1. Introduction
Diabetic ketoacidosis (DKA) and hypoglycemia are the
most common diabetes emergencies that can occur in a hospital
emergency department (ED) (1).
Along with these, less common, hyperglycemic hyperosmolar state
(HHS) is associated with unpredictable evolution and increased risk
of mortality. DKA and HHS are biochemically different conditions
that require different approaches to treatment depending on the
precipitating factor. Optimal treatment requires the involvement of
a multidisciplinary team. The disorder can have significant
mortality in the absence of early diagnosis and treatment
instituted.
In recent years, DKA management has changed, the
diagnosis is made only when all three components are present (‘D =
diabetes’, ‘K = ketosis’ and ‘A = acidosis’). In addition, constant
monitoring of the level of plasma ketones is crucial. Instead, for
HHS the first therapeutic step is the rehydration of the patient,
followed by initiation of insulin treatment, as a means of
decreasing glucose levels.
In the present review, we performed a literature
search in the PubMed and Scopus databases using the key words,
‘diabetic coma’, in combination with ‘diabetic emergencies’ and
‘hypoglycemia’ and ‘diabetic ketoacidosis’ and ‘hyperglycemic
hyperosmolar state’ and ‘emergency therapy’ between 1990 and 2020.
Relevant articles and reviews regarding the new strategies of
diagnostic and therapeutic approach to emergencies in the evolution
of patients with diabetes mellitus were included. Exclusion
criteria included studies written in languages other than English,
letters to the editor, conference presentations, editorials,
comments, opinions and articles without free access.
2. Diabetic ketoacidosis
Features of DKA
The main features of DKA are hyperglycemia,
metabolic acidosis with a high anion gap and heavy ketonuria. The
usual features of DKA include hyperglycemia (>250 md/dl),
metabolic acidosis (pH<7.35 and bicarbonate <15 mmol/l), high
anion gap and ketonemia/heavy (3+) ketonuria (2).
This contrasts with the other hyperglycemic diabetic
emergency of hyperosmolar non-ketonic hyperglycemia where there is
no acidosis, absent or minimal ketonuria but often extremely high
glucose levels (>33 mmol/l) and very high serum sodium levels
(>150 mmol/l) (3).
DKA precipitating factors
Factors to consider for type 1 diabetes (absolute
insulin deficiency) include: inaugural coronary artery disease;
discontinuation of insulin treatment (intentional, limited access
to health care services, and technical defects in insulin delivery
devices such as pens and insulin pumps); associated acute
conditions (e.g., surgery, stroke, acute myocardial infarction,
infections and trauma) that increase the level of counterregulatory
hormones (catecholamines, cortisol and glucagon) (4). Factors to consider for type 2 diabetes
(relative insulin deficiency) include: associated acute conditions
(e.g., surgery, stroke, myocardial infarction, infections and
trauma).
Diagnostic criteria and classification
of DKA
DKA is a complex state of metabolic disorders
defined by the American Diabetes Association (ADA) as severe
hyperglycemia (plasma glucose levels >250 mg/dl, ketonemia
(ketosis) and metabolic acidosis (pH<7.3; serum bicarbonate
<18 mmol/l) (Table I). Depending
on the severity, in 2009, the ADA classified DKA as mild, moderate
and severe (5).
 | Table IClassification of DKA. |
Table I
Classification of DKA.
| | DKA |
|---|
| Factors | Normal | Mild | Moderate | Severe |
|---|
| Arterial pH | 7.35-7.45 | 7.25-7.30 | 7.00-7.24 | <7.00 |
| Serum bicarbonate
(mEq/l) | 22-28 | 15-18 | 10-14 | <10 |
| Serum/urine
ketone | Absent | Present | Present | Present |
| Glucose level
(mg/dl) | 70-110 | >250 | >250 | >250 |
| Effective serum
osmolarity | 275-295 | Variable | Variable | Variable |
| Anion gap | <11 | >10 | >12 | >12 |
| Mental status | Normal | Alert | Alert/drowsy | Stupor/coma |
In 2013, the Joint British Diabetes Societies
Inpatient (JBDS IP) Group DKA Guidelines introduced serum ketone
(3-beta-hydroxybutyrate [pHBA]) into the definition of DKA,
although pHBA measurement for the diagnosis and monitoring of DKA
was recommended in the ADA Diabetes Laboratory Guidelines in 2011
(5-8)
The markers by which the severity of DKA can be quantified are
depicted in Table II.
| Table IIMarkers of severity in DKA. |
Table II
Markers of severity in DKA.
| Variable | DKA |
|---|
| Marker of
severity | JBDS IP Group
2013 |
| Mental status | GCS <12 or
abnormal AVPU |
| Oxygen
saturation | <92% on air
(assuming normal baseline respiratory function) |
| Venous/arterial
pH | pH<7.1 |
| Potassium | Hypokalemia
(<3.5 mmol/l) or hyperkalemia (>6 mmol/l) |
| Systolic blood
pressure | <90 mmHg |
| Pulse | >100 or <60
bpm |
| Urine output | <0.5 ml/kg/h or
other evidence of AKI |
| Blood ketones | >6 mmol/l |
| Bicarbonate
level | <5 mmol/l |
| Anion gap
sodium | >16 mmol/l |
Treatment of DKA
The overall aims in the treatment of DKA are to
improve circulatory volume and tissue perfusion, decrease blood
glucose, and correct the acidosis and electrolyte imbalances. The
administration of low-dose insulin (0.1 U/kg/h) and intravenous
fluid and electrolyte replacement solutions may contribute to these
objectives (9). Frequent monitoring
of serum glucose, venous pH and pHBA is required. It is important
to identify and treat the cause that triggered DKA, the infection
being often the most common trigger of DKA.
The essential elements that must be provided to
patients with DKA include fluids, insulin, potassium and education.
Early venous approach and urinary catheterization are also
required, especially if the patient is hemodynamically unstable or
requires accurate measurement of diuresis.
