Introduction
To date, the potential side-effects of alternative
medicine remedies have remained largely elusive. Sodium bicarbonate
(baking soda) is a low-cost, accessible, over-the-counter
substance, widely recognized for its multiple uses. Most
frequently, it is consumed as an antacid, despite the availability
of proton pump inhibitors and H2 blockers (1). The undesired effects of baking soda
misuse may present as different clinical scenarios, which have not
been systematized until now. While baking soda is generally
considered safe, various cases who developed metabolic alkalosis
and electrolyte imbalances due to baking soda overdose have been
documented (1). The present study
reported on a case of metabolic alkalosis caused by baking soda
misuse and provided a review of similar cases published to date. To
the best of our knowledge, the patient of the present study is the
first reported case of baking soda toxicity related to its oral
ingestion as an alternative remedy for gout.
Case report
Case presentation
A 69-year-old male patient was referred to the
neurology emergency department of ‘N. Oblu’ Emergency Hospital
(Iasi, Romania) in October 2021, by his family due to altered
mental state, including confusion, which started 2 days prior to
admission, with progressive worsening. The neurological exam did
not reveal any focal clinical signs and craniocerebral CT excluded
the possibility of an acute neurological event. A brief biological
investigation indicated elevated serum creatinine levels (4.02
mg/dl; normal range, 0.6-1.2 mg/dl), metabolic alkalosis (pH 7.61;
normal range, 7.31-7.41) bicarbonate levels in blood plasma of 53.2
mmol/l (normal range, 22-29 mmol/l) and hypokalemia (serum
potassium K+, 2.6 mEq/l; normal range, 3.5-5.1 mEq/l).
On the next day, the patient was consequently referred to the
Nephrology Department of the Clinical Hospital ‘Dr C.I. Parhon’
(Iasi, Romania) for further investigation.
Medical history. The patient's medical
