Introduction
Diabetic foot is one of the most mutilating and
severe complications of diabetes, the prevalence of which is
gradually increasing over the past decade. The global prevalence of
diabetic foot ulcer in 2019 is estimated to be 463 million, which
is expected to rise to 578 million by 2030 (1,2). In
2015, the International Diabetes Federation estimated that diabetic
foot ulcers develop in 9.1-26.1 million individuals worldwide
annually (2). The prevalence of
both type 1 and type 2 diabetes is increasing, such that in 2019,
463 million adult individuals were afflicted with diabetes
worldwide (3). In addition,
diabetes is now becoming a increasingly common pathological
condition because the lifestyle of the world population is becoming
increasingly problematic (4).
Diabetes is known to be associated with obesity and a sedentary
lifestyle (5). The prevalence of
diabetes has increased dramatically over recent decades especially
in developing countries, reaching global pandemic proportions. The
International Diabetes Federation estimated that 451 million adults
live with diabetes worldwide in 2017, with a projected increase to
693 million by 2,045 if no effective prevention methods are adopted
(6). Age is the most important
factor influencing the prevalence of type 2 diabetes (7). However, the prevalence of type 2
diabetes is also increasing among young adults aged ≤20 years
(8). In the USA, estimates are as
high as 5,000 new cases every year (8). Type 2 diabetes is increasingly
diagnosed in young adults, which now accounts for 20-50% of all
patients with new-onset diabetes (8). The subsequent growth rate of the
incidence increases with age, which is typically more evident in
societies where the general prevalence of the disease is higher
(9).
It has been found that as the cardiovascular event
risk decreases, so does the risk of mortality (10). In a previous study conducted by
Pinto et al (11), patients
with type 2 diabetes mellitus and diabetic foot were predicted to
have worse prognoses in terms of faster progression of
cardiovascular damage and are at higher risks of cardiovascular
morbidity. This previous study also proposed that the main cause of
mortality in these patients was coronary artery disease (11). However, the average healing time of
diabetic foot ulcers without surgery is ~12 weeks, but it is
associated with an exceptionally high risk of amputation (12). The latest data regarding mortality
due to diabetic foot ulcers, according to the Veterans Health
Administration Population, reported that the 1-year survival rate
in patients with diabetic foot ulcer is 81%, 69% survive up to 2
years and only 29% survive up to 5 years (13,14).
Complications in the leg are among the most severe
and costly complications of diabetes (15). Amputation of the entire or part of
the leg is frequently caused by diabetic ulcers (16). A strategy for tackling this
includes preventative interventions, methods of educating both the
patient and the medical staff, multidisciplinary treatments of the
diabetic foot, such as pharmacological treatment, treatment of
oedema and malnutrition, local wound care and careful monitoring
(17). Altogether, they have been
reported to reduce the rate of amputations by 49-85% (17).
Neuropathy and ischemia are two of the main
etiological causes of diabetic foot, which together lead to
ulceration and Charcot neuroarthropathy (18). A triad of neuropathy, trauma with
secondary infection and peripheral arterial disease all account for
the pathophysiology of diabetic foot ulcer (19). Peripheral neuropathy produces
intrinsic muscle atrophy, leading to functional anatomical changes
in hammer toe formation and the development of ‘high-pressure’
zones on the plantar surface of the foot at the metatarsal heads
(19). By contrast, repetitive
trauma whilst walking, in association with decreased sensation and
proprioception, predisposes the skin to injury by producing atrophy
and dislocation of the protective plantar fat pads, leading to
ulceration and infection (19). In
association with the infection, it increases the risk of mortality
among the diabetic population, having an adverse impact both
clinically and economically (20).
Ischemia in the form of peripheral arterial disease provides an
important contribution to causing diabetic foot, which mainly
affects the lower limb, specifically the parts distal to the knee
joint (21). In patients with
diabetes, the risk of developing a diabetic foot ulcer is between
19 and 34% (18). However, relapse
is common after a healed episode. In total, typically ~40% of
patients experience recurrence of a diabetic ulcer within 1 year of
healing, ~60% within 3 years and 65% within 5 years (18,22).
Therefore, it is a common and highly severe complication given its
deforming nature, with an incidence of 3-4% among patients already
diagnosed with diabetes (23). In
addition to impairments in insulin signalling, environmental
factors, such as sedentary lifestyles or an unhealthy diet coupled
with genetic predispositions, have all been reported to be involved
in altering glucose homeostasis (24). Diabetic foot is also one of the
most expensive complications of diabetes. The burden it places on
medical services is enormous, with the overall cost estimated to be
~$1.3 trillion in 2015 worldwide (25). The latest studies in the UK
estimate an annual cost of >£1 billion ($1.32 billion) for
diabetic foot management alone, which is ~1% of the budget of the
National Health Service (25).
In particular, the association of diabetic foot with
various risk factors or comorbidities can accelerate its
deterioration. Therefore, the present study performed a
comprehensive analysis of the risk factors of patients with
diabetic foot injuries. The present study also assessed the risk of
a diabetic patient who has already developed diabetic foot injuries
requiring amputation. Therefore, the diabetologist or surgeon
treating the patient would have the opportunity to input the
patient's risk factors into a working model that can automatically
calculate the risk of amputation. The main objective of the present
study is to assess the impact of individual risk factors on
surgical treatment and the risk of amputation.
The present study starts from the hypothesis that a
system of classification, grading or description of foot injuries
in the practice of the clinician would facilitate the placement of
patients and interdisciplinary communication between diabetologists
and surgeons. The inclusion of a scoring system can provide an
estimated prognosis useful for optimizing the management protocol
of the appropriate treatment schemes. Numerous classification
schemes have been introduced over time, with the most well-known
being the Size (Area, Depth), Sepsis, Arteriopathy and Denervation
(SAD) system (26), which grades
the diabetic foot ulceration according to five ulcer features
(size, depth, sepsis, arteriopathy, and denervation) on a 4-point
scale (0-3). In addition, there is also the
Sanders-Eichenholtz-Rogers-Wagner (SERW) system (27), which describes the entire complex
of pathological changes in neuropathic diabetic foot and offer a
combination of classification. The SERW system is typically used to
describe the anatomical division of the foot, pathophysiological
stage of the process, clinical degree of deformation, the presence
and depth of the wound and the infection process (27). Other systems used include the
Meggitt-Wagner System (28) and
the Site, Ischemia, Neuropathy, Bacterial Infection, Area and Depth
system (29).
Patients and methods
Study design
The present retrospective, observational and
longitudinal cohort study was performed between 1st January 2018
and 31st December 2020. The present study included a group of 181
patients with diabetes from the first and second surgery wards in
the Sibiu County Emergency University Clinical Hospital (Sibiu,
Romania) and a group of 47 patients with diabetes from the
Proctoven Clinic (Sibiu, Romania). Therefore, the present study
included a total number of 228 patients.
All patients involved in the present study met the
main criterion for inclusion, which was the presence of lesions in
the sphere of the diabetic foot (ischemia, ulceration, gangrene,
neuropathy, callus and arteriopathy). All patients were between the
ages of 18 and 90 years, including both 178 males and 50 females.
In terms of pathology, all patients had either type I or II
diabetes with a diabetic foot complication. All patients who
underwent surgery for diabetic foot lesions by various methods,
such as amputation, necrectomy, debridement, disarticulation and
lower limb by-pass, were also included. Patients aged <18 or
>90 years, those with incomplete medical records and those
without diabetic foot lesions were excluded from the present study.
The present study followed international regulations under the
Declaration of Helsinki. The present study was approved by the
Ethics Committee of the Sibiu County Clinical Emergency University
Hospital (approval no. 5281; Sibiu, Romania) and the Ethics
Committee of the Proctoven Clinic Sibiu (approval no. 314; Sibiu,
Romania). Written informed consent for publication was obtained
from all the patients involved in the present study.
