1. Definition and risk factors
Diabetic neuropathy (DN) may be defined as the
presence of certain signs or specific symptoms and suggestive for
neuropathy in patients with diabetes mellitus (DM), after excluding
other possible causes of neuronal damage (1). DN is the most common microvascular
complication encountered in DM individuals; after 20 years of
disease progression, more than 50% of DM patients are affected by
this complication with a significant impact on their life quality,
considering the characteristic chronic pain in their lower limbs
(2). DN currently remains an
important cause of morbidity. It is a recognized risk factor for
diabetic foot syndrome and falls generated by balance disorders,
especially in the elderly (3).
Diabetic foot syndrome is also associated with a high risk of
infection and amputation (3). DN
prevalence significantly differs in observational studies due to
the varying diagnostic methods used. In a UK study (4), 22.7% of individuals with type 1 DM had
DN; also, 65% of DM patients treated with insulin, and 59% of
patients on oral antidiabetic drugs have DN. Other studies
demonstrated that the DN prevalence in patients with type 2 DM was
32.1% (5). In young diabetic
patients, its prevalence is 7% in type 1 DM, and 22% type 2 DM,
respectively (6). In Romania, the
prevalence of self-reported DN was estimated to be around 79% in a
population of 21,261 patients. That study included both type 1 and
type 2 diabetes patients and did not further analyze the prevalence
according to diabetes type (7).
Distal DN, the most common form, accounts for 75% of
all DN cases. The ‘American Diabetes Association’ (ADA) recommends
physicians involved in DM screen for DN at five years after the DM
type 1 debut, and at the time of diagnosis in individuals with type
2 DM (8). Screening for DN is of
high importance since approximately 50% of patients with DN are
asymptomatic (8). DN increases the
risk of lower limb amputations by 1.7-fold; in the presence of a
leg deformity, the risk increases by 12-fold, whereas in cases with
a history of lower limb ulceration, the risk increases by 36-fold
(9). This increased frequency of
lower limb amputations in patients with DM and DN is attributed to
lower limb micro-traumatisms, due to the fact that affected
individuals have diminished pain sensation. Another form of DN,
cardiac autonomic neuropathy, is associated with extremely high
10-year mortality of 25-50%, mainly due to the generation of
cardiac arrhythmias (10). The most
investigated and documented predictor factors for the development
of DN are hyperglycaemia, DM duration and age, as well as the
presence of microvascular complications including hypertension,
dyslipidaemia, diabetic retinopathy and chronic kidney disease
(11).
Hyperglycaemia is an essential factor in the onset
and progression of DN (1). The
finding is highly specific in individuals with type 1 DM but
incompletely validated in those with type 2 DM. The ‘Diabetes
Control and Complications Trial’ (DCCT) (12) followed subjects with type 1 DM for
6.5 years, who underwent either intensive treatment of
hyperglycaemia or standard treatment (12). In the intensive treatment group, DN
was developed significantly less frequently, whereas, in those who
already had DN, its progression was slower (12). This considerable impact of high
blood glucose levels on the risk of DN was demonstrated by the
finding that a 2% elevation of HbA1c correlated with an increase in
DN frequency by 20% (13). Another
study performed on 3,000 subjects with type 1 DM showed that the
prevalence of DN in patients with HbA1c <5.4% was 15%, while in
those with HbA1c >7.8% it was 40% (14). Similarly, a meta-analysis revealed
that optimal blood glucose control decreases the incidence of DN in
types 1 and 2 DM individuals. In type 1 DM the risk reduction per
year was 1.84% (95% CI: 1.11-2.56, P<0.01), while in individuals
with type 2 DM the annual risk reduction was 0.58% (95% CI: 0.01 to
-1.17, P=0.06) (15). It can be
observed that in type 1 DM the DN risk is reduced, while in type 2
the decrease is not statistically significant, which means that
additional risk factors influence to the development and evolution
of DN in type 2 DM (15). The
Addition-Denmark study (16) and
the ‘Action to Control Cardiovascular Risk in Type 2 Diabetes’
(ACCORD) study (17), with a large
number of type 2 DM patients (n=10,251), also failed to prove any
positive results of intensive blood-glucose control on the
reduction of distal DN incidence or prevention of cardiac autonomic
neuropathy. The Steno-2 study demonstrated no effects of blood
glucose control on the risk of developing somatic DN but found a
significant decrease in the risk of developing cardiac autonomic
neuropathy with HR 0.37 (95% CI: 0.18-0.79, P<0.01) (18).
Previous findings showed that, the choice of
antidiabetic treatment may play a role in the rate of DN
occurrence. In the ‘Bypass Angioplasty Revascularization
Investigation 2 Diabetes’ (2D BARI) study (19), information regarding DN presence was
available for 2,314 of 2,368 patients. This large number of
patients was divided into groups according to their diabetes
mellitus therapy, 1,669 patients received non-insulin therapies
(metformin and/or thiazolidinedione or a sulphonylurea), while 645
received insulin therapy. After adjusting for multiple cofactors
such as HbA1c and DM duration, the risk of DN remained over 30%
higher in patients who were taking insulin compared to patients who
were not taking insulin (OR=1.34, 95% CI 1.08-1.67) (19).
Hypertension is the most important and also an
independent risk factor for DN (20). Experimental studies compared the
impact of hypertension on nerve function in rodents with
streptozotocin-induced DM. Both groups of DM rodents with and
without hypertension showed thermal hyperalgesia, decreasing nerve
conduction, nerve ischemia and axonal atrophy. The group with
hypertension and DM showed thinly myelinated nerve fibres with
supernumerary Schwann cells and decreased nerve levels of myelin
basic protein. These alterations were not present in rodents
without hypertension. Overlapping diabetes on hypertension led to
modifications in nerve blood flow, conduction, axonal atrophy or
nerve ischemia, and increased the ratio of the thinly myelinated
fibres (21).
Dyslipidaemia is another risk factor that can
contribute to the development of DN since high levels of total
cholesterol, triglycerides, low-density lipoprotein cholesterol
(LDL-C) and high-density lipoprotein cholesterol (HDL-C) are
associated with an increased risk of neuropathy. Of all the lipid
fractions, triglycerides have the most significant effect on the
risk of neuropathy (22). In this
context, fibrate and statins may reduce DN occurrence (23). The presence of smoking is also
associated with increased DN prevalence (24). Indeed, the frequency of DN was
related to the number of packs of cigarettes smoked per year
(24). There are other factors
involved in DN development, including obesity, metabolic syndrome,
insulin resistance, alcohol consumption, platelet activation and
increased aggregability, low vitamin D, subclinical inflammation
(25,26), a paraneoplastic syndrome in
different cancers (27-29),
associated chemotherapy treatment (30), genetic factors (31), and increased oxidative stress
(32,33).