history included gout diagnosed in 1974, without any rheumatology
consultation, for which the patient received intermittent treatment
with colchicine 1 mg once daily (od) (3-6 months/year), ketoprofen
100 mg twice daily (bid) and allopurinol 100 mg/day od. The
patient's cardiovascular antecedents included third-degree arterial
hypertension and permanent atrial fibrillation since 2015, for
which he was chronically anticoagulated with a direct oral
anticoagulant (DOAC) (apixaban 5 mg bid). The patient's home
medication also included a β-blocker (carvedilol 6.25 mg bid), an
angiotensin II receptor blocker (candesartan 8 mg bid), a diuretic
(indapamide 1.5 mg od) and a statin (atorvastatin 20 mg od). The
patient had recently undergone surgical interventions for a
perianal fistula, and on this occasion, examination revealed
elevated creatinine levels, interpreted in the context of chronic
uric acid nephropathy (1.9 mg/dl in April 2021). The perianal
fistula was interpreted in the context of prolonged sitting due to
the patient's occupation as a bus driver.
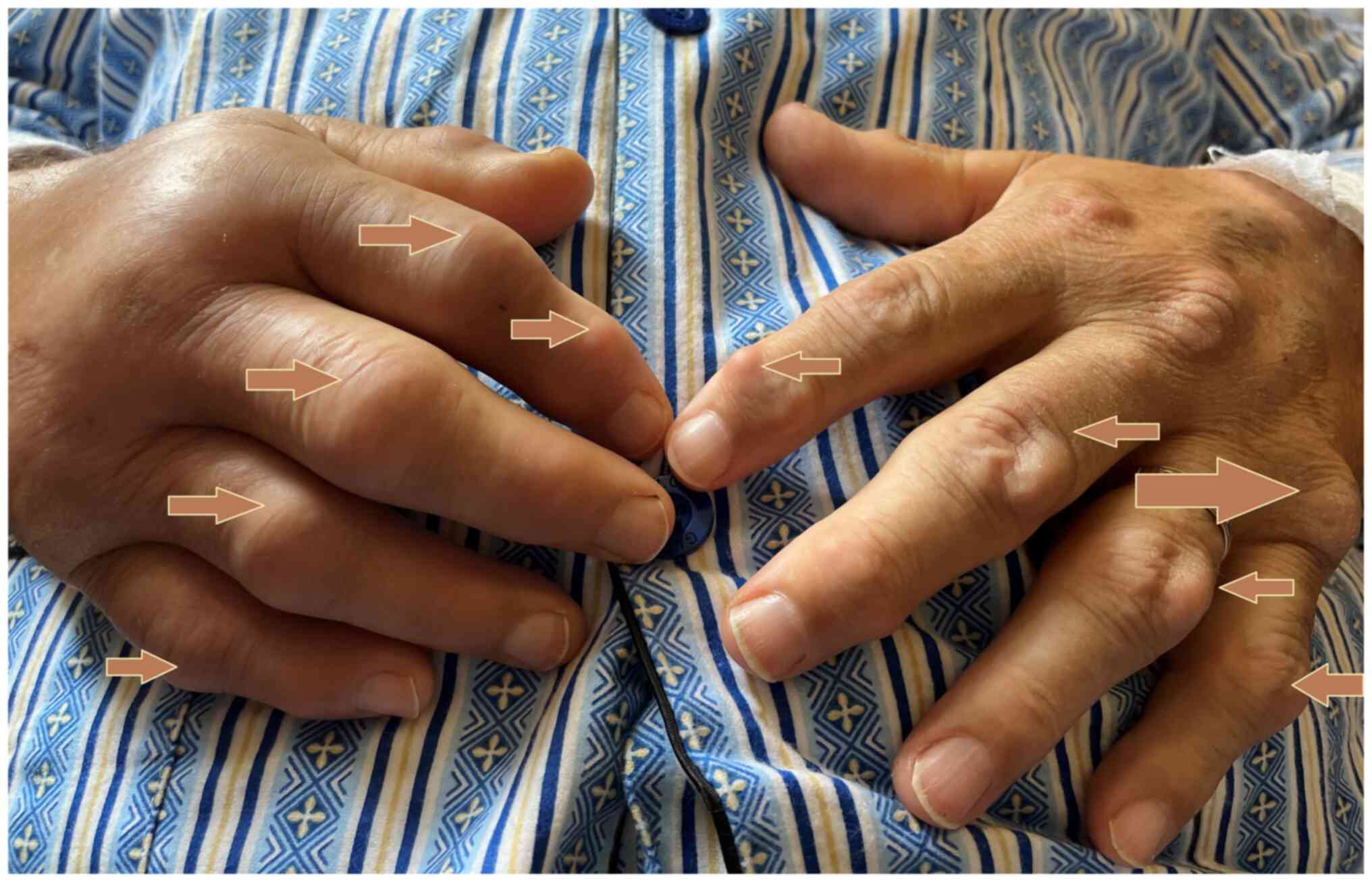
Physical examination upon admission. The
patient had an altered mental state, namely he was confused and
agitated, without fever (temperature of 36.5˚C), with a heart rate
of 100 beats/min, blood pressure of 110/80 mmHg, respiratory rate
of 13 breaths/min and oxygen saturation of 98% on room air. Close
examination revealed multiple tophi on the extremities and celsian
signs on the extremities (redness, swelling, heat and pain)
(Fig. 1). According to the 2015
ACR-EULAR Gout Classification Criteria, the score calculated for
our patient is 20 (out of 23) (2).
Cardiac examination revealed an irregular heart rate and rhythm
with no murmur or extra heart sounds. The lungs were clear of
auscultation bilaterally. No peripheral edema was noted.
The electrocardiogram on admission revealed atrial
fibrillation with a ventricular rate of 104 beats/min, a -15˚ QRS
axis and left anterior fascicular block.
