Introduction
Gastric cancer is one of the leading causes of
cancer-related mortality worldwide. A total of 989,600 new stomach
cancer cases and 738,000 deaths are estimated to have occurred in
2008, accounting for 8% of the total cases and 10% of total deaths
(1). Depth of invasion and lymph
node status or optimization of pT (primary tumor) and pN (regional
lymph nodes) category are important prognostic factors for gastric
cancer (2–4). In 2002, the 6th edition of the
International Union Against Cancer (UICC)/American Joint Committee
on Cancer (AJCC) further divided pT2 gastric adenocarcinomas into
type pT2a [invasion of the muscularis propria (MP)] and type pT2b
[invasion of the subserosa (SS)] (5). Moreover, previous studies have clearly
demonstrated that multiple genetic alterations are responsible for
the development and progression of gastric cancer similar to other
human cancers (6,7).
Programmed cell death 4 (PDCD4) has been
demonstrated to inhibit tumor promoter-induced neoplastic
transformation in a murine JB6 cell model system (8). The human PDCD4 gene was found to be
localized on chromosome 10q24 (9).
Its encoding product is a 64-kDa protein involved in the apoptotic
machinery, which suppresses cell transformation, tumorigenesis and
invasion (10–12). PDCD4 is expressed in many normal
tissues, such as normal mammary gland and normal human lung tissue
(13,14). Its levels were found to be markedly
decreased in primary patient tumor samples from lung cancer
(14), breast carcinoma (10), colon cancer (15) and hepatocellular carcinoma (16).
Previous research has demonstrated the relationship
between gastric cancer and PDCD4 (17). However, to the best of our knowledge
no studies have shown whether PDCD4 is associated with pT2a and
pT2b stage gastric cancers. In the present study, gastric cancer
specimens were classified as stages pT2a and pT2b and the levels of
PDCD4 mRNA and protein were evaluated. Finally, we used
immunohistochemistry to determine the expression of PDCD4 protein
and analyzed the relationship between PDCD4 expression and the
clinicopathological features of the patients with pT2 stage gastric
cancer.
Patients and methods
Subjects
Specimens from 122 patients with pT2 stage gastric
cancer were obtained from the Department of Surgical Oncology,
First Affiliated Hospital, China Medical University (Shenyang,
China) from January 2001 to December 2010 and classified into pT2a
and pT2b stages according to the UICC/AJCC pT staging system. None
of the patients underwent radiotherapy or chemotherapy prior to
surgery. This study was in compliance with the Helsinki
Declaration. All patients provided written informed consent for
participation, and the procedure was approved by our university
ethics committee.
Semi-quantitative real-time PCR
Total tissue RNA was isolated using TRIzol reagent
(Invitrogen, Carlsbad, CA, USA) and was reverse transcribed using
SuperScript II reverse transcriptase (Invitrogen) according to the
manufacturer’s protocol. Real-time PCR was performed using primers
specific for PDCD4 and GAPDH. The following primer
sets were used: PDCD4 sense, 5′-GTATGATGTGGAGGAGGTGGAT-3′
and antisense, 5′-CCCTCCAATGCTAAGGATACTG-3′; GAPDH sense,
5′-GAAGGTGAAGGTCGGAGT-3′ and antisense,
5′-CATGGGTGGAATCATATTGGAA-3′. Real-time PCR analysis was performed
using the ABI PRISM 7500 sequence detection system (Applied
Biosystems, Foster City, CA, USA) using the SYBR-Green PCR Master
mixture (Takara, Dalian, China). The PCR conditions were as
follows: 1 cycle at 95°C for 10 min followed by 40 cycles at 95°C
for 15 sec and at 60°C for 1 min. Relative quantitation was
calculated by the ΔΔCt method. Each reaction was repeated
independently three times in triplicate.
Western blot analysis
Tissues were lysed in lysis buffer (20 mM Tris-HCl,
150 mM NaCl, 2 mM EDTA, 1% Triton X-100) containing a protease
inhibitor cocktail (Sigma-Aldrich, St. Louis, MO, USA). Protein
amounts from the cell extract were quantified using the BCA protein
assay kit. Equivalent amounts of protein (60 μg) were separated
using 12% SDS-PAGE and transferred to PVDF membranes (Millipore
Corp., Billerica, MA, USA). Western blot analysis was performed
using primary antibodies: PDCD4 (Cell Signaling Technology,
Beverly, MA, USA) and β-actin (Santa Cruz Biotechnology, Santa
Cruz, CA, USA). Binding of each specific antibody was detected with
horseradish peroxidase (HRP)-conjugated respective secondary
antibodies (Amersham Biosciences, Amersham, UK) and ECL solutions
(Amersham Biosciences).
