Introduction
The incidence of endometriosis (EMS) has increased
in recent years, and has become one of the most common
gynecological diseases affecting numerous women at childbearing age
(1). The present treatment method
for EMS mainly includes hormone therapy and surgery since the
efficacy of drug treatment is not ideal and the disease easily
recurs (2). Somatostatin (SS) is a
peptide hormone with extensive physiological effects. It is a
natural polypeptide hormone containing 14 or 28 amino acids, which
widely occurs in human endocrine and exocrine systems, and has
extensive biological effects, which are mainly inhibitory (3). SS and its analogues have been used to
treat neurological diseases, including Alzheimer's disease, chorea
and epilepsy, tumor types, including pituitary, pancreatic islet
cell and carcinoid tumor; and certain gastrointestinal diseases,
including gastric ulcer, stomach bleeding and digestive tract
ulcer, acute pancreatitis and bleeding from esophageal varices
(4–6). The physiological functions of SS
include hormone regulation, inhibition of cell proliferation,
neurotransmitter release, inhibition of gastric acid, secretion of
pepsin and gastrin, reduction of splanchnic blood flow, as well as
the inhibition of the release of insulin-like growth factor
(IGF)-1, platelet-derived growth factor, epidermal growth factor,
white blood cell interleukin (IL)-6 and interferon (IFN)-γ
(4,7).
Numerous studies have indicated that SS inhibits the
proliferation of tumor cells (8,9). It acts
by binding to specific cell surface receptors, SS receptors
(SSTRs), which occurs as 5 SSTR subtypes named as SSTR1-5 (10). SSTR exists in a wide variety of
neuroendocrine tumors and tumors of the nervous system (11). Certain studies have reported the
expression of SSTR in endometrial and ovarian cancer (12,13).
However, few studies have focused on the expression of SSTR in EMS
lesions. The present study was designed to detect the expression of
the SS and SSTR1-5 genes in EMS tissue and its association with the
disease.
Materials and methods
Tissue samples
The EMS tissues and cells were extracted from 30
female patients during gynecological laparotomy or laparoscopic
surgeries at the Department of Obstetrics and Gynecology, Xiangya
Hospital of Central South University (Changsha, China) between July
2009 and December 2012. The specimens included cystic walls from 28
cases with ovarian chocolate cyst and samples from 2 patients with
pelvic peritoneal EMS. Specimens were confirmed by the Department
of Pathology of Central South University, fixed with 10% formalin
and embedded in common paraffin. The patients had no particular
disease history, had not received any hormone therapy
pre-operatively within 3 months, and were aged between 20 and 45
years (mean age, 35.68 years). The patients were staged in line
with the Revised American Fertility Society I system (14): 2 Patients were stage I, 7 cases were
stage II, 16 cases were stage III and 5 cases were stage IV. The
eutopic endometrium was derived from 12 additional EMS patients
undergoing gynecologic abdominal hysterectomy or uterine
laparoscopy between July 2009 and December 2012 in the Department
of Obstetrics and Gynecology of Xiangya Hospital of Central South
University, all samples were endometrium at the proliferative
phase, and the average age of the donors was 40.52 years. A total
of 14 specimens for the control group were collected from cervical
intraepithelial neoplasia (CIN) patients undergoing surgical
resection with normal endometrium between July 2009 and December
2012 in the Department of Obstetrics and Gynecology of Xiangya
Hospital of Central South University, all samples were endometrium
at the proliferative phase, the age of the patients was 40–48
years, and their average age was 45.18 years. The present study was
approved by Ethics Committee of Xiangya Hospital of Central South
University and informed consent was obtained from all subjects.
Cell sources
Normal endometrium (NE) cells were obtained from 15
healthy females of childbearing age undergoing curettage at the
outpatient department of Xiangya Hospital of Central South
University between September 2012 and April 2013. The ectopic
endometrial (EE) cells were obtained from 15 hospitalized patients
undergoing ovarian EMS cyst or laparoscopic surgery at the same
time. The specimens were collected from a 0.5–1 mm-thick portion in
the inner cystic walls from ovarian chocolate cysts. The mean age
in the two groups was 30.25±4.35 and 32.05±5.29 years, respectively
(P>0.05). None of the patients had any tumors or any endocrine,
immune or metabolic diseases and no hormonal drugs had been
administered within 3 months. No pathological change was found in
the NE group on histological examination. The histological staging
was consistent with the actual menstrual cycle, and ovarian EMS
cyst was diagnosed in EE cell group.
Reagents
Primary antibodies against SSTR1 (cat. no. BA1405;
1:100) and SSTR3 (cat. no. BA1407; 1:100) were purchased from
(Wuhan Boster Biological Technology, Co., Ltd., Wuhan, China).
Primary antibodies of SSTR2 (cat. no. ab134152; 1:100), SSTR4 (cat.
no. ab28578; 1:2,500) and SSTR5 (cat. no. ab109495; 1:100) were
purchased from Abcam (Cambridge, MA, USA). Dulbecco's modified
Eagle's medium (DMEM)/F12 was purchased from Beijing Dingguo
Biotechnology Co., Ltd (Beijing, China), fetal bovine serum was
purchased from Shanghai Sijiqing Co., Ltd (Shanghai, China) and
collagenase IV and trypsin were purchased from Sigma-Aldrich (Merck
KGaA, Darmstadt, Germany).
