1. Introduction
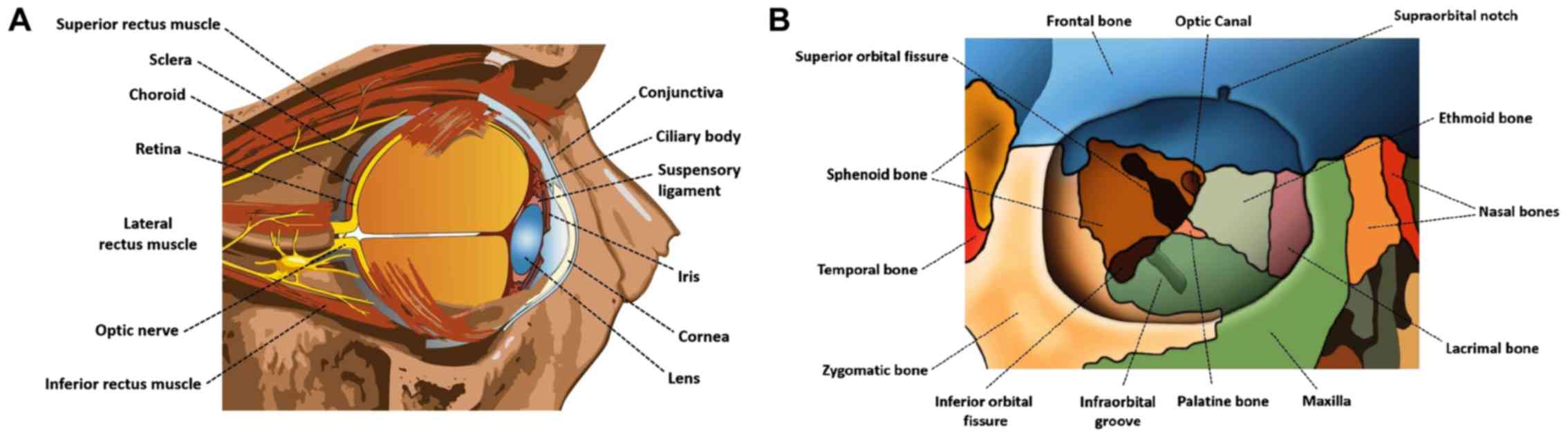
The orbital and ocular space consists of several
anatomical structures (Fig. 1) out
of which various tumors may arise, while orbital or ocular
metastases from several primary malignancies can be encountered,
often being the first sign of cancer dissemination. Prompt
diagnosis, accurate staging and restaging, and effective assessment
of treatment response are crucial for designing patient-tailored
therapeutic strategies. Cross-sectional imaging with conventional
modalities [computed tomography (CT) and magnetic resonance imaging
(MRI)] has being widely used for the management of these lesions.
However, in recent years, with the emergence of advanced hybrid
imaging techniques using positron emission tomography (PET)/CT and
PET/MRI systems, as the corner-stone of diagnostic imaging for
oncologic purposes, an emerging role of these modalities has been
recorded in the management of patients with orbital and ocular
tumors. This review focuses on current applications and future
directions of PET/CT and PET/MRI in ophthalmic oncology.
PET is a diagnostic imaging technique that enables
targeting, visualization and quantification of biochemical
processes at the cellular and sub-cellular level, via the
three-dimensional (3-D) reconstruction of the bio-distribution of
several molecules radiolabeled with positron-emitting isotopes.
Hybrid PET/CT systems combine the functional information provided
by the PET component with the structural information obtained from
CT, enabling attenuation correction of PET-images, accurate
anatomic localization of the distribution of the PET-tracer and
morphological characterization of lesions, leading to increased
diagnostic performance (1).
Moreover, the employment of contrast-enhanced CT as part of PET/CT
studies, can provide additional diagnostic information, further
improving the diagnostic capabilities of the modality (2).
Hybrid PET/MRI systems hold promise for superior
diagnostic capabilities for oncologic applications, since MRI is an
ionizing-radiation free method, that can be used for the MR-based
attenuation correction of the PET-images, while offering superior
soft-tissue contrast resolution, together with a broad spectrum of
imaging applications such as dynamic contrast enhanced MRI
(DCE-MRI), MR-spectroscopy (MRS) and diffusion weighted imaging
(DWI), enabling the acquisition of both anatomical and functional
information (3). In recent years,
technological advancements have led to the development of clinical
simultaneous PET/MRI systems, allowing superior spatial
registration of PET and MR images and enabling temporal correlation
between PET and MRI data, opening a broad new horizon of diagnostic
capabilities (4).
The PET-radiopharmaceuticals discussed in the
current review are summarized in Table
I. 18Fluoride-fludeoxyglucose (18F-FDG)
is a glucose analogue radiolabeled with fluorine-18
(18F), reflecting glucose consumption and therefore,
whole-body 18FDG PET/CT studies can produce a whole-body
metabolic map of the patient (5).
Increased glucose uptake is one of the major metabolic features
encountered in cancer cells, making 18F-FDG the most
widely employed PET-tracer for oncologic purposes (1,6-8).
However, abnormally increased 18F-FDG activity is not
cancer-specific, since various benign processes, such as adenomas,
or infectious and inflammatory lesions exhibit hyper-metabolism
(9-13). 18F-sodium fluoride
(18F-NaF) is a bone seeking PET-radiopharmaceutical,
which can effectively target both osteoblastic and osteolytic
processes, leading to increased bone surface area being exposed to
the blood flow (14). The
favorable 18F-NaF pharmacokinetics, the superior spatial
resolution of PET, together with the inherent quantitative
capabilities of PET-imaging and the capability for morphologic
characterization of lesions by the CT, render 18F-NaF
PET/CT a powerful diagnostic tool for oncologic skeletal imaging
(15-18). 68Ga-DOTA-compounds are
somatostatin (SST) analogs, radiolabeled with the positron emitting
isotope gallium-68 (68Ga) through the chelator
1,4,7,10-tetraazacyclododecane-1, 4,7,10-tetraacetic acid (DOTA)
(18). The employment of these
compounds enables highly efficient targeting of lesions which are
characterized by cell-surface over-expression of SST receptors
(SSTRs), such as neuroendocrine tumors (NETs), for which PET/CT
imaging with 68Ga-DOTA-compounds is evolving as the
imaging standard of reference (19-33).
 | Table IPET-radiopharmaceuticals employed for
PET/CT studies in patients with orbital and ocular tumors. |
Table I
PET-radiopharmaceuticals employed for
PET/CT studies in patients with orbital and ocular tumors.
| Feature |
18F-FDG |
18F-NaF |
68Ga-DOTA- compounds |
18F-fluorocholine
(18F-FCH) |
11C-methionine Methyl
(11C-MET) |
Alpha-[11C] -L-Tryptophan
(11C-AMT) |
|---|
| Half-life | 110 min | 110 min | 68 min | 110 min | 20 min | 20 min |
| Synthesis
requirements | Cyclotron | Cyclotron | In-house
generator | Cyclotron | Cyclotron | Cyclotron |
| Molecular
target | Metabolic
activity | Bone
remodeling | SSTRs cell surface
overexpression | Cell membrane
synthesis | Amino acid
transport | Tryptophan
metabolism |
| Orbital or ocular
tumor | Lymphoma, uveal
melanoma, retinoblastoma conjunctival melanoma, sebaceous
carcinoma, squamous cell carcinoma, optic nerve glioma, ocular and
orbital metastases, inflammatory orbital pseudotumor, fibrous
dysplasia | Fibrous
dysplasia | Ocular and orbital
metastases from neuroendocrine tumors (NETs) | Optic nerve
glioma | | |
2. Orbital lymphoma and ocular adnexal
lymphoma
Orbital lymphoma (OL) and ocular adnexal lymphoma
(OAL), are lypmphoproliferative malignancies, involving the orbit,
the eyelid, the conjunctiva, the lacrimal gland, or a combination
of these structures (34). OL is
the most common primary malignant tumor of the orbits among adults
(35), whereas OAL accounts for
55% of orbital malignancies among adults and represents 1-2% of
non-Hodgkin’s lymphoma (NHL) cases and 8% of extra-nodal
mucosa-associated lymphoid tissue (MALT) lymphomas (36,37).
