Introduction
Intertrochanteric fractures are common to elderly
patients and show an increased morbidity and a higher risk of
mortality, especially within the first year (1,2).
According to the literature, over one-third of all hip fractures
are intertrochanteric (3,4). The main goal of surgical treatment is
to restore patient mobility. The ideal treatment allows immediate
weight-bearing on the affected limb, but this requires an
acceptable reduction and a secured fixation of the fracture. An
early mobilization significantly decreases the risk of
postoperative complications such as pneumonia, deep vein
thrombosis, pulmonary embolism or death (5-7).
In the last decade, cephalomedullary nailing has become the most
popular surgical treatment for pertrochanteric fractures (8,9). The
main benefit of the intramedullary nail is considered the early
mobilization and the possibility of an aggressive
rehabilitation.
There are still controversies around the long-term
benefits and risk of complications after fixation using short or
long cephalomedullary nails after unstable intertrochanteric
fractures. Some studies report that the short nail does not provide
an adequate diaphyseal fixation; thus, the risk of femoral fracture
at the tip of the implant may be higher. On the other hand, with
the newer nail designs available, this risk has significantly
decreased (10-14).
Considering that in Romania there are not many
articles regarding this subject, we aimed to conduct a study to
compare the ambulatory function of patients with intertrochanteric
fractures surgically fixed with either short or long
cephalomedullary nails (Gamma 3 Nail, Stryker MedEd).
Patients and methods
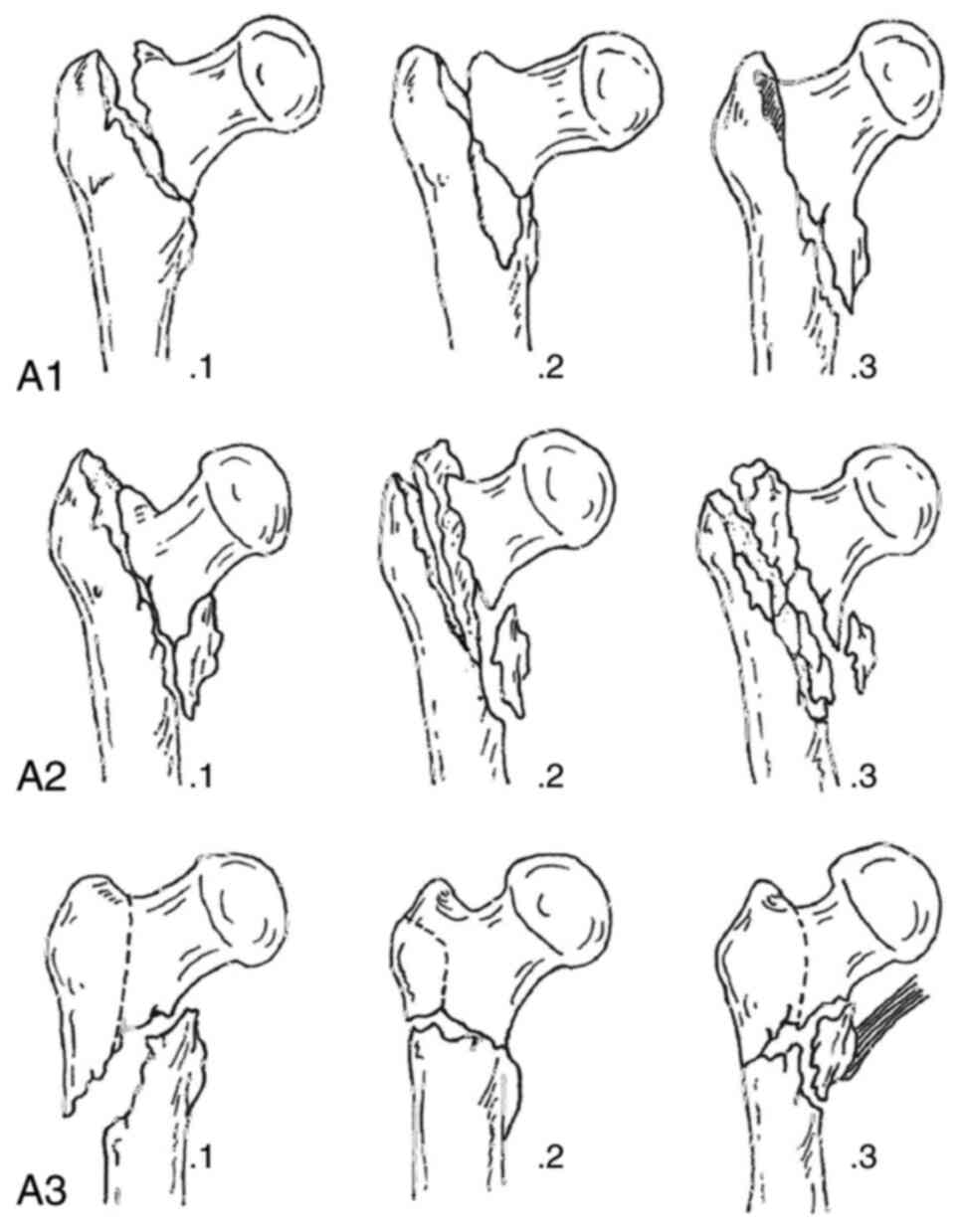
This randomized prospective single center study was
conducted between May 2017 and April 2020 and 61 patients with
unstable (AO 31-A2) and intertrochanteric fractures (AO 31-A3) were
included (Fig. 1). From the
patients initially reviewed, 5 were lost during the follow-up and 3
were deceased before the first year of assessment; thus, they were
excluded from our study. Patients with stable trochanteric
fractures (AO 31-A1), bone tumors, subtrochanteric fractures and
polytrauma were also excluded from this research. Among the studied
cases, 26 patients underwent internal fixation using a short nail
system and 27 using the long nail system.
The study was approved by the Ethics Committee of
