Introduction
Skin melanomas are malignant neoplasms derived from
neuroectodermal melanocytes. Although they can develop on
pre-existing melanocytic nevi, in more than 50% of cases they arise
de novo (1). There are three
subtypes of melanoma: Cutaneous (the most common), mucosal and
ocular (in most cases choroidal), the latter being the most common
extracutaneous melanoma. Compared to other neoplasms, melanomas
have the highest rate growth. There are over 100,000 new cases
every year, with the highest incidences found in Australia and New
Zealand, high-income European countries (Switzerland, Norway,
Sweden) and in the US (1). In Poland,
the standardized incidence rate is of the order of 5/100,000, which
corresponds to approximately 3,100 cases per year (2). Skin melanoma accounts for approximately
2% of all cancers diagnosed in Polish men and women (3). The incidence of skin melanoma is greater
after the age of 20, with the highest incidence in both sexes
between 50 and 64 years of age. The risk of melanoma increases with
age, reaching its maximum in the eighth decade of life. Skin
melanoma causes about 1.4% of deaths due to cancer in men and 1.5%
in women. The standardized mortality rate in Poland reaches
2.3/100,000 men and 1.5/100,000 women (2). The relative 5-year survival rate for
stage IV melanoma in Poland is 5–10%, whereas in Western Europe and
the US this rate reach 28%, which is probably related to earlier
detection, and thus a less advanced stage at diagnosis (3–5). The
outcomes of cancer treatment in Poland are worse than in most
European countries. The largest differences in effectiveness of
treatment occur in the case of melanoma (Germany 93.1 vs. Poland
69.8) (3).
The most significant factors in an increased risk of
malignant melanoma include: Ultraviolet radiation, mechanical or
chemical irritation, low content of pigment in the skin, previous
melanoma and genetic predisposition, including familial atypical
multiple mole melanoma syndrome (1).
At the time of diagnosis, skin melanoma in approximately 80% of
patients is present in the form of a local lesion, while in
approximately 15% it is locally advanced and metastatic in 5%. The
location in the integument makes early identification of a lesion
possible, which is conducive to curing the tumor completely using
surgical methods (6).
Surgical treatment remains the main method of
melanoma treatment (7). It consists
in complete excision of the scar after an excisional biopsy
performed at the diagnostic stage (micro-staging I) with a
sufficiently large margin of healthy tissue, which depends on the
infiltration depth of the lesion. To date, no increase in survival
has been confirmed for margins of more than 2 mm around excised
lesions with an infiltration depth greater than 2 cm (8).
A sentinel node biopsy (micro-staging II) is
performed concurrently with the widening of the resection margins.
Sentinel lymph node biopsy (SLNB) should be considered in all
patients in stage IB or II due to the fact that the presence of
metastases in local lymph nodes is the most significant prognostic
factor in patients with cutaneous melanoma (7). Research has confirmed the importance of
SLNB in cancer staging and in the identification of patients with
lymph node metastases whose survival time may be extended by
selective lymphadenectomy (9,10). However, it has been shown that it only
affects relapse-free survival, not overall survival. In the case of
patients with no lymph node metastases, the overall survival rate
is approximately 90% (9). Routine
elective lymphadenectomy is not recommended (11).
Melanomas are typically highly radioresistant and
chemoresistant. Before the era of immunotherapy, inoperable lesions
were treated with chemotherapy based mainly on dacarbazine,
temozolomide or fotemustine. It has been shown that the immune
system and mechanisms play an important role in oncology and that
new principles of immunotherapy are also used for melanoma because
it is a form of cancer suitable for treament with immunotherapy
(12). Qualification for novel
therapies should be preceded by testing for the presence of certain
changes in cell metabolism or alterations of the genetic profile
which can be targeted during treatment. It is crucial for directing
patients to the appropriate targeted treatment or clinical trial.
In the case of melanoma, tumor tissues should be screened for
mutations of BRAF V600 to identify patients who may benefit from
treatment with BRAF or MEK inhibitors. If the results are negative,
further molecular testing can be carried out for NRAS or c-Kit
(11). The influence of programmed
death receptor-1 (PD-1) expression on treatment with anti-PD-L1 is
still debated and is not unambiguous (11). Unfortunately, responses to targeted
therapy are generally not complete or long-lasting as resistance
mechanisms develop upon continuous drug exposure. Combination of
different types of molecular-targeted therapy agents co-inhibiting
two or more targets in single or complementary pathways may improve
treatment efficacy (11). The most
common melanoma treatment is a combination of BRAF and MEK
inhibitors.
Immunotherapy
Cytokines
Interferon (IFN)-α is a cytokine produced primarily
by plasmacytoid dendritic cells as a result of stimulation of their
TLR7 and TLR9 receptors (Toll-like receptors) by cytokine
stimulation [interleukin (IL)-1, IL-2, tumor necrosis factor
(TNF)-α] and viral infection (13).
Binding of IFN-α to the receptor, JAK tyrosine kinase
(Janus-activated kinase) is activated, which results in an increase
in immune system responses, inhibition of cell proliferation and
stimulation of their differentiation (14). Recombinant IFN-α-2b (Intron A) was the
first agent shown to significantly improve survival in a phase III
randomized trial in which survival time was prolonged by about one
year in adjuvant therapy in patients treated with the drug in
comparison to the observed group (15). As early as 1995, IFN-α-2b has been
registered by the FDA (Food and Drug Administration) for adjuvant
treatment of melanoma in patients at high risk of relapse (15). Alfa-Peginterferon-2b, an interferon
derivative, was created by coupling with polyethylene glycol and
has been approved by the FDA for adjuvant therapy in 2011 on the
basis of a study showing prolongation of relapse-free survival
compared to non-treated patients (34.8 months vs. 25.5 months)
(16). Cytokines can act through an
increase in natural killer (NK) cell activity (17,18). Side
effects related to the ingestion of interferons usually include
flu-like symptoms.
IL-2 is a cytokine secreted primarily by T helper 1
(Th1) lymphocytes that recognise antigens (19). The IL-2 receptor couples to JAK
tyrosine kinases and activates the signal transducer and activator
of transcription 5 (STAT5) (16). It
is mainly responsible for the regulation of lymphocyte activity and
protection against autoimmunization (19). It was approved by the FDA in 1998 for
the treatment of stage IV patients. The median survival time in 8
different clinical trials was 11.4 months. If complete responses to
treatment were obtained, they were long; even up to 40 months
(20). A pooled analysis showed a
complete response to IL-2 administration to in-transit lesions in
50% of subjects and excellent tolerability of treatment in 78%
(21).
Anti-CTLA4 antibodies, (CD152)
Cytotoxic T-lymphocyte antigen 4 (CTLA-4) is a
receptor found on regulatory T lymphocytes and on activated
CD4+ and CD8+ T lymphocytes (22). There are two forms of the CTLA-4
receptor: flCTLA-4, which is anchored to the cell membrane, and
sCTLA-4, which is soluble in serum (23).
The ligands for this receptor are B7.1 (CD80) and
B7.2 (CD86) molecules present on antigen-presenting cells (APCs),
which are also ligands for the CD28 molecule (24). The binding of CD28 to CD86 or CD80
enhances the secretion of IL-2 and the proliferation of T
lymphocytes (24). CTLA-4 has a
higher affinity for ligands than CD28. Binding of the CTLA-4
receptor to a B7 ligand inhibits activation and proliferation as
well as depression of the effector functions of T lymphocytes, thus
constituting an element of negative feedback of the immune response
(25). This results in inhibition of
the immune system responses and encouragement of neoplastic
processes. The use of antibodies blocking the CTLA-4 receptor
prevents its binding to a ligand, thereby increasing the activation
of lymphocytes and the antitumor immune response.
Ipilimumab (trade name Yervoy) is a human IgG1k
monoclonal antibody targeting CTLA-4. It is the first drug shown to
prolong survival and periods of remission in metastatic melanoma.
In 2011, it was approved by the FDA for the treatment of
disseminated melanoma based on a phase III study (26), and in 2015 for adjuvant treatment
(27). The registration trial for
adjuvant treatment was a phase III trial where the remission period
in the drug group was approximately 26 months on average, compared
to 17 months in the placebo group (27). The use of ipilimumab is also
associated with prolonged survival (26–28). In a
single-arm phase II trial of pretreated metastatic malignant
melanoma, the median overall survival was about 10 months (28). Phase I trials have also shown a
response to ipilimumab administered with IL-2 to the tumor site
resulting in a reduction in the injected primary in 67% of subjects
and the local metastatic lesions in 89% (29). Its efficacy has been shown to be
higher for the dose of 10 mg/kg of body weight than for 3 mg/kg of
body weight (30).
Another drug in this group is tremelimumab (human
monoclonal antibody against CTLA-4). A phase III study on
disseminated melanoma did not show that it had any significant
advantage over chemotherapeutics (dacarbazine, temozolomide). The
median survival in patients receiving tremelimumab was 12.6 months,
compared to 10.7 months in patients receiving cytostatics (31). Tremelimumab has not been approved by
the FDA.
The use of CTLA-4 antibodies is associated with
significant adverse autoimmune effects such as dermatitis,
endophthalmitis, colitis and diarrhea (32).
