Introduction
After a severe burn injury, the wound healing
response involves the dynamic interaction of many
pathophysiological processes such as inflammation, proliferation,
and tissue remodeling (1). The
first phase consists of releasing a prolonged immune response
(cytokines and chemokines in the endothelium) that activates
proinflammatory effector cells at the site of injury and increases
vasodilation and tissue edema (2).
In early inflammation, increased levels of proinflammatory
cytokines bring neutrophils and monocytes to the site (3). Further, proteolytic enzymes, such as
matrix metalloproteinases (MMPs), are released from neutrophils
(4). MMPs are the main class of
enzymes responsible for the degradation or resorption of all
extracellular matrix (ECM) components (5,6).
Consequently, in acute inflammation, MMPs break down
the ECM and basement membranes and contribute to vascular
permeability in burn injury by stimulating remodeling of the
connective tissue (7). The ideal
tissue remodeling after injury requires a balance between MMPs and
their tissue inhibitors (TIMPs), increasing TIMPs, resulting in
either the accumulation of ECM or fibrosis. Simultaneously, the
decrease in TIMPs leads to intense matrix proteolysis (5-8).
Virtually, any imbalance between MMPs and TIMPs may lead to low
healing processes such as chronic wounds or excessive healing,
including hypertrophic scars and keloids (9).
Several studies have shown that matrix
metalloproteinase-9 (MMP-9) and its tissue inhibitor (TIMP-1) are
increased in plasma after thermal injury (10-12).
MMP-9 is a dynamic marker, which is released from neutrophil
granulocytes very early, according to the literature just 1-3 h
after the triggering insult (13,14).
TIMP-1 is known to inhibit the catalytic activity of MMP-9 in a 1:1
stoichiometric relationship (15).
Circulating levels of TIMP-1 are maximal two days after a severe
burn (11). Unfortunately, the role
of MMP-9 and TIMP-1 in early inflammation associated with a burn
injury is poorly understood.
As no prospective study has specifically examined
the serum levels of MMP-9 and TIMP-1 in the early shock phase of
burn-injured patients, we aimed to detect early changes, activity
dynamics, and predictive value of MMP-9, TIMP-1, and the
MMP-9/TIMP-1 ratio to better understand the early repair mechanisms
for the development of future therapies for patients with thermal
burns.
Patients and methods
Patients and study protocol
This prospective study enrolled 25 patients with
burn wounds (16 males/9 females, mean age 49.40±17.55 years)
admitted to the Clinical Emergency Hospital for Plastic,
Reconstructive, and Burns Surgery in Bucharest, between 2018 and
2019. All cases had domestic accidents and among the reported
comorbidities, high blood pressure was present in 4 patients. No
history of diabetes or allergic reactions were reported.
The severity of burn trauma is represented by the
burn depth and burn size. Burn size can be estimated by reference
to the total body surface area (TBSA) using several methods [palms
rule (16), nines rule (16), Lund and Browder chart (17), and mobile applications (17)]. Inclusion criteria included thermal
burns with a TBSA affected by the burn <25% and patients over 18
years of age. All burn patients were clinically assessed and
presented with second- and third-degree burns. According to the
updated guidelines for burn care (European Practice Guidelines for
Burn Care), the treatment strategies for patients were carried out
(18) and local protocols were
followed. All patients were examined at admission and after 2 and 7
days. Exclusion criteria were as follows: i) patients of age under
18 years; ii) patients presenting with known cancer disease; iii)
patients presenting with chronic heart failure or renal failure;
iv) patients presenting with primary or secondary immunosuppressive
disorders; v) patients receiving previous treatment with
immunosuppressive drugs affecting the body's inflammatory response
to burns (systemic corticosteroids); vi) patients receiving
antibiotics from the tetracycline group, especially doxycycline
(known as an MMP inhibitor) (19).
In addition, 30 healthy subjects (19 males/11
females, mean age 49.7±8.04 years) were randomly selected and were
similar in regards to the age and sex of the cases.