In the majority of cases, OALs mainly arise from the lacrimal gland
and the conjunctiva, with 7-24% of patients presenting with
bilateral involvement (36). OL
and OAL can either be primary malignancies or metastases from
systemic disease. Histologically, the most common type of OAL is
MALT lymphoma, which is a low-grade B-cell NHL (35). Once the diagnosis of OL or OAL has
been established, accurate disease staging is of utmost importance
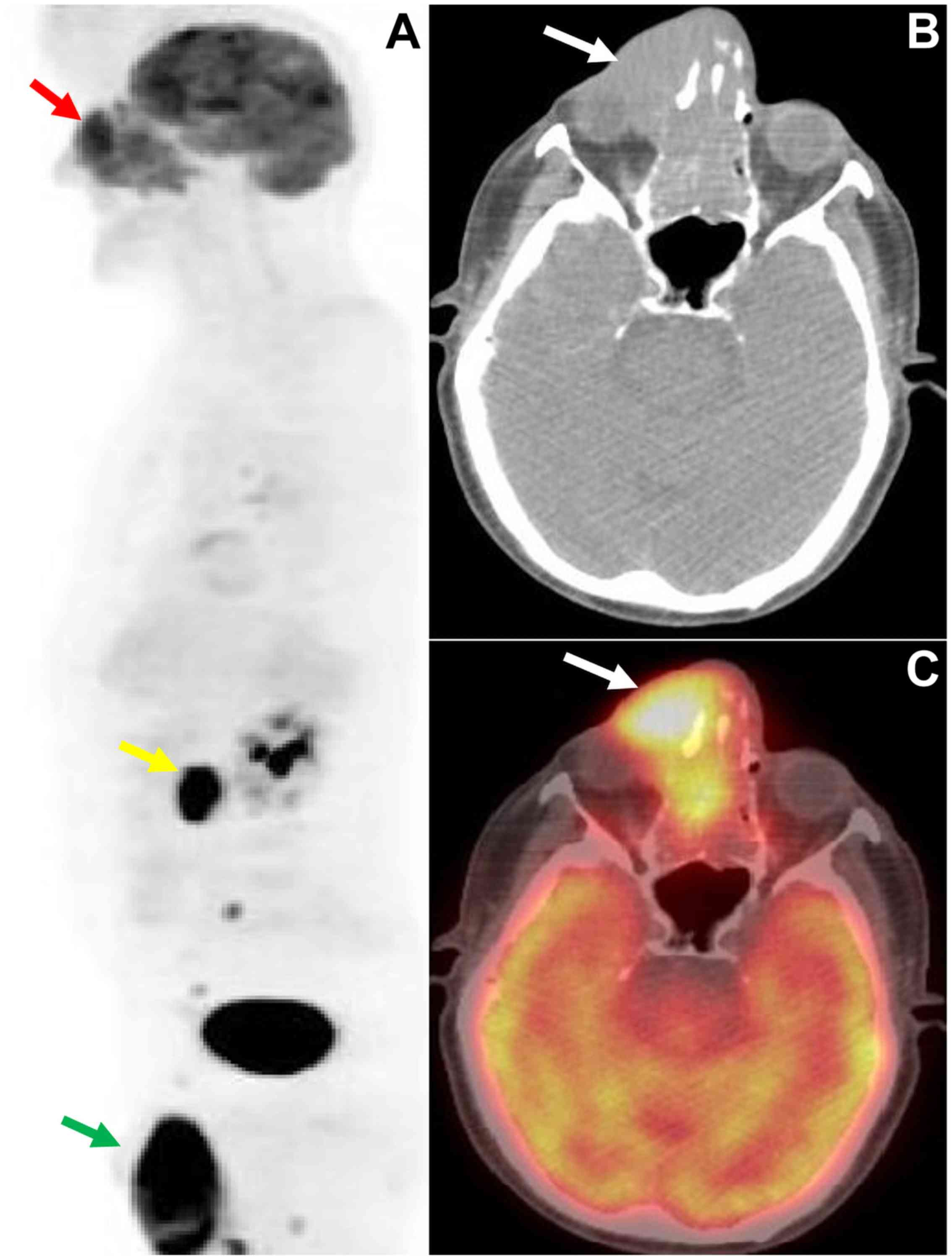
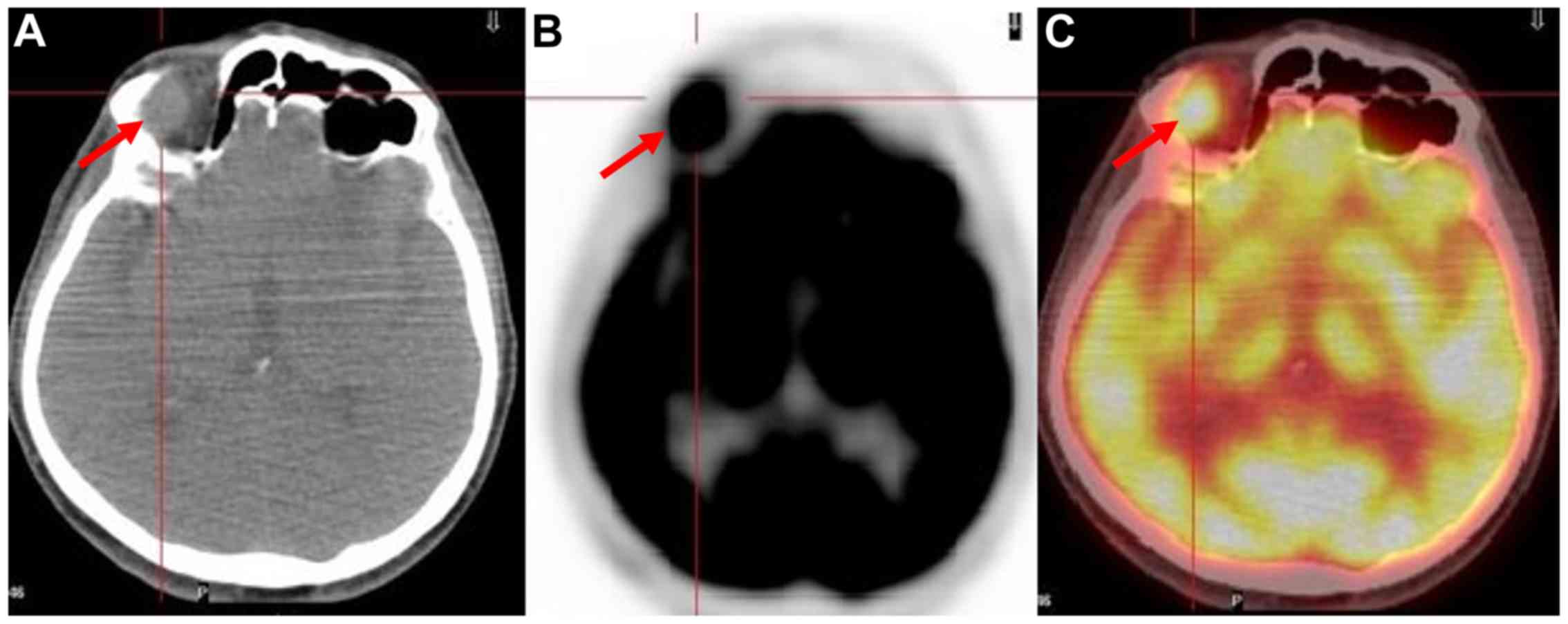
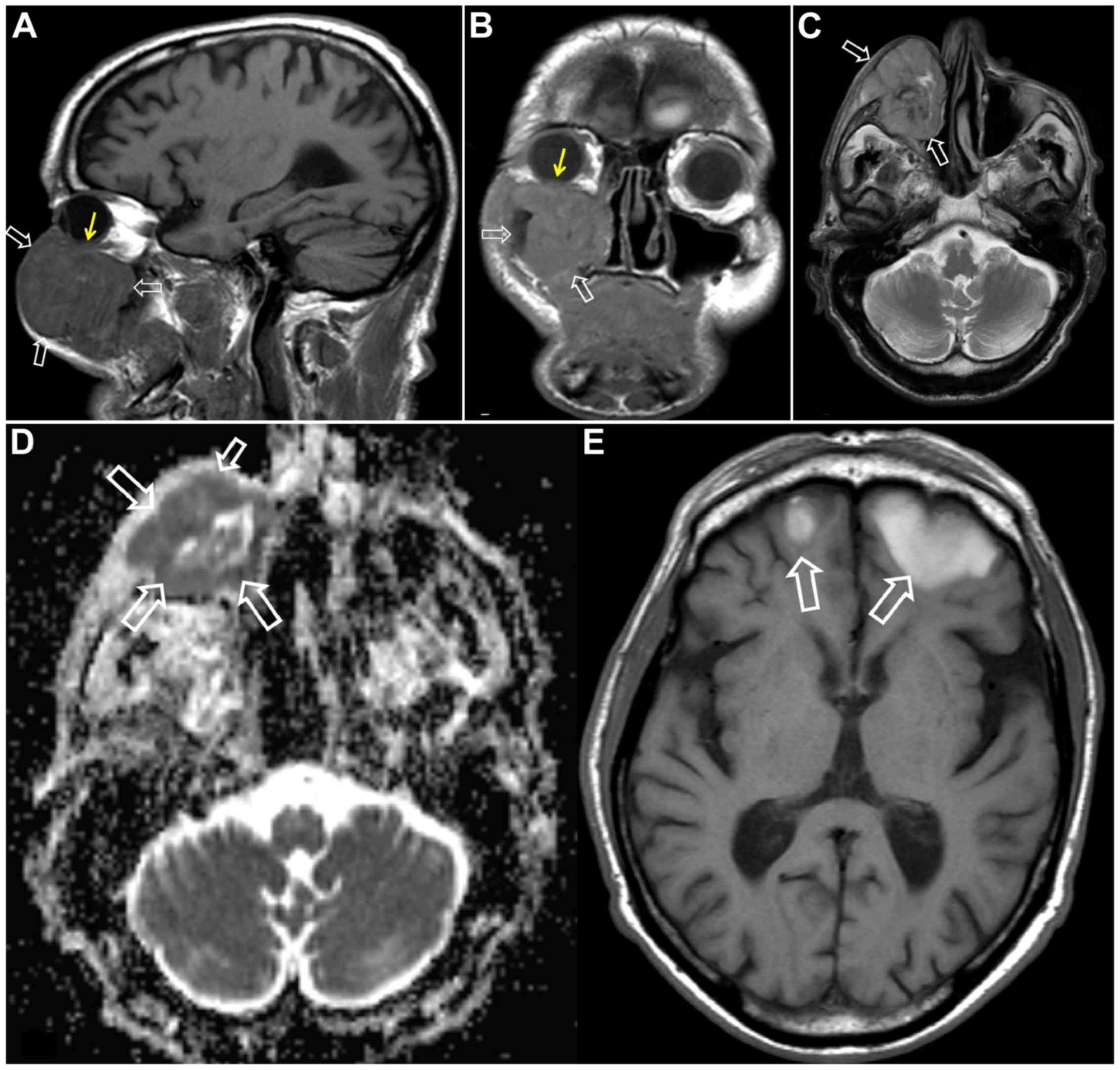
for optimal patient management. Whole-body PET/CT post
18F-FDG administration has evolved as the standard of
care for initial disease staging and post-treatment evaluation,
rendering OL and OAL the main orbital and ocular tumors, for which
PET/CT is routinely employed (35)
(Figs. 2-4). Low-grade MALT lymphomas may exhibit
low hyper-metabolic activity and therefore low-level
18F-FDG uptake, or may even present false negative
findings on 18F-FDG PET/CT. However, even for low-grade
OLs and OALs, 18F-FDG PET/CT has been proven to be
highly sensitive for accurate disease staging by detecting distant
metastases, missed on conventional imaging (35,36).
In a retrospective study of 11 patients with an
established diagnosis of OAL who underwent whole-body
18F-FDG PET scans at initial staging, Valenzuela et
al reported that 18F-FDG PET exhibited higher
sensitivity in detecting systematic extra-nodal disease compared to
conventional imaging with CT, leading to disease upstaging and
significantly affecting patient management; however, the efficacy
of the modality in detecting orbital lesions was limited, mainly
due to the small size of the lesions and physiologic
18F-FDG uptake by the extraocular muscles (38). English and Sullivan, in a series of
34 patients who also underwent 18F-FDG PET at initial
staging, confirmed the enhanced performance of the modality in
accurate disease staging, by detecting sites of systemic disease
missed on CT, and therefore, significantly altering management
strategies; their study also confirmed the limited performance of
18F-FDG PET in comparison to CT in detecting local OAL
lesions (37).
However, the advent of hybrid PET/CT technology had
a direct impact on OL and OAL detection performance. Roeet
al, in a series of 4 patients with biopsy-proven OAL,
demonstrated that hybrid 18F-FDG PET/CT was capable of
detecting the orbital tumor in 3 patients (75%), while revealing
systematic involvement in 2 of the 4 patients (50%) (39). Sugaet al reported that in a
patient with orbital MALT lymphoma, 18F-FDG PET/CT was
able to identify a small lesion in the contralateral orbit, which
had been missed on MR-imaging, and an unexpected metastatic gastric
lesion, indicating the increased efficacy of the method in accurate
disease staging (40).
Furthermore, post-treatment 18F-FDG PET/CT scans
revealed progressive regression and finally the disappearance of
18F-FDG activity at disease sites, suggesting the
utility of the modality for monitoring treatment response (40). Several other studies have confirmed
the usefulness of 18F-FDG PET/CT for the initial staging
and assessment of treatment response in patients with OLs and OALs
(41-43).
Fujiet al, in a recent series of 9 patients
with histologically proven OAL [diffuse large B-cell lymphoma,
MALT, follicular lymphoma, natural killer (NK)/T-cell lymphoma,
lymphoplas-macytic lymphoma, Hodgkin’s lymphoma (HL)] who underwent
pre- and post- treatment 18F-FDG PET/CT investigated the
utility of the modality in assessing treatment response (44). 18F-FDG uptake was
assessed by means of maximum standard-ized uptake value (SUVmax),
and a decrease was recorded in 8 out of the 9 patients
post-treatment, while in 7 patients there was a complete metabolic
response from the first post-treatment scan, which was in
accordance with the clinical condition of the patients during the
follow-up period. Only in one patient there was a false-negative
conjunctival lesion on 18F-FDG PET/CT, indicating that
the usefulness of the modality may be affected by the histological
type and the anatomic location.
3. Uveal melanoma
Uveal melanoma (UM) (Fig. 5) is the most common primary
intraocular malignancy among adults, and most frequently arises
from the choroid (85% of cases) (36,45).
Singhet al, in a systematic review including 4,070 patients
with primary UM in the USA over a 36-year period from 1973 to 2008,
reported a mean age-adjusted incidence of 5.1 per million of
population (95% CI, 4.8-5.3), a predilection for the Caucasian
population (97.8% of cases) and an unaltered 5-year survival rate
of 81.6% (46). Tumor size, an age
>60 years, intense tumor pigmentation and localization in the
anterior uvea have been shown to indicate a poor prognosis
(36). Although distant metastases
can occur to the lungs, bones and the central nervous system, UM
presents a unique metastatic pattern to the liver, as the main site
for disease dissemination (36,45,47).
Therefore, accurate disease staging is critical for guiding
decision-making in patients diagnosed with UM.
In an early study by Reddyet al, including a
cohort of 50 patients with untreated choroidal melanomas [American
Joint Cancer Committee (AJCC); T1:18 patients, 36%; T2:24 patients,
48%; T3:8 patients, 16%], 18F-FDG PET/CT failed to
detect any of the AJCC-T1 tumors, while increased
18F-FDG activity (SUVmax >2.5) was observed in 33 and
75% of AJCC-T2 and AJCC-T3 choroidal melanomas, respectively
(48). According to these
findings, it was suggested that 18F-FDG PET/CT most
likely cannot differentiate small UMs from suspicious nevi, and
does not seem to be superior over standard clinical evaluation with
ophthalmoscopy, fluorescein angiography and ophthalmic
ultrasonography (US) in the detection of primary choroidal
melanomas. Fingeret al, in a series of 14 patients with
choroidal melanomas (AJCC-T2, 1 patient; AJCC-T3, 13 patients),
reported that the one T2 tumor and 10 out of the 13 (77%) T3 tumors
demonstrated elevated 18F-FDG uptake (SUVmax >2.5)
with the highest SUV value (9.0) observed in the tumor which was
largest in size (49).