Immunohistochemical staining
Immunohistochemistry was used to detect the
expression of PDCD4 protein in gastric cancer samples. The study
population included 122 patients as described above.
Immunohistochemical staining was performed on 4-μm sections
obtained from formalin-fixed, paraffin-embedded blocks. Endogenous
peroxidase activity was blocked with 3% hydrogen peroxide for 30
min. Antigen retrieval was carried out in citrate buffer (10 mM, pH
6.0) for 30 min at 95°C. PDCD4 antibody (Cell Signaling Technology)
at a dilution of 1:500 was applied and sections were incubated at
4°C overnight. Afterward, sections were incubated with a
biotinylated secondary antibody and then exposed to a streptavidin
complex (HRP). Positive reactions were visualized with
3,3′-diaminobenzidine tetrahydrochloride (DAB; Sigma-Aldrich),
followed by counterstaining with hematoxylin. Normal tissue was
used as a control. Sections treated without primary antibodies were
used as negative controls. The percentage of positive-stained cells
was graded semi-quantitatively according to a four-tier scoring
system: negative (−), 0–5%; weakly positive (+), 6–25%; moderately
positive (++), 26–50% and strongly positive (+++), 51–100%.
Cell cycle distribution and analysis of
apoptosis
pT2a and pT2b gastric cancer samples and paired
normal tissues were subjected to chemical digestion by incubation
with 0.5% pepsin (pH 1.5; Sigma-Aldrich) at 37°C in a water bath
for 30 min with intermittent stirring. Disaggregated tissues were
filtered through a 50-μm nylon mesh, washed twice with PBS and
re-suspended in PBS. Cells were collected in PBS and fixed on ice
with 1% paraformaldehyde, followed by 70% cold ethanol. After
treatment with 10 μg/ml RNase, the cells were stained with 50 μg/ml
propidium iodide (PI; KeyGen, Nanjing, China) for 15 min at room
temperature for cell cycle analysis. The apoptotic cells were
detected with Annexin V-FITC/PI double staining. The cells were
trypsinized and stained with Annexin V-FITC and PI following the
manufacturer’s instructions for the Apoptosis Assay kit (KeyGen).
The stained cells were analyzed by flow cytometry. Data analysis
was performed with CellQuest software (BD Biosciences, Rockville,
MD, USA).
Statistical analysis
All statistical analyses and graphics were performed
using GraphPad Prism 5. Overall survival rates were determined
using the Kaplan-Meier estimator. Kaplan-Meier survival plots were
generated and comparisons were made with log-rank statistics. Cox’s
proportional hazard model was used to identify significant factors
correlated with prognosis in multivariate analysis. For all
analyses, P<0.05 was considered to indicate a statistically
significant result.
Results
Evaluation of the levels of PDCD4 mRNA
and protein in pT2a and pT2b stage gastric cancer specimens
Real-time PCR was carried out to investigate the
level of PDCD4 mRNA in gastric cancer specimens. The results
indicated that the level of PDCD4 mRNA was lower in the gastric
cancer specimens compared to that in the normal tissues (P<0.05;
Fig. 1A). To examine the
relationship between the level of PDCD4 protein and the level of
PDCD4 transcription, western blot analysis of the PDCD4 protein was
carried out in gastric cancer specimens and the results showed that
the level of PDCD4 protein was lower compared to that in the normal
tissues and coincident with the level of mRNA (P<0.05; Fig. 1B). Notably, the levels of PDCD4 mRNA
and protein were higher in pT2a stage cancer tissues compared with
that in pT2b stage cancer tissues (Figs. 1 and 2).
