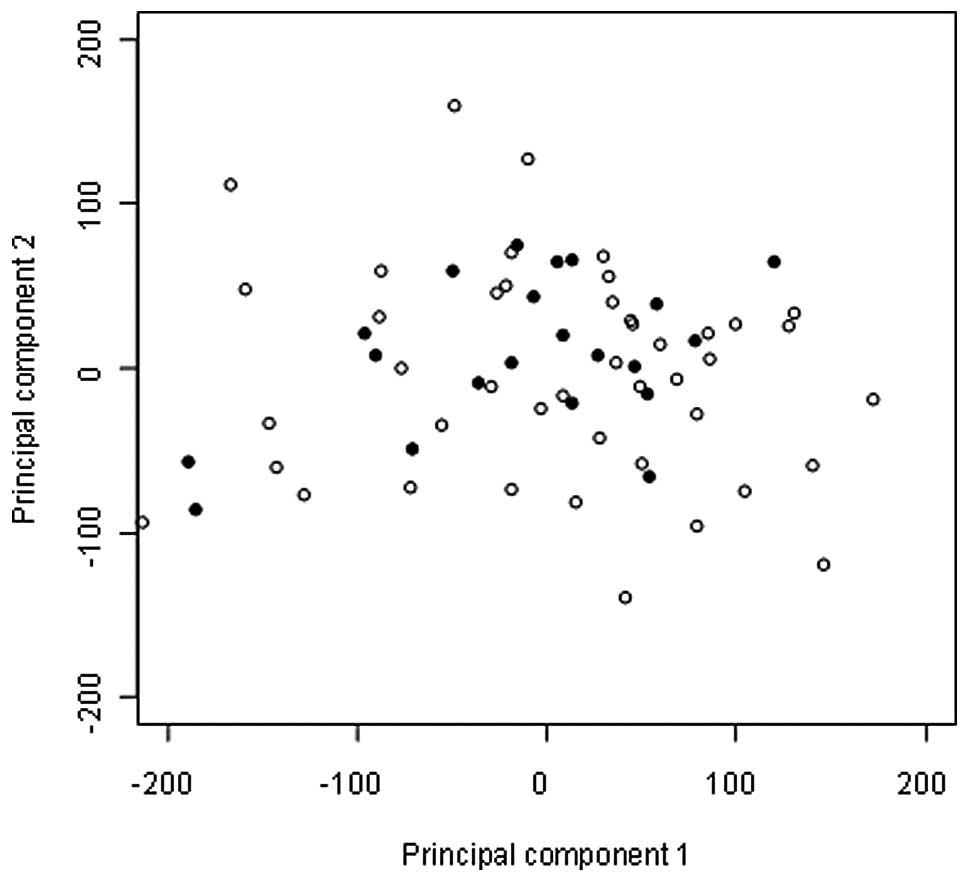
Unsupervised analysis was performed to organize the
results of TMA immunostaining into meaningful structures. Classical
Multidimensional Scaling (CMDS), also known as Principal Component
Analysis, is a transformation procedure used to reduce
multidimensional data sets to lower dimensions for analysis. This
procedure provides information about the spatial ‘proximity’
(similarity) or ‘distance’ (difference) in a multidimensional space
where each dimension is one marker of the panel. Results of CMDS
can be plotted into the most informative two-dimensional
construction in which one point represents one tumor.
The performance of each MMP was quantified with
respect to discrimination. Discrimination (i.e., whether the
relative ranking of individual predictions is in the correct order)
was quantified with the concordance index (C index) and its 95%
confidence interval, which is similar to the area under the
receiver operating characteristic curve (AUROC) but appropriate for
censored data. The C index is the probability that given two
randomly selected patients, the patient with the worse score will
actually have a worse outcome. It ranges from 0 to 1, with 1
indicating perfect concordance, 0.5 indicating no better
concordance than chance, and 0 indicating perfect discordance. The
optimal threshold for each MMP was determined using the function
‘optimal.thresholds’ (PresenceAbsence) of the R package.
Survival curves were constructed according to
Kaplan-Meier method. Survival was defined from primary surgery or
the beginning of neoadjuvant chemotherapy to date of death and
evaluated in 2007. Kaplan-Meier survival curves were calculated
using univariate analysis and compared by the log-rank test.
Statistical significance was set at P<0.05.
All analyses were performed using the R package
(http://lib.stat.cmu.edu/R/CRAN/).
