Introduction
Oral squamous cell carcinoma (OSCC) has a poor
prognosis and outcome. It is one of the six most common types of
cancer, with an annual incidence of >300,000 cases worldwide
(1–3). Although cancer therapy has improved
within the last three decades (particularly advanced radiotherapy
with or without chemotherapy and enhanced surgical procedures), the
prognosis remains poor, with an average 5-year survival rate of 55%
(1,4,5).
Promising immunotherapies that use specific antigen-antibody
interactions may diminish this disappointing outcome. MAGE-A
antigens are only expressed in certain cancer cells, fetal tissue,
placenta and testis but not in healthy tissue, except in the
thyroid where it is expressed only to a small degree (6). MAGE-A antigens belong to MAGE antigen
group I, a type of cancer/testis antigen (CTA) that is localized on
the X chromosome and appears to play a key role in tumorigenesis in
many types of cancer, including those of the head and neck
(7,8). MAGE-A1, which is the first type of
antigen recognized by cytotoxic T lymphocytes, marks the first of
these subtypes. The remaining subtypes A2-A12 (with the exception
of MAGE-A7, which presents itself as a pseudogene) all appear to be
interesting immunogenic markers that could be used for cancer
therapy (8). Their expression has
been described for several types of tumors, such as breast
carcinoma, non-small cell lung cancer and squamous cell carcinoma
of the head and neck (9–11). Several authors have suggested that
MAGE-A antigens are associated with the development and maintenance
of aggressive characteristics in tumors (12,13).
Therefore, these antigens could represent tools to improve the
diagnosis, therapy and prognosis of OSCC. Recently, a cocktail of
more than five MAGE-A subgroups (stained by the antibody MAGE57B)
was shown to have interesting expression rates in OSCC (14–19).
Therefore, the detailed expression of each subtype is now of
particular interest and should be determined. The rates for each
MAGE-A subtype in OSCC were investigated in this study.
Furthermore, the differences in the tumor center and invasive front
were examined. Previous studies have described different
characteristics of cells in the center and at the invasive front of
the same tumor. These studies showed that there were higher
mutation rates of p53 or kinase-inhibitor p21 and a higher rate of
cell proliferation at the invasive front (20–22).
Expression rates of MAGE-A antigens at different tumor sites could
have clinical value as indicators of high progressive tumor growth,
guiding the switch to more radical therapeutic strategies or the
generation of individual patient protocols. Hartmann et al
have already investigated the efficacy of chemotherapeutics on
tumor cell lines that expressed several MAGE-A types (23) and also evaluated the use of
monoclonal antibodies such as cetuximab and panitumumab (24). Their investigations clarified the
need to even more precisely identify the particular MAGE-A subtypes
that influence the failure of chemotherapy and immune therapy in
OSCC.
Materials and methods
Patients and tissue microarrays
The pathological samples for this study were
selected from the archives of the Department of Pathology of the
University of Würzburg, Germany. Sixty-eight paraffin-embedded
OSCCs with clear evidence of invasive fronts at the deep surface of
the biopsy were chosen. The anatomic source of the biopsy specimens
included the tongue, lip, tonsil, cheek, palate, oropharynx and
other sites of the oral cavity, but no sites with respiratory
epithelia. The mean age of the patients at diagnosis was 56.85
years (SD: 13.0 years), and the study sample included 51 males and
17 females. Twenty-seven tumors were stage T1, 17 were stage T2 and
21 cancers were stage T3 or higher. The staging for 3 samples was
not evaluable (Table I).
 | Table IThe patient specimens: Separate
examination of the different clinical parameters was performed due
to the heterogeneous retrospective data. |
Table I
The patient specimens: Separate
examination of the different clinical parameters was performed due
to the heterogeneous retrospective data.
| T1 | T2 | T3 | T4 |
|---|
| n=65 | 27 | 17 | 9 | 12 |
| N0 | N1 | N2 | |
| n=52 | 36 | 9 | 7 | |
| UICC 1 | UICC 2 | UICC 3 | UICC 4 |
| n=65 | 25 | 13 | 12 | 15 |
From each case, a representative block was
retrieved, and tissue microarrays (TMAs) of the tumor invasive
front and the tumor center were constructed such that each case was
represented by three 0.6 mm cores (Fig.
1). One-micron-thick sections were cut and mounted on
saline-coated slides.
Immunohistochemical staining
As a positive control for immunohistochemical
staining, normal adult testis tissue was used. As negative
controls, either healthy lung tissue or testis without the use of
secondary antibodies was used. One-micron-thick sections of the
TMAs were cut and mounted on saline-coated slides.
Phosphate-buffered saline (PBS) was used as the diluent for washing
and rinsing steps throughout the immunohistochemistry protocol,
except for the purposes of antigen retrieval. The antibodies of
MAGE-A1-A12 were diluted as shown in Table II.
| Table IIOrigin, dilution and source of the
MAGE-A antibodies used in the study. |
Table II
Origin, dilution and source of the
MAGE-A antibodies used in the study.