Molecules blocking the PD-1 receptor
(programmed death receptor-1)
The PD-1 receptor of the CD28 family is found on
CD4+ and CD8+ T lymphocytes, B lymphocytes,
NK cells, monocytes and activated dendritic cells (33,34). Like
CTLA-4, it is responsible for inhibiting antitumor responses. It
has two ligands: Programmed death-ligand 1 (PD-L1) found in many
different tissues and the less widespread programmed death-ligand 2
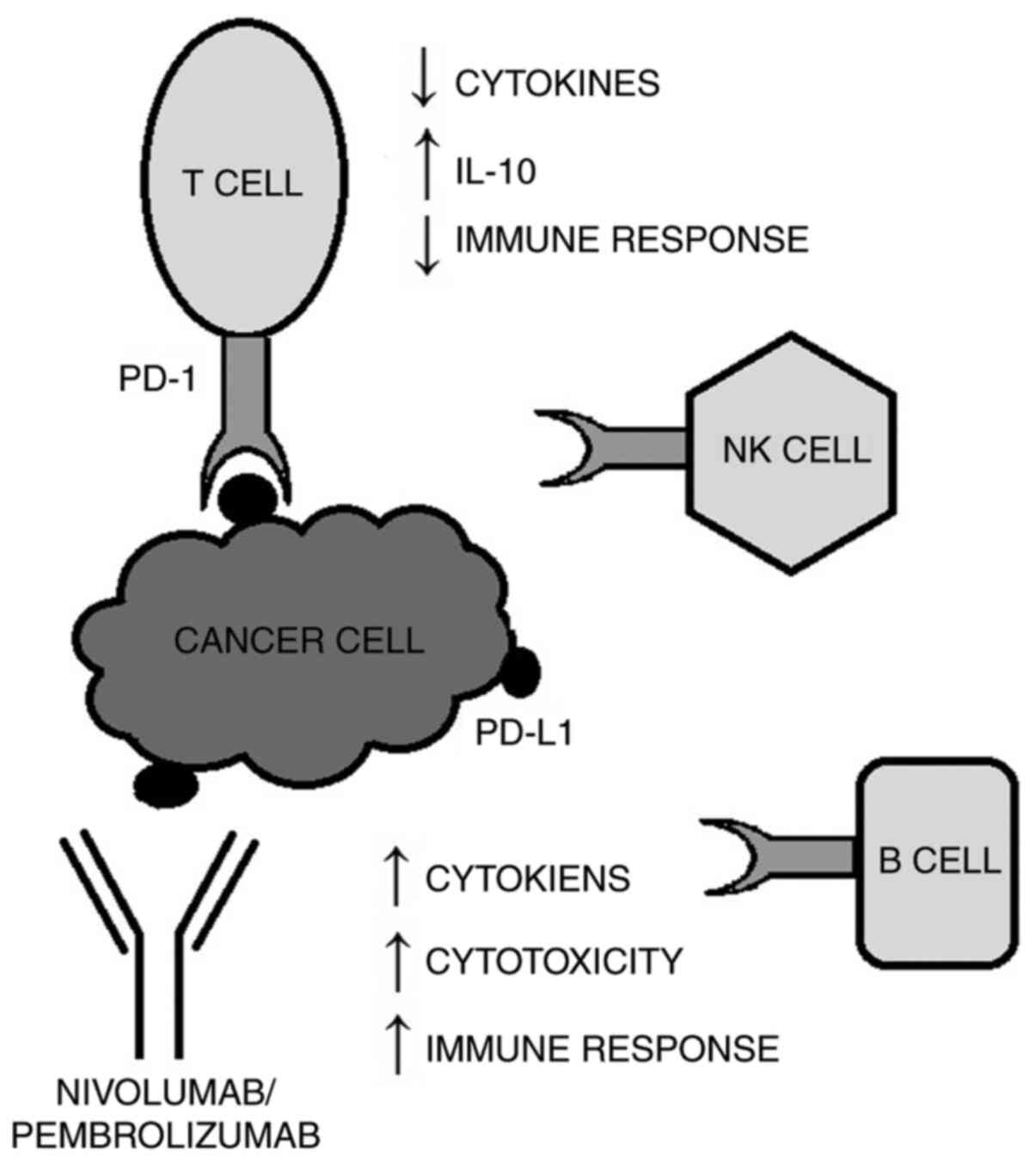
(PD-L2) present on specialized antigen-presenting cells (35). The combination of the PD-1 receptor
with either PD-L1 or PD-L2 results in suppression of the immune
system, for example by reducing the production of cytokines and
increasing the synthesis of IL-10 which inhibits the immune
response (36,37). Activation of the PD-1/PD-L1/PD-L2
pathway allows cancer cells to evade the immune system response
through negative regulation of effector T lymphocytes (Fig. 1). PD-L1 expression has been observed
in the case of lung, prostate and kidney cancer, as well as in
melanoma (38–40). The mechanism responsible for
modulation of PD-L1 expression by cancer cells has not yet been
identified. Currently, most drugs in this group block the PD-1
receptor.
Pembrolizumab is a humanized monoclonal IgG4
antibody targeting the PD-1 receptor and blocking its interaction
with PD-L1 and PD-L2 ligands. It has higher efficacy and better
tolerance in patients in advanced stages, compared to ipilimumab
[response rate (RR), 33 vs. 12%] (41). In 2014, it was approved by the FDA for
the treatment of metastatic melanoma based on a phase Ib trial
(42), becoming the first registered
PD-1 inhibitor. In subsequent years, its indications have been
extended to include the treatment of head, neck and lung cancer. In
2019 the FDA approved pembrolizumab for the adjuvant treatment of
patients with melanoma with involvement of lymph node(s) following
complete resection. The approval was based on a randomized,
double-blind, placebo-controlled, trial which demonstrated that
pembolizumab provided a clinically meaningful sustained improvement
in recurrence-free survival in resected high-risk stage III
melanoma (43).
Another drug in this group is nivolumab, a human
IgG4 antibody targeting the PD-1 receptor, which is used in the
treatment of kidney, liver and lung cancer. In 2014, the FDA
approved the use of nivolumab in patients with inoperable
metastatic melanoma with a mutation resulting in the substitution
of valine at position 600 with another amino acid in the BRAF
protein (V600) (44). In 2015, the
combination of nivolumab and ipilimumab was approved on the basis
of a phase II trial (45). In a
randomized phase III trial, the efficacy of adjuvant treatment of
patients in stages IIIB, IIIC and IV with nivolumab was shown to be
higher than with ipilimumab. It also results in a longer
progression-free survival (PFS) and less frequent occurrence of
severe side effects in comparison to ipilimumab. The trial involved
906 patients, half of whom received nivolumab at a dose of 3 mg/kg
of body weight every 2 weeks, while the others received ipilimumab
at a dose of 10 mg/kg of body weight every 3 weeks, then every 12
weeks, for about a year. The 12-month relapse-free survival rate
for nivolumab was 70.5%, and for ipilimumab it was 60.8% (46). This study became the basis for the FDA
approval of nivolumab for the adjuvant treatment of patients with
advanced melanoma in 2017 (47).
Research shows that antitumor effects may be induced
not only by blocking the PD-1 receptor, as blocking PD-L1 on
dendritic cells also leads to an increase in the activity and
function of effector lymphocytes and slowing tumor growth (48). In a phase I clinical trial on the
BMS-936559 antibody targeting PD-L1, a response was obtained in 9
out of 52 patients with advanced melanoma (49).
Because of the activation of the immune system, PD-1
and PD-L1 inhibitors can cause a specific set of inflammatory side
effects, known as immune-related adverse events (irAEs) (50). irAEs can occur in any organ system and
can be categorized into five ascending grades of symptoms:
Asymptomatic/mild (grade 1), moderate (grade 2), severe (grade 3),
life-threatening (grade 4), and death (grade 5) (51). Anti-PD-1 agent toxicities appear to be
dose-independent and the overall incidence of severe or
life-threatening irAEs (grade ≥ 3) ranges from 10 to 15% for
patients during this type of treatment (51). The organs with the highest reported
irAE incidences are skin, gastrointestinal tract, liver and lungs
(51). Although mild irAEs can
generally be treated supportively, severe toxicity may be fatal and
requires urgent intervention (51).
The most common irAEs are dermatological toxicities, which usually
appear around 3 to 6 weeks after therapy initiation (51).
