Introduction
Esophageal cancer ranks among the ten most common
cancers in the world, and lymph node metastasis is a critical
determinant of poor prognosis for this cancer (1,2).
Lymph node classification is based on the number of nodes with
metastatic foci within the most recent (7th) edition of the tumor,
node, metastasis (TNM) system of classification defined by the
International Union Against Cancer (UICC) (3). This reflects a distinct prognostic
difference from the 6th edition of these guidelines, in which nodal
metastasis was graded as either present or absent. By contrast, the
lymph node classification endorsed by the Japanese Society for
Esophageal Disease is based on anatomical lymphatic spread to lymph
node stations and is also useful for the assessment of prognosis
(4). However, to date, there is no
consensus as to which nodal classification system is the most
useful for assessment of prognosis, although several other nodal
classification have been proposed.
The aim of this study was to examine the utility and
feasibility of a novel metastatic node classification system that
combines the intensity of node metastasis (represented by the TNM
classification system) and anatomical lymphatic spread (represented
by the Japanese classification system) for the assessment of
prognosis of patients undergoing surgical management for esophageal
cancer.
Patients and methods
Patients
Data were obtained from 257 patients (224 males and
33 females; mean age, 64.0 years) who underwent transthoracic
esophagectomy via the right transthoracic route for esophageal
cancer without preoperative chemotherapy or radiotherapy between
January 1991 and December 2008. Data were collected and analyzed
retrospectively, and all patients employed in the analysis were
followed until death or until December 2010 (i.e., at least 2 years
after surgery).
Clinicopathological characteristics including tumor
invasion, node metastasis and stage were based on the TNM
classification, 7th edition, by the International Union Against
Cancer, and on the Japanese Guidelines for the Clinical and
Pathologic Studies on Carcinoma of the Esophagus. Lymph node
station spread was determined according to the Japanese
classification system (3,4).
Classification of lymph node status
The mode of lymph node metastasis was divided into
two groups: single-station (S) and multi-station (M). In addition,
the S group was subclassified into a single-node-single-station
(SS) group, in which lymph node metastasis was detected in only one
node, and a multi-node-single-station (MS) group, in which lymph
node metastasis was detected in two or more nodes within a single
lymph node station. Furthermore, the M group was also subclassified
into a multi-station in pN1 (two metastasis-positive nodes) by TNM
classification (MM-pN1) group, a multi-station in pN2 or 3 in TNM
classification (MM-pN2,3) group, a multi-station-single-area (MMS)
group, in which the metastasis-positive lymph node station was
localized to the cervical, thoracic or abdominal area, and a
multi-station-multi-area (MMM) group, in which metastasis-positive