‘Foişor’ Orthopaedics-Traumatology and Osteoarticular TB Hospital
in Bucharest, Romania. All patients provided a signed informed
consent. The choice of implant was based on the randomization of
the cases using sealed envelopes prepared by an independent
individual, which contained the instructions regarding the type of
fixation. The nails used in this paper and available in our center
were the standard 180-mm Stryker Gamma3 Trochanteric Nail (Stryker
MedEd) (Stryker for the short nail group and Stryker Gamma3 Long
Nail for the long nail group, both with a 135 degree proximal nail
angle. The distal screw was locked for the short nail and dynamic
for the long nail. The diameters were 11 mm for both types of
nail.
All patients received a spinal or general anesthesia
with preoperative antibiotics (1 g cefuroxime and postoperative
antibiotics for 24 h). Patients were positioned supine on the
fracture table, and the fracture was reduced under fluoroscopic
guidance while applying traction and internal rotation of the lower
limb. After the surgical preparation and draping, the patients were
treated according to the Stryker Gamma 3 nail surgical technique
recommended by the manufacturer. For the long nail group, a
previous reaming 2 mm larger than the distal nail diameter was
used. In all cases, the position of the lag screw was assessed and
measured using the tip-apex distance (TAD) (15). The surgical time, surgical blood
loss and length of stay were recorded for each case.
All cases followed the standard rehabilitation
protocol if the patient's clinical status and the nail stability
allowed it. It consisted of assisted walking with weight bearing as
tolerated using a walking frame for 6 weeks. All patients were
followed up at 3 weeks, 6 weeks, 3 months, 6 months and 12 months,
and clinical and functional assessments were undertaken by a
different surgeon blinded to the type of treatment received. X-rays
were taken each time, in order to evaluate the fracture union and
complications. The Visual Analogue Scale (VAS), Harris Hip Score
(HHS) (16) and Functional
Ambulation Category scale (FAC) were also used for the
assessment.
The VAS is a subjective index, used in our study to
determine the amount of pain, which consists of a score between 0
(minimum) and 10 (maximum). This scale is considered a reliable and
simple tool for describing the pain intensity felt by the patient
(17).