The blood tests indicated elevated serum creatinine
and urea levels [creatinine, 4.02 mg/dl; urea, 148 mg/dl (normal
range, 20-49 mg/dl)]; hypochloremic metabolic alkalosis (pH 7.61);
bicarbonate, 53.2 mmol/l; pCO2, 53 mmHg; Cl, 78 mEq/l
(normal range, 94-110 mEq/l in blood plasma), hypokalemia
(K+, 2.6 mEq/l), elevated hepatic cytolysis enzymes,
including alanine transaminase (955 U/l; normal range, 4-33 U/l);
aspartate transaminase (1,091 U/l; normal range, 8-35 U/l),
hyperuricemia [serum uric acid (SUA), 10.3 mg/dl; normal range,
3.5-7 mg/dl], inflammatory syndrome [white blood cells,
10,920/mm3; normal range, 4,000-10,000/mm3;
C-reactive protein, 440 mg/l; normal range, <5 mg/l; erythrocyte
sedimentation rate (ESR) >140 mm/h; normal range, 1-10 mm/h];
and normocytic normochromic anemia [red blood cells, 3,49
million/mm3 (normal range,
4.6-6.0x106/mm3); hemoglobin, 10.5 g/dl,
(normal range, 13-16 g/dl); hematocrit, 35.2% (normal range,
40-50%). The secretion culture from the perianal fistula was
positive for Staphylococcus aureus and Proteus
mirabilis.
Treatment of the patient
Given the patient's altered mental state, a thorough
anamnesis was only possible on the second day of hospitalization at
the nephrology department, revealing that the patient had consumed
20 g of baking soda dissolved in 2 liters of water per day as an
alternative treatment for ‘dissolving the tophi’ in the week prior
to admission.
Intravenous (iv) hydration with physiological serum
0.9% 1,000 ml, iv KCl 60 mEq/l/day was initiated along with
potassium correction, iv dexamethasone 6 mg and per os
colchicine 0.5 mg (1 tablet twice per day) for gout attack and
antibiotic therapy with ceftriaxone 1 g twice per day in accordance
with the antibiogram for 7 days. The in-hospital response of the
patient was favorable, with remission of the hydro-electrolyte and
acid-base imbalances. At discharge, the hepatic injury and
inflammation markers were within normal limits and the creatinine
serum level was 1.9 mg/dl. Angiotensin II receptor blocker
treatment was ceased, with normal in-hospital blood pressure
control. Given the atrial fibrillation, heart rate,
CHA2D2-VASc score (a score used to assess the
risk of stroke in atrial fibrillation patients defined by the
Congestive heart failure, Hypertension, Age ≥75 years, Diabetes
mellitus, Stroke, Vascular disease, Age 65-74 years, Sex
category-female) of 3 points and HAS-BLED score of 3 points (a
score to predict bleeding risk based on the following risk factors:
Hypertension, Abnormal renal/liver function, Stroke, Bleeding
history or predisposition, Labile INR, Elderly - >65 years,
drugs/alcohol; a score over 3 indicates high bleeding risk), the
patient was discharged with instructions to continue his DOAC and
β-blocker therapy (3). In
addition, febuxostat therapy with a low starting dose (40 mg od)
was prescribed.
Treatment outcomes and follow-up
The 1-month follow-up revealed a euvolemic,
hemodynamically stable patient. Post-discharge creatinine levels
were stationary, while SUA levels improved (SUA, 6.5 mg/dl).
At-home blood pressure control was adequate without angiotensin II
receptor blocker. However, the patient complained about the acute
gout arthritis of his upper left limb (Fig. 2). At 1 day prior to his follow-up,
the patient consulted a rheumatologist who recommended short-term
colchicine administration and an increase of the dose of febuxostat
to 80 mg od.
Discussion
A literature search was performed in the
PubMed/MEDLINE and ScienceDirect/Elsevier electronic databases for
reported cases of sodium bicarbonate toxicity in adult patients.
Search terms included ‘baking soda misuse’, ‘baking soda toxicity’,
‘baking soda overdose’, ‘sodium bicarbonate misuse’, ‘sodium
bicarbonate toxicity’ and ‘sodium bicarbonate overdose’. References
from the included articles were also scanned to identify possible
additional publications.
EndNote X7 (Thomson Reuters) bibliography manager
was used to check the title and abstracts of the retrieved and
screened articles. Duplicate articles were electronically and
manually removed (in the case of differences in the citation style
of the different journals). After screening all the relevant
articles found, a total of 21 clinical cases published between 1986
and 2020 were included. Basic characteristics of the studies were
summarized in Table I (name of the
first author, year of publication, medical history, baking soda
exposure, methods of diagnosis, laboratory values, reference test).