2. DN classification and diagnosis
The primary clinical forms of DN fall into three
broad categories considering pathophysiology and anatomy (31): i) Sensory DN with the following
types: Acute hyperglycemic neuropathy and chronic sensory-motor
neuropathy; ii) focal or multifocal DN that include
mononeuropathies (median, ulnar, radial nerve, and cranial nerves),
radiculopathies, plexopathies, amyotrophy; iii) autonomic
neuropathies that include: Cardiovascular autonomic neuropathy
manifesting as reduction of heart rate variation, tachycardia
during resting intervals, postural hypotension as well as sudden
cardiac death (especially malignant arrhythmias); gastrointestinal
autonomic neuropathy such as diabetic gastroparesis, colonic
hypomotility or hypermotility, and diabetic enteropathy;
genitourinary autonomic neuropathy meaning erectile, bladder and
sudomotor dysfunction.
The ADA advises physicians to use at least two
semi-quantitative tests to diagnose DN (8). The tests used to evaluate the
functioning of thin nerve fibres include the temperature perception
test, and the pinprick pain perception test, whereas those that
assess long nerve fibres function are the vibration perception
test, the monofilament touch perception test, and the evaluation of
ankle reflexes (8). The unity of at
least two tests is necessary to increase the specificity of DN
diagnosis (8). Confirmation of DN
diagnosis requires complex and rarely performed examinations such
as nerve conduction tests that demonstrate the slowing of nerve
conduction as a consequence of segmental demyelination of the axons
(34).
Autonomic DN includes a group of diseases in which
the nerve fibres belonging to the sympathetic and the
parasympathetic nervous system are damaged, especially
non-myelinated vegetative filaments (31). Autonomic DN can affect the cardiac,
digestive, urinary and genital systems, being often undiagnosed,
although it can occur within the first years after the diagnosis of
DM (35). Cardiac autonomic
neuropathy correlates with increased cardiac mortality (36). Its clinical manifestations include
resting sinus tachycardia, silent myocardial ischemia, diminished
tolerance to physical effort, orthostatic hypotension, syncope and
intra-operative cardiac instability (36). The prevalence of autonomic cardiac
neuropathy is approximately 30% in subjects with type 1 DM after 20
years of disease, and 60% in subjects with type 2 DM after 15 years
of disease progression (8). The
presence of autonomic cardiac neuropathy increases cardiovascular
risk, being involved either directly as a cause of cardiovascular
diseases, or indirectly as an aggravating factor of pre-existing
pathologies. Part of this risk is contributed to the presence of
silent myocardial infarction that occurs with a much higher
frequency in DM individuals (37).
Autonomic cardiac neuropathy also involves significant damage to
the parasympathetic system; this accentuates the predominance of
the sympathetic nervous system, which may produce a chronic
increase in blood pressure and eventually, hypertension (38). Nevertheless, DN does not spare the
sympathetic system; it can be affected by the appearance of
postural hypotension (35,36).
Sinus tachycardia occurs as a result of an imbalance
between the sympathetic and parasympathetic nervous systems over
the sinoatrial node (37),
different from atrial fibrillation (39). Cardiac neuropathy is also associated
with impaired diastolic filling (38). In the initial stages, sinus
tachycardia with a heart rate >90 bpm occurs, followed by sinus
tachycardia with a fixed frequency. For diagnosis tachycardia,
clinicians use bedside tests developed from Ewing's methods in
1970. It includes the analysis of R-R interval changes on the
electrocardiogram during deep breathing, standing, or Valsalva
manoeuvre (increased intrathoracic pressure) (38). Additionally, head-up-tilt-table test
or imaging techniques such as positron emission tomography (PET) or
[123I] meta-iodobenzylguanidine (MIBG) can be used in
dedicated centres (8). Autonomic DN
can affect the gastrointestinal tract (40,41).
Impairment of the sympathetic and parasympathetic nervous system
innervating the digestive tract, with the predominant loss of
inhibitory neurons and the imbalance between neuropeptides, can
lead to diarrhoea or constipation, gastroparesis, disorders of
oesophageal motility, faecal incontinence or biliary tract
dyskinesia (40,41). A series of tests are performed to
exclude other organic causes, most frequently
esophagogastroduodenoscopy, colonoscopy, or a barium study of the
stomach. The gold standard for diagnosing gastroparesis is
scintigraphy of digestible solids with the measurement of gastric
emptying (8).
At the urinary level, the clinical manifestation of
DN is bladder dysfunction (42).
The sensation of filling the bladder is no longer perceived, so
there is urinary retention, dysuria, nocturia, and incomplete
emptying. This can be evaluated by echography after voiding. In
later stages of the disease, control over the smooth sphincter is
lost, and thus urinary incontinence appears (43). The presence of bladder urine stasis
predisposes these patients to severe urinary infections (43). In men suffering from DM, sexual
dysfunction is three times more prevalent than in individuals with
normal glucose tolerance (44).
Sexual dysfunction, especially erectile dysfunction, is a
disability to obtain or maintain a normal erection for sexual
intercourse (44,45). The ‘International Index of Erectile
Function’ study is a validated diagnostic tool (46). The prevalence of erectile
dysfunction seems to be very high; in a study, 67% of the evaluated
subjects with DM were diagnosed with erectile dysfunction (44). A urologic examination is required
for these conditions. In women with DM, sexual dysfunction is
manifested by decreased libido and dyspareunia and should be
evaluated by the gynaecologist (47).
3. Current treatment options
Pathogenesis-oriented treatment
Glycaemic control
Glycaemic control is particularly important in the
primary and secondary prevention of distal symmetrical diabetic
polyneuropathy in patients with type 1 DM (12). The DCCT
study included 1,400 subjects with type 1 DM, which were randomly
divided into an intensive HbA1c target group (<6%), and a
conventional one (12). After a
follow-up period of around 6.5 years, HbA1c was 7.4% in the
intensive group and 9.1% in the conventional group (12). The prevalence of confirmed DN
markedly increased in the conventional treatment participants (from
5 to 17%; P<0.001), and only slightly among the intensive
treatment group participants (from 7 to 9%). Adjusting for the
presence of confirmed DN at baseline, the risk reduction for
incident DN with intensive glucose control during DCCT was 64% (95%
CI: 45-76, P<0.01). Subjects included in the DCCT study were
then followed up to observe the long-term effects of glycaemic
control on the incidence of microvascular and macrovascular DM
complications. Patients in the DCCT study who were included in the
conventional control arm were switched at the start of the
‘Epidemiology of Diabetes Interventions and Complications’ (EDIC)
study to an intensive treatment arm. It was observed that the HbA1c
difference between intensive and conventional glycemia treatment
groups in the DCCT study was rapidly reduced; by the fifth year of
EDIC follow-up, there was no statistically significant A1c division
(7.9% vs. 8.2%) (48). Prevalence
of DN was raised during EDIC follow-up in the two groups. Despite
no measurable difference in glucose control, a 30% risk decrease in
evolving DN was observed in patients with prior intensive glucose,
confirming that early benefits in achieving glucose control are
persistent over time (48). The
EDIC/DCCT studies demonstrated that good glycaemic management can
reduce DN occurrence and progression in subjects with type 1 DM and
that initial intensive glucose control maintains its benefits for a
long time (47,48).