The HHS was originally developed in 1969 and was
intended to evaluate hip disabilities and various types of
treatment (16). It is a
questionnaire that covers mainly four domains which are pain, range
of motion, function and the absence of deformities (16). The maximum score is 100. The higher
the score, the better the patient outcome. A score below 70 is
equivalent to a poor functional result.
The FAC scale, first described by Holden et
al in 1984, ranges from 0 (nonfunctional ambulatory) and 5
(independent ambulatory) and evaluates the amount of human support
the patients require while walking (18). It is a quick, simply to use and easy
to interpret test that requires only stairs and an indoor floor
with a length of at least 15 m (19) (Table
I).
 | Table IFunctional ambulatory category (FAC)
scale. |
Table I
Functional ambulatory category (FAC)
scale.
| Score | Category | Interpretation |
|---|
| 0 | Nonfunctional
ambulatory | Patient cannot
ambulate, requires more than one person to ambulate safely |
| 1 | Ambulatory, dependent
for physical assistance Level II | Patient requires
continuous manual contact to support body weight and to maintain
balance or assist coordination |
| 2 | Ambulatory, dependent
for physical assistance Level I | Patient requires
intermittent or continuous light touch to assist balance or
coordination |
| 3 | Ambulatory, dependent
for supervision | Patient can ambulate
on level surfaces without manual contact of another person but
requires supervision for guarding or verbal cueing |
| 4 | Ambulatory,
independent only on leveled surfaces | Patient can ambulate
independently on level surfaces but requires supervision or
physical assistance on stairs, inclines or other non-level
surfaces |
| 5 | Ambulatory,
independent | Patient can ambulate
independently on non-level and level surfaces, stairs and
inclines |
Statistical analysis was performed using SPSS
version 27.0. Continuous variables were compared between the groups
using the independent sample t-test and Mann-Whitney U test. The
categorical variables were compared using the Chi Square test. A
P-value <0.5 was considered as indicative of a statistically
significant difference.
Results
The baseline characteristics of the patients are
presented in Table II. Out of the
53 patients included, 42 (79.2%) had a 31.A2 fracture (21 in the
long nail group and 21 in the short nail group) and 11 patients
(20.8%) had a 31.A3 fracture (6 in the long nail group and 5 in the
short nail group). Both groups presented comparable results
regarding the age of the patients included (P=0.67), sex (P=0.67),
and length of hospital stay (P=0.07). The surgical time was
significantly longer (P<0.05) in the long nail group, the
average time recorded being 81.38 (±12.01) min, while the result
for the short nail group was 53.11 (±8.36) min. In addition, the
blood loss was significantly higher (P<0.05) in the patients
treated with long nails (210±12.1 ml) compared to the short nail
group (75.4±14.8). Even though the surgical time was significantly
longer for the long nail group, the length of hospital stay showed
no significant difference (P=0.07). The average TAD was 17.8±1.69
mm for the long nail group and 18.1±1.53 mm for the short nail
group; thus, the differences were not statistically significant
(P=0.98). The fracture union time was 11.9±2.51 for the long nail
group and 12.2±2.36 for the short nail group (P=0.28).
| Table IIBaseline characteristics and
intraoperative data. |
Table II
Baseline characteristics and
intraoperative data.