PDCD4 expression is correlated with
clinicopathological parameters of the patients with pT2 stage
gastric cancer
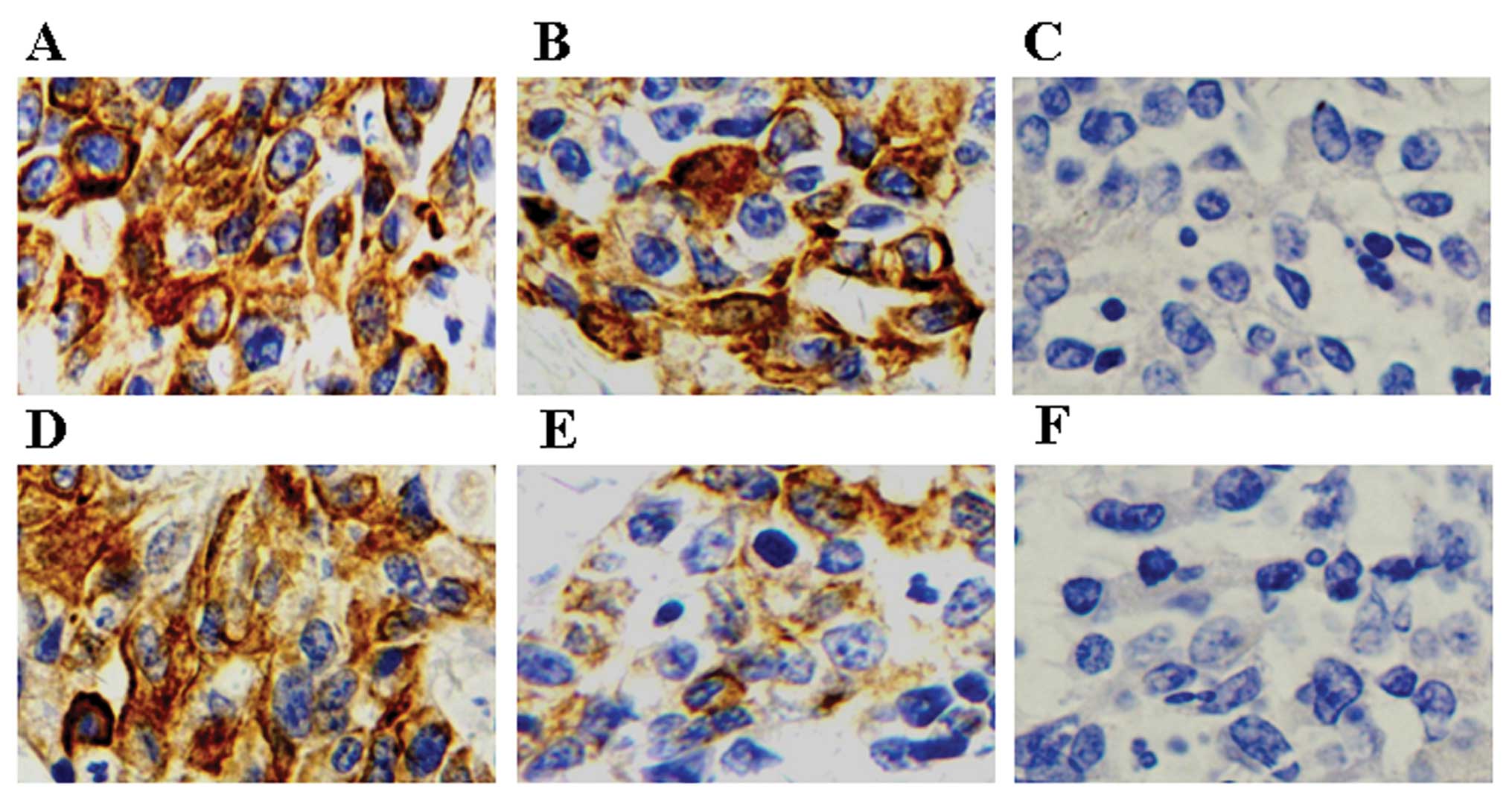
The immunostaining results showed that PDCD4
expression was distributed in the cytoplasm of normal gastric and
gastric cancer cells (Fig. 2).