On the other hand, glycaemic control seemed not to
influence the frequency of DN in type 2 DM subjects. Briefly, in
the UKPDS study (performed on 3,867 types 2 DM patients with a
similar methodology to that of the DCCT study) patients were
divided into the intensive and the conventional glucose control
(49). At 10 years, no significant
difference was observed regarding the prevalence of distal
symmetrical DN and autonomic cardiovascular neuropathy between the
two groups, in the intensive treatment group the average HbA1c was
7% while in the conventional treatment group the average HbA1c was
7.9%, P<0.01(49). The treatment
used for diabetic control, and not HbA1c decrease per se, could
have a role in neuropathy prevention. This explains the reason for
the population from BARI 2D, following treatment with insulin
sensitizers, having reduced chronic distal polyneuropathy incidence
(19). A meta-analysis, conducted
in 2011, analyzed six trials performed on 21,702 type 2 DM
individuals, showing no effect of intensive glucose control on DN
development or progression (50).
Similarly, in another meta-analysis, including 6,669 type 2 DM
patients from four studies, enhanced glucose control
non-significantly reduced the incidence of clinical neuropathy
(15).
Aldose-reductase inhibitors
In patients with DM, glucose metabolism via the
polyols pathway begins with the transformation of glucose into
sorbitol, a reaction catalyzed by aldose-reductase (51). Sorbitol exerts a robust osmotic
effect that alters Na+/K+-ATPase in neurons.
Aldose-reductase inhibitors act by decreasing the cellular levels
of sorbitol (51). Aldose-reductase
inhibitors were previously reported to improve symptoms and nerve
conduction in the motor nerves in patients with distal symmetrical
DN (52). However, a meta-analysis,
including 32 trials, demonstrated that aldose-reductase inhibitors
are no more effective than placebo in improving the symptoms of DN
and nerve conduction; thus the medication is not included in the
ADA guidelines (8,53). By contrast, another meta-analysis
(n=10 trials) showed that aldose-reductase inhibitors ameliorated
automatic cardiac neuropathy, mostly mild or asymptomatic cases
(54).
a-lipoic acid
α-lipoic acid (ALA) may reduce oxidative stress,
which is a central component in the etiopathogenesis of DN
(55). Hyperglycaemia enhances the
generation of reactive oxygen species (ROS) and depletes endogenous
antioxidant mechanisms (55). ROS
are crucial contributors to neuronal apoptosis, thus predisposing
to DN progression (55). Previous
studies in rodents have shown that ALA decreased lipid peroxidation
in a dose-dependent manner (56).
ALA has been used in DN, since nerve fibres, especially in the
myelin sheath, exhibit a large amount of lipids. The main action of
ALA is a ‘scavenger effect’ on lipophilic-free radicals (55). A series of experimental studies have
shown that ALA may improve the local blood flow and increase the
speed of nerve conduction in peripheral nerves (57).
In the ‘Alpha-Lipoic Acid in Diabetic Neuropathy’
(ALADIN) study, ALA was administered intravenously for three weeks
in subjects with symptomatic DN at a dose of 600 or 1,200 mg daily;
this treatment reduced the symptoms of DN without significant
adverse effects (58). Similarly,
in the ‘Oral Pilot’ (ORPIL) study, ALA, administered orally at a
dose of 600 mg for three weeks, decreased DN symptoms, including
pain, burning sensation, paraesthesia and numbness (59). The ‘Symptomatic Diabetic Neuropathy’
(SYDNEY) study demonstrated that, in addition to DN symptoms, nerve
conduction was also improved by ALA, administered intravenously for
five days in 14 perfusions (60).
In the SYDNEY 2 study, the oral 600 mg dose of ALA was proven the
most effective dose (among 600, 1,200 and 1,800 mg) in reducing
symptoms and with the fewest side effects during a follow-up of 5
weeks (61). A meta-analysis (4
studies) showed that ALA administered both orally and intravenously
can reduce the symptoms of DN as assessed by the ‘Total Symptom
Score’ (TSS), i.e., a scoring system for neuropathic symptoms
(burning, pain, numbness and paresthesia) (59). However, clinically relevant
reductions in TSS (i.e., >30%) were only observed with
intravenously administered ALA at 600 mg/day for 3 weeks, but not
with orally administered ALA at a dose of >600 mg/day for 3-5
weeks (62). Another meta-analysis
(15 trials) revealed that the intravenous administration of ALA at
a dose of 300-600 mg/day for 2-4 weeks significantly elevated the
nerve conduction velocity and positive neuropathic symptoms
(63).
Benfotiamine
Benfotiamine is a synthetic derivative form of
vitamin B1 that is highly soluble in lipids. Thiamine is recognized
as a cofactor of an enzyme known as transketolase, which is part of
the fructose-6 phosphate metabolism and glyceraldehyde-3-phosphate
metabolism by pentose-pathway, leading to their conversion to
pentose-5 phosphates and other sugars (64). In DM, a thiamine deficiency is
frequently present, partially attributed to an increased renal
clearance of this vitamin; serum thiamine levels were 75% lower in
patients with DM than in healthy subjects (65). By administering benfotiamine,
fundamental pathogenetic pathways involved in the onset of DN are
inhibited (i.e., the hexosamine and the diacylglycerol-protein
kinase C pathways), thus resulting in the reduced formation of
advanced glycosylation products (66). In animal studies, benfotiamine given
to rodents reduced inflammatory and neuropathic nociception
(66). Furthermore, in rodents with
streptozotocin-induced DM, thiamine, and benfotiamine significantly
decreased advanced glycosylation end products levels (67).
In patients with DM, benfotiamine (orally
administered at a dose of 100 mg, four times a day, for three
weeks) was reported to reduce the symptoms of neuropathy (68). In another study, benfotiamine was
given in combination with vitamin B6 and B12 at two different doses
(i.e., high: 320 mg/day and medium: 150 mg/day), as well as
monotherapy (150 mg/day) for 6 weeks in 36 DM patients with DN
(69). Both symptoms and
semi-quantitative tests were improved in all the groups with the
best results being obtained in the patients receiving the highest
dose of benfotiamine (69). Other
findings have shown that benfotiamine, in combination with
pyridoxine, not only reduces DN symptoms but also increases the
speed of nerve conduction (70).
Overall, benfotiamine significantly improves the symptoms of DN in
DM patients, the benefit being greater with a higher amount and
longer duration of treatment (71).