Targeted treatment
RAS/RAF/MAPK pathway disorders and
drugs blocking its activity
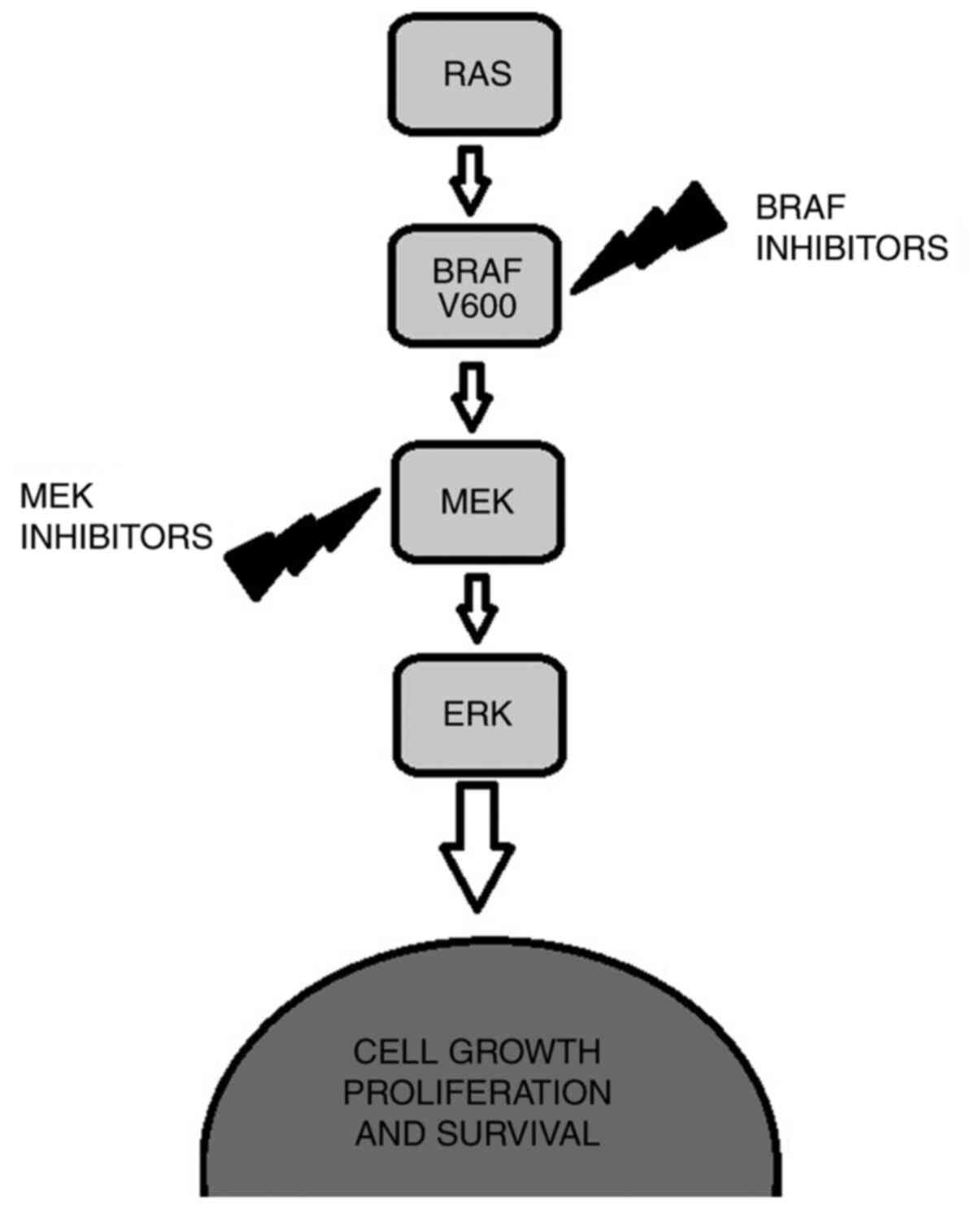
The RAS/RAF/MAPK (mitogen-activated protein kinase)
signaling pathway transmitting the signal from the cell surface to
the cell nucleus is responsible for the control of cell
proliferation, differentiation, migration and survival. After a
signal molecule attaches to the receptor in the cell membrane, the
RAS protein (product of the RAS proto-oncogene-rat sarcoma
viral oncogene homolog) is stimulated and becomes an active kinase
through phosphorylation, activating another protein of the pathway,
the RAF protein with serine/threonine kinase activity. The RAF
protein has 3 isoforms: ARAF, BRAF and CRAF, with BRAF being the
strongest activator of MEK kinase (mitogen/extracellular
signal-regulated kinase). The active BRAF kinase phosphorylates
MEK1 and MEK2 proteins that activate extracellular signal-regulated
kinase (ERK)1 and ERK2 proteins. The activated ERKs transmit the
signal to the cell nucleus, which induces the expression of genes
responsible for cell growth and survival (52,53). In
melanoma cells, hyperactivity of the RAS/RAF/MEK/ERK(MAPK) pathway
is observed. During the development of melanoma, its autocrine and
paracrine cells secrete growth factors, including transforming
growth factor (TGF)-β, IL-6 and IL-8, vascular endothelial growth
factor (VEGF), and platelet-derived growth factor subunit A(PDGF-A)
(54), which cause constitutive
activation of the RAS/RAF/MAPK pathway. The most frequent cause of
hyperactivity of this pathway is a BRAF kinase mutation, which is
observed in approximately 50% of advanced melanomas (55). The main point mutations are missense
mutations where valine (V) is substituted at position 600 with
glutamic acid (E) or lysine (K) (V600E, V600K). V600E mutations
(around 80%) occur most often in young people, whereas V600K
mutations (around 20%) in the elderly. Both mutations determine a
more aggressive course of advanced melanoma (56). Patients with BRAF mutations are more
likely to present with metastases to local lymph nodes (57) (Fig.
2).
BRAF inhibitors
Sorafenib is a broad-spectrum inhibitor. It inhibits
the activity of many RAF serine/threonine kinases (CRAF, BRAF,
V600E BRAF) and membrane receptor tyrosine kinases such as:
Mast/stem cell growth factor receptor (CD117), FMS-like tyrosine
kinase 3 (FLT3), vascular endothelial growth factor receptors
(VEGFRs), and platelet-derived growth factor receptors (PDGRs).
Despite FDA approval for the treatment of kidney, liver and thyroid
cancer, the results of studies concerning sorafenib in melanoma
treatment were unsatisfactory. It was found to have little or no
activity either in monotherapy (median PFS was 11 weeks) (58) or in combination with chemotherapy (the
RR for carboplatin+paclitaxel+sorafenib vs.
carboplatin+paclitaxel+placebo was 12% vs. 11%) (59).
Selective inhibitors include vemurafenib and
dabrafenib, which block BRAF activity. A phase III clinical trial
on a group of 675 previously untreated patients with disseminated
melanoma with a BRAF V600E mutation showed a 74% reduction in risk
of progression and a 63% reduction in risk of death in the
vemurafenib group, compared to the dacarbazine group. The RR was
48% for vemurafenib and only 5% for dacarbazine (60). Based on the results of this study,
vemurafenib became the first molecular-targeted drug registered in
the European Union and the US for the treatment of patients with
advanced disseminated melanoma and a confirmed BRAF V600 mutation
(61). Dabrafenib had equally
positive results. In a phase III trial, the median PFS was
approximately 5 months, compared to about 2 months for dacarbazine,
with a worse response in patients with a V600K mutation, compared
to a V600E mutation (62). This study
became the basis for the approval of dabrafenib by the FDA in
2013.
Oral administration of both vemurafenib and
dabrafenib has been associated with adverse effects. In the case of
the first drug, they included joint pain, rash, nausea and
diarrhea, hypersensitivity to ultraviolet (UV) radiation, hair loss
and proliferation of keratinocytes (in about 20% of subjects); in
the case of the second drug, adverse effects consisted of fever,
skin lesions, headaches and joint pain. Their occurrence entailed
the need to reduce the doses in both cases by approximately 30%
(60,62,63).
MEK inhibitors (mitogen-activated
protein kinase kinase, MAP2K)
One of the drugs in this group is binimetinib. It
was shown to have greater benefits in the treatment of metastatic
melanoma, compared to dacarbazine (increase in PFS: 2.8 months vs.
1.5 months) (64). Another drug in
this group is selumetinib, an inhibitor of MEK1 and MEK2. In a
phase II study concerning selumetinib, there was no significant
difference found in PFS compared to treatment with temozolomide (78
days vs. 80 days) (65). Similar
results were obtained in phase II studies in which docetaxel was
administered either alone or in combination with selumetinib (PFS:
3.9 months vs. 4.2 months) (66). The
FDA has not approved treatment of disseminated melanoma with either
binimetinib in monotherapy or selumetinib. The activity of
trametinib, a selective inhibitor of MEK1 and MEK2, has been
confirmed both in patients with a BRAF mutation and without it
(wild-type BRAF). In a phase III study, in which patients with a
V600 mutation were randomly assigned to either chemotherapy or
trametinib group, it was shown that treatment with the inhibitor
prolongs median PFS by just over 3 months, compared to monotherapy
with a chemotherapeutic agent. After 6 months of treatment, a
higher survival rate was found in the trametinib group, compared to
the group treated with chemotherapy (81 and 67%, respectively).
Based on this study, the drug was approved by the FDA in 2013 for
the treatment of melanoma, becoming the first commercially
available MEK inhibitor. The most serious adverse effects observed
during the study were reduction of the heart's ejection fraction
and impaired vision, whereas the most common ones were diarrhea,
rash and limb edema (67).
Cobimetinib is another selective MEK inhibitor. It
was registered by the FDA in 2015 for the treatment of metastatic
melanoma with a BRAF V600E or V600K mutation in combination with
vemurafenib. In a phase III registration trial, the group receiving
cobimetinib in combination with vemurafenib showed an increase in
PFS, compared to the vemurafenib group (9.9 months vs. 6.2 months)
(68).
Combination of BRAF and MEK
inhibitors
Due to the resistance that develops during treatment
with BRAF inhibitors, combination therapies with MEK inhibitors
have been attempted. A phase III study concerning a
dabrafenib/trametinib combination administered to previously
untreated patients with metastatic melanoma showed higher median
PFS for combination therapy than for dabrafenib monotherapy (9.3
months vs. 8.8 months), with RR of 67 and 51%, respectively
(69). In another study, in which
patients received either dabrafenib with trametinib or only
vemurafenib, the median PFS was 11.4 and 7.3 months, respectively,
with RR of 64% vs. 51% (70). Studies
involving patients with a good initial response to the BRAF
inhibitor and a subsequent worsening of the treatment results found
that combination therapy with these drugs had low efficacy
(71,72). In patients treated with a combination
of the two drugs, systemic adverse effects were more frequently
observed, whereas patients treated with dabrafenib monotherapy were
more likely to develop hyperkeratosis (72). In 2018, the FDA granted regular
approval to dabrafenib and trametinib in combination for the
adjuvant treatment of patients with melanoma with BRAF mutations
and involvement of lymph nodes following complete resection. The
approval was based on an international, multi-center, randomized,
double-blind, placebo-controlled trial in 870 patients with stage
III melanoma with BRAF V600E or V600K mutations, and pathologic
involvement of regional lymph nodes. Patients who received the
combination treatment had a statistically significant improvement
in RFS (relapse-free survival) compared with those receiving
placebo (73).
Recent studies have investigated new combinations of
BRAF and MEK inhibitors. The latest published study results concern
encorafenib (a BRAF kinase inhibitor) which has been shown to be
more effective than vemurafenib for the treatment of metastatic
patients, and its combination with binimetinib (a MEK inhibitor)
has an even more beneficial effect on RR (median PFS for drug
combination vs. encorafenib monotherapy vs. vemurafenib monotherapy
is 14.9 months vs. 9.6 months vs. 7.3 months, respectively)
(74). Consequently, the FDA issued a
decision in June 2018 to approve the combination of encorafenib and
binimetinib for treatment of metastatic melanoma with a BRAF V600E
or V600K mutation.
Farnesyltransferase inhibitors
Farnesyltransferase is a cytosolic enzyme
responsible for the transfer of the farnesyl group of farnesyl
diphosphate to the CAAX motif (C, cysteine; A, aliphatic residue;
X, any amino acid) of the RAS protein, which facilitates its
attachment to the internal membrane of a plasma cell and allows
initiation of transmission (75). The
inhibition of this process is a method of blocking RAS
activity.
The only farnesyltransferase inhibitor investigated
to date is tipifarnib, which is characterized by significant
toxicity. Moreover, its antitumor activity has not yet been
confirmed (76).
Genetic disorders of the PI3K/AKT/mTOR
pathway
The phosphatidylinositol 3-kinase/serine/threonine
kinase/mammalian target of rapamycin (PI3K/AKT/mTOR) pathway is an
intracellular signalling pathway that can be activated in a variety
of ways, including growth factors: Epidermal growth factor receptor
(EGFR) or insulin-like growth factor-1 receptor (IGF-1R).