The study conformed to the principles outlined in
the Declaration of Helsinki and was approved by the Clinical
Emergency Hospital's Ethics Committee for Plastic, Reconstructive,
and Burns Surgery. Written informed consent was obtained from
enrolled patients or their legal representatives and
volunteers.
Blood sample collection and
processing
Blood samples were collected by venous puncture into
BD Vacutainer® SST™ Tubes (purchased from Becton,
Dickinson and Company) as soon as possible after admission of the
patients with burn wounds at the emergency department and following
that at 48 h and 7 days. The serum samples were obtained by
centrifugation at 2,500 x g for 15 min after 30 min of clotting
time at room temperature. Serum samples were then immediately
aliquoted into labelled cryo-vials and stored at -70˚C until
further analysis.
Detection of serum MMP-9 and TIMP-1 by
ELISA
The quantitative determination of serum MMP-9 and
TIMP-1 concentrations was performed using ELISA kits purchased from
R&D Systems Inc. for human MMP-9 (cat. no. DMP900) and TIMP-1
(cat. no. DTM100), according to the manufacturer's instructions.
Contamination may lead to falsely high serum concentrations. As
MMP-9 and TIMP-1 are present in saliva, protective measures were
taken to prevent contamination during the test. For both MMP-9 and
TIMP-1, three serum samples of known concentration were tested 10
times on one plate to assess intra-assay precision and in 20
separate assays to assess inter-assay precision. The intra-assay
precision values were identical to those of the inter-assay study
with coefficients of variation (CVs) ranging from 2 to 7.9%. The
within CVs for MMP-9 were 1.9% at a mean concentration of 204 ng/ml
and for TIMP-1 were 3.9% at a mean concentration of 127 ng/ml. The
MMP-9/TIMP-1 ratio was calculated using the following formula:
MMP-9 (ng/ml)/TIMP-1 (ng/ml). All assays were performed in
duplicate and in such a way, this minimized any effects of repeated
freeze-thaw cycles.
Statistical analysis
Statistical analysis was conducted by using SPSS
version 25 software (IBM Corp.). The difference between MMP-9 and
TIMP-1 serum concentrations measured in dynamics was analyzed by
one-way ANOVA test, comparing their evolution during the 7-day
monitoring period from the initial burn injury. The
Anderson-Darling, Shapiro-Wilk, and Kolmogorov-Smirnov tests were
also used to verify the data obtained after preliminary analysis
and to check the group's consistency. The diagnostic power of the
MMP-9 and TIMP-1 biomarkers was assessed by calculating the areas
under the receiver operating characteristic (ROC) curves (AUC). The
ROC curves were plotted using as a variable the value of MMP-9,
TIMP-1, or MMP-9/TIMP-1 ratio for patients admitted to the
emergency department compared to the healthy controls, and as a
classification criterion, the TBSA burn <25%. The AUC is an
overall summary of diagnostic accuracy as follows: AUC >0.9,
excellent diagnostic accuracy; AUC between 0.7 and 0.9, good
diagnostic accuracy; AUC between 0.5 and 0.7, poor diagnostic
accuracy; AUC <0.5, lack of diagnostic value of the biomarker
(20). ROC curves have determined
cut-off values for optimal sensitivity and specificity. For all
tests, the significance level for statistical analysis was set at
P-values <0.05.
