Breast cancer (BC) is the most diagnosed disease
among women and has the second highest incidence among all types of
cancer worldwide (1.7 million cases, 11.9%) (1). Excessive expression of human epidermal
growth factor receptor-2 (HER2) has been investigated in 20–30% of
BC patients and generally recognized as a marker for invasive
disease, which is likely to be highly metastatic, to be drug
resistant and to spread rapidly (2–4). HER2 is
a member of the HER/EGFR/ERBB group of protein kinase superfamily,
which receives signals to regulate cell survival, adhesion,
motility, proliferation and resistance to apoptosis (5,6). A
tyrosine kinase (TK) domain located in the HER2 receptor plays an
important role in the occurrence of BC, as it is induced by
phosphorylation after HER2 homo/hetero dimerization and then
activates multiple signal transduction pathways (5,7). The
phosphatidylinositol 3-kinase (PI3K) pathway and the Ras/Raf
mitogen-activated protein kinase (MAPK) pathway are the most fully
investigated of these pathways, both of which may contribute to the
acquired resistance against targeted therapy drugs (8–10).
Related research has identified that inhibition of the PI3K-Akt
pathway with PI3K inhibitors is effective to reverse tumor growth
(11–13). When the HER2 proto-oncogene undergoes
mutation and conversions into the HER2 oncogene (14), HER2 receptor protein is highly
expressed at the cell membrane, and multiple downstream signaling
pathways are excessively activated, resulting in uncontrollable
cell growth, repeated division of cells, and altered adhesion
properties (7,14,15).
Based on its unique role in the development of HER2+ BC,
HER2 and its downstream signaling pathways have become extremely
important targets for therapy. HER2+ BC that is induced
by HER2 amplification was significantly reversed by treatments that
targeted HER2 and HER2 TK (15,16).
Targeted therapy that depends on the expression levels of HER2 has
made great progress, although a considerable portion of the
population are resistant.
Among all of the drugs that target HER2 and HER2 TK,
trastuzumab, pertuzumab, trastuzumab emtansine (T-DM1) and
lapatinib have been proven to be effective in treating
HER2+ BC in several clinical trials compared with
chemotherapy drugs alone (17–20).
Trastuzumab, the first-generation targeted therapy drug, is a
humanized monoclonal antibody targeting the extracellular domain of
HER-2 (21,22) and has the ability to downregulate the
signaling pathways involving PI3K/Akt and MAPK (23,24),
which in turn inhibits the proliferation of BC cells that
overexpress HER2. Trastuzumab, both administered as a single agent
or injected in combination with a series of chemotherapy agents
(such as docetaxel or vinorelbine plus trastuzumab (25–27),
showed anti-tumor effects and remarkably improved time to
progression, response and survival rate (22,28,29).
Furthermore, several randomized control trials have revealed that
trastuzumab plus chemotherapy drugs significantly reduce the risk
of recurrence and death and promote survival incidence compared to
chemotherapy drugs alone (26,27),
making trastuzumab the cornerstone of adjuvant treatments for
HER2+ BC.
Pertuzumab belongs to the second-generation targeted
drug family, which elicits similar effects to trastuzumab and can
significantly promote survival outcomes (25,30).
Pertuzumab binds to HER2 and thus blocks the signaling pathways by
blocking a binding pocket necessary for receptor dimerization
(31). Pertuzumab was approved by
FDA as a neoadjuvant therapy in combination with trastuzumab and
cytotoxic chemotherapy (32).
Related research demonstrated that pertuzumab in combination with
trastuzumab was more effective in the blockade of HER2 signaling
pathways in vitro and in vivo than either antibody
alone (33).
T-DM1, a second-generation antibody, has attracted
great interest from researchers for its effective role as an
adjuvant and neoadjuvant (34). The
phase III EMILIA study and RESA study proved that T-DM1 was
efficacious as afunctional treatment and facilitated better
prognosis and improvements in health-related quality of life
(35–37). T-DM1 has been investigated to promote
progression-free survival (PFS) and overall survival (OS) in
patients who were HER2+ and previously treated with
trastuzumab and taxane (17).
Lapatinib is a reversible HER2 TK inhibitor that
reacts with the ATP binding site, which in turn improves PFS and
clinical benefit rate (CBR) by inhibiting the autophosphorylation
of ErbB1 and ErbB2 and downstream proliferative signaling pathways
(25,38,39).
Similarly, in some neoadjuvant clinical trials, lapatinib has been
used in dual blockade with trastuzumab to treat patients with
HER2+ BC (18,40–42).
In addition to the gradual increase in resistance,
another important issue that hampers the application of trastuzumab
in clinical patients is side effects, especially cardiomyopathy,
which was reported to affect 2.8–3.3% of patient (52,53).
More concerning, when trastuzumab was administered in combination
with anthracyclines, cardiac dysfunction, such as left ventricular
ejection fraction (LVEF) and congestive heart failure (CHF),
affected about a quarter of patients as reported by some studies
(28,54).
It has been confirmed that pertuzumab could
strengthen the effect of trastuzumab (33). Similarly, a clinical study found that
trastuzumab plus pertuzumab received an ORr of 24.2% and a CBR of
50% (55). In another clinical
trial, a response rate of 18% was demonstrated after treatment with
trastuzumab and pertuzumab combination (56); however, over half of the patients did
not benefit from treatment.
Lapatinib yielded response rates from 24–53.2% in
clinical activity in advanced HER2-overexpression BC (17,19,40).
Although lapatinib was speculated to play a vital role in treating
trastuzumab-resistant, HER2-overexpressed tumors, the response
rates ranged from 1.4–8.8% after lapatinib monotherapy (19,61). The
addition of lapatinib and capecitabine received a 51% reduction in
the risk of disease progression and a 2-fold time to progression
compared to capecitabine alone (16). However, at least half of the patients
showed no benefit from treatment.
Furthermore, with the presence of two kinds of drug
resistance, ‘a primary or inherent resistance and a secondary or
acquired resistance’ (24,46,62), we
are facing two serious challenges: i) Overcoming the drug
resistance; and ii) searching for new effective drugs.