Results
Patients and tumors
Out of the 69 patients included, 43 (62%) underwent
primary surgery and the remaining 26 (38%) were treated by
neoadjuvant chemotherapy followed by interval surgery. Clinical and
biological characteristics were not significantly different between
the groups: median age 64 years (range 26–84) and 62 years (range
21–76) respectively; FIGO stages III in 41/43 patients (95%) and
22/26 patients (85%), respectively; peritoneal carcinomatosis in
35/43 patients (81%) and 18/26 patients (69%), respectively; median
CA125 plasmatic level 395 U/ml (range 43–8845) and 988 U/ml (range
34–31210), respectively.
Epithelial and stromal expressions of MMPs and TIMPs
were determined in 92% (range, 89–94) and 98% (range, 97–99) of
tissue samples. Immunostaining data for all markers were available
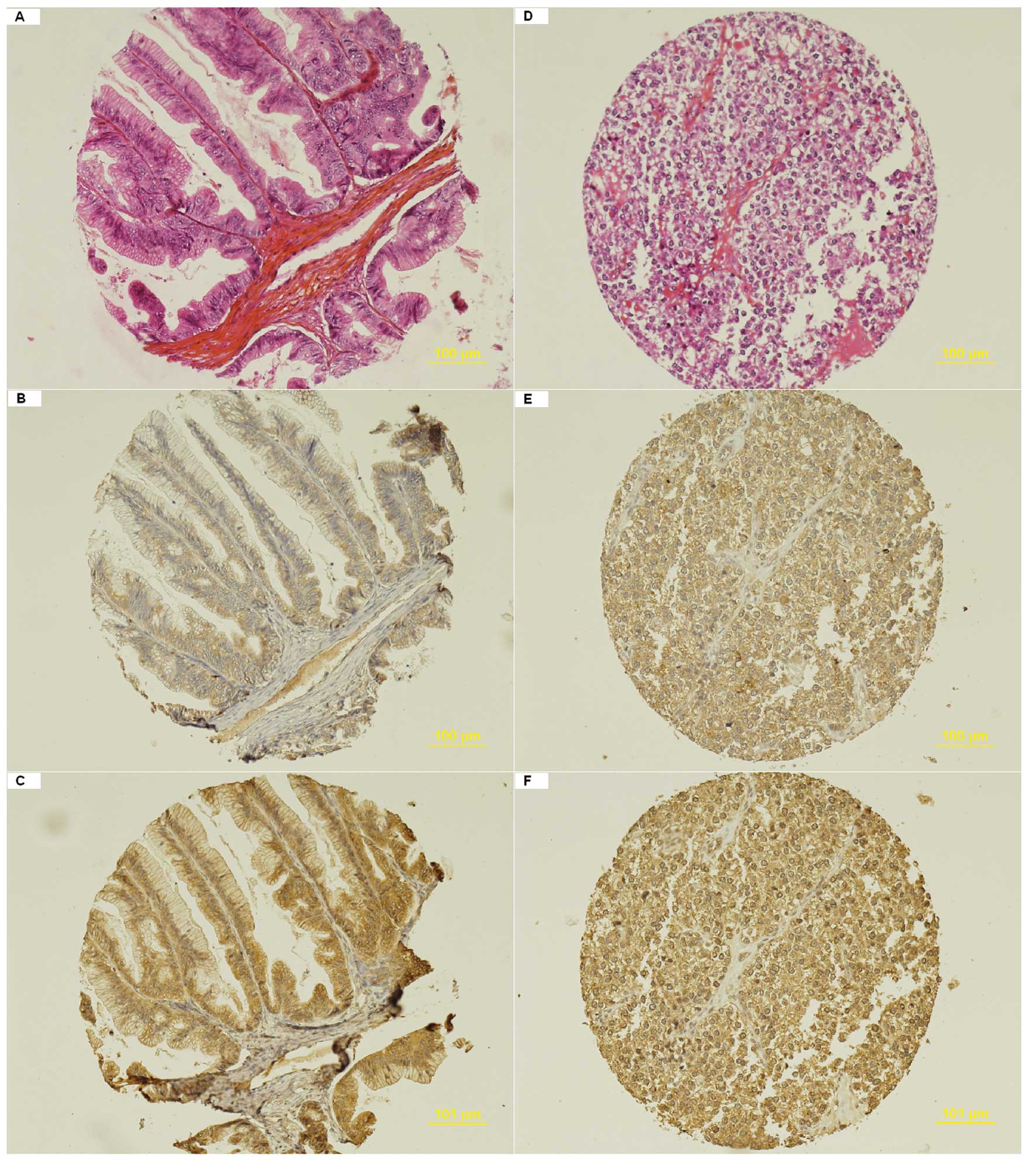
in 58 of the 69 patients (84%). The mean (SD) epithelial HSCORE
values of MMPs and TIMPs were as follows: MMP-2, 96 (47); MMP-7, 66
(59); MMP-9, 133 (47); MT1-MMP, 120 (67); TIMP-1, 84 (44); TIMP-2,
151 (46). The mean (SD) stromal HSCORE values of MMPs and TIMPs
were as follows: MMP-2, 31 (40); MMP-7, 11 (19); MMP-9, 25 (19); MT1-MMP, 11 (12); TIMP-1, 6 (8); TIMP-2, 31 (23). Representative cases of
haematoxylin-eosin stained sections, MMP-9 expression and TIMP-2
expression in two specimens are shown in Fig. 1.