| Antigen | Origin | Code | Heat buffer | Dilution | Source |
|---|
| MAGE A1 | Rabbit | Cat # RP 144,
144-05, Lot # 066N, ABIN125659 | CA | 1:100 | Antibodies online
(Aachen, Germany) |
| MAGE A2 | Rabbit | (N-18)
sc-130164
Lot # D0209 | TR | 1:20
| Santa Cruz
biotechnology, Inc., Dallas, TX, USA |
| MAGE A3 | Rabbit |
NBP-1-02506
Lot # 20930 | CA | 1:100 | Novus Biologicals
(LLC, CO, USA) |
| MAGE A4 | Rabbit | Cat # PAB 4746, Lot
# SH030122L | TR | 1:40 | Abnova, Taipei
City, Taiwan |
| MAGE A5 | Rabbit | Cat #
PAB-10795
Lot # RB 2085 | CA | 1:100 | Antibodies online
(Aachen, Germany), www.allele.biotech.com |
| MAGE A6 | Rabbit | ABIN303468, Lot #
20945 | CA | 1:100 | Antibodies online
(Aachen, Germany) |
| MAGE A8 | Rabbit | (v-25), sc-102016,
Lot # G0708 | TR | 1:30 | Santa Cruz
biotechnology, Inc. |
| MAGE A9 | Rabbit | (G-24), sc-130811,
Lot # H2010 | TR | 1:10 | Santa Cruz
biotechnology, Inc. |
| MAGE A10 | Rabbit | Cat # PAB4741, Lot
# SH030124Q | TR | 1:10 | Abnova |
| MAGE A11 | Rabbit | (N-16), sc-130162,
Lot # I1809 | TR | 1:40 | Santa Cruz
biotechnology, Inc. |
| MAGE A12 | Rabbit | Cat # PAB4743, Lot
# SA110311AH | TR | 1:10 | Abnova |
The TMA sections were deparaffinized, rehydrated and
subjected to antigen retrieval by autoclaving for 15 min in
individually tested buffer saline as shown in the Table II. The sections were incubated with
primary antibody for 1 h at room temperature, followed by detection
using the DAKO Advance+ detection system (DakoCytomation, Pathology
Products Dako Deutschland GmbH, Hamburg, Germany) and DAB as the
chromogen. The slides were counterstained with hematoxylin and
evaluated.
For investigation, the dual system of Remmele and
Stegner (25) that was first used
in breast cancer was used to evaluate the levels of antigen
expression and generate a score [amount of staining (SI): 0, no
reaction, 1, weak reaction, 2, moderately high reaction, 3, strong
reaction; number of positive cells (PP): 0, negative, 1, <10%
positive cells, 2, 10–50% positive cells, 3, 21–80% positive cells,
4, >80% positive cells]: SI × PP = Immunoreactive score
(IRS).
As different punches of the tumor center and the
tumor invasive front were prepared, an IRS (C) for the center, an
IRS (F) for the front and an IRS (T) were evaluated. The IRS (T)
represents the whole tumor tissue in this study, and its value was
determined through summation as follows: IRS (T) = IRS (total) =
IRS (C) + IRS (F).
For graphical presentation, IRS (T) has been
simplified into four score groups of staining grade (0, negative,
1, weak, 2, medium and 3, high).
Statistical analysis of expression rates and
clinical parameters was performed with the help of the Department
of the Mathematical Branch of the University of Würzburg using
Statistica 10® (StatSoft, Tulsa, OK, USA) and SPSS
20® (IBM, Armonk, NY, USA). Investigation included using
the Spearman's correlation, Mann-Whitney U test, Kruskal-Wallis
test and Gehan's test. For additional investigation of detailed
information within the groups, the post hoc test was applied.
Results
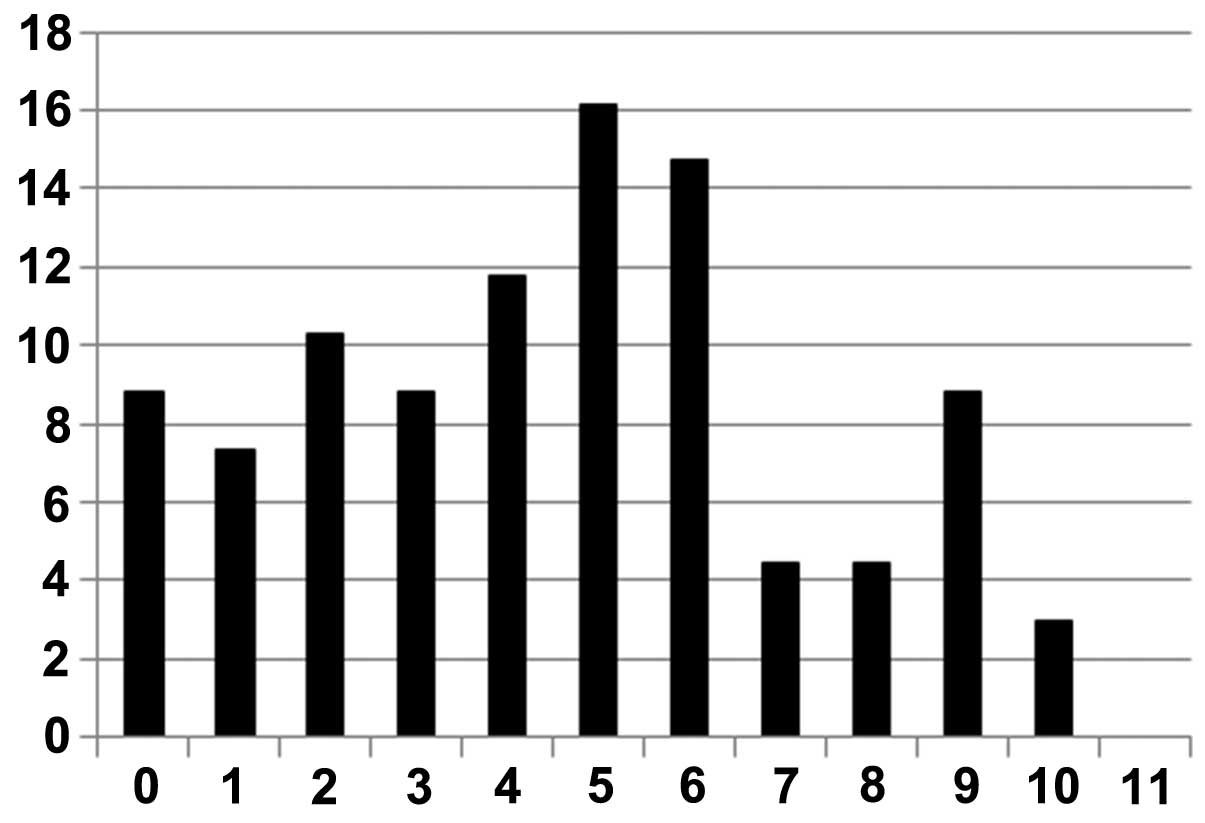
General expression rates of MAGE-A
Among 68 tumors, 62 (91.17%) had antigen expression
of several individual MAGE-A subtypes, and 6 tumors (8.82%) had no
staining.