Activation of phosphatidylinositol 3-kinase (PI3K kinase) leads to
increased production of phosphatidylinositol (3–5)-trisphosphate (PIP3), which in turn leads
to increased recruitment of serine/threonine kinase-protein kinase
B (AKT/PKB) to the cell membrane and its activation (77). The AKT kinase family includes 3
proteins: AKT-1, AKT-2, AKT-3 (72).
Active AKT kinase regulates the activity of the Bcl-2-associated
death promoter (BAD) protein, the nuclear factor
κ-light-chain-enhancer of activated B cells (NF-κB) protein and the
serine/threonine kinase mammalian target of rapamycin (mTOR), thus
regulating the processes of apoptosis, angiogenesis and
proliferation. This pathway is controlled by the phosphatase and
tensin homolog (PTEN) phosphatase, whose mutation or expression
disorders are quite often found in melanomas. Activation of this
pathway in cancer cells results in a decrease in apoptosis and an
increase in proliferation (77).
Inhibitors of the PI3K/AKT/mTOR
pathway
One of the first drugs in this group subjected to
trials was perifosine (an inhibitor of AKT and PI3K). In phase II
trials, it was characterized by good tolerance of treatment, but no
objective response was observed in 14 subjects, and 11 of them
showed disease progression (78). In
a phase II trial of another drug, temsirolimus (an inhibitor of
mTOR kinase), which was successfully used to treat kidney cancer,
only 1 out of 33 patients responded to the treatment, with a
partial remission lasting 2 months (79). Phase II trials concerning everolimus
(an mTOR kinase inhibitor), which also belongs to this group, did
not find sufficient activity of this drug or any significant impact
on PFS either (2 months on average) (80).
c-Kit inhibitors (CD117-receptor
tyrosine kinase)
The c-KIT receptor is a surface receptor with
tyrosine kinase activity. It is activated by binding a ligand,
which is a stem cell growth factor (SCF). Activation of the c-KIT
receptor by SCF leads to the activation of cell signaling that
regulates the processes of cell migration, survival, proliferation
and differentiation (81,82). The ultimate effect is uncontrolled
growth and proliferation of cancer cells, inhibition of apoptosis,
promotion of angiogenesis and metastasis (83). Tyrosine kinase inhibitors bind and
block the domain responsible for the binding of ATP
(adenosine-5′-triphosphate). This combination prevents activation
of the kinase and, consequently, a cascade of proteins transmitting
a proliferative signal to the cell nucleus. Most of the inhibitors
are non-specific and have affinity for several tyrosine kinases
(84). It is currently believed that
c-KIT mutations in melanoma are rare and occur only in some of its
subtypes.
Imatinib is an antibody that acts by, for example,
competitively blocking the kinase activity resulting from the
fusion of the BCR gene (breakpoint cluster region) and the ABL gene
(ABL1-Abelson murine leukaemia viral oncogene homolog 1). It is
also an inhibitor of receptor tyrosine kinases of platelet-derived
growth factor (PDGF) and SCF. In two independent phase II clinical
trials conducted on patients with metastatic melanoma, the efficacy
of treatment with imatinib was found to be low. In the 2008 study,
the median time to progression was 1.4 months and the median total
survival time was 7.5 months (85).
The median PFS in the 2011 study was 3.5 months (86). Another drug in this group was
nilotinib, whose mechanism of action is similar to imatinib. In a
phase II study, its activity was comparable to imatinib, with the
objective response rate at 26.2% and a slightly higher activity in
subjects with a mutation in exon 11. The median PFS was 4.2 months,
and the total survival time was 18 months (87). Dasatinib, another drug in this group,
inhibits the activity of c-KIT and BCR-ABL kinases as well as the
SRC family of kinases. However, no significant activity of this
drug was demonstrated in a phase II study. The median PFS was 8
weeks, but the toxicity of treatment was significant and a
reduction in the doses was required (88).
TRK inhibitors
The tropomyosin receptor kinase (TRK) is a family of
three transmembrane receptor tyrosine kinases (TRKA, TRKB, TRKC)
which are encoded respectively by neurotrophic receptor tyrosine
kinase 1 (NTRK1), NTRK2, NTRK3 genes and have a role in the
development and normal functioning of the nervous system (89). The TRK receptors are activated by four
different neurotrophins (89). Nerve
growth factor (NGF) has affinity for TRKA (84), brain-derived neurotrophic factor
(BDNF) and neurotrophin 4 (NT-4) bind to TRKB and neurotrophin 3
(NT-3) has affinity for TRKC (89).
Phosphorylation is required for activation of the TRK receptor and
is preceded by neurotrophin binding to TRK receptors at the cell
surface which causes the formation of receptor dimmers. The binding
of TRKA by NGF causes activation of the RAS/MAPK pathway which
results in increased cellular proliferation and growth via ERK
signaling (90). Activation of TRKB
leads to activation of the RAS-ERK, PI3K and PLCγ pathway,
resulting in neuronal differentiation and survival (90). Activation of TRKC leads to activation
of the PI3K/AKT pathway, preventing apoptosis and increasing cell
survival (90). Fusions involving the
NTRK gene family (NTRK1, NTRK2, and NTRK3) lead to
the expression of chimeric rearrangements in TRKA, TRKB, and TRKC,
respectively, with constitutively active kinase function, promoting
cell proliferation and survival (91). In the NTRK gene fusion the 3′
region of the NTRK gene is joined with the 5′ end of a
fusion partner gene (91).
NTRK gene fusions have been estimated to occur predominantly
in less than 1% of all solid tumors and less than 5% of all
melanomas (92). To date, there are
two TRK inhibitors approved for treatment of NTRK
fusion-positive melanoma.
Larotrectinib is a potent and highly selective
small-molecule inhibitor of all three TRK proteins (93). In 2018, larotrectinib was approved by
the FDA for the treatment of adult and pediatric patients with
solid tumors that harbor a NTRK gene fusion. The FDA based
its approval on 3 clinical trials that included 55 adults and
children with several different cancer types, 4 of whom had
melanoma (94). The overall RR was
75% with uncommon clinically significant adverse events (94).
Entrectinib is a potent oral inhibitor of the
tyrosine kinases TRKA/B/C, as well as ROS proto-oncogene 1 (ROS1)
and anaplastic lymphoma kinase (ALK) (94). The robust antitumor activity of
entrectinib has been demonstrated in three phase 1 and 2 trials
(ALKA-372-001, STARTRK-1 and STARTRK-2). Fast and durable response
for treatment was observed across a broad range of solid tumors,
including melanoma (94). What is
more, entrectinib showed promising antitumor activity in the
central nervous system which is particularly important in melanomas
regarding their proclivity for central nervous system metastasis
(94). This study became the basis
for FDA approval in 2019 of entrectinib for adults and adolescents
with tumors that test positive for NTRK gene changes.
Inhibitors of the heat shock protein
Hsp90
Heat shock proteins are a group of proteins whose
expression increases when cells are exposed to stress factors. They
supervise the processes of creating and protecting the spatial
structure of all proteins. Based on their molecular weight, they
are divided into five main groups: Low-molecular-weight Hsps,
Hsp60s, Hsp70s, Hsp90s and Hsp100s (95). Hsp90s are the most well studied HSPs
in cancer as they play important roles in carcinogenesis. They can
form protein complexes protecting RAF and AKT, proteins involved in
tumor growth (95). When combined
with immunotherapy, blocking Hsp90 proteins may be a promising part
of the therapeutic strategy due to the enhanced effect of T-cell
lymphocytes killing cancer cells, potentiation of therapy targeting
checkpoints and enhancement of the functions of cytotoxic
lymphocytes when combined with anti-CTLA4 antibodies (96). Hsp inhibitors are intended to inhibit
the induction of myeloid-derived suppressor cells. These cells are
activated by melanoma cells and are responsible for the suppression
of immunity, thus increasing the risk of metastasis (97). Clinical trials confirmed the activity
of XL888 in combination with vemurafenib in patients with a V600
mutation. The possibility of XL888 reducing the resistance
developed during treatment with BRAF inhibitors was also indicated
(98).
Proteasome inhibitors
Proteasomes are multi-enzymatic complexes involved
in the degradation of abnormal proteins. Inhibition of proteasomes
causes an accumulation of pathological proteins, activation of
caspases and cell death. In the course of cancer, cancer cells
become genetically unstable and synthesize abnormal proteins.
Blocking the breakdown of such proteins by inhibiting proteasomes
causes their accumulation within the cell, resulting in its death
through the activation of caspases. Therefore, compounds that
inhibit proteasomal activity are currently used in cancer therapy
(99).
Bortezomib is used to treat multiple myeloma.
However, a phase II trial did not confirm its efficacy in the
treatment of disseminated melanoma (100). Despite promising results of
preclinical studies, phase I clinical trials did not show any
significant activity for the combination of bortezomib and
temozolomide (100,101) or for the combination of bortezomib
and sorafenib (102).
Other treatment options
Imiquimod, an immune response modulator, can be used
in the treatment of inoperable superficial skin lesions by
administering it locally to the lesion surface (103). The mechanism of action of imiquimod
is to stimulate macrophages and monocytes to produce interferon-α
and cytokines (studies have shown its efficacy in reducing
cutaneous metastases from the primary) (103). Talimogene laherparepvec is an
attenuated herpes simplex virus type-1 (HSV-1) lacking the ICP34.5
and ICP47 genes with an inserted coding sequence for the human
granulocyte-macrophage colony-stimulating factor (GM-CSF), which is
administered to a neoplastic lesion and captured by HSV-1 receptors
on cancer cells and normal cells (104–106).
After administration, the virus replicates only in cancer cells.
The presence of GM-CSF is intended to additionally stimulate a
systemic antitumor immune response and effector T-cell response
(104–106). In a phase III study, the drug was
compared to subcutaneously administered GM-CSF in patients with
stage IIIB, IIIC and IV melanoma who were not eligible for surgery
(106). The percentage of permanent
response was 16.3% in the drug group and 2.1% in the GM-CSF group.
