Introduction
Nasopharyngeal carcinoma (NPC), an Epstein-Barr
virus (EBV)-associated cancer, is a major public health concern in
Southeast Asia and Southern China, especially in the Guangdong
province (1). Primary NPC (pNPC)
has unique pathological and clinical characteristics, and
radiotherapy with or without chemotherapy is the mainstream
treatment. Although the 5-year survival of patients with NPC has
steadily improved over the past three decades (2,3),
overall 15–58% of patients experienced recurrence after radical
radiotherapy in the era of conventional radiotherapy (4,5), and
13–22% have experienced recurrence in the era of
intensity-modulated radiation therapy (6,7). In
most patients with recurrence after complete remission following
radical radiotherapy, the cancer returns within an average of 1.5
years, with local recurrences accounting for 70% of such cases
(8,9). Recurrent NPC (rNPC) may be local,
regional, or distant and is usually treated with radiation therapy
and/or chemotherapy and occasionally with surgery. Retreatment for
rNPC poses a critical challenge given its poor efficacy and serious
toxicities (10).
Improved identification of prognostic factors by
means of molecular testing may be useful in the diagnosis of
diseases and their exact subtypes and may aid physicians in
selecting individualized treatment, increasing the likelihood of
local salvage. Several prognostic factors have been identified in
recent years including recurrent tumor T stage, histologic type,
patient age and disease-free interval to recurrence (ITR) (11–16).
Of these factors, short-term ITR has been shown to correlate with
poor outcome (14,15). Therefore, identification of
molecular markers that may lead to an improved understanding of
rNPC and to individualized treatment is imperative.
NPC arises from the mucosal epithelium of the
nasopharynx, and recurrence is a complex multistep process
involving several factors, such as maintenance of stem cells and
epithelial-mesenchymal transition (17,18).
Over 30 molecular markers have been studied as potential prognostic
and/or predictive biomarkers for NPC, including markers associated
with key cell functions such as cell proliferation, apoptosis,
autophagy, and necrosis (19–22).
However, the framework of rNPC has yet to be well established. The
c-Jun activation domain-binding protein-1/constitutive
photomorphogenic-9 (COP9) signalosome complex subunit 5 (Jab1/Csn5)
has been shown to be involved in the pathogenesis of NPC and has
been previously established as a tumor target by our group
(23–25). Two additional critical signaling
pathways, the phosphorylation of the signal transducer and
activator of transcription 3 (Stat3) pathway and the
phosphatidylinositol-3-kinase (PI3K)/Akt pathway, have also been
identified in head and neck squamous cell carcinoma (HNSCC) and NPC
(26–28). In addition, emerging evidence has
shown that endoplasmic reticulum (ER) stress-activated unfolded
protein response (UPR) has multiple roles in tumor development.
C/EBP homologous protein (CHOP), also known as GADD153, is a
critical protein that mediates ER stress-induced apoptosis
(29,30). Therefore, we hypothesized that these
factors contribute to the progression of rNPC.
However, the mechanistic link between ITR and
outcome for rNPC has yet to be fully understood. In the present
study, we collected paired pNPC and rNPC samples from 45
individuals from two institutions and compared the expression of
Jab1/Csn5 (nuclear and cytoplasmic), phosphor-Stat3 (p-Stat3)
(Tyr705), Akt (nuclear and cytoplasmic), CHOP, Ki-67, and terminal
deoxynucleotidyl transferase (TdT)-mediated dUTP nick end-labeling
(TUNEL) in the paired tumor tissues. Subsequently, we evaluated the
differences between short- and long-term ITR.
Materials and methods
Ethics statement
All human tissues were collected using protocols
approved by the Ethics Committee of the First People’s Hospital of
Foshan and Shantou Central Hospital affiliated with Sun Yat-Sen
University. Clinical and pathological data of patients were
analyzed anonymously.
Data collection and eligibility
criteria
The cancer center databases at two institutions
affiliated with Sun Yat-Sen University, the First People’s Hospital
of Foshan and Shantou Central Hospital, were retrospectively
reviewed for the period 2001–2012. The inclusion criteria for
paired specimens of pNPC and rNPC were: i) the patient achieved
complete remission of the primary tumor after radical radiotherapy
(total dose of radiotherapy ≥70 Gy for the nasopharyngeal site);
ii) rNPC was pathologically diagnosed in non-keratinizing cancer
and was the same pathological type as pNPC; and iii) paired tissues
were available from the primary tumor and the asynchronous local
recurrence in the same patient. Two pathologists histologically
confirmed all the biopsies. Clinical information including age,
gender, and dates of diagnosis for pNPC and rNPC were obtained from
the medical records. The clinical stage was designated according to
the tumor, node, and metastasis (TNM) classification system of the
American Joint Committee on Cancer/International Union Against
Cancer (6th edition, 2002).
Definitions of short- and long-term
ITR
ITR was defined as the time between diagnosis of
pNPC and rNPC. Although various time cutoffs for ITR have been
evaluated previously, (including 12, 18, and 24 months), we defined
short-term ITR as ITR <18 months and long-term ITR as ITR ≥18
months, following the studies of Teo et al and Oksüz et
al (14,15).