Baking soda is a commonly used remedy to counteract high acidity
symptoms, such as heartburn. However, other uses include the
treatment of hyperkalemia, metabolic acidosis, prevention of
contrast-induced nephropathy and urine alkalinization (4). According to popular beliefs, sodium
bicarbonate, as a strong base, neutralizes the acidic state in
which uric acid precipitates. Although no scientific evidence
supports these effects, baking soda has gained popularity as an
alternative treatment for gout. As an over-the-counter antacid,
baking soda is considered safe by the Food and Drug Administration
at a maximum daily dosage of 200 mEq sodium bicarbonate in young
individuals and 100 mEq sodium bicarbonate in those aged >60
years (5). One teaspoon (5 g) of
baking soda contains ~59 mEq of sodium bicarbonate (6). The patient of the present study
declared the intake of ~20 g of sodium bicarbonate, which
translates into ~238 mEq sodium bicarbonate, exceeding the
recommended safe dose.
 | Table IList of reported cases of baking soda
toxicity in adult patients. |
Table I
List of reported cases of baking soda
toxicity in adult patients.
| First author,
year | Presentation | Medical history | Baking soda
exposure | Laboratory
values | (Refs.) |
|---|
| Al-Abri and Olson,
2013 | Metabolic alkalosis
Ventricular tachycardia | HTN DM
Zollinger-Ellison syndrome | Antacid replacement:
1 teaspoon of baking soda on an as needed basis for years | pH 7.5
HCO3 | (6) |
| 46 mmol/l |
| K+ 2.0
mEq/l |
| Na+ 122
mEq/l |
| Cl- 59
mEq/l |
| Cr 0.9 mg/dl |
| Cervantes et
al, 2020 | Metabolic
alkalosis | CKD G3bA1 HTN AF
Hyperlipidemia GERD | Topical use three
times/day for tooth hygiene for the previous 6 months | pH 7.5 | (8) |
| HCO3 44
mmol/l |
| K+ 3.6
mEq/l |
| Na+ 146
mEq/l |
| Cl- 95
mEq/l |
| Cr 1.37 mg/dl |
| Solak et al,
2009 | Metabolic alkalosis
Sleep apnea Volume overload Uncontrolled HTN | ESRD CHF DM type 2
Hypothyroidism Chronic gastritis | Antacid abuse: 4-5
packs of baking soda a day over the last month Cl- 83
mEq/l | pH 7 637 | (9) |
| HCO3 45
mmol/l |
| K+ 3.3
mEq/l |
| Na+ 141
mEq/l |
| Sahani et al,
2001 | Metabolic
alkalosis | ESRD | Hiccup relief:
Consumption of ¾ bottle of Bromo-Seltzer (containing 89 g sodium
bicarbonate) | pH 7.53
HCO3 | (10) |
| 40 mmol/l
K+ |
| 3.5 mEq/l |
| Na+ 143
mEq/l |
| Cl- 89
mEq/l |
| Cr 1.0 mg/dl |
| Galinko et al,
2017 | Metabolic alkalosis
Acute kidney injury Acute hypoxic respiratory failure Lactic
acidosis Altered mental state Ventricular tachycardia | HTN Meningioma
(surgical resection, ventriculoperitoneal shunt and radiation
therapy) Breast cancer | Alternative topical
treatment for breast cancer -113 g of baking soda applied topically
every 4 days for several weeks | pH 7.66 | (11) |
| HCO3
>45 mmol/l |
| K+ 2.6
mEq/l |
| Na+ 158
mEq/l |
| Cl- 92
mEq/l |
| Cr 1.9 mg/dl |
| Soliz et al,
2014 | Metabolic
alkalosis | Colon cancer
Sinonasal melanoma | Alternative
treatment for colon cancer: 1 liter of pH 7.8-8 water obtained from
bottled water, key lime juice a quarter of tablespoon baking
soda | pH 7.65 | (12) |
| HCO3 39
mmol/l |
| K+ 2.6
mEq/l |
| Na+ 123
mEq/l |
| Okada et al,
1996 | Metabolic alkalosis
and myoclonus | HTN Cerebral
infarction Gastrectomy (gastric ulcer) | Antacid (625 mg
sodium bicarbonate) for a 6-month period | pH 7.481 | (13) |