Results
Dynamics of MMP-9, TIMP-1, and
MMP-9/TIMP-1 ratio
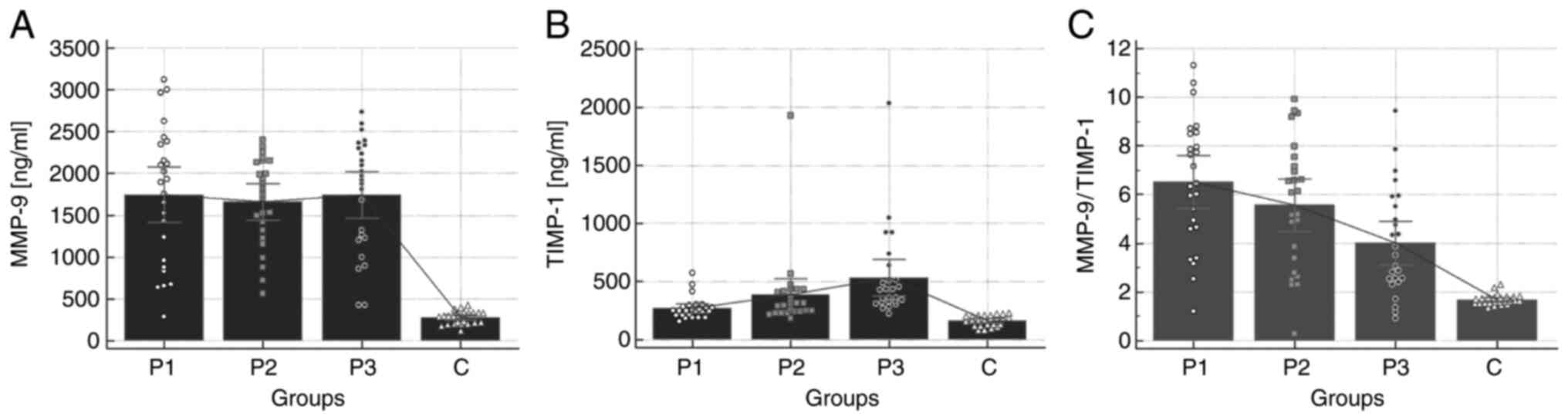
Fig. 1 depicts the
dynamics of MMP-9, TIMP-1, and the MMP-9/TIMP-1 ratio in patients
with burn injury compared to the healthy control group.
Serum MMP-9 concentrations upon admission (P1) and
on days 2 (P2) and 7 (P3) were significantly higher in the burn
patients than that in the healthy control group (C) (P1, 1,744.19
ng/ml; P2, 1,659.62 ng/ml; P3, 1,744.95 ml vs. C, 279.36
ng/ml, P<0.001). Basically, MMP-9 levels were maintained at a
plateau throughout the trial period of 7 days (Fig. 1A).
TIMP-1 showed an increasing tendency during the
entire study period (P1, 269.92 ng/ml; P2, 385.86 ng/ml; P3, 534.71
ng/ml vs. C, 166.68 ng/ml, P=0.023), its levels being significantly
higher on days 2 to 7 compared to admission levels (Fig. 1B).
The time course of the MMP-9/TIMP-1 ratio followed
the inverse dynamics of TIMP-1. MMP-9/TIMP-1 ratios were
significantly higher in the burn patients at all time points of the
study (regardless of harvest time) compared to the healthy controls
(P1, 6.51; P2, 5.58; P3, 4.008 vs. C, 1.68, P<0.001), following
a continuous decrease from the day of admission until the end of
the 7-day study interval (Fig.
1C).
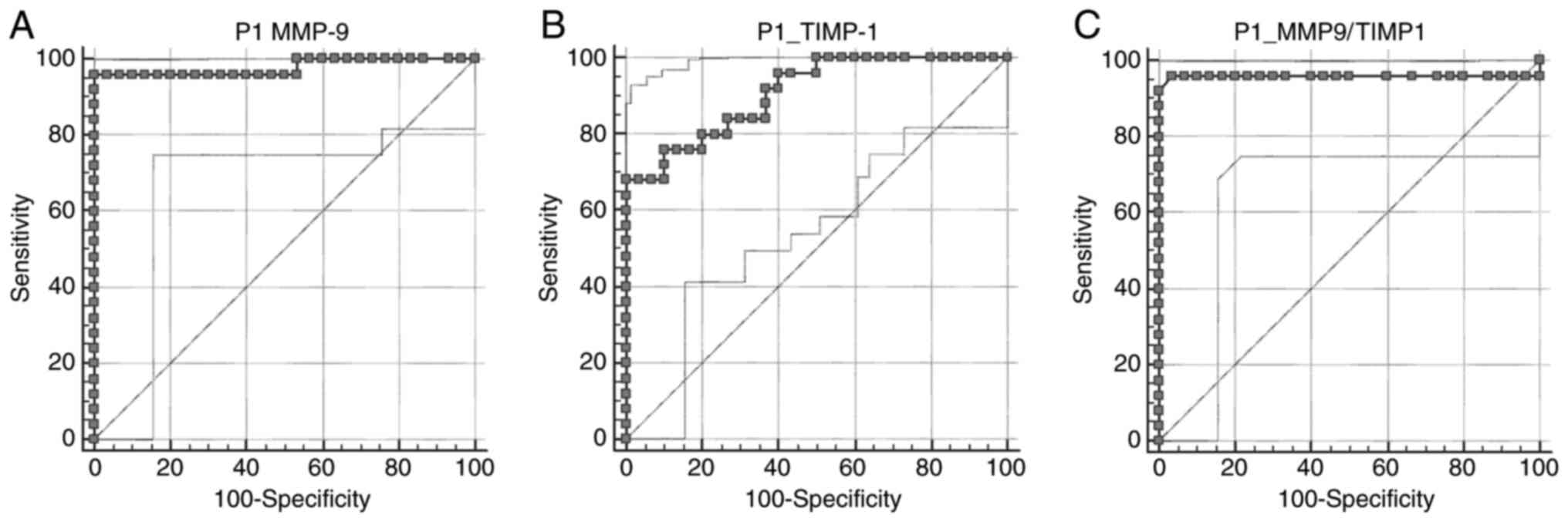
Analysis of the ROC curves for MMP-9,
TIMP-1, and MMP-9/TIMP-1 ratio
The second objective of the present study was to
compare the predictive value of MMP-9 with TIMP-1 and the
MMP-9/TIMP-1 ratio in patients with burn injuries. The analysis of
the ROC curves was performed to test the predictive value of the
three biomarkers. AUC usually ranges from 0.5 to 1, with values
close to 1 indicating a high discriminatory ability. As shown in