Human tissues and immunohistochemical
analysis
Expression of Jab1/Csn5 (nuclear and cytoplasmic),
p-Stat3, Akt (nuclear and cytoplasmic), CHOP, and Ki-67 was
analyzed by immunohistochemical (IHC) techniques. An analysis was
conducted of the paired tumor tissues used as well as the 4-μm
continuous sections cut from the formalin-fixed, paraffin-embedded
paired pNPC and rNPC specimens. IHC analyses of p-Stat3 (Tyr705)
(M9C6, dilution 1:100; Cell Signaling Technology, Danvers, MA,
USA), Jab1/Csn5 (Ab495, dilution 1:150; Abcam, Cambridge, UK), Akt1
(C73H10, dilution 1:200; Cell Signaling Technology), Ki-67 (M7240,
dilution 1:80; Dako Cytoformation, Glostrup, Denmark), and CHOP
(Ab27539, dilution 1:50; Abcam) were performed using the
streptavidin-biotin-peroxidase complex technique. The procedure was
as follows: conventional dewaxing hydration, 3% hydrogen peroxide
treatment, then blocking by dropper solution for 20 min, antibody
incubation at 4°C overnight, then goat anti-rabbit/goat anti-mouse
IgG by dropper, incubation for 30 min at 37°C, followed by baths of
diaminobenzidine and hematoxylin. Negative controls were analyzed
along with each assay by replacing the primary antibody with
phosphate-buffered saline.
TUNEL
The TUNEL assay was used to determine cell
apoptosis. Paraffin-embedded tissue sections (4-μm) were mounted on
xylene-coated slides and dried at 37°C overnight. The sections were
deparaffinized in xylene followed by sequential washes in graded
ethanol and in phosphate-buffered saline. The samples were
denatured by 15-min exposure to 20 μg/ml proteinase K at room
temperature, and endogenous peroxidase activity was blocked with 3%
hydrogen peroxide for 10 min. Apoptotically-fragmented cell DNA was
identified by the TUNEL assay using the ApoTag kit (KeyGen,
Nanjing, China). The samples were incubated with bovine TdT at 30
U/ml in a humid atmosphere at 37°C for 60 min, followed by exposure
to anti-digoxigenin-labeled secondary antibody for 30 min at room
temperature. After 2–10 min exposure to 0.05% diaminobenzidine in
0.02% hydrogen peroxide solution, the samples were counterstained
with methyl green (0.5% in 0.1 M sodium citrate, pH 4.0), mounted,
and dried.
Scoring
The paired samples were independently evaluated by
two investigators (W.C.H. and S.B.J.) without knowledge of the
clinical information. The IHC results for the expression of
Jab1/Csn5 (nuclear and cytoplasmic), p-Stat3, Akt (nuclear and
cytoplasmic), CHOP, and Ki-67 were evaluated using a five-tiered
semi-quantitative method. Five ×400 magnification fields for each
section were scored as 0 for no membrane staining, 1 for weak
staining, 2 for moderate, or 3 for strong staining. The extent of
tumor cell membrane staining was scored from 0 to 5 (0%, <1%,
1–10%, 11–33%, 34–67% and >67%), and the staining intensity was
scored from 0 to 3 (absent, weak, moderate and strong). Tumor
proliferation and apoptosis were evaluated by semi-quantitative
analysis using Ki-67 and TUNEL, respectively. The cells were
counted under ×400 magnification fields, with positive cells
defined as nuclei staining for Ki-67 (for the proliferation index)
or cell staining for TUNEL (apoptotic index). Scores for each tumor
were reported as the means of the percentage of positive cells per
high-power field.
Statistical analysis
SPSS 16.0 for Windows (SPSS, Inc., Chicago, IL, USA)
was used for the statistical analysis. Stata 12.0 (StataCorp,
College Station, TX, USA) was used to generate the forest plots.
Expression of Jab1/Csn5 (nuclear and cytoplasmic), p-Stat3, Akt
(nuclear and cytoplasmic), CHOP, Ki-67, and TUNEL was compared
using the Wilcoxon signed-rank test in the paired pNPC and rNPC
samples. Baseline values of these biomarkers were compared using
the Mann-Whitney test. The Kaplan-Meier method was used to
calculate cumulative survival. The log-rank test was used to
compare the survival curves. The Cox proportional hazards model was
used to analyze multiple prognostic factors for survival, including
gender, age (<46 or ≥46 years), pT and pN category, pTNM
staging, rT and rN category, rTNM staging, and ITR (<18 or ≥18
months). Two-tailed P-values <0.05 were considered statistically
significant.
