Introduction
Circulating tumor cells (CTCs) are tumor cells that
are shed from the primary tumor and circulate in the peripheral
blood. CTCs, as a surrogate of distant metastasis, can be
potentially useful for the diagnosis and monitoring of therapeutic
effects in malignant tumors (1).
However, the isolation of rare CTCs contaminated in a large number
of normal hematologic cells is a technical challenge. Among a
variety of systems for the detection of CTCs that have been
developed and tested, CellSearch® (Veridex, LLC,
Raritan, NJ, USA) is the only system approved for clinical use
(2). CellSearch is a semi-automated
system for quantitative evaluation of CTCs; CTCs are isolated using
ferrofluid nanoparticles coupled with an antibody against
epithelial cell adhesion molecule (EpCAM), which is highly
expressed in tumor cells of epithelial origin. The most important
advantage of the CellSearch system is its high reproducibility and
the CTC-testing peformed with CellSearch which has proven to be
clinically useful in monitoring the blood from patients with
metastatic breast, colorectal and prostate carcinoma (3–5).
Conversely, the most critical issue with CellSearch is its low
sensitivity in the detection of CTCs. In fact, our previous study
evaluating the CTC-test in primary lung cancer revealed that CTCs
were not detected in 29% of patients with clinically detectable
distant metastases (6), suggesting
a need for more sensitive detection systems. We also conducted a
study with the CTC-test in malignant pleural mesothelioma (MPM), a
highly aggressive malignant tumor associated with asbestos exposure
(7), and it revealed a very low
diagnostic capability with a sensitivity of 33%. Its low
sensitivity may be largely caused by its incapability to capture
EpCAM-negative tumor cells, such as MPM, which originates from the
mesothelium and may not or only weakly express EpCAM (8), suggesting a need for novel systems of
EpCAM-independent detection of CTCs.
Among a variety of EpCAM-independent CTC-capture
systems including size-based or density-based separation systems
(9), a microfluidic system called a
‘CTC-chip’ has an advantage with its capability of capturing
specific cells with an antibody attached to microposts. Nagrath
et al and Maheswaran et al first reported a higher
sensitivity in the detection of CTCs with a CTC-chip coated with
anti-EpCAM antibodies (10,11). Despite the promising results
reported in a pilot study, no additional study to confirm or
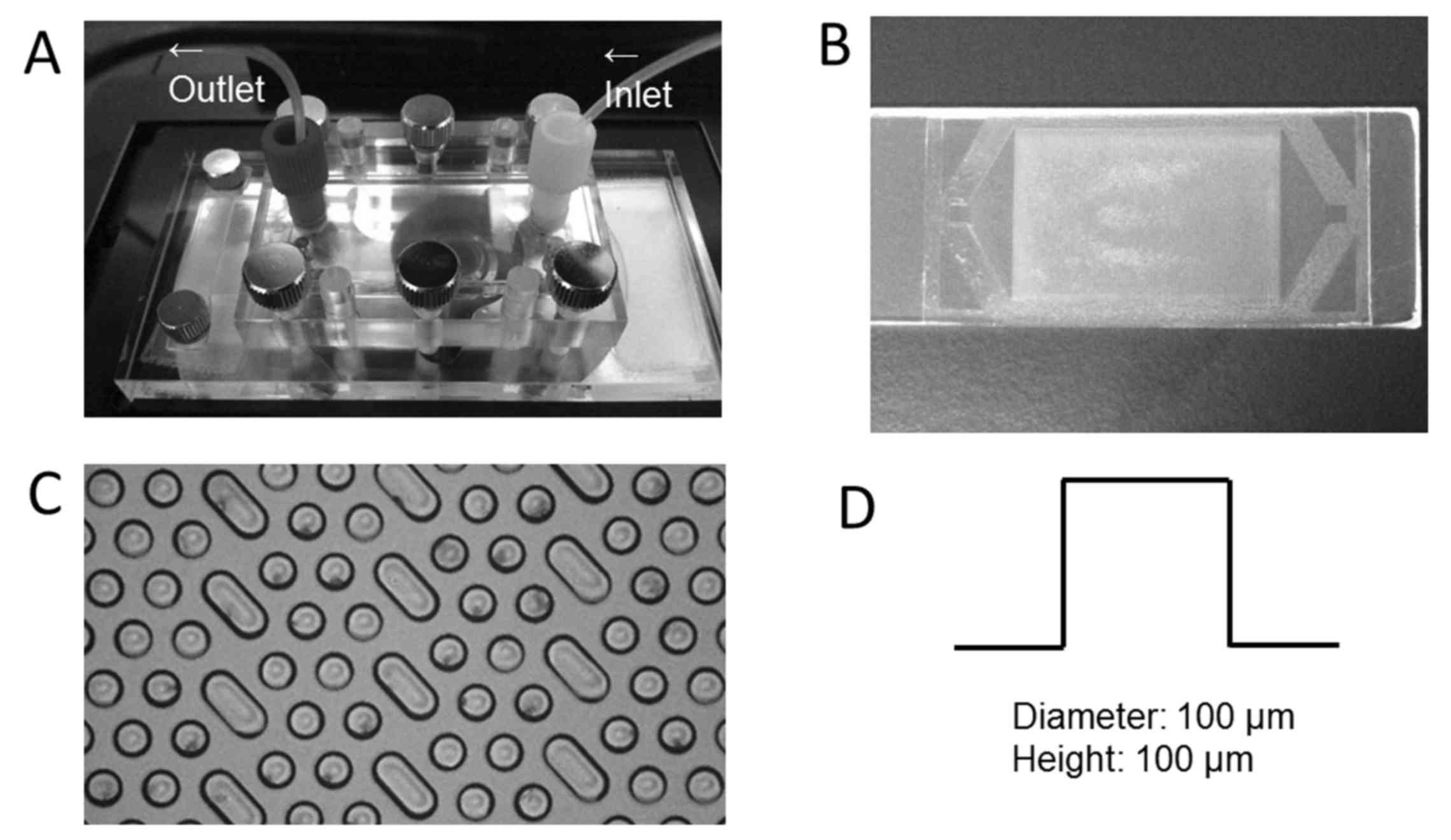
validate its high performance has been reported. A novel polymeric
CTC-chip comprised of light-curable resins has been designed by the
author (T.O.) (12). Among a