The histological and immunohistological
characteristics of the tumors according to primary or interval
surgery are shown in Table I. No
histological difference was observed between the groups except for
tumor size which was significantly reduced after neoadjuvant
chemotherapy. Immunohistochemistry showed epithelial expressions of
MMPs and TIMPs to be higher in tumors from patients treated by
primary surgery than those undergoing interval surgery. P-values
<0.05 were obtained for epithelial MT1-MMP and TIMP-2. However,
none of these differences remained significant after Bonferroni
correction.
 | Table IHistological and immunohistological
characteristics of the tumors according to primary or interval
surgery. |
Table I
Histological and immunohistological
characteristics of the tumors according to primary or interval
surgery.
| Tumor
characteristics | Primary surgery
(n=43) (%) | Interval surgery
(n=26) (%) | P-valuea |
|---|
| Tumor size (mm) | 96 (47) | 69 (53) | 0.042 |
| Histology |
| Serous (n=40) | 24 (56) | 16 (61) | 0.236 |
| Mucinous (n=2) | 1 (2) | 1 (4) | |
| Endometrioid
(n=15) | 9 (21) | 6 (23) | |
| Clear cells
(n=7) | 7 (16) | 0 | |
| Other (n=5) | 2 (5) | 3 (12) | |
| Grade |
| Well differentiated
(n=7) | 5 (12) | 2 (8) | 0.867 |
| Moderately
differentiated (n=32) | 19 (44) | 13 (50) | |
| Poorly
differentiated (n=26) | 17 (39) | 9 (34) | |
| Not determined
(n=4) | 2 (5) | 2 (8) | |
| Lymphovascular space
involvement |
| No (n=46) | 26 (61) | 20 (77) | 0.320 |
| Yes (n=22) | 16 (37) | 6 (23) | |
| Not determined
(n=1) | 1 (2) | 0 | |
| Lymph node
involvement when sampled |
| Not involved,
N− (n=15) | 8 (33) | 7 (47) | 0.405 |
| Involved,
N+ (n=24) | 16 (66) | 8 (53) | |
| MMP-2 |
| Epithelial | 98 (43) | 93 (54) | 0.689 |
| Stromal | 25 (37) | 41 (43) | 0.142 |
| MMP-7 |
| Epithelial | 73 (66) | 54 (43) | 0.192 |
| Stromal | 9 (16) | 15 (23) | 0.217 |
| MMP-9 |
| Epithelial | 139 (45) | 121 (48) | 0.125 |
| Stromal | 25 (21) | 25 (17) | 0.878 |
| MT1-MMP |
| Epithelial | 132 (72) | 97 (49) | 0.049 |
| Stromal | 12 (15) | 8 (7) | 0.232 |
| TIMP-1 |
| Epithelial | 85 (46) | 82 (42) | 0.804 |
| Stromal | 6 (8) | 7 (8) | 0.609 |
| TIMP-2 |
| Epithelial | 159 (44) | 135 (47) | 0.041 |
| Stromal | 31 (26) | 31 (17) | 0.990 |
Cytoreductive surgery
Cytoreductive surgery was considered optimal
(residual tumor ≤1 cm) in 27/43 patients (63%) treated by primary
surgery and in 18/26 patients (69%) treated by interval
surgery.
Clinical and biological characteristics (age, FIGO
stage, CA125 plasmatic level) were not significantly different in
patients with optimal cytoreduction and in patients with suboptimal
cytoreduction. However, peritoneal carcinomatosis was present in
30/45 patients (66%) with optimal cytoreduction and in 22/24
patients (96%) with suboptimal cytoreduction (P=0.007).
The histological and immunohistological
characteristics of the tumors according to optimal or suboptimal
cytoreduction are shown in Table
II. There was no significant histological difference between
the groups. Lymphovascular space involvement tended to be more
present in tumors from patients with suboptimal cytoreduction.