nodes were present in two or more of these areas.
Statistical analysis
The correlation between prognosis and lymph node
metastasis mode was assessed. The Kaplan-Meier method by Wilcoxon
test was used to assess prognosis after surgery. A p-value <0.05
was considered to indicate statistical significance in each
analysis.
Results
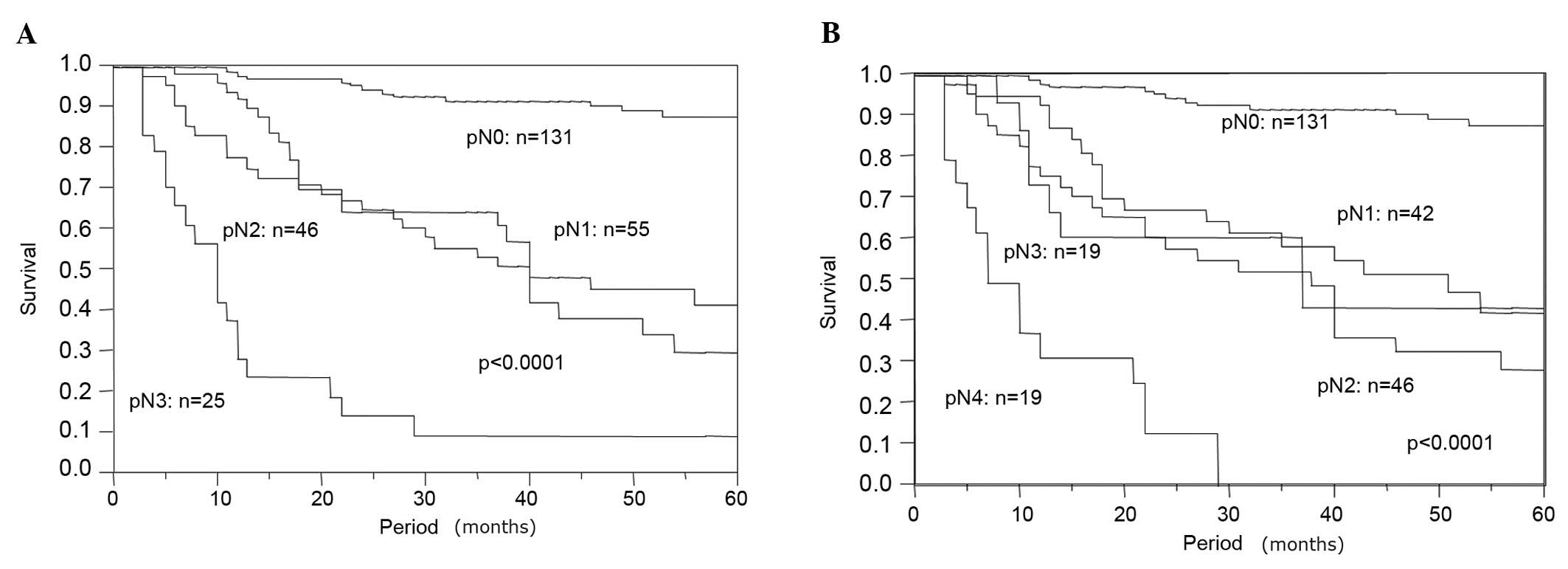
Patient characteristics are shown in Table I. Of the 257 patients, 131 (51.0%)
had no lymph node metastasis. Of the 126 patients with lymph node
metastasis, 55 patients (43.7%) were classified as pN1, 46 (36.5%)
were classified as pN2, and 25 (19.8%) were classified as pN3 by pN
category of the TNM classification based on the number of
metastasis-positive lymph nodes. By contrast, 42 patients (33.3%)
were classified as pN1, 46 (36.5%) were classified as pN2, 19
(15.1%) were classified as pN3 and 19 (15.1%) were classified as
pN4 by the Japanese classification system based on lymphatic spread
to lymph node station. Disease-specific survivals according to TNM
and Japanese classifications are shown in Fig. 1A and B, and both classifications
revealed significant prognostic differences between pN categories
(p<0.0001).
 | Table ICharacteristics of the patients
undergoing thoracoscopic surgery for esophageal cancer. |
Table I
Characteristics of the patients
undergoing thoracoscopic surgery for esophageal cancer.
| Characteristic | No. of patients |
|---|
| Age (years) | 64 (36–84) |
| Gender | |
| Male | 224 |
| Female | 33 |
| Tumor location | |
| Upper thoracic | 32 |
| Middle
thoracic | 143 |
| Lower thoracic | 82 |
| Histology | |
| Squamous cell
carcinoma | 228 |
| Adenosquamous
carcinoma | 5 |
| Adenocarcinoma | 9 |
| Basaloid
carcinoma | 10 |
| Spindle cell
carcinoma | 1 |
| Neuroendocrine
carcinoma | 1 |
| Small cell
carcinoma | 2 |
| Undifferentiated
carcinoma | 1 |
| Tumor depth (pT) | |
| in situ | 5 |
| 1 | 116 |
| 2 | 35 |
| 3 | 99 |
| 4 | 2 |
| Lymph node metastasis
(TNM classification) | |
| 0 | 131 |
| 1 | 55 |
| 2 | 46 |
| 3 | 25 |
| Lymph node metastasis
(Japanese classification) | |
| 0 | 131 |
| 1 | 42 |
| 2 | 46 |
| 3 | 19 |
| 4 | 19 |
| Lymphatic vessel
invasion | |
| Negative | 108 |
| Positive | 149 |
| Blood vessel
invasion | |
| Negative | 179 |
| Positive | 78 |
Of the 126 patients who were node
metastasis-positive, 47 (37.3%) were classified as S group, and 79
patients (62.7%) were classified as M group. Among the S-group
patients, 11 (23.4%) were classified as the MS group, and 36
(76.6%) were classified as the SS group. Of the M group patients,
12 patients (15.2%) were classified as MM-pN1, 67 patients (84.8%)
were classified as MM-pN2,3. Using another system to subdivide the
M group, 55 patients (69.6%) were classified as MMM group, and 24
(30.4%) were classified as MMS group. In the present lymph node
metastasis classification system, M-group patients preferentially
comprised those with cancer arising from the lower or upper
thoracic esophagus (p=0.036), cases with advanced invasion depth
(p<0.0001), cases with lymphatic vessel invasion (p<0.0001)
and cases with blood vessel invasion (p<0.0001) (Table II).