Furthermore, they reported a positive association between SUV
values with known clinical, pathological and US characteristics
related to increased metastatic potential, indicating possible
prognostic value of 18F-FDG uptake observed on PET/CT in
the setting of UM (49).
In a cohort of 7 patients with choroidal melanoma,
Matsuoet al explored the association between
18F-FDG avidity and the clinicopathological
characteristics of the tumors. 18F-FDG PET/CT detected
the primary tumor in 5 out of 7 patients, concluding that large
nodular choroidal melanomas can be effectively identified by
18F-FDG PET/CT, in contrast to diffusely infiltrating
choroidal melanomas without nodular formation, which proved to be
18F-FDG-negative (50).
However, all distant liver and bony metastases in 2 of the patients
in the cohort were effectively targeted with 18F-FDG
PET/CT, suggesting the employment of the modality for disease
staging. Furthermore, a positive association was reported between
tumor size, as defined by histopathological measurements and
18F-FDG uptake, as determined by SUVmax (50). McCannelet al, in a
retrospective study including 37 patients with primary choroidal
melanomas, reported significant association between
18F-FDG positivity of the tumors (SUVmax >2.5) with
larger tumor size and with chromosome 3 loss, which is a known risk
factor related with increased metastatic potential of choroidal
melanomas (51). This data
indicated that apart from tumor size, 18F-FDG positivity
may be associated with molecular features of UMs and that
18F-FDG avidity holds promise to serve as an independent
prognostic biomarker for patients with UM.
Papastefanouet al, in a retrospective study
of 76 patients diagnosed with UM who underwent pre-operative
18F-FDG PET/CT scans, reported 18F-FDG
positivity (SUVmax >2.5) in 92% of the tumors (52). In addition, 94% of patients with
chromosome 3 monosomy exhibited 18F-FDG avidity (SUVmax
>2.5), whereas patients with abnormalities (gains) in chromosome
8, which is also associated with a poor prognosis in UM did not
exhibit significantly higher 18F-FDG activity. Moreover,
increased tumor size and AJCC tumor-node-metastases (TNM)
prognostic groups were positively associated with
18F-FDG uptake, as determined by SUVmax, further
implying the prognostic application of 18F-FDG PET/CT
imaging in the setting of patients with UM (52).
However, the main indication for the employment of
18F-FDG PET/CT in the work-up of patients with UM is the
detection of regional and distant metastasis. Kurliet al
reported 100% sensitivity and 100% specificity of
18F-FDG PET/CT in detecting liver metastases compared to
12.5% sensitivity of liver function tests (LFTs). Furthermore,
18F-FDG PET/CT significantly contributed to the
detection of osseous extra-hepatic metastatic lesions, implying the
application of this technique for disease staging at the time of
initial diagnosis as well as for follow-up purposes (53). In a large retrospective series of
333 patients with UM, who underwent whole-body 18F-FDG
PET/CT studies for staging purposes at the time of initial
diagnosis, Fretonet al confirmed the value of the modality
as a screening tool for initial staging (54). All 18F-FDG-positive
liver lesions observed on PET/CT were subsequently confirmed as
metastases via biopsies, indicating 100% positive predictive value
(PPV), providing significant advantages over anatomic imaging
techniques, which exhibit a higher rate of false-positive liver
findings. Furthermore, 18F-FDG PET/CT enabled the
detection of extra-hepatic disease sites missed on blood tests or
conventional imaging, and revealed synchronous second primary
malignancies in 3.3% (95% CI: 0.9-5.5) of the study population,
significantly affecting patient management (54).
However, Strobelet al, in a retrospective
study of 13 patients with UM, questioned the usefulness of
18F-FDG PET/CT in UM staging, since 16 out of 27 liver
lesions (59%) were 18F-FDG-negative, all of which were
detected by anatomic imaging with CT or MRI (55). Furthermore, liver metastases from
UM demonstrated significantly (P<0.001) lower 18F-FDG
uptake in terms of SUVmax in comparison to liver metastases from
cutaneous melanoma, although histological analysis did not reveal
any difference in glucose transporter-1 (GLUT-1) expression between
UM and CM liver metastases (55).
In accordance with the findings of the study by Strobelet al
(55), Orcurtoet al
reported the superiority of MRI over 18F-FDG PET/CT in
detecting small metastatic liver lesions in patients with UM
(56). However, Orcurtoet
al (56) observed that during
chemotherapy, 18F-FDG activity in liver lesions with a
stable size on MRI, exhibited a significantly decreased
lesion-to-liver SUV ratio, while enlarging lesions on MRI exhibited
an increased lesion-to-liver SUV ratio. These data suggest the
application of 18F-FDG PET/CT in the early assessment of
treatment response (56).
4. Retinoblastoma
Retinoblastoma (RB) is a malignant tumor of the
retina originating from precursor cells of the retinal
neuroepithelium (36). RB is the
most common intraocular tumor in childhood, with 95% of patients
being diagnosed by the age of 5 (57). RB can be encountered either in a
hereditary (40%) or in a sporadic form (60%), with patients with
hereditary RB presenting with an increased risk of developing
intracranial primitive neuroecto-dermal tumor (PNET), most
frequently pineoblastomas (58-60).
The combination of unilateral or bilateral hereditary RB with an
intracranial PNET is termed trilateral RB, which is often
associated with a poor prognosis due to spinal dissemination
(61). RBs typically present with
leukocoria, while proptosis, pain, redness and swelling can be
common RB manifestations (62).
Radhakrishnanet al, in a prospective
evaluation of the role of 18F-FDG PET/CT in staging and
assessment of the response to neoadjuvant chemotherapy,
demonstrated that intraocular RB did not take up the radiotracer,
in contrast to the 18F-FDG avidity of extraocular RBs
(63). Furthermore, no significant
difference was revealed between staging with CT or MRI and staging
based on 18F-FDG PET/CT findings. However, the detection
of 18F-FDG uptake by the optic nerve at the baseline
PET/CT study was strongly associated with poor event-free survival
(EFS) and overall survival (OS), indicating a strong prognostic
value, in comparison to patients with no 18F-FDG uptake
by the optic nerve. In addition, a complete or partial response to
neoadjuvant chemotherapy assessed by 18F-FDG PET/CT was
associated with an improved EFS and OS, further supporting the
prognostic value of the modality (63).
5. Conjunctival melanoma
Conjunctival melanoma (CM) is a relatively rare, yet
potentially lethal malignancy with an increasing incidence rate
(64). Folberget al
reported that approximately 75% of CMs typically arise from primary
acquired melanosis (PAM), with 9-25% of patients with CM presenting
local or systematic spread with lymph node (LN) involvement
(65,66). In a retrospective cross-sectional
study including 85 patients with primary CM, aiming to elucidate
the metastatic pattern of this neoplasm, Tuomaala and Kivelä
demonstrated that initial regional LN and systematic metastasis
were equally encountered, with LN infiltration being associated
with a better prognosis (67).
Major metastatic sites are the lungs, the liver, the
gastrointestinal track and the central nervous system (68).
18F-FDG PET/CT has been employed for
staging purposes in patients with CM. Kurliet al
investigated 14 patients with CM (13 patients with T3 tumors, 1
patient with T4 tumor), who were evaluated with whole body
18F-FDG PET/CT scans for the detection of metastatic
disease (68). Seven of these
patients were scanned with 18F-FDG PET/CT at initial
diagnosis and 7 were imaged post-treatment (surgical removal with
adjuvant cryotherapy and/or chemotherapy). The study concluded that
18F-FDG PET/CT failed to reveal local, regional or
systemic disease in any of the 13 patients with diffuse, multifocal
T3 CM, either at initial diagnosis or post-treatment. On the
contrary, the post-treatment 18F-FDG PET/CT scan
revealed widespread metastases in the nasal fossa, liver, pleural
space, mediastinal lymph nodes, lungs, peritoneal cavity, lumbar
spine and right supraclavicular lymph node in the patient with T4
CM. Based on these data, Kurliet al suggested the limited
application of 18F-FDG PET/CT at the initial staging of
patients with CM, with potential usefulness for follow-up and
re-staging purposes (68).
Damianet al reported the positive
contribution of 18F-FDG PET/CT in the effective
management of a patient with CM, by successfully detecting the
primary ocular lesion and an infiltrated preauricular node, and by
excluding other LN involvement or systemic dissemination of the
disease (66). Tsaiet al
described the usefulness of 18F-FDG PET/CT in revealing
CM as a second primary neoplasm, in a patient with lymphocytic
lymphoma/chronic lymphocytic leukemia (CLL) and nasal cavity
carcinoma (69). Given these data,
further studies are required to explore the potential usefulness of
18F-FDG PET/CT in the management of CM.
6. Sebaceous carcinoma
Sebaceous carcinoma (SebCa) is a rare type of cancer
with a low incidence rate (0.11 to 0.65 cases/100,000
individuals/year) and a higher prevalence in the female population
(70,71). With the face being the most common
anatomical region for SebCa due to the abundance of sebaceous
glands, it is usually presented as a nodule or diffuse thickening
of the eyelids (71). Although the
upper lid and the palpebral conjunctiva are the most common sites,
SebCa may also arise in the bulbar conjunctiva and the caruncle
(71). Eyelid SebCa can often be
misdiagnosed both clinically and pathologically (72). Typically, there is a delay in the
diagnosis associated with a higher recurrence rate following
surgical excision, ranging from 18 to 19.4% (71,72).
Distant and nodal metastases have been associated with eyelid SebCa
in 3-8 and 8-18% of cases, respectively (71).
In a series of 15 patients with biopsy-proven
periorbital tumors Baeket al, reported that in the subset of
patients (5 out of 15) with SebCa of the upper eyelid
18F-FDG PET/CT successfully detected all cases with
regional LN involvement, even when contrast-enhanced CT was falsely
negative (73). Krishnaet
al reported the employment of 18F-FDG PET/CT in
successfully staging 2 patients with ocular SebCa, critically
contributing to optimal patient management, guiding the decision to
preserve the eye and implying the application of the modality in
accurate staging of ocular and non-ocular SebCas (74). Furthermore, follow-up in patients
with SebCa can be facilitated with 18F-FDG PET/CT.
Ishiguroet al reported the detection of a colon
adenocarcinoma 42 months following the surgical removal of a left
upper eyelid SebCa, in a patient with Muir-Torre syndrome, which is
characterized by the presence of at least one sebaceous skin tumor
(75). Thus, 18F-FDG
PET/CT is of value for staging and restaging purposes in patients
with SebCa.
7. Squamous cell carcinoma
Squamous cell carcinoma (SCC) is a type of skin
cancer which manifests as a scaled, indurated, keratinized or
ulcerated raised nodule or plaque, which is most commonly
encountered in the lower eyelid and medial canthus, with an
incidence rate 3-fold higher in males than in females (71). SCC arises from abnormal
keratinocyte proliferation and either emerges for the first time
without any previous predisposition or in sites of pre-existing
actinic or solar keratosis (71).
The clinical presentation of SCC may vary from erythematous patches
to large ulcerated lesions. The 5-year recurrence rate ranges from
2.4 to 36.9% with regional LN involvement at 25% of cases, and
distant metastases in 6.2% of cases, with the most common regional
metastatic sites being the parotid, the preauricular and the
submandibular nodes (76,77). Periocular SCC is highly metastatic
in the case of delayed treatment, invading orbital and intracranial
structures and leading to considerably increased mortality and
morbidity (78,79).