Symptomatic treatment
Symptomatic treatment aims to significantly reduce
self-reported pain in the lower limbs by 30-50% and thus improve
the quality of life (8). A series
of symptomatic medications are included in the guidelines by the
‘American Academy of Neurology’ (AAN) (72) (Table
I) or the ‘European Federation of Neurological Societies’
(EFNS) (73). Beneficial results
have been obtained with tricyclic antidepressants (for example
amitriptyline), serotonin reuptake inhibitors, such as duloxetine
(74,75) or opioids (76) or pregabalin (77) and gabapentin (78). The ADA recommends duloxetine as a
first-line treatment for the symptoms of painful DN, the other
alternative being pregabalin (Table
II) (8). Previous findings
demonstrated the efficacy of duloxetine for the treatment of pain
in patients with DN. The usually administered dose is 60 or 120
mg/day (74). Duloxetine at a dose
of 60 mg/day is safe and effective in the treatment of DN, but it
should be elided in patients with liver disease and/or advanced
chronic kidney disease. Administration of >60 mg/day is not
indicated since efficacy is not significantly higher, and the side
effects are greater (74). Of note,
duloxetine is cost-effective compared to other drugs used in DN
treatment (75). A meta-analysis of
23 studies confirmed the efficacy of duloxetine in the symptomatic
treatment of DN (79).
 | Table IRecommendations of the American
Neurology Association (AAN) for the treatment of symptoms of
painful symmetrical polyneuropathy. |
Table I
Recommendations of the American
Neurology Association (AAN) for the treatment of symptoms of
painful symmetrical polyneuropathy.
| Level of
recommendation | Drug | Effective dose | Not recommended
drugs |
|---|
| A | Pregabalin | 300-600 mg/day | Oxcarbazepine |
| B | Gabapentin | 500-1,200
mg/day | Lamotrigine |
| | Duloxetine | 60-120 mg/day | Clonidine |
| | Venlafaxine | 75-225 mg/day | Laser therapy with
low intensity |
| | Sodium
valproate | 500-1,200
mg/day | |
| | Amitriptyline | 25-100 mg/day | |
| | Tramadol | 210 mg/day | |
| | Capsaicin | 0.075% topic use 4
times a day | |
| Table IIRecommendations of the American
Diabetes Association (ADA) regarding therapeutic options for
symptomatic diabetic neuropathy. |
Table II
Recommendations of the American
Diabetes Association (ADA) regarding therapeutic options for
symptomatic diabetic neuropathy.
| Level of
recommendation | Therapeutic
class | Active
substance | Effective
dosage | Observations |
|---|
| A | Anticonvulsant | Pregabalin | 300-600 mg/day | FDA approved |
| | | | | Side effects:
Ataxia, blurred vision, constipation, diplopia, dizziness,
drowsiness, fatigue |
| | Serotonin reuptake
inhibitors | Duloxetine | 60-120 mg/day | FDA approved |
| B | Anticonvulsant | Gabapentin | 900-3,600
mg/day | More important side
effects than pregabalin |
| | Tricyclic
antidepressant | Amitriptyline | 25-100 mg/day | Important side
effects: Cardiotoxicity, hepatotoxicity, suicidal ideation, risk of
fractures |
| E | Opioids | Tramadol | 210 mg/day | Significant side
effects: Drowsiness, nausea, vomiting, constipation, arrhythmias,
shortness of breath, seizures, addiction |
| | | Tapentadol | Immediate release:
700 mg/day, day 1 then 60 mg/day Prolonged release: 50 mg twice a
day | Important side
effects: Drowsiness, nausea, vomiting, constipation, arrhythmias,
shortness of breath, seizures, addiction |
Furthermore, tramadol was more effective than
placebo in treating pain in patients with DN given at a dose of 200
mg/day, also improving patients' quality of life (80). Overall, tramadol, in combination
with paracetamol, is useful in the symptomatic therapy of DN by
reducing the severity of pain, improving sleep and quality of life
(81).
4. Experimental treatment
As technology advances, novel biomarkers and
diagnostic procedures for DN are implemented (82,83),
leading to innovative therapies.
Experimental drug treatment for DN includes
vixotirgine, a voltage-gated sodium-channel agonist (84); trazodone/pregabalin combination, a
combination between a second-generation antidepressant with
sedative activity and an anticonvulsant that has been effective in
reducing symptoms (85);
olodanrigan, an angiotensin 2 type 2 receptor antagonist (86); inhibitors of enkephalinases that
increase the concentrations of enkephalin substances known for
their natural analgesic proprieties (87); and vitamin D which can improve mood
and decrease pain severity as shown in small trials (88).
Capsaicin can be used as topical treatment based on
the local tissue reduction in P-substance responsible for pain
sensation (89,90) but is not generally recommended
because it can determine a reversible loss of small epidermal
fibres (8).
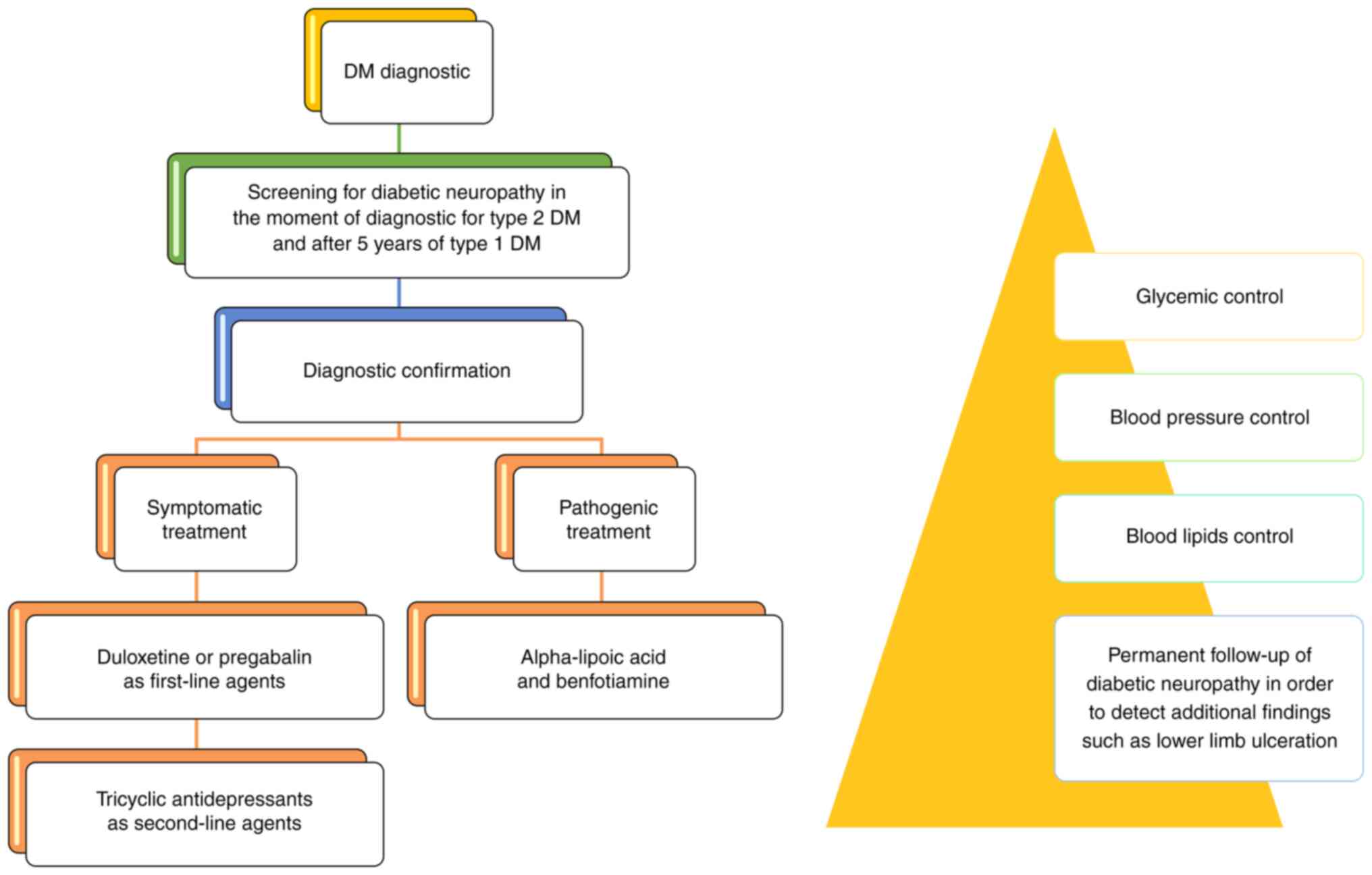
5. Suggestions for a therapeutic
approach
DN treatment needs a multitarget approach, as
depicted in Fig. 1. In our opinion,
no treatment is effective if metabolic control is not achieved.