The inherent or acquired resistance to targeted
therapy drugs, as well as the relatively serious side effects,
limit the application of targeted therapy drugs. These two kinds of
unfavorable factors are the driving forces to continue to develop
new drugs. To overcome the development of drug resistance, some
studies explored the possible treatment methods and identified some
substances that had potential value. Specifically, the discovery
and application of Taxol greatly improved the prognosis of
patients. Interestingly, several studies investigated natural
anti-cancer substances that had shown significant anti-cancer
effects, which might prevent the tumorigenesis of BC. Furthermore,
the new ADC and targeted delivery of drugs were found to be
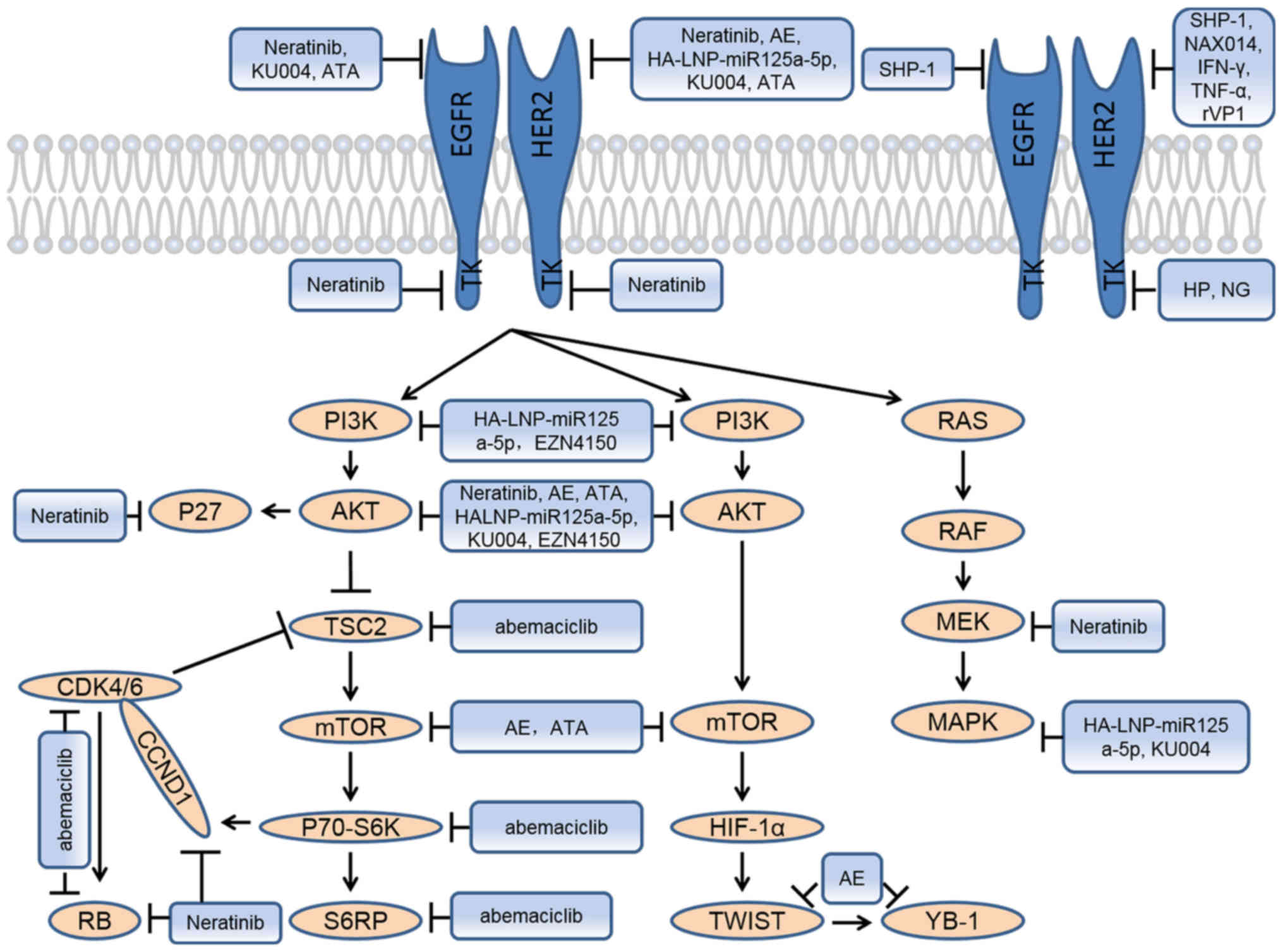
effective in treating HER2+ BC patients. In this review,
we concentrate on some research studies for putative application in
clinical treatment. And we summarize the signaling pathways of
corresponding effective potential clinical drugs (Fig. 1).
Neratinib is an irreversible kinase inhibitor and a
derivative of EKB-569 (EGFR inhibitor) (63–65).
Neratinib significantly inhibited EGFR/HER2 kinase after binding to
the ATP pocket and blocking downstream signaling pathways (59) and showed anti-cancer bioactivities in
HER2-overexpression cell lines and in patients with or without
prior trastuzumab treatment (66–68).
Neratinib inhibited proliferation and promoted G1-S phase arrest by
regulating HER2 and its downstream signaling pathways, specifically
through downregulation of pEGFR, pHER2, pAKT, pMEK and pRb levels
and cyclin D1 (CCND1) expression and increase of p27 levels in a
HER2-dependent manner (69). Some
studies also discovered that neratinib improved trastuzumab
resistance and restored sensitivity to trastuzumab in
HER2+ BC (69,70). Many clinical trials investigated the
functions of neratinib in treating HER2+ BC alone or in
combination with trastuzumab, which exhibited great clinical
application prospects. A more important role of neratinib was
observed when combined with paclitaxel in treating patients who
received prior taxane, trastuzumab and lapatinib therapies
(71). Neratinib was effective as a
single agent or in combination with different chemotherapy drugs in
the treatment of HER2+ MBC patients and early BC patients (68,72–74). In
a multicenter, randomized, double-blind and placebo-controlled
phase III trial (ExteNET), which involved 2,840 women, a total of
invasive disease-free survival events of 70 patients in the
neratinib group and 109 patients in the placebo group occurred,
corresponding to 93.9 and 91.6% 2-year invasive disease-free
survival rates, respectively (75).
All of these results above show that neratinib is quite effective
and is close to clinical application.
Antibody-drug conjugates (ADCs) are constructed by
covalently attaching small-molecule toxins to antibodies (85–87).
T-DM1 is a ADCs that has shown significant activity in treating
HER2+ BC (86,87). A new biparatopic ADC was constructed,
consisting of the trastuzumab scFv unit, the 39S Fv unit, and
AZ13599185, which inhibits microtubule polymerization during
mitosis. The new biparatopic ADC retained HER2 binding specificity
and could effectively deliver cytotoxic agents into the targeted
tumors. Compared to T-DM1, the new biparatopic ADC demonstrated at
least 10-fold cell killing activity in HER2-expressing cancer cell
lines in a HER2-dependent manner and showed activity in cancer
cells that were intrinsically resistant to T-DM1. In vivo
study suggested the possibility of clinical application of the new
biparatopic ADC, as it induced full tumor degradation and inhibited
tumor growth in a primary BC xenograft model and an intrinsically
or acquired T-DM1-resistant xenograft model, which was not observed
after treatment with T- DM1 alone or in combination with
pertuzumab. These valuable results show that development of the new
biparatopic ADC was necessary to explore a more effective drug for
the treatment of HER2+ BC (88).
Due to the putative role of EGFR in trastuzumab
resistance, blocking EGFR and its corresponding downstream
signaling pathways may produce better prognosis. The src homology 2
(SH2) containing tyrosine phosphatase-1 (SHP-1) regulated the
intracellular phosphotyrosine level and was reduced or absent in
many kinds of cancer cell lines and tissues (89–91).
Overexpression of wild-type SHP-1 sensitized trastuzumab-resistant
cells to trastuzumab treatment. Furthermore, overexpression of
wild-type SHP-1 also significantly upregulated apoptosis and
decreased EGFR and HER2, as well as their phosphorylation levels,
in trastuzumab-resistant cells. Wild-type SHP-1 could bind to pEGFR
and pHER2, and thus reduced both pEGFR and pHER2 protein levels.
In vivo study demonstrated that SHP-1-overexpression mice
showed delayed tumor progression and growth and achieved a better
OS after treatment with trastuzumab compared with the control
(92).
Fatty acid synthase (FASN) showed activity in
promoting tumorigenesis by activating HER2/PI3K/AKT/mTOR and MAPK
signaling pathways (93–95). EGFR and pEGFR increased in
trastuzumab resistant cells noticeably, which was consistent with
the study of Wu et al (92).
Pertuzumab combined with EGCG, a classical FASN inhibitor, was more
effective than pertuzumab alone against resistant HER2+
BC cells and increased the apoptosis of cancer cells in a
trastuzumab plus lapatinib-resistant HER2+ PDX model
compared with pertuzumab alone. In vivo study showed that
dual FASN and HER2 blockade achieved more effective tumor reduction
compared with EGCG or pertuzumab as single agent (50).
The occurrence of all tumors is due to genetic
mutations, so gene therapy is the most effective treatment approach
for all cancers. Using an effective vector to accurately deliver
drugs to the tumors is a very valid treatment method to stop the
tumor progression.