Analysis
Data collection and integration were performed based
on the medical records that were extracted from the database of the
Sibiu County Emergency University Clinical Hospital and Proctoven
Clinic in addition to the clinical observation sheets of each of
the patients hospitalized in both wards. Based on the collected
data, analysis was performed and a comparison of the cases was
represented in the tables and figures generated. These results were
then associated with the most up-to-date data from the
international literature on the complications of diabetes,
specifically the diabetic foot. Regarding the search strategy, to
associate data from the present study with those from the
internationally specialized literature, the following online
databases were used: PubMed (https://pubmed.ncbi.nlm.nih.gov); Elsevier (https://www.elsevier.com); Springer https://link.springer.com) and Research gate
(https://www.researchgate.net). In these
databases, the following search terms were used: ‘Diabetic foot
injuries’, ‘diabetic foot complications’, ‘surgical treatment of
diabetic foot complications’, ‘risk factors in diabetic foot
injuries’, ‘importance of risk factors in surgical treatment of
diabetic foot injuries’. Systematic reviews and meta-analyses on
the treatment of the diabetic foot, articles that analysed the
influence of risk factors in the diabetic foot and those that
analysed the complications of the diabetic foot were included.
Studies and articles that did not refer to the surgical treatment
of the diabetic foot, case reports and those that did not report
concrete conclusions were excluded. Regarding date restrictions,
for the most up-to-date information, articles and specialized
studies published online between 2015 and 2022 were searched.
Assessment methods
The following parameters were studied: Age, sex,
living environment, comorbidities, the presence or absence of risk
factors, their influence on the occurrence of lesions grouped under
the name of diabetic foot, type of diabetes, therapy applied, type
of surgery performed and their relationship with risk factors and
comorbidities.
Statistical methods
P<0.05 was considered to indicate a statistically
significant association or significant difference between
means/percentages. Following statistical analysis of the processed
data, the risk score was obtained using the following formula: X=(Y
x100)/Z, where X represents the amputation risk percentage, Y
represents patients who received amputation from the risk group and
Z represents the total number of patients in the risk group. This
formula was used in the Microsoft Excel 2016 program (Microsoft
Corporation) to calculate the risk score using Pearson's
χ2 test.
In addition, the binary logistic regression model
implemented in SPSS version 22 (IBM Corp.) was used for the
multidimensional evaluation of amputation risk factors.
Results
Baseline data
The present study was conducted over a period of
three years between 2018 and 2020, which included a total of 228
patients diagnosed with diabetes who had associated complications
in the area of the foot treated and hospitalized within the Sibiu
County Emergency University Clinical Hospital and Proctoven Clinic
(Sibiu, Romania).
After dividing the patients by age groups, a
predominance of the number of cases was observed in the 60-70 years
age group (n=103; 45%), followed by the 70-80 years age group
(n=66; 29%). In particular, patients aged between 60 and 80 years
represent >74% of the total cases included in the present study
group. In the 80-90 years age group, 20 patients (9%) were
identified whereas 32 cases (14%) belonged to the 50-60 years age
group. The fewest cases were observed in the 40-50 years (n=6;
2.6%) and 30-40 years (n=1; 0.4%) age groups (Table I). The statistical analysis
revealed significant differences between the percentages (P=0.0285,
Pearson's χ2 test).
 | Table IAnnual distribution of patients
diagnosed with diabetic foot according to demographic data
analysis. |
Table I
Annual distribution of patients
diagnosed with diabetic foot according to demographic data
analysis.
| | Year of study | |
|---|
| Parameter | 2018 | 2019 | 2020 | No. of cases | Percentage, % | P-value |
|---|
| Age group,
years | | | | | | |
|
30-40 | 0 | 0 | 1 | 1 | 0.4 | 0.0285 |
|
40-50 | 0 | 6 | 0 | 6 | 2.6 | |
|
50-60 | 18 | 9 | 5 | 32 | 14 | |
|
60-70 | 49 | 38 | 16 | 103 | 45 | |
|
70-80 | 39 | 14 | 13 | 66 | 29 | |
|
80-90 | 9 | 7 | 4 | 20 | 9 | |
| Sex | | | | | | |
|
Male | 86 | 53 | 39 | 178 | 78 | 0.0097 |
|
Female | 26 | 14 | 10 | 50 | 22 | |
| Living
environment | | | | | | |
|
Urban | 77 | 64 | 41 | 182 | 80 | 0.0091 |
|
Rural | 29 | 11 | 6 | 46 | 20 | |
| Type of
diabetes | | | | | | |
|
Type I | 18 | 9 | 3 | 30 | 13 | 0.0074 |
|
Type II | 83 | 61 | 54 | 198 | 87 | |
The patients included in the study group were also
divided into two groups according to their sex. Among all the
patients included in the study group, the diabetic foot was
predominantly more common among males (n=178; 78%) compared with
females (n=50; 22%) during the 3 years of study (P=0.0097,
Pearson's χ2 test; Table
I).
Regarding the distribution of patients according to
the living environment, among the 228 patients included in the
present study, 182 (80%) lived in an urban environment, whereas 46
(20%) patients came from the rural area (P=0.0091; Table I). This increased incidence of
cases in urban areas can be explained by the greater accessibility
and addressability to more specialized medical care but also by the
more developed medical knowledge, compared with patients from rural
areas. It has been observed that patients in rural areas in the
present study frequently approached the institutions already at
advanced stages of the underlying disease. Consequently, they
typically present with acute complications and require emergency
surgery because of the lack of easy access to specialized
consultations.
After grouping the patients according to the type of
diabetes, a predominance of type II diabetes was observed in close
association with the diabetic foot (n=198; 87%). Only 30 patients
(13%) in the study group were diagnosed with type I diabetes. In
addition, the prevalence of type II diabetes was observed in each
year of the study (P=0.0074, Pearson's χ2 test; Table I). In addition, there was a steady,
annual decrease in the number of patients admitted to the
institutions involved in the present study. This can be explained
by the Coronavirus pandemic and the low addressability of patients
to medical services during this period.
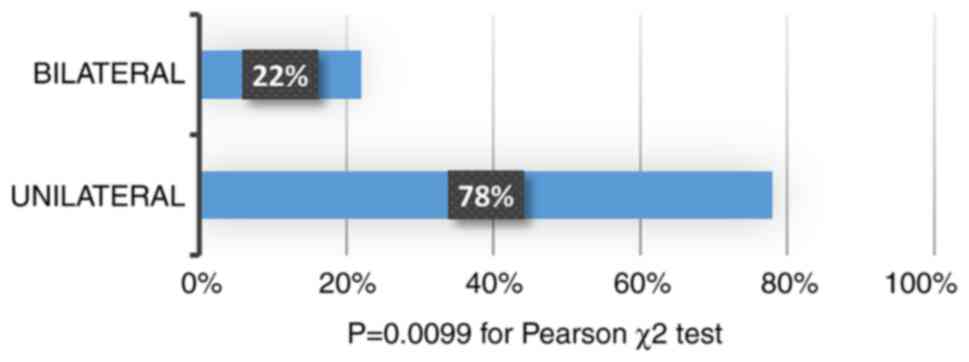
The diabetic foot can affect either one or both of
the lower limbs. Therefore, the present study also analysed the
prevalence of unilateral and bilateral lesions. Amongst the 228
patients included in the present study, 178 (78%) have one affected
limb, whereas 50 (22%) had both affected limbs (P=0.0099, Pearson's
χ2 test; Fig. 1).