| HCO3
33.9 mmol/l |
| K+ 2.7
mEq/l |
| John et al,
2012 | Metabolic alkalosis
Respiratory alkalosis High-anion gap metabolic acidosis | Foot ulcers for 2
years | Ingestion and
application of baking soda to leg ulcers for 1.5 years | pH 7.69 | (14) |
| HCO3 54
mmol/l |
| K+ 1.8
mEq/l |
| Na+ 148
mEq/l |
| Cl- 73
mEq/l |
| Cr 3.4 mg/dl |
| Hughes et
al, 2016 | Metabolic alkalosis
Hypernatremia Hemorrhagic encephalopathy Altered mental state | Schizophrenia
Polysubstance abuse | Patient was unable
to explain cause of ingestion- 1 box of baking soda (454 g) | pH 7.53 | (15) |
| HCO3 50
mEq/l |
| K+ 2.5
mEq/l |
| Na+ 172
mEq/l |
| Cl- 98
mEq/l |
| Glucose |
| 433 mg/dl Cr |
| 1.85 mg/dl |
| Ajbani et
al, 2011 | Metabolic
alkalosis | HTN COPD | Antacid
replacement: Unknown quantity of baking soda over several
weeks | pH 7.59 | (16) |
| HCO3 56
mmol/l |
| K+ 1.7
mEq/l |
| Na+ 121
mEq/l |
| Cl- 53
mEq/l |
| Cr 3.3 mg/dl |
| Fitzgibbons and
Snoey, 1999 (Case 1) | Metabolic alkalosis
Ventricular tachydysrhythmia | Peptic ulcer
disease with perforation | Antacid
replacement: Several tablespoons of baking soda | pH 7.56 | (17) |
| HCO3 58
mmol/l |
| K+ 1.8
mEq/l |
| Na+ 129
mEq/l |
| Cl- 55
mEq/l |
| Cr 2.8 mg/dl |
| Fitzgibbons and
Snoey, 1999 (Case 2) | Metabolic alkalosis
Altered mental state | HTN Herpes zoster
infection Hepatitis | Antacid
replacement: One box of baking soda | pH 7.49 | (17) |
| HCO3 41
mmol/l |
| K+ 2.8
mEq/l |
| Na+ 146
mEq/l |
| Cl- 90
mEq/l |
| Cr 0.9 mg/dl |
| Thomas and Stone,
1994 | Metabolic
alkalosis | Alcoholic
esophagitis and gastritis | Antacid misuse:
10-12 oz of baking soda | pH 7.55 | (18) |
| HCO3
44.5 mmol/l |
| Na+ 136
mEq/l |
| K+ 2.5
mEq/l |
| Cl- 77
mEq/l |
| Cr 2.4 mg/dl |
| Gawarammana et
al, 2007 | Metabolic alkalosis
Coma (GCS 3/15) | N/A | Antacid: 2 liters
of Gaviscon in the prior 48 h | pH 7.54 | (19) |
| HCO3
50.6 mmol/l |
| K+ 1.6
mEq/l |
| Na+ 127
mEq/l |
| Cl- 66
mEq/l |
| Mennen and Slovis,
1988 | Metabolic alkalosis
Cardiopulmonary arrest Death | HTN Peptic ulcer
disease Alcohol abuse Seizure disorder | Antacid misuse:
Amount unknown | pH 7.73 | (20) |
| HCO3
>40 mmol/l |
| Na+ 154
mEq/l |
| K+ 3.2
mEq/l |
| Cl- 53
mEq/l |
| Cr 1.4 mg/dl |
| Forslund et
al, 2008 | Metabolic alkalosis
Epileptiformic convulsions Subdural hemorrhage Rhabdomyolysis | Alcohol abuse | Antacid abuse: 40
years history of baking soda abuse; 10-15 g daily initially, slowly
increasing up to 50 g daily during last year | pH 7.57 | (21) |
| HCO3 85
mmol/l |
| K+ 2.3
mEq/l |
| Na+ 147
mEq/l |
| Cl- 46
mEq/l |
| Yi et al,
2012 | Metabolic
alkalosis | Alcohol abuse | Antacid
replacement: 3-5 tablespoons daily | pH 7.6 | (22) |
| HCO3 53
mmol/l |
| K+ 1.6
mEq/l |
| Na+ 131
mEq/l |
| Cl- 65
mEq/l |
| Cr 3.8 mg/dl |
| Scolari Childress
and Myles, 2013 | Rhabdomyolysis
Peripartum cardiomyopathy | Pregnant, at 37
weeks of gestation with history of hyperemesis and iron-deficiency
anemia | Hiccup remedy: A
box of baking soda (454 g) every day for several years | Hb 8.2 g/dl Ht
26.3% | (23) |
| K+ 2.1
mmol/l |
| AST 134 U/l |
| ALT 60 U/l |
| Lazebnik et
al, 1986 | Stomach
rupture | N/A | Antacid misuse: One
tablespoon of sodium bicarbonate | N/A | (24) |
| Linford and James,
1986 | Metabolic
alkalosis | N/A | Bicarbonate abuse:
50-150 g daily | HCO3
>40 mmol/l K+ 1.8 mEq/l | (25) |