variety of advantages of the novel CTC-chip over the ‘original’
CTC-chip including its lower cost, higher durability and improved
transparency, the most important and unique advantage is that any
antibody which captures CTCs is easily conjugated to the chip, as
the chip surface is made reactive with any antibody by the
incorporation of monomers having an epoxy group in the resin
(Fig. 1). Accordingly,
EpCAM-negative CTCs can be potentially captured by the ‘novel’
CTC-chip coated with an antibody against a specific antigen which
is expressed in tumor cells and which may be referred to as a
‘universal CTC-chip’. In the present study, we first showed that
EpCAM-negative MPM cells were effectively captured by the
‘universal CTC-chip’ coated with an antibody against podoplanin
that is expressed in MPM cells.
Materials and methods
Cell lines
Human lung cancer cell line, PC-9 and human
mesothelioma cell line, ACC-MESO-4 established in Aichi Cancer
Research Center (Nagoya, Japan) (13) were purchased from Riken BioResource
Center (Tsukuba, Japan). These cells were cultured in RPMI-1640
medium (Wako Pure Chemical Industries, Osaka, Japan) and
supplemented with 10% fetal bovine serum (Invitrogen, San Diego,
CA, USA) at 37°C in 5% CO2.
Immunocytochemistry
Cells (1×104) were plated on a 24-well
dish and cultured for three days. Cells were fixed with 4%
paraformaldehyde followed by permeabilization with 0.25% Triton
X-100 and blocking with Protein Block (Dako, Glostrup, Denmark).
Then, cells were incubated with a primary antibody, a mouse
anti-human EpCAM monoclonal antibody (clone HEA125) or a mouse
anti-human podoplanin monoclonal antibody (clone E1; both from
Santa Cruz Biotechnology, Dallas, TX, USA) diluted to 1:100 and
incubated for 60 min at room temperature. After 30 min of
incubation at room temperature with a secondary antibody (goat
anti-mouse IgG) conjugated with Alexa Fluor 594 (Life Technologies,
Carlsbad, CA, USA) and diluted to 1:100 containing 1 µg/ml Hoechst
33342 (Cell Signaling Technology, Danvers, MA, USA), images were
acquired with the CKX41 inverted fluorescence microscope (Olympus,
Tokyo, Japan) equipped with a DP73 digital camera (Olympus).
Flow cytometry
Cells were collected and incubated with a primary
antibody, an anti-EpCAM antibody (clone HEA125) or an
anti-podoplanin antibody (clone E1), diluted to 1:100 and incubated
for 20 min at room temperature. Then, the cells were incubated with
a goat anti-mouse IgG antibody conjugated with FITC (BD
Biosciences, San Jose, CA, USA) diluted to 1:20. Flow cytometric
analysis was performed using the EC800 Cell Analyzer (Sony
Biotechnology, Inc., Tokyo, Japan) and FlowJo software (Tree Star,
Inc., Ashland, OR, USA).