Cell separation and culture
To establish in vitro cultures, the method
reported previously was used (4,7), with
certain modifications: The obtained tissues were washed three times
with PBS, dissected it into 0.5–1 mm3 pieces and placed
in a 20-ml centrifugal tube. Following addition of 2.5–5.0 volumes
of 0.1% collagenase and 0.25% trypsin digestion solution and even
mixing, the samples were incubated in a water bath at 37°C with
continuous agitation for 50–100 min in NE group and 80–120 min in
the EE group. Subsequently, DMEM was added to stop the digestion,
followed by repeated pipetting of the samples. The cells were then
filtered through a 100-mesh stainless steel net. The filtrate,
mainly containing the mesenchymal and epithelial cells, was
centrifuged at 170 × g for 10 min, the supernatant was removed, and
the pellet was resuspended in DMEM/F12 with 15% fetal bovine serum,
and after the cell count was determined under trypan blue staining,
the cell concentration in the suspension was adjusted to
5×105 cells/ml. The cells were inoculated into a culture
dish and cultured in an incubator with 5% CO2 at 37°C
with the medium replaced once every 2–3 days until cell convergence
was reached in the primary culture. The cell shapes and growth were
observed with an inverted microscope and images were captured.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
The PCR primers were designed based on the human SS
mRNA sequences from GenBank, and GAPDH was used as a control. The
primers were synthesized by Nanjing GenScript Biotechnical Co., Ltd
(Nanjing, China) and had the following sequences (in 5′-3′
direction): SS upstream, GCTGCTGTCTGAACCC and downstream,
CGTTCTCGGGGTGCCATAG (product length, 138 bp); GAPDH upstream,
TGCACCACCAACTGC and downstream, GGCATGGACTGTGGTCATGAG (product
length, 87 bp). Total RNA was extracted using TRIZOL reagent
(Invitrogen; Thermo Fisher Scientific, Inc., Waltham, MA, USA)
according to the manufacturer's protocol. A cDNA Reverse
Transcription lit (Applied Biosystems; Thermo Fisher Scientific,
Inc.) was used for reverse transcription. Briefly, 3 µg total RNA
(0.5 µg/µl), 1 µl Oligo dT Primer, 1 µl dNTP Mixture (both Takara
Biotechnology Co., Ltd., Dalian, China) and RNase-free doubly
distilled (dd)H2O (Beijing Solarbio Science &
Technology Co., Ltd., Beijing, China) were mixed with the total
mixture of 10 µl. The mixture was stirred at 70°C for 5 min and
then the 10 µl mixture, 4 µl 5X PrimeScript II Buffer, 0.5 µl RNase
inhibitor, 1 µl PrimeScript II RTase and 4.5 µl RNase-free
ddH2O were mixed followed by a reaction at 45°C for 45
min and 95°C for 5 min. PCR was performed on a
Mastercycler® RealPlex2 thermal cycler
(Eppendorf, Hamburg, Germany) and data were analyzed by MxPro
software (version 4.0; (Stratagene; Agilent Technologies, Inc.,
Santa Clara, CA, USA). The reaction system (18 µl) comprised
diethyl pyrocarbonate-treated H2O (3.6 µl), 1.2 µl of a
10-µM solution of each primer, 10 µl SYBR® Green
Realtime PCR Master Mix and 2 µl complementary DNA. Each condition
was performed in 3 parallel wells. The following thermocycling
program was used: 95°C for 10 min, followed by 42 cycles of 95°C
for 30 sec and 58°C for 20 sec, and 72°C for 30 sec. Following
determination of the ΔCq value, the relative expression level of
the target mRNA was calculated. Using GAPDH as an internal
reference, the relative changes in gene expression were calculated
as 2−ΔΔCq (15).
Immunohistochemical method
Samples were prepared according to the protocol of
immunohistochemical staining kit (SA1098; Wuhan Boster Biological
Technology, Co., Ltd.) using the streptavidin-biotin complex
approach. A negative control was prepared by using PBS instead of
primary antibody and normal endometrial tissues sections were used
as positive controls. Following incubation, DAB regent (AR1025;
Wuhan Boster Biological Technology, Co., Ltd.) was used for further
staining; samples were incubated with DAB reagent at room
temperature for 5 min. The film was read by blinded observers under
a light microscope. Yellow or brown staining indicated positive
results. Brown or yellow granules indicating SSTR staining were
mainly localized in the cytoplasm, and the expression of SSTR was
determined by using a quantitative method. The scores were summed
up based on the coloring depth and the positive cell numbers, where
0 indicated positive staining, 1 light brown staining, 2 dark brown
staining and 3 tan staining. A total of 10 high-magnification
fields of view were counted per sample to determine the positive
rates and the average was determined. The score(s) for the
proportion of cells with positive staining were as follows: 0,
<5%; 1, 5–24%; 2, 25–49%; 3, 50–74% and 4, ≥75%. The scores for
staining intensity and proportion of stained cells were multiplied
and patients with a score of <1 were considered as negative,
while the remaining patients were considered as positive. A score
of 1–3 indicated weakly positive (+), 4 and 5 indicated positive
(+) and ≥6 indicated highly positive (++) staining.
Statistical methods
Values are expressed as the mean ± standard
deviation. Comparison between two groups was performed using
Student's t-test. Comparison of rates was performed using the
Chi-square test. P<0.05 was considered to indicate a
statistically significant difference. All calculations were
performed using SPSS 19.0 (IBM Corp., Armonk, NY, USA).
Results
Expression of SS mRNA in the different
groups
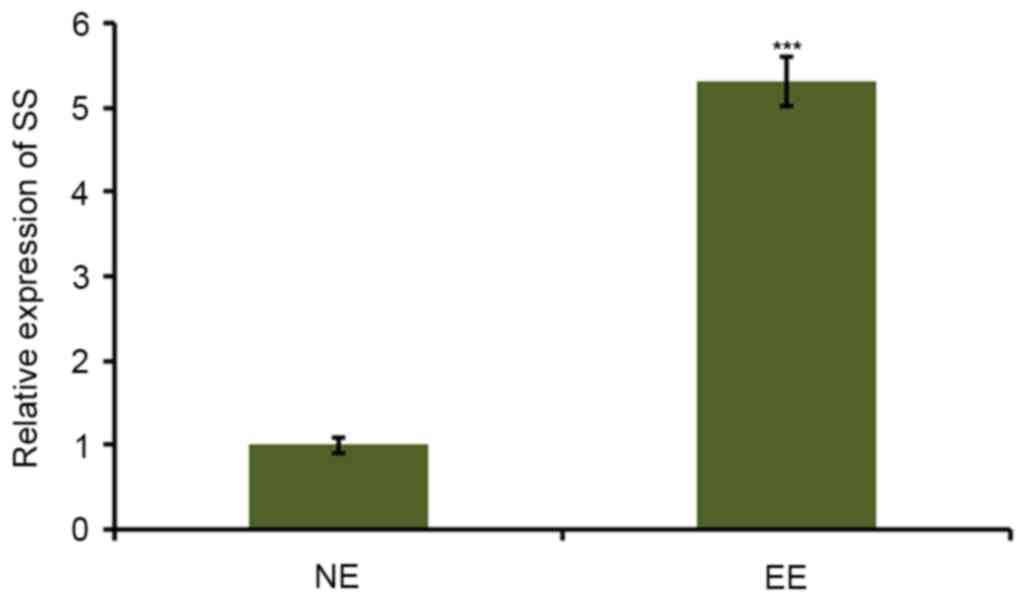
The relative expression of SS mRNA in the cells of
the EE and NE groups was automatically output by MxPro software
(Fig. 1). Results demonstrated that
the expression of SS was significantly higher in the EE group
compared with that in the NE group (P<0.05).