| Table IICorrelation between lymphatic spread
and clinicopathological factors. |
Table II
Correlation between lymphatic spread
and clinicopathological factors.
| Lymphatic spread
| p-value |
|---|
| Negative | Single station | Multi-station | |
|---|
| Gender | | | | |
| Male | 116 | 41 | 67 | 0.74 |
| Female | 15 | 6 | 12 | |
| Age (years) | 62.8 | 65.2 | 65.4 | |
| Location | | | | |
| Lower | 35 | 17 | 30 | 0.036 |
| Middle | 85 | 21 | 37 | |
| Upper | 11 | 9 | 12 | |
| Tumor invasion
(pT) | | | | |
| Superficial (pTis,
1) | 95 | 18 | 8 | <0.0001 |
| Advanced (pT2,
3) | 36 | 29 | 71 | |
| Lymphatic vessel
invasion | | | | |
| Negative | 82 | 16 | 10 | <0.0001 |
| Positive | 49 | 31 | 69 | |
| Blood vessel
invasion | | | | |
| Negative | 109 | 34 | 36 | <0.0001 |
| Positive | 22 | 13 | 43 | |
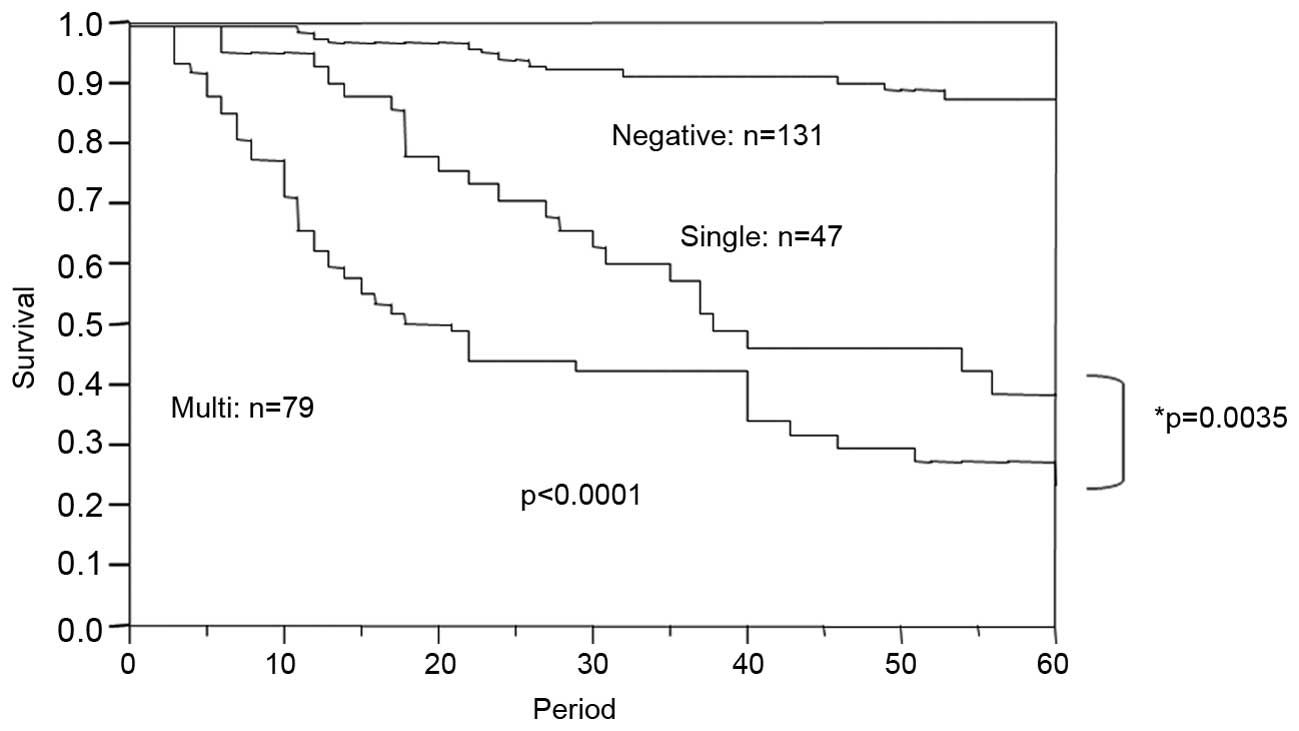
Lymph node metastasis classification in the present
study revealed a distinct prognostic significance (p<0.0001).