The reduction of untreated metastatic lesions by 50% was observed
in 27 out of 79 patients (34.2%) with lesions located outside
abdominal organs, and in 8 out of 71 patients (11.3%) with lesions
in abdominal organs. The drug was registered in the European Union
and in the US for the treatment of adult patients with unresectable
melanomas with metastases to local lymph nodes or with distant
metastases not involving bones, brain, lungs or other internal
organs (stages IIIB/IIIC/IVM1a) (106).
There are also other substances that appear to be
promising, for instance: Modulators of Toll-like receptors (TLRs),
inhibitors of poly(ADP-ribose) polymerase(PARP), anti-angiogenic
agents, monoclonal antibodies against CD40 costimulatory molecules,
anti-integrin antibodies or antisense therapy, i.e. therapy
involving the use of short fragments of DNA or RNA to silence the
expression of disease-causing genes, although the studied compound
oblimersen did not show high efficacy (107).
Current recommendations for immunotherapy
and targeted therapy of melanoma
According to the 2020 guidelines of the National
Comprehensive Cancer Network (NCCN) (7), adjuvant treatment outside of a clinical
trial is not recommended for patients with stage I or II disease
(7).
Stage IIIA (sentinel node positive) is the lowest
risk group for which the NCCN Guidelines recommend considering
adjuvant treatment. Risk of toxicity is one of the major
considerations when deciding whether a patient with stage III
disease should receive adjuvant treatment. The recommended drugs
for adjuvant therapy in the case of disease with lymph node
metastases (stage III) are: Nivolumab, pembrolizumab, dabrafenib or
trametinib for patients with a BRAF V600 mutation (7). In stage III patients with satellite or
in-transit metastases who have undergone a complete excision to
clear margins, it is recommended to supplement systemic therapy
with an oncolytic virus, talimogene laherparepvec (T-VEC),
administered directly to the lesion (99,101). In
addition, in patients with unresectable disease, the
recommendations include Bacillus Calmette-Guérin (BCG) vaccines,
IFN and IL-2 (7). Imiquimod is
recommended for use on the surface of superficial lesions (7,103).
Nivolumab or pembolizumab are recommended for stage
IV patients with limited metastases after total resection. The
recommended first-line therapy in the case of disseminated or
unresectable disease are PD-1 inhibitors (pembrolizumab/nivolumab)
or a combination of nivolumab and ipilimumab. The recommended
targeted therapy (in the presence of a BRAF V600 mutation) is a
combination of dabrafenib+trametinib, vemurafenib+cobimetinib or
encorafenib and binimetinib (7).
Other recommended regimens include vemurafenib and cobimetinib in
combination with atezolizumab in BRAF V600 activating mutation
presence (7). Second-line therapy
includes pembrolizumab or nivolumab monotherapy or a
nivolumab+ipilimumab combination, targeted therapy with
dabrafenib+trametinib or vemurafenib+cobimetinib or
encorafenib+binimetinib, ipilimumab monotherapy, high doses of
IL-2, imatinib in the presence of a mutation activating c-KIT,
larotrectinib or entrectinib for NTRK gene fusion-positive
tumors and binimetinib for NRAS-mutated tumors that have progressed
after prior immune checkpoint inhibitor therapy (7).
Immunotherapy and targeted therapy of
melanoma in Poland
Since novel cancer therapies are still expensive,
they are intended only for a certain group of patients. In Poland,
immunotherapy and targeted therapy are available within the Drug
Reimbursement Programme of the Ministry of Health. These
therapeutic programmes define eligibility criteria for treatment,
programme exclusion criteria, dosing regimen, method of
administration, the list of diagnostic procedures performed at
screening for the programme and necessary for treatment
monitoring.
Combination of dabrafenib+trametinib or vemurafenib+
cobimetinib, or encorafenib+binimetinib can be applied in any line
of treatment in patients with advanced melanoma (unresectable stage
III or stage IV) (108). Another
treatment option for this group of patients, independent of the
BRAF mutation status, is anti-PD1 antibodies as monotherapy or in
combination with an anti-CTLA4 antibody (108). Nivolumab and pembrolizumab in
monotherapy or the combination nivolumab+ipilimumab are available
as first- or second-line treatment whereas ipilimumab in the second
line of treatment (108).
The recommended drug for adjuvant therapy in the
case of disease with distant metastases is nivolumab (108). Patients with lymph node metastases
can be treated with nivolumab or pemborlizumab. In the presence of
a BRAF V600 mutation, patients with stage IIIA, IIIB, IIIC or IIID
who have undergone total resection can be treated with a
combination of dabrafenib and trametinib (108).
Clinical trials in progress
Increased biological understanding and access to
innovative therapeutic substances have improved the treatment of
melanoma. Many clinical trials on different pathways are in
progress. They mainly assess the effectiveness of the combination
of drugs that are currently used in melanoma treatment but also aim
to compare new drugs to already approved and active agents. As most
of these trials are in phase II, we must remain patient for the
full results, and hopefully, for another breakthrough in the
treatment of melanoma. Table I
presents some of currently ongoing trials.
 | Table I.Some of the current ongoing trials
(109). |
Table I.
Some of the current ongoing trials
(109).
| Drug | Clinical trial | Phase |
|---|
| Cytokines | A study of NKTR-214
combined with nivolumab vs. nivolumab alone in participants with
previously untreated inoperable or metastatic melanoma | III |
| BRAF
inhibitors |
Encorafenib+binimetinib+pembrolizumab in
patients with unresectable or metastatic BRAF V600 mutant melanoma
(Germany) | I |
|
|
Dabrafenib/trametinib/hydroxochloroquine
for advanced pretreated BRAF V600 mutant melanoma (Belgium) | I |
|
| A study to evaluate
RAF265, an oral drug administered to subjects with locally advanced
or metastatic melanoma (USA) | II |
|
| Induction therapy
with vemurafenib and cobimetinib to optimize nivolumab and
ipilimumab therapy (Netherlands) | II |
| MEK inhibitors | BGB324 in
combination with pembrolizumab or dabrafenib/trametinib in
metastatic melanoma (Norway) | I/II |
|
| Intermittent
selumetinib for uveal melanoma (USA) | I |
| Combination of BRAF
and MEK inhibitors | Study of
neo-adjuvant use of vemurafenib plus cobimetinib for BRAF mutant
melanoma with palpable lymph node metastases (Canada) | II |
|
| Neoadjuvant
vemurafenib+cobimetinib+atezolizumab in melanoma: NEO-VC
(France) | II |
|
| Neoadjuvant
dabrafenib+trametinib for AJCC stage IIIB-C BRAF V600 mutation
positive melanoma (Australia) | II |
|
| MCS110 with
BRAF/MEK inhibition in patients with melanoma (USA) | II |
|
| Study of
dabrafenib+trametinib in the adjuvant treatment of stage III BRAF
V600+melanoma after complete resection to evaluate the impact on
pyrexia related outcomes (USA) | III |
| Farnesyltransferase
inhibitors | Tipifarnib in
treating patients with metastatic malignant melanoma (USA) | II |
| KIT inhibitors | Efficacy and safety
of nintedanib combined with paclitaxel chemotherapy for patients
with BRAF wt metastatic melanoma (Germany) | II |
| TRK inhibitors | A study to test the
safety of the investigational drug selitrectinib in children and
adults that may treat cancer (USA) | I/II |
| Inhibitors of the
PI3K/AKT/mTOR pathway | Everolimus in
treating patients with stage IV melanoma (USA) | II |
|
| CCI-779
(temsilorimus) in treating patients with metastatic melanoma
(USA) | II |
| Proteasome
inhibitors | An expanded cohort
trial of bortezomib and sorafenib in advanced malignant melanoma
(USA) | I |
|
| Bortezomib,
paclitaxel, and carboplatin in treating patients with metastatic
melanoma (USA) | I |
| Anti-CTLA4
antibodies | A national phase IV
study with ipilimumab for patients with advanced malignant melanoma
(Norway) | IV |
|
| Immunogenicity and
biomarker analysis of neoadjuvant ipilimumab for melanoma
(USA) | 0 |
|
| Phase I clinical
trial of tremelimumab plus MEDI3617 in patients with unresectable
stage III or stage IV melanoma (USA) | I |
|
| Study of the
combination of IMCgp100 with durvalumab and/or tremelimumab in
cutaneous melanoma (USA) | Ib/II |
| Antibodies blocking
PD-1 and PD-L1 molecules | Efficiacy, safety
and tolerability of V937 administered intravenously or
intratumorally with pembrolizumab (MK-3475) vs. pembrolizumab alone
in participiants with advanced/metastatic melanoma (V937-011)
(USA) | II |
|
| Cabozatinib and
pembrolizumab for advanced metastatic melanoma (USA) | I/II |
|
| Nivolumab in
combination with talazoparib in melanoma and mutations in BRCA or
BRCA-ness genes (USA) | II |
|
| Ipilimumab and
nivolumab with or without hypofractionated radiotherapy in patients
with metastatic melanoma (USA) | II |
|
| Immunotherapy with
ipilimumab and nivolumab preceded or not by targeted therapy with
encorafenib and binimetinib (France, Belgium) | II |
| Antisense
therapy | Dacarbazine with or
without oblimersen (G3139) in treating patients with advanced
malignant melanoma (USA) | III |
| Other | Imiquimod and
pembrolizumab in treating patients with stage IIIB-IV melanoma | I |
Summary
Melanoma is characterized by high mortality,
especially at the metastatic stage. The best treatment results are
achieved with radical surgical resection of a limited lesion;
however, in the case of a disseminated process where surgery is of
limited use, systemic treatment is necessary. Treatment of
metastatic patients with conventional chemotherapy has not brought
the expected results in terms of extending their survival time or
improving their comfort. Therefore, there has emerged a need to
seek other solutions. Although immunotherapy of melanoma is still
in its infancy, many published studies indicate that it is already
highly promising. In most cases, the use of immunological treatment
or targeted therapy has had a positive impact on survival time and
relapse-free survival. However, these periods are still relatively
short, and most of the patients diagnosed with advanced melanoma
succumb to the disease soon after diagnosis. For this reason,
further research and improvement of treatment are needed. The main
focus should be placed on antibodies blocking PD-1 and PD-L1
molecules, anti-CTLA4 antibodies and therapy with BRAF and MEK
inhibitors, as they provide the greatest benefits and are already
included in the treatment guidelines. New drug combinations should
also be tested, as combined treatment often has a better effect and
a more favorable toxicity profile. However, the main emphasis
should still be placed on early detection before the cancer
metastasizes, since full recovery in such a situation is almost
never achieved. One of the possible reasons may be the generalized
immunosuppression usually observed in the advanced stages which is
related to the extensive production of cytokines (110).