Regulation of glucose, blood pressure and lipids are key components
of a reliable approach for reducing the progression of DN since
nerve fibres are highly sensitive to hyperglycaemia, hypertension
and hyperlipidaemia by the generation of excessive free radicals in
the nervous tissue or plasma (8).
Therefore, patients may benefit from both symptomatic and
pathogenic treatment. The quality of life is also very important,
and symptomatic treatment can improve it by the use of drugs such
as duloxetine, pregabalin or gabapentin (8,71).
Some guidelines do not refer to pathogenetic therapy, such as ALA
or benfotiamine. However, proof exists that, especially ALA
administered intravenously is effective in reducing neuropathic
pain and improving nerve conduction (58). Overall, pathogenic treatment can,
not only promote specific nerve function, but also improve the
patient's symptoms as a consequence of neuroprotection against
oxidative stress and advanced glycosylation end products (55,56,67,68).
In clinical practice, ALA is usually administered intravenously for
10-14 days, at a dose of 600 mg/day, followed by a long term oral
administration of a combination of ALA (600 mg/day) and
benfotiamine 300 mg/day.
6. Conclusions
Timely diagnosis of DN is required to avoid several
complications, including lower limb amputations and cardiac
arrhythmias. Glucose, blood pressure and lipids control are of high
importance in DN therapy. Symptomatic treatment improves the
quality of life of patients. Of note, pathogenetic therapeutic
agents such as ALA and benfotiamine should not be ignored as they
have shown positive results in clinical practice.
Acknowledgements
Fig. 1 was made by
CMV in PowerPoint, using only information from clinical
practice.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
AB, APS, MP, CMV conceived the structure of the
review. ARP, NK, RAS and CD collected the data and performed the
literature search. NP, CMV, MS, and RAS revised the study for
intellectual content. All authors were involved in writing the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
NK has given talks, attended conferences and
participated in trials sponsored by Astra Zeneca, Bausch Health,
Boehringer Ingelheim, Elpen, Mylan, Novo Nordisk, Sanofi and
Servier. APS is currently Vice President of the Romanian National
Diabetes Committee and has given talks, attended conferences and
participated in advisory boards sponsored by Astra Zeneca, Novo
Nordisk, Sanofi, Medtronic, Roche, Lilly, Merck, Amgen and
Coca-Cola. NP has been an advisory board member of Astra-Zeneca,
Boehringer Ingelheim, MSD, Novo Nordisk, Pfizer, Takeda and
TrigoCare International; has participated in sponsored studies by
Astra-Zeneca, Eli-Lilly, GSK, MSD, Novo Nordisk, Novartis and
Sanofi-Aventis; has received honoraria as a speaker for
Astra-Zeneca, Boehringer Ingelheim, Eli-Lilly, Elpen, MSD, Mylan,
Novo Nordisk, Pfizer, Sanofi-Aventis and Vianex; and attended
conferences sponsored by TrigoCare International, Eli-Lilly,
Galenica, Novo Nordisk, Pfizer and Sanofi-Aventis. RAS has attended
conferences sponsored by Novo Nordisk, Worwag Pharma, Eli-Lilly.
The remaining authors have no competing interests to declare.
References
|
1
|
Bansal V, Kalita J and Misra UK: Diabetic
neuropathy. Postgrad Med J. 82:95–100. 2006.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kaur S, Pandhi P and Dutta P: Painful
diabetic neuropathy: An update. Ann Neurosci. 18:168–175.
2011.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Román-Pintos LM, Villegas-Rivera G,
Rodríguez-Carrizalez AD, Miranda-Díaz AG and Cardona-Muñoz EG:
Diabetic polyneuropathy in type 2 diabetes mellitus: Inflammation,
oxidative stress, and mitochondrial function. J Diabetes Res.
2016(3425617)2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Dyck PJ, Kratz KM, Karnes JL, Litchy WJ,
Klein R, Pach JM, Wilson DM, O'Brien PC, Melton LJ III and Service
FJ: The prevalence by staged severity of various types of diabetic
neuropathy, retinopathy, and nephropathy in a population-based
cohort: The rochester diabetic neuropathy study. Neurology.
43:817–824. 1993.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Young MJ, Boulton AJ, MacLeod AF, Williams
DR and Sonksen PH: A multicentre study of the prevalence of
diabetic peripheral neuropathy in the United Kingdom hospital
clinic population. Diabetologia. 36:150–154. 1993.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Jaiswal M, Lauer A, Martin CL, Bell RA,
Divers J, Dabelea D, Pettitt DJ, Saydah S, Pihoker C, Standiford
DA, et al: SEARCH for Diabetes in Youth Study Group: Peripheral
neuropathy in adolescents and young adults with type 1 and type 2
diabetes from the SEARCH for Diabetes in Youth follow-up cohort: A
pilot study. Diabetes Care. 36:3903–3908. 2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Veresiu AI, Bondor CI, Florea B, Vinik EJ,
Vinik AI and Gâvan NA: Detection of undisclosed neuropathy and
assessment of its impact on quality of life: A survey in 25,000
Romanian patients with diabetes. J Diabetes Complications.
29:644–649. 2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Pop-Busui R, Boulton AJ, Feldman EL, Bril
V, Freeman R, Malik RA, Sosenko JM and Ziegler D: Diabetic
neuropathy: A position statement by the American diabetes
association. Diabetes Care. 40:136–154. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Vinik AI: Advances in diabetes for the
millennium: New treatments for diabetic neuropathies. MedGenMed. 6
(3 Suppl)(S13)2004.PubMed/NCBI
|
|
10
|
Rathmann W, Ziegler D, Jahnke M, Haastert
B and Gries FA: Mortality in diabetic patients with cardiovascular
autonomic neuropathy. Diabet Med. 10:820–824. 1993.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Bansal D, Gudala K, Muthyala H, Esam HP,
Nayakallu R and Bhansali A: Prevalence and risk factors of
development of peripheral diabetic neuropathy in type 2 diabetes
mellitus in a tertiary care setting. J Diabetes Investig.
5:714–721. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Diabetes Control and Complications Trial
Research Group. Nathan DM, Genuth S, Lachin J, Cleary P, Crofford
O, Davis M, Rand L and Siebert C: The effect of intensive treatment
of diabetes on the development and progression of long-term
complications in insulin-dependent diabetes mellitus. N Engl J Med.