| | Long nail (n=27) | Short nail
(n=26) | P-value |
|---|
| Unstable
(AO31-A2) | 21 (77.7%) | 21 (80.7%) | n/a |
| Transtrochanteric
(AO31-A3) | 6 (22.2%) | 5 (19.3%) | n/a |
| Age, mean
(years) | 78.07±5.03 | 78.65±4.84 | 0.67 |
| Sex (M/F) | 13/14 | 14/12 | 0.678 |
| Surgical time
(min) | 81.38±12.01 | 53.11±8.36 | <0.05 |
| Length of hospital
stay (days) | 9.07±1.32 | 8.5±0.88 | 0.07 |
| Estimative blood loss
(ml) | 210±12.1 | 75.4±14.8 | <0.05 |
| TAD (mm) | 17.8±1.69 | 18.1±1.53 | 0.98 |
The results at each follow-up are presented in
Table III. No statistical
differences were noted regarding the VAS score at 1 day after
surgery (P=0.74), 6 weeks (P=0.56), 6 months (P=0.86) and 12 months
(P=0.40). At 6 months, the HHS demonstrated a statistical
difference (P<0.05) with a better result for the short nail
group (84.76±3.68). At 12 months, we recorded no significant
differences between the groups (P=0.15). Regarding the FAC scale,
no significant differences were noted either before the fracture
(P=0.465) or after 12 months (P=0.28).
| Table IIIVAS, HHS and FAC scale average results
during each follow-up. |
Table III
VAS, HHS and FAC scale average results
during each follow-up.
| | Follow-up time | Long nail (n=27) | Short nail
(n=26) | P-value |
|---|
| VAS | 1 day | 5.92±1.38 | 5.8±1.26 | 0.74 |
| | 6 weeks | 3.44±1.05 | 3.11±1.07 | 0.56 |
| | 6 months | 1.81±1.17 | 1.8±1.09 | 0.86 |
| | 12 months | 0.51±0.7 | 0.3±0.47 | 0.406 |
| HHS | 6 months | 82.37±3.79 | 84.76±3.68 | <0.05 |
| | 12 months | 87.29±3.43 | 88.53±3.32 | 0.15 |
| FAC | Preoperative | 4.14±0.86 | 4.34±0.74 | 0.465 |
| | 12 months | 3.7±0.84 | 4.03±0.72 | 0.28 |
Proximal screw cut-out occurred in 2 cases in the
short nail group and 1 case from the long nail group, which
resulted in reoperations that consisted of total hip replacement
for all cases. The screw position was optimal, except for the case
with the long implant, where the screw position was eccentric on
the lateral view. Only 1 peri-implant fracture occurred distal to
the implant, in a case with a long cephalomedullary nail; it was
treated with open reduction and internal fixation with plates and
screws. No other complications were recorded in our study, except a
single case with local postoperative hematoma that did not require
reintervention.
Discussion
The goal of treatment in the management of
pertrochanteric fractures is to allow weight-bearing as soon as
possible and to avoid the complications following prolonged
immobilization, as well as to provide a rapid recovery (20,21).
We used the Functional Ambulation Categories (FAC) scale and Harris
hip score (HHS) to evaluate the hip disability, independence and
the burden of care. We did not find any statistically significant
differences after 12 months regarding the FAC scale. Conversely, we
noticed a statistically better HHS after 6 months for the short
nail group (P<0.05).
After 12 months, the short nail group still showed
better results, but not statistically significant; thus, the length
of the nail may not influence the long-term functional result
(P=0.28). In the literature, we found studies that demonstrated
acceptable and comparable results regarding HHS (22-25).
Sellan et al observed a better HHS for the short nail group,
but did not find any significance from the clinical point of view.
One hypothesis is that usually, cases with such fractures are
geriatric patients with low motor functions required to return to
the baseline (26).
The short nail group experienced a 28-min shorter
operative time than the long nail group. This result is a
consequence of the aiming guide usage for the short nail, unlike
the other group of patients where the distal screw is fixed by free
hand and under assistance of intraoperative fluoroscopic imaging.
Despite the significant differences, we were not able to correlate
these results with the functional outcome. Zhang et al also
demonstrated that the operative time does not influence the average
length of hospital stay (25). We
also found that the intraoperative blood loss was significantly
higher in the long nail group. This may be linked to the longer
operative time and the longer distal reaming distance necessary for
the insertion of the long nail (27-29).
Regarding the postoperative complications, we noted
2 screw cut-outs in the short nail group and 1 screw cut-out in the
long nail group, but without statistically significant differences.