Comorbidities
The following comorbidities were observed in the
patients included in the present study: i) High blood pressure; ii)
chronic ischemic heart disease; iii) heart failure; iv) chronic
kidney failure; v) chronic venous insufficiency; vi)
macroangiopathy in chronic obliterative arteriopathy; vii) stroke;
viii) chronic obstructive pulmonary disease; ix) hepatitis; and x)
neoplasia (Fig. 2)
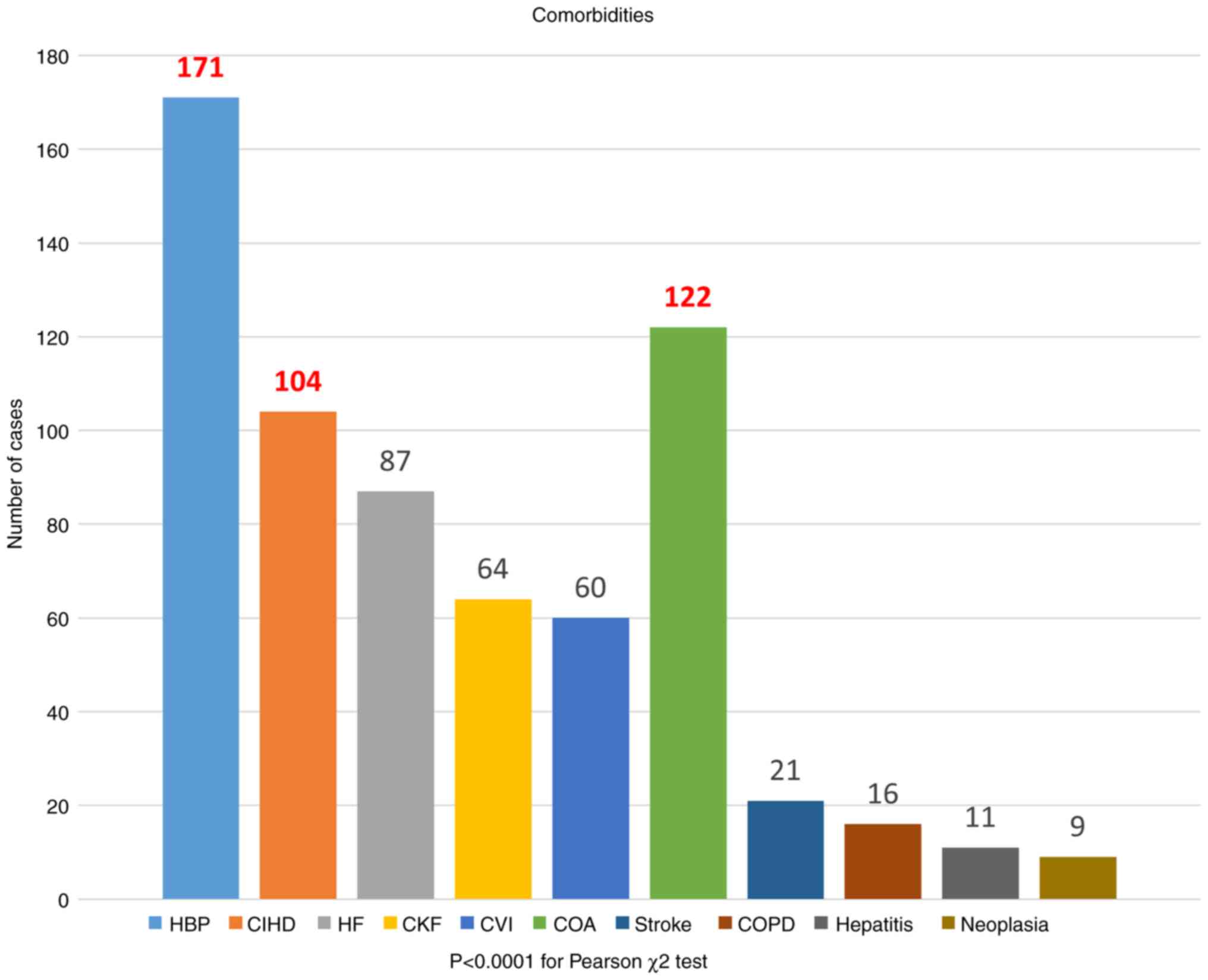 | Figure 2Distribution of the number of
patients according to the identified comorbidities. On the X-axis,
the comorbidities analyzed in the study are illustrated, whereas on
the Y-axis, the number of cases associated with the studied
comorbidities is highlighted. The most frequent comorbidities were
HBP, COA and CIHD. HBP, high blood pressure; CIHD, chronic ishemic
heart disease; HF, heart failure; CKF, chronic kidney failure; CVI,
chronic venous insufficiency; COA, chronic obliterative
arteriopathy; COPD, chronic obstructive pulmonary disease. |
Following the analysis of comorbidities associated
with diabetic foot, high blood pressure was observed in 171 cases
(75.13%), followed by arteriopathy [122 (53.5%)] and chronic
ischemic heart disease [104 (45.8%)], whereas heart failure was
present in 87 (38.1%) patients. Chronic kidney failure and chronic
venous insufficiency were present in 64 (28.17%) and 60 (26.5%)
patients, respectively. Other pathologies, such as hepatitis,
neoplasia, stroke and chronic obstructive pulmonary disease, have
also been identified, but with relatively smaller percentages
(<10%) compared with the others. The results were found to be
statistically significant (P<0.0001, Pearson's χ2
test; Fig. 2).
Risk factors
The risk factors identified in the patients included
in the present study were subsequently analysed. These included
smoking, obesity, dyslipidaemia, duration of diabetes >5 years,
hepatic steatosis, various pre-existing heart conditions and
unbalanced diabetes [glycated haemoglobin (HbA1c) >7.5%;
Table II)].
| Table IIDistribution of patients according to
associated risk factors. |
Table II
Distribution of patients according to
associated risk factors.
| Risk factors | No. of cases | Percentage, % |
P-valuea |
|---|
| Smoking | 16 | 7.1 | <0.001 |
| Obesity | 127 | 55.8 | |
| Pre-existing heart
conditions | 190 | 83.4 | |
| Dyslipidaemia | 112 | 49.1 | |
| Duration of
diabetes >5 years | 92 | 40.3 | |
| Hepatic
steatosis | 30 | 13.2 | |
| Glycated | 83 | 36.4 | |
| haemoglobin
>7,5% | | | |
Following the analysis of the risk factors
associated with diabetic foot, the prevalence of pre-existing
cardiac pathologies was 83.4%, whilst the prevalence for obesity
and dyslipidaemia was 55.8 and 49.1%, respectively. The prevalence
of diabetes with a duration >5 years was 40.3%, whereas 36.4% of
patients had unbalanced diabetes (HbA1c >7.5%). The risk factors
with the lowest cases were hepatic steatosis and smoking, with a
share of 13.2 and 7.1% of the studied group, respectively. The
results were found to be statistically significant (P<0.001,
Pearson's χ2 test; Table
II).