Fig. 2, all biomarkers had a very
high AUC of over 0.90; the P-value being statistically significant
in all analyzed cases.
The largest AUC was for MMP-9 (0.979); MMP-9
demonstrating an excellent accuracy for patients with TBSA affected
by the burn <25% (Fig. 2A). The
ROC curve showed that these patients tended to have an MMP-9 value
higher than 421.5 ng/ml. This cut-off point was calculated for a
sensitivity of 96% and a specificity of 100%.
Analysis of the ROC curve for the TIMP-1 biomarker
showed that patients with TBSA affected by the burn <25% tended
to have a TIMP-1 value greater than 231.6 ng/ml; the cut-off point
calculated for a sensitivity of 68% and a specificity of 100%
(Fig. 2B). The AUC for TIMP-1 was
very large (0.908) (P<0.001).
Considering the MMP-9/TIMP-1 ratio, AUC was
extremely large (0.959) (P<0.001). Patients with a TBSA affected
by the burn <25% tended to have an MMP-9/TIMP-1 ratio greater
than 2.31; the cut-off point calculated for a sensitivity of 96%
and a specificity of 96.67% (Fig.
2C).
Discussion
The main findings of the current study were the
following: i) MMP-9 serum levels were increased immediately after
injury and remained at a plateau, while TIMP-1 showed an upward
trend throughout the study period and the time course of
MMP-9/TIMP-1 followed the inverse dynamics of TIMP-1; ii) the
relationship between the MMP-9-TIMP-1 system and the extent of the
injury was highly statistically significant (P<0.001); iii)
analysis of the ROC curves showed that patients with a TBSA
affected by the burn <5% tended to have an MMP-9 value higher
than 421.5 ng/ml (AUC=0.979), a TIMP-1 value higher than 231.6
ng/ml (AUC=0.908), and an MMP-9/TIMP-1 ratio higher than 2.31
(AUC=0.959).