18F-FDG PET/CT has been reported to be an
effective tool for the detection of distant metastases in patients
with recurrent head and neck SCCs (HNSCCs). In a series of 82
patients with histologically confirmed HNSCCs, Yiet al
reported that whole-body 18F-FDG PET/CT correctly
identified distant metastases in 12 of 14 patients and their
absence in 57 of 68 patients, exhibiting sensitivity, specificity,
accuracy, PPVs and negative predictive values (NPVs) of 86% (95%
CI, 57-98%), 84% (72-91%), 84% (74-91%), 52% (30-73%) and 97%
(88-99%), respectively (80).
Literature on the employment of 18F-FDG PET/CT in the
work-up of patients with eyelid or conjunctival SCC is rather
limited. Linet al reported high 18F-FDG avidity
(SUVmax: 8) by a biopsy proven left bulbar conjunctiva SCC, in a
patient with previous history of endometrial lymphoma (81). Abdelmaliket al reported a
patient with a biopsy-proven left orbital SCC, which was intensely
18F-FDG avid in the pre-treatment PET/CT scan (82). Furthermore, several
retromandibular, mediastinal and abdominal LNs demonstrated
increased 18F-FDG activity, with only the
retromandibular being metastatic and the remainder being
inflammatory, highlighting the limitations of the modality in
cancer staging, since both malignant and inflammatory processes
exhibit elevated 18F-FDG uptake (82). Therefore, based on the existing
literature, further studies are required to justify the usefulness
of 18F-FDG PET/CT in the setting of periocular SCC.
8. Rhabdomyosarcoma
Rhabdomyosarcoma (RMS) is the most common
mesenchymal tumor in childhood accounting for approximately 4-5% of
all pediatric cancers, with orbits being the commonest site in the
head and neck (36,83). Orbital RMS usually presents as a
unilateral rapidly progressive mass, leading to proptosis or globe
displacement, while eyelid edema, hemorrhage, pain, vision
impairment, blepharoptosis, conjunctival edema and inflammatory
signs consist non-specific RMS manifestations. RMS of the orbits is
an aggressive, life-threatening malignancy with high potential to
infiltrate adjacent tissues, while metastatic dissemination can
occur to the lungs, bones, bone marrow and LNs (83). Therefore, accurate initial staging
and restaging is critical for the optimal and individualized
patient management.
Normanet al, in a systematic review
including 272 patients with RMS, with orbits being the primary
tumor site in at least 13 cases (not all included studies provided
information on the location of the primary tumor), investigated the
role of 18F-FDG PET and 18F-FDG PET/CT in the
management of childhood RMS (84).
They reported that 18F-FDG PET and 18F-FDG
PET/CT had been consistently superior over conventional imaging
(contrast-enhanced CT, standard MRI, technetium-99m bone
scintigraphy) at the initial RMS staging, since LN involvement and
distant metastases were determined with higher accuracy.
Furthermore, the management strategy was altered based on
18F-FDG PET and 18F-FDG PET/CT findings in
7/40 (17.5%) RMS patients (not all the included studies provided
information on this outcome) (84). However, the role of
18F-FDG PET/CT as a prognostic indicator of the outcome
in patients with RMS, is controversial (85). Moreover, patients and particularly
pediatric patients with RMS may benefit from 18F-FDG
PET/MRI, which promises more accurate locoregional staging and
follow-up evaluation (36,86).
9. Optic nerve glioma
Optic nerve glioma (ONG), also known as optic
pathway glioma (OPG), is the most common primary optic nerve tumor,
accounting for approximately 1% of all intracranial tumors. ONG is
divided into two types: A low-grade benign form and an aggressive
highly malignant form. Benign ONGs are slow-growing tumors, which
are mostly encountered in children and are often associated with
neurofibromatosis type 1 (NF-1). Bilateral ONGs are almost
pathognomonic for NF-1. ONGs in pediatric patients usually present
with painless proptosis, decreased visual acuity, visual fields, or
color vision, while compression effects can cause hypothalamic
symptoms or obstructive hydrocephalus due to the compression of the
third ventricle and central retinal vein occlusion (CRVO) because
of the compression of the central retinal vein. The aggressive form
of ONGs is mainly encountered among adults and consists a
life-threatening malignancy with poor prognosis. ONGs among adults
are rapidly-growing neoplasms, which present with acute vision loss
bilaterally due to the involvement of the optic chiasm (36,87-89).
Miyamotoet al first reported intense
18F-FDG uptake by an ONG in an adult patient, guiding
decision for surgical excision (90). Penget al reported the
utility of PET imaging with
alpha-[11C]methyl-L-tryptophan in assessing the
treatment response in a child with symptomatic ONG (91). Mohariret al, in a small
retrospective study of pediatric patients with NF-1, implied that
18F-FDG PET/CT may play a role in ONG surveillance by
differentiating those tumors with a higher likelihood to advance
and become symptomatic (92).
Roselliet al reported the application of PET/CT with
18F-fluorocholine (18F-FCH), which targets
the biosynthesis of cell membranes, in assessing treatment response
of ONG in the setting of NF-1 (93). Rizzoet al, in a recent case
report, described intense 11C-methionine
(11C-MET) activity by an ONG in an 80-year-old male
patient (94). 11C-MET,
is a PET-tracer, targeting amino acid utilization processes, which
exhibits advantages over 18F-FDG in detecting brain
tumors, such as very low-level activity by inflammatory sites and
by normal brain tissue (95).
These data hold promise for the application of 11C-MET
PET imaging in patients with ONG. However, larger prospective
series of patients are required to elucidate the role of
PET-imaging utilizing several PET-tracers beyond 18F-FDG
in the management of both benign and malignant ONG types.
10. Ocular and orbital metastases
Intra-ocular metastases are the most common
intra-ocular malignancy, and often the first sign of systemic
cancer spreading (96). The uvea,
due to its rich vascularity, is the commonest metastatic site with
the choroid being the most often metastatic location, while iris or
ciliary body involvement is less commonly encountered (97). In patients with presumed uveal
metastases, conventional imaging modalities (CT and MRI) often fail
to detect the primary tumor. In this setting of patients,
whole-body 18F-FDG PET/CT studies can vitally contribute
to accurate patient management, by successfully detecting the
primary site and other metastatic lesions not seen on CT or MRI
(98).
Orbital metastases stand for the most commonly
encountered orbital malignancy, accounting for approximately 20% of
all orbital cancers (36,99), and being the first disease
manifestation in 15% of the cases (100). Patients with orbital metastases
usually present with diplopia, pain, palpable mass, proptosis,
strabismus and visual loss. Breast, lung and prostatic cancer,
together with cutaneous melanoma and neuroblastomas in children are
the commonest tumors metastasizing to the orbit (36,99,101). Orbital metastases exhibit
18F-FDG avidity and therefore, 18F-FDG PET/CT
is a valuable diagnostic tool for these patients, enabling
detection of the primary tumor, accurate disease staging and
effective assessment of therapeutic response (99). Furthermore, orbital metastases
originating from NETs can be successfully detected on SSTRs imaging
with PET using 68Ga-DOTA-conjugated compounds (18,101). Both ocular and orbital metastases
harbor histological features identical to the primary malignancy,
and therefore, immunohistochemistry should be employed in
challenging cases, where imaging with advanced hybrid techniques
fails to detect the primary disease site.
11. Inflammatory orbital pseudotumor
Inflammatory orbital pseudotumor (IOP), also known
as idiopathic orbital pseudotumor, is a benign, non-infective,
inflammatory condition of the orbit without systematic or locally
identifiable causes, being reported as the most common cause of
painful orbital mass and the third most common orbital disease
following thyroid orbitopathy and lymphoproliferative disorder
(102,103). Typically, adult patients with IOP
suffer from unilateral orbital pain, proptosis and impaired ocular
movement, while in pediatric cohorts, IOP is bilaterally
manifested, commonly associated with disc edema, uveitis and
eosinophilia (103).
Histopathologically, IOPs are characterized by a mixed inflammatory
infiltrate, exhibiting a mixture of small lymphocytes, plasma cells
and histiocytes (36,102), while fibrosis is frequently
encountered (104).
Imaging-wise, IOP is a great 'mimicker’ (105). 18F-FDG PET/CT scans
demonstrate highly elevated radiotracer activity, in a
lymphoma-mimicking pattern and biopsy is further required for
establishing diagnosis (36).
However, 18F-FDG PET/CT can efficiently facilitate
accurate monitoring of treatment response, in cases of non-surgical
treatment approaches such as radiotherapy or administration of
steroids, or in cases of incomplete surgical resection and lesion
recurrence (106).
12. Fibrous dysplasia
Fibrous dysplasia (FD) of the bone is an uncommon,
developmental benign skeletal disorder, characterized by the
replacement of normal bone and normal bone marrow with abnormal
fibro-osseous tissue, leading to bone deformity, pain, fractures
and physical impairment (107).
FD may affect a single skeletal site (monostotic FD), or multiple
sites (polyostotic FD), and can be encountered either sporadically
or in combination with extra-skeletal manifestations, including
café-au-lait-like skin pigmentation and hyperfunctioning
endocrinopathies. The combination of skeletal FD lesions with one
or more extra-skeletal manifestations is termed McCune-Albright
syndrome (MAS) (107,108). FD involvement of the orbital
bones can lead to hypertelorism, exophthalmos, vision impairment or
even vision loss, due to narrowing of the optic nerve canal and
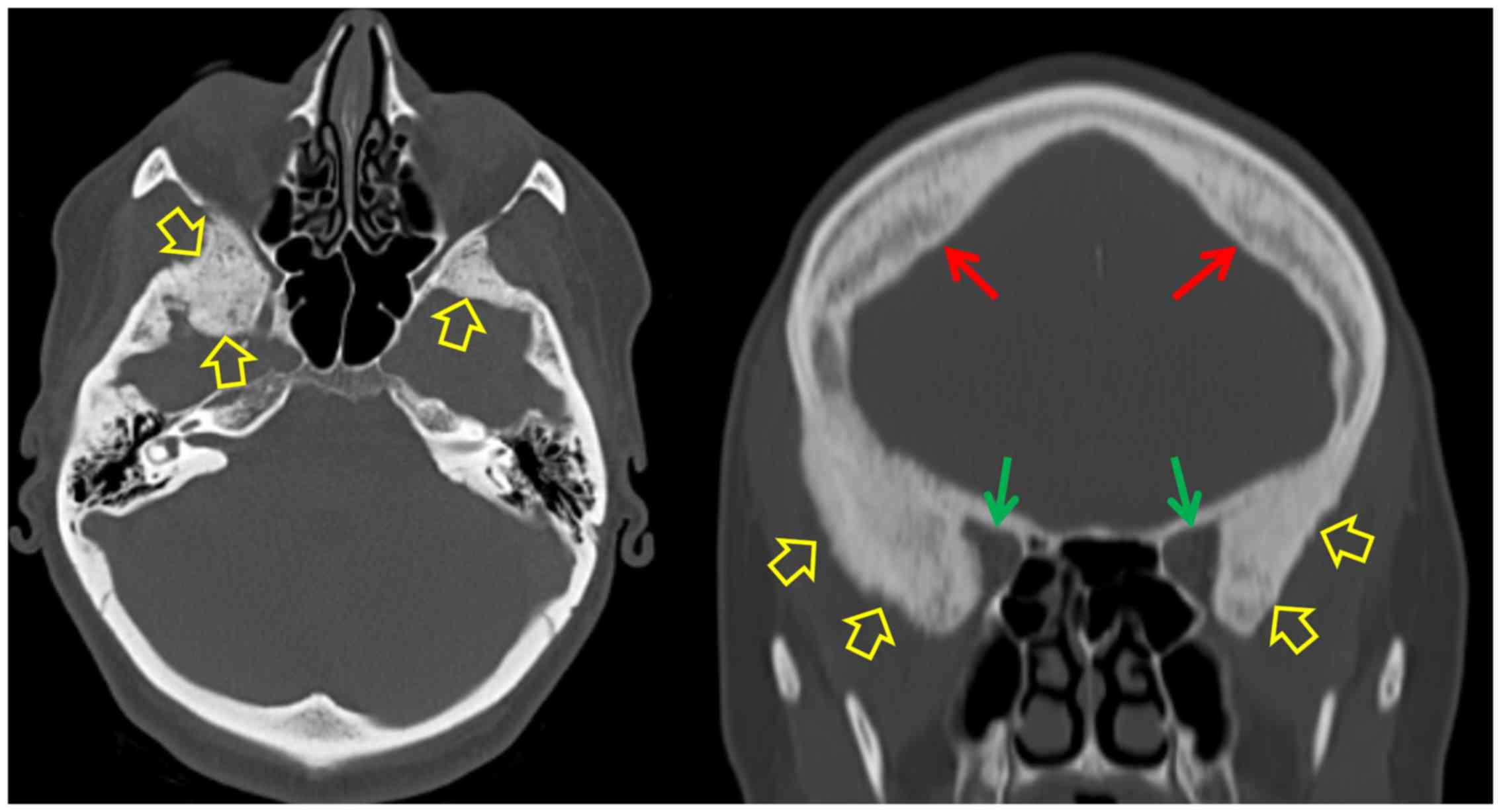
subsequent optic nerve compression (36). Typically, bone FD lesions present a
characteristic ground-glass appearance on the CT scan with
expansion of the medullary cavity (Fig. 6).