As shown in Fig. 2,
36 tumors (52.94%) had simultaneous expression of five or more
MAGE-A subtypes. Expression of one to four MAGE-A antigens was
observed in 26 (38.24%) specimens. Six tumors (8.82%) had no
staining for any of the MAGE-A subtypes, as shown in the first
column of Fig. 2.
The highest expression rates (summarized through
scoring grade 1, 2 and 3) were observed for MAGE-A2 (90%), -A3
(97%), -A4 (90%), -A10 (93%) and -A12 (94%).
Statistical investigation of the correlation between
expression of five or more antigen subtypes in a single tumor
revealed no significant differences in any clinical parameters
(P>0.05).
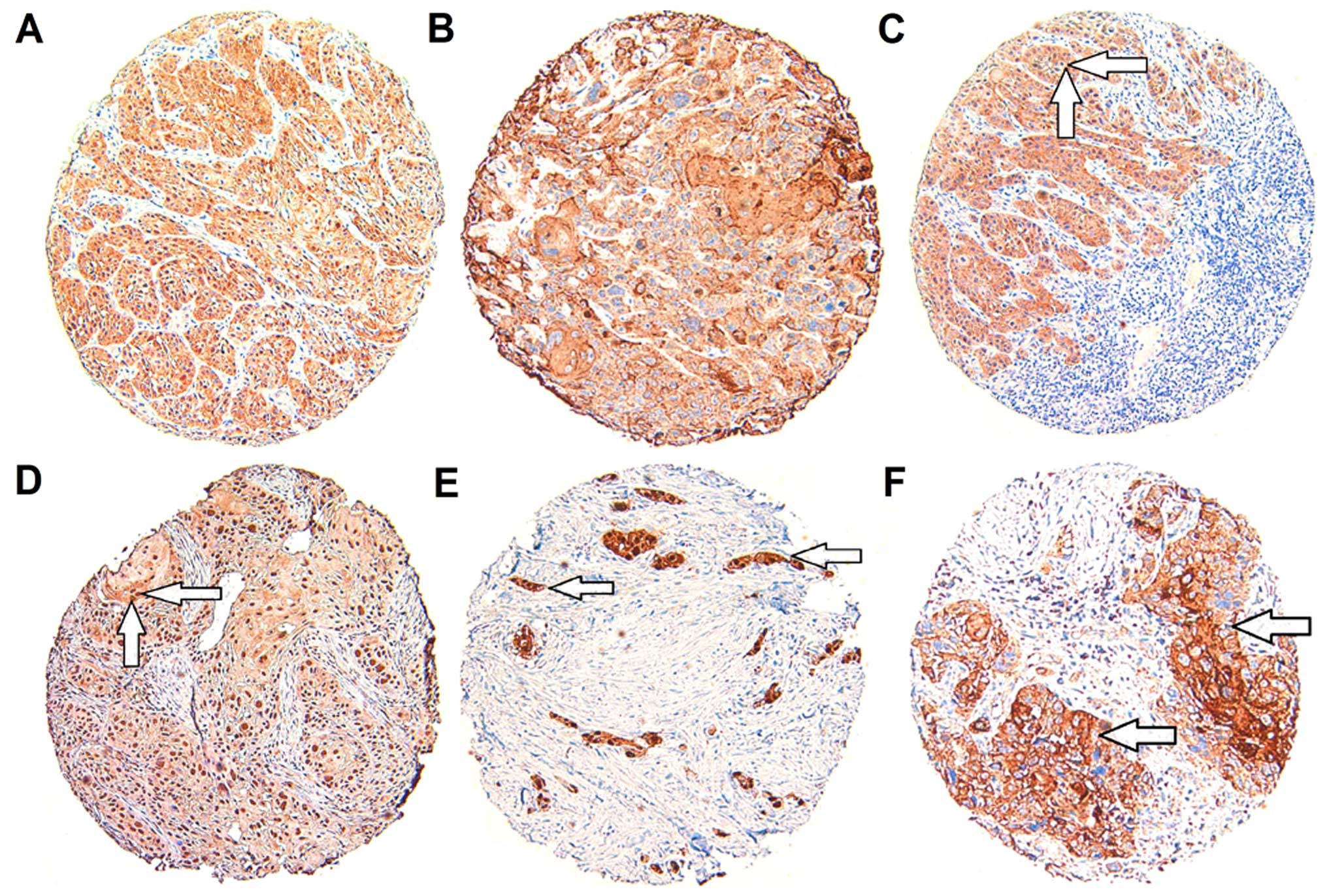
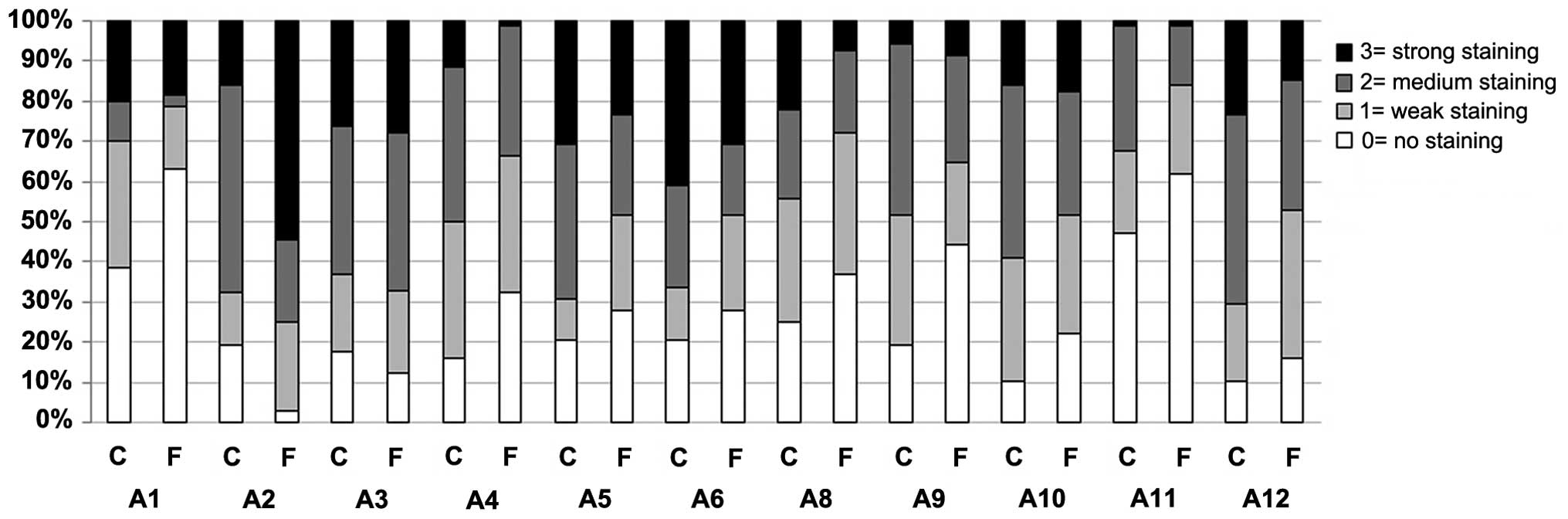
Expression in the tumor center and tumor
invasive front
For MAGE-A1, -A4, -A5, -A6, -A8, -A9, -A10, -A11 and
-A12, there was higher expression in the tumor center than in the
tumor invasive front. Only MAGE-A2 and -A3 clearly exhibited the
opposite behavior as shown in Fig.
4.
Statistical investigation using immunoreactive score
[IRS (C)/IRS (F)] showed a significant difference in the expression
between the tumor invasive front and tumor center for the MAGE-A
subtypes A1, A5, A6, A9 and A12 as shown in Table III. This difference occurred for
all of the subtypes with stronger expression in the tumor center.
For the other MAGE-A subgroups, the results were not
significant.
| Table IIIComparison of expression in the tumor
center and tumor front. |
Table III
Comparison of expression in the tumor
center and tumor front.
| A1 | A2 | A3 | A4 | A5 | A6 | A8 | A9 | A10 | A11 | A12 |
|---|
| P-value | 0.01 | 0.13 | 0.12 | 0.46 | 0.01 | 0.02 | 0.11 | 0.05 | 0.54 | 0.15 | 0.01 |
| Valid cases | 60a | 68 | 68 | 68 | 68 | 68 | 68 | 68 | 68 | 68 | 68 |
Correlation of MAGE-A expression with
clinical parameters
For correlation of expression with clinical
parameters, the overall MAGE-A expression for each subtype was
determined and the additional values, represented by IRS (T), were
used for statistical analysis.
Age
The study group was divided into 3 groups according
to age (1, 35–50 years, 2, 51–70 years and 3, 71–85 years). Within
these groups, MAGE-A subtypes were represented by staining score
(0, 1, 2 and 3). The highest scores occurred in group 2 (51–70
years), with the exception of MAGE-A10, for which group 3 (71–85
years) had the highest staining scores. Statistical investigation
using Spearman's correlation showed no significant results
(P>0.05) for any of the MAGE-A subtypes.