The most common complications after burns are sepsis
and respiratory, cardiac, and kidney failure, with the leading
causes of death being heart failure (67%) and respiratory failure
(33%) (13). None of the patients
enrolled in the study had septic complications, but our case series
included patients in a good health state and without a history of
major non-communicable diseases, such as diabetes, which could
influence the evolution of the burns (21). Although most studies have
investigated MMP-9 or TIMP-1 immunohistochemical reactivity
(4,22), we decided to measure the serum level
of biomarkers. Our decision was based on the following arguments:
i) MMP-9, or TIMP-1 immunohistochemical reactivity may not
correspond to in vivo enzymatic activity (12); ii) the study group was compared with
the control group of healthy volunteers, without thermal injury.
Moreover, the MMP-9 and TIMP-1 biomarkers were analyzed concerning
the clinical variables and the outcome at 48 h and 7 days after
injury. We hypothesized that the 7-day study interval opens a wide
window of time that may be sufficient to detect both ascending and
descending inflammatory responses; the 7-day period being the time
interval in which the systemic inflammatory response syndrome
post-injury usually occurs (14).
Starting with the idea that MMP-9 and TIMP-1 are
dynamic biomarkers released very early after the triggering insult,
we considered it useful to measure the changes in their serum
concentrations, depending on the evolution of inflammation for one
week. Dynamic changes in circulating levels of MMP-9 and TIMP-1
demonstrate their involvement in the early response after thermal
injury. A moderate increase in MMP-9 serum concentration is
beneficial because the epithelialization rate is partially
dependent on the presence of collagen. However, when the
physiological balance between protease and their inhibitors is
broken, the patient outcome is unfavorable (9). Our results showed an early increase in
the MMP-9 level, most likely due to its rapid release from
neutrophil granulocytes, over minutes to a few hours after the
triggering insult (P1, 1744.19 ng/ml vs. C, 279.36 ng/ml,
P<0.001). Other studies described a significantly lower level of
MMP-9 on days 4 to 6 (14,23). In contrast to these studies, in the
present study, MMP-9 levels were maintained at a plateau throughout
the trial period of 7 days, which may lead us to the hypothesis
that an early increased expression of MMP-9 (cut-off, 412.5 ng/ml)
could be associated with a better-quality scar and the
maintenance/decrease in MMP-9 serum concentrations may be an
indicator for better survival.
Several authors found significantly higher TIMP-1
concentrations in the plasma of TBSA <20% burn patients relative
to healthy controls, with a median time to peak TIMP-1
concentration at 2.09 days (10,11,14).
In contrast to these studies, our results showed that TIMP-1
presented an increasing tendency during the entire study period,
its levels being significantly higher on days 2 to 7 compared to
admission levels. According to the findings of Ulrich et al
(11), TIMP-1 serum expression has
been correlated with the TBSA% of injury; patients with TBSA
affected by the burn <25% tending to have a TIMP-1 value greater
than 231.6 ng/ml. The high response of TIMP-1 to burns could
explain the lower serum levels of MMP-9 than expected in our
study.
As shown in Fig. 1,
at all-time points of the study, the differences between serum
concentrations of MMP-9 and its inhibitor TIMP-1 in the study group
compared to the control group were statistically significant, with
the time-course of the MMP-9/TIMP-1 ratio following the inverse
dynamics of TIMP-1. The constant decrease in the MMP-9/TIMP-1 ratio
throughout the trial period of 7 days (decrease in 14.28% at 2 days
and decrease in 38.43% at 7 days from the value measured from
admission) indicates that the patients with a TBSA affected by the
burn <25% have an effective healing process without hypertrophic
scars and keloids.
Monitoring the levels of MMP-9 was not the most
accurate indicator of the time elapsed from the initial injury.
TIMP-1 proved to be better in this respect, and the MMP-9/TIMP-1
ratio showed the best sensitivity and specificity.
Healing processes evolve, as clinical practice
demonstrates, after necrotic tissues fall off. The factors
influencing local changes are not entirely known, but we can
hypothesize that local proteinases can be responsible for tissue
remodeling. In this respect, MMP-9 or TIMP-1 monitoring could prove
to be useful markers for local changes over time, indicating the
need for eventual surgery or other therapeutic approaches.