For example, multiple-station metastasis was a significant negative
prognostic parameter compared with single-station metastasis
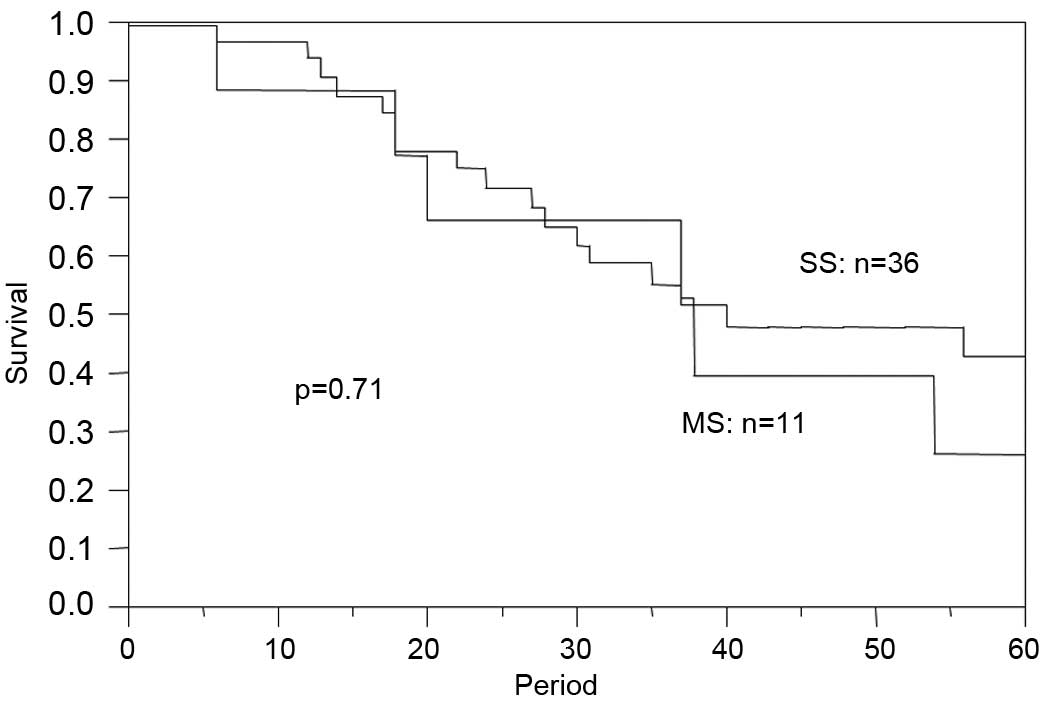
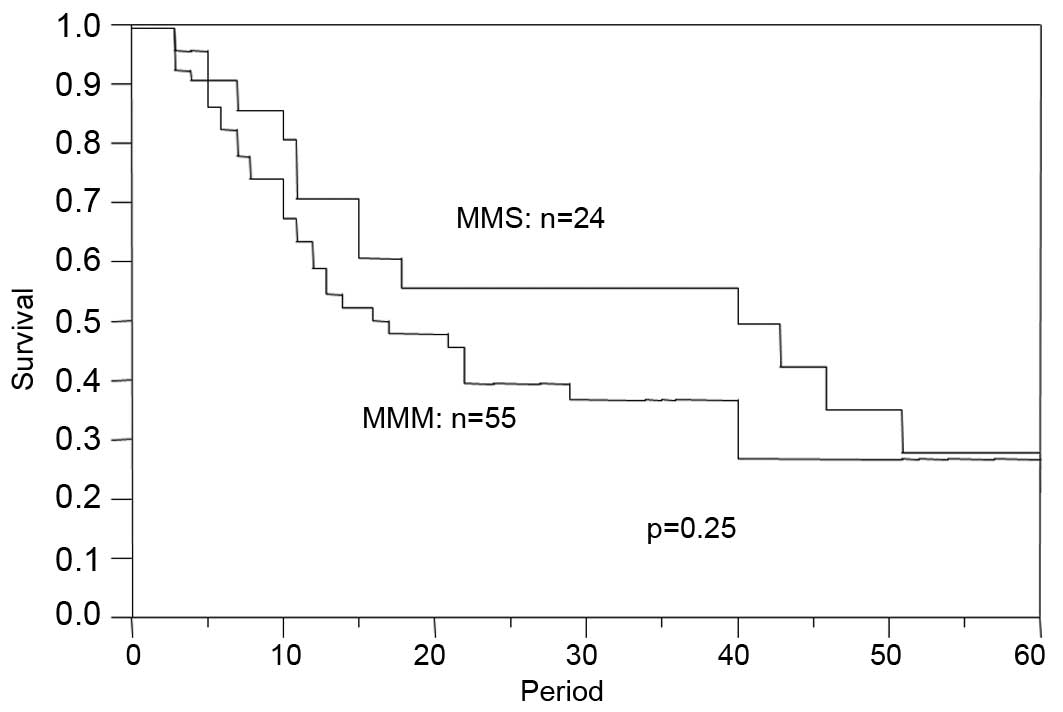
(p=0.0035) (Fig. 2). However,
prognosis was similar when comparing the MS and SS groups (p=0.71)
(Fig. 3). In the MS group, the
number of positive lymph nodes ranged from 2 to 8 (mean was 3.09).