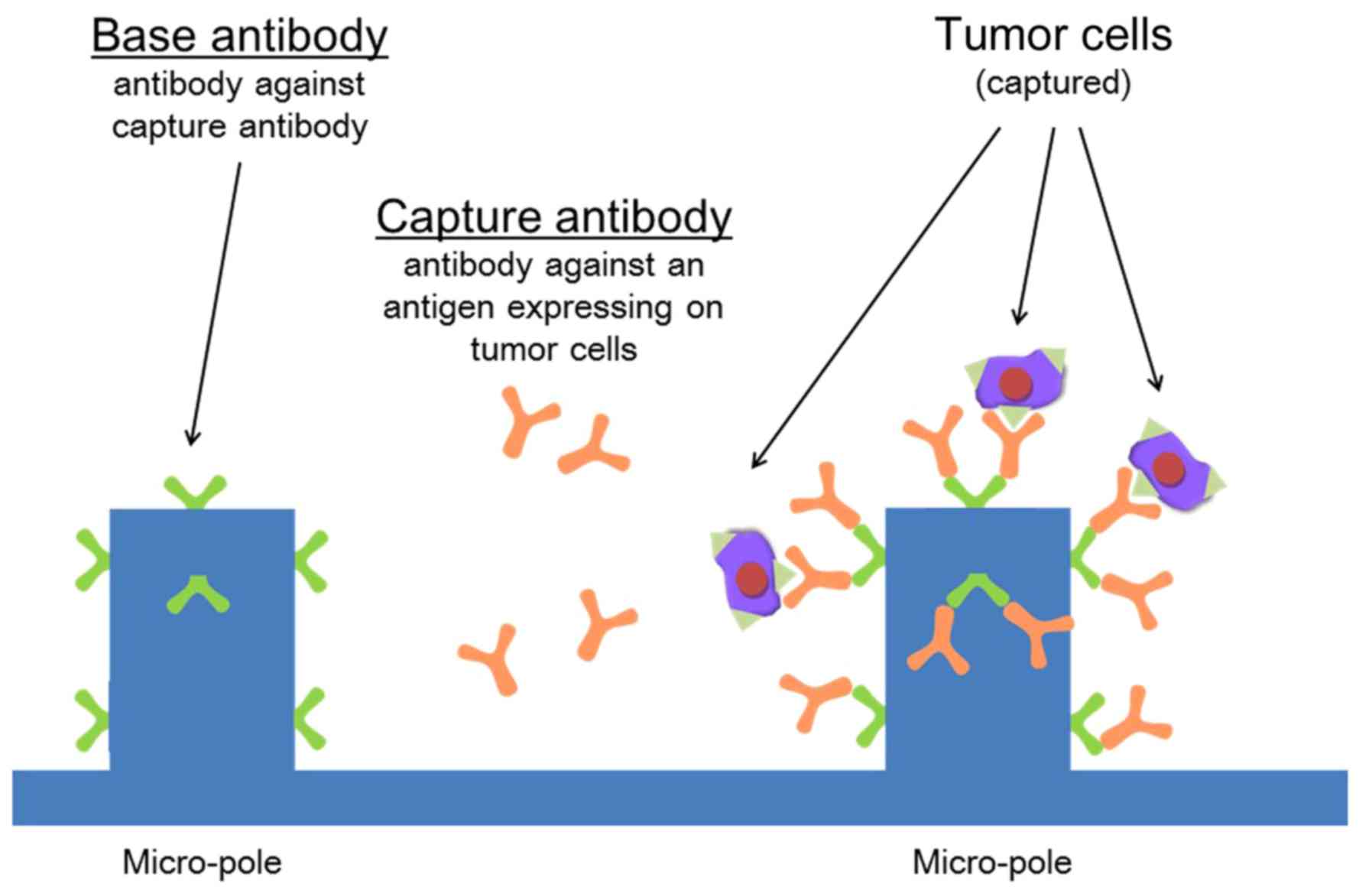
Preparation of CTC-chip
The polymeric CTC-chip system (Fig. 1) (12) was used after a two-step coating with
an antibody to capture CTCs (Fig.
2). In the first step, the chip surface was incubated with a
goat anti-mouse IgG antibody (SouthernBiotech, Birmingham, AL, USA)
in phosphate-buffered saline (PBS) at a concentration of 20 µg/ml
overnight at 4°C and then the chip surface was washed with PBS. In
the next step, the chip surface was incubated with an antibody to
capture CTCs, an anti-human EpCAM antibody (clone HEA125) or a
mouse anti-human podoplanin antibody (clone E1), diluted with PBS
at a concentration of 20 µg/ml and incubated for 1 h at 4°C in
order to react with the surface anti-mouse IgG antibody. After
being washed with PBS, the chip surface was kept wet. The
antibody-coated chip was referred to as the ‘EpCAM-chip’ when
coated with the anti-EpCAM antibody or as the ‘podoplanin-chip’
when coated with the anti-podoplanin antibody.
Sample preparation and flow test
Cells were labeled using the CellTrace™ CFSE Cell
Proliferation kit (Life Technologies) according to the
manufacturers protocol, and then 1,500 cells were suspended in 3 ml
of PBS containing 5% BSA or in 3 ml of the blood sampled from a
healthy volunteer (the author, C.Y.). A cell suspension sample of 1
ml (500 cells/ml) was applied to the CTC-chip system.