Expression of SSTR subtypes in EMS
tissues
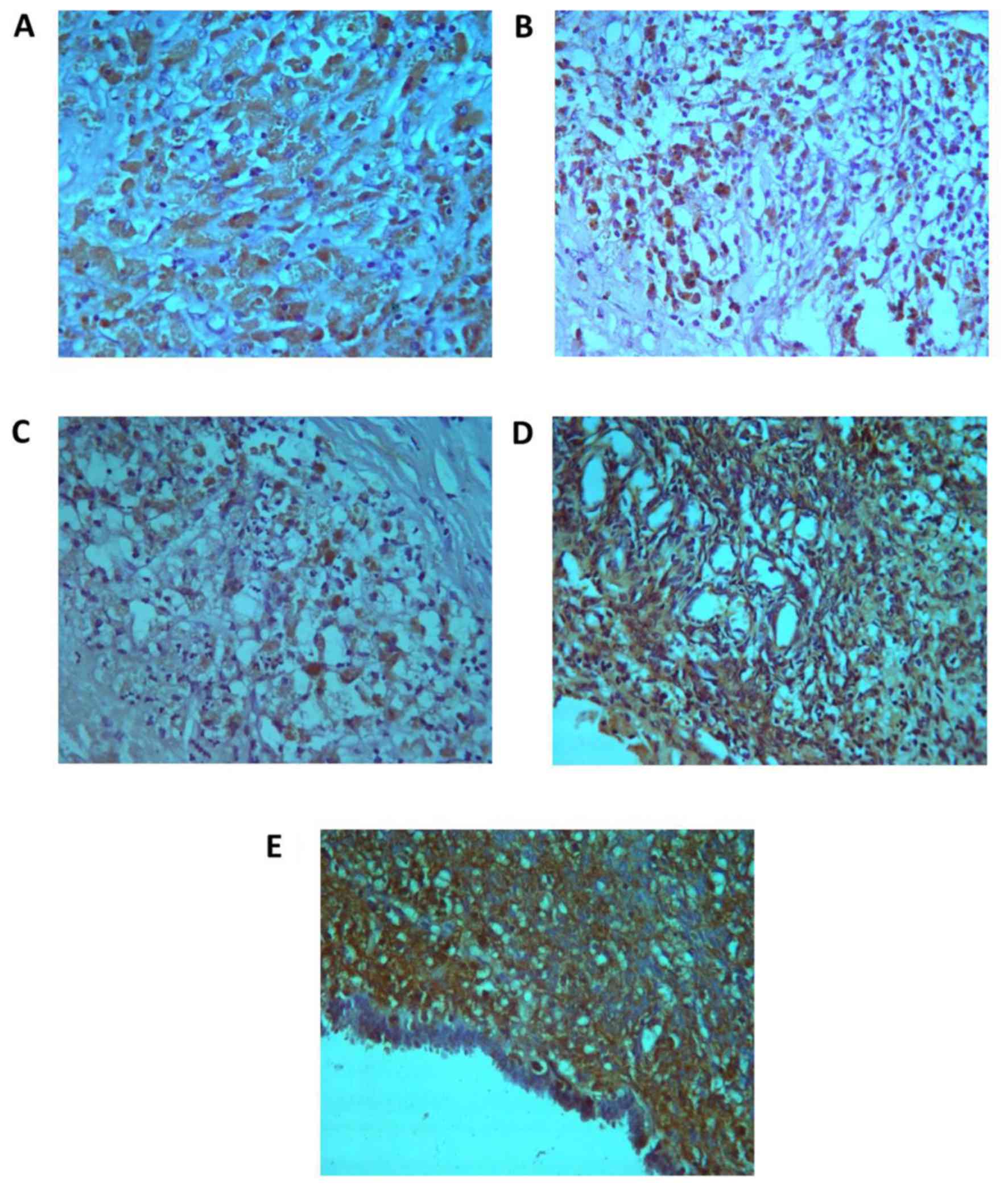
Immunohistochemical analysis revealed that in
ectopic endometrial cells, SSTR was mostly located in the cytoplasm
and cell membrane. Among the 30 cases of EMS, expression of SSTR1
was present in EMS cells of 13 patients (43.3%), SSTR2 in those of
21 patients (70%), SSTR3 in 16 (53.5%), SSTR4 in 15 (50%) and SSTR5
was expressed in EMS cells of 29 patients (96.7%; Fig. 2 and Table
I). Compared with the positive expression rate in the control
group (the NS cells), the expression rate of SSTR1, SSTR2, SSTR3
and SSTR5 was significantly increased in the EMS group (P<0.05;
Table II). In EMS tissue, the
expression of SSTR subtypes and the clinical stage were
significantly associated (P<0.001; Table I).
 | Table I.Positive rate of expression of SSTR
subtypes in endometriotic tissues and its association with clinical
staging. |
Table I.
Positive rate of expression of SSTR
subtypes in endometriotic tissues and its association with clinical
staging.
|
|
| Clinical stage, n
(%) |
|
|---|
|
|
|
|
|
|---|
| Expression
status/rate | N (%) | I | II | III | IV | P-value |
|---|
| SSTR1 |
|
|
|
|
|
|
|
Positive | 13 (43.3) | 0 (0) | 2 (15.38) | 7 (53.85) | 4 (30.77) | <0.001 |
|
Negative | 17 | 1 (5.88) | 5 (29.41) | 10 (58.82) | 1 (5.88) |
|
| SSTR2 |
|
|
|
|
|
|
|
Positive | 21 (70) | 0 (0) | 5 (23.81) | 11 (52.38) | 5 (23.81) | <0.001 |
|
Negative | 9 | 1 (11.11) | 2 (22.22) | 7 (77.77) | 0 (0) |
|
| SSTR3 |
|
|
|
|
|
|
|
Positive | 16 (53.3) | 1 (6.25) | 3 (18.75) | 3 (18.75) | 9 (56.25) | <0.001 |
|
Negative | 14 | 1 (7.14) | 4 (28.57) | 7 (50.00) | 2 (14.29) |
|
| SSTR4 |
|
|
|
|
|
|
|
Positive | 15 (50.0) | 0 (0) | 1 (6.67) | 10 (66.67) | 4 (26.67) | <0.001 |
|
Negative | 15 | 2 (13.33) | 6 (40.00) | 6 (40.00) | 1 (6.67) |
|
| SSTR5 |
|
|
|
|
|
|
|
Positive | 29 (96.7) | 2 (6.90) | 6 (20.69) | 16 (55.17) | 5 (17.24) | <0.001 |
|
Negative | 1 | 0 (0) | 1 (100.00) | 0 (0) | 0 (0) |
|
| Table II.Expression of SSTR subtypes in
endometrial tissues of ectopic (n=30), eutopic (n=12) and control
endometrium (n=14) groups. |
Table II.