Immunohistochemistry showed that expressions of epithelial MMP-9
and TIMP-2 were higher in patients with suboptimal cytoreduction
than in patients with optimal cytoreduction (P<0.05). However,
only the difference in epithelial MMP-9 was considered significant
after Bonferroni correction. The epithelial and stromal levels of
the other MMPs and TIMPs were not different in tumors from patients
with optimal or suboptimal cytoreduction.
| Table IIHistological and immunohistological
characteristics of the tumors according to optimal or suboptimal
cytoreduction. |
Table II
Histological and immunohistological
characteristics of the tumors according to optimal or suboptimal
cytoreduction.
|
Characteristics | Optimal
cytoreduction (n=45) (%) | Suboptimal
cytoreduction (n=24) (%) | P-valuea |
|---|
| Mean tumor size, mm
(SD) | 86 (51) | 87 (51) | 0.907 |
| 75 (25–220) | 65 (25–180) | 0.839 |
| Histology |
| Serous (n=41) | 27 (60) | 13 (54) | 0.885 |
| Mucinous
(n=2) | 1 (2) | 1 (4) | |
| Endometrioid
(n=15) | 9 (20) | 6 (25) | |
| Clear cells
(n=7) | 4 (9) | 3 (13) | |
| Other (n=5) | 4 (9) | 1 (4) | |
| Grade |
| Well
differentiated (n=7) | 5 (11) | 2 (8) | 0.629 |
| Moderately
differentiated (n=32) | 22 (51) | 10 (42) | |
| Poorly
differentiated (n=26) | 15 (38) | 11 (50) | |
| Lymphovascular
space involvement |
| No (n=46) | 34 (76) | 12 (52) | 0.051 |
| Yes (n=22) | 11 (24) | 11 (48) | |
| Lymph node
involvement when sampled |
| Not involved,
N− (n=15) | 14 (40) | 1 (25) | 1.000 |
| Involved,
N+ (n=24) | 21 (60) | 3 (75) | |
| MMP-2 |
| Epithelial | 94 (52) | 100 (37) | 0.608 |
| Stromal | 25 (27) | 42 (55) | 0.082 |
| MMP-7 |
| Epithelial | 67 (50) | 65 (74) | 0.889 |
| Stromal | 13 (20) | 8 (16) | 0.268 |
| MMP-9 |
| Epithelial | 120 (43) | 156 (45) | 0.002 |
| Stromal | 22 (20) | 30 (17) | 0.120 |
| MT1-MMP |
| Epithelial | 115 (71) | 130 (58) | 0.398 |
| Stromal | 11 (14) | 10 (9) | 0.749 |
| TIMP-1 |
| Epithelial | 84 (49) | 84 (33) | 0.974 |
| Stromal | 6 (8) | 6 (8) | 0.932 |
| TIMP-2 |
| Epithelial | 142 (48) | 168 (38) | 0.026 |
| Stromal | 30 (25) | 32 (19) | 0.682 |
In patients treated by primary surgery, the
expression of epithelial MMP-9 was higher in patients with
suboptimal cytoreduction than in patients with optimal
cytoreduction: mean (SD) HSCORE values 160 (45) and 127 (41),
respectively, P=0.019. In patients treated by interval surgery, the
epithelial and stromal levels of MMPs and TIMPs were not different
in tumors from patients with optimal or suboptimal
cytoreduction.
CMDS showed that the tumors distributed
homogeneously, independently from the surgical outcome (Fig. 2) indicating that the outcome of
cytoreductive surgery was poorly influenced by MMP and TIMP profile
of the tumors.
Survival
Survival was assessed according to clinical,
histological and immunohistological data. The median follow-up was
24 months (range 7–78). As expected, the 2-year survival
probability differed significantly according to surgical outcome:
86% in patients with optimal cytoreduction and 63% in patients with
suboptimal cytoreduction (Table
III). Survival was also negatively influenced by tumors with
clear cell/other histological types or with lymph node involvement.
However, lymphovascular space involvement did not influence
survival.
| Table IIIPatient and tumor characteristics and
survival outcome. |
Table III
Patient and tumor characteristics and
survival outcome.