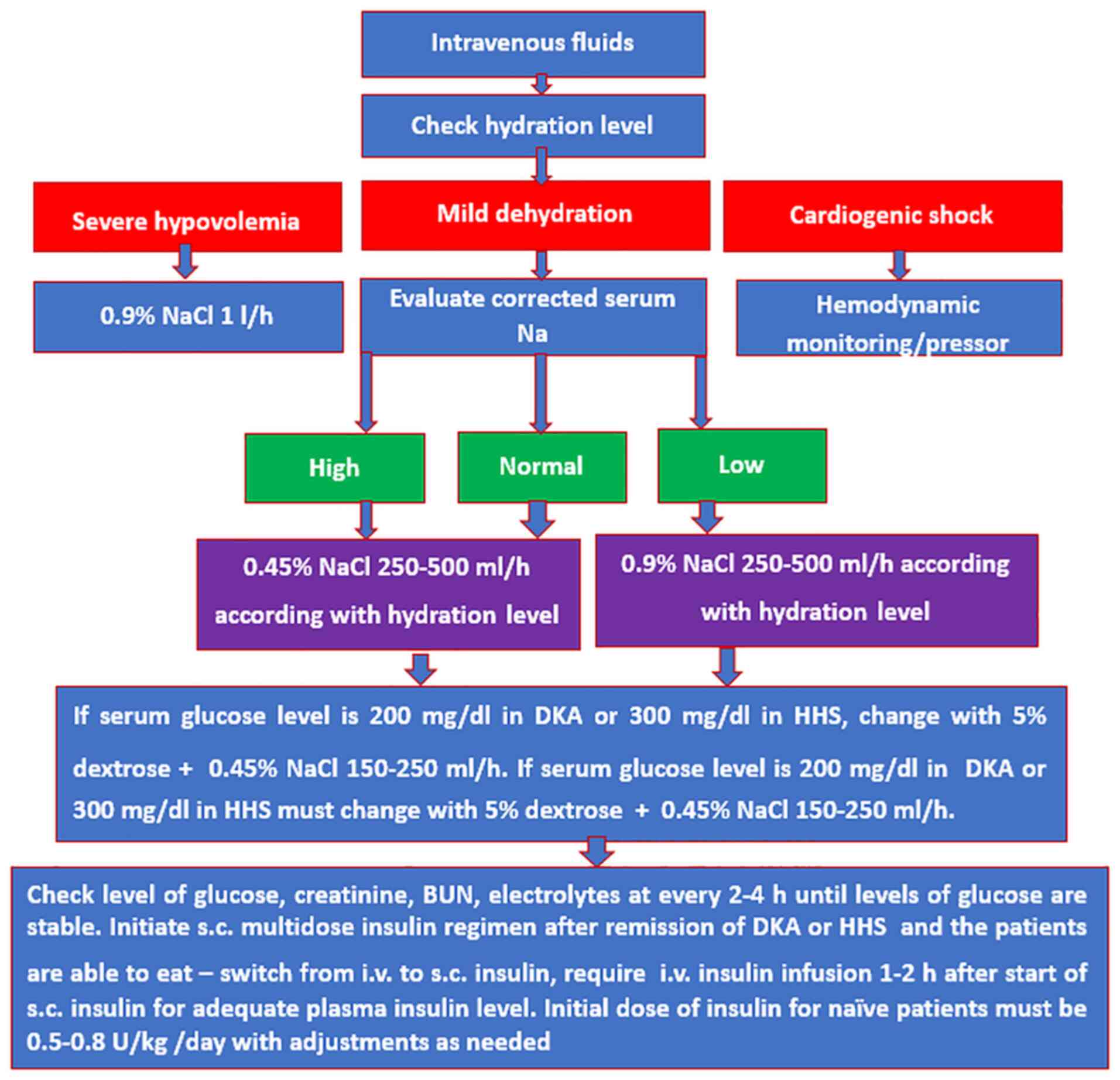
Hydration
If the patient is not in shock or oliguric,
hydration is provided by administering 500 ml/h of 0.9% saline for
4 h, followed by 250 ml/h for the next 4 h. Simultaneous correction
of acidosis and hyperglycemia should be performed at the same time
as hydration. Excess fluid should not be given as there is a risk
of cerebral edema. The most commonly used hydration solution is
saline (0.9%), although no adverse effects have been reported with
0.45% saline or Ringer's solution (1,2).
Volume recovery can be clinically quantified by measuring the heart
rate and BP, diuresis, urea dosage, and serum creatinine.
After the serum glucose level has dropped <250
mg/dl, 5% dextrose (with adequate potassium) may be introduced into
the infusion regimen rather than saline. Administering hypertonic
dextrose (1 liter 10% dextrose + 40 units insulin at 250 ml/h)
rather than isotonic dextrose (1 liter 5% dextrose + 10 units
insulin at 250 ml/h) may accelerate the clearance of ketone bodies
but also causes a rise in glucose levels without additional
improvement in blood pH or bicarbonate (9) (Fig.
1).