A new delivery platform, which was able to escape
from lysosomal degradation and distribute symmetrical in the
cytoplasm, was established to send mature tumor suppressor
microRNA125a-5p to treat HER2+ MBC. miR125a-5p
significantly decreased cellular proliferation and migration in
comparison with control cells, which might have been largely caused
by knockdown of the HER2 mRNA levels. HA-LNP-miR125a-5p reduced the
levels of HER2, PI3K, pAKT, Ki67 and pERK1/2 by over 30, 35, 40,
~40 and 20%, respectively, which indicated that HA-LNP-miR125a-5p
could treat BC through inhibiting HER2 and its downstream signaling
pathways (96).
Natural anti-cancer substances played an important
role in the treatment of BC and some new natural anti-cancer
substances will play a role in the treatment of HER2+
BC. Paclitaxel is the most successful natural anti-cancer drug,
which was extracted first from the bark and wood of Pacific Yew
tree (98). Hesperetin (HP) and
naringenin (NG) belong to flavonoids, which have shown anti-cancer
and pro-apoptotic activity (99). An
anthraquinone compound, aloe-emodin (AE), effectively suppressed
HER2 expression and cell proliferation in a dose-dependent manner
consistent with promotion of apoptosis and G1 cell cycle arrest in
HER2+ BC cells. Twist and Y-box binding protein 1 (YB-1)
have been investigated for promoting cell proliferation, tumor
metastasis, invasion, angiogenesis and anticancer-drug resistance
(100,101). In vitro study showed that AE
observably inhibited cancer cell migration and invasion rates
through promoting E-cadherin levels, which restored the epithelial
cell adhesion, and inhibiting factors, which activated cancer cell
metastasis. These results had important clinical significance and
were confirmed by in vivo study in a SkBr3 cell xenograft
model (102). Irisin is newly
discovered, secreted from muscle tissue and adipose tissue, and
recognized as an adipokine, which has been proven to participate in
breast carcinogenesis (103,104).
Irisin or its structural analogues may become new therapeutic drugs
(105). Several studies have
investigated the use of apigenin decreasing the risk of a variety
of cancers, including BC (106–108).
NAX014, a derivative of berberine (BBR), was effective in
inhibiting a variety of cancer cells (109,110)
tended to reduce HER2 expression in tumor tissues (111). Acetyl tanshinone IIA (ATA), a
tanshinone IIA derivative (112),
had shown activity against BC (113). In vivo study showed that
injection of ATA reduced tumor volume and tumor weight remarkably
(112).
Anti-ErbB2 mAb therapy failed to reduce tumor growth
in IL21R-/- mice; however, anti-ErbB2 mAb therapy succeeded in WT
mice, which indicated that the IL21 signaling pathway had a strong
correlation with trastuzumab resistance. Furthermore, IL21R
expressed by CD8+ T-cells was required for mice that
transferred with WT CD8+ T-cells to achieve anti-ErbB2
mAb therapy success, compared with the mice treated with
IL21R−/− CD8+ T-cells. Recombinant IL21
combined with anti-ErbB2 mAb therapy significantly inhibited tumor
growth and showed activity in lowering metastatic tumors (116).
Recombinant DNA-derived viral capsid protein-1
(rVP1) has been proven to induce apoptosis and suppress invasion in
several cancers. They investigated that both in vivo and
in vitro rVP1 treatment significantly inhibited cancer cell
metastasis and invasion, consistent with increased E-cadherin and
decreased a-vimentin levels in vitro. Furthermore, the mRNA
and protein expression of HER2 were inhibited by rVP1 in a
dose-dependent manner (117).
EZN4150, an antisense oligonucleotide, is an
inhibitor of the PIK3CA gene that encodes the p110α type I PI3K
catalytic subunit. EZN4150 combined with lapatinib or BKM120 (a
type I PI3K inhibitor) decreased pAkt and increased cleaved
caspase-3 levels, achieving a greater effect in combination than
either compound alone. Autophagy is a process that could inhibit
tumor initiation but support tumor progression (124,125).
The role of autophagy in promoting cell survival was blocked by
EZN4150 instead of BKM120 in a p110α-independent manner, which
might be mediated by Vps34 ablation, as EZN4150 downregulated both
p110α and Vps34 expression. The combined knockdown of p110α and
Vps34 significantly decreased cell numbers, increased the level of
cleaved caspase-3 and increased lapatinib-mediated growth
inhibition in BT474 and SKBR3 cell lines. Although both lapatinib
and BYL719 (a p110α-specific PI3K inhibitor (126) treatment robustly induced caspase
3/7 activity, SAR405, an inhibitor of Vps34, more significantly
increased caspase 3/7 activity than lapatinib, BYL719 or their
combination. These results established Vps34 as a new therapeutic
target, and EZN4150 was able to improve clinical prognosis by
increasing tumor cell killing (127).
Programmed death ligand 1 (PD-L1) is the ligand of
programmed death 1 (PD-1). Anti-PD-1/PD-L1 therapy is a novel
immune-checkpoint inhibition therapy and anti-PD-1/PD-L1 agents,
such as nivolumab, pembrolizumab, atezolizumab, durvalumab and
avelumab have been widely applied to treat various types of cancer
(128–130). Anti-PD-1/PD-L1 agents have shown
antitumor activity in BC, especially in the triple-negative
subtypes of breast cancer (TNBC) (131,132).
But PD-L1 expression is associated with HER2+ status and
there is an independent poor prognostic impact of PD-L1 in
HER2+ BCs (132–134). In a phase 1b trial which 168
patients with MBC received avelumab, avelumab showed an acceptable
clinical activity (135).
Currently, many clinical trials in HER2+ cohort are
ongoing, such as NCT02648477 and NCT02129556 for pembrolizumab,
NCT02605915 for atezolizumab and NCT02649686 for durvalumab
(131). Anti-PD-1/PD-L1 agents will
benefit the patients with HER2+ BC in the future.
The advent of targeted therapy drugs is a
revolutionary breakthrough in the history of BC treatment.
Trastuzumab is the first-generation targeted therapy drug and has
been used widely to treat HER2+ BC. Due to the
resistance to trastuzumab and severe side effects,
second-generation targeted therapy drugs have been successfully
developed and applied for clinical treatment, such as pertuzumab,
T-DM1 and lapatinib. Although all of them achieved efficacy in the
treatment of HER2+ BC, quite a number of patients did
not benefit on account of inherent insensitivity, acquired
resistance, or potential side effects. How should we treat this
subgroup of HER2+ BC patients? Elucidating the mechanism
of drug resistance and seeking effective drugs to overcome this
hurdle may benefit these patients. In addition, new drugs should be
developed for clinical application, and many researchers are
actively working in this direction, with particular focus on
natural anti-cancer substances and accurate delivery drugs that
were identified for putative ability to treat HER2+ BC.
Moreover, these new drugs may also strengthen the effect of
targeted therapy drugs in treating HER2+ BC patients who
are inherently sensitive to targeted therapy drugs. Based on this
review, further investigations are needed to strengthen these
findings and identify drugs that can overcome targeted therapy
drug-resistance or natural anti-cancer substances that are
effective in treating HER2+ BC.
Not applicable.
No funding was received.
All data generated or analyzed during this study
are included in this published article.
YC contributed to the conception of the study. NJ
contributed to manuscript preparation and wrote the manuscript.