|
Characteristics | Disease-free 2-year
survival (%) | P-valuea log-rank |
|---|
| Histology | | 0.004 |
| Serous (n=41) | 80 | |
| Mucinous
(n=2) | NA | |
| Endometrioid
(n=15) | 87 | |
| Clear cells
(n=7) | 67 | |
| Other (n=3) | 33 | |
| Grade | | 0.874 |
| Well
differentiated (n=7) | 100 | |
| Moderately
differentiated (n=32) | 75 | |
| Poorly
differentiated (n=29) | 73 | |
| Lymphovascular
space involvement | | 0.963 |
| No (n=76) | 78 | |
| Yes (n=22) | 74 | |
| Lymph node | |
<0.001 |
| Not involved,
N− (n=15) | 100 | |
| Involved,
N+ (n=24) | 81 | |
| Not sampled, Nx
(n=30) | 61 | |
| FIGO stage | | 0.492 |
| III (n=63) | 76 | |
| IV (n=6) | 83 | |
| Cytoreduction | | 0.002 |
| Optimal
(n=45) | 86 | |
| Suboptimal
(n=24) | 63 | |
The performance of MMPs and TIMPs for survival
quantified with the C index was poor. The AUROC values ranged from
0.48 to 0.65 (Table IV). P-values
<0.05 were obtained for epithelial MT1-MMP and TIMP-2. However,
none of these differences remained significant after Bonferroni
correction. Survival was negatively influenced by positive
expressions of epithelial TIMP-2 and stromal TIMP-1. Again, none of
these differences remained significant after Bonferroni
correction.
| Table IVMMP and TIMP expressions in tumors
and survival outcome. |
Table IV
MMP and TIMP expressions in tumors
and survival outcome.
| Concordance
indexa | 2-year disease-free
survival (%) |
|---|
|
|
|
|---|
|
Characteristics | AUC | P-value | Negative
expressionb | Positive
expressionc | P-valued log-rank |
|---|
| MMP-2 |
| Epithelial | 0.51 | 0.351 | 53.8 | 57.8 | 0.331 |
| Stromal | 0.57 | 0.072 | 54.4 | 54.8 | 0.472 |
| MMP-7 |
| Epithelial | 0.51 | 0.473 | 54.8 | 46.2 | 0.864 |
| Stromal | 0.48 | 0.590 | 52.5 | 58.3 | 0.988 |
| MMP-9 |
| Epithelial | 0.51 | 0.394 | 53.7 | 54.9 | 0.902 |
| Stromal | 0.56 | 0.077 | 58.6 | 51.4 | 0.302 |
| MT1-MMP |
| Epithelial | 0.65 | 0.007 | 56.2 | 48 | 0.371 |
| Stromal | 0.51 | 0.390 | 52.0 | 56.1 | 0.402 |
| TIMP-1 |
| Epithelial | 0.51 | 0.491 | 51.0 | 74 | 0.093 |
| Stromal | 0.57 | 0.078 | 58.1 | 40.2 | 0.016 |
| TIMP-2 |
| Epithelial | 0.61 | 0.023 | 72.2 | 47.9 | 0.050 |
| Stromal | 0.57 | 0.077 | 54.4 | 59.0 | 0.456 |
Discussion
This study confirms the relevance of MMPs and TIMPs
as markers of tumor proliferation and invasiveness as their
epithelial expressions were relatively high in advanced ovarian
cancers. However, we failed to demonstrate that they were of any
prognostic value as the distribution of the tumors was scattered in
the CMDS model and not influenced by the quality of cytoreduction.
In addition, MMP and TIMP expressions were found not to influence
survival.
In the present study, MMP and TIMP expressions were
higher in the epithelium than in the stroma of ovarian cancers with
mean HSCORE values ranging from 66–151 and 6–31, respectively. It
has already been demonstrated that high levels of epithelial MMPs
and TIMPs are not actually specific for malignant tumors. For
example, MMP-2 signal was shown to be present in 76% of malignant
tumors and 54% of benign tumors on immunohistochemical analysis
(2). Another study found MMP-2 to
be more frequently expressed in benign tumors with morphological
altered lesions than in established carcinomas (23). Similar MMP-7 profiles have been
observed in mucinous tumors whatever their benign, borderline or
malignant nature (24). MT1-MMP
mRNA was shown to be strongly expressed both in borderline and
malignant tumors (25). High TIMP-2
expressions have been found in malignant tumors compared to
borderline and benign ovarian tumors while various expressions were
observed for TIMP-1 in the same figure (26,27).
MMP-9 is probably the least controversial. Stronger epithelial
MMP-9 expressions have been reported in malignant tumors than in
benign or borderline tumors (28,29).
These discrepancies between studies can be partly
explained by different methods of analysis and detection and also
because the MMP and TIMP values were evaluated separately rather
than by a translational approach. In a previous study using the
same scoring system, we found alterations in all MMP and TIMP
expressions in malignant serous tumors compared to benign and
borderline serous tumors in univariate analysis though the
alterations were less marked in malignant mucinous tumors (18). By cluster analysis, only MT1-MMP,
MMP-7 and MMP-9 could distinguish malignant serous tumors from
borderline and benign ovarian tumors. By CMDS analysis, the tumors
were distributed first according to the mucinous or serous
histological type, then according to the benign, borderline or
malignant nature of the tumor. The influence of histological type
has also been underlined in a study showing high level expressions
of MMP-2 and MT1-MMP in ovarian clear cell carcinoma relative to
other histotypes (30).