Results
Patient characteristics and survival
Formalin-fixed, paraffin-embedded archive specimens
were retrospectively available from 45 patients with paired
biopsy-confirmed rNPC and pNPC samples. The baseline
characteristics of these 45 rNPC patients are shown in Table I. All the patients were treated with
radical radiotherapy at a median dose of 74 Gy (range, 70–76 Gy)
for the nasopharyngeal tumor, and 80% of patients received combined
chemotherapy. The 40 patients were treated again with radiotherapy
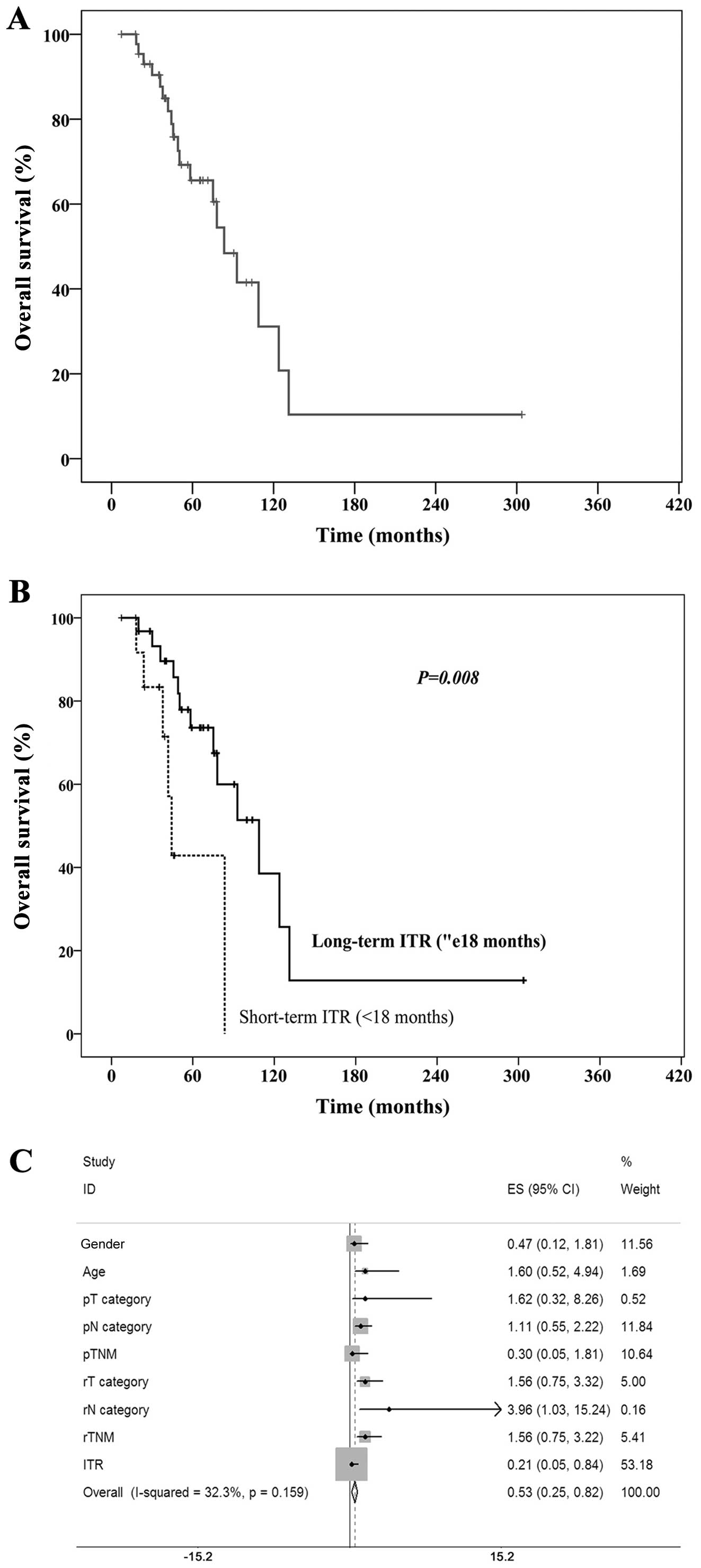
and 5 patients underwent surgery. The median follow-up was 49
months (range, 7–147 months), and the median survival of the 45
patients with paired samples was 83.4 months (Fig. 1A).
 | Table IBaseline characteristics of the
patients with paired specimens of primary and recurrent
nasopharyngeal carcinoma. |
Table I
Baseline characteristics of the
patients with paired specimens of primary and recurrent
nasopharyngeal carcinoma.
|
Characteristics | No. of cases
(%) |
|---|
| Total patients | 45 (100) |
| Age (years) |
| <46 | 19 (42.2) |
| ≥46 | 26 (57.8) |
| Gender |
| Male | 37 (82.2) |
| Female | 8 (17.8) |
| pT category |
| T1–2 | 13 (28.9) |
| T3–4 | 32 (71.1) |
| pN category |
| N0–1 | 20 (44.4) |
| N2–3 | 25 (55.6) |
| pTNM |
| II | 5 (11.1) |
| III | 30 (66.7) |
| IV | 10 (22.2) |
| rT category |
| T1–2 | 12 (26.7) |
| T3–4 | 33 (73.3) |
| rN category |
| N− | 39 (86.7) |
| N+ | 6 (13.3) |
| rTNM |
| I | 4 (8.9) |
| II | 9 (20.0) |
| III | 20 (44.4) |
| IV | 12 (26.7) |
| Interval to
recurrence (months) |
| <18 | 14 (31.1) |
| ≥18 | 31 (68.9) |
Confirmation of ITR as an independent
prognostic factor
In the present study, the median ITR was 26 months
(range, 5.0–281.5 months). There were 14 patients with ITR <18
months and 31 patients with ITR ≥18 months. For the 45 patients
with paired tumor specimens, the median survivals of patients with
short- and long-term ITR were 44.3 and 108.7 months (P=0.008),
respectively (Fig. 1B). The
multivariate analysis using Cox’s regression model revealed that
ITR (<18 or ≥18 months) was the most important prognostic factor
for overall survival (hazard ratio, 0.211; 95% confidence interval,
0.053–0.841; P=0.027) (Fig.
1C).
Analysis of Jab1/Csn5, p-Stat3, Akt, and
CHOP in paired pNPC and rNPC
Successful IHC evaluations of Jab1/Csn5, p-Stat3,
Akt, and CHOP were performed in 44, 42, 41, and 29 specimens,
respectively. The increased expression of nuclear Jab1/Csn5
(P<0.001) and nuclear Akt (P=0.008) was observed in rNPC
compared with the paired pNPC specimens. There was no significant
difference with p-Stat3 staining between paired pNPC and rNPC
(P=0.433). In addition, we observed no change in cytoplasmic
Jab1/Csn5 (P=0.478), cytoplasmic Akt (P=0.176), or CHOP (P=0.229)
(Fig. 2).