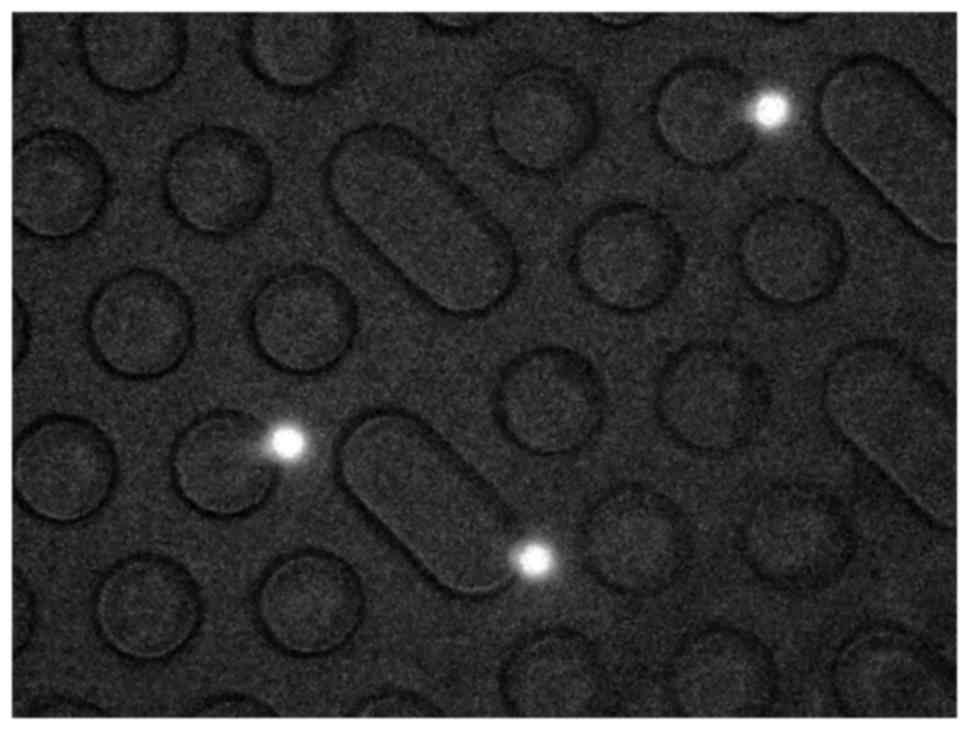
Each sample was sent to the chip using a syringe
pump at a constant flow rate (1.5 ml/h when suspended in PBS or 1.0
ml/h when suspended in the blood). Meanwhile, each sample tube was
shaken to ensure that the cell suspension was homogeneous. Images
and videos of the cells in the chip were monitored and recorded
with a fluorescence microscope CKX41 (Olympus) and a digital video
camera (Sony Biotechnology, Inc.) (Fig.
3). Each experiment, sample preparation and flow test was
performed in triplicate.
Evaluation of cell capture
efficiency
We determined the actual number of cells that were
sent into the chip (N-total) by counting the number of cells that
passed through the inlet of the chip. We also determined the number
of captured cells (N-captured) by counting CFSE-labeled cells
remaining on the chip after completion of the flow test. The cell
capture efficiency was evaluated as N-captured/N-total. The average
value of capture efficiency was calculated from the results
obtained in the triplicate experiments.