In the present study, tumors from patients with
optimal cytoreduction demonstrated low epithelial MMP-9 expression
by univariate analysis. The other expressions were not
discriminative. In addition, CMDS failed to demonstrate any
influence of MMPs and TIMPs on the quality of cytoreduction.
The prognostic impact of MMP-9 has been underlined
in two studies assessing the latent and the active forms of
gelatinases by zymography. In one study, it was found that only
MMP-9, but not MMP-2, had an impact on recurrence (31). Activities of proMMP-9 (the latent
form of MMP-9) and active MMP-9 in the tumor were higher in
patients with recurrence. However, no values were available on the
quality of cytoreduction in this study. In the other study, only
proMMP-9 had an impact on prognosis (32). ProMMP-9 was associated with short
survival only in the subgroup of patients with optimal
cytoreduction, while for patients with residual disease proMMP-9
did not predict survival. Therefore, proMMP-9 is of strong
prognostic power in patients with no postoperative residual
disease.
By immunohistochemistry, epithelial MMP-9 has been
associated with no or ≤2 cm residual disease only if there is a
strong signal in a high proportion of cancer cells (16). In addition, low stromal MMP-9
expression was significantly related to tumors with no residual
disease. These results contrast with ours and the literature.
However, we demonstrate in the present study that MMP-9 loses its
prognostic impact in terms of cytoreduction once a translation
approach is adopted.
MMP and TIMP expressions did not influence survival
in our study population. Their prognostic values were outweighed by
clinical and histological data such as tumor type, lymph node
involvement and cytoreduction. Our study is the first to assess the
concomitant expressions of 6 MMPs and TIMPs in the prognosis of
ovarian cancer. Most of the other trials evaluating prognosis not
only analyzed MMPs and TIMPs selectively but also only investigated
1 to 3 MMPs or TIMPs. Studies including more than 4 MMPs or TIMPs
have mainly dealt with physiopathology.
One study questioned the association between the
expression of 4 MMPs or TIMPs and disease outcome (8–10). By
univariate analysis, high levels of MMP-2, MMP-9, MT1-MMP and
TIMP-2, were detected by immunohistochemistry and/or mRNA in
situ hybridization in tumor cells from peritoneal or pleural
effusions, metastatic lesions and primary ovarian tumors. A
multivariate analysis was carried out in one of the reports on
primary tumors (8). Surprisingly,
epithelial MMP-9 and stromal TIMP-2 expressions correlated with
poor survival, while tumor type, grade and stage did not. In
another study assessing MMP-2, MMP-9 and MT1-MMP in 77 patients
with ovarian cancer, strong epithelial MT1-MMP and stromal MMP-9
and FIGO stage were independently associated with shorter survival
(33). On the other hand, as in our
study, clinical (FIGO stage, residual disease) and histological
(grade) characteristics were found to be independent prognostic
factors and outweighed MMP-9 epithelial and stromal expressions
which influenced clinical outcome in univariate analysis (16).
Discrepancies may be explained by the absence of a
given threshold for each MMP evaluated by immunohistochemistry as
this differs from study to study (16,33).
We used the concordance index to evaluate the discrimination of
quantitative values of MMPs and TIMPs for survival. With this
approach, the alternatives are compared directly, without having to
set a possibly arbitrary threshold. In addition, none of the
studies mentioned above referred to the Bonferroni correction of
P-values in case of multiple tests. Thus, the significance of
certain MMPs or TIMPs could be overestimated.
Technically, immunohistochemistry procedures require
multiple steps which may cause concern. In a recent study, the
HSCORE technique was used to assess the prognostic significance of
six biomarkers including gelatinases in a TMA of 185 specimens
(34). Unfortunately, MMP-2 and
MMP-9 staining was observed at very low levels in serous and
endometrioid carcinomas; thus, gelatinase expressions failed to
demonstrate any influence in contrast to the other biomarkers
studied. In our center, numerous tests were run before finding the
best method for antigen unmasking, to select the concentration of
primary antibody staining, and to test the advantage of using the
Ventana amplification kit.
To conclude, standard statistical analysis adjusted
after Bonferroni correction as well as classical multidimensional
scaling failed to demonstrate any influence of MMPs and TIMPs in
the prognosis of ovarian tumors. Despite the lack of standardized
methods for MMP and TIMP detection and the underuse of
translational approach in the literature, the impact of MMPs and
TIMPs on prognosis is probably less important than previously
thought. Further studies must address these concerns as
considerable hopes are pinned on the success of targeted therapy in
patients with advanced ovarian cancer.