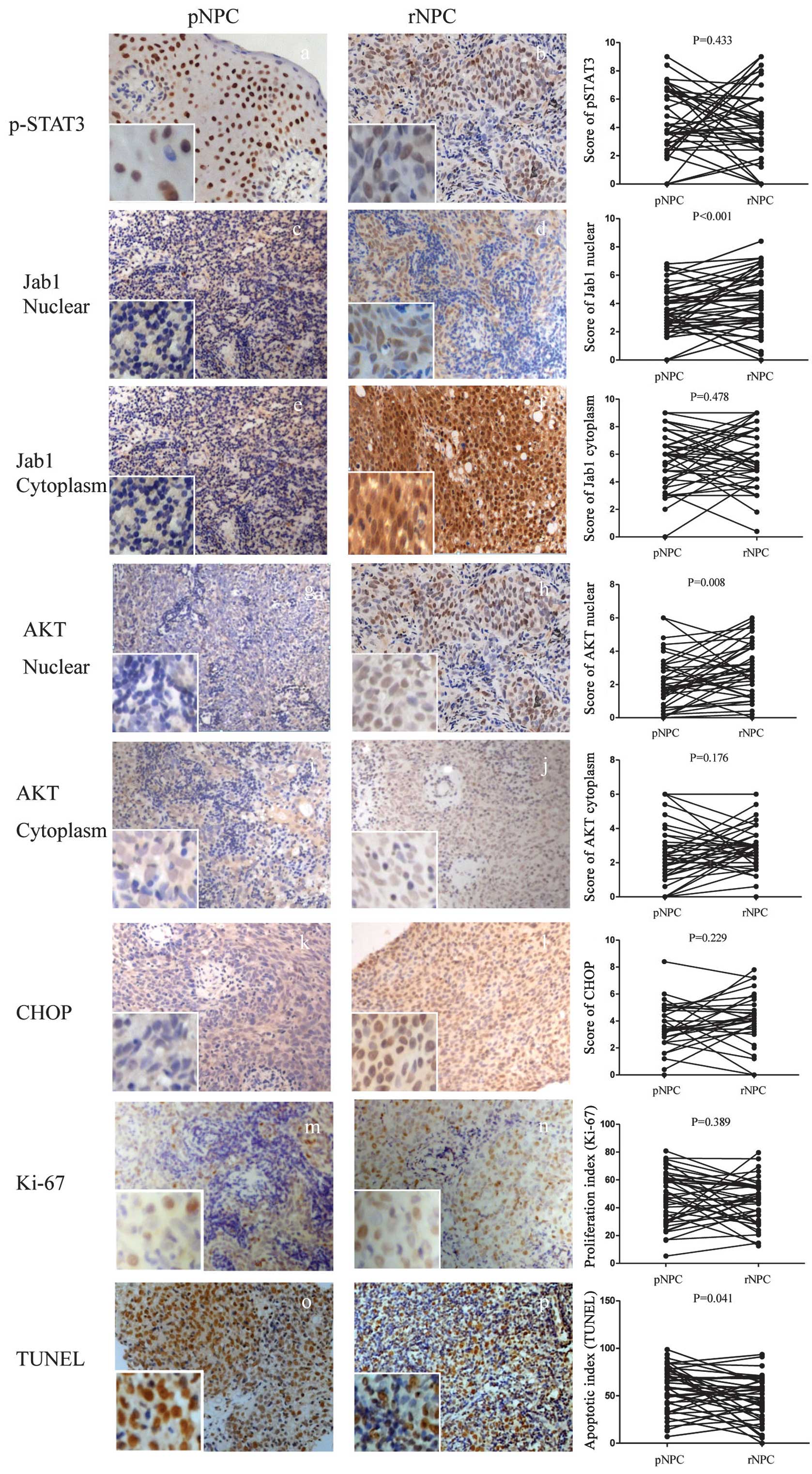 | Figure 2Immunohistochemical staining of (A
and B) p-Stat3, (C and D) Jab1 nuclear, (E and F) Jab1 cytoplasm,
(G and H) Akt nuclear, (I and J) Akt cytoplasm, (K and L) CHOP, and
(M and N) Ki-67 in paired primary nasopharyngeal carcinoma (pNPC)
and recurrent nasopharyngeal carcinoma (rNPC) samples. Apoptosis
was measured by (O and P) TUNEL in paired pNPC and rNPC samples.