Except in the case with a long implant, the screw position was
acceptable (lower half of the femoral neck on the AP view and
central on the lateral view). The screw cut-out is the most
frequent reason for reoperation and is usually caused by a screw
malposition or an increased TAD (27-30).
According to Baumgartner and Solberg, the TAD should be less than
25 mm to prevent the screw cutout. In our study, the TAD showed no
statistically significant differences between the groups, and the
mean distance was not longer than 19 mm. Therefore, the screw
cut-out could be due to the higher leverage, a decreased length of
the short nail and a higher instability of the construct (15). Regarding the case with a long nail,
an eccentric screw position was noted on the lateral view. This
kind of screw malposition may have caused a rotational force of the
femoral neck around the proximal screw. The central position of the
screw on the lateral plane is considered optimal in order to
decrease the torsional forces (31,32).
We also recorded a peri-implant distal femur
fracture in a case with a long nail implant. The fracture was
caused by a fall from ground-level after 8 weeks. The patient was
surgically treated with open reduction and internal fixation with a
locking plate. We did not report peri-implant fractures in the
short nail group. Even though short proximal femoral nails
demonstrated an increased risk of fractures at the distal tip of
the implant in the early 1990's, later designs have demonstrated
that this is not an issue anymore (13,14,33).
Some retrospective studies have demonstrated that
the peri-implant fracture rate after short and long proximal
femoral nail fixation showed no significant differences. The
fracture rates reported in the literature are between 0 and 3.3%
for the short femoral nail and 0 and 2.3% for the long femoral nail
(27-29,34,35).
The inclusion of two groups of patients with
unstable trochanteric fractures to determine the outcome of long
compared with short proximal femoral nails in a prospective
randomized study is the main strength of our study. We considered
that the sample size was not adequate to analyze the complications,
this being one of the main limitations. We consider that a larger
sample is required to properly evaluate and to find correlations
between complications and surgical errors. The blood loss being
estimated and the inability to blind patient and the surgeon data
represent other limitations of our study.
In conclusion, the present study showed no
significant differences between short and long proximal femoral
nails regarding the functional outcome after 12 months, which
reinforces other findings available in the literature. The long
cephalomedullary nail requires a longer surgical time and is
associated with an increase in intraoperative blood loss without
improving the patient function. We recorded only one peri-implant
fracture in a patient with a long nail construct, which required
surgical treatment. A larger sample of cases is required to
thoroughly analyze the postoperative complications.
Acknowledgements
Professional editing, linguistic and technical
assistance performed by Irina Radu, Individual Service Provider
(credentials: E0048/2014, Medicine-Pharmacy).
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
SD planned the clinical study, contributed to the
conception and design of the study, and the acquisition, analysis
and interpretation of the data. CDMD planned the clinical study and
contributed to the conception and design of the study. DCC
contributed to the conception and design of the study, translation
and critical revision for important intellectual content. CIS
contributed to the analysis and interpretation of the data and the
critical revision for important intellectual content. All authors
read and approved the final version of the manuscript and agreed to
be accountable for all aspects of the study.
Ethics approval and consent to
participate
All procedures performed in studies involving human
participants were in accordance with the national ethical standards
and with the 1964 Helsinki declaration and its later amendments or
comparable ethical standards. The study was approved by the Ethics
Committee of ‘Foişor’ Orthopaedics-Traumatology and Osteoarticular
TB Hospital in Bucharest, Romania (no. 1309/2020). Informed consent
was obtained from all individual participants included in the
study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Zuckerman JD: Hip fracture. N Engl J Med.
334:1519–1525. 1996.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Miyamoto RG, Kaplan KM, Levine BR, Egol KA
and Zuckerman JD: Surgical management of hip fractures: An
evidence-based review of the literature. I: Femoral neck fractures.
J Am Acad Orthop Surg. 16:596–607. 2008.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kannus P, Parkkari J, Sievänen H, Heinonen
A, Vuori I and Järvinen M: Epidemiology of hip fractures. Bone. 18
(Suppl 1):S57–S63. 1996.PubMed/NCBI View Article : Google Scholar
|
|
4
|
National hip fracture database (NHFD)
annual report 2017: https://www.nhfd.co.uk/files/2017ReportFiles/NHFD-AnnualReport2017.pdf.