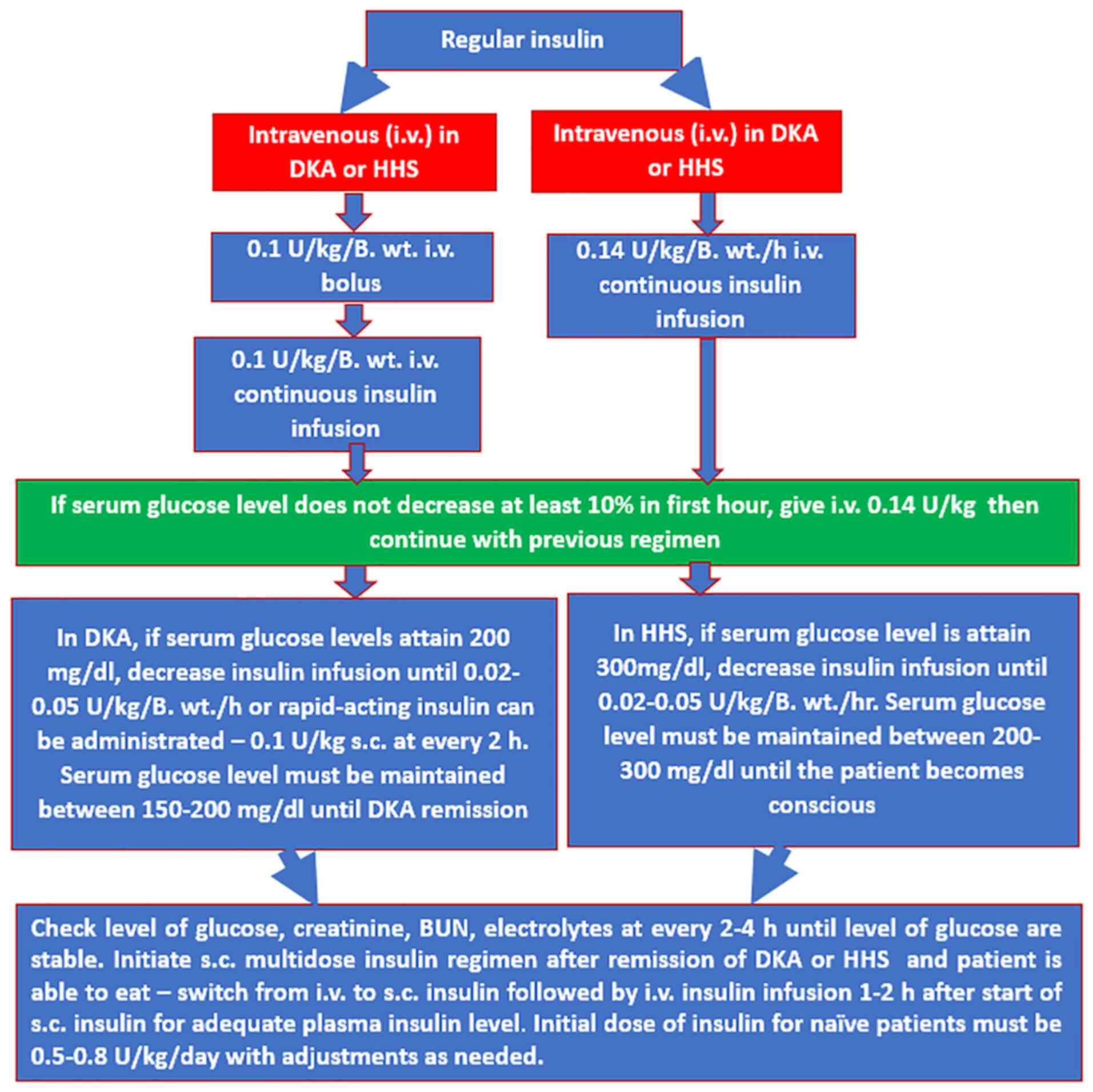
Insulin
A soluble fast-acting insulin is used to reduce high
serum blood glucose levels, even if there is no evidence that the
use of insulin analogues increases the risk of DKA.
The insulin level is reached very quickly when an
intravenous bolus is followed by an intravenous infusion. The
half-life of circulating insulin is 5 min. The administration of an
intravenous infusion has the advantage that it allows a more rapid
reduction of the insulin level compared to the administration of
intermittent bolus (8).
Usually, a bolus of 6 units is used followed by an
infusion of 6 U/h at the beginning of the treatment in the case of
an adult with DKA (usually for a patient weighing <60 kg, 0.1
U/kg are used). When there is a severe drop in blood sugar levels,
a sudden change in the osmolality of the extracellular fluid can
occur, which can cause cerebral edema (5).
Lack of therapeutic response, in the absence of a
mechanical cause, raises the suspicion of a present infection or
insufficient hydration. In this case, the dose of insulin that
should be increased or even doubled should be reconsidered.
Ketone bodies are cleared more slowly than glucose
during DKA treatment. The mean duration of treatment until blood
glucose is <250 mg/dl (~14 mmol/l) and ketoacidosis (pH>7.30;
bicarbonate >18 mmol/l) is corrected, is between 6 and 12 h,
respectively (10).
Insulin infusion is required until the disappearance
of ketone bodies and the subsequent correction of acidosis.
Otherwise, discontinuation of the insulin infusion once the
glycemic level is normalized may result in a recurrence of
ketoacidosis, unless hypertonic dextrose is used in the infusion.
Subcutaneous administration of insulin should be initiated prior to
stopping the insulin infusion, preferably in the morning.
For the treatment of type 1 diabetes, continuous
infusions of subcutaneous insulin are commonly used in continental
Europe with an increasing use in the UK (10). This type of treatment was initially
associated with an increased risk of DKA due to equipment failure
(11); however, as this equipment
was improved, this high risk of DKA decreased.