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All information included in this review is
documented by relevant references.
Authors' contributions
PSS and LGS were involved in the conceptualization
of the study. PS and LGS were involved in project administration.
PSS, MC, MJ and LGS were involved in the investigative aspects of
the study. PSS, MC, MJ and LGS were involved in data validation.
All authors have read and agreed to the published version of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ali Z, Yousaf N and Larkin J: Melanoma
epidemiology, biology and prognosis. EJC Suppl. 201:81–91. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rutkowski P, Wysocki PJ,
Nasierowska-Guttmejer A, Jeziorski A, Wysocki WM, Kalinka-Warzocha
E, Świtaj T, Kozak K, Kamińska-Winciorek G, Wiśniewski P, et al:
Cutaneous melanomas. Oncol Clin Pract. 13:241–258. 2017.
|
|
3
|
Didkowska J, Wojciechowska U, Czaderny K,
Olasek P and Ciuba A: Cancer In Poland In 2017, Polish National
Cancer Registry. http://onkologia.org.pl/wp-content/uploads/Nowotwory_2017.pdfDecember.
2020
|
|
4
|
Svedman FC, Pillas D, Taylor A, Kaur M,
Linder R and Hansson J: Stage-specific survival and recurrence in
patients with cutaneous malignant melanoma in Europe-a systematic
review of the literature. Clin Epidemiol. 8:109–122. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Merrill RM and Bateman S: Conditional
melanoma cancer survival in the United States. Cancer (Basel).
8:202016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kimbrough CW, McMasters KM and Davis EG:
Principles of surgical treatment of malignant melanoma. Surg Clin
North Am. 94:973–988. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
NCCN Clinical Practice Guidelines in
Oncology, . Melanoma (version 4.2020). https://www.nccn.org/professionals/physician_gls/pdf/cutaneous_melanoma.pdfDecember.
2020
|
|
8
|
Utjés D, Malmstedt J, Teras J, Drzewiecki
K, Gullestad HP, Ingvar C, Eriksson H and Gillgren P: 2-cm versus
4-cm surgical excision margins for primary cutaneous melanoma
thicker than 2 mm: Long-term follow-up of a multicentre, randomised
trial. Lancet. 394:471–477. 2019. View Article : Google Scholar
|
|
9
|
Morton DL, Thompson JF, Cochran AJ,
Mozzillo N, Elashoff R, Essner R, Nieweg OE, Roses DF, Hoekstra HJ,
Karakousis CP, et al: Sentinel-node biopsy or nodal observation in
melanoma. N Engl J Med. 355:1307–1317. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Morton DL, Thompson JF, Essner R, Elashoff
R, Stern SL, Nieweg OE, Roses DF, Karakousis CP, Mozzillo N,
Reintgen D, et al: Validation of the accuracy of intraoperative
lymphatic mapping and sentinel lymphadenectomy for early-stage
melanoma: A multicenter trial. Multicenter selective
lymphadenectomy trial group. Ann Surg. 230:453–465. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dummer R, Hauschild A, Lindenblatt N,
Pentheroudakis G and Keilholz U; ESMO Guidelines Committee, :
Cutaneous melanoma: ESMO clinical practice guidelines for
diagnosis, treatment and follow-up. Ann Oncol. 26 (Suppl
5):v126–v132. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jurisic V: Multiomic analysis of cytokines
in immuno-oncology. Expert Rev Proteomics. 17:663–674. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Asselin-Paturel C, Brizard G, Chemin K,
Boonstra A, O'Garra A, Vicari A and Trinchieri G: Type I interferon
dependence of plasmacytoid dendritic cell activation and migration.
J Exp Med. 201:1157–1167. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nicola Raftery N and Stevenson NJ:
Advances in anti-viral immune defence: Revealing the importance of
the IFN JAK/STAT pathway. Cell Mol Life Sci. 74:2525–2535. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kirkwood JM, Strawderman MH, Ernstoff MS,
Smith TJ, Borden EC and Blum RH: Interferon alfa-2b adjuvant
therapy of high-risk resected cutaneous melanoma: The Eastern
cooperative oncology group trial EST 1684. J Clin Oncol. 14:7–17.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Herndon TM, Demko SG, Jiang X, He K,
Gootenberg JE, Cohen MH, Keegan P and Pazdur R: U.S. Food and drug
administration approval: Peginterferon-alfa-2b for the adjuvant
treatment of patients with melanoma. Oncologist. 17:1323–1328.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mirjačić Martinović KM, Vuletić AM, Lj
Babović N, Džodić RR, Konjević GM and Jurišić VB: Attenuated in
vitro effects of IFN-α, IL-2 and IL-12 on functional and receptor
characteristics of peripheral blood lymphocytes in metastatic
melanoma patients. Cytokine. 96:30–40. 2017. View Article : Google Scholar
|
|
18
|
Mirjačić Martinović KM, Babović NL, Džodić
RR, Jurišić VB, Ninković AZ and Konjević GM: Beneficial in-vitro
effects of interleukin-2, interleukin-12, and their combination on
functional and receptor characteristics of natural killer cells in
metastatic melanoma patients with normal serum lactate
dehydrogenase levels. Melanoma Res. 26:551–564. 2016. View Article : Google Scholar
|
|
19
|
Ross SH and Cantrell DA: Signaling and
function of interleukin-2 in T lymphocytes. Annu Rev Immunol.
36:411–433. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Atkins MB, Lotze MT, Dutcher JP, Fisher
RI, Weiss G, Margolin K, Abrams J, Sznol M, Parkinson D, Hawkins M,
et al: High-dose recombinant interleukin 2 therapy for patients
with metastatic melanoma: Analysis of 270 patients treated between
1985 and 1993. J Clin Oncol. 17:2105–2116. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Temple-Oberle CF, Byers BA, Hurdle V, Fyfe
A and McKinnon JG: Intra-lesional interleukin-2 therapy for in
transit melanoma. J Surg Oncol. 109:327–331. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Brunet JF, Denizot F, Luciani MF,
Roux-Dosseto M, Suzan M, Mattei MG and Golstein P: A new member of
the immunoglobulin superfamily-CTLA-4. Nature. 328:267–270. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Walker LS: Treg and CTLA-4: Two
intertwining pathways to immune tolerance. J Autoimmun. 45:49–57.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Khailaie S, Rowshanravan B, Robert PA,
Waters E, Halliday N, Badillo Herrera JD, Walker LSK, Sansom DM and
Meyer-Hermann M: Characterization of CTLA4 trafficking and
implications for its function. Biophys J. 115:1330–1343. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Korecka A, Duszota A and Korczak-Kowalska
G: The role of the CD28 molecule in immunological tolerance.
Postepy Hig Med Dosw (Online). 61:74–82. 2007.(In Polish).
PubMed/NCBI
|
|
26
|
Hodi FS, O'Day SJ, McDermott DF, Weber RW,
Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel
JC, et al: Improved survival with ipilimumab in patients with
metastatic melanoma. N Engl J Med. 363:711–723. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Eggermont AM, Chiarion-Sileni V, Grob JJ,
Dummer R, Wolchok JD, Schmidt H, Hamid O, Robert C, Ascierto PA,
Richards JM, et al: Adjuvant ipilimumab versus placebo after
complete resection of high-risk stage III melanoma (EORTC 18071): A
randomised, double-blind, phase 3 trial. Lancet Oncol. 16:522–530.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
O'Day SJ, Maio M, Chiarion-Sileni V,
Gajewski TF, Pehamberger H, Bondarenko IN, Queirolo P, Lundgren L,
Mikhailov S, Roman L, et al: Efficacy and safety of ipilimumab
monotherapy in patients with pretreated advanced melanoma: A
multicenter single-arm phase II study. Ann Oncol. 21:1712–1717.
2010. View Article : Google Scholar
|
|
29
|
Ray A, Williams MA, Meek SM, Bowen RC,
Grossmann KF, Andtbacka RH, Bowles TL, Hyngstrom JR, Leachman SA,
Grossman D, et al: A phase I study of intratumoral ipilimumab and
interleukin-2 in patients with advanced melanoma. Oncotarget.
7:64390–64399. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wolchok JD, Neyns B, Linette G, Negrier S,
Lutzky J, Thomas L, Waterfield W, Schadendorf D, Smylie M, Guthrie
T Jr, et al: Ipilimumab monotherapy in patients with pretreated
advanced melanoma: A randomised, double-blind, multicentre, phase
2, dose-ranging study. Lancet Oncol. 11:155–164. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ribas A, Kefford R, Marshall MA, Punt CJ,
Haanen JB, Marmol M, Garbe C, Gogas H, Schachter J, Linette G, et
al: Phase III randomized clinical trial comparing tremelimumab with
standard-of-care chemotherapy in patients with advanced melanoma. J
Clin Oncol. 31:616–622. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kähler KC, Hassel JC, Heinzerling L,
Loquai C, Mössner R, Ugurel S, Zimmer L and Gutzmer R; ‘Cutaneous
Side Effects’ Committee of the Work Group Dermatological Oncology
(ADO), : Management of side effects of immune checkpoint blockade
by anti-CTLA-4 and anti-PD-1 antibodies in metastatic melanoma. J
Dtsch Dermatol Ges. 14:662–681. 2016. View Article : Google Scholar
|
|
33
|
Ohaegbulam KC, Assal A, Lazar-Molnar E,
Yao Y and Zang X: Human cancer immunotherapy with antibodies to the
PD-1 and PD-L1 pathway. Trends Mol Med. 21:24–33. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Brown KE, Freeman GJ, Wherry EJ and Sharpe
AH: Role of PD-1 in regulating acute infections. Curr Opin Immunol.