Accessed: November, 2020.
|
|
5
|
Fisher AA, Davis MW, Rubenach SE,
Sivakumaran S, Smith PN and Budge MM: Outcomes for older patients
with hip fractures: The impact of orthopedic and geriatric medicine
cocare. J Orthop Trauma. 20:172–178. 2006.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Erez O and Dougherty PJ: Early
complications associated with cephalomedullary nail for
intertrochanteric hip fractures. J Trauma. 72:E101–E105.
2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Rogers FB, Shackford SR and Keller MS:
Early fixation reduces mobility and mortality in elderly patients
with hip fractures form low-impact falls. J Trauma. 39:261–265.
1995.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Anglen JO and Weinstein JN: American Board
of Orthopaedic Surgery Research Committee. Nail or plate fixation
of intertrochanteric hip fractures: Changing pattern of practice. A
review of the American board of orthopaedic surgery database. J
Bone Joint Surg Am. 90:700–707. 2008.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Werner BC, Fashandi AH, Gwathmey FW and
Yarboro SR: Trends in the management of intertrochanteric femur
fractures in the United States 2005-2011. Hip Int. 25:270–276.
2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Valverde JA, Alonso MG, Porro JG, Rueda D,
Larrauri PM and Soler JJ: Use of the gamma nail in the treatment of
fractures of the proximal femur. 1998. J Orthop Trauma. 17 (Suppl
8):S51–S56. 2003.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lorich DG, Geller DS and Nielson JH:
Osteoporotic pertrochanteric hip fractures: Management and current
controversies. Instr Course Lect. 53:441–454. 2004.PubMed/NCBI
|
|
12
|
Hesse B and Gachter A: Complications
following the treatment of trochanteric fractures with the gamma
nail. Arch Orthop Trauma Surg. 124:692–698. 2004.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Radford PJ, Needoff M and Webb JK: A
prospective randomised comparison of the dynamic hip screw and the
gamma locking nail. J Bone Joint Surg Br. 75:789–793.
1993.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Bridle SH, Patel AD, Bircher M and Calvert
PT: Fixation of intertrochanteric fractures of the femur. A
randomised prospective comparison of the gamma nail and the dynamic
hip screw. J Bone Joint Surg Br. 73:330–334. 1991.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Baumgaertner MR and Solberg BD: Awareness
of tip-apex distance reduces failure of fixation of trochanteric
fractures of the hip. J Bone Joint Surg Br. 79:969–971.
1997.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Harris WH: Traumatic arthritis of the hip
after dislocation and acetabular fractures: Treatment by mold
arthroplasty. An endresult study using a new method of result
evaluation. J Bone Joint Surg Am. 51:737–755. 1969.PubMed/NCBI
|
|
17
|
Katz J and Melzack R: Measurement of pain.
Surg Clin North Am. 79:231–252. 1999.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Holden MK, Gill KM, Magliozzi MR, Nathan J
and Piehl-Baker L: Clinical gait assessment in the neurologically
impaired. Reliability and meaningfulness. Phys Ther. 64:35–40.
1984.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Wade DT: Measurement in neurological
rehabilitation. Curr Opin Neurol Neurosurg. 5:682–686.
1992.PubMed/NCBI
|
|
20
|
Oldmeadow LB, Edwards ER, Kimmel LA, Kipen
E, Robertson VJ and Bailey MJ: No rest for the wounded: Early
ambulation after hip surgery accelerates recovery. ANZ J Surg.
76:607–611. 2006.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Dragosloveanu Ş, Dragosloveanu CDM, Stanca
HT, Cotor DC, Dragosloveanu CI and Stoica CI: A new perspective
towards failure of gamma nail systems. Exp Ther Med.