Bone FD lesions may present
18F-FDG-negative (109,110) or exhibit variable degrees of
18F-FDG activity on PET/CT, mimicking malignancy
(111-116). However, co-registration with CT
enables confident characterization of lesions and avoidance of
erroneous interpretation of 18F-FDG positive skeletal
findings. Moreover, intensely increasing 18F-FDG
activity by FD lesions should raise suspicion for the rare
possibility of malignant transformation (<2% of all FD cases)
(117,118). In this particular setting of
malignantly transformed FD lesions, whole-body 18F-FDG
PET/CT has a role in the early detection of the transformation and
in the management of these patients, by facilitating accurate
biopsy guidance, staging, optimal surgical planning, detection of
recurrence and efficient follow-up (118).
Bone FD has been visualized with conventional SSTRs
scintigraphy using 111ln-pentetreotide, suggesting cell
surface over-expression of SSTRs by fibrous dysplastic cells
(119). The introduction of
68Ga-DOTA-conjugated-peptides into clinical practice has
enabled the employment of PET-imaging in targeting lesions,
characterized by SSTRs-overexpressi on (18,19-33).
Papadakiset al reported intensely increased
68Ga-DOTATE (radiolabeled somatostatin analogue suitable
for PET-imaging, which targets SSTRs) activity on PET/CT, by a
biopsy proven FD lesion in the temporal bone (22). These data suggest the potential
application of PET/CT with 68Ga-DOTA-conjugated-peptides
in assessing and monitoring FD activity or even prognostic value of
68Ga-DOTATATE uptake in FD lesions that need to be
further investigated. Furthermore, bone FD can be effectively
targeted with 18F-NaF PET/CT (Fig. 7), which has been shown to be
strongly associated with bone turnover markers in the blood, while
exhibiting prognostic value for clinical manifestations of the
disorder (120-124).
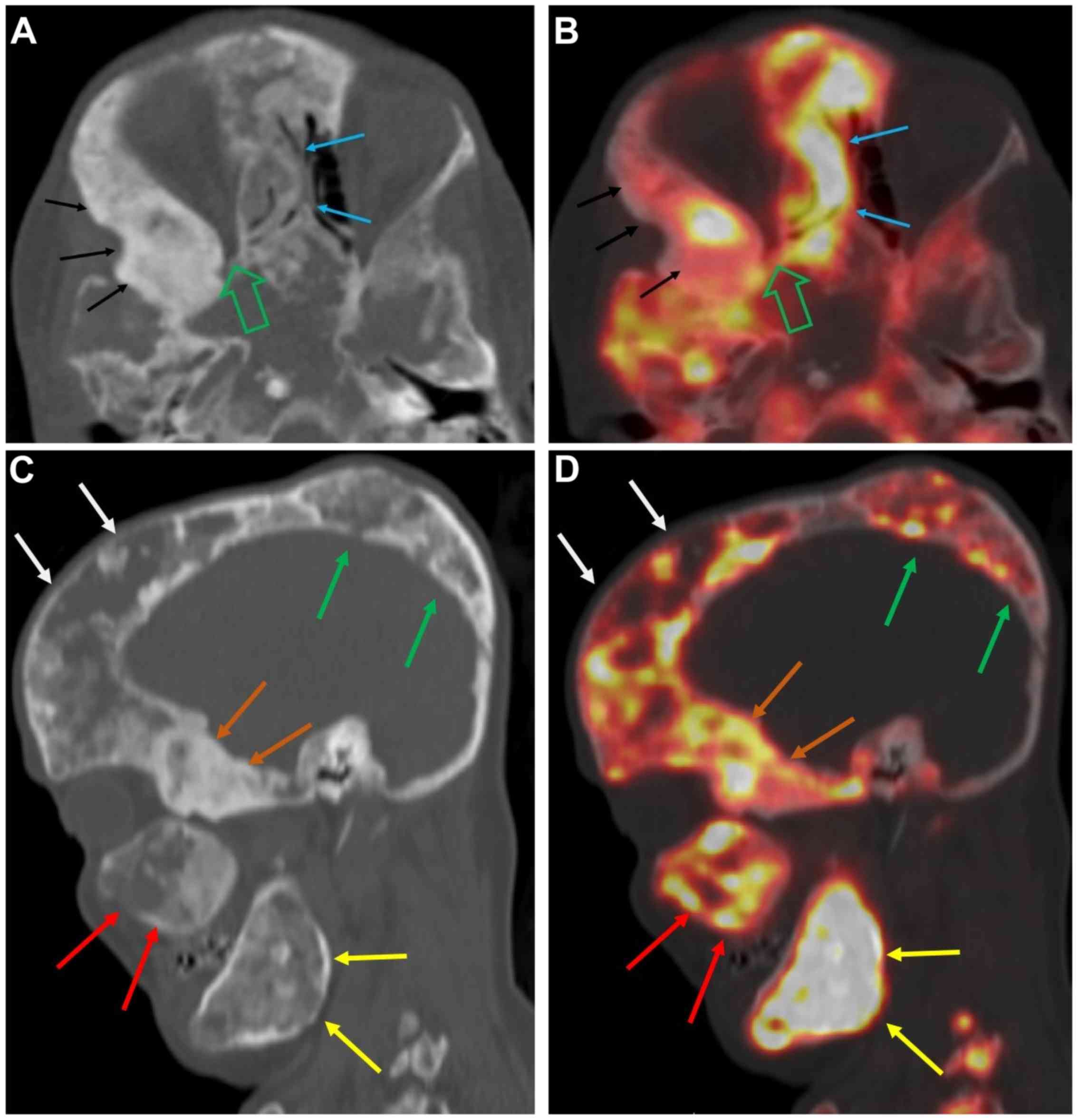 | Figure 7A 46-year-old female with extensive
fibrous dysplastic bone lesions with both hypodense and hyperdense
lesions on the CT. (A and B) Axial CT and fused 18F-NaF
PET/CT images of the skull showing marked narrowing of the right
orbital apex (open green arrow) and FD lesions involving the nasal
bones (blue arrows) and the right sphenoid bone (black arrows),
with abnormally increased 18F-NaF uptake. (C and D)
Sagittal CT and fused 18F-NaF PET/CT images of the skull
showing FD lesions involving the right frontal bone (white arrows),
right parietal bone (green arrows), right sphenoid (orange arrows),
right maxilla (red arrows), and right ramus of mandible (yellow
arrows), all of which exhibit abnormally elevated
18F-NaF activity. (Figure is courtesy of Dr M.T. Collins
and Dr A.M. Boyce, National Institute of Dental and Craniofacial
Research (NIDCR), National Institutes of Health (NIH), Bethesda,
MD, USA. 18F-NaF, 18F-sodium fluoride;
PET/CT, positron emission tomography/computed tomography; FD,
fibrous dysplasia. |
13. PET-MRI
PET/MRI combines the functional information of PET
with the superior soft-tissue contrast and the functional
MR-sequences, providing enhanced oncologic applications, especially
in small anatomic regions with complex anatomy such as the orbital
and ocular space. Furthermore, pediatric and pregnant oncologic
patients with need for follow-up studies, can take advantage of the
reduced radiation exposure of PET/MRI compared to PET/CT. In recent
years, PET-MRI technology has evolved into an established clinical
diagnostic tool, with instrumentation advancements leading to PET
detectors compatible with the MRI field, enabling simultaneous PET
and MRI acquisition (125,126).
These advancements hold promise for superior diagnostic
capabilities, improved image quality with reduced PET-image noise,
more accurate co-registration of PET-data with MRI anatomy,
correction for respiratory, heart and bulk patient motion, and
temporal synchronization of the data acquired by the two modalities
(4).
PET/MRI has already been widely employed in the
management of head and neck cancers, providing incremental
diagnostic information for the local staging of the primary tumor
and regional lymph node status, while facilitating more accurate
radiation treatment planning (4,36,127,128). Patients with lymphomas,
neuroblastomas and soft tissue sarcomas may benefit from PET/MRI
evaluation, which holds promise for improved oncologic applications
(36,127-130), with further studies being needed
in order to elucidate the role and the added value of this modality
in ophthalmic oncology.
14. Conclusions
The introduction of hybrid PET/CT and PET/MRI
systems into clinical practice has opened new broad horizons in
ophthalmic oncology. The challenges of managing orbital and ocular
tumors, can be addressed more effectively, through these multimodal
imaging approaches. For the detection of primary orbital and ocular
tumors, 18F-FDG PET/CT imaging does not seem to offer
additional information over clinical evaluation and conventional
anatomic imaging modalities (CT, MRI and US). However,
18F-FDG PET/CT has an established role for patients with
OL and OAL both at initial staging and post-treatment assessment.
In addition, despite contradictory data, patients with UM most
likely will have significant benefit from evaluation with
18F-FDG PET/CT for staging and follow-up. Moreover,
18F-FDG PET/CT is of utmost value for patients
presenting with intraocular or orbital metastases, and unknown
primary cancer. For the remaining set of ophthalmic tumors,
18F-FDG PET/CT seems to be of value for advanced
malignancies with an increased suspicion of regional or distant
disease dissemination. PET/CT with 18F-NaF is the
imaging modality of choice for the evaluation and monitoring of
disease activity in patients with FD of the orbital bones. Finally,
in patients with well-differentiated NETs, PET/CT using
68Ga-DOTA-compounds is the imaging technique of
reference for detecting orbital or ocular metastases. The
development of novel cancer-specific PET-tracers together with the
advent of clinical simultaneous PET/MRI systems and the employment
of artificial intelligence (AI)-based multi-modal predictive models
(130), hold promise for more
efficient personalized management strategies of ophthalmic oncology
patients.
Funding
Part of this study was financially supported by the
Stavros Niarchos Foundation within the framework of the project
ARCHERS ('Advancing Young Researchers’ Human Capital in Cutting
Edge Technologies in the Preservation of Cultural Heritage and the
Tackling of Societal Challenges’).
Availability of data and materials
Not applicable.
Authors’ contributions
GZP and MSK conceived and designed the study. GZP
and MSK researched the literature, performed analysis and
interpretation of data and drafted the manuscript. AHK, DE, ETD,
OZ, KM, CM, UB, IP, AS, IK KP, PK, GAK, DAS and AT critically
revised the article for important intellectual content, and
assisted in the literature search for this review article. All
authors agree to be accountable for all aspects of the work in
ensuring that questions related to the accuracy or integrity of any
part of the work are appropriately investigated, and finally
approved the version of the manuscript to be published. IK also
designed Fig. 1.
Ethics approval and consent to
participate
The patient images presented in Figs. 2-7
were obtained after acquiring ethics approval from the relevant
ethics committees and patient consent. The images in Figs. 2-6
were provided by the author DE, from the PET/CT department of
Evangelismos Hospital in Athens; all patients have provided written
consent forms prior to scanning. Fig.
7 was provided by esteemed physicians at the NIH, with whom the
senior and corresponding author of the article collaborates. All
study participants at the NIH clinical protocols provided all the
extensive consent forms and strict ethical approval documents that
the NIH standards require.