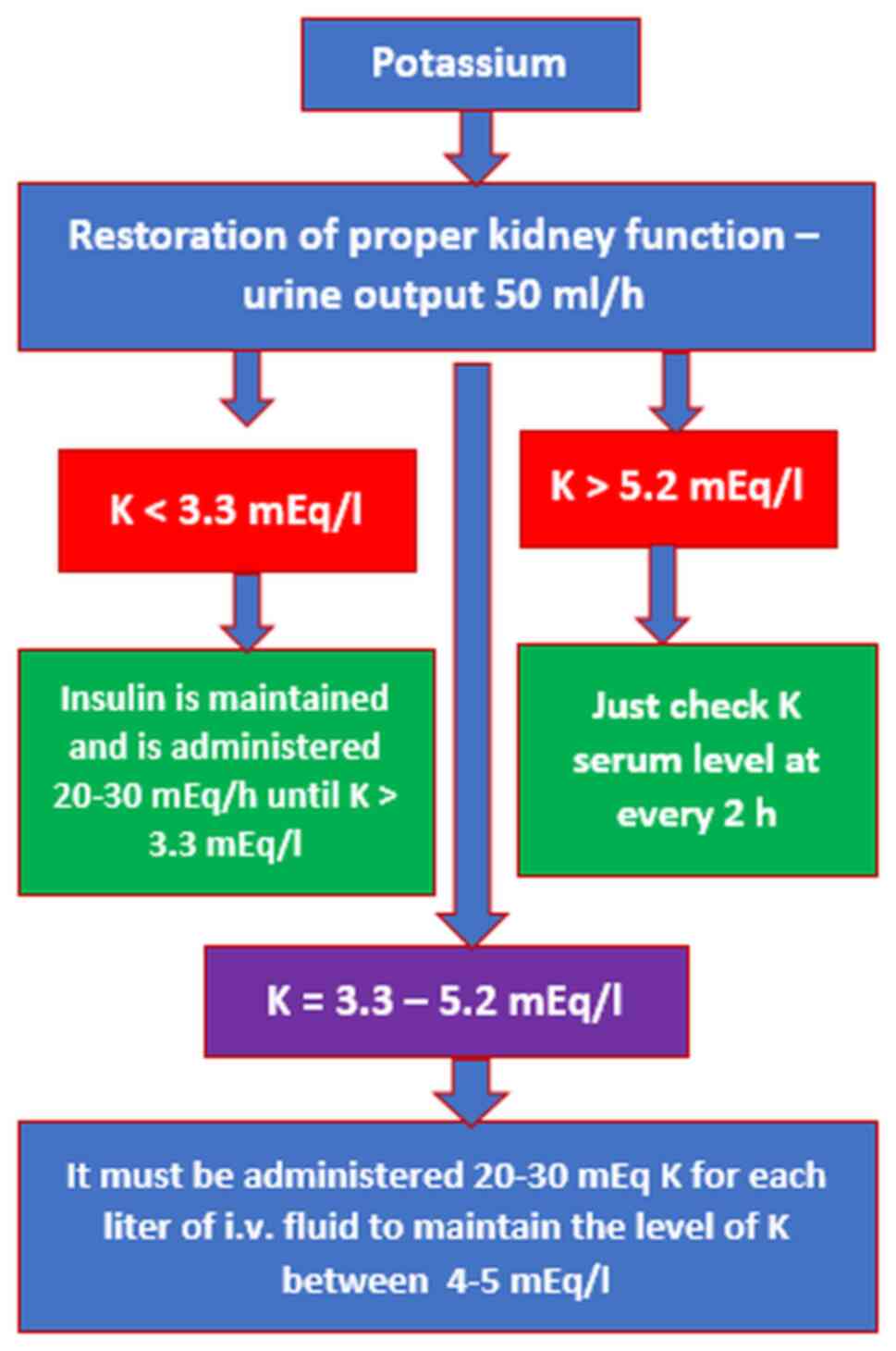
Potassium level (K)
Subsequent to the administration of insulin,
potassium enters the cells, and there is a risk of hypokalemia, the
most common electrolyte disorder that can endanger the life of a
patient. Therefore, intravenous potassium administration is
absolutely necessary with insulin. Potassium administration before
initiating insulin therapy is not indicated, as it may result in an
increase in the extracellular level of potassium (12).
Potassium administration is recommended to be
initiated at the same time as insulin and fluid start, even if the
potassium level is within normal limits. The appropriate potassium
replacement regimen (11) should
adhere to the following rules: start KCl when K is normal or low
with an average dose of 20 mmol/h, but if initially K is increased,
KCl administration should be delayed until levels decrease to
within normal range (Fig. 2). In
DKA, it is essential to administer potassium in order to avoid
cardiovascular complications due to hypokalemia, hyperkalemia or
HHS (12).
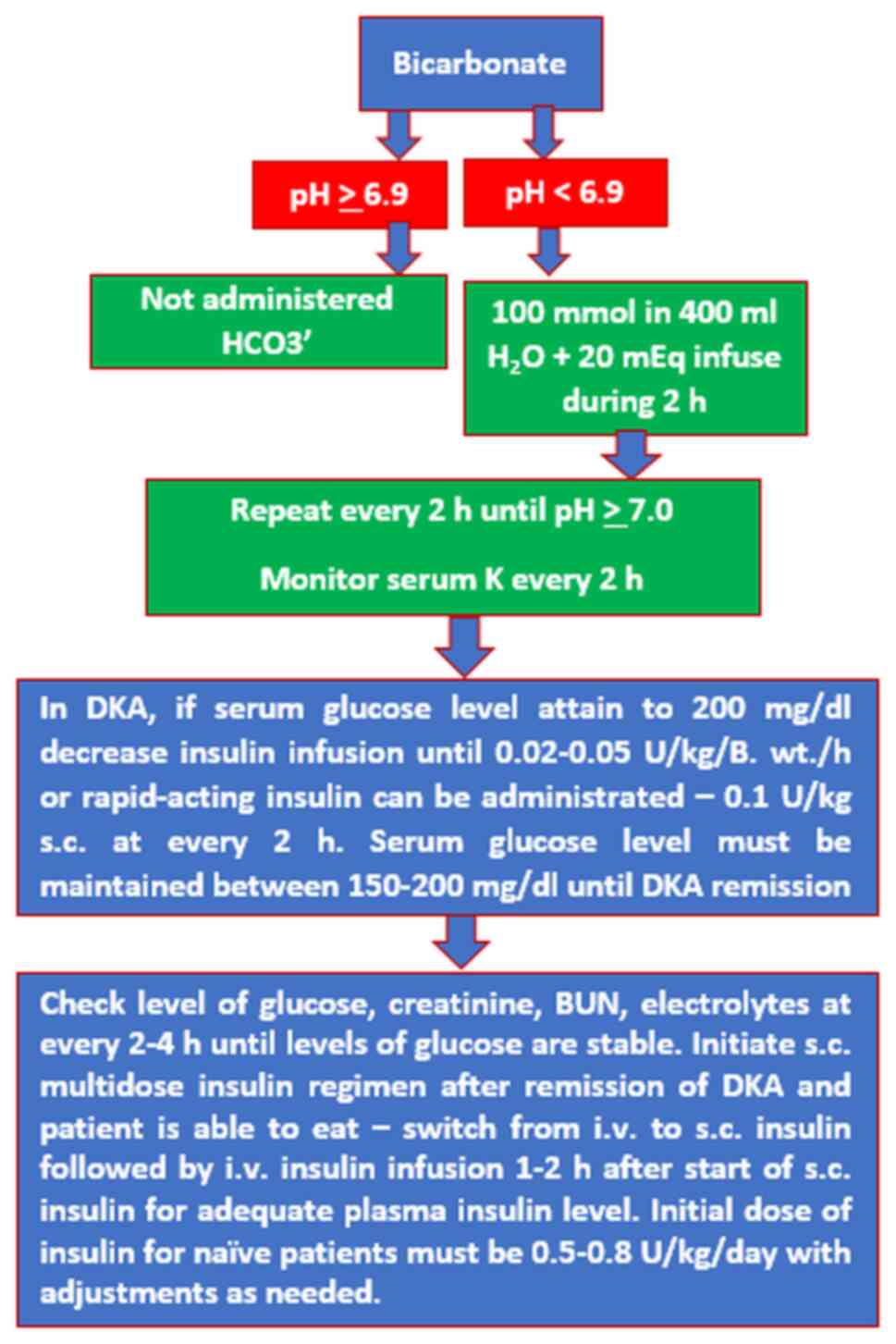
Bicarbonate
In clinical trials and in practice, bicarbonate
administration in DKA has not been shown to be useful in the
clinical and biochemical recovery of patients and it is even
associated with delayed disappearance of ketone bodies and lactate
levels. In addition, bicarbonate can depress cardiac activity, and
increase intravascular volume at risk of pulmonary edema as it is
hypertonic and hyperosmolar (12-16).
It is recognized that an increase in pH is
associated with a shift to the left in the Hb-O2
dissociation curve, leading to a decrease of tissue oxygenation as
well as an increase in the lactate production.
PaCO2 rises due to bicarbonate infusion. In
addition, intracellular acidosis can be exacerbated by the rapid
diffusion across cell membranes. This phenomenon is more serious
especially in situations when the patient is unable to compensate
by increasing CO2 excretion (14,15).
During the recovery period of DKA, lactate produced
during tissue hypoxia is metabolized to bicarbonate, leading to
alkalosis (17,18). The correction of the bicarbonate
level that appears in the DKA must be carried out under permanent
pH control, to ensure optimal insulin treatment (Fig. 3).
Phosphate
In DKA, phosphate levels are altered in the same way