The main limitation of our work is related to the
small number of patients included. However, despite the small
sample size, we used a homogenous population because none of the
patients enrolled in our study had septic complications.
In summary, our study found a significant increase
in serum levels of MMP-9 and TIMP-1 in patients with a TBSA
affected by the burn <25%, compared to unaffected controls.
Although the variations in the two biomarkers were different
regarding the time of the initial insult, their ratio is a specific
and sensitive indicator of burn evolutivity. Further investigations
comparing local and general protease responses after such trauma
may provide new insights into the mechanism involved in burn wound
healing. Detailed studies are needed to elucidate the exact
sequence of local events that occur in the first 7 days after
severe burn injury to better predict when local inflammation
triggers systemic inflammatory processes.
Acknowledgements
Not applicable.
Funding
Funding: This research did not receive any specific grant from
any funding agency in the public, commercial or not-for-profit
sector.
Availability of data and materials
All data generated or analyzed during this study are
included in the manuscript.
Authors' contributions
AES and AZCA conceived and planned the experiments.
Experiments were performed by AES. AZCA, FLF, and MMS performed
statistical analysis of the results. AES, AZCA, MMS, MG, RH, FLF
and DCG contributed to the interpretation of the results. AES took
the lead in writing the manuscript. All authors provided critical
feedback and helped shape the research, analysis, and manuscript.
All authors read and approved the final manuscript for
publication.
Ethics approval and consent to
participate
The study conformed to the principles outlined in
the Declaration of Helsinki and was approved by the Clinical
Emergency Hospital for Plastic, Reconstructive, and Burns Surgery
Ethics Committee (approval no. 6627/04.10.2017). Written informed
consent was obtained from the enrolled patients or their legal
representatives and volunteers.
Patient consent for publication
Not applicable.
Authors' information
Adina Elena Stanciu: ORCID ID: https://orcid.org/0000-0002-9494-6686.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lateef Z, Stuart G, Jones N, Mercer A,
Fleming S and Wise L: The cutaneous inflammatory response to
thermal burn injury in a murine model. Int J Mol Sci.
20(538)2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Hofmann E, Fink J, Eberl A, Prugger EM,
Kolb D, Luze H, Schwingenschuh S, Birngruber T, Magnes C, Mautner
SI, et al: A novel human ex vivo skin model to study early local
responses to burn injuries. Sci Rep. 11(364)2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Suceveanu AI, Mazilu L, Katsiki N, Parepa
I, Voinea F, Pantea-Stoian A, Rizzo M, Botea F, Herlea V, Serban D
and Suceveanu AP: NLRP3 inflammasome biomarker-could be the new
tool for improved cardiometabolic syndrome outcome. Metabolites.
10(448)2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Yu G, Li Y, Ye L, Wang X, Zhang J, Dong Z
and Jiang D: Exogenous peripheral blood mononuclear cells affect
the healing process of deep-degree burns. Mol Med Rep.
16:8110–8122. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Cabral-Pacheco GA, Garza-Veloz I,
Castruita-De la Rosa C, Ramirez-Acuña JM, Perez-Romero BA,
Guerrero-Rodriguez JF, Martinez-Avila N and Martinez-Fierro ML: The
roles of matrix metalloproteinases and their inhibitors in human
diseases. Int J Mol Sci. 21(9739)2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Raeeszadeh-Sarmazdeh M, Do LD and Hritz
BG: Metalloproteinases and their inhibitors: Potential for the
development of new therapeutics. Cells. 9(1313)2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Plichta JK, Holmes CJ, Gamelli RL and
Radek KA: Local burn injury promotes defects in the epidermal lipid
and antimicrobial peptide barriers in human autograft skin and burn
margin: Implications for burn wound healing and graft survival. J
Burn Care Res. 38:e212–e226. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Tokuhara CK, Santesso MR, Oliveira GSN,
Ventura TMDS, Doyama JT, Zambuzzi WF and Oliveira RC: Updating the
role of matrix metalloproteinases in mineralized tissue and related
diseases. J Appl Oral Sci. 27(e20180596)2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Guo HF, Ali RM, Hamid RA, Chang SK, Rahman
MH, Zainal Z and Khaza'ai H: Temporal changes in the cell
population and wound healing-related gene expression in deep
partial-thickness burn wound model. Biomed Dermatol 4, 2020.
|
|
10
|
Dasu MR, Spies M, Barrow RE and Herndon
DN: Matrix metalloproteinases and their tissue inhibitors in
severely burned children. Wound Repair Regen. 11:177–180.