JJL, JW, BNZ, AL, ZYC, SG, BBL, YZD, RYY, HFY, XYF, JLZ and HMY
contributed in the writing of the manuscript and assisted in the
literature research.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hudis CA: Trastuzumab-mechanism of action
and use in clinical practice. N Engl J Med. 357:39–51. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Adamczyk A, Niemiec J, Janecka A,
Harazin-Lechowska A, Ambicka A, Grela-Wojewoda A, Domagała-Haduch
M, Cedrych I, Majchrzyk K, Kruczak A, et al: Original paper
prognostic value of PIK3CA mutation status, PTEN and androgen
receptor expression for metastasis-free survival in HER2-positive
breast cancer patients treated with trastuzumab in adjuvant
setting. Pol J Pathol. 66:133–141. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Loibl S and Gianni L: HER2-positive breast
cancer. Lancet. 389:2415–2429. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Arteaga CL and Engelman JA: ERBB
receptors: From oncogene discovery to basic science to
mechanism-based cancer therapeutics. Cancer Cell. 25:282–303. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Petrelli F, Tomasello G, Barni S, Lonati
V, Passalacqua R and Ghidini M: Clinical and pathological
characterization of HER2 mutations in human breast cancer: A
systematic review of the literature. Breast Cancer Res Treat.
166:339–349. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yarden Y and Sliwkowski MX: Untangling the
ErbB signalling network. Nat Rev Mol Cell Biol. 2:127–137. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wang Q, Liu P, Spangle JM, Von T, Roberts
TM, Lin NU, Krop IE, Winer EP and Zhao JJ: PI3K-p110α mediates
resistance to HER2-targeted therapy in HER2+, PTEN-deficient breast
cancers. Oncogene. 35:3607–3612. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ritter CA, Perez-Torres M, Rinehart C,
Guix M, Dugger T, Engelman JA and Arteaga CL: Human breast cancer
cells selected for resistance to trastuzumab in vivo overexpress
epidermal growth factor receptor and ErbB ligands and remain
dependent on the ErbB receptor network. Clin Cancer Res.
13:4909–4919. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Larionov AA: Current therapies for human
epidermal growth factor receptor 2-positive metastatic breast
cancer patients. Front Oncol. 8:892018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Junttila TT, Akita RW, Parsons K, Fields
C, Lewis Phillips GD, Friedman LS, Sampath D and Sliwkowski MX:
Ligand-independent HER2/HER3/PI3K complex is disrupted by
trastuzumab and is effectively inhibited by the PI3K inhibitor
GDC-0941. Cancer Cell. 15:429–440. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yakes FM, Chinratanalab W, Ritter CA, King
W, Seelig S and Arteaga CL: Herceptin-induced inhibition of
phosphatidylinositol-3 kinase and Akt Is required for
antibody-mediated effects on p27, cyclin D1, and antitumor action.
Cancer Res. 62:4132–4141. 2002.PubMed/NCBI
|
|
13
|
Fry EA, Taneja P and Inoue K: Oncogenic
and tumor-suppressive mouse models for breast cancer engaging
HER2/neu. Int J Cancer. 140:495–503. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Parsa Y, Mirmalek SA, Kani FE, Aidun A,
Salimi-Tabatabaee SA, Yadollah-Damavandi S, Jangholi E, Parsa T and
Shahverdi E: A review of the clinical implications of breast cancer
biology. Electron Physician. 8:2416–2424. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nami B and Wang Z: HER2 in breast cancer
stemness: A negative feedback loop towards trastuzumab resistance.
Cancers (Basel). 9(pii): E402017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gajria D and Chandarlapaty S:
HER2-amplified breast cancer: Mechanisms of trastuzumab resistance
and novel targeted therapies. Expert Rev Anticancer Ther.
11:263–275. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Verma S, Miles D, Gianni L, Krop IE,
Welslau M, Baselga J, Pegram M, Oh DY, Diéras V, Guardino E, et al:
Trastuzumab emtansine for HER2-positive advanced breast cancer. N
Engl J Med. 367:1783–1791. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rimawi MF, Mayer IA, Forero A, Nanda R,
Goetz MP, Rodriguez AA, Pavlick AC, Wang T, Hilsenbeck SG,
Gutierrez C, et al: Multicenter phase II study of neoadjuvant
lapatinib and trastuzumab with hormonal therapy and without
chemotherapy in patients with human epidermal growth factor
receptor 2-overexpressing breast cancer: TBCRC 006. J Clin Oncol.
31:1726–1731. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Robidoux A, Tang G, Rastogi P, Geyer CE
Jr, Azar CA, Atkins JN, Fehrenbacher L, Bear HD, Baez-Diaz L,
Sarwar S, et al: Lapatinib as a component of neoadjuvant therapy
for HER2-positive operable breast cancer (NSABP protocol B-41): An
open-label, randomised phase 3 trial. Lancet Oncol. 14:1183–1192.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Joensuu H: Escalating and de-escalating
treatment in HER2-positive early breast cancer. Cancer Treat Rev.
52:1–11. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ban M, Viculin J, Tomic S, Capkun V,
Strikic A, Mise BP, Utrobicic I and Vrdoljak E: Retrospective
analysis of efficacy of trastuzumab in adjuvant treatment of HER 2
positive early breast cancer-single institution experience.
Neoplasma. 63:761–767. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cameron D, Piccart-Gebhart MJ, Gelber RD,
Procter M, Goldhirsch A, de Azambuja E, Castro G Jr, Untch M, Smith
I, Gianni L, et al: 11 years' follow-up of trastuzumab after
adjuvant chemotherapy in HER2-positive early breast cancer: Final
analysis of the HERceptin Adjuvant (HERA) trial. Lancet.
389:1195–1205. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
De P, Hasmann M and Leyland-Jones B:
Molecular determinants of trastuzumab efficacy: What is their
clinical relevance? Cancer Treat Rev. 39:925–934. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Maximiano S, Magalhães P, Guerreiro MP and
Morgado M: Trastuzumab in the treatment of breast cancer. BioDrugs.
30:75–86. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Figueroa-Magalhães MC, Jelovac D, Connolly
RM and Wolff AC: Treatment of HER2-positive breast cancer. Breast.
23:128–136. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhu ZL, Zhang J, Chen ML and Li K:
Efficacy and safety of trastuzumab added to standard treatments for
HER2-positive metastatic breast cancer patients. Asian Pac J Cancer
Prev. 14:7111–7116. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Osoba D, Slamon DJ, Burchmore M and Murphy
M: Effects on quality of life of combined trastuzumab and
chemotherapy in women with metastatic breast cancer. J Clin Oncol.
20:3106–3113. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Slamon DJ, Leyland-Jones B, Shak S, Fuchs
H, Paton V, Bajamonde A, Fleming T, Eiermann W, Wolter J, Pegram M,
et al: Use of chemotherapy plus a monoclonal antibody against HER2
for metastatic breast cancer that overexpresses HER2. N Engl J Med.
344:783–792. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Rugo HS, Barve A, Waller CF,
Hernandez-Bronchud M, Herson J, Yuan J, Sharma R, Baczkowski M,
Kothekar M, Loganathan S, et al: Effect of a proposed trastuzumab
biosimilar compared with trastuzumab on overall response rate in
patients with ERBB2 (HER2)-positive metastatic breast cancer: A
randomized clinical trial. JAMA. 317:37–47. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Laakmann E, Müller V, Schmidt M and Witzel
I: Systemic treatment options for HER2-positive breast cancer
patients with brain metastases beyond trastuzumab: A literature
review. Breast Care (Basel). 12:168–171. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Franklin MC, Carey KD, Vajdos FF, Leahy
DJ, de Vos AM and Sliwkowski MX: Insights into ErbB signaling from
the structure of the ErbB2-pertuzumab complex. Cancer Cell.
5:317–328. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Tiwari SR, Mishra P, Raska P, Calhoun B,
Abraham J, Moore H, Budd GT, Fanning A, Valente S, Stewart R, et
al: Retrospective study of the efficacy and safety of neoadjuvant
docetaxel, carboplatin, trastuzumab/pertuzumab (TCH-P) in
nonmetastatic HER2-positive breast cancer. Breast Cancer Res Treat.