| Okada et al,
1999 | Metabolic alkalosis
Sleep apnea Hypertension | ESRD | Antacid
replacement: | pH 7.47
HCO3 | (26) |
| 40.1 mmol/l |
The increase in renal tubular pH by baking soda
alters the excretion of anti-inflammatory medications, increasing
their serum levels (7). In the
specific case of the present study, this may explain the onset of
acute kidney injury and liver toxicity as a result of high intake
of baking soda combined with ketoprofen. Caution should be advised
when prescribing sodium bicarbonate, particularly when combined
with non-steroidal anti-inflammatory drugs or other
anti-inflammatory drugs.
Chronic interstitial nephritis that is associated
with hyperuricemia may be considered when SUA levels are
disproportionately high in contrast with the patient's renal
impairment (4). Patients usually
consult the medical unit with hypertension and mildly impaired
renal function. Minor proteinuria and tubular dysfunction may be
present (4). Given the patient's
poor response to allopurinol over the years, the choice of chronic
treatment recommendation for the present case was febuxostat, a
selective xanthine oxidase inhibitor, with a low starting dose (40
mg od). In contrast to allopurinol, febuxostat does not require
dose adjustments at a lower estimated glomerular filtration rate
and is associated with a smaller incidence of hypersensitivity or
nephrotoxicity (4). At the 1-month
follow-up, the patient's condition was under good control with
febuxostat treatment, with normal SUA levels.
Metabolic alkalosis due to baking soda oral
ingestion to treat dyspepsia has been previously reported. A number
of cases of adverse toxic effects of topically applied baking soda
have been reported, which was used as an alternative to
chemotherapy for breast (5) and
colon cancer (6), for the
treatment of leg ulcer (7) and as
a toothpaste additive (8). A
review indicated that the most common reasons for bicarbonate
exposure were antacid misuse (60.4%), urinary drug testing
alterations (11.5%), treatment of urinary tract infections (4.7%)
and as a means for body detoxification (4.7%) (1). A case of misuse as a remedy for gout
was also identified (1).
The most common presentation of baking soda toxicity
is metabolic alkalosis and electrolyte changes. Usually, the kidney
responds by increasing bicarbonate excretion, which may become
impaired in the setting of renal insufficiency or volume
contraction. Metabolic acidosis is a common finding in chronic
kidney disease (4). Though less
common in patients with end-stage renal disease undergoing
hemodialysis, there were 2 reported cases of metabolic alkalosis
attributed to oral baking soda intake (9,10).
In spite of a history of third-degree arterial
hypertension, the patient of the present study had controlled blood
tension values without the use of any hypotensive agent both during
hospitalization and at the 1-month follow-up. However, further
monitoring is necessary to evaluate whether the effect is temporary
and investigate its cause. Previously, 2 cases who developed
hypotension and required vasopressors for hemodynamic support were
reported (11,12). One of them also exhibited a
decrease in anesthetic demand (12). On the other hand, transient daytime
hypertension has been observed, but was interpreted in the context
of sleep apnea (13).