Five cases with more than 3 positive nodes were included in the MS
group, 4 cases were classified as pN2 and 1 case was classified as
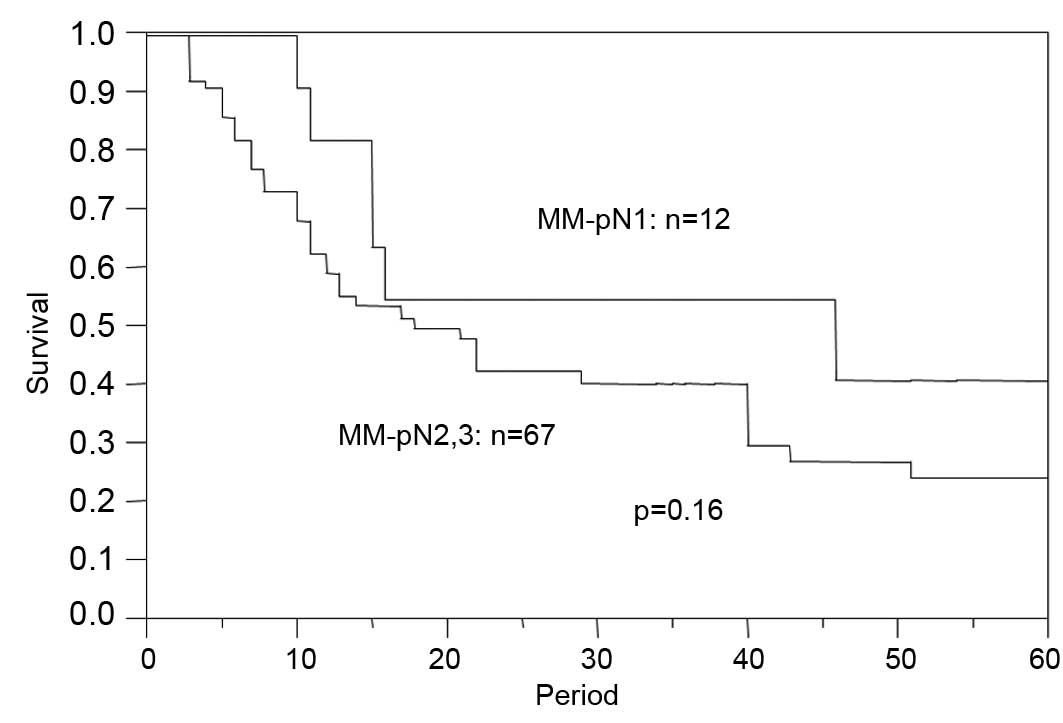
pN3 in the TNM classification. Furthermore, there was no
significant difference in prognosis when comparing the MM-pN1 and
MM-pN2,3 groups (p=0.16) or when comparing the MMM and MMS groups
(p=0.25) (Figs. 4 and 5).