158:189–193. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Scheuer W, Friess T, Burtscher H,
Bossenmaier B, Endl J and Hasmann M: Strongly enhanced antitumor
activity of trastuzumab and pertuzumab combination treatment on
HER2-positive human xenograft tumor models. Cancer Res.
69:9330–9336. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Perez EA, Barrios C, Eiermann W, Toi M, Im
YH, Conte P, Martin M, Pienkowski T, Pivot X, Burris H III, et al:
Trastuzumab emtansine with or without pertuzumab versus trastuzumab
plus taxane for human epidermal growth factor receptor 2-positive,
advanced breast cancer: Primary results from the phase III MARIANNE
study. J Clin Oncol. 35:141–148. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Cairns L and Curigliano G: Highlights from
the 38th SABCS annual meeting, 8th-12th December 2015, San Antonio,
USA. Ecancermedicalscience. 10:6182016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Welslau M, Diéras V, Sohn JH, Hurvitz SA,
Lalla D, Fang L, Althaus B, Guardino E and Miles D:
Patient-reported outcomes from EMILIA, a randomized phase 3 study
of trastuzumab emtansine (T-DM1) versus capecitabine and lapatinib
in human epidermal growth factor receptor 2-positive locally
advanced or metastatic breast cancer. Cancer. 120:642–651. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Krop IE, Kim SB, Martin AG, LoRusso PM,
Ferrero JM, Badovinac-Crnjevic T, Hoersch S, Smitt M and Wildiers
H: Trastuzumab emtansine versus treatment of physician's choice in
patients with previously treated HER2-positive metastatic breast
cancer (TH3RESA): Final overall survival results from a randomised
open-label phase 3 trial. Lancet Oncol. 18:743–754. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Blackwell KL, Burstein HJ, Storniolo AM,
Rugo H, Sledge G, Koehler M, Ellis C, Casey M, Vukelja S, Bischoff
J, et al: Randomized study of Lapatinib alone or in combination
with trastuzumab in women with ErbB2-positive,
trastuzumab-refractory metastatic breast cancer. J Clin Oncol.
28:1124–1130. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Spector NL, Xia W, Burris H III, Hurwitz
H, Dees EC, Dowlati A, O'Neil B, Overmoyer B, Marcom PK, Blackwell
KL, et al: Study of the biologic effects of lapatinib, a reversible
inhibitor of ErbB1 and ErbB2 tyrosine kinases, on tumor growth and
survival pathways in patients with advanced malignancies. J Clin
Oncol. 23:2502–2512. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Guarneri V, Frassoldati A, Bottini A,
Cagossi K, Bisagni G, Sarti S, Ravaioli A, Cavanna L, Giardina G,
Musolino A, et al: Preoperative chemotherapy plus trastuzumab,
lapatinib, or both in human epidermal growth factor receptor
2-positive operable breast cancer: Results of the randomized phase
II CHER-LOB study. J Clin Oncol. 30:1989–1995. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Xu ZQ, Zhang Y, Li N, Liu PJ, Gao L, Gao X
and Tie XJ: Efficacy and safety of lapatinib and trastuzumab for
HER2-positive breast cancer: A systematic review and meta-analysis
of randomised controlled trials. BMJ Open. 7:e0130532017.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Solinas C, Ceppi M, Lambertini M,
Scartozzi M, Buisseret L, Garaud S, Fumagalli D, de Azambuja E,
Salgado R, Sotiriou C, et al: Tumor-infiltrating lymphocytes in
patients with HER2-positive breast cancer treated with neoadjuvant
chemotherapy plus trastuzumab, lapatinib or their combination: A
meta-analysis of randomized controlled trials. Cancer Treat Rev.
57:8–15. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Hanker AB, Pfefferle AD, Balko JM, Kuba
MG, Young CD, Sánchez V, Sutton CR, Cheng H, Perou CM, Zhao JJ, et
al: Mutant PIK3CA accelerates HER2-driven transgenic mammary tumors
and induces resistance to combinations of anti-HER2 therapies. Proc
Natl Acad Sci USA. 110:14372–14377. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Nagata Y, Lan KH, Zhou X, Tan M, Esteva
FJ, Sahin AA, Klos KS, Li P, Monia BP, Nguyen NT, et al: PTEN
activation contributes to tumor inhibition by trastuzumab, and loss
of PTEN predicts trastuzumab resistance in patients. Cancer Cell.
6:117–127. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Singh JC, Jhaveri K and Esteva FJ:
HER2-positive advanced breast cancer: Optimizing patient outcomes
and opportunities for drug development. Br J Cancer. 111:1888–1898.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Vu T and Claret FX: Trastuzumab: Updated
mechanisms of action and resistance in breast cancer. Front Oncol.
2:622012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Rexer BN, Chanthaphaychith S, Dahlman K
and Arteaga CL: Direct inhibition of PI3K in combination with dual
HER2 inhibitors is required for optimal antitumor activity in HER2+
breast cancer cells. Breast Cancer Res. 16:R92014. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Narayan M, Wilken JA, Harris LN, Baron AT,
Kimbler KD and Maihle NJ: Trastuzumab-induced HER reprogramming in
‘resistant’ breast carcinoma cells. Cancer Res. 69:2191–2194. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Diermeier S, Horváth G, Knuechel-Clarke R,
Hofstaedter F, Szöllosi J and Brockhoff G: Epidermal growth factor
receptor coexpression modulates susceptibility to Herceptin in
HER2/neu overexpressing breast cancer cells via specific
erbB-receptor interaction and activation. Exp Cell Res.
304:604–619. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Blancafort A, Giró-Perafita A, Oliveras G,
Palomeras S, Turrado C, Campuzano Ò, Carrión-Salip D, Massaguer A,
Brugada R, Palafox M, et al: Dual fatty acid synthase and HER2
signaling blockade shows marked antitumor activity against breast
cancer models resistant to anti-HER2 drugs. PLoS One.
10:e01312412015. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
O'Donovan N, Byrne AT, O'Connor AE, McGee
S, Gallagher WM and Crown J: Synergistic interaction between
trastuzumab and EGFR/HER-2 tyrosine kinase inhibitors in HER-2
positive breast cancer cells. Invest New Drugs. 29:752–759. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Perez EA, Suman VJ, Davidson NE, Sledge
GW, Kaufman PA, Hudis CA, Martino S, Gralow JR, Dakhil SR, Ingle
JN, et al: Cardiac safety analysis of doxorubicin and
cyclophosphamide followed by paclitaxel with or without trastuzumab
in the North central cancer treatment group N9831 adjuvant breast
cancer trial. J Clin Oncol. 26:1231–1238. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Dokmanovic M, King KE, Mohan N, Endo Y and
Wu WJ: Cardiotoxicity of ErbB2-targeted therapies and its impact on
drug development, a spotlight on trastuzumab. Expert Opin Drug
Metab Toxicol. 13:755–766. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Keefe DL: Trastuzumab-associated
cardiotoxicity. Cancer. 95:1592–1600. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Baselga J, Gelmon KA, Verma S, Wardley A,
Conte P, Miles D, Bianchi G, Cortes J, McNally VA, Ross GA, et al:
Phase II trial of pertuzumab and trastuzumab in patients with human
epidermal growth factor receptor 2-positive metastatic breast
cancer that progressed during prior trastuzumab therapy. J Clin
Oncol. 28:1138–1144. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Portera CC, Walshe JM, Rosing DR,
Denduluri N, Berman AW, Vatas U, Velarde M, Chow CK, Steinberg SM,
Nguyen D, et al: Cardiac toxicity and efficacy of trastuzumab
combined with pertuzumab in patients with [corrected] human
epidermal growth factor receptor 2-positive metastatic breast
cancer. Clin Cancer Res. 14:2710–2716. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Burris HA III, Rugo HS, Vukelja SJ, Vogel
CL, Borson RA, Limentani S, Tan-Chiu E, Krop IE, Michaelson RA,
Girish S, et al: Phase II study of the antibody drug conjugate
trastuzumab-DM1 for the treatment of human epidermal growth factor
receptor 2 (HER2)-positive breast cancer after prior HER2-directed
therapy. J Clin Oncol. 29:398–405. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
LoRusso PM, Weiss D, Guardino E, Girish S
and Sliwkowski MX: Trastuzumab emtansine: A unique antibody-drug
conjugate in development for human epidermal growth factor receptor
2-positive cancer. Clin Cancer Res. 17:6437–6447. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Kowalczyk L, Bartsch R, Singer CF and Farr
A: Adverse events of trastuzumab emtansine (T-DM1) in the treatment
of HER2-positive breast cancer patients. Breast Care (Basel).