The altered mental state of the patient of the
present study delayed the accurate identification of the underlying
cause of metabolic alkalosis. Mental state alterations are common
in patients with severe metabolic alkalosis. Agitation and
confusion (14-16),
dizziness with or without loss of consciousness (17,18),
stuttering (15), obnubilation
(11) and coma (19,20)
have been reported. For 1 case, hypernatremic hemorrhagic
encephalopathy due to baking soda ingestion was reported, with
multiple areas of intracranial and subarachnoid hemorrhage observed
on the cranial computed tomography (15). Neuromuscular symptoms are commonly
described in patients with severe metabolic alkalosis. Paresthesia
and carpopedal spasm without a positive Chvostek's sign (20), involuntary facial twitching
(15), increased motor tone with
flexion of elbows and wrists (20), myoclonus (13) and epileptiform convulsions
(21) have also been described.
Furthermore, 2 patients with sleep apnea were referred, which may
occur in the metabolic alkalosis setting due to central ventilatory
drive depression (9,13).
Patients with a history of alcohol abuse may have an
increased susceptibility to developing metabolic alkalosis due to
high baking soda intake (17,18,20-22).
Chronic alcoholics are more inclined to ingest antacids for
dyspepsia relief, while their dehydration status may promote and
aggravate metabolic alterations. Rhabdomyolysis has been reported
in an alcoholic patient (21) and
in pregnant patients with pica leading to baking soda intake
(23). Other systemic
complications, such as spontaneous gastric rupture, have also been
described (24).
In conclusion, the present study reported a case of
baking soda toxicity resulting in metabolic alkalosis, toxic acute
hepatitis and acute kidney injury. The case described herein
provided a challenge in establishing a diagnosis of metabolic
alkalosis with unknown etiology until thorough anamnesis was
possible. The present case report and literature review highlights
the importance of closely evaluating all the alternative therapies
that patients resort to. Exposure to these substances may not be
easily disclosed, as their implications are frequently underrated.
Physicians should be aware of the potential practices and
associated side effects in order to ensure prompt diagnosis and
adequate treatment.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
All authors substantially contributed to this paper.
AD and LF designed the study, searched the literature and wrote the
first draft of the manuscript. CEV, IF and RA collected and
interpreted the relevant data. AD, LF and IF confirm the
authenticity of all the raw data. CEV and LF supervised the
literature review and revised the manuscript for important
intellectual content. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent for
the publication of this case report, including medical information
and the accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Al-Abri SA and Kearney T: Baking soda
misuse as a home remedy: Case experience of the california poison
control system. J Clin Pharm Ther. 39:73–77. 2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Neogi T, Jansen TL, Dalbeth N, Fransen J,
Schumacher HR, Berendsen D, Brown M, Choi H, Edwards NL, Janssens
HJ, et al: 2015 gout classification criteria: An American college
of Rheumatology/European league against rheumatism collaborative
initiative. Arthritis Rheumatol. 67:2557–2568. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Hindricks G, Potpara T, Dagres N, Arbelo
E, Bax JJ, Blomstrom-Lundqvist C, Boriani G, Castella M, Dan GA,
Dilaveris PE, et al: 2020 ESC Guidelines for the diagnosis and
management of atrial fibrillation developed in collaboration with
the European association for cardio-thoracic surgery (EACTS): The
task force for the diagnosis and management of atrial fibrillation
of the European society of cardiology (ESC) Developed with the
special contribution of the European heart rhythm association
(EHRA) of the ESC. Eur Heart J. 42:373–498. 2021.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Feehally J, Floege J, Tonelli M and
Johndon RJ: Comprehensive Clinical Nephrology. 6th edition,
2019.
|
|
5
|
Jouffroy R and Vivien B: Sodium
bicarbonate administration and subsequent potassium concentration
in hyperkalemia treatment: Do not forget the initial pH-value. Am J
Emerg Med. 56:302–303. 2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Al-Abri SA and Olson KR: Baking soda can
settle the stomach but upset the heart: Case files of the Medical
Toxicology fellowship at the university of California, San
Francisco. J Med Toxicol. 9:255–258. 2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Senewiratne NL, Woodall A and Can AS:
Sodium Bicarbonate. StatPearls Publishing, Treasure Island, FL,
2022.