Notably, the association between prognosis and node
metastasis classification in this study (p<0.0001) was similar
to that between prognosis and lymph node involvement of the TNM and
Japanese classification systems in the multivariate analysis
including conservative clinicopathological prognostic parameters
despite close interaction with each other (Table III).
| Table IIIMultivariate analysis of prognostic
impact with other clinicopathological parameters. |
Table III
Multivariate analysis of prognostic
impact with other clinicopathological parameters.
| Risk ratio | 95% Confidence
interval | p-value |
|---|
| Tumor invasion
(pT) | 4.412 | 0.6989–15.36 | 0.049 |
| Lymphatic vessel
invasion | 0.6984 | 0.4915–0.9611 | 0.027 |
| Blood vessel
invasion | 1.075 | 0.8291–1.391 | 0.58 |
| No. of positive LN
stations | 1.919 | 1.359–2.737 | <0.0001 |
Discussion
TNM classification can be used to predict prognosis
in patients with esophageal cancer according to cancer stage
(3). In the 6th edition of the TNM
classification, lymph node involvement is classified as either
present or absent. However, the 7th edition of the TNM
classification, published in 2010, incorporates the number of lymph
nodes with metastatic involvement and may be a more accurate
prognostic parameter. This revised system still does not
acknowledge the anatomical lymphatic spread, which may limit its
overall utility. Thus, the present study utilized the revised TNM
system in combination with the Japanese classification, which does
assess anatomical lymphatic spread of metastasis. This node
classification has prognostic significance, but the lymph node
station category can vary with tumor location despite having the
same lymph node station (4).
Therefore, the present study used a simple modification of this
system, in which the pN category of the lymph node station is not
determined in detail, but the location of lymph node station is
still taken into account.
In this study, patients with multi-station lymph
node metastasis preferentially comprised those with cancer arising
from the lower or upper thoracic esophagus (p= 0.036), cases with
advanced invasion depth (p<0.0001), cases with lymphatic vessel
invasion (p<0.0001) and cases with blood vessel invasion
(p<0.0001). Lamb et al and Kim et al reported that
multiple sentinel nodes were detected more frequently in patients
with lower thoracic esophageal cancer, which may account for the
implied finding that lower thoracic esophageal cancers are more
prone to metastasize to multiple nodes or stations (5,6).
However, there has been no previous report suggesting that upper
thoracic esophageal cancers are associated with a higher
metastasis-positive station. Concerning the correlation between
tumor invasion and lymphatic spread, Feith et al reported
that deeper tumor invasion was associated with the increased number
of metastasis-positive lymph nodes in patients with Barrett's
esophageal adenocarcinoma (7). By
contrast, the present result, which took into account the number of
stations, may be consistent with the previous findings despite the
fact that the majority of cases in the present study consisted of
squamous cell carcinoma. This indicates that deeper invasive cancer
in the lower thoracic esophagus requires much more extended lymph
node dissection regardless of the histological type of esophageal
cancer.
In the univariate analysis of the prognostic impact,
the lymph node metastasis classification system utilized in the
present study exhibited a distinct prognostic significance when
comparing the S and M groups, and the M group exhibited less
favorable prognosis following surgery. Several other lymph node
classification systems have been proposed to predict outcomes in
patients undergoing surgical management of esophageal cancer. For
example, Roder et al, Eloubeidi et al and Wilson
et al described the utility of involved lymph node ratios
for predicting an unfavorable prognosis (8–10).
Roder et al and Eloubeidi et al set the cut-off
values at 20 and 10%, and the increased ratio of metastatic nodes
revealed an unfavorable prognosis. However, when Wilson et
al set the cut-off values at 25 and 50%, there was no
difference in prognosis when comparing the two groups. Altorki
et al suggested that the increased number of dissected lymph
nodes in the context of extended lymphadenectomy resulted in a
decreased positive node ratio and a more favorable prognosis
(11). By contrast, Dhar et
al reported that the longer diameter of the largest metastatic
lymph node was a strong negative prognostic factor, whereas Komori
et al emphasized that the size of the cancer nest in the
lymph node, but not lymph node size, had a prognostic impact
(12,13). These previous reports were limited
by the fact that they only examined very limited lymph node
metastatic mode parameters. However, the present study takes into
account the number of positive nodes represented by the TNM
classification and the anatomical lymphatic spread represented by
the Japanese classification, which likely resulted in a stronger
independent prognostic factor, even within multivariate analysis
including conservative pathological parameters.