Gender
For MAGE-A1, -A2, -A5, -A6, -A8, -A10 and -A12,
higher staining and therefore higher expression occurred in
specimens from men, while MAGE-A3, -A4, -A9 and -A11 exhibited the
opposite behavior. This result must be regarded differentially
because of the small number of female specimens (n=17) in the
study. Only MAGE-A1 had significantly higher expression in the
whole tumor of male specimens as evaluated by the Mann-Whitney U
test (P=0.034). In the tumor center, only a trend in the expression
of MAGE-A1 for higher grade male specimens was observed (P=0.05).
No other results were significant (P>0.05).
Tumor size
In this study, we found that for all MAGE-A
antigens, the tumors in stage T3 showed the highest expression.
Tumors in stage T1 had less expression than those in stage T2.
However, a difference in expression rates was not observed between
T3 and T4. Nevertheless, statistical investigation using
Kruskal-Wallis test did not show any significant difference between
the stages for any of the tested MAGE-A antigens (P>0.05).
Lymph node status
For MAGE-A1, -A2, -A6, -A8, -A10, -A12, no
significant differences were observed between the groups N0, N1 and
N2. For MAGE-A3, there was significantly higher expression in the
tumor center of tumors with associated lymph node metastasis (N1)
compared with those with N0 status (P=0.04). Investigation of the
overall expression in both regions of the tumor (center and front)
revealed significant differences in MAGE-A4 (P=0.02), MAGE-A5
(P=0.02) and MAGE-A9 (P=0.02) with regards to lymph node stages.
For MAGE-A11, a significant difference was only observed for the
tumor invasive front (P=0.04).
Grading
Regarding the grading stage of the tumors, no
significant differences between the stage groups and any of the
tested MAGE-A antigens were found (P>0.05).
UICC (Union International Contre le
Cancer) stage (disease stage)
Only MAGE-A9 expression significantly differed in
the invasive tumor front region of the tumors with regards to UICC
stage (P=0.02). Detailed post hoc testing showed that the highest
significance was between groups I and IV (P=0.04), which suggests
increased malignancy when the expression is elevated.
Survival time
Neither MAGE-A expression nor the expression of five
or more antigens were significantly correlated to the survival
time. Because of the heterogeneity of the available data, a
connection between expression and decreased survival time should
not be generally disregarded.