Expression of SSTR subtypes in
endometrial tissues of ectopic (n=30), eutopic (n=12) and control
endometrium (n=14) groups.
|
| Immunohistochemical
staining (n) |
|
|
|---|
|
|
|
|
|
|---|
| Group/subtype | − | +− | + | ++ | Positive rate
(%) |
P-valuea |
|---|
| Control |
|
|
|
|
|
|
|
SSTR1 | 13 | 1 | 0 | 0 | 7.1 |
|
|
SSTR2 | 13 | 1 | 0 | 0 | 7.1 |
|
|
SSTR3 | 11 | 2 | 1 | 0 | 21.4 |
|
|
SSTR4 | 10 | 2 | 2 | 0 | 28.6 |
|
|
SSTR5 | 6 | 4 | 3 | 1 | 64.3 |
|
| Eutopic
endometrium |
|
|
|
|
|
|
|
SSTR1 | 8 | 2 | 2 | 0 | 33.3 | <0.001 |
|
SSTR2 | 7 | 3 | 2 | 0 | 41.7 | <0.001 |
|
SSTR3 | 5 | 4 | 2 | 1 | 58.3 | <0.001 |
|
SSTR4 | 5 | 5 | 1 | 1 | 58.3 | <0.001 |
|
SSTR5 | 2 | 4 | 4 | 2 | 83.3 | 0.002 |
| Ectopic
endometrium |
|
|
|
|
|
|
|
SSTR1 | 17 | 6 | 4 | 3 | 43.3 | <0.001 |
|
SSTR2 | 9 | 11 | 6 | 4 | 70.0 | <0.001 |
|
SSTR3 | 14 | 7 | 6 | 3 | 53.3 | <0.001 |
|
SSTR4 | 15 | 8 | 5 | 2 | 50.0 | 0.002 |
|
SSTR5 | 1 | 6 | 14 | 9 | 96.7 | <0.001 |
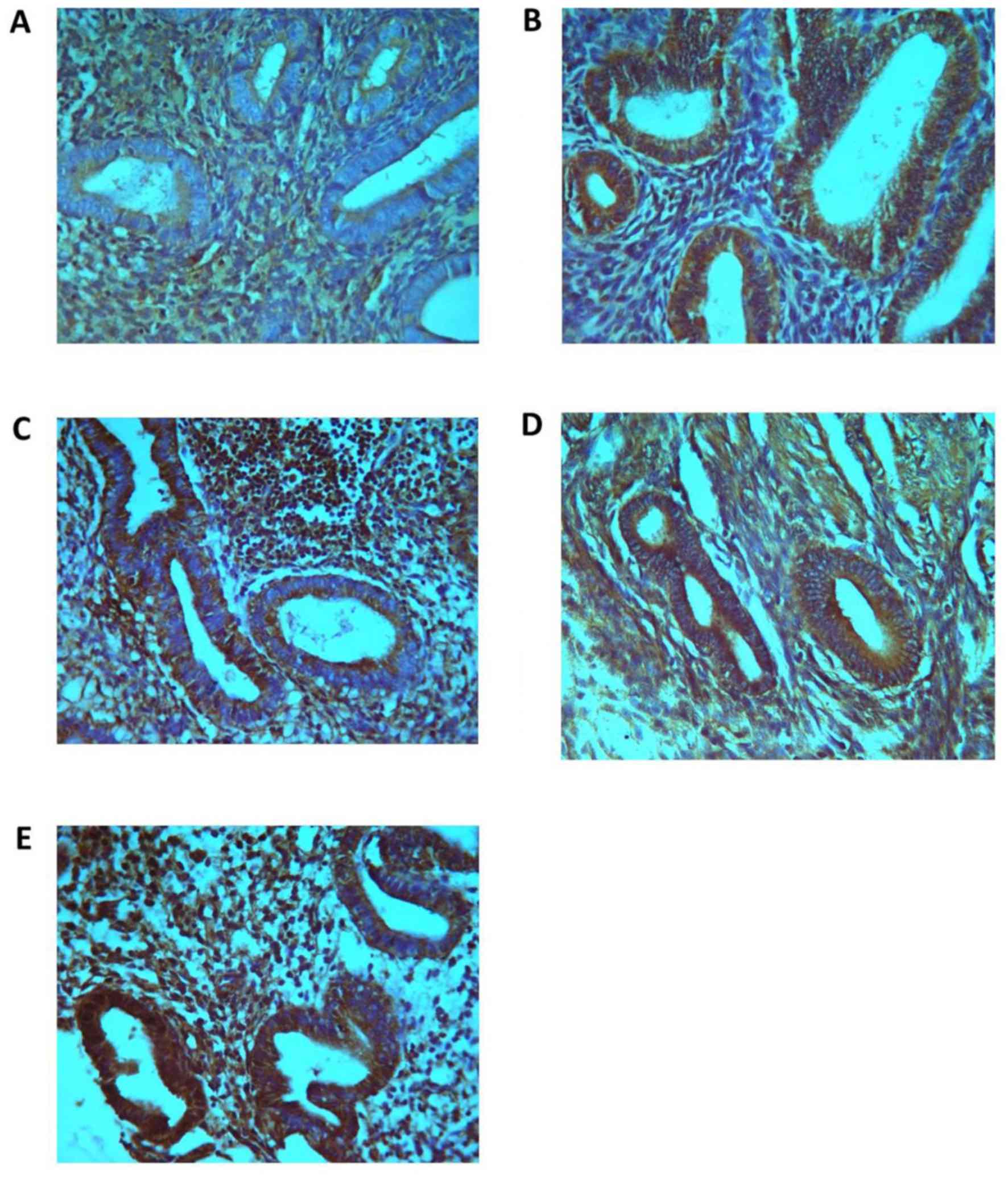
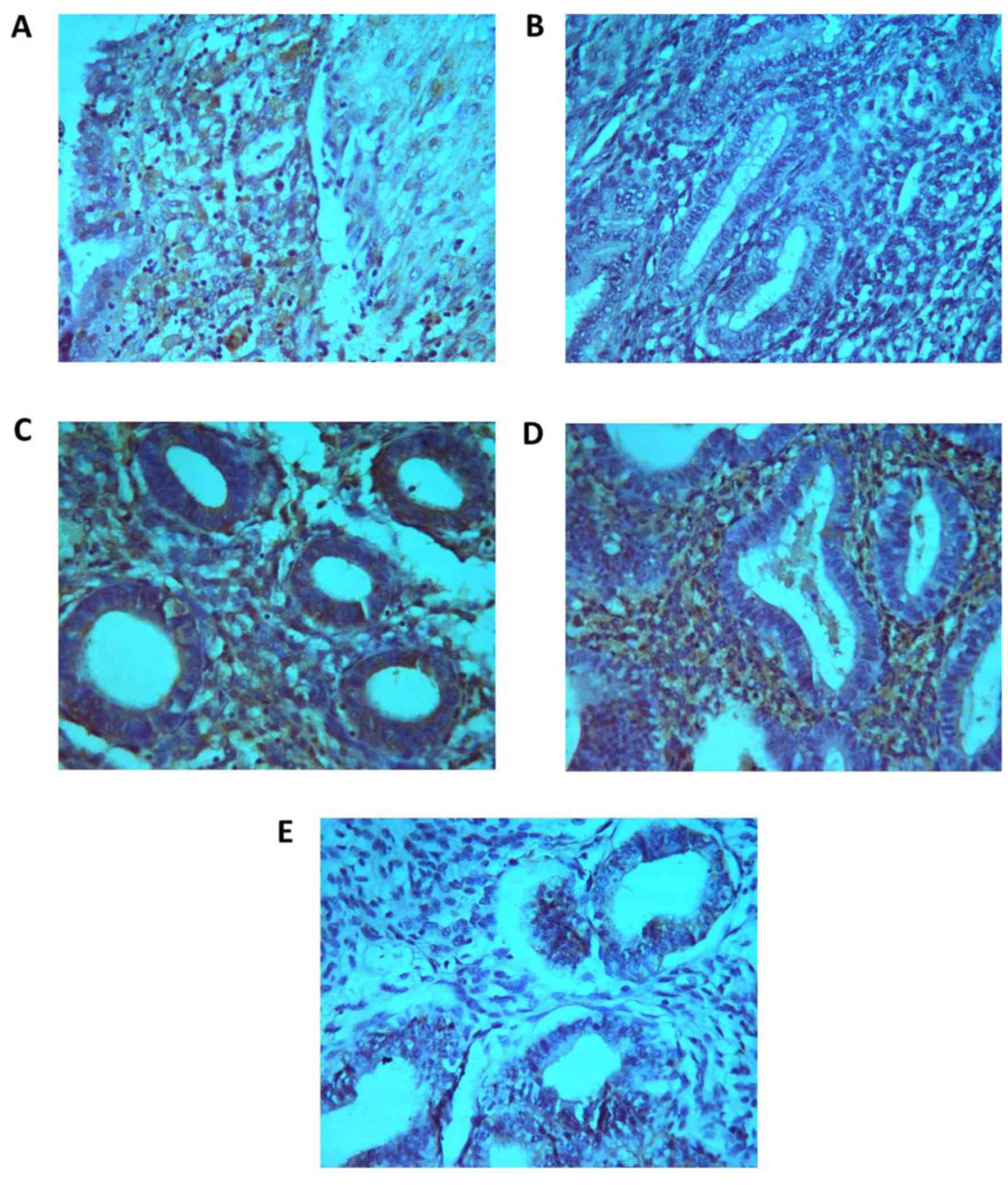
Expression of SSTR subtypes in eutopic
and ectopic endometrial tissues in the EMS and normal control
group
The positive expression rates of SSTR1-5 in eutopic
endometrium from 12 cases were 33.3, 41.7, 58.3, 58.3 and 83.3%
(Fig. 3 and Table II), and the positive expression
rates of SSTR1-5 were all significantly higher compared with the
control group (P<0.05). The positive expression rates of SSTR1-5
in normal endometrium (7.1, 7.1, 21.4, 28.6 and 64.3%) were lower
compared with those in the ectopic (43.3, 70.0, 53.3, 50.0 and
96.7%) and eutopic endometrium (33.3, 41.7, 58.3, 58.3 and 83.3%)
groups (Fig. 4; Table II).
Discussion
SS is a natural polypeptide that is extensively
distributed in the digestive and nervous system, and exhibits