329:977–986. 1993.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Klein R, Klein BE and Moss SE: Relation of
glycemic control to diabetic microvascular complications in
diabetes mellitus. Ann Intern Med. 124:90–96. 1996.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Tesfaye S, Chaturvedi N, Eaton SE, Ward
JD, Manes C, Ionescu-Tirgoviste C, Witte DR and Fuller JH: EURODIAB
Prospective Complications Study Group. Vascular risk factors and
diabetic neuropathy. N Engl J Med. 352:341–350. 2005.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Action to Control Cardiovascular Risk in
Diabetes Study Group. Gerstein HC, Miller ME, Byington RP, Goff DC
Jr, Bigger JT, Buse JB, Cushman WC, Genuth S, Ismail-Beigi F, et
al: Effects of intensive glucose lowering in type 2 diabetes. N
Engl J Med. 358:2545–2559. 2008.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Callaghan BC, Little AA, Feldman EL and
Hughes RA: Enhanced glucose control for preventing and treating
diabetic neuropathy. Cochrane Database Syst Rev.
6(CD007543)2012.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ismail-Beigi F, Craven T, Banerji MA,
Basile J, Calles J, Cohen RM, Cuddihy R, Cushman WC, Genuth S,
Grimm RH Jr, et al: Effect of intensive treatment of hyperglycaemia
on microvascular outcomes in type 2 diabetes: An analysis of the
ACCORD randomized trial. Lancet. 376:419–430. 2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Gaede P, Vedel P, Larsen N, Jensen GV,
Parving HH and Pedersen O: Multifactorial intervention and
cardiovascular disease in patients with type 2 diabetes. N Engl J
Med. 348:383–393. 2003.PubMed/NCBI View Article : Google Scholar
|
|
19
|
BARI 2D Study Group. Frye RL, August P,
Brooks MM, Hardison RM, Kelsey SF, MacGregor JM, Orchard TJ,
Chaitman BR, Genuth SM, et al: A randomized trial of therapies for
type 2 diabetes and coronary artery disease. N Engl J Med.
360:2503–2515. 2009.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Ardeleanu V, Toma A, Pafili K, Papanas N,
Motofei I, Diaconu CC, Rizzo M and Stoian AP: Current
pharmacological treatment of painful diabetic neuropathy: A
narrative review. Medicina (Kaunas). 56(25)2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Gregory JA, Jolivalt CG, Goor J, Mizisin
AP and Calcutt NA: Hypertension-induced peripheral neuropathy and
the combined effects of hypertension and diabetes on nerve
structure and function in rats. Acta Neuropathol. 124:561–573.
2012.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Elliott J, Tesfaye S, Chaturvedi N, Gandhi
RA, Stevens LK, Emery C and Fuller JH: EURODIAB Prospective
Complications Study Group: Large-fiber dysfunction in diabetic
peripheral neuropathy is predicted by cardiovascular risk factors.
Diabetes Care. 32:1896–1900. 2009.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Perez-Matos MC, Morales-Alvarez MC and
Mendivil CO: Lipids: A suitable therapeutic target in diabetic
neuropathy? J Diabetes Res. 2017(6943851)2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Clair C, Cohen MJ, Eichler F, Selby KJ and
Rigotti NA: The effect of cigarette smoking on diabetic peripheral
neuropathy: A systematic review and meta-analysis. J Gen Intern
Med. 30:1193–1203. 2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Papanas N and Ziegler D: Risk factors and
comorbidities in diabetic neuropathy: An update 2015. Rev Diabet
Stud. 12:48–62. 2015.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Tesfaye S, Stevens LK, Stephenson JM,
Fuller JH, Plater M, Ionescu-Tirgoviste C, Nuber A, Pozza G and
Ward JD: Prevalence of diabetic peripheral neuropathy and its
relation to glycaemic control and potential risk factors: The
EURODIAB IDDM complications study. Diabetologia. 39:1377–1384.
1996.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Mazilu L, Stanculeanu DL, Gheorghe AD,
Suceveanu AP, Parepa IR, Stoian Pantea A and Suceveanu AI: Clinical
impact of association between diabetes and lung cancer. Rev Chim.
70:1149–1151. 2019.
|
|
28
|
Suceveanu AI, Suceveanu AP, Gheorghe AD
and Mazilu L: Diabetes and cancer-is there a link? In: Diabetes and
its complications, Gaber AR (ed). InTech, pp119-137, 2017.
|
|
29
|
Suceveanu AI, Mazilu L, Nitipir C, Stoian
AP, Parepa I, Voinea C and Suceveanu AP: Diabetes mellitus raise
the risk for interval colorectal cancer and advanced adenomas. Rev
Chim. 70:1808–1811. 2019.
|
|
30
|
Mazilu L, Stanculeanu DL, Gheorghe AD,
Voinea F, Suceveanu AP, Pituru S, Diaconu CC, Parepa IR, Pantea
Stoian A, Pop CS and Suceveanu AI: Incidence of chemotherapy
induced peripheral neuropathy in cancer patients in clinical
practice. Farmacia. 66:904–908. 2018.
|
|
31
|
Boulton AJ, Vinik AI, Arezzo JC, Bril V,
Feldman EL, Freeman R, Malik RA, Maser RE, Sosenko JM and Ziegler
D: American Diabetes Association. Diabetic neuropathies: A
statement by the American Diabetes Association. Diabetes Care.
28:956–962. 2005.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Gheorghe G, Stoian AP, Gaman M, Socea B,
Neagu TP, Stanescu AMA, Bratu OG, Mischianu DLD, Suceveanu AI and
Diaconu CC: The benefits and risks of antioxidant treatment in
liver diseases. Rev Chim. 70:651–655. 2019.
|
|
33
|
Stoian AP, Mitrofan G, Colceag F,
Suceveanu AI, Hainarosie R, Pituru S, Diaconu CC, Timofte D,
Nitipir C, Poiana C and Serafinceanu C: Oxidative stress in
diabetes. A model of complex thinking applied in medicine. Rev
Chim. 69:2515–2519. 2018.
|
|
34
|
Bromberg MB: An electrodiagnostic approach
to the evaluation of peripheral neuropathies. Phys Med Rehabil Clin
N Am. 24:153–168. 2013.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Verrotti A, Prezioso G, Scattoni R and
Chiarelli F: Autonomic neuropathy in diabetes mellitus. Front
Endocrinol (Lausanne). 5(205)2014.
|
|
36
|
Serhiyenko VA and Serhiyenko AA: Cardiac
autonomic neuropathy: Risk factors, diagnosis and treatment. World
J Diabetes. 9:1–24. 2018.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Vinik AI, Erbas T and Casellini CM:
Diabetic cardiac autonomic neuropathy, inflammation and
cardiovascular disease. J Diabetes Investig. 4:4–18.
2013.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Vinik AI and Ziegler D: Diabetic
cardiovascular autonomic neuropathy. Circulation. 115:387–397.