20(216)2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Okcu G, Ozkayin N, Okta C, Topcu I and
Aktuglu K: Which implant is better for treating reverse obliquity
fractures of the proximal femur: A standard or long nail? Clin
Orthop Relat Res. 471:2768–2775. 2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Schipper IB, Steyerberg EW, Castelein RM,
van der Heijden FH, den Hoed PT, Kerver AJ and van Vugt AB:
Treatment of unstable trochanteric fractures. Randomized comparison
of the gamma nail and the proximal femoral nail. J Bone Joint Surg
Br. 86:86–94. 2004.PubMed/NCBI
|
|
24
|
Elis J, Chechik O, Maman E and Steinberg
EL: Expandable proximal femoral nails versus 95 dynamic condylar
screw-plates for the treatment of reverse oblique intertrochanteric
fractures. Injury. 43:1313–1317. 2012.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Zhang Y, Zhang S, Wang S, Zhang H, Zhang
W, Liu P, Ma J, Pervaiz N and Wang J: Long and short intramedullary
nails for fixation of intertrochanteric femur fractures (OTA 31-A1,
A2 and A3): A systematic review and meta-analysis. Orthop Traumatol
Surg Res. 103:685–690. 2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Sellan M, Bryant D, Tieszer C, Papp S,
Lawendy A, Liew A, Viskontas D, MacLeod M, Coles C, Carey T, et al:
Short versus long interTAN fixation for geriatric intertrochanteric
hip fractures: A multicentre head-to-head comparison. J Orthop
Trauma. 33:169–174. 2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Hou Z, Bowen TR, Irgit KS, Matzko ME,
Andreychik CM, Horwitz DS and Smith WR: Treatment of
pertrochanteric fractures (OTA 31-A1 and A2): Long versus short
cephalomedullary nailing. J Orthop Trauma. 27:318–324.
2013.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Boone C, Carlberg KN, Koueiter DM, Baker
KC, Sadowski J, Wiater PJ, Nowinski GP and Grant KD: Short versus
long intramedullary nails for treatment of intertrochanteric femur
fractures (OTA 31-A1 and A2). J Orthop Trauma. 28:e96–e100.
2014.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Kleweno C, Morgan J, Redshaw J, Harris M,
Rodriguez E, Zurakowski D, Vrahas M and Appleton P: Short versus
long cephalomedullary nails for the treatment of intertrochanteric
hip fractures in patients older than 65 years. J Orthop Trauma.
28:391–397. 2014.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Vicario C, Marco F, Ortega L, Alcobendas
M, Dominguez I and López-Durán L: Necrosis of the femoral head
after fixation of trochanteric fractures with gamma locking nail. A
cause of late mechanical failure. Injury. 34:129–134.
2003.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Den Hartog BD, Bartal E and Cooke F:
Treatment of the unstable intertrochanteric fracture. Effect of the
placement of the screw, its angle of insertion, and osteotomy. J
Bone Joint Surg Am. 73:726–733. 1991.PubMed/NCBI
|
|
32
|
Lenich A, Bachmeier S, Prantl L, Nerlich
M, Hammer J, Mayr E, Al-Munajjed AA and Füchtmeier B: Is the
rotation of the femoral head a potential initiation for cutting
out? A theoretical and experimental approach. BMC Musculoskelet
Disord. 12(79)2011.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Parker MJ and Handoll HH: Gamma and other
cephalocondylic intramedullary nails versus extramedullary implants
for extracapsular hip fractures in adults. Cochrane Database Syst
Rev: CD000093, 2010.
|
|
34
|
Vaughn J, Cohen E, Vopat BG, Kane P,
Abbood E and Born C: Complications of short versus long
cephalomedullary nail for intertrochanteric femur fractures,
minimum1 year follow-up. Eur J Orthop SurgTraumatol. 25:665–670.
2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Lindvall E, Ghaffar S, Martirosian A and
Husak L: Short versus long intramedullary nails in the treatment of
pertrochanteric hip fractures: Incidence of ipsilateral fractures
and costs associated with each implant. J Orthop Trauma.
30:119–124. 2016.PubMed/NCBI View Article : Google Scholar
|