22:397–401. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Yamazaki T, Akiba H, Iwai H, Matsuda H,
Aoki M, Tanno Y, Shin T, Tsuchiya H, Pardoll DM, Okumura K, et al:
Expression of programmed death 1 ligands by murine T cells and APC.
J Immunol. 169:5538–5545. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Keir ME, Butte MJ, Freeman GJ and Sharpe
AH: PD-1 and its ligands in tolerance and immunity. Annu Rev
Immunol. 26:677–704. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Dong H, Strome SE, Matteson EL, Moder KG,
Flies DB, Zhu G, Tamura H, Driscoll CL and Chen L: Costimulating
aberrant T cell responses by B7-H1 autoantibodies in rheumatoid
arthritis. J Clin Invest. 111:363–370. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Blank C, Gajewski TF and Mackensen A:
Interaction of PD-L1 on tumor cells with PD-1 on tumor-specific T
cells as a mechanism of immune evasion: Implications for tumor
immunotherapy. Cancer Immunol Immunother. 54:307–314. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Dong H, Strome SE, Salomao DR, Tamura H,
Hirano F, Flies DB, Roche PC, Lu J, Zhu G, Tamada K, et al:
Tumor-associated B7-H1 promotes T-cell apoptosis: A potential
mechanism of immune evasion. Nat Med. 8:793–800. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Zang X and Allison JP: The B7 family and
cancer therapy: Costimulation and coinhibition. Clin Cancer Res.
13:5271–5279. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Robert C, Schachter J, Long GV, Arance A,
Grob JJ, Mortier L, Daud A, Carlino MS, McNeil C, Lotem M, et al:
Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med.
372:2521–2532. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Raedler LA: Keytruda (Pembrolizumab):
First PD-1 inhibitor approved for previously treated unresectable
or metastatic melanoma. Am Health Drug Benefits. 8:96–100.
2015.PubMed/NCBI
|
|
43
|
Eggermont AM, Blank CU, Mandalà M, Long
GV, Atkinson V, Dalle S, Haydon AM, Meshcheryakov A, Khattak M,
Carlino MS, et al: Pembrolizumab versus placebo after complete
resection of high-risk stage III melanoma: New recurrence-free
survival results from the EORTC 1325-MG/Keynote 054 double-blinded
phase III trial at three-year median follow-up. J Clin Oncol. 38
(Suppl 15):S100002020. View Article : Google Scholar
|
|
44
|
Raedler LA: Opdivo (Nivolumab): Second
PD-1 inhibitor receives FDA approval for unresectable or metastatic
melanoma. Am Health Drug Benefits. 8:180–183. 2015.PubMed/NCBI
|
|
45
|
Postow MA, Chesney J, Pavlick AC, Robert
C, Grossmann K, McDermott D, Linette GP, Meyer N, Giguere JK,
Agarwala SS, et al: Nivolumab and ipilimumab versus ipilimumab in
untreated melanoma. N Engl J Med. 372:2006–2017. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Weber J, Mandala M, Del Vecchio M, Gogas
HJ, Arance AM, Cowey CL, Dalle S, Schenker M, Chiarion-Sileni V,
Marquez-Rodas I, et al: Adjuvant nivolumab versus ipilimumab in
resected stage III or IV melanoma. N Engl J Med. 377:1824–1835.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Beaver JA, Theoret MR, Mushti S, He K,
Libeg M, Goldberg K, Sridhara R, McKee AE, Keegan P and Pazdur R:
FDA approval of nivolumab for the first-line treatment of patients
with BRAFV600 wild-type unresectable or metastatic
melanoma. Clin Cancer Res. 23:3479–3483. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Brown JA, Dorfman DM, Ma FR, Sullivan EL,
Munoz O, Wood CR, Greenfield EA and Freeman GJ: Blockade of
programmed death-1 ligands on dendritic cells enhances T cell
activation and cytokine production. J Immunol. 170:1257–1266. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ,
Topalian SL, Hwu P, Drake CG, Camacho LH, Kauh J, Odunsi K, et al:
Safety and activity of anti-PD-L1 antibody in patients with
advanced cancer. N Engl J Med. 366:2455–2465. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Zubiri L, Allen IM, Taylor MS, Guidon AC,
Chen ST, Schoenfeld SR, Neilan TG, Sise ME, Mooradian MJ, Rubin KM,
et al: Immune-related adverse events in the setting of PD-1/L1
inhibitor combination therapy. Oncologist. 25:e398–e404. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Darnell EP, Mooradian MJ, Baruch EN,
Yilmaz M and Reynolds KL: Immune-related adverse events (irAEs):
Diagnosis, management, and clinical pearls. Curr Oncol Rep.
22:392020. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Rahman MA, Salajegheh A, Smith RA and Lam
AK: B-Raf mutation: A key player in molecular biology of cancer.
Exp Mol Pathol. 95:336–342. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Hall RD and Kudchadkar RR: BRAF mutations:
Signaling, epidemiology, and clinical experience in multiple
malignancies. Cancer Control. 21:221–230. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Elias EG, Hasskamp JH and Sharma BK:
Cytokines and growth factors expressed by human cutaneous melanoma.
Cancers (Basel). 2:794–808. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Cheng L, Lopez-Beltran A, Massari F,
MacLennan GR and Montironi R: Molecular testing for BRAF mutations
to inform melanoma treatment decisions: A move toward precision
medicine. Mod Pathol. 3:24–38. 2018. View Article : Google Scholar
|
|
56
|
Menzies AM, Haydu LE, Visintin L, Carlino
MS, Howle JR, Thompson JF, Kefford RF, Scolyer RA and Long GV:
Distinguishing clinicopathologic features of patients with V600E
and V600K BRAF-mutant metastatic melanoma. Clin Cancer Res.
18:3242–3249. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Viros A, Fridlyand J, Bauer J,
Lasithiotakis K, Garbe C, Pinkel D and Bastian BC: Improving
melanoma classification by integrating genetic and morphologic
features. PLoS Med. 5:e1202008. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Eisen T, Ahmad T, Flaherty KT, Gore M,
Kaye S, Marais R, Gibbens I, Hackett S, James M, Schuchter LM, et
al: Sorafenib in advanced melanoma: A phase II randomised
discontinuation trial analysis. Br J Cancer. 95:581–586. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Hauschild A, Agarwala SS, Trefzer U, Hogg
D, Robert C, Hersey P, Eggermont A, Grabbe S, Gonzalez R, Gille J,
et al: Results of a phase III, randomized, placebo-controlled study
of sorafenib in combination with carboplatin and paclitaxel as
second-line treatment in patients with unresectable stage III or
stage IV melanoma. J Clin Oncol. 27:2823–2830. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Chapman PB, Hauschild A, Robert C, Haanen
JB, Ascierto P, Larkin J, Dummer R, Garbe C, Testori A, Maio M, et
al: Improved survival with vemurafenib in melanoma with BRAF V600E
mutation. N Engl J Med. 364:2507–2516. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Bollag G, Tsai J, Zhang J, Zhang C,
Ibrahim P, Nolop K and Hirth P: Vemurafenib: The first drug
approved for BRAF-mutant cancer. Nat Rev Drug Discov. 11:873–886.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Hauschild A, Grob JJ, Demidov LV, Jouary
T, Gutzmer R, Millward M, Rutkowski P, Blank CU, Miller WH Jr,
Kaempgen E, et al: Dabrafenib in BRAF-mutated metastatic melanoma:
A multicentre, open-label, phase 3 randomised controlled trial.
Lancet. 380:358–365. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Rutkowski P and Blank C: Dabrafenib for
the treatment of BRAF V600-positive melanoma: A safety evaluation.
Expert Opin Drug Saf. 13:1249–1258. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Dummer R, Schadendorf D, Ascierto PA,
Arance A, Dutriaux C, Di Giacomo AM, Rutkowski P, Del Vecchio M,
Gutzmer R, Mandala M, et al: Binimetinib versus dacarbazine in
patients with advanced NRAS-mutant melanoma (NEMO): A multicentre,
open-label, randomised, phase 3 trial. Lancet Oncol. 18:435–445.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Kirkwood JM, Bastholt L, Robert C, Sosman
J, Larkin J, Hersey P, Middleton M, Cantarini M, Zazulina V,
Kemsley K and Dummer R: Phase II, open-label, randomized trial of
the MEK1/2 inhibitor selumetinib as monotherapy versus temozolomide
in patients with advanced melanoma. Clin Cancer Res. 18:555–567.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Gupta A, Love S, Schuh A, Shanyinde M,
Larkin JM, Plummer R, Nathan PD, Danson S, Ottensmeier CH, Lorigan
P, et al: DOC-MEK: A double-blind randomized phase II trial of
docetaxel with or without selumetinib in wild-type BRAF advanced
melanoma. Ann Oncol. 25:968–974. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Flaherty KT, Robert C, Hersey P, Nathan P,
Garbe C, Milhem M, Demidov LV, Hassel JC, Rutkowski P, Mohr P, et
al: Improved survival with MEK inhibition in BRAF-mutated melanoma.
N Engl J Med. 367:107–114. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Larkin J, Ascierto PA, Dréno B, Atkinson
V, Liszkay G, Maio M, Mandalà M, Demidov L, Stroyakovskiy D, Thomas
L, et al: Combined vemurafenib and cobimetinib in BRAF-mutated
melanoma. N Engl J Med. 371:1867–1876. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Long GV, Stroyakovskiy D, Gogas H,
Levchenko E, de Braud F, Larkin J, Garbe C, Jouary T, Hauschild A,
Grob JJ, et al: Combined BRAF and MEK inhibition versus BRAF
inhibition alone in melanoma. N Engl J Med. 371:1877–1888. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Robert C, Karaszewska B, Schachter J,
Rutkowski P, Mackiewicz A, Stroiakovski D, Lichinitser M, Dummer R,
Grange F, Mortier L, et al: Improved overall survival in melanoma
with combined dabrafenib and trametinib. N Engl J Med. 372:30–39.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Johnson DB, Flaherty KT, Weber JS, Infante
JR, Kim KB, Kefford RF, Hamid O, Schuchter L, Cebon J, Sharfman WH,
et al: Combined BRAF (dabrafenib) and MEK inhibition (trametinib)
in patients with BRAFV600-mutant melanoma experiencing progression
with single-agent BRAF inhibitor. J Clin Oncol. 32:3697–3704. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Long GV, Stroyakovskiy D, Gogas H,
Levchenko E, de Braud F, Larkin J, Garbe C, Jouary T, Hauschild A,
Grob JJ, et al: Dabrafenib and trametinib versus dabrafenib and
placebo for Val600 BRAF-mutant melanoma: A multicentre,
double-blind, phase 3 randomised controlled trial. Lancet.