12:401–408. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Watanabe J, Ito Y, Saeki T, Masuda N,
Takano T, Takao S, Nakagami K, Tsugawa K, Nakagawa S, Kanatani K
and Nakayama T: Safety evaluation of trastuzumab emtansine in
japanese patients with HER2-positive advanced breast cancer. In
Vivo. 31:493–500. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Blackwell KL, Pegram MD, Tan-Chiu E,
Schwartzberg LS, Arbushites MC, Maltzman JD, Forster JK, Rubin SD,
Stein SH and Burstein HJ: Single-agent lapatinib for
HER2-overexpressing advanced or metastatic breast cancer that
progressed on first- or second-line trastuzumab-containing
regimens. Ann Oncol. 20:1026–1031. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Ahmad S, Gupta S, Kumar R, Varshney GC and
Raghava GP: Herceptin resistance database for understanding
mechanism of resistance in breast cancer patients. Sci Rep.
4:44832014. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Rabindran SK, Discafani CM, Rosfjord EC,
Baxter M, Floyd MB, Golas J, Hallett WA, Johnson BD, Nilakantan R,
Overbeek E, et al: Antitumor activity of HKI-272, an orally active,
irreversible inhibitor of the HER-2 tyrosine kinase. Cancer Res.
64:3958–3965. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Tsou HR, Overbeek-Klumpers EG, Hallett WA,
Reich MF, Floyd MB, Johnson BD, Michalak RS, Nilakantan R,
Discafani C, Golas J, et al: Optimization of
6,7-disubstituted-4-(arylamino)quinoline-3-carbonitriles as orally
active, irreversible inhibitors of human epidermal growth factor
receptor-2 kinase activity. J Med Chem. 48:1107–1131. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Keyvanjah K, DiPrimeo D, Li A, Obaidi M,
Swearingen D and Wong A: Pharmacokinetics of neratinib during
coadministration with lansoprazole in healthy subjects. Br J Clin
Pharmacol. 83:554–561. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Saura C, Garcia-Saenz JA, Xu B, Harb W,
Moroose R, Pluard T, Cortés J, Kiger C, Germa C, Wang K, et al:
Safety and efficacy of neratinib in combination with capecitabine
in patients with metastatic human epidermal growth factor receptor
2-positive breast cancer. J Clin Oncol. 32:3626–3633. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Burstein HJ, Sun Y, Dirix LY, Jiang Z,
Paridaens R, Tan AR, Awada A, Ranade A, Jiao S, Schwartz G, et al:
Neratinib, an irreversible ErbB receptor tyrosine kinase inhibitor,
in patients with advanced ErbB2-positive breast cancer. J Clin
Oncol. 28:1301–1307. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Echavarria I, López-Tarruella S,
Márquez-Rodas I, Jerez Y and Martin M: Neratinib for the treatment
of HER2-positive early stage breast cancer. Expert Rev Anticancer
Ther. 17:669–679. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Canonici A, Gijsen M, Mullooly M, Bennett
R, Bouguern N, Pedersen K, O'Brien NA, Roxanis I, Li JL, Bridge E,
et al: Neratinib overcomes trastuzumab resistance in HER2 amplified
breast cancer. Oncotarget. 4:1592–1605. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Mohd Nafi SN, Generali D, Kramer-Marek G,
Gijsen M, Strina C, Cappelletti M, Andreis D, Haider S, Li JL,
Bridges E, et al: Nuclear HER4 mediates acquired resistance to
trastuzumab and is associated with poor outcome in HER2 positive
breast cancer. Oncotarget. 5:5934–5949. 2014.PubMed/NCBI
|
|
71
|
Jankowitz RC, Abraham J, Tan AR, Limentani
SA, Tierno MB, Adamson LM, Buyse M, Wolmark N and Jacobs SA: Safety
and efficacy of neratinib in combination with weekly paclitaxel and
trastuzumab in women with metastatic HER2-positive breast cancer:
An NSABP foundation research program phase I study. Cancer
Chemother Pharmacol. 72:1205–1212. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Kourie HR, Chaix M, Gombos A, Aftimos P
and Awada A: Pharmacodynamics, pharmacokinetics and clinical
efficacy of neratinib in HER2-positive breast cancer and breast
cancer with HER2 mutations. Expert Opin Drug Metab Toxicol.
12:947–957. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Chan A: Neratinib in HER-2-positive breast
cancer: Results to date and clinical usefulness. Ther Adv Med
Oncol. 8:339–350. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Kourie HR, El Rassy E, Clatot F, de
Azambuja E and Lambertini M: Emerging treatments for HER2-positive
early-stage breast cancer: Focus on neratinib. Onco Targets Ther.
10:3363–3372. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Chan A, Delaloge S, Holmes FA, Moy B,
Iwata H, Harvey VJ, Robert NJ, Silovski T, Gokmen E, von Minckwitz
G, et al: Neratinib after trastuzumab-based adjuvant therapy in
patients with HER2-positive breast cancer (ExteNET): A multicentre,
randomised, double-blind, placebo-controlled, phase 3 trial. Lancet
Oncol. 17:367–377. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Tian C, Ding P, Yuan Z, Li H, Zhao Y, Sun
L, Guo Q, Wang Z, Sun L, Zhang L and Jiang Z: A novel dual
EGFR/HER2 inhibitor KU004 induces cell cycle arrest and apoptosis
in HER2-overexpressing cancer cells. Apoptosis. 20:1599–1612. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Choi YJ, Li X, Hydbring P, Sanda T,
Stefano J, Christie AL, Signoretti S, Look AT, Kung AL, von Boehmer
H and Sicinski P: The requirement for cyclin D function in tumor
maintenance. Cancer Cell. 22:438–451. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Yu Q, Geng Y and Sicinski P: Specific
protection against breast cancers by cyclin D1 ablation. Nature.
411:1017–1021. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Iwata H: Clinical development of CDK4/6
inhibitor for breast cancer. Breast Cancer. 25:402–406. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Walker AJ, Wedam S, Amiri-Kordestani L,
Bloomquist E, Tang S, Sridhara R, Chen W, Palmby TR, Fourie
Zirkelbach J, Fu W, et al: FDA approval of palbociclib in
combination with fulvestrant for the treatment of hormone
receptor-positive, HER2-negative metastatic breast cancer. Clin
Cancer Res. 22:4968–4972. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Kwapisz D: Cyclin-dependent kinase 4/6
inhibitors in breast cancer: Palbociclib, ribociclib, and
abemaciclib. Breast Cancer Res Treat. 166:41–54. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Gianni L, Bisagni G, Colleoni M, Del
Mastro L, Zamagni C, Mansutti M, Zambetti M, Frassoldati A, De Fato
R, Valagussa P and Viale G: Neoadjuvant treatment with trastuzumab
and pertuzumab plus palbociclib and fulvestrant in HER2-positive,
ER-positive breast cancer (NA-PHER2): An exploratory, open-label,
phase 2 study. Lancet Oncol. 19:249–256. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Witkiewicz AK, Cox D and Knudsen ES:
CDK4/6 inhibition provides a potent adjunct to Her2-targeted
therapies in preclinical breast cancer models. Genes Cancer.