Acknowledgements
The authors thank Anita Rodenas for advice in
setting up tissue microarray and for technical assistance in
testing MMP antibodies for immunohistochemistry, and Felicity
Neilson for reviewing this manuscript.
References
|
1
|
Schröpfer A, Kammerer U, Kapp M, Dietl J,
Feix S and Anacker J: Expression pattern of matrix
metalloproteinases in human gynecological cancer cell lines. BMC
Cancer. 13:5532010.PubMed/NCBI
|
|
2
|
Wu X, Li H, Kang L, Wang W and Shan B:
Activated matrix metalloproteinase-2: a potential marker of
prognosis for epithelial ovarian cancer. Gynecol Oncol. 84:126–134.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Planagumà J, Liljeström M, Alameda F, et
al: Matrix metalloproteinase-2 and matrix metalloproteinase-9
codistribute with transcription factors RUNX1/AML1 and ETV5/ERM at
the invasive front of endometrial and ovarian carcinoma. Hum
Pathol. 42:57–67. 2011.PubMed/NCBI
|
|
4
|
Wang FQ, So J, Reierstad S and Fishman DA:
Matrilysin (MMP-7) promotes invasion of ovarian cancer cells by
activation of progelatinase. Int J Cancer. 114:19–31. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Moss NM, Barbolina MV, Liu Y, Sun L,
Munshi HG and Stack MS: Ovarian cancer cell detachment and
multicellular aggregate formation are regulated by membrane type 1
matrix metalloproteinase: a potential role in I.p. metastatic
dissemination. Cancer Res. 69:7121–7129. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Huang LW, Garrett AP, Bell DA, Welch WR,
Berkowitz RS and Mok SC: Differential expression of matrix
metalloproteinase-9 and tissue inhibitor of metalloproteinase-1
protein and mRNA in epithelial ovarian tumors. Gynecol Oncol.
77:369–376. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kim TJ, Rho SB, Choi YL, et al: High
expression of tissue inhibitor of metalloproteinase-2 in serous
ovarian carcinomas and the role of this expression in ovarian
tumorigenesis. Hum Pathol. 37:906–913. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Davidson B, Goldberg I, Gotlieb WH, et al:
High levels of MMP-2, MMP-9, MT1-MMP and TIMP-2 mRNA correlate with
poor survival in ovarian carcinoma. Clin Exp Metastasis.
17:799–808. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Davidson B, Reich R, Berner A, et al:
Ovarian carcinoma cells in serous effusions show altered MMP-2 and
TIMP-2 mRNA levels. Eur J Cancer. 37:2040–2049. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Davidson B, Goldberg I, Gotlieb WH,
Kopolovic J, Ben-Baruch G, Nesland JM and Reich R: The prognostic
value of metalloproteinases and angiogenic factors in ovarian
carcinoma. Mol Cell Endocrinol. 187:39–45. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kamat AA, Fletcher M, Gruman LM, et al:
The clinical relevance of stromal matrix metalloproteinase
expression in ovarian cancer. Clin Cancer Res. 12:1707–1714. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Périgny M, Bairati I, Harvey I, et al:
Role of immunohistochemical overexpression of matrix
metalloproteinases MMP-2 and MMP-11 in the prognosis of death by
ovarian cancer. Am J Clin Pathol. 129:226–231. 2008.PubMed/NCBI
|
|
13
|
Rauvala M, Puistola U and
Turpeenniemi-Hujanen T: Gelatinases and their tissue inhibitors in
ovarian tumors; TIMP-1 is a predictive as well as a prognostic
factor. Gynecol Oncol. 99:656–663. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sillanpää SM, Anttila MA, Voutilainen KA,
et al: Prognostic significance of matrix metalloproteinase-7 in
epithelial ovarian cancer and its relation to β-catenin. Int J
Cancer. 119:1792–1799. 2006.PubMed/NCBI
|
|
15
|
Sillanpää S, Anttila M, Suhonen K, et al:
Prognostic significance of extracellular matrix metalloproteinase
inducer and matrix metalloproteinase 2 in epithelial ovarian
cancer. Tumour Biol. 28:280–289. 2007.PubMed/NCBI
|
|
16
|
Sillanpää S, Anttila M, Voutilainen K, et
al: Prognostic significance of matrix metalloproteinase-9 (MMP-9)
in epithelial ovarian cancer. Gynecol Oncol. 104:296–303.