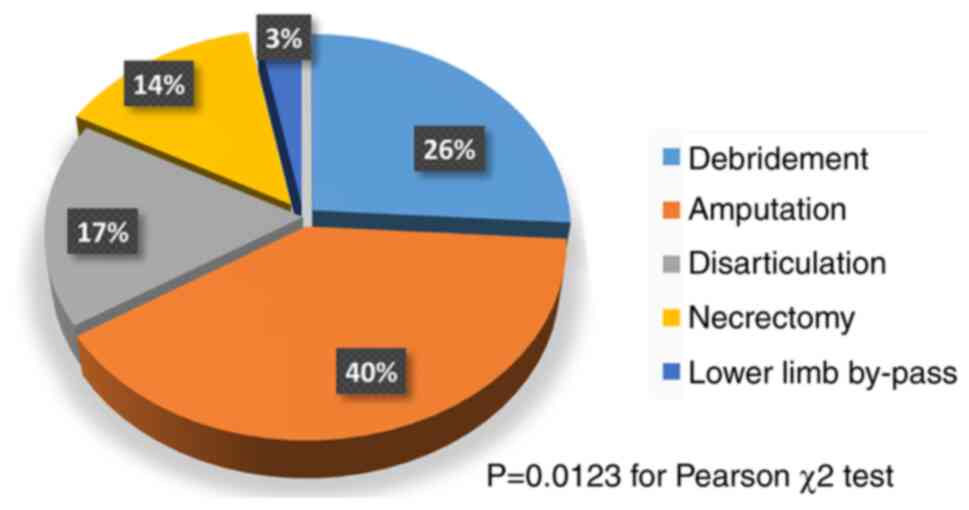
Type of surgery
During the present study, analysis of the type of
surgery performed was then performed. Therefore, for the 3-year
study period, five types of classical types of surgeries were
performed, namely debridement, amputation, disarticulation, lower
limb bypass and necrectomy. Following analysis of the
interventions, it was observed that amputation and debridement
represented 40 and 26% of all cases, respectively. These were
followed by disarticulation and necrectomy, with 17 with 14%
prevalence, respectively. The least common intervention was
represented by the bypass of the lower limb, with a prevalence of
3%. The statistical analysis revealed significant differences among
the interventions (P=0.0123, Pearson χ2 test; Fig. 3).
The types of amputations performed in the two
institutions in the present study were also analysed. Finger
amputation was performed in 26 patients (29%), followed by
amputation above the knee in 24 cases (26%) and amputation below
the knee in 17 cases (18%). Transmetatarsal and mediotarsal
amputations were performed in 14 (15%) and 11 (12%) patients,
respectively (P=0.0413, Pearson's χ2 test; Table III).
| Table IIIDistribution of patients according to
the type of amputation. |
Table III
Distribution of patients according to
the type of amputation.
| Amputation | No. of cases | Percentage, % |
P-valuea |
|---|
| Finger | 26 | 29 | 0.0413 |
| Below the knee | 17 | 18 | |
| Above the knee | 24 | 26 | |
| Mediotarsal | 11 | 12 | |
|
Transmetatarsal | 14 | 15 | |
| Total | 92 | 100 | |
Association analysis
Taking into account that risk factors and
comorbidities serve a major role in the evolution of diabetes and
indirectly of the diabetic foot, the association between surgeries
and the risk factors/comorbidities were studied. The risk factors
analysed were the following: i) Smoking; ii) obesity; iii) heart
disease; iv) dyslipidaemia; v) duration of diabetes >5 years;
vi) hepatic steatosis; and vii) HbA1c >7.5% (Table IV).
| Table IVDistribution of surgical
interventions in relation to risk factors. |
Table IV
Distribution of surgical
interventions in relation to risk factors.
| | Surgical
interventions | |
|---|
| Risk factors | Debridement | Amputation |
Disarticulation | Necrectomy | By-pass | Total, N |
|---|
| Smoking | 0 | 8 | 0 | 4 | 4 | 16 |
| Obesity | 4 | 74 | 18 | 23 | 8 | 127 |
| Pre-existing heart
conditions | 41 | 84 | 31 | 18 | 16 | 190 |
| Dyslipidaemia | 7 | 58 | 8 | 32 | 7 | 112 |
| Duration of
diabetes >5 years | 16 | 39 | 9 | 23 | 5 | 92 |
| Hepatic
steatosis | 10 | 12 | 2 | 6 | 0 | 30 |
| HbA1c >7.5% | 15 | 29 | 9 | 20 | 10 | 83 |
|
P-valuea | <0.001 | 0.0257 | 0.0123 | 0.001 | 0.0439 | - |
In the present study, amputation was the most common
surgical intervention in patients with the aforementioned risk
factors, followed by necrectomy, debridement, disarticulation and
by-pass. There was also an increased prevalence of heart disease
among all patients who underwent surgery, followed by obesity and
dyslipidaemia. Amputation (P=0.0257, Pearson's χ2 test)
and necrectomy (P=0.001, Pearson's χ2 test) were
observed more frequently in patients with HbA1c >7.5%, in those
with a duration of diabetes >5 years and those with
dyslipidaemia. Surgical debridement was more associated with
patients with heart disease and duration of diabetes >5 years,
HbA1c >7.5% and hepatic steatosis (P<0.001, Pearson's
χ2 test). The incidence of disarticulation (P=0.0123,
Pearson's χ2 test) and bypass (P=0.0439, Pearson's
χ2 test)was most common in cases of heart disease,
obesity and diabetics with HbA1c >7.5% (Table IV).
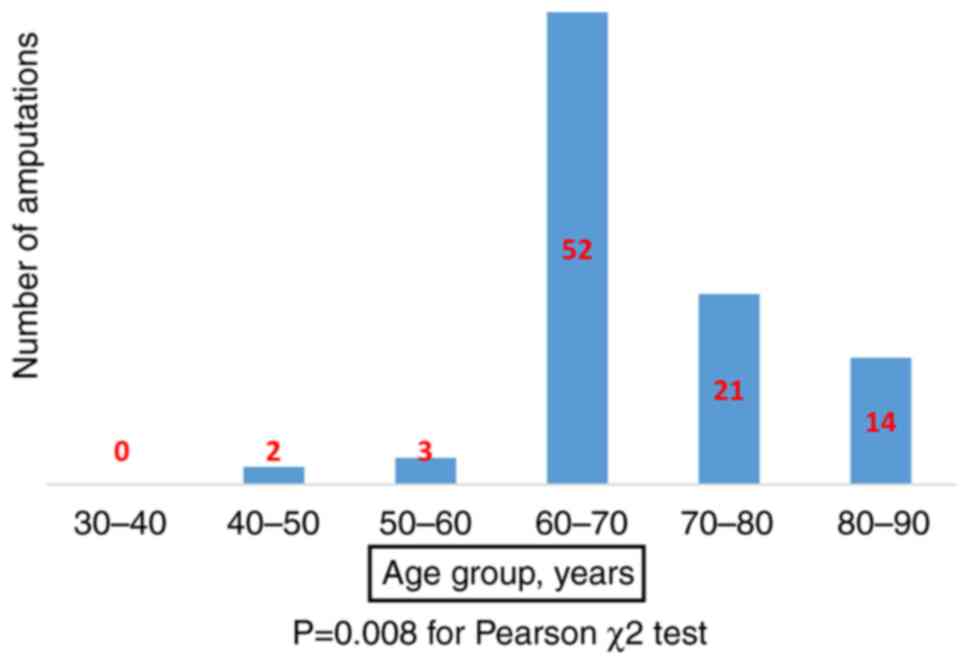
Age-related amputation analysis was particularly
beneficial for analysing assess the most affected age groups. The
same age groups as aforementioned in the demographic data were used
for analysis. This analysis was performed on the 92 patients in the
study group who underwent amputation surgery. The majority of the
amputations were performed in the 60-70 years age group with 52
cases (56.5%), followed by the 70-80 years age group with 21 cases
(22.8%). By contrast, 14 amputations (15.2%) were performed in the
80-90 years age group. Amputations were less common in the 50-60
and 40-50 years age groups with three (3.3%) and two cases (2.2%),
respectively (P=0.008, Pearson's χ2 test; Fig. 4).