2007.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Gaman MA, Dobrica EC, Pascu EG, Cozma MA,
Epingeac ME, Gaman AM, Pantea Stoian AM, Bratu OG and Diaconu CC:
Cardio metabolic risk factors for atrial fibrillation in type 2
diabetes mellitus: Focus on hypertension, metabolic syndrome and
obesity. J Mind Med Sci. 6:157–161. 2019.
|
|
40
|
Yarandi SS and Srinivasan S: Diabetic
gastrointestinal motility disorders and the role of enteric nervous
system: Current status and future directions. Neurogastroenterol
Motil. 26:611–624. 2014.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Parkman HP, Yates K, Hasler WL, Nguyen L,
Pasricha PJ, Snape WJ, Farrugia G, Koch KL, Calles J, Abell TL, et
al: Similarities and differences between diabetic and idiopathic
gastroparesis. Clin Gastroenterol Hepatol. 9:1056–1064.
2011.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Yuan Z, Tang Z, He C and Tang W: Diabetic
cystopathy: A review. J Diabetes. 7:442–447. 2015.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Zaha DC, Kiss R, Hegedűs C, Gesztelyi R,
Bombicz M, Muresan M, Pallag A, Zrinyi M, Pall D, Vesa CM and Micle
O: Recent advances in investigation, prevention, and management of
healthcare-associated infections (HAIs): Resistant multidrug strain
colonization and its risk factors in an intensive care unit of a
university hospital. Biomed Res Int. 2019(2510875)2019.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Maiorino MI, Bellastella G and Esposito K:
Diabetes and sexual dysfunction: Current perspectives. Diabetes
Metab Syndr Obes. 7:95–105. 2014.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Sáenz de Tejada I, Angulo J, Cellek S,
González-Cadavid N, Heaton J, Pickard R and Simonsen U:
Pathophysiology of erectile dysfunction. J Sex Med. 2:26–39.
2005.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Rhoden EL, Telöken C, Sogari PR and Vargas
Souto CA: The use of the simplified international index of erectile
function (IIEF-5) as a diagnostic tool to study the prevalence of
erectile dysfunction. Int J Impot Res. 14:245–250. 2002.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Enzlin P, Rosen R, Wiegel M, Brown J,
Wessells H, Gatcomb P, Rutledge B, Chan KL and Cleary PA: DCCT/EDIC
Research Group. Sexual dysfunction in women with type 1 diabetes:
Long-term findings from the DCCT/EDIC study cohort. Diabetes Care.
32:780–785. 2009.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Pop-Busui R, Herman WH, Feldman EL, Low
PA, Martin CL, Cleary PA, Waberski BH, Lachin JM and Albers JW:
DCCT/EDIC Research Group. DCCT and EDIC studies in type 1 diabetes:
Lessons for diabetic neuropathy regarding metabolic memory and
natural history. Curr Diab Rep. 10:276–282. 2010.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Intensive blood-glucose control with
sulphonylureas or insulin compared with conventional treatment and
risk of complications in patients with type 2 diabetes (UKPDS 33).
UK prospective diabetes study (UKPDS) group. Lancet. 352:837–853.
1998.PubMed/NCBI
|
|
50
|
Boussageon R, Bejan-Angoulvant T,
Saadatian-Elahi M, Lafont S, Bergeonneau C, Kassaï B, Erpeldinger
S, Wright JM, Gueyffier F and Cornu C: Effect of intensive glucose
lowering treatment on all cause mortality, cardiovascular death,
and microvascular events in type 2 diabetes: Meta-analysis of
randomized controlled trials. BMJ. 343(d4169)2011.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Ramirez MA and Borja NL: Epalrestat: An
aldose reductase inhibitor for the treatment of diabetic
neuropathy. Pharmacotherapy. 28:646–655. 2008.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Sharma SR and Sharma N: Epalrestat, an
aldose reductase inhibitor, in diabetic neuropathy: An Indian
perspective. Ann Indian Acad Neurol. 11:231–235. 2008.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Chalk C, Benstead TJ and Moore F: Aldose
reductase inhibitors for the treatment of diabetic polyneuropathy.
Cochrane Database Syst Rev: CD004572, 2007.
|
|
54
|
Hu X, Li S, Yang G, Liu H, Boden G and Li
L: Efficacy and safety of aldose reductase inhibitor for the
treatment of diabetic cardiovascular autonomic neuropathy:
Systematic review and meta-analysis. PLoS One.
9(e87096)2014.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Vallianou N, Evangelopoulos A and Koutalas
P: Alpha-lipoic acid and diabetic neuropathy. Rev Diabet Stud.
6:230–236. 2009.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Nickander KK, McPhee BR, Low PA and
Tritschler H: Alpha-lipoic acid: Antioxidant potency against lipid
peroxidation of neural tissues in vitro and implications for
diabetic neuropathy. Free Radic Biol Med. 21:631–639.
1996.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Nagamatsu M, Nickander KK, Schmelzer JD,
Raya A, Wittrock DA, Tritschler H and Low PA: Lipoic acid improves
nerve blood flow, reduces oxidative stress, and improves distal
nerve conduction in experimental diabetic neuropathy. Diabetes
Care. 18:1160–1167. 1995.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Ziegler D, Hanefeld M, Ruhnau KJ, Meissner
HP, Lobisch M, Schütte K and Gries FA: Treatment of symptomatic
diabetic peripheral neuropathy with the anti-oxidant alpha-lipoic
acid. A 3-week multicentre randomized controlled trial (ALADIN
Study). Diabetologia. 38:1425–1433. 1995.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Ruhnau KJ, Meissner HP, Finn JR,
Reljanovic M, Lobisch M, Schütte K, Nehrdich D, Tritschler HJ,
Mehnert H and Ziegler D: Effects of 3-week oral treatment with the
antioxidant thioctic acid (alpha-lipoic acid) in symptomatic
diabetic polyneuropathy. Diabet Med. 16:1040–1043. 1999.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Ametov AS, Barinov A, Dyck PJ, Hermann R,
Kozlova N, Litchy WJ, Low PA, Nehrdich D, Novosadova M, O'Brien PC,
et al: The sensory symptoms of diabetic polyneuropathy are improved
with alpha-lipoic acid: The SYDNEY trial. Diabetes Care.
26:770–776. 2003.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Ziegler D, Ametov A, Barinov A, Dyck PJ,
Gurieva I, Low PA, Munzel U, Yakhno N, Raz I, Novosadova M, et al:
Oral treatment with alpha-lipoic acid improves symptomatic diabetic
polyneuropathy: The SYDNEY 2 trial. Diabetes Care. 29:2365–2370.
2006.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Mijnhout GS, Kollen BJ, Alkhalaf A,
Kleefstra N and Bilo HJ: Alpha lipoic acid for symptomatic
peripheral neuropathy in patients with diabetes: A meta-analysis of
randomized controlled trials. Int J Endocrinol.
2012(456279)2012.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Han T, Bai J, Liu W and Hu Y: A systematic
review and meta-analysis of α-lipoic acid in the treatment of
diabetic peripheral neuropathy. Eur J Endocrinol. 167:465–471.