Results
Expression of EpCAM and
podoplanin
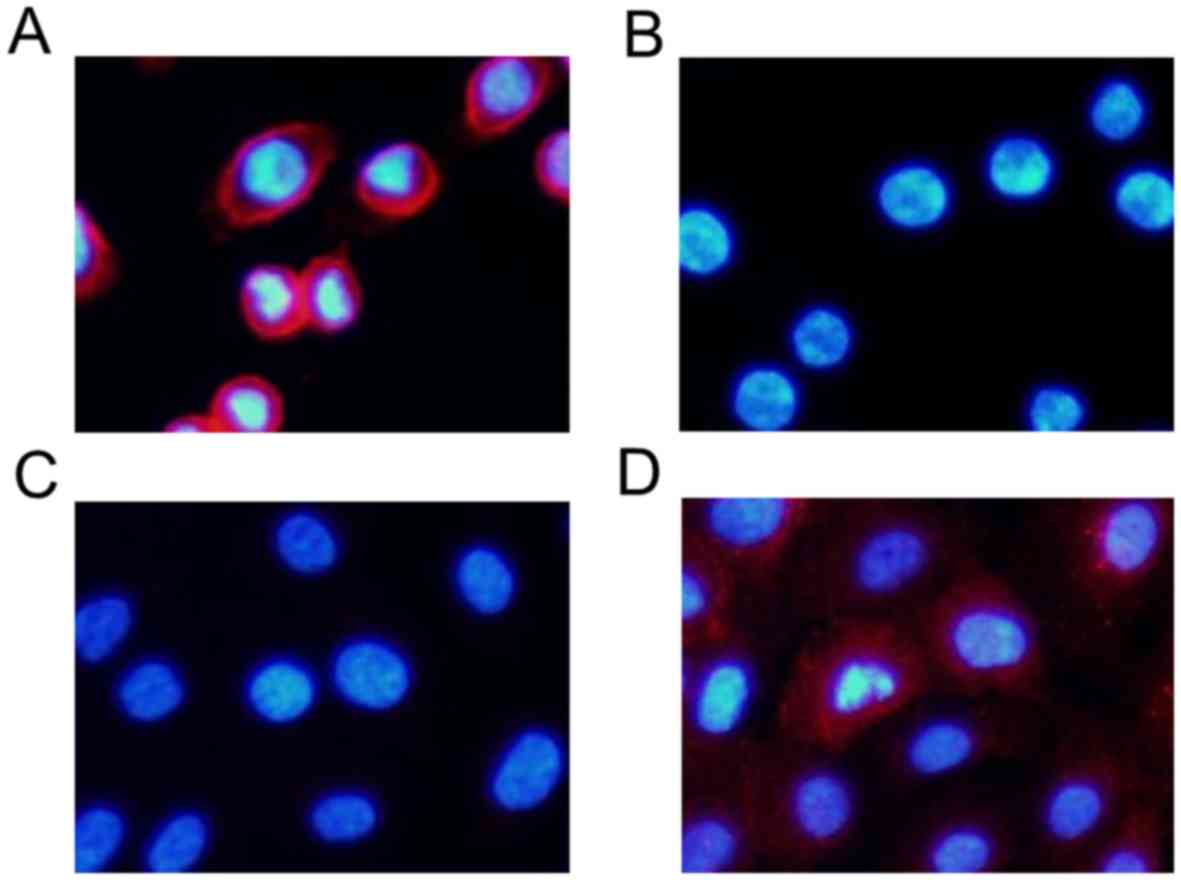
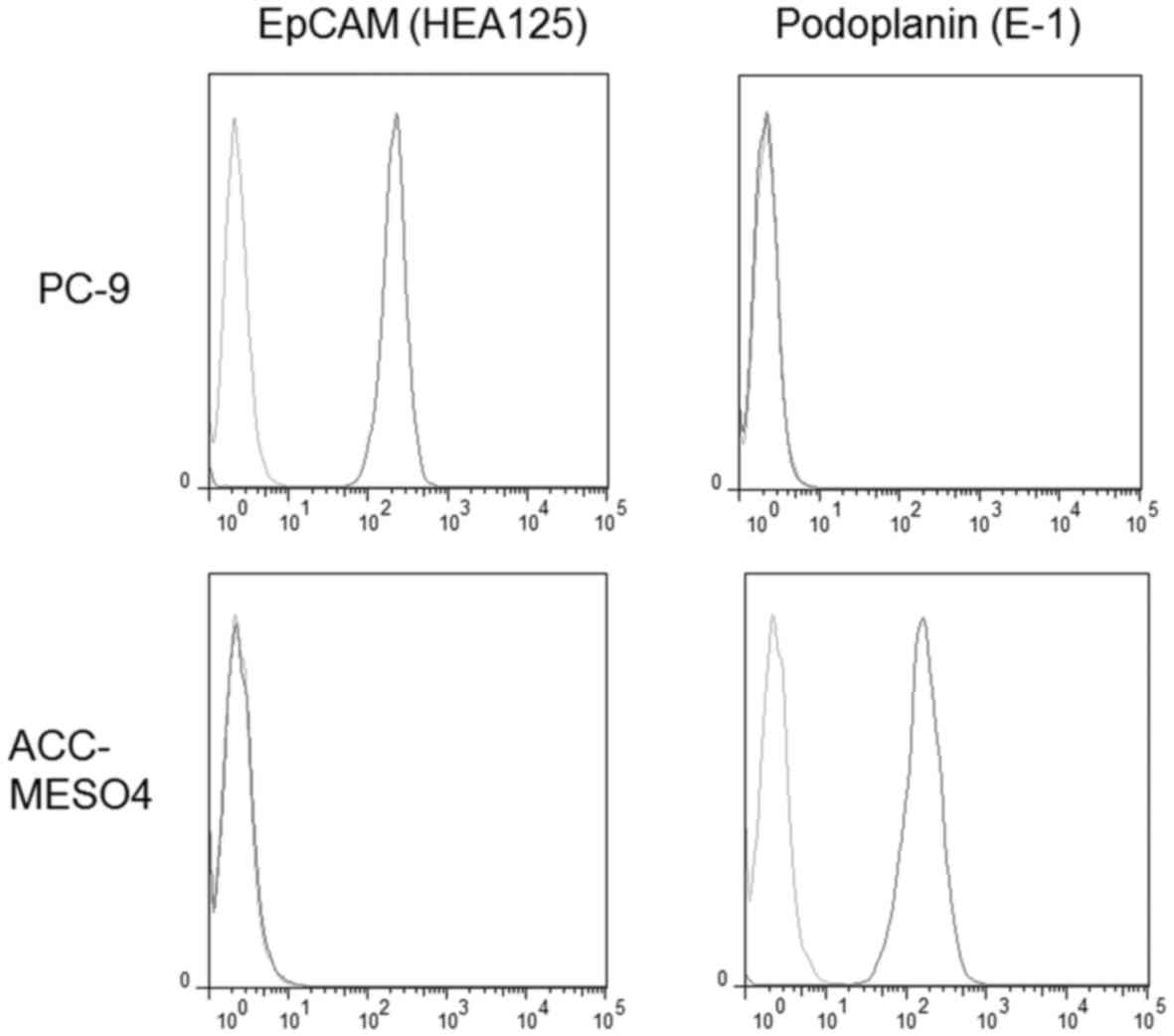
PC-9, a human lung adenocarcinoma cell line,
strongly expressed EpCAM in immunocytochemical staining (Fig. 4) and flow cytometry (Fig. 5). In contrast, ACC-MESO-4, a human
MPM cell line, did not express EpCAM (Figs. 4 and 5).
Conversely, ACC-MESO-4 strongly expressed
podoplanin, an MPM-specific antigen, in immunocytochemical staining
(Fig. 4) and flow cytometry
(Fig. 5), while PC-9 did not
express podoplanin (Figs. 4 and
5).
Cell capture efficiency
Capture from the cell suspension spiked in PBS
(
Fig. 6 and
Table I)
When PC-9 cells were suspended in PBS, the average
capture efficiency for the EpCAM-chip was 101.1%. However, when
ACC-MESO-4 cells were spiked in PBS, the average capture efficiency
for the EpCAM-chip was only 3.0%.
In contrast, when the podoplanin-chip was used to
capture ACC-MESO-4 cells, the average capture efficiency was
markedly increased (78.3%). In contrast, when PC-9 cells were
spiked, the average capture efficiency for the podoplanin-chip was
only 2.3%.
Capture from cell suspension spiked in the blood
(
Fig. 7 and
Table II)
When ACC-MESO-4 cells were suspended in the blood,
the average capture efficiency for the EpCAM-chip was only 2.2%,
but that for the podoplanin-chip was much higher (38.4%). When PC-9
cells were suspended in the blood, the average capture efficiency
of the EpCAM-chip and the podoplanin-chip were 88.0 and 6.9%,
respectively.
Discussion
In the present study, we showed that EpCAM-negative
tumor cells were effectively captured with the novel CTC-chip. This
is the first study to report the isolation of EpCAM-negative tumor
cells using the ‘universal’ CTC-chip, suggesting that the system is
a promising modality to detect a variety of CTCs without EpCAM