Risk score analysis
The risk score system constructed in the present
study was designed for patients with diabetes who already developed
diabetic foot-specific lesions to assess their risk of amputation
due to the associated risk factors (Table IV). To achieve this score on the
risk of amputation in patients with diabetes, the risk factors that
were analysed and presented in the study were incorporated. They
are represented by the following: i) Smoking, 16 cases (7.1%); ii)
obesity, 127 cases (55.8%); iii) pre-existing heart conditions, 190
cases (83.4%); iv) dyslipidaemia, 112 cases (49.1%); v) duration of
diabetes >5 years, 92 cases (40.3%); vi) hepatic steatosis, 30
cases (13.2%); and vii) HbA1c >7.5%, 83 cases (36.4%). To create
the model for calculating the risk score based on the seven risk
factors and the data obtained from the 228 patients with diabetes
who developed specific lesions of the diabetic foot, the patients
were divided into four risk stratification groups as follows: i)
Group A, patients who have zero or one risk factor; ii) group B,
patients who have two or three risk factors; iii) group C, patients
who have four or five risk factors; and v) group D, patients who
have > five risk factors (Table
V).
| Table VRisk factor stratification for
amputation. |
Table V
Risk factor stratification for
amputation.
| Risk group | No. of risk
factors | No. of
patients | Patients who
received amputation | Risk of amputation,
% |
P-valuea |
|---|
| A | 0-1 | 121 | 15 | 12.40 | <0.001 |
| B | 2-3 | 76 | 51 | 67.11 | |
| C | 4-5 | 21 | 18 | 85.71 | |
| D | >5 | 10 | 8 | 90.00 | |
The present study revealed that the risk of
amputation among patients who have at most one risk factor was low
at 12.2% (Table V). By contrast,
the simultaneous presence of two or three risk factors in the same
patient increased the risk of amputation to 67.11%. The risk of
amputation was 85.71% in patients in group C with four or five risk
factors whilst the highest risk was shown in patients with >
five risk factors, with a risk of amputation of 90%. It can
therefore be concluded that the simultaneous presence of a greater
number of risk factors in the same patient is directly proportional
to the increase in the risk of amputation.
All data collected were used to construct the risk
score system. Therefore, to calculate it, a database with the
patients in the present study and the risk factors they presented
was constructed according to the model shown in Table SI.
Table SI contains
all patients included in the study group along with the risk
factors identified for each patient, their total number of risk
factors and the risk group they are assigned to. In addition, the
last column mentions patients who have had underwent amputation
(Yes/No). For columns two to eight, which correspond to each of the
risk factors, the following applies: 1=true and 0=false. Therefore,
patients who presented with one of the risk factors studied were
marked with ‘1’, whereas those without risk factors were marked
with ‘0’. Table SI continues up
to patient 228.
Statistical analysis
All data collected were extracted from clinical
observation sheets and surgical protocols. These data were also
analysed and entered into a table using Microsoft Office Excel 2016
(Microsoft Corporation). An additional column was then inserted,
representing the risk group for amputation in percentages, based on
the number of risk factors present on each patient. A statistically
significant association between the risk groups and amputation was
found (P<0.001, Pearson's χ2 test; Table V). The risk of amputation is found
to be 12.4% in cases with up to one risk factor, which increased up
to 85.71-90% in cases that have ≥ four risk factors. Based on the
number of risk factors encountered in any single patient which,
combined with the statistical analysis results previously performed
on the database used in the present study, the clinician may use
this system to automatically generate an estimation of the risk of
amputation. This may serve to be a beneficial tool for planning the
individualized therapeutic strategy (Table VI). In order to be able to use
this functionality, Table SII is
available as an additional Excel file.
| Table VICalculating the risk score using
Microsoft Excel 2016. |
Table VI
Calculating the risk score using
Microsoft Excel 2016.
| | Risk Factors | |
|---|
| Patient No. | Smoking | Obesity | Heart
conditions | Dyslipidaemia | Durati on of
diabetes >5 years | Hepatic
steatosis | Glycated
haemoglobin >7,5% | Total Risk
factors | Risk group | Risk of amputation,
% |
|---|
| 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 6 | D | 87.5 |
Logistic regression approach
The present study didn't demonstrate if all analysed
risk factors can significantly increase the amputation risk. The
binary logistic regression model was implemented with the dependent
variable of amputation (1=true or 0=false) and the following
independent variables: i) HbA1c >7.5%; ii) duration of diabetes
>5 years; iii) smoking; iv) hepatic steatosis; v) obesity; vi)
dyslipidaemia; and vii) pre-existing heart conditions (Table VII). The minimal value of the
confidence interval for each OR is >1, except for ‘duration of
diabetes >5 years’ (Table
VII). For ‘duration of diabetes >5 years’, B was found to be
0.923 with 95% CI of -0.16-2.01 and an OR=e0.923=2.52
and CI: (e- 0.16 - e2.01)=(0.85-7.44).
Therefore, OR>1 but the left side of 95% CI is 0.85<1 (i.e.
the risk of OR <1 is >5%). This meant that each risk factor
listed in Table VII adds a
95%-significant extra hazard, except for ‘duration of diabetes
>5 years’ (which adds only a 90%-significant extra hazard).
Using the Logistic regression model from Table VII, the probability of amputation
for patient ‘k’ can be computed using the following function
formula:
| Table VIILogistic regression model for the
dependent variable of amputationb. |
Table VII
Logistic regression model for the
dependent variable of amputationb.
| | | | | | | | 95% CI for OD |
|---|
| Risk | Estimated
co-efficient | Standard error | Wald | Degrees of
freedom | P-value | OR | Lower | Upper |
|---|
| HbA1c >7.5% | 2.001 | 0.614 | 10.611 | 1 | 0.001 | 7.393 | 2.219 | 24.638 |
| Dyslipidaemia | 0.988 | 0.468 | 4.465 | 1 | 0.035 | 2.687 | 1.074 | 6.721 |
| Duration of
diabetes >5 yearsa | 0.923 | 0.553 | 2.787 | 1 | 0.095a | 2.517 | 0.852a | 7.441 |
| Smoking | 2.983 | 0.807 | 13.656 | 1 | 0.000 | 19.740 | 4.058 | 96.026 |
| Obesity | 1.658 | 0.533 | 9.676 | 1 | 0.002 | 5.250 | 1.847 | 14.924 |
| Pre-existing heart
conditions | 1.890 | 0.516 | 13.387 | 1 | 0.000 | 6.616 | 2.405 | 18.206 |
| Hepatic
steatosis | 2.577 | 0.702 | 13.458 | 1 | 0.000 | 13.156 | 3.321 | 52.123 |
| Constant | -3.750 | 0.552 | 46.153 | 1 | 0.000 | 0.024 | | |
In this formula, k represents a patient,
B0 and Bi are estimated co-efficients of the
logistic regression model and i is the index for risks. The sum is
computed for all risks, where xik is the value of risk i
for patient k (in this present case, xik is 1 or 0
depending on presence/absence of risk i) and exp(z)=ez
is the natural exponential function. Subsequently, knowing the risk
values for a new patient, the probability of Eventk=1
can be computed. In the present case, the prediction would yield
Amputation=yes if prob(Eventk=1) >0.5 or
Amputation=no if prob(Eventk=1) <0.5. Therefore,
except for the duration of diabetes >5 years, each risk factor
listed in Table VII added an
extra hazard, whether or not these risk factors are statistically
associated.
Discussion
Diabetes rarely presents a ‘one-size-fits-all’
pathology. Patients with diabetes frequently present with a unique
but diverse series of comorbidities and complications (30). They can also present numerous risk
factors for the occurrence of diabetic foot lesions, which may
accumulate over time due to an inappropriate lifestyle (31). As a result, comorbidities that can
accelerate progression to diabetic foot have to be identified and
analysed, since they can serve a significant role in increasing the
risk of patient mortality (32).
The majority of the patients investigated in the
present study had ≥ one associated comorbidities. Several studies
had previously shown that comorbidities associated with diabetes
increase the demand for medical care, cost of hospitalization and
frequency of medical follow-ups (33,34).
Therefore, a deeper understanding of the comorbidities and
associated factors may improve the management of patients with
diabetes and the selection of individualized treatment protocols
(33,34).