several biological effects (16).
The clinical application of SS is restricted, as natural SS has a
short half-life in vivo of 4 min only (17). The SS analogue (SSTA) has the
advantages of a long half-life, relatively long-lasting effect,
high selectivity and ease of application (18). Numerous types of cancer cell,
inflammatory cell and immune cell (e.g., lymphocytes, phagocytic
cells, endothelial cells and thymus cells) also produce SS
(19). Growth hormones IGF, IL-1,
IL-6, TNF-α and IFN-γ, and other growth factors and cytokines as
well as glucocorticoid, androgen and estrogen may increase the
expression of SS, whilst insulin and leptin may inhibit its
expression (4,7). The intracellular factors regulating the
expression of SS mainly include cyclic adenosine monophosphate
(AMP), Ca2+, cyclic guanine monophosphate and nitric
oxide (19). cAMP has a promoting
effect on the expression and secretion of the SS gene, which
resembles a signal transduction pathway to regulate the function of
SS (19).
The RT-qPCR results of the present study indicated
that the expression of SS mRNA in EMS cells was significantly
higher compared with the normal endometrial cells. Sbracia and
Scarpellini (20) demonstrated that
the occurrence of EMS is associated with immune mechanisms. The
activity of intraperitoneal mononuclear macrophages in EMS patients
is increased, and they secrete large amounts of inflammatory
mediators, including IL-1, IL-6 and TNF-α, which creates an
environment that drives EMS cell proliferation (21). These factors also promote the
expression of the SS gene (22). The
present study indicated that the expression of the SS gene is
elevated in EMS cells, and this increase is likely to be associated
with the occurrence and development of the disease.