as potassium. However, available studies have not shown that the
addition of phosphate to the treatment regimen leads to a more
rapid recovery of bicarbonate, pH or glucose levels (19,20).
3. Hyperglycemic hyperosmolar state
Features of HHS
HHS is characterized by marked hyperglycemia [blood
glucose levels >600 mg/dl (33.3 mmol/l)]; hyperosmolarity
(plasma osmolarity >320 mOsm/kg) and dehydration; and the
absence of ketoacidosis and depression of the sensorium (6).
The 2013 JBDS IP Group HHS definition includes
(6): marked hyperglycemia [>540
mg/dl (30 mmol/l)]; no significant ketonemia (<3 mmol/l); no
acidosis (pH >7.3; bicarbonate >15 mmol/); hypovolemia;
osmolality usually >320 mOsm/kg.
These guidelines also highlight that a mixed picture
of HHS and DKA may occur. HHS is identified most frequently in
individuals with type 2 diabetes; however, approximately 20% of
cases have no history of this diagnosis. Markers by which the
severity of HHS can be quantified are presented in Table III.
| Table IIIMarkers of severity in HHS. |
Table III
Markers of severity in HHS.
| Variable | HHS |
|---|
| Marker of
severity | JBDS IP Group
2012 |
| Mental status | GCS <12 or
abnormal AVPU |
| Oxygen
saturation | <92% on air
(assuming normal baseline respiratory function) |
| Venous/arterial
pH | pH <7.1 |
| Potassium | Hypokalemia
(<3.5 mmol/l) or hyperkalemia (>6 mmol/l) |
| Systolic blood
pressure | <90 mmHg |
| Pulse | >100 or <60
bpm |
| Urine output | <0.5 ml/kg/h or
other evidence of acute kidney injury (AKI) |
| Blood ketones | >1 mmol/l |
| Bicarbonate
level | mEq/l |
| Anion gap
sodium | >160 mmol/l |
| Osmolality | >350
mOsm/kg |
| Miscellaneous | Hypothermia |
| | Acute or serious
comorbidity (e.g., ACS, heart failure, or stroke) |
Management of HHS
The therapeutic management of HHS is different from
DKA. Patients with HHS tend to be elderly with multiple
complications and comorbidities (1,2).
The main aims of HHS treatment include the gradual
normalization of osmolality, replacement of fluid and electrolyte
losses and normalization of blood glucose. In addition, as in the
case of DKA, the trigger factor must be identified and addressed,
arterial or venous thrombosis must be prevented, as well as
potential complications (cerebral edema). The recommendations of
the 2012 JBDS IP Group (6) can be
followed in the management of HHS.