The occurrence of diabetic foot injuries is
dependent on a number of risk factors, especially those related to
the lifestyle (35). Although the
number of smoking patients identified in the present study was
small, there is a close association between smoking and diabetic
foot. Smoking is an important risk factor in the development of
peripheral vascular disease in patients with diabetes. In addition,
it was found to exacerbate the risk of peripheral neuropathy by
12-fold compared with that in non-smokers (36,37).
Dyslipidaemia also serves an important role in the
progression of vascular complications caused by diabetes. A recent
study indicated a high prevalence of dyslipidaemia among patients
with diabetes (38). Sex,
advancing age, long duration of diabetes, increased body-mass index
(BMI) and high blood pressure were risk factors associated with the
prevalence of dyslipidaemia (39).
In addition, dyslipidaemia has been previously considered to be an
independent predictor of the development of cardiovascular diseases
(40,41). In the present study, a close
association between obesity (translated into high BMI) and diabetic
foot was found, which was consistent with findings from specialized
studies (42,43). It has also been previously
concluded that obesity is a major risk factor for the development
and progression of macrovascular complications of diabetes, such as
coronary heart disease, peripheral arterial disease and
hypertension (44,45).
The duration of diabetes is a major contributing
factor to the increased incidence of diabetic foot disorders
(46). In the present study, 92
patients with a duration of diabetes >5 years were identified.
In particular, diabetic foot disorders are common among patients
with diabetes even during the early stages of diabetes or when they
are first diagnosed (47).
Although the duration of diabetes is not a modifiable risk factor,
it is of great importance for the early identification and
management of diabetic foot, as previously stated by Fawzy et
al (48) and Alzahrani et
al (49).
In the present study, it was highly important to
identify patients with unbalanced diabetes because longer exposure
to high HbA1c levels is associated with complications in patients
with diabetes (50). In total, 83
patients had HbA1c>7.5%. Poor glycaemic control is strongly
associated with the development of diabetic foot over time
(50). Although the prevalence of
unbalanced diabetes was only 36.4% in the present study, previous
studies by Fawzy et al (48) and Abdissa and Hirpa (41), show a much higher frequency among
patients with diabetic feet, at 89 and 63.8%, respectively. These
same studies showed that high levels of HbA1c can contribute to the
development of the diabetic foot. This may be due to
hyperglycaemia, which is considered a risk factor for diabetic foot
due to its contribution to the development of peripheral neuropathy
and microvascular complications (49,51).
Another risk factor identified in the present study
is hepatic steatosis, which was found in 30 patients. Previous
studies mentioned the existence of a bidirectional relationship
between hepatic steatosis and type 2 diabetes, given the vital role
of the liver in the pathophysiology of both conditions (52). This in turn leads to the
development of insulin resistance and aggravation of hepatic
steatosis and type 2 diabetes (52). The presence of hepatic steatosis
increases the likelihood of complications of type 2 diabetes, which
likely explains the increased screening rates for this disease in
patients with type 2 diabetes (52,53).
Several studies previously indicated that hepatic steatosis is
closely associated with an increased risk of chronic vascular
complications of diabetes (54-56).
In addition, other studies on patients with type 2 diabetes found
that the prevalence of vascular disease is higher in patients with
hepatic steatosis compared with that among healthy individuals
(52,53).
Treatment of diabetic foot ulcers is complex and
typically involves both conventional and innovative methods, such
as antibiotic therapy, wound dressing, negative pressure therapy,
necrotic tissue debridement, hyperbaric oxygen therapy, stem cell
therapy, growth factor therapy and maggot therapy, all to prevent
amputation (57,58). However, the use of any of the
aforementioned methods alone may not be effective in preventing
pain and/or mechanical damage in the healthy underlying tissues. In
the majority of cases, it may be advisable to combine different
therapeutic strategies according to the particularities of the
patient and the therapeutic possibilities available (57-59).
Early recognition and management of risk factors
associated with the diabetic foot can influence the decision on the
type of surgery but also the subsequent outcome for patients,
thereby preventing major debilitating amputations (60-63).
Diabetic foot ulcers remain to be a major public health issue,
being one of the most debilitating chronic complications of
diabetes, the prevalence of which has been increasing exponentially
globally (20,64). In addition, the annual decrease in
the number of cases admitted to our service can be at least
partially explained by the Coronavirus pandemic, which led to a
decrease in the addressability of patients to medical services
during this period.
The most affected age group found in the present
study was the 60-70 years age, followed by the 70-80 years age
group. Therefore, age was considered to be an important aggravating
factor in the evolution of diabetic foot, which could be seen in
the present study, since the majority of amputations were performed
in the 60-70 age group.
Risk factors serve an important role in the
occurrence of diabetic foot injuries. The results of the present
study, in terms of risk factors, were in agreement with the
literature and previous studies (6,65-67).
The identification of risk factors and types of treatment, in
addition to their analysis, allowed the development of the risk
score. The novelty of the present findings consists of the
establishment of a risk score system that enables clinicians to
have, from the time of admission, a perspective on the prospective
outcome and complications to guide the designation of personalized
treatment methods for patients with diabetic foot injuries. This
risk score system enables the early identification of patients with
diabetes who have developed diabetic foot injuries and are at high
risk of amputation, allowing them to take preventive measures. A
limitation of the present study is that this risk score system has
not been tested on another independent patient cohort. Patients
with diabetes should pursue a self-care education, since successful
control of the disease depends to a large extent on the application
of this behaviour throughout the life of the patients. In the
future, the study will be expanded to other medical facilities to
increase the size of the cohort.
Supplementary Material
Database with all the patiens included
in the study along with the risk factors identified.
Calculating the risc score using
Microsoft Excel 2016
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Ministry of
Research, Innovation and Digitalization Romania through the funding
scheme PC-101-2021 of Lucian Blaga University of Sibiu (Sibiu,
Romania) aiming at supporting excellence in research (grant no. 28
PFE; 30 December 2021).
Availability of the data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CT, AM and DT contributed substantially to the
conception and design of the study, the acquisition, analysis and
interpretation of the data. DS, CG, RF and CB contributed
substantially to the analysis and interpretation of the data. CT,
CM, AM and CB contributed substantially to the interpretation of
the data and were involved in the critical revisions of the
manuscript for important intellectual content. CB, CM and CT
confirm the authenticity of all the raw data. All authors agreed to
be accountable for all aspects of the work in ensuring that
questions related to the accuracy or integrity of any part of the
work are appropriately investigated and resolved. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
The present study followed international regulations
under the Declaration of Helsinki. The present study was approved
by the Ethics Committee of the Sibiu County Clinical Emergency
University Hospital (approval no. 5281; Sibiu, Romania) and the
Ethics Committee of the Proctoven Clinic Sibiu (approval no. 314;
Sibiu, Romania). Written patient informed consent for publication
of the data associated with the manuscript was obtained.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Armstrong DG, Boulton AJM and Bus SA:
Diabetic foot ulcers and their recurrence. N Engl J Med.
376:2367–2375. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Saeedi P, Petersohn I, Salpea P, Malanda
B, Karuranga S, Unwin N, Colagiuri S, Guariguata L, Motala AA,
Ogurtsova K, et al: Global and regional diabetes prevalence
estimates for 2019 and projections for 2030 and 2045: Results from
the International diabetes federation diabetes atlas, 9th edition.