Discussion
This is the first study to use the expression rates
of all MAGE-A subtypes to compare the tumor center and tumor front
in OSCC via detailed immunohistochemistry. The study showed that
there was expression of MAGE-A antigens in 62 of 68 specimens
(91.17%). Furthermore, 36 of 68 (52.94%) tumors expressed five or
more of the eleven tested antigens. This rate is higher than those
previously reported in other studies (14–18).
Comparison of the expression in the tumor center and
the invasive front revealed that MAGE-A1, -A4, -A5, -A6, -A8, -A9,
-A10, -A11 and -A12 were more highly expressed in the center and
that the results were statistically significant for MAGE-A1, -A5,
-A6, -A8 and -A12. In contrast, expression was higher in the
invasive front for MAGE-A2 and -A3, but this difference was not
statistically significant.
Because the invasive front is regarded as the site
associated with malignant characteristics such as a higher
incidence of p53 mutation, higher levels of Ki-67, more
proliferating cells and high epithelial-mesenchymal transition
(EMT), our findings are peculiar (20–22).
The transition from the somatic cell type to cells with mesenchymal
characteristics includes loss of apical-basal polarity, impairment
of important cell-cell interactions and therefore higher fragility,
higher cell mortality and destabilization of the basal membrane
layer (26,27). Because EMT is related to
de-differentiation and MAGE-A expressing cells can also exhibit
de-differentiation, a relationship between MAGE-A expression and
EMT may exist (28,29). Because our results appear to be
contrary to those of previous studies, further investigation is
needed to clarify the association between EMT and MAGE-A expression
at the tumor front and center.
Promoter demethylation and histone deacetylation are
regarded as the key steps for inducing MAGE-A expression in tumor
cells (13,30–33).
However, several authors have also described the absence of CTA
expression in tumors with general DNA hypomethylation (34,35).
Moreover, there is an assumption that a necessary
'switching-on' of a gameto-genetic program exists that is derived
from germ cell development and leads somatic cells to express CTAs
(30,36).
Higher expression of MAGE-A antigens in the tumor
center of the specimens in this study group could be explained by
this process of reverting back to a developmental stage and
augmenting the life span of tumor cells.
However, Aprelikova et al showed a connection
between downregulation of MAGE-A11 and a negative influence on
hypoxia-inducible factor HIF-1α in OSCC; HIF-1α is believed to play
a key role in malignant behavior (e.g., resistance to radiotherapy
or chemotherapy) of tumor cells with hypoxic surroundings, which
are typically found at the center of tumors (37). Moreover, Hartmann et al
investigated the negative impact on the effectiveness of therapy
for the chemotherapeutics diamindichloridoplatin (DDP) and
5-fluorouracil when high levels of MAGE-A11 were present and found
that expression of MAGE-A5 and -A8 resulted in a negative effect on
anti-neoplastic therapy including panitumumab treatment (23,24).
Interestingly, in our study, the same subgroups have higher
expression in the center of the tumor, particularly MAGE-A5.
Because the tumor center is the location where so-called 'cancer
stem cells' originate and typically proliferate slowly, it is
possible that these cells are less practical targets for
chemotherapy, which clarifies the frequent occurrence of refractory
lapses of the disease (38). These
findings clarify the influence of malignant characteristics through
the effects of MAGE-A expression on development.
The correlation between patient age and MAGE-A
expression was not significant. Nevertheless, the study group with
the highest staining rates was the patients between 51 and 70 years
of age. These findings can be explained by the fact that genomic
hypomethylation increases the probability of MAGE-A expression and
increasing age promotes this condition (39,40).
However, in terms of oral cancer, patients of this age group often
present with typical risk factors such as smoking and simultaneous
alcoholism, which suggests the potential of a relationship or even
a direct interaction between MAGE-A expression with the presence of
risk factors.
As was shown significantly for MAGE-A1 as well as
for MAGE-A2, -A5, -A6, -A8, -A10 and -A12, male specimens have a
tendency to present higher expression rates of CTAs or rather
higher staining rates by immunohistochemistry. Because males are
much more frequently heavy smokers and drinkers, a direct
connection between these risk factors and augmented MAGE-A
expression could also be hypothesized.
In addition, tumor size did not significantly
correlate with increased MAGE-A expression, as was described in
most previous studies. Nevertheless, Müller-Richter et al
showed an augmentation of expression rates with the increase of
tumor size, and napoletano et al showed a significant
correlation between tumor size of cervical cancer and expression of
MAGE-A1, -A2,- A3, -A4, -A6, -A12 using a global MAGE57B antibody
(40,41).
However, based on their use of this special global
antibody, the studies must be compared and regarded
differentially.
Our results showed a correlation of MAGE-A
expression with the general presence of lymph node metastasis
(N+) that was significant for MAGE-A3, -A4, -A5, -A9,
and -A11. This correlation did not impact on whether the tumor was
stage N1 or N2. Again, the evaluation of Hartmann et al
(23) is of interest because they
clearly specified that MAGE-A5, -A8 and -A11 are negative
predictors of OSCC. The presence of lymph node metastasis normally
leads to application of adjuvant therapy, which is often combined
with additional chemotherapy (42,43).
Therefore, the currently discussed MAGE-A types may represent novel
indicators that could lead to more aggressive approaches, even in
cases with no positive lymph node status but high expression of
certain MAGE-A subtypes. The present study is the first time a
significant correlation between MAGE-A expression and further lymph
node status in OSCC has been investigated (15,18).
Similar results have been reported only for other types of tumors,
such as ductal breast, colorectal or gastric cancer (44–46).
Here, significant results for all tests regarding
lymph node status were obtained, especially for MAGE-A4. In
addition, Forghanifard et al described similar results in
their studies for MAGE-A4 in SCC of the esophagus (47). MAGE-A4 was also one of the most
expressed subtypes in the present study, and Ries et al
(14) showed that MAGE-A4 had the
highest expression rates in OSCC.