Osmolality can be measured or calculated using the
formulae:
[2x Na (mEq/l) + glucose (mg/dl)]/18 + BUN
(mg/dl)/2.8
or
[2x Na (mmol/l) + glucose (mmol/l) + urea
(mmol/l)]
The aim of the initial therapy is expansion of the
intra- and extravascular volume and to restore peripheral
perfusion. As blood glucose drops, plasma osmolarity decreases and
water moves into the intracellular space, resulting in increased
serum sodium levels. This increase is not necessarily an indication
of the administration of isotonic solutions. A decrease in plasma
glucose at a rate of up to 90 mg/dl/h is accompanied by an increase
in serum sodium levels but also a decrease in osmolarity. In
hypernatremic dehydration, 0.5 mmol/l/h is the optimal rate of
serum sodium depletion which is recommended. The rate of depletion
of plasma sodium should not exceed 12 mmol/l per day. In the first
24 h it is indicated to replace approximately 50% of the estimated
fluid losses, the rest being insured in the next 12 h (5).
Significant ketonemia (PHBA >1 mmol/l) indicates
relative hypoinsulinemia which requires initiation of insulin
therapy. If significant ketonemia is not present (PHBA <1
mmol/l), insulin should not be started until the fluid deficit is
corrected by administration of 0.9% sodium chloride which may lead
to a decrease in blood glucose. Insulin administration prior to
proper fluid replacement can lead to cardiovascular collapse, as
water moves from the intravascular space, resulting in a decrease
in intravascular volume. The recommended insulin dose is 0.05
U/kg/h. Lowering blood sugar by a rate of up to 90 mg/dl/h is ideal
(5).
In order to avoid hypoglycemia, a reasonable
objective in the first 24 h is a blood glucose target of 180-270
mg/dl. If the blood glucose falls <250 mg/dl, 10% dextrose at
125 ml/h should commence, to be continued with the 0.9% sodium
chloride solution (5).
In order to replace the potassium level, the
indication is to proceed in the same way as in DKA. Complete
normalization of electrolytes and osmolarity can take up to 72 h.
Due to the increased risk of arterial and venous thromboembolism,
all the patients should receive low molecular weight prophylactic
heparin (LMWH) (21,22).
The 2009 ADA Hyperglycemic Crises Consensus and the
JBDS IP Guidelines remain the predominant protocols of choice for
the management of patients with DKA and HHS (Fig. 4).
4. Hypoglycemia
The annual prevalence of severe hypoglycemia is
approximately 30% in individuals with type 1 diabetes (5). It is higher in those with risk factors
including strict glycemic control, impaired awareness of
hypoglycemia and increasing duration of diabetes (Table IV). It is also common during sleep,
i.e., nocturnal hypoglycemia.
| Table IVRisk factors for hypoglycemia. |
Table IV
Risk factors for hypoglycemia.
| Risk factors for
adults | Risk factors for
children |
|---|
| Tight glycemic
control | Fasting or long
duration of poor or nil intake |
| Malabsorption | Inborn errors of
metabolism (e.g., glycogen storage disorders) |
| Injection into
lipohypertrophy sites | Insulinoma |
| Alcohol | Congenital or
primary hyperinsulinism |
| Insulin
prescription error (notable in hospitalized patients) | Accidental
ingestion of medications; e.g., salicylate, |
| Long duration of
diabetes | sulfonylureas, iron
supplements, paracetamol |
| Renal dialysis | Poorly controlled
diabetes mellitus in pregnancy is a risk for |
| Drug interactions
between hypoglycemic agents; e.g., quinine, | neonatal
hypoglycemia |
| selective serotonin
reuptake inhibitors | Sepsis is also a
risk for neonatal hypoglycemia |
| Impaired renal
function | |
| Lack of
anti-insulin hormone function; e.g., Addison's disease, | |
| hypothyroidism | |
Clinical manifestations of
hypoglycemia
The symptoms and signs of hypoglycemia are
non-specific and can be classified into neuroglycopenic symptoms
that are the direct result of lack of glucose in the brain and
neurogenic or autonomic symptoms responsible for awareness of
hypoglycemia (Table V) (23,24).
| Table VClassification of symptoms and signs
of hypoglycemia. |
Table V
Classification of symptoms and signs
of hypoglycemia.
| | Neurogenic (or
autonomic) symptoms |
|---|
| Neuroglycopenic
symptoms | Adrenergic symptoms
(catecholamine-mediated) | Cholinergic
symptoms (acetylcholine-mediated) |
|---|
| Cognitive
impairments | Palpitations | Sweating |
| Behavioral
changes | Tremor | Hunger |
| Psychomotor
abnormalities |
Anxiety/arousal | Paresthesia |
| Seizures | | |
| Coma | | |
Diagnosis
The diagnosis of hypoglycemia is based on three
criteria (Whipple's triad): symptoms and signs suggestive of
hypoglycemia (feeling faint, dizziness and sweating); low blood
sugar levels during seizures (<70 mg/dl); and resolution of
symptoms after glucose administration.
Management of hypoglycemia in
adults
In case of hypoglycemia a quick-acting carbohydrate
(sugar) should be administered followed by a longer-acting
carbohydrate (toast, a normal meal) (25,26).
The steps to be taken for the management of patients with
hypoglycemia depend on the clinical condition and the environment
where the patient is affected by diabetes mellitus (Table VI).
| Table VIManagement of hypoglycemia. |
Table VI
Management of hypoglycemia.
| Initially |
|---|
| Glucose 10-20 g is
given by mouth, either in liquid form or as granulated sugar (two
teaspoons) or sugar lumps |
| Repeat capillary
blood glucose after 10-15 min; if the patient is still hypoglycemic
then the above can be repeated (probably up to 1-3 times) |
| If hypoglycemia
causes unconsciousness, or the patient is uncooperative |
| Intravenous
administration of 75-80 ml 20% glucose or 150-160 ml of 10% glucose
(the volume will be determined by the clinical scenario) |
| Of note, 25 ml of
50% glucose concentration is viscous, making it more irritant and
more difficult to administer intravenously. |
| It is rarely used
now |
| Once the patient
regains consciousness, oral glucose should be administered, as
above |
| If the patient is
at home, or intravenous (IV) access cannot be rapidly
established |
| Glucagon 1 mg
should be given by intramuscular (IM), or subcutaneous (SC)
injection |
| This dose is used
in insulin-induced hypoglycemia (by SC, IM, or IV injection), in
adults and in children >8 years (or body weight, >25 kg) |
If hypoglycemia is caused by an oral antidiabetic
drug, the patient must be admitted to hospital, because the
hypoglycemic effects of these drugs may persist for 12-24 h, and
receive an ongoing glucose infusion.