Patient consent for publication
Not applicable.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this article.
All the other authors declare that they have no competing
interests.
Abbreviations:
|
EFS
|
event-free survival
|
|
OS
|
overall survival
|
|
AJCC
|
American Joint Cancer Committee
|
|
SUVmax
|
maximum standardized uptake value
|
|
OL
|
orbital lymphoma
|
|
OAL
|
ocular adnexal lymphoma
|
|
NHL
|
non-Hodgkin’s lymphoma
|
|
HL
|
Hodgkin’s lymphoma
|
|
UM
|
uveal melanoma
|
|
RB
|
retinoblastoma
|
|
CM
|
conjunctival melanoma
|
|
IOP
|
inflammatory orbital pseudotumor
|
|
18F-FDG
|
18fluoride-fludeoxyglucose
|
|
GLUT-1
|
glucose transporter-1
|
|
LN
|
lymph node
|
|
US
|
ultrasonography
|
|
PET
|
positron emission tomography
|
|
CT
|
computed tomography
|
|
PET/CT
|
positron emission tomography/computed
tomography
|
|
MRI
|
magnetic resonance imaging
|
|
TNM
|
tumor-node-metastases
|
|
LFTs
|
liver function tests
|
|
PPV
|
positive predictive value
|
|
NPV
|
negative predictive value
|
|
HNSCC
|
head and neck squamous cell
carcinoma
|
|
ONG
|
optic nerve glioma
|
|
OPG
|
optic pathway glioma
|
|
NF-1
|
neurofibromatosis type 1
|
|
CRVO
|
central retinal vein occlusion
|
|
18F-FCH
|
18F-fluorocholine
|
|
11C-MET
|
11C-methionine
|
|
FD
|
fibrous dysplasia
|
|
MAS
|
McCune-Albright syndrome
|
|
SSTRs
|
somatostatin receptors
|
Acknowledgments
Not applicable.
References
|
1
|
Boellaard R, Delgado-Bolton R, Oyen WJG,
Giammarile F, Tatsch K, Eschner W, Verzijlbergen FJ, Barrington SF,
Pike LC, Weber WA; European Association of Nuclear Medicine (EANM);
et al: FDG PET/CT: EANM procedure guidelines for tumour imaging:
version 2.0. Eur J Nucl Med Mol Imaging. 42:328–354. 2015.
View Article : Google Scholar :
|
|
2
|
Pfannenberg AC, Aschoff P, Brechtel K,
Müller M, Klein M, Bares R, Claussen CD and Eschmann SM: Value of
contrast-enhanced multiphase CT in combined PET/CT protocols for
oncological imaging. Br J Radiol. 80:437–445. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bashir U, Mallia A, Stirling J, Joemon J,
MacKewn J, Charles-Edwards G, Goh V and Cook GJ: PET/MRI in
Oncological Imaging: State of the Art. Diagnostics (Basel).
5:333–357. 2015. View Article : Google Scholar
|
|
4
|
Broski SM, Goenka AH, Kemp BJ and Johnson
GB: Clinical PET/MRI: 2018 Update. AJR Am J Roentgenol.
211:295–313. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Papadakis GZ, Manikis GC, Hannah-Shmouni
F, O’Brien KJ, Gahl WA and Estrada-Veras JI: Higher metabolic
activity seen on 18F-FDG PET/CT, in the adrenal glands
of patients with Erdheim-Chester Disease harboring the BRAF V600E
mutation. Pediatr Blood Cancer. 64(Suppl): S29. 2017.
|
|
6
|
Papadakis GZ, Patronas NJ, Chen CC, Carney
JA and Stratakis CA: Combined PET/CT by 18F-FDOPA,
18F-FDA, 18F-FDG, and MRI correlation on a
patient with Carney triad. Clin Nucl Med. 40:70–72. 2015.
View Article : Google Scholar
|
|
7
|
Diker-Cohen T, Abraham SB, Rauschecker M,
Papadakis GZ, Munir KM, Brown E, Lyssikatos C, Belyavskaya E,
Merino M and Stratakis CA: Reninoma presenting in pregnancy. J Clin
Endocrinol Metab. 99:2625–2626. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Karageorgiadis AS, Papadakis GZ, Biro J,
Keil MF, Lyssikatos C, Quezado MM, Merino M, Schrump DS, Kebebew E,
Patronas NJ, et al: Ectopic adrenocorticotropic hormone and
corticotropin-releasing hormone co-secreting tumors in children and
adolescents causing cushing syndrome: A diagnostic dilemma and how
to solve it. J Clin Endocrinol Metab. 100:141–148. 2015. View Article : Google Scholar :
|
|
9
|
Hammoud DA, Boulougoura A, Papadakis GZ,
Wang J, Dodd LE, Rupert A, Higgins J, Roby G, Metzger D, Laidlaw E,
et al: Increased metabolic activity on
18F-Fluorodeoxyglucose positron emission
tomography-computed tomography in human immunodeficiency
virus-associated immune reconstitution inflammatory syndrome. Clin
Infect Dis. 68:229–238. 2019. View Article : Google Scholar
|
|
10
|
Hannah-Shmouni F, Papadakis GZ, Stratakis
CA and Blau J: Enlarging hypermetabolic nodule: Benign
non-functional adrenocortical adenoma. BMJ Case Rep.
2017:bcr20172208202017. View Article : Google Scholar
|
|
11
|
Papadakis GZ, Millo C and Stratakis CA:
Benign hormone-secreting adenoma within a larger adrenocortical
mass showing intensely increased activity on 18F-FDG
PET/CT. Endocrine. 54:269–270. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Papadakis GZ, Holland SM, Quezado M and
Patronas NJ: Adrenal cryptococcosis in an immunosuppressed patient
showing intensely increased metabolic activity on
18F-FDG PET/CT. Endocrine. 54:834–836. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Papadakis GZ, Millo C, Bagci U, Patronas
NJ and Stratakis CA: Talc pleurodesis with intense
18F-FDG activity but no 68Ga-DOTA-TATE
activity on PET/CT. Clin Nucl Med. 40:819–820. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bastawrous S, Bhargava P, Behnia F, Djang
DS and Haseley DR: Newer PET application with an old tracer: Role
of 18F-NaF skeletal PET/CT in oncologic practice.
Radiographics. 34:1295–1316. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Papadakis GZ, Jha S, Bhattacharyya T,
Millo C, Tu TW, Bagci U, Marias K, Karantanas AH and Patronas NJ:
18F-NaF PET/CT in extensive melorheostosis of the axial
and appendicular Skeleton With Soft-Tissue Involvement. Clin Nucl
Med. 42:537–539. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Papadakis GZ, Jha S, Karantanas AH, Marias
K, Bagci U and Bhattacharyya T: Prospective evaluation of the
application of 18F-NaF PET/CT imaging in melorheostosis.
Eur J Nucl Med Mol Imaging. 45(Suppl 1): S231–S232. 2018.
|
|
17
|
Papadakis GZ, Millo C, Bagci U, Blau J and
Collins MT: 18F-NaF and 18F-FDG PET/CT in
Gorham-Stout Disease. Clin Nucl Med. 41:884–885. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Papadakis GZ, Millo C, Bagci U, Patronas
NJ and Collins MT: Value of 18F-NaF PET/CT imaging in
the assessment of Gorham-Stout disease activity. Eur J Nucl Med Mol
Imaging. 43(Suppl 1): S597. 2016. View Article : Google Scholar
|
|
19
|
Hofman MS, Lau WF and Hicks RJ:
Somatostatin receptor imaging with 68Ga DOTATATE PET/CT:
Clinical utility, normal patterns, pearls, and pitfalls in
interpretation. Radiographics. 35:500–516. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tirosh A, Papadakis GZ, Millo C, Hammoud
D, Sadowski SM, Herscovitch P, Pacak K, Marx SJ, Yang L, Nockel P,
et al: Prognostic utility of total 68Ga-DOTATATE-avid
tumor volume in patients with neuroendocrine tumors.
Gastroenterology. 154:998–1008.e1. 2018. View Article : Google Scholar
|
|
21
|
Tirosh A, Papadakis GZ, Millo C, Sadowski
SM, Herscovitch P, Pacak K, Marx SJ, Yang L, Nockel P, Shell J, et
al: Association between neuroendocrine tumors biomarkers and
primary tumor site and disease type based on total
68Ga-DOTATATE-Avid tumor volume measurements. Eur J
Endocrinol. 176:575–582. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Papadakis GZ, Millo C, Sadowski SM,
Karantanas AH, Bagci U and Patronas NJ: Fibrous Dysplasia Mimicking
Malignancy on 68Ga-DOTATATE PET/CT. Clin Nucl Med.
42:209–210. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Papadakis GZ, Sadowski SM, Bagci U and
Millo C: Application of 68Ga-DOTA-TATE PET/CT in
metastatic neuroendocrine tumor of gastrointestinal origin. Ann
Gastroenterol. 30:1302017.
|
|
24
|
Papadakis GZ, Millo C, Jassel IS, Bagci U,
Sadowski SM, Karantanas AH and Patronas NJ: 18F-FDG and
68Ga-DOTATATE PET/CT in von Hippel-Lindau
disease-associated retinal heman-gioblastoma. Clin Nucl Med.
42:189–190. 2017. View Article : Google Scholar
|
|
25
|
Papadakis GZ, Millo C, Karantanas AH,
Bagci U and Patronas NJ: Avascular necrosis of the hips with
increased activity on 68Ga-DOTATATE PET/CT. Clin Nucl
Med. 42:214–215. 2017. View Article : Google Scholar :
|
|
26
|
Papadakis GZ, Millo C, Sadowski SM,
Karantanas AH, Bagci U and Patronas NJ: Breast fibroadenoma with
increased activity on 68Ga DOTATATE PET/CT. Clin Nucl
Med. 42:145–146. 2017. View Article : Google Scholar :
|
|
27
|
Papadakis GZ, Millo C, Sadowski SM, Bagci
U and Patronas NJ: Kidney Tumor in a von Hippel-Lindau (VHL)
patient with intensely increased activity on
68Ga-DOTA-TATE PET/CT. Clin Nucl Med. 41:970–971. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
El-Maouche D, Sadowski SM, Papadakis GZ,
Guthrie L, Cottle-Delisle C, Merkel R, Millo C, Chen CC, Kebebew E
and Collins MT: 68Ga-DOTATATE for tumor localization in
tumor-induced osteomalacia. J Clin Endocrinol Metab. 101:3575–3581.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Papadakis GZ, Millo C, Sadowski SM, Bagci
U and Patronas NJ: Epididymal cystadenomas in von Hippel-Lindau
disease showing increased activity on 68Ga DOTATATE
PET/CT. Clin Nucl Med. 41:781–782. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Papadakis GZ, Millo C, Sadowski SM, Bagci
U and Patronas NJ: Endolymphatic sac tumor showing increased
activity on 68Ga-DOTATATE PET/CT. Clin Nucl Med.
41:783–784. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Papadakis GZ, Millo C, Bagci U, Sadowski
SM and Stratakis CA: Schmorl nodes can cause increased
68Ga-DOTATATE activity on PET/CT, mimicking metastasis
in patients with neuroendocrine malignancy. Clin Nucl Med.
41:249–250. 2016. View Article : Google Scholar :
|
|
32
|
Papadakis GZ, Bagci U, Sadowski SM,
Patronas NJ and Stratakis CA: Ectopic ACTH and CRH co-secreting
tumor localized by 68Ga-DOTA-TATE PET/CT. Clin Nucl Med.