However, PDCD4 protein was weakly expressed in the gastric cancer
tissues, while highly in the corresponding normal tissues. There
was a significant difference in PDCD4 expression between the normal
gastric tissues, when compared with that in the pT2a and pT2b stage
gastric cancer tissues (P<0.05; Table I). We then analyzed the potential
relationship between the expression of PDCD4 and the
clinicopathological characteristics of these patients. The results
are summarized in Table II. No
correlation was found with patient gender, age, lymphatic invasion,
venous invasion, lymph node metastasis and pN category (P>0.05).
However, PDCD4 expression was significantly associated with the
level of tumor differentiation and tumor size (P<0.05).
 | Table IPDCD4 expression in the normal gastric
tissues and pT2a and pT2b stage gastric cancer tissue. |
Table I
PDCD4 expression in the normal gastric
tissues and pT2a and pT2b stage gastric cancer tissue.
| | PDCD4 expression | | | |
|---|
| |
| | | |
|---|
| Groups | n | − | + | ++ | +++ | PR (%) | χ2
value | P-value |
|---|
| Normal gastric
tissue | 122 | 0 | 31 | 35 | 56 | 100.0 | 139.1 | 0.027 |
| pT2a gastric cancer
tissue | 60 | 39 | 10 | 6 | 5 | 35.0 | | |
| pT2b gastric cancer
tissue | 62 | 47 | 5 | 6 | 4 | 24.2 | | |
| Table IIRelationship between PDCD4 expression
and clinicopathological parameters of the patients with pT2 stage
gastric cancer. |
Table II
Relationship between PDCD4 expression
and clinicopathological parameters of the patients with pT2 stage
gastric cancer.
| | PDCD4 expression | | | |
|---|
| |
| | | |
|---|
| Clinicopathological
parameters | n | − | + | ++ | +++ | PR (%) | χ2
value | P-value |
|---|
| Gender | | | | | | | 2.68 | 0.125 |
| Female | 48 | 31 | 7 | 7 | 3 | 31.3 | | |
| Male | 74 | 55 | 8 | 5 | 6 | 25.7 | | |
| Age (years) | | | | | | | 4.78 | 0.227 |
| <65 | 55 | 35 | 6 | 8 | 6 | 36.4 | | |
| ≥65 | 67 | 51 | 9 | 4 | 3 | 23.9 | | |
| Tumor
differentiation | | | | | | | 9.03 | 0.032 |
| Differentiated | 53 | 30 | 10 | 8 | 5 | 43.4 | | |
|
Undifferentiated | 69 | 56 | 5 | 4 | 4 | 18.8 | | |
| Lymphatic
invasion | | | | | | | 0.53 | 0.148 |
| − | 50 | 34 | 6 | 6 | 4 | 32.0 | | |
| + | 72 | 52 | 9 | 6 | 5 | 27.8 | | |
| Venous