If it is available, glucagon can also be
administered subcutaneously (SC) or intramuscularly (IM). It has a
relatively slow onset of action and relies on glycogen stores and
thus, it may not be effective in cachectic patients, those with
liver disease and in young children. It is contra-indicated in
insulinoma and phaeochromocytoma. For inpatients, an infusion of
100 ml/h of 10% glucose may need to be considered (27).
Prolonged hypoglycemic coma
Prolonged hypoglycemic coma occurs due to cerebral
edema and is defined by a duration of >5 h. In this case it is
necessary to administer mannitol i.v. and dexamethasone with
constant monitoring of glucose, and glucose i.v. to maintain the
serum level at 90-180 mg/dl until consciousness has been restored,
otherwise permanent brain damage can occur. If hypoglycemia has
been caused by an overdose of insulin or sulfonylurea, 80 g/h of
25-50% glucose may be required via a central line (25).
Treatment of hypoglycemia in
children
Rapid treatment of hypoglycemia in children is
crucial to prevent neurological damage. If the state of
consciousness is maintained, the treatment is commenced by
administering 10-20 g of glucose orally followed by the
administration of fast carbohydrates in liquid form (milk 200 ml)
or in solid form (2 teaspoons of sugar). If necessary, this can be
repeated after 10-15 min (28,29).
Severe hypoglycemia, with unconscious state is an
emergency as sugar cannot be administered orally; thus, the only
solution is to inject glucagon (29-34).
If glucagon is not effective within 10 min, administration of 33 or
10% glucose intravenously is required. After regaining
consciousness, carbohydrates should be administered as soon as
possible to restore liver glycogen.
Another possibility of treatment of hypoglycemia
consists in the administration of octreotide in a bolus of 1-2
µg/kg every 6-8 h or in an infusion of 30 µg/kg/min. Glucagon is
not effective in treating hypoglycemia due to fatty acid oxidation
or glycogen storage disorders. It is also not indicated for the
treatment of chronic hypoglycemia (29-34).
5. Conclusions
The current diagnostic and therapeutic approach to
emergencies that occur in the evolution of diabetes is based on
fairly well-developed guidelines and is consistent with scientific
data known thus far regarding this condition. However, at present,
the addressability of patients with acute complications of diabetes
to EDs, especially those with diabetic coma, remains extremely
high.
Most emergencies that occur in the evolution of
diabetes and presented to the EDs have diabetes, ketoacidosis,
hyperosmolar and hypoglycemic comas, all of which are
life-threatening and with very high lethal potential. The
therapeutic approach to coma in the ED may require intubation and
ventilation of the patient, correction of acid-base and
hydroelectrolytic imbalances, but especially correction of the
level of serum blood glucose.
In addition to the correction of specific changes
induced in addition to or without the glycemic level, the treatment
of the causes that induce diabetic comas must be considered,
especially in those with DKA or HHS. Currently the avoidance of
these complications is based only on proper diet, stress avoidance,
judicious treatment with numerous adjustments of oral antidiabetic
doses or insulin doses which makes it considerably complicated for
the contemporary world.
Despite recent discoveries in genetics and molecular
medicine, no therapy or method has yet been found to allow the
diabetic patient to lead a normal life in terms of diet and
adaptability to daily stress and compliance to the therapeutic
regime imposed by this condition.
Acknowledgements
Not applicable.
Funding
Funding: This work was supported by the dates obtained from the
grant (research contract no. 26/40C/06.10.2021) with the research
topic: Adult cardiovascular diseases in the context of acquired
carbohydrate and lipid metabolic imbalances-from the silence of
evolution to the drama of acute episodes in emergency units and
compartments conducted by Maria Forțofoiu, as project director, in
collaboration with the ‘Didactica Association’ and the University
of Medicine and Pharmacy Craiova.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
MF, IMV, MCF, RP, DC, DR and VP contributed equally
to the acquisition, analysis and systematization of data,
manuscript writing and critical revision thereof for important
intellectual content. All authors read and approved the final
version of the manuscript. Data authentication is not
applicable.
Ethics approval and consent to
participate
Not applicable.
Patients consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Singh RK, Perros P and Frier BM: Hospital
management of diabetic ketoacidosis: Are clinical guidelines
implemented effectively? Diabet Med. 14:482–486. 1997.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Hardern RD and Quinn ND: Emergency
management of diabetic ketoacidosis in adults. Emerg Med J.
20:210–213. 2003.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Basu A, Close CF, Jenkins D, Krentz AJ,
Nattrass M and Wright AD: Persisting mortality in diabetic
ketoacidosis. Diabet Med. 10:282–284. 1993.PubMed/NCBI
|
|
4
|
Kitabchi AE and Wall BM: Diabetic
ketoacidosis. Med Clin North Am. 79:9–37. 1995.PubMed/NCBI View Article : Google Scholar
|
|
5
|
American Diabetes Association (ADA):
Hyperglycemic Crises Consensus Guidelines, 2009. https://care.diabetesjournals.org/content/32/Supplement_1/S13.
Access date: September 1, 2021.
|
|
6
|
Dhatariya K, Savage M, Claydon A, Dyer P,
Evans P, Khan A, et al: Joint British Diabetes Societies (JBDS).
Inpatient Care Group: The management of diabetic ketoacidosis in
adults, Second edition, 2013. http://www.diabetologists-abcd.org.uk/JBDS/JBDS_IP_DKA_Adults_Revised.pdf.