386:444–451. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Dummer R, Brase JC, Garrett J, Campbell
CD, Gasal E, Squires M, Gusenleitner D, Santinami M, Atkinson V,
Mandalà M, et al: Adjuvant dabrafenib plus trametinib versus
placebo in patients with resected, BRAFV600-mutant,
stage III melanoma (COMBI-AD): Exploratory biomarker analyses from
a randomised, phase 3 trial. Lancet Oncol. 21:358–372. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Dummer R, Ascierto PA, Gogas HJ, Arance A,
Mandala M, Liszkay G, Garbe C, Schadendorf D, Krajsova I, Gutzmer
R, et al: Encorafenib plus binimetinib versus vemurafenib or
encorafenib in patients with BRAF-mutant melanoma (COLUMBUS): A
multicentre, open-label, randomised phase 3 trial. Lancet Oncol.
19:603–615. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Long SB, Casey PJ and Beese LS: Reaction
path of protein farnesyltransferase at atomic resolution. Nature.
419:645–650. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Gajewski TF, Salama AK, Niedzwiecki D,
Johnson J, Linette G, Bucher C, Blaskovich MA, Sebti SM, Haluska F;
Cancer and Leukemia Group B: Phase II study of the
farnesyltransferase inhibitor R115777 in advanced melanoma (CALGB
500104). J Transl Med. 10:2462012. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
LoPiccolo J, Blumenthal GM, Bernstein WB
and Dennis PA: Targeting the PI3K/Akt/mTOR pathway: Effective
combinations and clinical considerations. Drug Resist Updat.
11:32–50. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Ernst DS, Eisenhauer E, Wainman N, Davis
M, Lohmann R, Baetz T, Belanger K and Smylie M: Phase II study of
perifosine in previously untreated patients with metastatic
melanoma. Invest New Drugs. 23:569–575. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Margolin K, Longmate J, Baratta T, Synold
T, Christensen S, Weber J, Gajewski T, Quirt I and Doroshow JH:
CCI-779 in metastatic melanoma: A phase II trial of the california
cancer consortium. Cancer. 104:1045–1048. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Vera Aguilera J, Rao RD, Allred JB, Suman
VJ, Windschitl HE, Kaur JS, Maples WJ, Lowe VJ, Creagan ET,
Erickson LA and Markovic S: Phase II study of everolimus in
metastatic malignant melanoma (NCCTG-N0377, Alliance). Oncologist.
23:887–e94. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Wehrle-Haller B: The role of Kit-ligand in
melanocyte development and epidermal homeostasis. Pigment Cell Res.
16:287–296. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Lennartsson J and Rönnstrand L: Stem cell
factor receptor/c-Kit: From basic science to clinical implications.
Physiol Rev. 92:1619–1649. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Arora A and Scholar EM: Role of tyrosine
kinase inhibitors in cancer therapy. J Pharmacol Exp Ther.
315:971–979. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Broekman F, Giovannetti E and Peters GJ:
Tyrosine kinase inhibitors: Multi-targeted or single-targeted?
World J Clin Oncol. 2:80–93. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Kim KB, Eton O, Davis DW, Frazier ML,
McConkey DJ, Diwan AH, Papadopoulos NE, Bedikian AY, Camacho LH,
Ross MI, et al: Phase II trial of imatinib mesylate in patients
with metastatic melanoma. Br J Cancer. 99:734–740. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Guo J, Si L, Kong Y, Flaherty KT, Xu X,
Zhu Y, Corless CL, Li L, Li H, Sheng X, et al: Phase II,
open-label, single-arm trial of imatinib mesylate in patients with
metastatic melanoma harboring c-Kit mutation or amplification. J
Clin Oncol. 29:2904–2909. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Guo J, Carvajal RD, Dummer R, Hauschild A,
Daud A, Bastian BC, Markovic SN, Queirolo P, Arance A, Berking C,
et al: Efficacy and safety of nilotinib in patients with
KIT-mutated metastatic or inoperable melanoma: Final results from
the global, single-arm, phase II TEAM trial. Ann Oncol.
28:1380–1387. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Kluger HM, Dudek AZ, McCann C, Ritacco J,
Southard N, Jilaveanu LB, Molinaro A and Sznol M: A phase 2 trial
of dasatinib in advanced melanoma. Cancer. 117:2202–2208. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Amatu A, Sartore-Bianchi A, Bencardino K,
Pizzutilo EG, Tosi F and Siena S: Tropomyosin receptor kinase (TRK)
biology and the role of NTRK gene fusions in cancer. Ann Oncol. 30
(Suppl 8):viii5–viii15. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Amatu A, Sartore-Bianchi A and Siena S:
NTRK gene fusions as novel targets of cancer therapy across
multiple tumour types. ESMO Open. 1:e0000232016. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Vaishnavi A, Le AT and Doebele RC: TRKing
down an old oncogene in a new era of targeted therapy. Cancer
Discov. 5:25–34. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Cocco E, Scaltriti M and Drilon A: NTRK
fusion-positive cancers and TRK inhibitor therapy. Nat Rev Clin
Oncol. 15:731–747. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Drilon A, Laetsch TW, Kummar S, DuBois SG,
Lassen UN, Demetri GN, Nathenson M, Doebele RC, Farago AF, Pappo
AS, et al: Efficacy of larotrectinib in TRK fusion-positive cancers
in adults and children. N Engl J Med. 378:731–739. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Doebele RC, Drilon A, Paz-Ares L, Siena S,
Shaw AT, Farago AF, Blakely CM, Seto T, Cho BC, Tosi D, et al:
Entrectinib in patients with advanced or metastatic NTRK
fusion-positive solid tumours: Integrated analysis of three phase
1–2 trials. Lancet Oncol. 21:271–282. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Chatterjee S and Burns TF: Heat shock
proteins in cancer: A promising therapeutic approach. Int J Mol
Sci. 18:19782017. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Mbofung RM, McKenzie JA, Malu S, Zhang M,
Peng W, Liu C, Kuiatse I, Tieu T, Williams L, Devi S, et al: HSP90
inhibition enhances cancer immunotherapy by upregulating interferon
response genes. Nat Commun. 8:4512017. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Janssen N, Speigl L, Pawelec G, Niessner H
and Shipp C: Inhibiting HSP90 prevents the induction of
myeloid-derived suppressor cells by melanoma cells. Cell Immunol.
327:68–76. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Eroglu Z, Chen YA, Gibney GT, Weber JS,
Kudchadkar RR, Khushalani NI, Markowitz J, Brohl AS, Tetteh LF,
Ramadan H, et al: Combined BRAF and HSP90 inhibition in patients
with unresectable BRAF V600E-mutant melanoma. Clin
Cancer Res. 24:5516–5524. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Qureshi N, Vogel SN, Van Way C III,
Papasian CJ, Qureshi AA and Morrison DC: The proteasome: A central
regulator of inflammation and macrophage function. Immunol Res.
31:243–260. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Markovic SN, Geyer SM, Dawkins F, Sharfman
W, Albertini M, Maples W, Fracasso PM, Fitch T, Lorusso P, Adjei AA
and Erlichman C: A phase II study of bortezomib in the treatment of
metastatic malignant melanoma. Cancer. 103:2584–2589. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Su Y, Amiri KI, Horton LW, Yu Y, Ayers GD,
Koehler E, Kelley MC, Puzanov I, Richmond A and Sosman JA: A phase
I trial of bortezomib with temozolomide in patients with advanced
melanoma: Toxicities, antitumor effects, and modulation of
therapeutic targets. Clin Cancer Res. 16:348–357. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Sullivan RJ, Ibrahim N, Lawrence DP,
Aldridge J, Giobbie-Hurder A, Hodi FS, Flaherty KT, Conley C, Mier
JW, Atkins MB and McDermott DF: A phase I trial of bortezomib and
sorafenib in advanced malignant melanoma. Oncologist. 20:617–618.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Sisti A, Sisti G and Oranges CM: Topical
treatment of melanoma skin metastases with imiquimod: A review.
Dermatol Online J. 21:13030/qt8rj4k7r6. 2014.PubMed/NCBI
|
|
104
|
Liu BL, Robinson M, Han ZQ, Branston RH,
English C, Reay P, McGrath Y, Thomas SK, Thornton M, Bullock P, et
al: ICP34.5 deleted herpes simplex virus with enhanced oncolytic,
immune stimulating, and anti-tumour properties. Gene Ther.
10:292–303. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Chou J and Roizman B: The gamma 1(34.5)
gene of herpes simplex virus 1 precludes neuroblastoma cells from
triggering total shutoff of protein synthesis characteristic of
programed cell death in neuronal cells. Proc Natl Acad Sci USA.
89:3266–3270. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Andtbacka RH, Kaufman HL, Collichio F,
Amatruda T, Senzer N, Chesney J, Delman KA, Spitler LE, Puzanov I,
Agarwalaet SS, et al: Talimogene laherparepvec improves durable
response rate in patients with advanced melanoma. J Clin Oncol.
33:2780–2788. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Bedikian AY, Garbe C, Conry R, Lebbe C and
Grob JJ; Genasense Melanoma Study Group, : Dacarbazine with or
without oblimersen (a Bcl-2 antisense oligonucleotide) in
chemotherapy-naive patients with advanced melanoma and low-normal
serum lactate dehydrogenase: ‘The AGENDA trial’. Melanoma Res.
24:237–243. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
https://www.gov.pl/web/zdrowie/choroby-onkologiczneMarch.
2021
|
|
109
|
https://clinicaltrials.gov/December. 2020
|
|
110
|
Jurišić V, Vuletić A, Mirjačić Martinović
K and Konjević G: The pole of NK cells in cancer. Cancer
Immunology. Rezai N: Springer; New York, NY: pp. 133–146. 2020,
View Article : Google Scholar
|