invasion | | | | | | | 6.01 | 0.275 |
| − | 68 | 48 | 9 | 9 | 2 | 29.4 | | |
| + | 54 | 38 | 6 | 3 | 7 | 29.6 | | |
| Lymph node
metastasis | | | | | | | 6.18 | 0.353 |
| − | 42 | 27 | 8 | 2 | 5 | 35.7 | | |
| + | 80 | 59 | 7 | 10 | 4 | 26.3 | | |
| Tumor size
(cm) | | | | | | | 10.57 | 0.041 |
| <4 | 57 | 33 | 12 | 6 | 6 | 42.1 | | |
| ≥4 | 65 | 53 | 3 | 6 | 3 | 18.5 | | |
| pN category | | | | | | | 4.47 | 0.079 |
| pN0 | 32 | 22 | 3 | 4 | 3 | 31.2 | | |
| pN1 | 34 | 22 | 5 | 5 | 2 | 35.3 | | |
| pN2 | 30 | 21 | 5 | 2 | 2 | 30.0 | | |
| pN3 | 26 | 21 | 2 | 1 | 2 | 19.2 | | |
Kaplan-Meier survival analysis and Cox’s
proportional hazard analysis
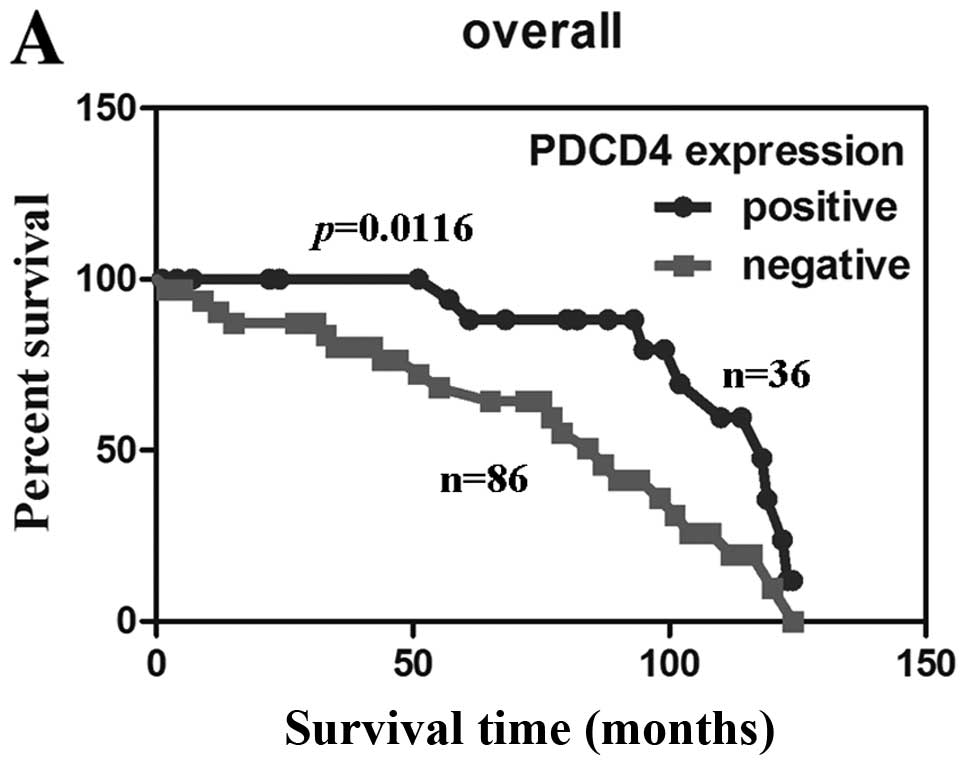
Follow-up information was available for 122 patients
with gastric cancer for periods ranging from 3 months to 7 years
(median, 42 months). Kaplan-Meier analysis showed that PDCD4
expression was closely correlated with a favorable prognosis of
patients with pT2 stage gastric cancer (P<0.05; Fig. 3A). Notably, the major clinical
distinction between pT2a stage gastric cancer patients and pT2b
stage gastric cancer patients was that PDCD4 expression showed no
statistically significant effects on pT2b patient survival
(P>0.05; Fig. 3C) when compared
with the pT2a patients (P<0.05; Fig.
3B). Cox’s proportional hazard analysis indicated that PDCD4
was an independent prognostic factor for pT2a and pT2b stage
gastric cancer (P<0.05; Tables
III and IV).
| Table IIIMultivariate analysis of clinical
variables for pT2a gastric cancer. |
Table III
Multivariate analysis of clinical
variables for pT2a gastric cancer.
| Clinicopathological
parameters | Relative risk (95%
CI) | P-value |
|---|
| Gender (male) | 1.98
(1.27–3.24) | 0.305 |
| Age (>65
years) | 1.12
(0.61–1.72) | 0.428 |
|
Differentiation | 1.22
(0.67–1.34) | 0.291 |
| Lymphatic
invasion | 1.43
(0.85–2.42) | 0.278 |
| Venous
invasion | 0.51
(0.21–1.52) | 0.456 |
| Lymph node
metastasis | 0.78
(0.34–1.75) | 0.334 |
| Tumor size (≥4
cm) | 0.62
(0.27–1.61) | 0.347 |
| PDCD4 expression (+
to +++) | 5.94
(1.53–12.34) | 0.015 |
| Table IVMultivariate analysis of clinical
variables for pT2b stage gastric cancer. |
Table IV
Multivariate analysis of clinical
variables for pT2b stage gastric cancer.