2003.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ulrich D, Noah EM, von Heimburg D and
Pallua N: TIMP-1, MMP-2, MMP-9, and PIINP as serum markers for skin
fibrosis in patients following severe burn trauma. Plast Reconstr
Surg. 111:1423–1431. 2003.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Hästbacka J, Fredén F, Hult M, Bergquist
M, Wilkman E, Vuola J, Sorsa T, Tervahartiala T and Huss F: Matrix
Metalloproteinases-8 and -9 and tissue inhibitor of
metalloproteinase-1 in burn patients. A prospective observational
study. PLoS One. 10(e0125918)2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Lang TC, Zhao R, Kim A, Wijewardena A,
Vandervord J, Xue M and Jackson CJ: A critical update of the
assessment and acute management of patients with severe burns. Adv
Wound Care (New Rochelle). 8:607–633. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Nagy B, Szelig L, Rendeki S, Loibl C,
Rézmán B, Lantos J, Bogár L and Csontos C: Dynamic changes of
matrix metalloproteinase 9 and tissue inhibitor of
metalloproteinase 1 after burn injury. J Crit Care. 30:162–166.
2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Stanciu AE, Zamfir-Chiru-Anton A, Stanciu
MM, Pantea-Stoian A, Nitipir C and Gheorghe DC: Serum melatonin is
inversely associated with matrix metalloproteinase-9 in oral
squamous cell carcinoma. Oncol Lett. 19:3011–3020. 2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Giretzlehner M, Dirnberger J, Owen R,
Haller HL, Lumenta DB and Kamolz LP: The determination of total
burn surface area: How much difference? Burns. 39:1107–1113.
2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Chong HP, Quinn L, Jeeves A, Cooksey R,
Lodge M, Carney B and Molony D: A comparison study of methods for
estimation of a burn surface area: Lund and Browder, e-burn and
Mersey Burns. Burns. 46:483–489. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Brychta P and Magnette A: the Executive
Committee and PAM Committee of European Burn Association (EBA)
(2017). European Practice Guidelines for Burn Care 2017. Available
from: https://www.euroburn.org/wp-content/uploads/EBA-Guidelines-Version-4-2017.pdf.
|
|
19
|
Stagg HW, Whaley JG, Tharakan B, Hunter
FA, Jupiter D, Little DC, Davis ML, Smythe WR and Childs EW:
Doxycycline attenuates burn induced microvascular
hyperpermeability. J Trauma Acute Care Surg. 75:1040–1046.
2013.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Stanciu AE, Zamfir-Chiru-Anton A, Stanciu
MM, Stoian AP, Jinga V, Nitipir C, Bucur A, Pituru TS, Arsene AL,
Dragoi CM, et al: Clinical significance of serum melatonin in
predicting the severity of oral squamous cell carcinoma. Oncol
Lett. 19:1537–1543. 2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Stoian Pantea A, Mitrofan G and Colceag F:
Oxidative Stress in Diabetes. A model of complex thinking applied
in medicine. Rev Chim. 96:2515–2519. 2018.
|
|
22
|
Stanciu AE: Cytokines in heart failure.
Adv Clin Chem. 93:63–113. 2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Lorente L, Martin MM, Labarta L, Diaz C,
Solé-Violán J, Blanquer J, Orbe J, Rodriguez JA, Jimenez A,
Borreguero-Leon JM, et al: Matrix metalloproteinase-9, -10, and
tissue inhibitor of matrix metalloproteinases-1 blood levels as
biomarkers of severity and mortality in sepsis. Crit Care.
13(R158)2009.PubMed/NCBI View
Article : Google Scholar
|