40:576–578. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Tirosh A, Papadakis GZ, Millo C, Sadowski
SM, Herscovitch P, Pacak K, Marx SJ, Yang L, Nockel P, Shell J, et
al: High total 68Ga-DOTATATE-Avid Tumor Volume (TV) is
associated with low progression-free survival and high
disease-specific mortality rate in patients with neuroendocrine
tumors. Endocrine Abstracts. 49:OC7.32017.
|
|
34
|
Honavar SG and Manjandavida FP: Recent
Advances in Orbital Tumors - A Review of Publications from
2014-2016. Asia Pac J Ophthalmol (Phila). 6:153–158. 2017.
|
|
35
|
Hui KH, Pfeiffer ML and Esmaeli B: Value
of positron emission tomography/computed tomography in diagnosis
and staging of primary ocular and orbital tumors. Saudi J
Ophthalmol. 26:365–371. 2012. View Article : Google Scholar
|
|
36
|
Purohit BS, Vargas MI, Ailianou A, Merlini
L, Poletti PA, Platon A, Delattre BM, Rager O, Burkhardt K and
Becker M: Orbital tumours and tumour-like lesions: Exploring the
arma-mentarium of multiparametric imaging. Insights Imaging.
7:43–68. 2016. View Article : Google Scholar
|
|
37
|
English JF and Sullivan TJ: The Role of
FDG-PET in the diagnosis and staging of ocular adnexal
lymphoproliferative disease. Orbit. 34:284–291. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Valenzuela AA, Allen C, Grimes D, Wong D
and Sullivan TJ: Positron emission tomography in the detection and
staging of ocular adnexal lymphoproliferative disease.
Ophthalmology. 113:2331–2337. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Roe RH, Finger PT, Kurli M, Tena LB and
Iacob CE: Whole-body positron emission tomography/computed
tomography imaging and staging of orbital lymphoma. Ophthalmology.
113:1854–1858. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Suga K, Yasuhiko K, Hiyama A, Takeda K and
Matsunaga N: 18F-FDG PET/CT findings in a patient with
bilateral orbital and gastric mucosa-associated lymphoid tissue
lymphomas. Clin Nucl Med. 34:589–593. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Gayed I, Eskandari MF, McLaughlin P, Pro
B, Diba R and Esmaeli B: Value of positron emission tomography in
staging ocular adnexal lymphomas and evaluating their response to
therapy. Ophthalmic Surg Lasers Imaging. 38:319–325. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Sallak A, Besson FL, Pomoni A, Christinat
A, Adler M, Aegerter JP, Nguyen C, de Leval L, Frossard V and Prior
JO: Conjunctival MALT lymphoma: Utility of FDG PET/CT for
diagnosis, staging, and evaluation of treatment response. Clin Nucl
Med. 39:295–297. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Yildirim-Poyraz N, Ozdemir E, Basturk A,
Kilicarslan A and Turkolmez S: PET/CT findings in a case with
FDG-avid disseminated lacrimal gland MALToma with sequential
development of large B-cell lymphoma and gastric MALToma. Clin Nucl
Med. 40:141–145. 2015. View Article : Google Scholar
|
|
44
|
Fujii H, Tanaka H, Nomoto Y, Harata N,
Oota S, Isogai J and Yoshida K: Usefulness of 18F-FDG
PET/CT for evaluating response of ocular adnexal lymphoma to
treatment. Medicine (Baltimore). 97:e05432018. View Article : Google Scholar
|
|
45
|
Hu DN, Yu GP, McCormick SA, Schneider S
and Finger PT: Population-based incidence of uveal melanoma in
various races and ethnic groups. Am J Ophthalmol. 140:612–617.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Singh AD, Turell ME and Topham AK: Uveal
melanoma: Trends in incidence, treatment, and survival.
Ophthalmology. 118:1881–1885. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Finger PT, Kurli M, Wesley P, Tena L, Kerr
KR and Pavlick A: Whole body PET/CT imaging for detection of
metastatic choroidal melanoma. Br J Ophthalmol. 88:1095–1097. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Reddy S, Kurli M, Tena LB and Finger PT:
PET/CT imaging: Detection of choroidal melanoma. Br J Ophthalmol.
89:1265–1269. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Finger PT, Chin K and Iacob CE:
18-Fluorine-labelled 2 - deoxy-2 -fluoro - D – glucose positron
emission tomography/computed tomography standardised uptake values:
A non-invasive biomarker for the risk of metastasis from choroidal
melanoma. Br J Ophthalmol. 90:1263–1266. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Matsuo T, Ogino Y, Ichimura K, Tanaka T
and Kaji M: Clinicopathological correlation for the role of
fluorodeoxy-glucose positron emission tomography computed
tomography in detection of choroidal malignant melanoma. Int J Clin
Oncol. 19:230–239. 2014. View Article : Google Scholar
|
|
51
|
McCannel TA, Reddy S, Burgess BL and
Auerbach M: Association of positive dual-modality positron emission
tomography/computed tomography imaging of primary choroidal
melanoma with chromosome 3 loss and tumor size. Retina. 30:146–151.
2010. View Article : Google Scholar
|
|
52
|
Papastefanou VP, Islam S, Szyszko T,
Grantham M, Sagoo MS and Cohen VML: Metabolic activity of primary
uveal melanoma on PET/CT scan and its relationship with monosomy 3
and other prognostic factors. Br J Ophthalmol. 98:1659–1665. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Kurli M, Reddy S, Tena LB, Pavlick AC and
Finger PT: Whole body positron emission tomography/computed
tomography staging of metastatic choroidal melanoma. Am J
Ophthalmol. 140:193–199. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Freton A, Chin KJ, Raut R, Tena LB, Kivelä
T and Finger PT: Initial PET/CT staging for choroidal melanoma:
AJCC correlation and second nonocular primaries in 333 patients.
Eur J Ophthalmol. 22:236–243. 2012. View Article : Google Scholar
|
|
55
|
Strobel K, Bode B, Dummer R, Veit-Haibach
P, Fischer DR, Imhof L, Goldinger S, Steinert HC and von Schulthess
GK: Limited value of 18F-FDG PET/CT and S-100B tumour
marker in the detection of liver metastases from uveal melanoma
compared to liver metastases from cutaneous melanoma. Eur J Nucl
Med Mol Imaging. 36:1774–1782. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Orcurto V, Denys A, Voelter V,
Schalenbourg A, Schnyder P, Zografos L, Leyvraz S, Delaloye AB and
Prior JO: (18) F-fluorodeoxyglucose positron emission
tomography/computed tomography and magnetic resonance imaging in
patients with liver metastases from uveal melanoma: Results from a
pilot study. Melanoma Res. 22:63–69. 2012. View Article : Google Scholar
|
|
57
|
Ries LAG, Smith MA, Gurney JG, Linet M,
Tamra T, Young JL and Bunin GR: Cancer incidence and survival among
children and adolescents: United States SEER program 1975-1995.
(NIH Pub No 99-4649). National Cancer Institute; Bethesda, MD:
1999
|
|
58
|
Jakobiec FA, Tso MO, Zimmerman LE and
Danis P: Retinoblastoma and intracranial malignancy. Cancer.
39:2048–2058. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
de Jong MC, Kors WA, de Graaf P,
Castelijns JA, Kivelä T and Moll AC: Trilateral retinoblastoma: A
systematic review and meta-analysis. Lancet Oncol. 15:1157–1167.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Kamihara J, Bourdeaut F, Foulkes WD,
Molenaar JJ, Mossé YP, Nakagawara A, Parareda A, Scollon SR,
Schneider KW, Skalet AH, et al: Retinoblastoma and Neuroblastoma
Predisposition and Surveillance. Clin Cancer Res. 23:e98-e1062017.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Yamanaka R, Hayano A and Takashima Y:
Trilateral retinoblastoma: A systematic review of 211 cases.
Neurosurg Rev. 42:39–48. 2019. View Article : Google Scholar
|
|
62
|
Honavar SG, Manjandavida FP and Reddy VAP:
Orbital retinoblastoma: An update. Indian J Ophthalmol. 65:435–442.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Radhakrishnan V, Kumar R, Malhotra A and
Bakhshi S: Role of PET/CT in staging and evaluation of treatment
response after 3 cycles of chemotherapy in locally advanced
retinoblastoma: A prospective study. J Nucl Med. 53:191–198. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Yu GP, Hu DN, McCormick S and Finger PT:
Conjunctival melanoma: Is it increasing in the United States? Am J
Ophthalmol. 135:800–806. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Folberg R, McLean IW and Zimmerman LE:
Malignant melanoma of the conjunctiva. Hum Pathol. 16:136–143.
1985. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Damian A, Gaudiano J, Engler H and Alonso
O: (18)F-FDG PET-CT for Staging of Conjunctival Melanoma. World J
Nucl Med. 12:45–47. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Tuomaala S and Kivelä T: Metastatic
pattern and survival in disseminated conjunctival melanoma:
Implications for sentinel lymph node biopsy. Ophthalmology.
111:816–821. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Kurli M, Chin K and Finger PT: Whole-body
18 FDG PET/CT imaging for lymph node and metastatic staging of
conjunctival melanoma. Br J Ophthalmol. 92:479–482. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Tsai SY, Shiau YC, Wang SY and Wu YW:
Conjunctival Melanoma on 18F-FDG PET/CT as a Second
Primary Cancer. Clin Nucl Med. 41:237–238. 2016. View Article : Google Scholar
|
|
70
|
Muqit MM, Foot B, Walters SJ, Mudhar HS,
Roberts F and Rennie IG: Observational prospective cohort study of
patients with newly-diagnosed ocular sebaceous carcinoma. Br J
Ophthalmol. 97:47–51. 2013. View Article : Google Scholar
|
|
71
|
Yin VT, Merritt HA, Sniegowski M and
Esmaeli B: Eyelid and ocular surface carcinoma: Diagnosis and
management. Clin Dermatol. 33:159–169. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Shields JA, Demirci H, Marr BP, Eagle RC
Jr and Shields CL: Sebaceous carcinoma of the eyelids: Personal
experience with 60 cases. Ophthalmology. 111:2151–2157. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Baek CH, Chung MK, Jeong HS, Son YI, Choi
J, Kim YD, Choi JY, Kim HJ and Ko YH: The clinical usefulness of
(18) F-FDG PET/CT for the evaluation of lymph node metastasis in
periorbital malignancies. Korean J Radiol. 10:1–7. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Krishna SM, Finger PT, Chin K and Lacob
CE: 18-FDG PET/CT staging of ocular sebaceous cell carcinoma.
Graefes Arch Clin Exp Ophthalmol. 245:759–760. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Ishiguro Y, Homma S, Yoshida T, Ohno Y,
Ichikawa N, Kawamura H, Hata H, Kase S, Ishida S, Okada-Kanno H, et
al: Usefulness of PET/CT for early detection of internal
malignancies in patients with Muir-Torre syndrome: Report of two
cases. Surg Case Rep. 3:712017. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Faustina M, Diba R, Ahmadi MA and Esmaeli
B: Patterns of regional and distant metastasis in patients with
eyelid and peri-ocular squamous cell carcinoma. Ophthalmology.
111:1930–1932. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Donaldson MJ, Sullivan TJ, Whitehead KJ
and Williamson RM: Squamous cell carcinoma of the eyelids. Br J
Ophthalmol. 86:1161–1165. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Soysal HG and Markoç F: Invasive squamous
cell carcinoma of the eyelids and periorbital region. Br J
Ophthalmol. 91:325–329. 2007. View Article : Google Scholar
|
|
79
|
Reifler DM and Hornblass A: Squamous cell
carcinoma of the eyelid. Surv Ophthalmol. 30:349–365. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Yi JS, Kim JS, Lee JH, Choi SH, Nam SY,
Kim SY and Roh JL: 18F-FDG PET/CT for detecting distant
metastases in patients with recurrent head and neck squamous cell
carcinoma. J Surg Oncol. 106:708–712. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Lin LF, Chang CY and Cherng SC: Advanced
squamous cell carcinoma of the bulbar conjunctiva seen on PET/CT.
Clin Nucl Med. 33:929–930. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Abdelmalik AG, Fajnwaks P, Osman MM and
Nguyen NC: Squamous cell carcinoma of the bulbar conjunctiva seen
on F-18 FDG PET/CT. Clin Nucl Med. 35:962–964. 2010. View Article : Google Scholar
|
|
83
|
Jurdy L, Merks JHM, Pieters BR, Mourits
MP, Kloos RJ, Strackee SD and Saeed P: Orbital rhabdomyosarcomas: A
review. Saudi J Ophthalmol. 27:167–175. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Norman G, Fayter D, Lewis-Light K,
Chisholm J, McHugh K, Levine D, Jenney M, Mandeville H, Gatz S and
Phillips B: An emerging evidence base for PET-CT in the management
of childhood rhabdomyosarcoma: Systematic review. BMJ Open.