Original magnification, ×200; insets ×400. p-Stat3, phospho-Stat3;
CHOP, C/EBP homologous protein; TUNEL, TdT-mediated dUTP nick
end-labeling. |
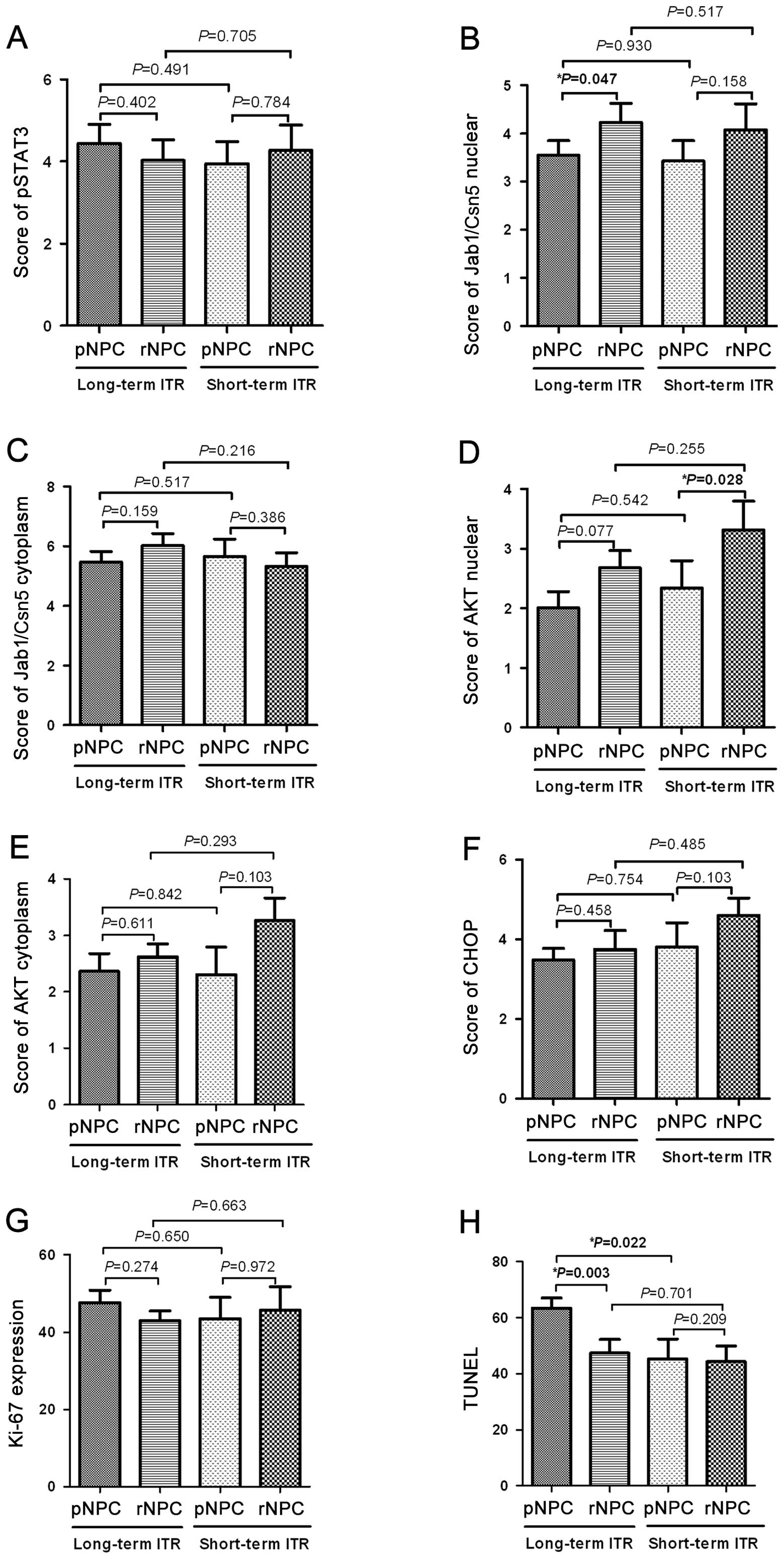
Subset analysis of Jab1/Csn5, p-Stat3,
Akt, and CHOP status in short- and long-term ITR groups
Results for Jab1/Csn5, p-Stat3, Akt, and CHOP status
in the short-Cox regression multivariate analysis and long-term ITR
groups are shown in Fig. 3. p-Stat3
increased in the short-term ITR group and decreased in the
long-term ITR group but did not reach statistical significance.
Compared with pNPC, Jab1/Csn5 nuclear expression significantly
increased (P=0.047) in paired rNPC in the long-term ITR group.
However, there was no significant difference in Jab1/Csn5 nuclear
expression in the short-term ITR group (P=0.158). In contrast to
Jab1/Csn5 status, an increased expression of Akt1 was associated
with the short-term ITR group (P=0.028) in paired tissue samples.
However, there was no significant difference in Jab1/Csn5 nuclear
expression in the short-term ITR group (P=0.158). No significant
difference in CHOP expression was observed in the short-term
(P=0.103) or the long-term (P=0.458) ITR group.
Analysis of Jab1/Csn5, p-Stat3, Akt, and
CHOP status in pNPC and rNPC samples considering ITR subgroups
The pNPC samples in the long-term ITR group did not
significantly differ in expression of Jab1/Csn5 nuclear (P=0.930),
cytoplasmic Jab1/Csn5 (P=0.517), p-Stat3 (P=0.491), Akt nuclear
(P=0.542), cytoplasmic Akt (P=0.842), and CHOP (P=0.754) compared
with the short-term ITR group. Furthermore, no significant
differences were observed in Jab1/Csn5 nuclear (P=0.517),
cytoplasmic Jab1/Csn5 (P=0.216), p-Stat3 (P=0.705), Akt nuclear
(P=0.255), cytoplasmic Akt (P=0.293), and CHOP (P=0.485) expression
in the rNPC samples from the long-term ITR group, compared with
rNPC samples from the short-term ITR group (Fig. 3).