2007.PubMed/NCBI
|
|
17
|
Benedet JL, Bender H, Jones H III, Ngan
HYS and Pecorelli S: FIGO staging classifications and clinical
practice guidelines in the management of gynecologic cancers. FIGO
Committee on Gynecologic Oncology. Int J Gynecol Obstet.
70:209–262. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brun JL, Cortez A, Commo F, Uzan S,
Rouzier R and Daraï E: Serous and mucinous ovarian tumors express
different profiles of MMP-2, -7, -9, MT1-MMP, and TIMP-1 and -2.
Int J Oncol. 33:1239–1246. 2008.PubMed/NCBI
|
|
19
|
Skacel M, Skilton B, Pettay JD and Tubbs
RR: Tissue microarrays: a powerful tool for high-throughput
analysis of clinical specimen: a review of the method with
validation data. Appl Immunohistochem Mol Morphol. 10:1–6. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Graesslin O, Cortez A, Fauvet R, Lorenzato
M, Birembaut P and Darai E: Metalloproteinase-2, -7 and -9 and
tissue inhibitor of metalloproteinase-1 and -2 expressions in
normal, hyperplastic and neoplastic endometrium: a
clinical-pathological correlation study. Ann Oncol. 17:637–645.
2006. View Article : Google Scholar
|
|
21
|
Budwit-Novotny DA, McCarty KS, Cox EB, et
al: Immunohistochemical analyses of estrogen receptor in
endometrial adenocarcinoma using a monoclonal antibody. Cancer Res.
46:5419–5425. 1986.PubMed/NCBI
|
|
22
|
Bland JM and Altman DG: Multiple
significance tests: the Bonferroni method. BMJ. 310:1701995.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cai KQ, Yang WL, Capo-Chichi CD, et al:
Prominent expression of metalloproteinases in early stages of
ovarian tumorigenesis. Mol Carcinogen. 46:130–143. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Shigemasa K, Tanimoto H, Sakata K, et al:
Induction of matrix metalloprotease-7 is common in mucinous ovarian
tumors including early stage disease. Med Oncol. 17:52–58. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Afzal S, Lalani EN, Poulsom R, et al:
MT1-MMP and MMP-2 mRNA expression in human ovarian tumors: possible
implications for the role of desmoplastic fibroblasts. Hum Pathol.
29:155–165. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sakata K, Shigemasa K, Nagai N and Ohama
K: Expression of matrix metalloproteinases (MMP-2, MMP-9, MT1-MMP)
and their inhibitors (TIMP-1, TIMP-2) in common epithelial tumors
of the ovary. Int J Oncol. 17:673–681. 2000.PubMed/NCBI
|
|
27
|
Määttä M, Santala M, Soini Y,
Talvensaari-Mattila A and Turpeenniemi-Hujanen T: Matrix
metalloproteinases 2 and 9 and their tissue inhibitors in low
malignant potential ovarian tumors. Tumor Biol. 25:188–192.
2004.PubMed/NCBI
|
|
28
|
Behrens P, Rothe M, Florin A, Wellman A
and Wernert N: Invasive properties of serous human epithelial
ovarian tumors are related to Ets-1, MMP-1 and MMP-9 expression.
Int J Mol Med. 8:149–154. 2001.PubMed/NCBI
|
|
29
|
Ozalp S, Tanir HM, Yalcin OT, Kabukcuoglu
S, Oner U and Uray M: Prognostic value of matrix
metalloproteinase-9 (gelatinase B) expression in epithelial ovarian
tumors. Eur J Gynaecol Oncol. 24:417–420. 2003.PubMed/NCBI
|
|
30
|
Adley BP, Gleason KJ, Yang XJ and Stack
MS: Expression of membrane type 1 matrix metalloproteinase (MMP-14)
in epithelial ovarian cancer: high level expression in clear cell
carcinoma. Gynecol Oncol. 112:319–324. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Demeter A, Sziller I, Csapo Z, et al:
Molecular prognostic markers in recurrent and in non-recurrent
epithelial ovarian cancer. Anticancer Res. 25:2885–2889.
2005.PubMed/NCBI
|
|
32
|
Lengyel E, Schmalfeldt B, Konik E, et al:
Expression of latent matrix metalloproteinase 9 (MMP-9) predicts
survival in advanced ovarian cancer. Gynecol Oncol. 82:291–298.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lin YG, Han LY, Kamat AA, et al: EphA2
overexpression is associated with angiogenesis in ovarian cancer.
Cancer. 109:332–334. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lin CK, Chao TK, Yu CP, Yu MH and Jin JS:
The expression of six biomarkers in the four most common ovarian
cancers: correlation with clinicopathological parameters. APMIS.
117:162–175. 2009. View Article : Google Scholar : PubMed/NCBI
|