| Clinicopathological
parameters | Relative risk (95%
CI) | P-value |
|---|
| Gender (male) | 1.24
(0.71–1.35) | 0.247 |
| Age (>65
years) | 1.17
(0.56–1.22) | 0.291 |
|
Differentiation | 1.09
(0.43–1.12) | 0.357 |
| Lymphatic
invasion | 1.56
(0.93–2.58) | 0.294 |
| Venous
invasion | 0.64
(0.28–1.65) | 0.321 |
| Lymph node
metastasis | 0.71
(0.31–1.69) | 0.227 |
| Tumor size (≥4
cm) | 0.61
(0.23–1.58) | 0.289 |
| PDCD4 expression (+
to +++) | 4.86
(1.33–9.34) | 0.028 |
Assessment of cell cycle distribution and
apoptosis by flow cytometry
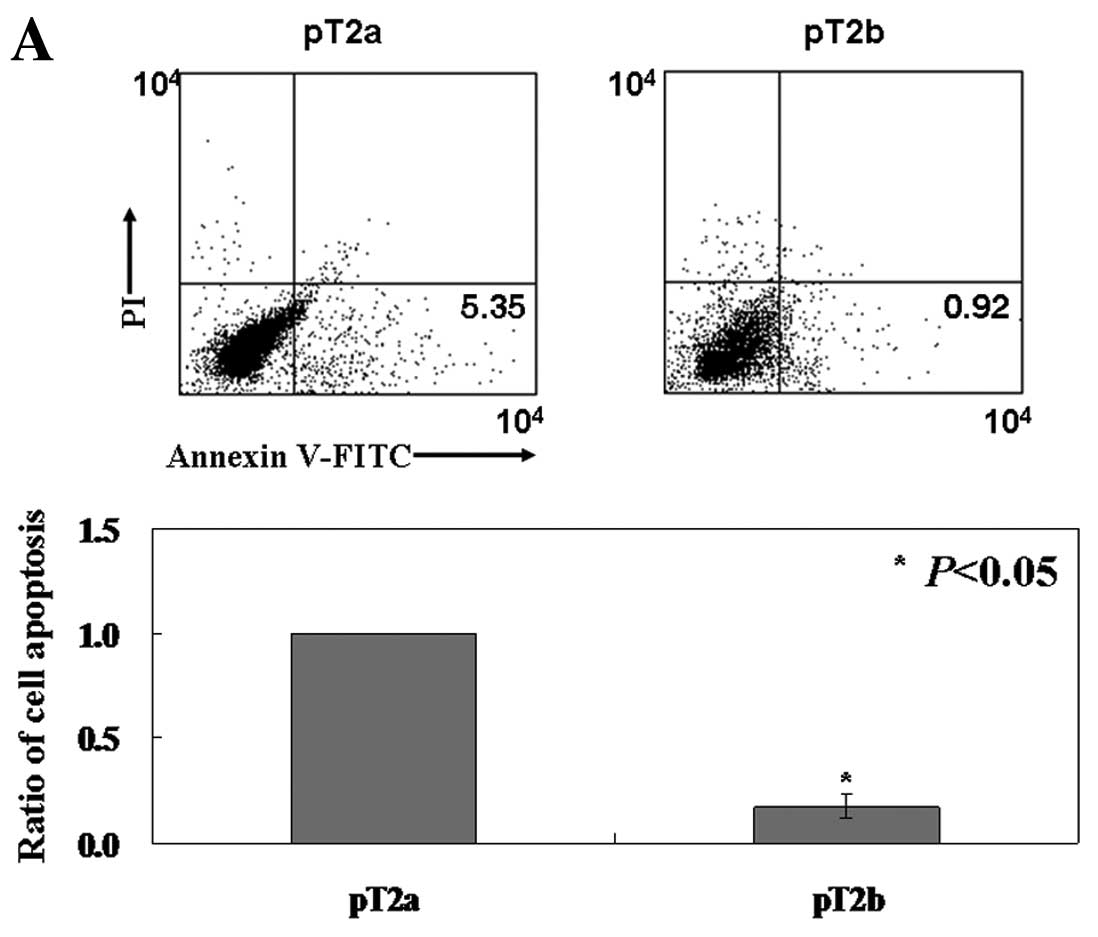
We compared the cell cycle distribution and
percentage of apoptotic cells obtained from pT2a and pT2b gastric
cancer tissue by flow cytometry. The percentage of apoptotic cells
present was determined using flow cytometry to detect cells
positively stained with Annexin V-FITC and propidium iodide (PI).