Numerous studies have indicated that SS is an
important hormone regulatory peptide that restrains cell
proliferation and differentiation, and which may be utilized to
inhibit the proliferation and angiogenesis of tumor cells (23). The mechanism underlying the
inhibitory effect of SS mainly includes direct inhibition and also
indirect effects (24). After
binding and activation, SS, SSTA and SSTR may exert
anti-proliferative effects through 4 major signaling pathways
(4): i) Via the cAMP pathway to
change cAMP metabolism. The decrease in cAMP leads to inhibition of
cell proliferation and affects protein synthesis (19); ii) changes in intracellular
Ca2+ to reduce the membrane permeability regarding
Ca2+, inhibit Ca2+ influx and block
Ca2+-mediated intracellular processes (6); iii) phosphate protein kinase pathways:
After the SSTR binds to ligands, tyrosine kinase is inactivated by
dephosphorylation to inhibit protein kinases, e.g.,
mitogen-activated protein kinase (MAPK), leading to inhibition of
cell proliferation (25,26); iv) the phosphatidylinositol-3-kinase
(PI3K) pathway: SSTA inhibits the proliferation of tumor cells
through the inhibition of PI3K (27). The indirect inhibitory effects of
SSTA comprise activation of Fas, Caspase-8 and MAPK pathways
mediated via receptors, blocking cell cycle progression from G1
phase to S phase, inhibition of the cell proliferation and
promotion of apoptosis (28,29). A further indirect inhibitory effect
of SSTA is the inhibition of angiogenesis (30,31). The
ectopic endometrium as autografts rather relies on vascular
support, and angiogenesis is crucial to the development of EMS
(32), and thus the occurrence and
development of EMS may be inhibited through the above mechanisms by
using SSTA, which requires to be further verified.
SS acts through binding to specific receptors on the
cell surface and SSTR is a membrane protein receptor, which is
divided into 5 subtypes and has 7 transmembrane domains (10). According to the similarity and
varying affinity towards SSTR, SS may be divided two types: i) High
affinity to SSTR, including SSTR2, SSTR3 and SSTR5; ii) weaker
affinity, with substrates including SSTRl and SSTR4. SSTRl, SSTR2
and SSTR5 mainly mediate the anti-proliferative effect of SS. SSTR
is distributed in all of the major human lymphoid organs, including
thymus, spleen, lymph nodes, tonsils and gut-associated lymphoid
tissues (33). SSTR, expressed as
different subtypes in different lesion tissue types, occurs in a
wide variety of neuroendocrine tumors and tumors of the nervous
system; it is differentially expressed in human tumor and healthy
tissues (11,34). It has been reported that SSTR is also
expressed in non-neuroendocrine tumor tissues; e.g., >50% of
breast cancer and 40% of colorectal cancer tissues were reported to
be positive for SSTR (35,36). SSTR is also expressed in liver,
prostate and pancreatic cancers, as well as in gastric
mucosa-associated lymphoid tissue lymphoma and its metastases
(37–40). Schulz et al (41) detected the expression of SSTRl, −2
and −3 in 12 patients with cervical carcinoma and the positive rate
was 38, 57 and 43%, respectively, while they were negative for the
expression of SSTR4 and −5; furthermore, SSTR1-5 was expressed in
18 patients with endometrial carcinoma with positive rates of 32,
39, 43, 4 and 4%, respectively.
Although a large number of studies have assessed
SSTA and SSTR in other systems, studies have not focused on the
expression of SSTR in EMS lesion tissues (35–40).
Green et al (13) have
assessed the expression of SSTR2 in the endometrium during the
human menstrual cycle using the immunohistochemistry and RT-qPCR,
and their results indicated that SSTR2 was expressed throughout the
menstrual cycle. Fasciani et al (42) discovered that SSTRl, SSTR2 and SSTR5
were highly expressed in ovarian and peritoneal endometrial lesions
using immunohistochemistry and RT-qPCR. Furthermore, a cell
experiment indicated that the octreotide inhibits the migration and
proliferation of endometrial cells (42). Annunziata et al (43) reported that SSTR1-5 were expressed in
EMS tissues and cells, and that in normal eutopic endometrial
cells, mainly SSTR1 was expressed, while the expression of STR3 and
−2 was low and SSTR4 and −5 were not expressed.
The immunohistochemical results of the present study
indicated that SSTR1-5 were expressed in EMS tissues from 30
patients at the rates of 43.3, 70, 53.3, 50 and 96.7%,
respectively, which was significantly associated with the clinical
stage of the patients. However, in previous results of Fasciani
et al (42) and Annunziata
et al (43), the expression
of SSTR1-5 was not significantly associated with the clinical
stage. It was hypothesized that the difference may be due to the
different clinical samples and populations, which require more
studies for confirmation. In the present study, the positive
expression rate of SSTR1-5 in eutopic endometrium from 14 EMS
patients was 33.3, 41.7, 58.3, 58.3 and 83.3%, respectively, whilst
that in normal endometrial tissue was lower than that in ectopic
(43.3, 70.0, 53.3, 50.0 and 96.7%) and eutopic endometrium at 7.1,
7.1, 21.4, 28.6 and 64.3%, respectively. The results verified that
SSTR1-5 was expressed in the ectopic and eutopic endometrium groups
and thus provides a therapeutic basis the use of SSTA for EMS.
The results of the present study indicated that the
positive expression rate of SSTR1-5 in EMS and eutopic endometrium
cells was higher than that in normal endometrium, suggesting that a
similarity between eutopic and EMS cells and a difference from
normal endometrium, further confirming the ‘eutopic endometrium
determinism’ theory. Therefore, the detection of SSTR expression in
the eutopic endometrium is of clinical significance.
Various clinical studies have confirmed that the
SSTA, including octreotide, has inhibitory effects on pancreatic
cancer, breast cancer, neuroendocrine tumors and carcinoid tumors
(4–6). Scintigraphy (SS receptor imaging, SS
receptor scintigraphy) with radiolabeled SSTA has been used for
diagnosing and locating tumors (44). Radiolabeled SS analogues bind to
SSTR-positive tumors and help in making a definite diagnosis
(45). Fasciani et al
(42) injected
111In-diethylene triamine pentaacetic acid octreotide in
8 EMS patients pre-operatively, and when scanning was performed
after 12 h, stronger signals were detected in the pelvic cavity of
6 patients and weaker signals in that of 2 patients, and no adverse
reactions were encountered. By scintigraphy using radiolabeled
SSTA, EMS may be located and diagnosed, EMS lesions that B
ultrasound and computed tomography cannot detect in the pelvic
cavity and intestinal duct may be discovered and it is possible to
make an auxiliary diagnosis for patients with EMS-induced chronic
pelvic pain (46).
Previous studies have indicated that in certain
types of cancer tissue with low or no expression of SSTR, including
pancreatic, gastric, colorectal and ovarian cancer, the expression
levels of SSTR may be improved by transfection of SSTR gene to thus
improve the efficacy of SSTA (47,48). For
endometrial cells with low expression levels of SSTR, high
expression of SSTR may be genetically induced (43), thus increasing the likelihood for the
successful treatment of EMS using SSTA.
The present study indicated that SS and its receptor
are expressed in EMS tissues or cells and enhanced the knowledge in
the field, on which novel methods for the diagnosis and treatment
of EMS using SSTR gene transfection and SSTA approaches may be
based.