Access date: September 1, 2021.
|
|
7
|
Westerberg DP: Diabetic ketoacidosis:
Evaluation and treatment. Am Fam Physician. 87:337–346.
2013.PubMed/NCBI
|
|
8
|
Umpierrez G and Korytkowski M: Diabetic
emergencies-ketoacidosis, hyperglycaemic hyperosmolar state and
hypoglycaemia. Nat Rev Endocrinol. 12:222–232. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Yared Z and Chiasson JL: Ketoacidosis and
the hyperosmolar hyperglycemic state in adult diabetic patients.
Diagnosis and treatment. Minerva Med. 94:409–418. 2003.PubMed/NCBI
|
|
10
|
Kitabchi AE and Nyenwe EA: Hyperglycemic
crises in diabetes mellitus: Diabetic ketoacidosis and
hyperglycemic hyperosmolar state. Endocrinol Metab Clin North Am.
35:725–751. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Kitabchi AE, Umpierrez GE, Miles JM and
Fisher JN: Hyperglycemic crises in adult patients with diabetes.
Diabetes Care. 32:1335–1343. 2009.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Palmer BF and Clegg DJ: Electrolyte and
acid-base disturbances in patients with diabetes mellitus. N Engl J
Med. 373:548–559. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Grigorescu ED, Lăcătușu CM, Crețu I,
Floria M, Onofriescu A, Ceasovschih A, Mihai BM and Șorodoc L:
Self-reported satisfaction to treatment, quality of life and
general health of type 2 diabetes patients with inadequate glycemic
control from North-Eastern Romania. Int J Environ Res Public
Health. 18(3249)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kamel KS and Halperin ML: Acid-base
problems in diabetic ketoacidosis. N Engl J Med. 372:1969–1970.
2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Magder S and Emami A: Practical approach
to physical-chemical acid-base management. Stewart at the bedside.
Ann Am Thorac Soc. 12:111–117. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Seifter JL: Integration of acid-base and
electrolyte disorders. N Engl J Med. 371:1821–1831. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Story DA and Kellum JA: New aspects of
acid-base balance in intensive care. Curr Opin Anaesthesiol.
17:119–123. 2004.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Schiraldi F and Guiotto G: Base excess,
strong ion difference, and expected compensations: As simple as it
is. Eur J Emerg Med. 21:403–408. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Fisher JN and Kitabchi AE: A randomized
study of phosphate therapy in the treatment of diabetic
ketoacidosis. J Clin Endocrinol Metab. 57:177–180. 1983.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wilson HK, Keuer SP, Lea AS, Boyd AE III
and Eknoyan G: Phosphate therapy in diabetic ketoacidosis. Arch
Intern Med. 142:517–520. 1982.PubMed/NCBI
|
|
21
|
Fayfman M, Pasquel FJ and Umpierrez GE:
Management of hyperglycemic crises: Diabetic ketoacidosis and
hyperglycemic hyperosmolar state. Med Clin North Am. 101:587–606.
2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
American Diabetes Association. Hospital
admission guidelines for diabetes (Position Statement). Diabetes
Care. 27 (Suppl 1)(S103)2004.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Tomky D: Detection, prevention, and
treatment of hypoglycemia in the hospital. Diabetes Spectrum.
18:39–44. 2005.
|
|
24
|
Greenhalgh T: Oxford Τextbook of Μedicine.
4th edition. Warrell DA, Cox TM, Firth JD and Benz Jr EJ (eds).
Family Practice 20, Oxford University Press, Oxford, 2003.
|
|
25
|
Walden E, Stanisstreet D, Graveling A, et
al: Joint British Diabetes Societies: The hospital management of
hypoglycaemia in adults with diabetes mellitus. Third edition.
Diabetes UK, 2013. https://www.diabetes.org.uk/professionals/position-statements-reports/specialist-care-for-children-and-adults-and-complications/the-hospital-management-of-hypoglycaemia-in-adults-with-diabetes-mellitus.
Access date: September 1, 2021.
|
|
26
|
Achoki R, Opiyo N and English M:
Mini-review: Management of hypoglycaemia in children aged 0-59
months. J Trop Pediatr. 56:227–234. 2010.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Frier BM: How hypoglycaemia can affect the
life of a person with diabetes. Diabetes Metab Res Rev. 24:87–92.
2008.PubMed/NCBI View
Article : Google Scholar
|
|
28
|
Pearson T: Glucagon as a treatment of
severe hypoglycemia: Safe and efficacious but underutilized.
Diabetes Educ. 34:128–134. 2008.PubMed/NCBI View Article : Google Scholar
|
|
29
|
International Diabetes Federation: IDF
Diabetes Atlas. 9th edition. International Diabetes Federation,
Belgium, 2019. https://diabetesatlas.org/atlas/ninth-edition/. Access
date: September 1, 2021.
|
|
30
|
Chen YT, Tan YZ, Cheen M and Wee HL:
Patient-reported outcome measures in registry-based studies of type
2 diabetes mellitus: A systematic review. Curr Diabetes Rep.
19(135)2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Grigorescu E, Sorodoc V, Floria M, Anisie
E, Popa AD, Onofriescu A, Ceasovschih A and Sorodoc L: The
inflammatory marker HSCRP as a predictor of increased insulin
resistance in type 2 diabetics without atherosclerotic
manifestations. Rev Chim (Bucharest). 70:1791–1794. 2019.
|
|
32
|
Trikkalinou A, Papazafiropoulou AK and
Melidonis A: Type 2 diabetes and quality of life. World J Diabetes.
8:120–129. 2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Palamenghi L, Carlucci MM and Graffigna G:
Measuring the quality of life in diabetic patients: A scoping
review. J Diabetes Res. 2020(5419298)2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Speight J, Holmes-Truscott E, Hendrieckx
C, Skovlund S and Cooke D: Assessing the impact of diabetes on
quality of life: What have the past 25 years taught us? Diabet Med.
37:483–492. 2020.PubMed/NCBI View Article : Google Scholar
|