Significant apoptosis increased in pNPC
between short- and long-term ITR
Proliferation and apoptosis were measured with Ki-67
and TUNEL, respectively. In the 45 paired tissue samples, Ki-67
staining did not differ significantly between pNPC and rNPC
(P=0.389). However, we found by TUNEL assay that apoptosis was
lower in rNPC compared with pNPC (P=0.041). In the subset analysis
of the long-term ITR group, the Ki-67 results did not differ
significantly between pNPC and rNPC samples (P=0.274). However,
apoptosis measured by TUNEL was conspicuously lower in the rNPC
samples than in the pNPC samples (P=0.003). We found that in the
pNPC samples the baseline TUNEL results differed significantly
between the short- and long-term ITR groups (median of 47.2 vs.
59.2%, P=0.022). Correlation analysis of Ki-67 and TUNEL indicated
that there was no correlation between proliferation and apoptosis
in the pNPC samples (P=0.566) or in the rNPC samples (P=0.890).
Compared with the pNPC samples from the short-term ITR group, we
only found a significant difference in TUNEL (P=0.022) in the pNPC
samples from the long-term ITR group.
Discussion
There are no generally acknowledged criteria for
determining which patients are likely to develop rNPC, and
identification of a subset of patients with worse clinical outcome
has not been well established in rNPC. To define such criteria,
prognostic factors for rNPC following radiotherapy treatment need
to be determined. To the best of our knowledge, this is the first
study on rNPC using paired initial and recurrent tumor specimens
from the same patients to evaluate the significance of ITR. Thus,
we analyzed the intra-individual changes between pNPC and rNPC of
several biomarkers, especially between the short-term (<18
months) and long-term (≥18 months) ITR groups, and we further
identified useful molecular markers for distinguishing the two
groups.
An accurate definition of rNPC and the careful
acquisition of study samples are crucial. Previous studies have
been hampered by rNPC samples mixed with persistent tumor as well
as by false-positive rNPC without pathologic confirmation (11–15).
Although no standardized definition of rNPC exists, confirmation by
biopsy is widely accepted as the ‘gold standard’. In most studies,
however, only a small proportion of rNPC samples could be obtained
and most patients had their disease diagnosed clinically, owing to
the technical difficulty of obtaining biopsy specimens from sites
of recurrence close to critical organs (10). In the present study, we analyzed 45
paired pNPC and rNPC samples from patients that presented at two
different institutions located within an endemic area and covering
a period of over a decade. We found that short-term ITR was closely
associated with poor survival, and the Cox regression model
supported ITR as an independent negative prognostic factor for rNPC
(HR 0.211; 95% CI, 0.053–0.841; P=0.027).
Although rNPC is considered an incurable disease and
patients need to receive palliative chemotherapy, several
investigators nonetheless have observed long-term ITR patients with
good outcomes (14,15). Heterogeneity of tumor cells and a
biological mechanism involved in this process may be due to
Jab1/Csn5, which positively regulates cell proliferation by
inactivating p27, cyclin E, Smad 4/7, and p53 or by stabilizing
hypoxia inducible factor (HIF-1α), which has been identified as a
poor prognostic factor in several cancer types (31). Recently, we found that Jab1/Csn5
positively regulates the DNA repair gene Rad51 and
contributes to radiation resistance in NPC (23); Therefore, we hypothesized that
Jab1/Csn5 participates in the process of recurrence after radical
radiotherapy in NPC patients. The results of the present study show
that nuclear Jab1/Csn5 was highly overexpressed in the paired rNPC
tissues compared with pNPC samples. However, the subgroup analysis
reveals that nuclear Jab1/Csn5 increased from pNPC to rNPC in the
long-term ITR group. Therefore, another signaling pathway may exist
in short-term ITR that facilitates tumor progression.
Stat3, an oncogenic transcriptional factor that is
activated to initiate transcription of Stat3-targeted genes, is
important in cell proliferation, invasion, and tumor formation.
p-Stat3 is the main type that undergoes activation, and it has the
potential to be an antitumor target (32,33).
Overexpression of Stat3 has been observed in various cancer tissues
including HNSCC (34) as well as in
NPC (35). However, there is a
contradiction between clinical outcomes and Stat3 activation.
Although 67.5% of NPC samples were stained with p-Stat3 and Stat3
activation was positively associated with stage III and IV disease
(28), Hsiao et al found
that coactivation of constitutively activated Stat3 and Stat5 is
associated with improved outcome. Thus, a geographic difference in
Stat3 status may exist (36). The
expression of p-Stat3 in rNPC has not been reported. In the present
study, positive p-Stat3 expression was 84.09 and 80.00% in paired
pNPC and rNPC, respectively. Pectasides et al deduced that
Stat3 may play a dual role in HNSCC during different stages,
depending on the genetic background (27). In the present study, we found that
p-Stat3 tended to be greater in the short-term ITR group than in
the long-term ITR group. Thus, p-Stat3 may play a dual role: in
support of carcinogenesis in early events and of tumor suppression
in late events.
The PI3K/Akt pathway is one of the most attractive
signaling pathways for targeted therapy, especially given emerging
evidence showing that this pathway plays a key role in EBV-induced
disease, as demonstrated by increases in genomic instability, cell
proliferation, and cytoskeleton dynamics and a decrease in
apoptosis (37). Downstream
activation of the Akt pathway is closely associated with
radio-resistance (38), and a high
expression of Akt1 has been associated with worse outcome after
radiotherapy in HNSCC (39). Those
findings support our results that Akt1 was highly expressed in rNPC
compared with pNPC. Subgroup analysis shows that Akt1 was
significantly elevated in the short-term ITR group (P=0.028) but
not the long-term ITR group. We hypothesized that Akt1 is a key
molecule in rNPC and that Akt activation contributes directly to
the invasiveness of recurrent cancer cells and to a short-term
ITR.