Acknowledgements
Not applicable.
Funding
No funding received.
Availability of data and materials
The analyzed data sets generated during the study
are available from the corresponding author on reasonable
request.
Authors' contributions
YaZ conducted the experiments and wrote the
manuscript, LP and XL collected the data and performed the
experiments, and YiZ designed the study. The final version of the
manuscript has been read and approved by all authors, and each
author believes that the manuscript represents honest work.
Ethical approval and consent to
participate
The present study was approved by Ethics Committee
of Xiangya Hospital of Central South University (Changsha, China)
and informed consent was obtained from all subjects.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Leyendecker G, Kunz G, Noe M, Herbertz M
and Mall G: Endometriosis: A dysfunction and disease of the
archimetra. Hum Reprod Update. 4:752–762. 2015. View Article : Google Scholar
|
|
2
|
Vercellini P, Viganò P, Somigliana E and
Fedele L: Endometriosis: Pathogenesis and treatment. Nat Rev
Endocrinol. 10:261–275. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gaudillère A, Misery L, Bernard C,
Souchier C, Claudy A and Schmitt D: Presence of somatostatin in
normal human epidermis. Br J Dermatol. 137:376–380. 2015.
View Article : Google Scholar
|
|
4
|
Modlin IM, Pavel M, Kidd M and Gustafsson
BI: Review article: Somatostatin analogues in the treatment of
gastroenteropancreatic neuroendocrine (carcinoid) tumours. Aliment
Pharmacol Ther. 31:169–188. 2010.PubMed/NCBI
|
|
5
|
Appetecchia M and Baldelli R: Somatostatin
analogues in the treatment of gastroenteropancreatic neuroendocrine
tumours, current aspects and new perspectives. J Exp Clin Cancer
Res. 29:192010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Pollak MN and Schally AV: Mechanisms of
antineoplastic action of somatostatin analogs. Proc Soc Exp Biol
Med. 217:143–152. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fanselow EE and Connors BW: The roles of
somatostatin-expressing (GIN) and fast-spiking inhibitory
interneurons in up-down states of mouse neocortex. J Neurophysiol.
104:596–606. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ludlam WH and Anthony L: Safety review:
Dose optimization of somatostatin analogs in patients with
acromegaly and neuroendocrine tumors. Adv Ther. 28:825–841. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Igarashi H, Hijioka M, Lee L and Ito T:
Biotherapy of pancreatic neuroendocrine tumors using somatostatin
analogs. J Hepatobiliary Pancreat Sci. 22:618–622. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Samimi M, Gardair C, Touze A, Coursagetb
P, Kerdraond R, Estevee E, Crouef A, Avenel-Audrang M, Hainaulth E,
Benetoni N, et al: Expression des récepteurs de la somatostatine
(SSTR-2A et SSTR-5) et relation avec les données cliniques dans une
cohorte de 99 patients avec carcinomes à cellules de Merkel.
Annales De Dermatologie Et De Venereologie. 141:S242–S243. 2014.
View Article : Google Scholar
|
|
11
|
Kaemmerer D, Schindler R, Mußbach F,
Dahmen U, Altendorf-Hofmann A, Dirsch O, Sänger J, Schulz S and
Lupp A: Somatostatin and CXCR4 chemokine receptor expression in
hepatocellular and cholangiocellular carcinomas: Tumor capillaries
as promising targets. BMC Cancer. 17:8962017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Halmos G, Sun B, Schally AV, Hebert F and
Nagy A: RAPID COMMUNICATION: Human ovarian cancers express
somatostatin receptors. J Clin Endocrinol Metabol. 85:3509–3512.
2000. View Article : Google Scholar
|
|
13
|
Green VL, Richmond I, Maguiness S,
Robinson J, Helboe L, Adams IP, Drummond NS and Atkin SL:
Somatostatin receptor 2 expression in the human endometrium through
the menstrual cycle. Clin Endocrinol (Oxf). 56:609–614. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Boujenah J, Hugues JN, Sifer C, Bricou A,
Cédrin-Durnerin I, Sonigo C, Monforte M and Poncelet C:
Endometriosis fertility index, or classification of the american
society of reproductive medicine for postoperative endometriosis
patients with infertility: Which is more relevant? Gynecol Obstet
Fertilite. 43:806–809. 2015.(In French). View Article : Google Scholar
|
|
15
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Szolcsányi J, Helyes Z, Oroszi G, Németh J
and Pintér E: Release of somatostatin and its role in the mediation
of the anti-inflammatory effect induced by antidromic stimulation
of sensory fibres of rat sciatic nerve. Br J Pharmacol.
123:936–942. 2010. View Article : Google Scholar
|
|
17
|
Nilsson CL, Brinkmalm A, Minthon L,
Blennow K and Ekman R: Processing of neuropeptide Y, galanin and
somatostatin in the cerebrospinal fluid of patients with Alzheimers
disease and frontotemporal dementia. Peptides. 22:2105–2112. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kang TC, Park SK, Do SG, Suh JG, Jo SM, Oh
YS, Jeong YG and Won MH: The over-expression of somatostatin in
gerbil entorhinal cortex induced by seizure. Brain Res. 882:55–61.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Patel YC: Somtostat in and its receptor
family. Front Neuroendocrinol. 20:157–198. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sbracia M and Scarpellini F: PIF
expression in endometriosis: Its possible role in inducing ectopic
endometrium immune-privilege. J Reprod Immunol. 122:402017.Ho HN,
Wu MY and Yang YS: Peritoneal cellular immunity and endometriosis.
Am J Reprod Immunol 38: 400.412, 2011. View Article : Google Scholar
|
|
21
|
Lang J: Further improve EMS basic and
clinical research. Chin J Obstet Gynecol. 36:711–713. 2001.(In
Chinese).
|
|
22
|
Scarborough DE, Lee SL, Dinarello CA and
Reichlin S: Interleukin-1 beta stimulates somatostatin biosynthesis
in primary cultures of fetal rat brain. Endocrinology. 124:549–551.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Dasgupta P: Somatostatin an alogues:
Multiple roles incellular proliferation, neoplasia,
andangiogenesis. Pharmacol Ther. 102:61–85. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ma W, Liu B, Li Y, Huang ZJ, Zhang LI and
Tao HW: Visual representations by cortical somatostatin inhibitory
neurons-selective but with weak and delayed responses. J Neurosci.