expression due to non-epithelial origin or undergoing
epithelial-mesenchymal transition (EMT).
As an EpCAM-negative tumor, we selected an MPM cell
line, ACC-MESO-4, and tested the capture efficiency of the CTC-chip
coated with anti-podoplanin antibody. MPM is a rare malignant tumor
associated with asbestos exposure, but its incidence is
increasingly prevalent worldwide. MPM is a highly aggressive tumor
with a median survival of 4–12 months due to lack of effective
diagnostic and/or treatment modalities (7). The diagnosis of MPM is principally
established with histologic examination, which usually requires
invasive procedures such as a core-needle biopsy or a
video-assisted thoracoscopic biopsy. These invasive procedures may
not be feasible for mass-screening or for patients with poor
performance status, and the development of less invasive diagnostic
procedures is clinically important. A number of noninvasive markers
including serum soluble mesothelin-related protein (SMRP) and serum
osteopontin have been evaluated, but there has been no established
marker for the diagnosis of MPM. In a previous study (8), we evaluated the diagnostic performance
of the CTC-test using CellSearch, and revealed a significant, but
modest diagnostic performance of MPM with a sensitivity of 33%. We
also examined EpCAM expression in MPM originating from the pleural
mesothelium that did not essentially express EpCAM, and revealed
that only 11 of the 21 MPM tumors were EpCAM-positive. In the
present study as well, the MPM cell line, ACC-MESO-4, did not
express EpCAM (Fig. 2A and B).
These results clearly indicate that MPM tumor cells without robust
expression of EpCAM could not effectively be captured with an
EpCAM-dependent CTC-capture system such as CellSearch, which led us
to develop an EpCAM-independent CTC-capture system such as the
‘universal’ CTC-chip.