This difference in expression might represent a
reliable tool for the prognosis of OSCC. Moreover, a significantly
worse response to the chemotherapeutics docetaxel and paclitaxel
occurred for tumors that expressed MAGE-A4, similar to the findings
reported by Müller-Richter et al (48). For MAGE-A5, significant results were
obtained in general and for the tumor center. Other studies have
not yet reported such results in OSCC but have done so for other
malignancies, such as lung cancer and colorectal cancer, with
comparable findings reported (49).
Our non-significant findings regarding tumor grade are in contrast
to the results of previous studies by Ries et al (14), Figueiredo et al (17) and Eura et al (11), who described significantly higher
malignancy and grading in connection with high MAGE-A expression in
their studies of OSCC and head and neck cancers.
Because the 'cancer stem-cell theory' exists and
other authors have proposed that only cells with the
characteristics of stem cells within a tumor mass are able to
express CTAs, de-differentiation could be explained. Literature
results regarding the heterogeneity of cells in a tumor and the
ability or inability to express antigens should be stressed
(50,51).
Correlation studies of UICC stage to expression
showed that there was significant expression of MAGE-A9 and a trend
for MAGE-A6 in the tumor center. Gu et al recently found
that in HCC, MAGE-A9 expression is an independent prognostic factor
for disease-free survival and overall survival and that high
MAGE-A9 expression suggests unfavorable survival outcomes in HCC
patients (52). In addition, Xu
et al recently reported similar results in breast cancer,
suggesting that the MAGE-A9 subtype should be regarded as a
favorable tool for the evaluation of the prognosis of patients with
malignant disease (53). Shigematsu
et al showed significantly higher expression of MAGE-A4 in
stage II–IV non-small cell lung cancer relative to stage I
(54). Because these results only
applied to the tumor center, this result also supports the often
postulated higher prognostic value of the tumor invasive front
(20–22,55,56).
Several authors have already described significantly lower 5-year
survival rates of patients with certain types of cancers (57–59)
that express MAGE-A antigens; therefore, the results of this study
have to be considered critically. Investigating larger patient
groups may allow us to draw more reliable conclusions.
Although cure rates in OSCC are improving slowly
with current therapeutic methods, the present study reveals that
MAGE-A3, -A4, -A5, -A9, -A11 are factors that are related to
metastatic tendencies and therefore could be used as prognostic
tools for improving the follow-up care of patients with OSCC.
References
|
1
|
Barnes L, Eveson JW, Reichart P and
Sidransky D: World Health Organization Classification of Tumours:
Pathology and Genetics of Head and Neck Tumours. IARC Press; Lyon:
2005
|
|
2
|
Al-Swiahb JN, Chen CH, Chuang HC, Fang FM,
Tasi HT and Chien CY: Clinical, pathological and molecular
determinants in squamous cell carcinoma of the oral cavity. Future
Oncol. 6:837–850. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Stucken E, Weissman J and Spiegel JH: Oral
cavity risk factors: Experts' opinions and literature support. J
Otolaryngol Head Neck Surg. 39:76–89. 2010.PubMed/NCBI
|
|
4
|
Folz BJ, Silver CE, Rinaldo A, Fagan JJ,
Pratt LW, Weir N, Seitz D and Ferlito A: An outline of the history
of head and neck oncology. Oral Oncol. 44:2–9. 2008. View Article : Google Scholar
|
|
5
|
Scully C and Bagan JV: Recent advances in
Oral Oncology 2007: Imaging, treatment and treatment outcomes. Oral
Oncol. 44:211–215. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jungbluth AA, Busam KJ, Kolb D, Iversen K,
Coplan K, Chen YT, Spagnoli GC and Old LJ: Expression of
MAGE-antigens in normal tissues and cancer. Int J Cancer.
85:460–465. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Katsura Y and Satta Y: Evolutionary
history of the cancer immunity antigen MAGE gene family. PLoS One.
6:e203652011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
van der Bruggen P, Traversari C, Chomez P,
Lurquin C, De Plaen E, Van den Eynde B, Knuth A and Boon T: A gene
encoding an antigen recognized by cytolytic T lymphocytes on a
human melanoma. Science. 254:1643–1647. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
van der Bruggen P, Bastin J, Gajewski T,
Coulie PG, Boël P, De Smet C, Traversari C, Townsend A and Boon T:
A peptide encoded by human gene MAGE-3 and presented by HLA-A2
induces cytolytic T lymphocytes that recognize tumor cells
expressing MAGE-3. Eur J Immunol. 24:3038–3043. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lee KD, Eura M, Ogi K, Nakano K,
Chikamatsu K, Masuyama K and Ishikawa T: Expression of the MAGE-1,
-2, -3, -4, and -6 genes in non-squamous cell carcinoma lesions of
the head and neck. Acta Otolaryngol. 116:633–639. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Eura M, Ogi K, Chikamatsu K, Lee KD,
Nakano K, Masuyama K, Itoh K and Ishikawa T: Expression of the MAGE
gene family in human head-and-neck squamous-cell carcinomas. Int J
Cancer. 64:304–308. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Barker PA and Salehi A: The MAGE proteins:
Emerging roles in cell cycle progression, apoptosis, and
neurogenetic disease. J Neurosci Res. 67:705–712. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Simpson AJ, Caballero OL, Jungbluth A,
Chen YT and Old LJ: Cancer/testis antigens, gametogenesis and
cancer. Nat Rev Cancer. 5:615–625. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ries J, Schultze-Mosgau S, Neukam F,
Diebel E and Wiltfang J: Investigation of the expression of
melanoma antigen-encoding genes (MAGE-A1 to -A6) in oral squamous
cell carcinomas to determine potential targets for gene-based
cancer immunotherapy. Int J Oncol. 26:817–824. 2005.PubMed/NCBI
|
|
15
|
Ries J, Vairaktaris E, Mollaoglu N,
Wiltfang J, Neukam FW and nkenke E: Expression of
melanoma-associated antigens in oral squamous cell carcinoma. J
Oral Pathol Med. 37:88–93. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kienstra MA, Neel HB, Strome SE and Roche
P: Identification of NY-ESO-1, MAGE-1, and MAGE-3 in head and neck
squamous cell carcinoma. Head Neck. 25:457–463. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Figueiredo DL, Mamede RC, Proto-Siqueira
R, Neder L, Silva WA Jr and Zago MA: Expression of cancer testis
antigens in head and neck squamous cell carcinomas. Head Neck.