Diabetes Res Clin Pract. 157(107843)2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Adem AM, Andargie AA, Teshale AB and Wolde
HF: Incidence of diabetic foot ulcer and its predictors among
diabetes mellitus patients at felege hiwot referral hospital, Bahir
Dar, Northwest Ethiopia: A retrospective follow-up study. Diabetes
Metab Syndr Obes. 13:3703–3711. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Galaviz KI, Narayan KMV, Lobelo F and
Weber MB: Lifestyle and the prevention of type 2 diabetes: A Status
Report. Am J Lifestyle Med. 12:4–20. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Park JH, Moon JH, Kim HJ, Kong MH and Oh
YH: Sedentary lifestyle: Overview of updated evidence of potential
health risks. Korean J Fam Med. 41:365–373. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Cho NH, Shaw JE, Karuranga S, Huang Y, da
Rocha Fernandes JD, Ohlrogge AW and Malanda B: IDF diabetes atlas:
Global estimates of diabetes prevalence for 2017 and projections
for 2045. Diabetes Res Clin Pract. 138:271–281. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Selvin E and Parrinello CM: Age-related
differences in glycaemic control in diabetes. Diabetologia.
56:2549–2551. 2013.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Nadeau KJ, Anderson BJ, Berg EG, Chiang
JL, Chou H, Copeland KC, Hannon TS, Huang TT, Lynch JL, Powell J,
et al: Youth-Onset type 2 diabetes consensus report: Current
status, challenges, and priorities. Diabetes Care. 39:1635–1642.
2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Sinnott SJ, McHugh S, Whelton H, Layte R,
Barron S and Kearney PM: Estimating the prevalence and incidence of
type 2 diabetes using population level pharmacy claims data: A
cross-sectional study. BMJ Open Diabetes Res Care.
5(e000288)2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Rubio JA, Jiménez S and Lázaro-Martínez
JL: Mortality in patients with diabetic foot ulcers: Causes, risk
factors, and their association with evolution and severity of
ulcer. J Clin Med. 9(3009)2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Pinto A, Tuttolomondo A, Di Raimondo D,
Fernandez P, La Placa S, Di Gati M and Licata G: Cardiovascular
risk profile and morbidity in subjects affected by type 2 diabetes
mellitus with and without diabetic foot. Metabolism. 57:676–682.
2005.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Bekele F and Chelkeba L: Amputation rate
of diabetic foot ulcer and associated factors in diabetes mellitus
patients admitted to Nekemte referral hospital, Western Ethiopia:
Prospective observational study. J Foot Ankle Res.
13(65)2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Brennan MB, Hess TM, Bartle B, Cooper JM,
Kang J, Huang ES, Smith M, Sohn MW and Crnich C: Diabetic foot
ulcer severity predicts mortality among veterans with type 2
diabetes. J Diabetes Complications. 31:556–561. 2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Killeen AL, Brock KM, Dancho JF and
Walters JL: Remote temperature monitoring in patients with visual
impairment due to diabetes mellitus: A proposed improvement to
current standard of care for prevention of diabetic foot ulcers. J
Diabetes Sci Technol. 14:37–45. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Everett E and Mathioudakis N: Update on
management of diabetic foot ulcers. Ann N Y Acad Sci. 1411:153–165.
2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Pemayun TG, Naibaho RM, Novitasari D, Amin
N and Minuljo TT: Risk factors for lower extremity amputation in
patients with diabetic foot ulcers: A hospital-based case-control
study. Diabet Foot Ankle. 6(29629)2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Bakker K, Apelqvist J and Schaper NC:
International working group on diabetic foot editorial board.
Practical guidelines on the management and prevention of the
diabetic foot 2011. Diabetes Metab Res Rev. 28 (Suppl 1):S225–S231.
2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Edmonds M, Manu C and Vas P: The current
burden of diabetic foot disease. J Clin Orthop Trauma. 17:88–93.
2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Bandyk DF: The diabetic foot:
Pathophysiology, evaluation, and treatment. Semin Vasc Surg.
31:43–48. 2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Jeyaraman K, Berhane T, Hamilton M,
Chandra AP and Falhammar H: Mortality in patients with diabetic
foot ulcer: A retrospective study of 513 cases from a single Centre
in the Northern Territory of Australia. BMC Endocr Disord.
19(1)2019.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Boyko EJ, Monteiro-Soares M and Wheeler
SGB: Peripheral arterial disease, foot ulcers, lower extremity
amputations, and diabetes. In: Diabetes in America. Cowie CC,
Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg
EW, Knowler WC, Barrett-Connor E, Becker DJ, et al (eds).
3rd edition. National Institute of Diabetes and Digestive and
Kidney Diseases (US), Bethesda, MD, 2018.
|
|
22
|
Andrade C: The P value and statistical
significance: Misunderstandings, explanations, challenges, and
alternatives. Indian J Psychol Med. 41:210–215. 2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Yazdanpanah L, Shahbazian H, Nazari I,
Arti HR, Ahmadi F, Mohammadianinejad SE, Cheraghian B and Hesam S:
Incidence and risk factors of diabetic foot ulcer: A
population-based diabetic foot cohort (ADFC Study)-two-year
follow-up study. Int J Endocrinol. 2018(7631659)2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
DeFronzo RA, Ferrannini E, Groop L, Henry
RR, Herman WH, Holst JJ, Hu FB, Kahn CR, Raz I, Shulman GI, et al:
Type 2 diabetes mellitus. Nat Rev Dis Primers.
1(15019)2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Jeffcoate WJ, Vileikyte L, Boyko EJ,
Armstrong DG and Boulton AJM: Current challenges and opportunities
in the prevention and management of diabetic foot ulcers. Diabetes
Care. 41:645–652. 2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Treece KA, Macfarlane RM, Pound N, Game FL
and Jeffcoate WJ: Validation of a system of foot ulcer
classification in diabetes mellitus. Diabet Med. 21:987–991.
2004.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Obolenskiy VN, Protsko VG and Komelyagina
LY: Classification of diabetic foot, revisited. Wound Med. 18:1–7.
2017.
|
|
28
|
Oyibo SO, Jude EB, Tarawneh I, Nguyen HC,
Harkless LB and Boulton AJ: A comparison of two diabetic foot ulcer
classification systems: The Wagner and the University of Texas
wound classification systems. Diabetes Care. 24:84–88.
2001.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Ince P, Abbas ZG, Lutale JK, Basit A, Ali
SM, Chohan F, Morbach S, Möllenberg J, Game FL and Jeffcoate WJ:
Use of the SINBAD classification system and score in comparing
outcome of foot ulcer management on three continents. Diabetes
Care. 31:964–967. 2008.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Cho YY and Cho SI: Treatment variation
related to comorbidity and complications in type 2 diabetes: A real
world analysis. Medicine (Baltimore). 97(e12435)2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Al-Rubeaan K, Al Derwish M, Ouizi S,
Youssef AM, Subhani SN, Ibrahim HM and Alamri BN: Diabetic foot
complications and their risk factors from a large retrospective
cohort study. PLoS One. 10(e0124446)2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Jodheea-Jutton A, Hindocha S and
Bhaw-Luximon A: Health economics of diabetic foot ulcer and recent
trends to accelerate treatment. Foot (Edinb).
52(101909)2022.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Piette JD and Kerr EA: The impact of
comorbid chronic conditions on diabetes care. Diabetes Care.
29:725–731. 2006.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Huang ES: Management of diabetes mellitus
in older people with comorbidities. BMJ. 353(i2200)2016.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Adeyemi TM, Olatunji TL, Adetunji AE and
Rehal S: Knowledge, practice and attitude towards foot ulcers and
foot care among adults living with diabetes in Tobago: A
qualitative study. Int J Environ Res Public Health.
18(8021)2021.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Mantey I, Foster AV, Spencer S and Edmonds
ME: Why do foot ulcers recur in diabetic patients? Diabet Med.