5:e0060302015. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Harrison DJ, Parisi MT and Shulkin BL: The
Role of 18F-FDG-PET/CT in Pediatric Sarcoma. Semin Nucl
Med. 47:229–241. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Teixeira SR, Martinez-Rios C, Hu L and
Bangert BA: Clinical applications of pediatric positron emission
tomography-magnetic resonance imaging. Semin Roentgenol.
49:353–366. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Nair AG, Pathak RS, Iyer VR and Gandhi RA:
Optic nerve glioma: An update. Int Ophthalmol. 34:999–1005. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Becker M, Masterson K, Delavelle J,
Viallon M, Vargas MI and Becker CD: Imaging of the optic nerve. Eur
J Radiol. 74:299–313. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Campen CJ and Gutmann DH: Optic Pathway
Gliomas in Neurofibromatosis Type 1. J Child Neurol. 33:73–81.
2018. View Article : Google Scholar
|
|
90
|
Miyamoto J, Sasajima H, Owada K and
Mineura K: Surgical decision for adult optic glioma based on
[18F]fluorodeoxy-glucose positron emission tomography study. Neurol
Med Chir (Tokyo). 46:500–503. 2006. View Article : Google Scholar
|
|
91
|
Peng F, Juhasz C, Bhambhani K, Wu D,
Chugani DC and Chugani HT: Assessment of progression and treatment
response of optic pathway glioma with positron emission tomography
using alpha-[(11)C]methyl-L-tryptophan. Mol Imaging Biol.
9:106–109. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Moharir M, London K, Howman-Giles R and
North K: Utility of positron emission tomography for tumour
surveillance in children with neurofibromatosis type 1. Eur J Nucl
Med Mol Imaging. 37:1309–1317. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Roselli F, Pisciotta NM, Aniello MS,
Niccoli-Asabella A, Defazio G, Livrea P and Rubini G: Brain F-18
Fluorocholine PET/CT for the assessment of optic pathway glioma in
neurofi-bromatosis-1. Clin Nucl Med. 35:838–839. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Rizzo V, Mattoli MV, Trevisi G, Coli A,
Calcagni ML and Montano N: Optic nerve glioblastoma detected by
11C-Methionine brain PET/CT. Rev Esp Med Nucl Imagen
Mol. 37:259–260. 2018.
|
|
95
|
Nakajima R, Kimura K, Abe K and Sakai S:
11C-methionine PET/CT findings in benign brain disease.
Jpn J Radiol. 35:279–288. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Konstantinidis L and Damato B: Intraocular
Metastases - A Review. Asia Pac J Ophthalmol (Phila). 6:208–214.
2017.
|
|
97
|
Konstantinidis L, Rospond-Kubiak I,
Zeolite I, Heimann H, Groenewald C, Coupland SE and Damato B:
Management of patients with uveal metastases at the Liverpool
Ocular Oncology Centre. Br J Ophthalmol. 98:92–98. 2014. View Article : Google Scholar
|
|
98
|
Donaldson MJ, Pulido JS, Mullan BP,
Inwards DJ, Cantrill H, Johnson MR and Han MK: Combined positron
emission tomography/computed tomography for evaluation of presumed
choroidal metastases. Clin Exp Ophthalmol. 34:846–851. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Shields JA, Shields CL and Scartozzi R:
Survey of 1264 patients with orbital tumors and simulating lesions:
The 2002 Montgomery Lecture, part 1. Ophthalmology. 111:997–1008.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Valenzuela AA, Archibald CW, Fleming B,
Ong L, O’Donnell B, Crompton JJ, Selva D, McNab AA and Sullivan TJ:
Orbital metastasis: Clinical features, management and outcome.
Orbit. 28:153–159. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Das S, Pineda G, Goff L, Sobel R, Berlin J
and Fisher G: The eye of the beholder: Orbital metastases from
midgut neuroendocrine tumors, a two institution experience. Cancer
Imaging. 18:472018. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Ding ZX, Lip G and Chong V: Idiopathic
orbital pseudotumour. Clin Radiol. 66:886–892. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Weber AL, Romo LV and Sabates NR:
Pseudotumor of the orbit. Clinical, pathologic, and radiologic
evaluation. Radiol Clin North Am. 37:151–168. xi1999. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Pakdaman MN, Sepahdari AR and Elkhamary
SM: Orbital inflammatory disease: Pictorial review and differential
diagnosis. World J Radiol. 6:106–115. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Patnana M, Sevrukov AB, Elsayes KM,
Viswanathan C, Lubner M and Menias CO: Inflammatory pseudotumor:
The great mimicker. AJR Am J Roentgenol. 198:W217–27. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Alongi F, Bolognesi A, Samanes Gajate AM,
Motta M, Landoni C, Berardi G, Alongi P, Gianolli L and Di Muzio N:
Inflammatory pseudotumor of mediastinum treated with tomotherapy
and monitored with FDG-PET/CT: Case report and literature review.
Tumori. 96:322–326. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Boyce AM, Florenzano P, de Castro LF,
Collins MT, Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH,
Stephens K and Amemiya A: Fibrous Dysplasia/McCune-Albright
Syndrome In: GeneReviews® [Internet]. University of
Washington; Seattle, WA: 1993-2019
|
|
108
|
Collins MT, Kushner H, Reynolds JC, Chebli
C, Kelly MH, Gupta A, Brillante B, Leet AI, Riminucci M, Robey PG,
et al: An instrument to measure skeletal burden and predict
functional outcome in fibrous dysplasia of bone. J Bone Miner Res.
20:219–226. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Toba M, Hayashida K, Imakita S, Fukuchi K,
Kume N, Shimotsu Y, Cho I, Ishida Y, Takamiya M and Kumita S:
Increased bone mineral turnover without increased glucose
utilization in sclerotic and hyperplastic change in fibrous
dysplasia. Ann Nucl Med. 12:153–155. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Shigesawa T, Sugawara Y, Shinohara I,
Fujii T, Mochizuki T and Morishige I: Bone metastasis detected by
FDG PET in a patient with breast cancer and fibrous dysplasia. Clin
Nucl Med. 30:571–573. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Stegger L, Juergens KU, Kliesch S,
Wormanns D and Weckesser M: Unexpected finding of elevated glucose
uptake in fibrous dysplasia mimicking malignancy: Contradicting
metabolism and morphology in combined PET/CT. Eur Radiol.
17:1784–1786. 2007. View Article : Google Scholar
|
|
112
|
Su MG, Tian R, Fan QP, Tian Y, Li FL, Li
L, Kuang AR and Miller JH: Recognition of fibrous dysplasia of bone
mimicking skeletal metastasis on 18F-FDG PET/CT imaging.
Skeletal Radiol. 40:295–302. 2011. View Article : Google Scholar
|
|
113
|
D’Souza MM, Jaimini A, Khurana A, Tripathi
M, Sharma R, Mondal A and Srivastava M: Polyostotic fibrous
dysplasia on F-18 FDG PET/CT imaging. Clin Nucl Med. 34:359–361.
2009. View Article : Google Scholar
|
|
114
|
Kim M, Kim HS, Kim JH, Jang JH, Chung KJ,
Shin MK, Hwang HS, Kim BC and Jung SY: F-18 FDG PET-positive
fibrous dysplasia in a patient with intestinal non-Hodgkin’s
lymphoma. Cancer Res Treat. 41:171–174. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Choi YY, Kim JY and Yang SO: PET/CT in
benign and malignant musculoskeletal tumors and tumor-like
conditions. Semin Musculoskelet Radiol. 18:133–148. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Kamaleshwaran KK, Joseph J, Kalarikal R
and Shinto AS: Image Findings of Polyostotic Fibrous Dysplasia
Mimicking Metastasis in F-18 FDG Positron Emission
Tomography/Computed Tomography. Indian J Nucl Med. 32:137–139.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Ruggieri P, Sim FH, Bond JR and Unni KK:
Malignancies in fibrous dysplasia. Cancer. 73:1411–1424. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Wei WJ, Sun ZK, Shen CT, Zhang XY, Tang J,
Song HJ, Qiu ZL and Luo QY: Value of 99mTc-MDP SPECT/CT
and 18F-FDG PET/CT scanning in the evaluation of
malignantly transformed fibrous dysplasia. Am J Nucl Med Mol
Imaging. 7:92–104. 2017.
|
|
119
|
Chen CC, Czerwiec FS and Feuillan PP:
Visualization of fibrous dysplasia during somatostatin receptor
scintigraphy. J Nucl Med. 39:238–240. 1998.PubMed/NCBI
|
|
120
|
Papadakis GZ, Manikis GC, Karantanas AH,
Florenzano P, Bagci U, Marias K, Collins MT and Boyce AM:
18F-NaF PET/CT imaging in fibrous dysplasia of bone. J
Bone Miner Res. 34:1619–1631. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Papadakis G, Manikis G, Karantanas A,
Marias K, Bagci U, Florenzano P, Collins M and Boyce A: Fibrous
dysplasia related 18F-NaF activity in the spine is
significantly higher in patients with scoliosis, compared to
patients without spinal deformity. J Nucl Med. 60(Suppl 1): 1298S.
2019.
|
|
122
|
Papadakis G, Manikis G, Karantanas A,
Marias K, Bagci U, Florenzano P, Collins M and Boyce A: Positive
Association between Fibrous Dysplasia (FD) related
18F-NaF activity and Bone Turnover Markers (BTMs). J
Nucl Med. 60(Suppl 1): 90S. 2019.
|
|
123
|
Papadakis G, Manikis G, Karantanas A,
Marias K, Collins M and Boyce A: Application of 18F-NaF
PET/CT imaging in prognosis of fractures and treatment planning in
patients with fibrous dysplasia. J Nucl Med. 58(Suppl 1): 308S.
2017.
|
|
124
|
Papadakis GZ, Manikis GC, Karantanas AH,
Marias K, Collins MT and Boyce AM: Application of
18F-NaF PET/CT imaging in fibrous dysplasia. Horm Res
Paediatr. 88(Suppl 1): 20. 2017.
|
|
125
|
Delso G, Fürst S, Jakoby B, Ladebeck R,
Ganter C, Nekolla SG, Schwaiger M and Ziegler SI: Performance
measurements of the Siemens mMR integrated whole-body PET/MR
scanner. J Nucl Med. 52:1914–1922. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Levin CS, Maramraju SH, Khalighi MM,
Deller TW, Delso G and Jansen F: Design features and mu-tual
compatibility studies of the time-of-flight PET capable GE SIGNA
PET/MR system. IEEE Trans Med Imaging. 35:1907–1914. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Partovi S, Kohan A, Rubbert C,
Vercher-Conejero JL, Gaeta C, Yuh R, Zipp L, Herrmann KA, Robbin
MR, Lee Z, et al: Clinical oncologic applications of PET/MRI: A new
horizon. Am J Nucl Med Mol Imaging. 4:202–212. 2014.PubMed/NCBI
|
|
128
|
Varoquaux A, Rager O, Poncet A, Delattre
BM, Ratib O, Becker CD, Dulguerov P, Dulguerov N, Zaidi H and
Becker M: Detection and quantification of focal uptake in head and
neck tumours: (18)F-FDG PET/MR versus PET/CT. Eur J Nucl Med Mol
Imaging. 41:462–475. 2014. View Article : Google Scholar
|
|
129
|
Platzek I, Beuthien-Baumann B, Langner J,
Popp M, Schramm G, Ordemann R, Laniado M, Kotzerke J and van den
Hoff J: PET/MR for therapy response evaluation in malignant
lymphoma: Initial experience. MAGMA. 26:49–55. 2013. View Article : Google Scholar :
|
|
130
|
Papadakis GZ, Karantanas AH, Tsiknakis M,
Tsatsakis A, Spandidos DA and Marias K: Deep learning opens new
horizons in personalized medicine. Biomed Rep. 10:215–217.
2019.PubMed/NCBI
|