Among a variety of EpCAM-independent CTC-capture
systems including size-based or density-based separation systems
(1), we adopted a microfluidic
system called the ‘CTC-chip’ due to its capability to capture
specific cells with an antibody attached to microposts. The
original CTC-chip coated with an anti-EpCAM antibody could capture
only EpCAM-positive tumor cells, because another antibody capturing
EpCAM-negative tumor cells was not available in the chip system
(10,11). The novel ‘universal’ CTC-chip, used
in the current study, has overcome this critical issue, as any
antibody for capture can be easily attached to the chip (12). In fact, EpCAM-positive cells of lung
cancer (PC-9) spiked in PBS were perfectly captured with an average
capture efficiency of 101.1% using the chip coated with an
anti-EpCAM antibody (‘EpCAM-chip’); while, when coated with an
anti-podoplanin antibody (‘podoplanin-chip’), podoplanin-positive
cells of MPM (ACC-MESO-4) were effectively captured with an average
capture efficiency of 78.3% (Table
I and Fig. 6). Podoplanin is a
mucin-type transmembrane glycoprotein. Podoplanin expression seen
in limited normal tissues such as lymphatic vessels and in type I
alveolar epithelium, is increased in some malignant tumors
including MPM (14). In fact,
ACC-MESO-4, an MPM cell line, strongly expressed podoplanin
(Figs. 4 and 5) and its cells were captured using the
podoplanin-chip. Some MPM cells do not express podoplanin, and
failed to be captured with an anti-podoplanin antibody. The
‘universal’ chip can capture such tumor cells by attaching other
antibodies against specific antigens such as mesothelin (14) and CD146 (15), which will be examined in future
studies. In addition, the ‘universal’ chip may be useful for
capturing a variety of tumor cells which originate from the
epithelium but do not express EpCAM due to various reasons such as
they may be undergoing EMT, and this topic will also be examined in
a future study.
We examined the capture efficiency of the
‘universal’ chip for tumor cells spiked in the blood to simulate
isolation of CTCs from the blood. PC-9 cells, spiked in the blood,
were effectively captured using the EpCAM-chip with an average
capture efficiency of 88.0%. However, ACC-MESO-4 cells could be
captured using the podoplanin-chip, but the efficacy was only
modest with an average capture efficiency of 38.4% (Table II and Fig. 7). These results indicate that some
components included in the blood may weaken or inhibit
antigen-antibody reaction, resulting in decreased capture
efficiency documented when ACC-MESO-4 cells were spiked in the
blood. In capturing PC-9 cells with the EpCAM-chip, the
antigen-antibody reaction may be stronger, and may be strong enough
for efficient capturing of tumor cells even if it is decreased in
the blood. Considering its clinical application, the capture
efficiency of the ‘universal’ chip in capturing tumor cells
contaminated in the blood should be increased, even when the chip
is coated with any capture antibody such as the anti-podoplanin
antibody. In addition, the sensitivity in detecting CTCs from the
blood sampled from cancer patients should be examined and may be
compared with that using the CellSearch system.
For monitoring cancer genetics in the blood (‘liquid
biopsy’), cell-free methods detecting fragments of DNA derived from
tumor cells may provide several advantages such as superior
sensitivity, as compared with cell-based methods detecting CTCs.
However, morphological visualization of tumor cells circulating in
the blood can be achieved only by direct detection of CTCs using
cell-based methods such as CellSearch and CTC-chips. More
importantly, molecular characterization of tumor cells can be
achieved at not only the genomic level (e.g. genomic alterations in
tumor cells) but also the cellular level (e.g. expression of
tumor-specific antigens on tumor cells) (16). In a future study, we will analyze
the expression of tumor-specific antigens such as HER2, especially
in correlation with the therapeutic effects of targeting agents,
which may provide new insights into personalized medicine.
In conclusion, using the novel CTC-chip, we
successfully captured EpCAM-positive tumor cells (PC-9) when the
chip was coated with an anti-EpCAM antibody, and also captured
EpCAM-negative tumor cells (ACC-MESO-4) when the chip was coated
with an antibody against an MPM-specific antigen (podoplanin). The
‘universal’ CTC-chip may provide new insights for the detection of
CTCs and personalized medicine.
Acknowledgements
We would like to thank Eri Kawashima for the
valuable technical assistance. This research was supported in part
by the UOEH Research Grant for Promotion of Occupational Health, by
the Fukuoka Medical Research Award granted by the Medical Care
Education Research Foundation, by a grant from the Takeda Science
Foundation, and by Grants-in-Aid for Scientific Research from the
Ministry of Education, Culture, Sports, Science and Technology
(MEXT), Japan.