16:245–249. 1999.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Xia N, Morteza A, Yang F, Cao H and Wang
A: Review of the role of cigarette smoking in diabetic foot. J
Diabetes Investig. 10:202–215. 2019.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Pitso L, Mofokeng TRP and Nel R:
Dyslipidaemia pattern and prevalence among type 2 diabetes mellitus
patients on lipid-lowering therapy at a tertiary hospital in
Central South Africa. BMC Endocr Disord. 21(159)2021.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Alzaheb RA and Altemani AH: Prevalence and
associated factors of dyslipidemia among adults with type 2
diabetes mellitus in Saudi Arabia. Diabetes Metab Syndr Obes.
13:4033–4040. 2020.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Bekele S, Yohannes T and Mohammed AE:
Dyslipidemia and associated factors among diabetic patients
attending Durame General Hospital in Southern Nations,
Nationalities, and People's Region. Diabetes Metab Syndr Obes.
10:265–271. 2017.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Abdissa D and Hirpa D: Dyslipidemia and
its associated factors among adult diabetes outpatients in West
Shewa zone public hospitals, Ethiopia. BMC Cardiovasc Disord.
22(39)2022.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Sohn MW, Budiman-Mak E, Lee TA, Oh E and
Stuck RM: Significant J-shaped association between body mass index
(BMI) and diabetic foot ulcers. Diabetes Metab Res Rev. 27:402–409.
2011.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Zantour B, Bouchareb S, El Ati Z, Boubaker
F, Alaya W, Kossomtini W and Sfar MH: Risk assessment for foot
ulcers among Tunisian subjects with diabetes: A cross sectional
outpatient study. BMC Endocr Disord. 20(128)2020.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Rizk MN and Ameen AI: Comorbidities
associated with Egyptian diabetic foot disease subtypes. Egypt J
Intern Med. 25:154–158. 2013.
|
|
45
|
Galal YS, Khairy WA, Taha AA and Amin TT:
Predictors of foot ulcers among diabetic patients at a tertiary
care center, Egypt. Risk Manag Healthc Policy. 14:3817–3827.
2021.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Almobarak AO, Awadalla H, Osman M and
Ahmed MH: Prevalence of diabetic foot ulceration and associated
risk factors: An old and still major public health problem in
Khartoum, Sudan? Ann Transl Med. 5(340)2017.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Ming A, Walter I, Alhajjar A, Leuckert M
and Mertens PR: Study protocol for a randomized controlled trial to
test for preventive effects of diabetic foot ulceration by
telemedicine that includes sensor-equipped insoles combined with
photo documentation. Trials. 20(521)2019.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Fawzy MS, Alshammari MA, Alruwaili AA,
Alanazi RTR, Alharbi JAM, Almasoud AMR, Alshammari RA and Toraih
EA: Factors associated with diabetic foot among type 2 diabetes in
Northern area of Saudi Arabia: A descriptive study. BMC Res Notes.
12(51)2019.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Alzahrani HA, Wang D, Alzahrani AH and Hu
FB: Incidence of diabetic foot disorders in patients with diabetes
in Jeddah, Saudi Arabia. Int J Diab Dev Countries. 35:115–122.
2015.
|
|
50
|
Rossboth S, Lechleitner M and Oberaigner
W: Risk factors for diabetic foot complications in type 2
diabetes-A systematic review. Endocrinol Diabetes Metab.
4(e00175)2020.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Al Kafrawy NA, Mustafa EA, Dawood ADA,
Ebaid OM and Ahmed Zidane OM: Study of risk factors of diabetic
foot ulcers. Menoufia Med J. 27:28–34. 2014.
|
|
52
|
Padda J, Khalid K, Khedr A, Tasnim F,
Al-Ewaidat OA, Cooper AC and Jean-Charles G: Non-Alcoholic fatty
liver disease and its association with diabetes Mellitus. Cureus.
13(e17321)2021.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Khneizer G, Rizvi S and Gawrieh S:
Non-alcoholic fatty liver disease and diabetes Mellitus. Adv Exp
Med Biol. 1307:417–440. 2021.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Targher G and Byrne CD: Clinical review:
Nonalcoholic fatty liver disease: A novel cardiometabolic risk
factor for type 2 diabetes and its complications. J Clin Endocrinol
Metab. 98:483–495. 2013.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Targher G, Byrne CD, Lonardo A, Zoppini G
and Barbui C: Non-alcoholic fatty liver disease and risk of
incident cardiovascular disease: A meta-analysis. J Hepatol.
65:589–600. 2016.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Guo K, Zhang L, Lu J, Yu H, Wu M, Bao Y,
Chen H and Jia W: Non-alcoholic fatty liver disease is associated
with late but not early atherosclerotic lesions in Chinese
inpatients with type 2 diabetes. J Diabetes Complications.
31:80–85. 2017.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Boulton AJM, Armstrong DG, Hardman MJ,
Malone M, Embil JM, Attinger CE, Lipsky BA, Aragón-Sánchez J, Li
HK, Schultz G and Kirsner RS: Diagnosis and management of diabetic
foot infections. American Diabetes Association, Arlington, VA,
2020.
|
|
58
|
Serban D, Papanas N, Dascalu AM, Stana D,
Nicolae VA, Vancea G, Badiu CD, Tanasescu D, Tudor C, Balasescu SA
and Pantea-Stoian A: Diabetic retinopathy in patients with diabetic
foot ulcer: A systematic review. Int J Low Extrem Wounds.
20:98–103. 2021.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Mponponsuo K, Sibbald RG and Somayaji R: A
comprehensive review of the pathogenesis, diagnosis, and management
of diabetic foot infections. Adv Skin Wound Care. 34:574–581.
2021.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Shojaiefard A, Khorgami Z and Larijani B:
Independent risk factors for amputation in diabetic foot. Int J
Diabetes Dev Ctries. 28:32–37. 2008.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Rismayanti IDA, Nursalam N, Farida VN,
Dewi NWS, Utami R, Aris A and Agustini NLPIB: Early detection to
prevent foot ulceration among type 2 diabetes mellitus patient: A
multi-intervention review. J Public Health Res.
11(2752)2022.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Serban D, Papanas N, Dascalu AM, Kempler
P, Raz I, Rizvi AA, Rizzo M, Tudor C, Silviu Tudosie M, Tanasescu
D, et al: Significance of neutrophil to lymphocyte ratio (NLR) and
platelet lymphocyte ratio (PLR) in diabetic foot ulcer and
potential new therapeutic targets. Int J Low Extrem Wounds: Nov 18,
2021 (Epub ahead of print).
|
|
63
|
Brănescu C, Serban D, Dascălu AM, Oprescu
SM and Savlovschi C: Interleukin 6 and lipopolysaccharide binding
protein-markers of inflammation in acute appendicitis. Chirurgia
(Bucur). 108:206–214. 2013.PubMed/NCBI
|
|
64
|
Adeleye OO, Ugwu ET, Gezawa ID, Okpe I,
Ezeani I and Enamino M: Predictors of intra-hospital mortality in
patients with diabetic foot ulcers in Nigeria: Data from the MEDFUN
study. BMC Endocr Disord. 20(134)2020.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Shi L, Wei H, Zhang T, Li Z, Chi X, Liu D,
Chang D, Zhang Y, Wang X and Zhao Q: A potent weighted risk model
for evaluating the occurrence and severity of diabetic foot ulcers.
Diabetol Metab Syndr. 13(92)2021.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Huang ZH, Li SQ, Kou Y, Huang L, Yu T and
Hu A: Risk factors for the recurrence of diabetic foot ulcers among
diabetic patients: A meta-analysis. Int Wound J. 16:1373–1382.
2019.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Tolossa T, Mengist B, Mulisa D, Fetensa G,
Turi E and Abajobir A: Prevalence and associated factors of foot
ulcer among diabetic patients in Ethiopia: A systematic review and
meta-analysis. BMC Public Health. 20(41)2020.PubMed/NCBI View Article : Google Scholar
|