Notably, there was no prognostic difference between
the SS and MS groups in this study. This indicates that a favorable
prognosis may occur when lymph node metastasis is limited to a
single station, even in the context of pN2 or 3 status in the TNM
classification. Furthermore, lymph node dissection may be very
effective in cases with limited anatomical lymphatic spread (e.g.,
S group), since all cases employed in the present series were
surgically resected with extended curative lymph node dissection.
Prognosis was also similar when comparing MM-pN1 cases and MM-pN2,3
cases, which supports inclusion of these two subclassifications
within the same M group. The results of the subgroup analysis also
indicate that anatomical lymphatic spread and the number of
metastasis-positive nodes play an important role in outcome
following surgical treatment of esophageal cancer, although
Kunisaki et al reported that the number of metastatic nodes
provides a more accurate estimate of prognosis than the anatomical
lymphatic spread (14).
The lymph node metastasis classification system used
in the present study was an independent prognostic parameter, even
within multivariate analysis including conservative pathological
parameters, such as tumor invasion depth and lymphatic or blood
vessel invasion. This result suggests that this classification
system is an effective alternative to the pN category in the TNM or
Japanese classification.
In conclusion, lymph node metastasis classification
based on the number of metastasis-positive stations is a useful
predictor of prognosis in patients undergoing surgical management
of esophageal cancer. This system relies on a simple classification
method that combines the Japanese classification based on lymphatic
spread and the TNM classification based on the number of positive
nodes.
References
|
1
|
Parkin DM, Pisani P and Ferlay J:
Estimates of the worldwide incidence of 25 major cancers in 1990.
Int J Cancer. 80:827–841. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pisani P, Parkin DM, Bray F, et al:
Erratum: Estimates of the worldwide mortality from 25 cancers in
1990. Int J Cancer. 83:18–29. 1999. View Article : Google Scholar
|
|
3
|
Sobin LH, Gospodarowicz MK and Wittekind
C: UICC TNM classification of malignant tumours. 7th edition.
Wiley-Blackwell; Oxford: pp. 63–72. 2009
|
|
4
|
Japanese Society for Esophageal Diseases:
Guide lines for the clinical and pathologic studies for carcinoma
of the esophagus. Jpn J Surg. 6:79–86. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lamb PJ, Griffin SM, Burt AD, et al:
Sentinel node biopsy to evaluate the metastatic dissemination of
oesophageal adenocarcinoma. Br J Surg. 92:60–67. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kim HK, Kim S, Park JJ, et al: Sentinel
node identification using technetium-99m neomannosyl human serum
albumin in esophageal cancer. Ann Thorac Surg. 91:1517–1522. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Feith M, Stein HJ and Siewert JR: Pattern
of lymphatic spread of Barrett's cancer. World J Surg.
27:1052–1057. 2003.
|
|
8
|
Roder JD, Busch R, Stein HJ, et al: Ratio
of invaded to removed lymph nodes as a predictor of survival in
squamous cell carcinoma of the oesophagus. Br J Surg. 81:410–413.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Eloubeidi MA, Desmond R, Arguedas MR, et
al: Prognostic factors for the survival of patients with esophageal
carcinoma in the U.S.: the importance of tumor length and lymph
node status. Cancer. 95:1434–1443. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wilson M, Rosato EL, Chojnacki KA, et al:
Prognostic significance of lymph node metastases and ratio in
esophageal cancer. J Surg Res. 146:11–15. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Altorki NK, Zhou XK, Stiles B, et al:
Total number of resected lymph nodes predicts survival in
esophageal cancer. Ann Surg. 248:221–226. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dhar DK, Tachibana M, Kinukawa N, et al:
The prognostic significance of lymph node size in patients with
squamous esophageal cancer. Ann Surg Oncol. 9:1010–1016. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Komori T, Doki Y, Kabuto T, et al:
Prognostic significance of the size of cancer nests in metastatic
lymph nodes in human esophageal cancers. J Surg Oncol. 82:19–27.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kunisaki C, Akiyama H, Nomura M, et al:
Developing an appropriate staging system for esophageal carcinoma.
J Am Coll Surg. 201:884–890. 2005. View Article : Google Scholar : PubMed/NCBI
|