28:614–619. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Montoro JR, Mamede RC, Neder Serafini L,
Saggioro FP, Figueiredo DL, Silva WA Jr, Jungbluth AA, Spagnoli GC
and Zago MA: Expression of cancer-testis antigens MAGE-A4 and
MAGE-C1 in oral squamous cell carcinoma. Head Neck. 34:1123–1128.
2012. View Article : Google Scholar
|
|
19
|
Cuffel C, Rivals JP, Zaugg Y, Salvi S,
Seelentag W, Speiser DE, Liénard D, Monnier P, Romero P, Bron L, et
al: Pattern and clinical significance of cancer-testis gene
expression in head and neck squamous cell carcinoma. Int J Cancer.
128:2625–2634. 2011. View Article : Google Scholar
|
|
20
|
Piffkò J, Bànkfalvi A, Tory K, Füzesi L,
Bryne M, Ofner D, Kusch F, Joos U and Schmid KW: Molecular
assessment of p53 abnormalities at the invasive front of oral
squamous cell carcinomas. Head Neck. 20:8–15. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Horta MC, de Assis LA, de Souza AF, de
Araújo VC, Gomez RS and Aguiar MC: p53 and p21WAF1/CIP1
overexpression at the invasive front of lower lip squamous cell
carcinoma. J Oral Pathol Med. 36:88–92. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tumuluri V, Thomas GA and Fraser IS: The
relationship of proliferating cell density at the invasive tumour
front with prognostic and risk factors in human oral squamous cell
carcinoma. J Oral Pathol Med. 33:204–208. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hartmann S, Kriegebaum U, Küchler N,
Brands RC, Linz C, Kübler AC and Müller-Richter UD: Correlation of
MAGE-A tumor antigens and the efficacy of various chemotherapeutic
agents in head and neck carcinoma cells. Clin Oral Investig.
18:189–197. 2014. View Article : Google Scholar
|
|
24
|
Hartmann S, Kriegebaum U, Küchler N,
Lessner G, Brands RC, Linz C, Schneider T, Kübler AC and
Müller-Richter UD: Efficacy of cetuximab and panitumumab in oral
squamous cell carcinoma cell lines: Prognostic value of MAGE-A
subgroups for treatment success. J Craniomaxillofac Surg.
41:623–629. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Remmele W and Stegner HE: Recommendation
for uniform definition of an immunoreactive score (IRS) for
immunohistochemical estrogen receptor detection (ER-ICA) in breast
cancer tissue. Pathologe. 8:138–140. 1987.In German. PubMed/NCBI
|
|
26
|
Thiery JP: Epithelial-mesenchymal
transitions in tumour progression. Nat Rev Cancer. 2:442–454. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yang CC, Zhu LF, Xu XH, Ning TY, Ye JH and
Liu LK: Membrane type 1 matrix metalloproteinase induces an
epithelial to mesenchymal transition and cancer stem cell-like
properties in SCC9 cells. BMC Cancer. 13:1712013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Thiery JP: Epithelial-mesenchymal
transitions in development and pathologies. Curr Opin Cell biol.
15:740–746. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kalluri R and Weinberg RA: The basics of
epithelial-mesenchymal transition. J Clin Invest. 119:1420–1428.
2009. View
Article : Google Scholar : PubMed/NCBI
|
|
30
|
Caballero OL and Chen YT: Cancer/testis
(CT) antigens: Potential targets for immunotherapy. Cancer Sci.
100:2014–2021. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Karpf AR, Bai S, James SR, Mohler JL and
Wilson EM: Increased expression of androgen receptor coregulator
MAGE-11 in prostate cancer by DNA hypomethylation and cyclic AMP.
Mol Cancer Res. 7:523–535. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Scanlan MJ, Gure AO, Jungbluth AA, Old LJ
and Chen YT: Cancer/testis antigens: An expanding family of targets
for cancer immunotherapy. Immunol Rev. 188:22–32. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wischnewski F, Pantel K and Schwarzenbach
H: Promoter demethylation and histone acetylation mediate gene
expression of MAGE-A1, -A2, -A3, and -A12 in human cancer cells.
Mol Cancer Res. 4:339–349. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wang Z, Zhang J, Zhang Y, Srivenugopal KS
and Lim SH: SPAN-XB core promoter sequence is regulated in myeloma
cells by specific CpG dinucleotides associated with the MeCP2
protein. Int J Cancer. 119:2878–2884. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lim SH, Zhang Y and Zhang J: Cancer-testis
antigens: The current status on antigen regulation and potential
clinical use. Am J Blood Res. 2:29–35. 2012.PubMed/NCBI
|
|
36
|
Old LJ: Cancer/testis (CT) antigens - a
new link between gametogenesis and cancer. Cancer Immun.
1:12001.
|
|
37
|
Aprelikova O, Pandolfi S, Tackett S,
Ferreira M, Salnikow K, Ward Y, Risinger JI, Barrett JC and
Niederhuber J: Melanoma antigen-11 inhibits the hypoxia-inducible
factor prolyl hydroxylase 2 and activates hypoxic response. Cancer
Res. 69:616–624. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Patel SS, Shah KA, Shah MJ, Kothari KC and
Rawal RM: Cancer stem cells and stemness markers in oral squamous
cell carcinomas. Asian Pac J Cancer Prev. 15:8549–8556. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Liu L, Wylie RC, Andrews LG and Tollefsbol
TO: Aging, cancer and nutrition: The DNA methylation connection.