As shown in Fig. 4A, the percentage
of apoptotic pT2a cells was 5.35±0.34%, whereas 0.92±0.12% of pT2b
cells were undergoing apoptosis (P<0.05). A higher percentage of
cells from pT2b stage gastric cancer tissue was noted in the
G2 phase of the cell cycle when compared with the
percentage of cells from the pT2a gastric cancer tissue. The mean
percentage of the G2 phase fraction of pT2a and pT2b
stage gastric cancer cells was 24.9±3.4 and 42.3±4.8%, respectively
(P<0.05; Fig. 4B).
Discussion
In the present study, levels of PDCD4 mRNA and
protein expression were assessed in a total of 122 gastric cancer
tissue specimens. We demonstrated a decreasing trend for both mRNA
and protein expression of PDCD4 in pT2a and pT2b stage gastric
cancer tissues. Motoyama et al(17) demonstrated through a panel of
primary specimens and cell culture models that PDCD4 mRNA/protein
expression is lower in gastric cancer tissues compared to
corresponding normal tissues. This indicates that PDCD4 may play a
role in human gastric carcinogenesis. Notably, we also found that
the levels of mRNA and protein expression of PDCD4 were higher in
pT2a gastric cancer tissues than that in pT2b gastric cancer
tissues. Consistent with a previous study, reduced expression of
PDCD4 is related to advanced tumor stage in gastric cancer
(17). Loss of PDCD4 in lung cancer
was correlated with higher histological grade, disease stage and
poor prognosis (14). In our study,
loss of PDCD4 expression was significantly associated with
differentiation and tumor size of both pT2a and pT2b stage gastric
cancer tissues. Previous studies have demonstrated that PDCD4 is an
independent risk factor in lung (14) and colon cancer (15,18).
However, to the best of our knowledge, no similar studies have been
carried out in gastric cancer. We initially found that PDCD4 was an
independent risk factor in pT2 stage gastric cancer. Furthermore,
we confirmed that reduced PDCD4 expression was significantly
associated with low overall survival rate. There is no doubt that
reduced PDCD4 is a negative prognostic factor in primary lung
cancer (14), colon cancer
(15), ovarian cancer (19) and glioma (20). However, we found that reduced PDCD4
did not affect the survival of pT2b stage gastric cancer patients.
The reason may be that the level of PDCD4 protein in pT2b stage
gastric cancer patients is too low to exert a function.
PDCD4 has been reported as an inducer of apoptosis
(21,22). In our study, we confirmed that cells
obtained from pT2a tumor specimens had a higher apoptotic ratio
than cells from pT2b tumor tissue specimens. This indicates that
PDCD4 induces apoptosis in gastric cancer cells. In addition, we
also found that PDCD4 inhibits the cell cycle. Cells obtained from
pT2a tumor tissue specimens consisted of a small percentage of
cells in the G2 phase when compared to cells from pT2b
tumor tissue specimens. To our knowledge, this is the first report
concerning the relationship between PDCD4 and the cell cycle in
gastric cancer.
Taken together, we demonstrated that PDCD4 is
associated with pT2 stage gastric cancer. The results are not only
of relevance for diagnosis and prognosis, but may also provide a
novel target for pT2a and pT2b stage gastric cancer therapies.
Acknowledgements
We are indebted to Wang Ning and Li Sun for their
help with the statistical analysis.
References
|
1
|
Jemal A, Bray F, Center MM, et al: Global
cancer statistics. CA Cancer J Clin. 61:9–90. 2011. View Article : Google Scholar
|
|
2
|
Sarela AI, Turnbull AD, Coit DG, et al:
Accurate lymph node staging is of greater prognostic importance
than subclassification of the T2 category for gastric
adenocarcinoma. Ann Surg Oncol. 10:783–791. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kunisaki C, Shimada H, Nomura M, et al:
Distribution of lymph node metastasis in gastric carcinoma.
Hepatogastroenterology. 53:468–472. 2006.PubMed/NCBI
|
|
4
|
Potrc S, Gadiijev E, Hajdinjak T, et al:
Clinicopathological and immunohistochemical markers after radical
gastrectomy for gastric cancer. Hepatogastroenterology. 54:308–314.