5:261–272. 2014.PubMed/NCBI
|
|
84
|
Goel S, Wang Q, Watt AC, Tolaney SM,
Dillon DA, Li W, Ramm S, Palmer AC, Yuzugullu H, Varadan V, et al:
Overcoming therapeutic resistance in HER2-positive breast cancers
with CDK4/6 inhibitors. Cancer Cell. 29:255–269. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Sievers EL and Senter PD: Antibody-drug
conjugates in cancer therapy. Annu Rev Med. 64:15–29. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Lianos GD, Vlachos K, Zoras O, Katsios C,
Cho WC and Roukos DH: Potential of antibody-drug conjugates and
novel therapeutics in breast cancer management. Onco Targets Ther.
7:491–500. 2014.PubMed/NCBI
|
|
87
|
Padayachee ER, Biteghe FAN, Malindi Z,
Bauerschlag D and Barth S: Human antibody fusion proteins/antibody
drug conjugates in breast and ovarian cancer. Transfus Med
Hemother. 44:303–310. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Li JY, Perry SR, Muniz-Medina V, Wang X,
Wetzel LK, Rebelatto MC, Hinrichs MJ, Bezabeh BZ, Fleming RL,
Dimasi N, et al: A biparatopic HER2-targeting antibody-drug
conjugate induces tumor regression in primary models refractory to
or ineligible for HER2-targeted therapy. Cancer Cell. 29:117–129.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Tsui FW, Martin A, Wang J and Tsui HW:
Investigations into the regulation and function of the SH2
domain-containing protein-tyrosine phosphatase, SHP-1. Immunol Res.
35:127–136. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Liu CY, Chen KF, Chao TI, Chu PY, Huang
CT, Huang TT, Yang HP, Wang WL, Lee CH, Lau KY, et al: Sequential
combination of docetaxel with a SHP-1 agonist enhanced suppression
of p-STAT3 signaling and apoptosis in triple negative breast cancer
cells. J Mol Med (Berl). 95:965–975. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Liu CY, Tseng LM, Su JC, Chang KC, Chu PY,
Tai WT, Shiau CW and Chen KF: Erratum to: Novel sorafenib analogues
induce apoptosis through SHP-1 dependent STAT3 inactivation in
human breast cancer cells. Breast Cancer Res. 19:52017. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Wu Y, Li R, Zhang J, Wang G, Liu B, Huang
X, Zhang T and Luo R: Protein tyrosine phosphatase SHP-1 sensitizes
EGFR/HER-2 positive breast cancer cells to trastuzumab through
modulating phosphorylation of EGFR and HER-2. Onco Targets Ther.
8:2577–2587. 2015.PubMed/NCBI
|
|
93
|
Puig T, Turrado C, Benhamú B, Aguilar H,
Relat J, Ortega-Gutiérrez S, Casals G, Marrero PF, Urruticoechea A,
Haro D, et al: Novel inhibitors of fatty acid synthase with
anticancer activity. Clin Cancer Res. 15:7608–7615. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Grunt TW, Wagner R, Grusch M, Berger W,
Singer CF, Marian B, Zielinski CC and Lupu R: Interaction between
fatty acid synthase- and ErbB-systems in ovarian cancer cells.
Biochem Biophys Res Commun. 385:454–459. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Menendez JA and Lupu R: Fatty acid
synthase (FASN) as a therapeutic target in breast cancer. Expert
Opin Ther Targets. 21:1001–1016. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Hayward SL, Francis DM, Kholmatov P and
Kidambi S: Targeted delivery of MicroRNA125a-5p by engineered lipid
nanoparticles for the treatment of HER2 positive metastatic breast
cancer. J Biomed Nanotechnol. 12:554–568. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Campbell DF, Saenz R, Bharati IS, Seible
D, Zhang L, Esener S, Messmer B, Larsson M and Messmer D: Enhanced
anti-tumor immune responses and delay of tumor development in human
epidermal growth factor receptor 2 mice immunized with an
immunostimulatory peptide in poly(D,L-lactic-co-glycolic) acid
nanoparticles. Breast Cancer Res. 17:482015. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Li J, Wang F, Sun D and Wang R: A review
of the ligands and related targeting strategies for active
targeting of paclitaxel to tumours. J Drug Target. 24:590–602.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Chandrika BB, Steephan M, Kumar TR, Sabu A
and Haridas M: Hesperetin and naringenin sensitize HER2 positive
cancer cells to death by serving as HER2 tyrosine kinase
inhibitors. Life Sci. 160:47–56. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Nishio S, Ushijima K, Yamaguchi T,
Sasajima Y, Tsuda H, Kasamatsu T, Kage M, Ono M, Kuwano M and
Kamura T: Nuclear Y-box-binding protein-1 is a poor prognostic
marker and related to epidermal growth factor receptor in uterine
cervical cancer. Gynecol Oncol. 132:703–708. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
He L, Che M, Hu J, Li S, Jia Z, Lou W, Li
C, Yang J, Sun S, Wang H and Chen X: Twist contributes to
proliferation and epithelial-to-mesenchymal transition-induced
fibrosis by regulating YB-1 in human peritoneal mesothelial cells.
Am J Pathol. 185:2181–2193. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Ma JW, Hung CM, Lin YC, Ho CT, Kao JY and
Way TD: Aloe-emodin inhibits HER-2 expression through the
downregulation of Y-box binding protein-1 in HER-2-overexpressing
human breast cancer cells. Oncotarget. 7:58915–58930.
2016.PubMed/NCBI
|
|
103
|
Housa D, Housová J, Vernerová Z and
Haluzík M: Adipocytokines and cancer. Physiol Res. 55:233–244.
2006.PubMed/NCBI
|
|
104
|
Vona-Davis L and Rose DP: Adipokines as
endocrine, paracrine, and autocrine factors in breast cancer risk
and progression. Endocr Relat Cancer. 14:189–206. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Provatopoulou X, Georgiou GP, Kalogera E,
Kalles V, Matiatou MA, Papapanagiotou I, Sagkriotis A, Zografos GC
and Gounaris A: Serum irisin levels are lower in patients with
breast cancer: Association with disease diagnosis and tumor
characteristics. BMC Cancer. 15:8982015. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Shukla S, Bhaskaran N, Babcook MA, Fu P,
Maclennan GT and Gupta S: Apigenin inhibits prostate cancer
progression in TRAMP mice via targeting PI3K/Akt/FoxO pathway.
Carcinogenesis. 35:452–460. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Seo HS, Ju JH, Jang K and Shin I:
Induction of apoptotic cell death by phytoestrogens by
up-regulating the levels of phospho-p53 and p21 in normal and
malignant estrogen receptor α-negative breast cells. Nutr Res.