References
|
1
|
Toss A, Mu Z, Fernandez S and
Cristofanilli M: CTC enumeration and characterization: Moving
toward personalized medicine. Ann Transl Med. 2:1082014.PubMed/NCBI
|
|
2
|
Allard WJ, Matera J, Miller MC, Repollet
M, Connelly MC, Rao C, Tibbe AG, Uhr JW and Terstappen LW: Tumor
cells circulate in the peripheral blood of all major carcinomas but
not in healthy subjects or patients with nonmalignant diseases.
Clin Cancer Res. 10:6897–6904. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cristofanilli M, Budd GT, Ellis MJ,
Stopeck A, Matera J, Miller MC, Reuben JM, Doyle GV, Allard WJ,
Terstappen LW, et al: Circulating tumor cells, disease progression,
and survival in metastatic breast cancer. N Engl J Med.
351:781–791. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cohen SJ, Punt CJ, Iannotti N, Saidman BH,
Sabbath KD, Gabrail NY, Picus J, Morse M, Mitchell E, Miller MC, et
al: Relationship of circulating tumor cells to tumor response,
progression-free survival, and overall survival in patients with
metastatic colorectal cancer. J Clin Oncol. 26:3213–3221. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
de Bono JS, Scher HI, Montgomery RB,
Parker C, Miller MC, Tissing H, Doyle GV, Terstappen LW, Pienta KJ
and Raghavan D: Circulating tumor cells predict survival benefit
from treatment in metastatic castration-resistant prostate cancer.
Clin Cancer Res. 14:6302–6309. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tanaka F, Yoneda K, Kondo N, Hashimoto M,
Takuwa T, Matsumoto S, Okumura Y, Rahman S, Tsubota N, Tsujimura T,
et al: Circulating tumor cell as a diagnostic marker in primary
lung cancer. Clin Cancer Res. 15:6980–6986. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tsiouris A and Walesby RK: Malignant
pleural mesothelioma: Current concepts in treatment. Nat Clin Pract
Oncol. 4:344–352. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yoneda K, Tanaka F, Kondo N, Hashimoto M,
Takuwa T, Matsumoto S, Okumura Y, Tsubota N, Sato A, Tsujimura T,
et al: Circulating tumor cells (CTCs) in malignant pleural
mesothelioma (MPM). Ann Surg Oncol. 21:(Suppl 4). 472–480. 2014.
View Article : Google Scholar
|
|
9
|
Joosse SA, Gorges TM and Pantel K:
Biology, detection, and clinical implications of circulating tumor
cells. EMBO Mol Med. 7:1–11. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nagrath S, Sequist LV, Maheswaran S, Bell
DW, Irimia D, Ulkus L, Smith MR, Kwak EL, Digumarthy S, Muzikansky
A, et al: Isolation of rare circulating tumour cells in cancer
patients by microchip technology. Nature. 450:1235–1239. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Maheswaran S, Sequist LV, Nagrath S, Ulkus
L, Brannigan B, Collura CV, Inserra E, Diederichs S, Iafrate AJ,
Bell DW, et al: Detection of mutations in EGFR in circulating
lung-cancer cells. N Engl J Med. 359:366–377. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ohnaga T, Shimada Y, Moriyama M, Kishi H,
Obata T, Takata K, Okumura T, Nagata T, Muraguchi A and Tsukada K:
Polymeric microfluidic devices exhibiting sufficient capture of
cancer cell line for isolation of circulating tumor cells. Biomed
Microdevices. 15:611–616. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Usami N, Fukui T, Kondo M, Taniguchi T,
Yokoyama T, Mori S, Yokoi K, Horio Y, Shimokata K, Sekido Y, et al:
Establishment and characterization of four malignant pleural
mesothelioma cell lines from Japanese patients. Cancer Sci.
97:387–394. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Husain AN, Colby TV, Ordóñez NG, Krausz T,
Borczuk A, Cagle PT, Chirieac LR, Churg A, Galateau-Salle F, Gibbs
AR, et al: Guidelines for pathologic diagnosis of malignant
mesothelioma: A consensus statement from the International
Mesothelioma Interest Group. Arch Pathol Lab Med. 133:1317–1331.
2009.PubMed/NCBI
|
|
15
|
Sato A, Torii I, Okamura Y, Yamamoto T,
Nishigami T, Kataoka TR, Song M, Hasegawa S, Nakano T, Kamei T, et
al: Immunocytochemistry of CD146 is useful to discriminate between
malignant pleural mesothelioma and reactive mesothelium. Mod
Pathol. 23:1458–1466. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ilie M, Hofman V, Long E, Bordone O, Selva
E, Washetine K, Marquette CH and Hofman P: Current challenges for
detection of circulating tumor cells and cell-free circulating
nucleic acids, and their characterization in non-small cell lung
carcinoma patients. What is the best blood substrate for
personalized medicine? Ann Transl Med. 2:1072014.PubMed/NCBI
|