30:14371–14379. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Reisine T and Bell GI: Molecular
properties of somatostatin receptor. Neuroscience. 67:777–790.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cordelier P, Estève JP, Bousquet C,
Delesque N, O'Carroll AM, Schally AV, Vaysse N, Susini C and
Buscail L: Characterization of the antiproliferative signal
meditated by the somatostatin receptor subtype SSTR5. Proc Natl
Acad Sci USA. 94:9343–9348. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Charland S, Boucher MJ, Houde M and Rivard
N: Somatostatin inhibits Aktphosphorylation and cell cycle entry,
but not p42/p 44 mitogen activated protein(MAP)kinase activation in
normal and tumoral pancreatic acinar cells. Endocrinology.
142:121–128. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Feooux G, Bousquet C, Cordelier P, Benali
N, Lopez F, Rochaix P, Buscail L and Susini C: Signal transduction
of somatostatin receptors negatively controlling cell
proliferation. J Physiol Paris. 94:205–210. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Feuoux G, Lopez E, Esteve JP, Ferrand A,
Vivier E, Vely F, Saint-Laurent N, Pradayrol L, Buscail L and
Susini C: Critical role of Src and SHP-2 in sst2 somatostatin
receptor-mediated activation of SHP-1 and inhibition of cell
proliferation. Mol Biol Cell. 14:3911–3928. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Woltering EA: Development of targeted
somatostatin-based antiangiogenic therapy: A review and future
perspectives. Cancer Biother Radiopharm. 18:601–609. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Adams RL, Adams IP, Lindow SW, Zhong W and
Atkin SL: Somatostatin receptors 2 and 5 are preferentially
expressed in proliferating endothelium. Br J Cancer. 92:1493–1498.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhang Y, Cao H, Hu YY, Wang H and Zhang
CJ: Inhibitory effect of curcumin on angiogenesis in ectopic
endometrium of rats with experimental endometriosis. Int J Mol Med.
27:87–94. 2011.PubMed/NCBI
|
|
33
|
Ferone D, Lombardi G and Colao A:
Somatostatin receptors inimmune system cells. Minerva Endocrinol.
26:165–173. 2001.(In Italian). PubMed/NCBI
|
|
34
|
Mehta S, de Reuver PR, Gill P, Andrici J,
D'Urso L, Mittal A, Pavlakis N, Clarke S, Samra JS and Gill AJ:
Somatostatin receptor SSTR-2a expression is a stronger predictor
for survival Than Ki-67 in pancreatic neuroendocrine tumors.
Medicine (Baltimore). 94:e12812015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Krenning EP, Kooij PP, Pauwels S, Breeman
WA, Postema PT, De Herder WW, Valkema R and Kwekkeboom DJ:
Somatostatin receptor: Scintigraphy and radionuclide therapy.
Digestion. 57 Suppl 1:S57–S61. 1996. View Article : Google Scholar
|
|
36
|
van Eijck CH, Krenning EP, Bootsma A, Oei
HY, van Pel R, Lindemans J, Jeekel J, Reubi JC and Lamberts SW:
Somatostatin-receptor scintigraphy in primary breast cancer.
Lancet. 343:640–643. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Reynaert H, Rombouts K, Vandermonde A,
Urbain D, Kumar U, Bioulac-Sage P, Pinzani M, Rosenbaum J and
Geerts A: Expression of somatostatin receptors in normal and
cirrhotic human liver and in hepatocellular carcinoma. Gut.
53:1180–1189. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Hansson J, Bjartell A, Gadaleanu V, Dizeyi
N and Abrahamsson PA: Expression of somatostatin receptor subtypes
2 and 4 in human benign prostatic hyperplasia and prostatic cancer.
Prostate. 53:50–59. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Li M, Li W, Kim HJ, Yao Q, Chen C and
Fisher WE: Characterization of somatostatin receptor expression in
human pancreatic cancer using real-time RT-PCR. J Surg Res.
119:130–137. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Raderer M, Traub T, Formanek M, Virgolini
I, Osterreicher C, Fiebiger W, Penz M, Jäger U, Pont J, Chott A and
Kurtaran A: Somatostatin-receptor scintigraphy for staging and
follow-up of patients with extraintestinal marginal zone B-cell
lymphoma of the mucosa associated lymphoid tissue(MALT)-type. Br J
Cancer. 85:1462–1466. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Schulz S, Schmitt J and Weise W: Frequent
expression of immunoreactive somatostatin receptors in cervical and
endometrial cancer. Gynecol Oncol. 89:385–390. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Fasciani A, Quilici P, Biscaldi E, Flamini
M, Fioravanti A, Orlandi P, Oliviero J, Repetti F, Bandelloni R,
Danesi R, et al: Overexpression and functional relevance of
somatostatin receptor-1, −2, and −5 in endometrium and
endometriotic lesions. J Clin Endocrinol Metab. 95:5315–5319. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Annunziata M, Luque RM, Durán-Prado M,
Baragli A, Grande C, Volante M, Gahete MD, Deltetto F, Camanni M,
Ghigo E, et al: Somatostatin and somatostatin analogues reduce
PDGF-induced endometrial cell proliferation and motility. Hum
Reprod. 27:2117–2129. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kumar S, Mishra Kumar A, Chhikara BS,
Chuttani K and Sharma Kumar R: Preparation and pharmacological
evaluation of a new radiopharmaceutical,
technetium-99m-5-fluorouracil, for tumor scintigraphy. Hell J Nucl
Med. 11:91–95. 2008.PubMed/NCBI
|
|
45
|
Hasegawa S, Kobayashi N, Tokuhisa M, Goto
A, Takano S, Takada Y, Kaneta T, Mori R, Matsuyama R, Endo I, et
al: Clinical usefulness of somatostatin receptor scintigraphy in
Japanese patients with gastroenteropancreatic neuroendocrine
tumors. Digestion. 96:132017. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kennedy SH, Mojiminiyi OA, Soper N,
Shepstone BJ and Barlow DH: Immunoscintigraphy of endometriosis. Br
J Obstet Gynecol. 97:667–670. 2010. View Article : Google Scholar
|
|
47
|
Rochaix P, Delesque N, Estève JP,
Saint-Laurent N, Voight JJ, Vaysse N, Susini C and Buscail L: Gene
therapy for pancreatic carcinoma: Local and distant antittmaor
effects after somatostatin receptor sst2 gene transfer. Human Gene
Therapy. 10:995–1008. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Chaudhuri TR, Rogers BE, Buchsbaum DJ,
Mountz JM and Zinn KR: A noninvasive receptor system to image
Adenoviral-mediated gene transfer to ovarian cancer xenogragts.
Gynecol Oncol. 83:432–438. 2001. View Article : Google Scholar : PubMed/NCBI
|