31:139–146. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Seo HS, Jo JK, Ku JM, Choi HS, Choi YK,
Woo JK, Kim HI, Kang SY, Lee KM, Nam KW, et al: Induction of
caspase-dependent extrinsic apoptosis by apigenin through
inhibition of signal transducer and activator of transcription 3
(STAT3) signalling in HER2-overexpressing BT-474 breast cancer
cells. Biosci Rep. 35(pii): e002762015. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Liu Q, Xu X, Zhao M, Wei Z, Li X, Zhang X,
Liu Z, Gong Y and Shao C: Berberine induces senescence of human
glioblastoma cells by downregulating the EGFR-MEK-ERK signaling
pathway. Mol Cancer Ther. 14:355–363. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Chu SC, Yu CC, Hsu LS, Chen KS, Su MY and
Chen PN: Berberine reverses epithelial-to-mesenchymal transition
and inhibits metastasis and tumor-induced angiogenesis in human
cervical cancer cells. Mol Pharmacol. 86:609–623. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Pierpaoli E, Damiani E, Orlando F,
Lucarini G, Bartozzi B, Lombardi P, Salvatore C, Geroni C, Donati A
and Provinciali M: Antiangiogenic and antitumor activities of
berberine derivative NAX014 compound in a transgenic murine model
of HER2/neu-positive mammary carcinoma. Carcinogenesis.
36:1169–1179. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Guerram M, Jiang ZZ, Yousef BA, Hamdi AM,
Hassan HM, Yuan ZQ, Luo HW, Zhu X and Zhang LY: The potential
utility of acetyltanshinone IIA in the treatment of
HER2-overexpressed breast cancer: Induction of cancer cell death by
targeting apoptotic and metabolic signaling pathways. Oncotarget.
6:21865–21877. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Tian HL, Yu T, Xu NN, Feng C, Zhou LY, Luo
HW, Chang DC, Le XF and Luo KQ: A novel compound modified from
tanshinone inhibits tumor growth in vivo via activation of the
intrinsic apoptotic pathway. Cancer Lett. 297:18–30. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Guan YQ, Li Z and Liu JM: Death signal
transduction induced by co-immobilized TNF-α plus IFN-γ and the
development of polymeric anti-cancer drugs. Biomaterials.
31:9074–9085. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Namjoshi P, Showalter L, Czerniecki BJ and
Koski GK: T-helper 1-type cytokines induce apoptosis and loss of
HER-family oncodriver expression in murine and human breast cancer
cells. Oncotarget. doi.org/10.18632/oncotarget.10298.
|
|
116
|
Mittal D, Caramia F, Michiels S, Joensuu
H, Kellokumpu-Lehtinen PL, Sotiriou C, Loi S and Smyth MJ: Improved
treatment of breast cancer with anti-HER2 therapy requires
interleukin-21 signaling in CD8+ T cells. Cancer Res. 76:264–274.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Hung SW, Chiu CF, Chen TA, Chu CL, Huang
CC, Shyur LF, Liang CM and Liang SM: Recombinant viral protein VP1
suppresses HER-2 expression and migration/metastasis of breast
cancer. Breast Cancer Res Treat. 136:89–105. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Takai N and Narahara H: Human endometrial
and ovarian cancer cells: Histone deacetylase inhibitors exhibit
antiproliferative activity, potently induce cell cycle arrest, and
stimulate apoptosis. Curr Med Chem. 14:2548–2553. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Travaglini L, Vian L, Billi M, Grignani F
and Nervi C: Epigenetic reprogramming of breast cancer cells by
valproic acid occurs regardless of estrogen receptor status. Int J
Biochem Cell Biol. 41:225–234. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Zhang L, Wang G, Wang L, Song C, Leng Y,
Wang X and Kang J: VPA inhibits breast cancer cell migration by
specifically targeting HDAC2 and down-regulating Survivin. Mol Cell
Biochem. 361:39–45. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Hrzenjak A, Moinfar F, Kremser ML,
Strohmeier B, Staber PB, Zatloukal K and Denk H: Valproate
inhibition of histone deacetylase 2 affects differentiation and
decreases proliferation of endometrial stromal sarcoma cells. Mol
Cancer Ther. 5:2203–2210. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Rocchi P, Tonelli R, Camerin C, Purgato S,
Fronza R, Bianucci F, Guerra F, Pession A and Ferreri AM:
p21Waf1/Cip1 is a common target induced by short-chain fatty acid
HDAC inhibitors (valproic acid, tributyrin and sodium butyrate) in
neuroblastoma cells. Oncol Rep. 13:1139–1144. 2005.PubMed/NCBI
|
|
123
|
Mawatari T, Ninomiya I, Inokuchi M, Harada
S, Hayashi H, Oyama K, Makino I, Nakagawara H, Miyashita T, Tajima
H, et al: Valproic acid inhibits proliferation of HER2-expressing
breast cancer cells by inducing cell cycle arrest and apoptosis
through Hsp70 acetylation. Int J Oncol. 47:2073–2081. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Kim J, Kundu M, Viollet B and Guan KL:
AMPK and mTOR regulate autophagy through direct phosphorylation of
Ulk1. Nat Cell Biol. 13:132–141. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Fan QW, Cheng C, Hackett C, Feldman M,
Houseman BT, Nicolaides T, Haas-Kogan D, James CD, Oakes SA,
Debnath J, et al: Akt and autophagy cooperate to promote survival
of drug-resistant glioma. Sci Signal. 3:ra812010. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Fritsch C, Huang A, Chatenay-Rivauday C,
Schnell C, Reddy A, Liu M, Kauffmann A, Guthy D, Erdmann D, De
Pover A, et al: Characterization of the novel and specific PI3Kα
inhibitor NVP-BYL719 and development of the patient stratification
strategy for clinical trials. Mol Cancer Ther. 13:1117–1129. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Young CD, Arteaga CL and Cook RS: Dual
inhibition of Type I and Type III PI3 kinases increases tumor cell
apoptosis in HER2+ breast cancers. Breast Cancer Res. 17:1482015.
View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Salmaninejad A, Khoramshahi V, Azani A,
Soltaninejad E, Aslani S, Zamani MR, Zal M, Nesaei A and Hosseini
SM: PD-1 and cancer: Molecular mechanisms and polymorphisms.
Immunogenetics. 70:73–86. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Berger KN and Pu JJ: PD-1 pathway and its
clinical application: A 20year journey after discovery of the
complete human PD-1 gene. Gene. 638:20–25. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Kythreotou A, Siddique A, Mauri FA, Bower
M and Pinato DJ: PD-L1. J Clin Pathol. 71:189–194. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
Hartkopf AD, Taran FA, Wallwiener M,
Walter CB, Krämer B, Grischke EM and Brucker SY: PD-1 and PD-L1
immune checkpoint blockade to treat breast cancer. Breast Care
(Basel). 11:385–390. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Schütz F, Stefanovic S, Mayer L, von Au A,
Domschke C and Sohn C: PD-1/PD-L1 pathway in breast cancer. Oncol
Res Treat. 40:294–297. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Tsang JY, Au WL, Lo KY, Ni YB, Hlaing T,
Hu J, Chan SK, Chan KF, Cheung SY and Tse GM: PD-L1 expression and
tumor infiltrating PD-1+ lymphocytes associated with outcome in
HER2+ breast cancer patients. Breast Cancer Res Trea. 162:19–30.
2017. View Article : Google Scholar
|
|
134
|
Hou Y, Nitta H, Wei L, Banks PM, Parwani
AV and Li Z: Evaluation of immune reaction and PD-L1 expression
using multiplex immunohistochemistry in HER2-positive breast
cancer: The association with response to Anti-HER2 neoadjuvant
therapy. Clin Breast Cancer. 18:e237–e244. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Dirix LY, Takacs I, Jerusalem G,
Nikolinakos P, Arkenau HT, Forero-Torres A, Boccia R, Lippman ME,
Somer R, Smakal M, et al: Avelumab, an anti-PD-L1 antibody, in
patients with locally advanced or metastatic breast cancer: A phase
1b JAVELIN solid tumor study. Breast Cancer Res Treat. 167:671–686.
2018. View Article : Google Scholar : PubMed/NCBI
|