2007.PubMed/NCBI
|
|
5
|
Greene FL, Page DL, Fleming ID, et al:
AJCC Cancer Staging Manual. 6th edition. Springer-Verlag; New York:
2002, View Article : Google Scholar
|
|
6
|
Ebert MP, Fei G, Kahmann S, et al:
Increased beta-catenin mRNA levels and mutational alterations of
the APC and beta-catenin gene are present in intestinal-type
gastric cancer. Carcinogenesis. 23:87–91. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
El-Rifai W and Powell SM: Molecular
biology of gastric cancer. Semin Radiat Oncol. 12:128–140. 2002.
View Article : Google Scholar
|
|
8
|
Cmarik JL, Min H, Hegamyer G, et al:
Differentially expressed protein Pdcd4 inhibits tumor
promoter-induced neoplastic transformation. Proc Natl Acad Sci USA.
96:14037–14042. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Soejima H, Miyoshi O, Yoshinaga H, et al:
Assignment of the programmed cell death 4 gene (PDCD4) to human
chromosome band 10q24 by in situ hybridization. Cytogenet Cell
Genet. 87:113–114. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Afonja O, Juste D, Das S, et al: Induction
of PDCD4 tumour suppressor gene expression by RAR agonists,
antiestrogen and HER-2/neu antagonist in breast cancer cells.
Evidence for a role in apoptosis. Oncogene. 23:8135–8145. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bitomsky N, Wethkamp N, Marikkannu R, et
al: siRNA-mediated knockdown of PDCD4 expression causes
upregulation of p21 (Waf1/Cip1) expression. Oncogene. 27:4820–4829.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Carayol N, Katsoulidis E, Sassano A, et
al: Suppression of programmed cell death 4 (PDCD4) protein
expression by BCR-ABL-regulated engagement of the mTOR/p70 S6
kinase pathway. J Biol Chem. 283:8601–8610. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yoshinaga H, Matsuhashi S, Fujiyama C, et
al: Novel human PDCD4 (H731) gene expressed in proliferative cells
is expressed in the small duct epithelial cells of the breast as
revealed by an anti-H731 antibody. Pathol Int. 49:1067–1077. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chen Y, Knosel T, Kristiansen G, et al:
Loss of PDCD4 expression in human lung cancer correlates with
tumour progression and prognosis. J Pathol. 200:640–646. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mudduluru G, Medved F, Grobholz R, et al:
Loss of programmed cell death 4 expression marks adenoma-carcinoma
transition, correlates inversely with phosphorylated protein kinase
B, and is an independent prognostic factor in resected colorectal
cancer. Cancer. 110:1697–1707. 2007. View Article : Google Scholar
|
|
16
|
Zhang H, Ozaki I, Mizuta T, et al:
Involvement of programmed cell death 4 in transforming growth
factor-beta1-induced apoptosis in human hepatocellular carcinoma.
Oncogene. 25:6101–6112. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Motoyama K, Inoue H, Mimori K, et al:
Clinicopathological and prognostic significance of PDCD4 and
microRNA-21 in human gastric cancer. Int J Oncol. 36:1089–1095.
2010.PubMed/NCBI
|
|
18
|
Asangani IA, Rasheed SA, Nikolova DA, et
al: MicroRNA-21 (miR-21) post-transcriptionally downregulates tumor
suppressor Pdcd4 and stimulates invasion, intravasation and
metastasis in colorectal cancer. Oncogene. 27:2128–2136. 2008.
View Article : Google Scholar
|
|
19
|
Wang X, Wei Z, Gao F, et al: Expression
and prognostic significance of PDCD4 in human epithelial ovarian
carcinoma. Anticancer Res. 28:2991–2996. 2008.PubMed/NCBI
|
|
20
|
Gao F, Wang X, Zhu F, et al: PDCD4 gene
silencing in gliomas is associated with 5′CpG island methylation
and unfavourable prognosis. J Cell Mol Med. 13:4257–4267. 2009.
|
|
21
|
Shibahara K, Asano M, Ishida Y, et al:
Isolation of a novel mouse gene MA-3 that is induced upon
programmed cell death. Gene. 166:297–301. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang Z and DuBois RN: Detection of
differentially expressed genes in human colon carcinoma cells
treated with a selective COX-2 inhibitor. Oncogene. 20:4450–4456.
2001. View Article : Google Scholar : PubMed/NCBI
|