Mech Ageing Dev. 124:989–998. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Müller-Richter UD, Dowejko A, Peters S,
Rauthe S, Reuther T, Gattenlöhner S, Reichert TE, Driemel O and
Kübler AC: MAGE-A antigens in patients with primary oral squamous
cell carcinoma. Clin Oral Investig. 14:291–296. 2010. View Article : Google Scholar
|
|
41
|
Napoletano C, Bellati F, Tarquini E, Tomao
F, Taurino F, Spagnoli G, Rughetti A, Muzii L, Nuti M and Benedetti
Panici P: MAGE-A and NY-ESO-1 expression in cervical cancer:
Prognostic factors and effects of chemotherapy. Am J Obstet
Gynecol. 198:99.e1–7. 2008. View Article : Google Scholar
|
|
42
|
Kreppel M, Drebber U, Eich HT, Dreiseidler
T, Zöller JE, Müller RP and Scheer M: Combined-modality treatment
in advanced oral squamous cell carcinoma: Primary surgery followed
by adjuvant concomitant radiochemotherapy. Strahlenther Onkol.
187:555–560. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Adelstein DJ, Lavertu P, Saxton JP, Secic
M, Wood BG, Wanamaker JR, Eliachar I, Strome M and Larto MA: Mature
results of a phase III randomized trial comparing concurrent
chemoradiotherapy with radiation therapy alone in patients with
stage III and IV squamous cell carcinoma of the head and neck.
Cancer. 88:876–883. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kavalar R, Sarcevic B, Spagnoli GC,
Separovic V, Samija M, Terracciano L, Heberer M and Juretic A:
Expression of MAGE tumour-associated antigens is inversely
correlated with tumour differentiation in invasive ductal breast
cancers: An immunohistochemical study. Virchows Arch. 439:127–131.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Li M, Yuan YH, Han Y, Liu YX, Yan L, Wang
Y and Gu J: Expression profile of cancer-testis genes in 121 human
colorectal cancer tissue and adjacent normal tissue. Clin Cancer
Res. 11:1809–1814. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Jung EJ, Kim MA, Lee HS, Yang HK, Lee YM,
Lee BL and Kim WH: Expression of family A melanoma antigen in human
gastric carcinoma. Anticancer Res. 25:2105–2111. 2005.PubMed/NCBI
|
|
47
|
Forghanifard MM, Gholamin M, Farshchian M,
Moaven O, Memar B, Forghani MN, Dadkhah E, Naseh H, Moghbeli M,
Raeisossadati R, et al: Cancer-testis gene expression profiling in
esophageal squamous cell carcinoma: Identification of specific
tumor marker and potential targets for immunotherapy. Cancer Biol
Ther. 12:191–197. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Müller-Richter UD, Dowejko A, Driemel O,
Reuther T, Reichert TE and Kübler AC: Impact of MAGE-A antigens on
taxane response in oral squamous cell carcinoma. Oncol Lett.
1:181–185. 2010.PubMed/NCBI
|
|
49
|
Kim YD, Park HR, Song MH, Shin DH, Lee CH,
Lee MK and Lee SY: Pattern of cancer/testis antigen expression in
lung cancer patients. Int J Mol Med. 29:656–662. 2012.PubMed/NCBI
|
|
50
|
Zajicek G: neoplasia - a stem cell
pathology. Med Hypotheses. 13:125–136. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Costa FF, Le Blanc K and Brodin B: Concise
review: Cancer/testis antigens, stem cells, and cancer. Stem Cells.
25:707–711. 2007. View Article : Google Scholar
|
|
52
|
Gu X, Fu M, Ge Z, Zhan F, Ding Y, Ni H,
Zhang W, Zhu Y, Tang X, Xiong L, et al: High expression of MAGE-A9
correlates with unfavorable survival in hepatocellular carcinoma.
Sci Rep. 4:66252014. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Xu X, Tang X, Lu M, Tang Q, Zhang H, Zhu
H, Xu N, Zhang D, Xiong L, Mao Y, et al: Overexpression of MAGE-A9
predicts unfavorable outcome in breast cancer. Exp Mol Pathol.
97:579–584. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Shigematsu Y, Hanagiri T, Shiota H, Kuroda
K, Baba T, Mizukami M, So T, Ichiki Y, Yasuda M, So T, et al:
Clinical significance of cancer/testis antigens expression in
patients with non-small cell lung cancer. Lung Cancer. 68:105–110.
2010. View Article : Google Scholar
|
|
55
|
Bryne M, Koppang HS, Lilleng R and
Kjaerheim A: Malignancy grading of the deep invasive margins of
oral squamous cell carcinomas has high prognostic value. J Pathol.
166:375–381. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Piffkó J, Bánkfalvi A, Ofner D, Kusch F,
Böcker W, Joos U and Schmid KW: In situ assessment of cell
proliferation at the invasive front of oral squamous cell
carcinomas. Virchows Arch. 429:229–234. 1996.PubMed/NCBI
|
|
57
|
Pastorcic-Grgic M, Sarcevic B, Dosen D,
Juretic A, Spagnoli GC and Grgic M: Prognostic value of MAGE-A and
NY-ESO-1 expression in pharyngeal cancer. Head Neck. 32:1178–1184.
2010. View Article : Google Scholar
|
|
58
|
Suzuki S, Sasajima K, Sato Y, Watanabe H,
Matsutani T, Iida S, Hosone M, Tsukui T, Maeda S, Shimizu K, et al:
MAGE-A protein and MAGE-A10 gene expressions in liver metastasis in
patients with stomach cancer. Br J Cancer. 99:350–356. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Metzler P, Mollaoglu N, Schwarz S, Neukam
FW, Nkenke E and Ries J: MAGE-A as a novel approach in the
diagnostic accuracy of oral squamous cell cancer: A case report.
Head Neck Oncol. 1:392009. View Article : Google Scholar : PubMed/NCBI
|