The imbalance between proliferation and apoptosis
may determine the recurrence of a tumor and its recurrent stage.
Aberrant apoptosis is required for rNPC development. In our study,
proliferation remained active in recurrent tumors, compared with
primary tumors, without significant change. However, apoptosis was
suppressed in recurrent tumors. This was similar to the findings of
Seong et al in paired colorectal cancer samples (40). We further analyzed the ITR subgroups
and observed, contrary to our hypothesis, a significant decrease in
apoptosis in the long-term ITR group. We found that the baseline
TUNEL level was higher in the long-term ITR group than in the
short-term ITR group. Hsiao et al found that ER stress/UPR
may occur prior to EBV infection and trigger genetic changes in NPC
carcinogenesis (29). CHOP
expression is low under non-stressed conditions, but when ER
stress-induced CHOP increases, it further triggers downstream
proteins and induces cells to undergo apoptosis. We failed to
observe any changes in CHOP expression between paired pNPC and rNPC
samples.
In summary, results of the present biomarker study
have shown that a biological mechanism is involved in the
carcinogenesis of rNPC and that differences between short- and
long-term ITR may predict outcome. Overexpression of Jab1/Csn5 and
Akt may contribute to the carcinogenesis of rNPC, and Akt seems to
promote the progression of short-term ITR. Intra-individual changes
of Jab1/Csn5, Akt, and TUNEL may help to identify short-term
ITR.
Acknowledgements
The present study was supported by a grant from the
National Natural Science Foundation of China (nos. 81172931 and
81071837) and the Scientific and Technological Project of
Guangdong, China (2010B050700016) and grants from the National
Cancer Institute (R01-CA90853 to FXC) and the Sister Institution
Network Fund (FXC).
References
|
1
|
Jemal A, Bray F, Center MM, et al: Global
cancer statistics. CA Cancer J Clin. 61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chan AT: Current treatment of
nasopharyngeal carcinoma. Eur J Cancer. 47(Suppl 3): S302–303.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lee AW, Sze WM, Au JS, et al: Treatment
results for nasopharyngeal carcinoma in the modern era: The Hong
Kong experience. Int J Radiat Oncol Biol Phys. 61:1107–1116. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chang JT, See LC, Liao CT, et al: Locally
recurrent nasopharyngeal carcinoma. Radiother Oncol. 54:135–142.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chua DT, Sham JS, Kwong DL, et al: Locally
recurrent nasopharyngeal carcinoma: treatment results for patients
with computed tomography assessment. Int J Radiat Oncol Biol Phys.
41:379–386. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ng WT, Lee MC, Hung WM, et al: Clinical
outcomes and patterns of failure after intensity-modulated
radiotherapy for nasopharyngeal carcinoma. Int J Radiat Oncol Biol
Phys. 79:420–428. 2011. View Article : Google Scholar
|
|
7
|
Su SF, Han F, Zhao C, Huang Y, et al:
Treatment outcomes for different subgroups of nasopharyngeal
carcinoma patients treated with intensity-modulated radiation
therapy. Chin J Cancer. 30:565–573. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yang TS, Ng KT, Wang HM, et al: Prognostic
factors of locoregionally recurrent nasopharyngeal carcinoma - a
retrospective review of 182 cases. Am J Clin Oncol. 19:337–343.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lee AW, Foo W, Law SC, et al: Recurrent
nasopharyngeal carcinoma: the puzzles of long latency. Int J Radiat
Oncol Biol Phys. 44:149–156. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Xu T, Tang J, Gu M, et al: Recurrent
nasopharyngeal carcinoma: a clinical dilemma and challenge. Curr
Oncol. 20:e406–e419. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chua DT, Sham JS, Kwong PW, et al: Linear
accelerator-based stereotactic radiosurgery for limited, locally
persistent, and recurrent nasopharyngeal carcinoma: efficacy and
complications. Int J Radiat Oncol Biol Phys. 56:177–183. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lee AW, Foo W, Law SC, et al: Total
biological effect on late reactive tissues following reirradiation
for recurrent nasopharyngeal carcinoma. Int J Radiat Oncol Biol
Phys. 46:865–872. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hwang JM, Fu KK and Phillips TL: Results
and prognostic factors in the retreatment of locally recurrent
nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys.
41:1099–1111. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Teo PM, Kwan WH, Chan AT, et al: How
successful is high-dose (> or = 60 Gy) reirradiation using
mainly external beams in salvaging local failures of nasopharyngeal
carcinoma? Int J Radiat Oncol Biol Phys. 40:897–913. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Oksüz DC, Meral G, Uzel O, Cağatay P and
Turkan S: Reirradiation for locally recurrent nasopharyngeal
carcinoma: treatment results and prognostic factors. Int J Radiat
Oncol Biol Phys. 60:388–394. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chou J, Lin YC, Kim J, et al:
Nasopharyngeal carcinoma - review of the molecular mechanisms of
tumorigenesis. Head Neck. 30:946–963. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kong QL, Hu LJ, Cao JY, et al:
Epstein-Barr virus-encoded LMP2A induces an epithelial-mesenchymal
transition and increases the number of side population stem-like
cancer cells in nasopharyngeal carcinoma. PLoS Pathog.