|
|
8
|
Cervantes CE, Menez S, Jaar BG and
Hanouneh M: An unusual cause of metabolic alkalosis: Hiding in
plain sight. BMC Nephrol. 21(296)2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Solak Y, Turkmen K, Atalay H and Turk S:
Baking soda induced severe metabolic alkalosis in a haemodialysis
patient. NDT Plus. 2:280–281. 2009.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Sahani MM, Brennan JF, Nwakanma C, Chow
MT, Ing TS and Leehey DJ: Metabolic alkalosis in a hemodialysis
patient after ingestion of a large amount of an antacid medication.
Artif Organs. 25:313–315. 2001.PubMed/NCBI
|
|
11
|
Galinko LB, Hsu SH, Gauran C, Fingerhood
ML, Pastores SM, Halpern NA and Chawla S: A basic therapy gone
awry. Am J Crit Care. 26:491–494. 2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Soliz J, Lim J and Zheng G: Anesthetic
management of a patient with sustained severe metabolic alkalosis
and electrolyte abnormalities caused by ingestion of baking soda.
Case Rep Anesthesiol. 2014(930153)2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Okada K, Kono N, Kobayashi S and Yamaguchi
S: Metabolic alkalosis and myoclonus from antacid ingestion. Intern
Med. 35:515–516. 1996.PubMed/NCBI View Article : Google Scholar
|
|
14
|
John RS, Simoes S and Reddi AS: A patient
with foot ulcer and severe metabolic alkalosis. Am J Emerg Med.
30:260 e5–8. 2012.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Hughes A, Brown A and Valento M:
Hemorrhagic encephalopathy from acute baking soda ingestion. West J
Emerg Med. 17:619–622. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ajbani K, Chansky ME and Baumann BM:
Homespun remedy, homespun toxicity: Baking soda ingestion for
dyspepsia. J Emerg Med. 40:e71–e74. 2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Fitzgibbons LJ and Snoey ER: Severe
metabolic alkalosis due to baking soda ingestion: Case reports of
two patients with unsuspected antacid overdose. J Emerg Med.
17:57–61. 1999.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Thomas SH and Stone CK: Acute toxicity
from baking soda ingestion. Am J Emerg Med. 12:57–59.
1994.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Gawarammana IB, Coburn J, Greene S, Dargan
PI and Jones AL: Severe hypokalaemic metabolic alkalosis following
ingestion of gaviscon. Clin Toxicol (Phila). 45:176–178.
2007.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Mennen M and Slovis CM: Severe metabolic
alkalosis in the emergency department. Ann Emerg Med. 17:354–357.
1988.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Forslund T, Koistinen A, Anttinen J,
Wagner B and Miettinen M: Forty years abuse of baking soda,
rhabdomyolysis, glomerulonephritis, hypertension leading to renal
failure: A case report. Clin Med Case Rep. 1:83–87. 2008.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Yi JH, Han SW, Song JS and Kim HJ:
Metabolic alkalosis from unsuspected ingestion: Use of urine pH and
anion gap. Am J Kidney Dis. 59:577–581. 2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Scolari Childress KM and Myles T: Baking
soda pica associated with rhabdomyolysis and cardiomyopathy in
pregnancy. Obstet Gynecol. 122(2 Pt 2):495–497. 2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Lazebnik N, Iellin A and Michowitz M:
Spontaneous rupture of the normal stomach after sodium bicarbonate
ingestion. J Clin Gastroenterol. 8:454–456. 1986.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Linford SM and James HD: Sodium
bicarbonate abuse: A case report. Br J Psychiatry. 149:502–503.
1986.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Okada H, Inoue T, Takahira S, Sugahara S,
Nakamoto H and Suzuki H: Daytime hypertension, sleep apnea and
metabolic alkalosis in a haemodialysis patient-the result of sodium
bicarbonate abuse. Nephrol Dial Transplant. 14:452–454.
1999.PubMed/NCBI View Article : Google Scholar
|