2012.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Pácal L, Kuricová K and Kaňková K:
Evidence for altered thiamine metabolism in diabetes: Is there a
potential to oppose gluco- and lipotoxicity by rational
supplementation? World J Diabetes. 5:288–295. 2014.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Thornalley PJ, Jahan I and Ng R:
Suppression of the accumulation of triosephosphates and increased
formation of methylglyoxal in human red blood cells during
hyperglycaemia by thiamine in vitro. J Biochem. 129:543–549.
2001.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Hammes HP, Du X, Edelstein D, Taguchi T,
Matsumura T, Ju Q, Lin J, Bierhaus A, Nawroth P, Hannak D, et al:
Benfotiamine blocks three major pathways of hyperglycemic damage
and prevents experimental diabetic retinopathy. Nat Med. 9:294–299.
2003.PubMed/NCBI View
Article : Google Scholar
|
|
67
|
Sánchez-Ramírez GM, Caram-Salas NL,
Rocha-González HI, Vidal-Cantú GC, Medina-Santillán R, Reyes-García
G and Granados-Soto V: Benfotiamine relieves inflammatory and
neuropathic pain in rats. Eur J Pharmacol. 530:48–53.
2006.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Haupt E, Ledermann H and Köpcke W:
Benfotiamine in the treatment of diabetic polyneuropathy-a
three-week randomized, controlled pilot study (BEDIP study). Int J
Clin Pharmacol Ther. 43:71–77. 2005.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Winkler G, Pál B, Nagybéganyi E, Ory I,
Porochnavec M and Kempler P: Effectiveness of different
benfotiamine dosage regimens in the treatment of painful diabetic
neuropathy. Arzneimittelforschung. 49:220–224. 1999.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Nikolić A, Kacar A, Lavrnić D, Basta I and
Apostolski S: The effect of benfothiamine in the therapy of
diabetic polyneuropathy. Srp Arh Celok Lek. 137:594–600.
2009.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Stracke H, Gaus W, Achenbach U, Federlin K
and Bretzel RG: Benfotiamine in diabetic polyneuropathy (BENDIP):
Results of a randomised, double blind, placebo-controlled clinical
study. Exp Clin Endocrinol Diabetes. 116:600–605. 2008.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Bril V, England J, Franklin GM, Backonja
M, Cohen J, Del Toro D, Feldman E, Iverson DJ, Perkins B, Russell
JW, et al: Evidence-based guideline: Treatment of painful diabetic
neuropathy: Report of the American academy of neurology, the
American association of neuromuscular and electrodiagnostic
medicine, and the American academy of physical medicine and
rehabilitation. Neurology. 76:1758–1765. 2011.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Attal N, Cruccu G, Baron R, Haanpää M,
Hansson P, Jensen TS and Nurmikko T: European Federation of
Neurological Societies. EFNS guidelines on the pharmacological
treatment of neuropathic pain: 2010 revision. Eur J Neurol.
17:1113–e88. 2010.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Goldstein DJ, Lu Y, Detke MJ, Lee TC and
Iyengar S: Duloxetine vs. placebo in patients with painful diabetic
neuropathy. Pain. 116:109–118. 2005.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Ormseth MJ, Scholz BA and Boomershine CS:
Duloxetine in the management of diabetic peripheral neuropathic
pain. Patient Prefer Adherence. 5:343–356. 2011.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Gilron I, Bailey JM, Tu D, Holden RR,
Weaver DF and Houlden RL: Morphine, gabapentin, or their
combination for neuropathic pain. N Engl J Med. 352:1324–1334.
2005.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Rosenstock J, Tuchman M, LaMoreaux L and
Sharma U: Pregabalin for the treatment of painful diabetic
peripheral neuropathy: A double-blind, placebo-controlled trial.
Pain. 110:628–638. 2004.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Wiffen P, Collins S, McQuay H, Carroll D,
Jadad A and Moore A: Anticonvulsant drugs for acute and chronic
pain. Cochrane Database Syst Rev. (CD001133)2000.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Hossain SM, Hussain SM and Ekram AR:
Duloxetine in painful diabetic neuropathy: A systematic review.
Clin J Pain. 32:1005–1010. 2016.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Harati Y, Gooch C, Swenson M, Edelman S,
Greene D, Raskin P, Donofrio P, Cornblath D, Sachdeo R, Siu CO and
Kamin M: Double-blind randomized trial of tramadol for the
treatment of the pain of diabetic neuropathy. Neurology.
50:1842–1846. 1998.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Freeman R, Raskin P, Hewitt DJ, Vorsanger
GJ, Jordan DM, Xiang J and Rosenthal NR: CAPSS-237 Study Group.
Randomized study of tramadol/acetaminophen versus placebo in
painful diabetic peripheral neuropathy. Curr Med Res Opin.
23:147–161. 2007.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Ghita MA, Caruntu C, Lixandru D, Pitea A,
Batani A and Boda D: The quest for novel biomarkers in early
diagnosis of diabetic neuropathy. Curr Proteomics. 14:86–99.
2017.
|
|
83
|
Caruntu C, Negrei C, Boda D, Constantin C,
Caruntu A and Neagu M: Biotechnological advances for diagnosis of
peripheral diabetic neuropathy. Rom Biotechnol Lett. 19:9846–9858.
2014.
|
|
84
|
Alsaloum M, Estacion M, Almomani R,
Gerrits MM, Bönhof GJ, Ziegler D, Malik R, Ferdousi M, Lauria G,
Merkies IS, et al: A gain-of-function sodium channel β2-subunit
mutation in painful diabetic neuropathy. Mol Pain.
15(1744806919849802)2019.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Mendelson WB: A review of the evidence for
the efficacy and safety of trazodone in insomnia. J Clin
Psychiatry. 66:469–476. 2005.PubMed/NCBI View Article : Google Scholar
|
|
86
|
Keppel Hesselink JM and Schatman ME:
EMA401: An old antagonist of the AT2R for a new indication in
neuropathic pain. J Pain Res. 10:439–443. 2017.PubMed/NCBI View Article : Google Scholar
|
|
87
|
Tesfaye S: PL37: A new hope in the
treatment of painful diabetic neuropathy? Pain Manag. 6:129–132.
2016.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Ghadiri-Anari A, Mozafari Z, Gholami S,
Khodaei SA, Aboutorabi-Zarchi M, Sepehri F, Nadjarzade A, Rahmanian
M and Namiranian N: Dose vitamin D supplementations improve
peripheral diabetic neuropathy? A before-after clinical trial.
Diabetes Metab Syndr. 13:890–893. 2019.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Căruntu C, Negrei C, Ghiţă MA, Căruntu A,
Bădărău AI, Buraga I, Boda D, Albu A and Brănişteanu D: Capsaicin,
a hot topic in skin pharmacology and physiology. Farmacia.
63:487–491. 2015.
|
|
90
|
Căruntu C and Boda D: Evaluation through
in vivo reflectance confocal microscopy of the cutaneous neurogenic
inflammatory reaction induced by capsaicin in human subjects. J
Biomed Opt. 17(085003)2012.PubMed/NCBI View Article : Google Scholar
|