6:e10009402010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Port RJ, Pinheiro-Maia S, Hu C, et al:
Epstein-Barr virus induction of the Hedgehog signalling pathway
imposes a stem cell phenotype on human epithelial cells. J Pathol.
231:367–377. 2013.PubMed/NCBI
|
|
19
|
Cho WC: Nasopharyngeal carcinoma:
molecular biomarker discovery and progress. Mol Cancer. 6:12007.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gao W, Li JZ, Ho WK, et al: Biomarkers for
use in monitoring responses of nasopharyngeal carcinoma cells to
ionizing radiation. Sensors (Basel). 12:8832–8846. 2012. View Article : Google Scholar
|
|
21
|
Wang HY, Sun BY, Zhu ZH, et al:
Eight-signature classifier for prediction of nasopharyngeal
[corrected] carcinoma survival. J Clin Oncol. 29:4516–4525. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Krikelis D, Bobos M, Karayannopoulou G, et
al: Expression profiling of 21 biomolecules in locally advanced
nasopharyngeal carcinomas of Caucasian patients. BMC Clin Pathol.
13:12013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pan Y, Zhang Q, Atsaves V, et al:
Suppression of Jab1/CSN5 induces radio- and chemo-sensitivity in
nasopharyngeal carcinoma through changes to the DNA damage and
repair pathways. Oncogene. 32:2756–2766. 2013. View Article : Google Scholar :
|
|
24
|
Pan Y, Wang M, Bu X, et al: Curcumin
analogue T83 exhibits potent antitumor activity and induces
radiosensitivity through inactivation of Jab1 in nasopharyngeal
carcinoma. BMC Cancer. 13:3232013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pan Y, Zhang Q, Tian L, et al: Jab1/CSN5
negatively regulates p27 and plays a role in the pathogenesis of
nasopharyngeal carcinoma. Cancer Res. 72:1890–1900. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chen CC, Chen WC, Lu CH, et al:
Significance of interleukin-6 signaling in the resistance of
pharyngeal cancer to irradiation and the epidermal growth factor
receptor inhibitor. Int J Radiat Oncol Biol Phys. 76:1214–1224.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pectasides E, Egloff AM, Sasaki C, et al:
Nuclear localization of signal transducer and activator of
transcription 3 in head and neck squamous cell carcinoma is
associated with a better prognosis. Clin Cancer Res. 16:2427–2434.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Liu YP, Tan YN, Wang ZL, et al:
Phosphorylation and nuclear translocation of STAT3 regulated by the
Epstein-Barr virus latent membrane protein 1 in nasopharyngeal
carcinoma. Int J Mol Med. 21:153–162. 2008.PubMed/NCBI
|
|
29
|
Hsiao JR, Chang KC, Chen CW, et al:
Endoplasmic reticulum stress triggers XBP-1-mediated up-regulation
of an EBV oncoprotein in nasopharyngeal carcinoma. Cancer Res.
69:4461–4467. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Xia Y, Wong NS, Fong WF and Tideman H:
Upregulation of GADD153 expression in the apoptotic signaling of
N-(4-hydroxyphenyl) retinamide (4HPR). Int J Cancer. 102:7–14.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shackleford TJ and Claret FX: JAB1/CSN5: a
new player in cell cycle control and cancer. Cell Div. 5:262010.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wang X, Crowe PJ, Goldstein D and Yang JL:
STAT3 inhibition, a novel approach to enhancing targeted therapy in
human cancers (Review). Int J Oncol. 41:1181–1191. 2012.PubMed/NCBI
|
|
33
|
Germain D and Frank DA: Targeting the
cytoplasmic and nuclear functions of signal transducers and
activators of transcription 3 for cancer therapy. Clin Cancer Res.
13:5665–5669. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Grandis JR, Drenning SD, Zeng Q, et al:
Constitutive activation of Stat3 signaling abrogates apoptosis in
squamous cell carcinogenesis in vivo. Proc Natl Acad Sci USA.
97:4227–4232. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lui VW, Yau DM, Wong EY, et al:
Cucurbitacin I elicits anoikis sensitization, inhibits cellular
invasion and in vivo tumor formation ability of nasopharyngeal
carcinoma cells. Carcinogenesis. 30:2085–2094. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hsiao JR, Jin YT, Tsai ST, et al:
Constitutive activation of STAT3 and STAT5 is present in the
majority of nasopharyngeal carcinoma and correlates with better
prognosis. Br J Cancer. 89:344–349. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Morrison JA, Gulley ML, Pathmanathan R and
Raab-Traub N: Differential signaling pathways are activated in the
Epstein-Barr virus-associated malignancies nasopharyngeal carcinoma
and Hodgkin lymphoma. Cancer Res. 64:5251–5260. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kim IA, Bae SS, Fernandes A, et al:
Selective inhibition of Ras, phosphoinositide 3 kinase, and Akt
isoforms increases the radiosensitivity of human carcinoma cell
lines. Cancer Res. 65:7902–7910. 2005.PubMed/NCBI
|
|
39
|
Nijkamp MM, Hoogsteen IJ, Span PN, et al:
Spatial relationship of phosphorylated epidermal growth factor
receptor and activated AKT in head and neck squamous cell
carcinoma. Radiother Oncol. 101:165–170. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Seong J, Chung EJ, Kim H, et al:
Assessment of biomarkers in paired primary and recurrent colorectal
adenocarcinomas. Int J Radiat Oncol Biol Phys. 45:1167–1173. 1999.
View Article : Google Scholar : PubMed/NCBI
|