Introduction
Hand, foot and mouth disease (HFMD) is generally a
benign and common self-limiting childhood illness characterized by
fever and vesicular eruption on the hands and feet and in the
mouth. This disease can be caused by several enterovirus serotypes,
such as coxsackievirus A2, A4, A5, A8, A10, A16 and enterovirus 71
(EV71) (1,2). Of these, coxsackievirus A16 (CVA16)
and human EV71 are the major etiologic agents of HFMD. The clinical
features of HFMD caused by these two viruses are indistinguishable,
but EV71 infection is associated to a greater extent with severe
neurological disease and fatalities (3–5). In
contrast, CVA16-associated HFMD has a milder outcome, with much
lower incidence of neurological disease (6).
EV71 has been classified into three genotypes
(A,B,C) and divided into 10 subgenotypes (A, B1-B5, C1-C5) based on
the complete VP1 gene over a 40-year period and different
geographical distribution (7–9).
Although a small number of studies have focused on the molecular
characteristics of CVA16, CVA16 has been classified into two
genotypes (A and B) based on the VP1 gene. The B genotype can be
divided into B1 and B2 subtypes, and subtype B2 is known to contain
clusters B2a and B2b (10–13). Whereas identification of the
genotypes or subgenotypes of CVA16 and EV71 has been used to reveal
the origins of virus in HFMD outbreaks, (9,10)
the relationship between the genotype of CVA16 and EV71 and their
geographical distribution has not been previously investigated.
In this study, we analyzed the genetic
characteristics of the partial VP1 gene of CVA16 and EV71 strains
in China using phylogenetic analysis, and we specifically aimed to
evaluate the relationship between genotype and geographical
epidemics.
Materials and methods
Clinical specimens, sample processing,
RNA extraction
A total of 399 stool specimens were obtained with
informed consent from children with signs of HFMD, including a
brief febrile illness and typical vesicular rashes on the palms and
soles in Zhejiang Province between May and August 2010. We
collected these specimens from the Pediatrics Department of The
First Affiliated Hospital, School of Medicine, Zhejiang University
(Hangzhou, China). Stool samples were immediately stored at −80˚C
until further analysis. Before commencement of this study, the
project was approved by the Ethics Committee of the First
Affiliated Hospital, College of Medicine, Zhejiang University.
A 10% stool suspension was made by adding 0.5 g of
stool (0.5 ml for fluid stools) to 5 ml of 1% phosphate-buffered
saline. The suspension was centrifuged at 12.000 × g for 10 min and
filtered, and then subsequently processed. Vial RNA extraction was
carried out using a high Pure Viral RNA kit (Roche Applied Science,
Mannheim, Germany) according to the manufacturer's procedures and
stored at −80˚C until further analysis.
Reverse transcription-semi-nested PCR and
sequencing
Reverse transcription-semi-nested PCR amplification
was performed using a set of primers for the VP1 gene as described
previously (14). Briefly, the
992-bp fragment encompassing the VP3 and VP1 gene was firstly
amplified with degenerate primers (AN32, AN33, AN34, AN35 and 224,
222). First round PCR condition was subjected to an initial cycle
for reverse transcription at 50˚C for 30 min and the following
cycling conditions: 94˚C for 10 min, 40 cycles of 94˚C for 30 sec,
42˚C for 30 sec and 60˚C for 1 min followed by a final extension at
72˚C for 4 min. Nested PCR was performed using 1 μl of the
first-round product as template, with the primers AN88
(5′-TACTGGACCACCTGGNGGNAYRWACAT-3′) and AN89
(5′-CCAGCACTGACAGCAGYNGARAYNGG-3′). Nested PCR was subjected to an
initial cycle of 95˚C for 4 min and 30 cycles (95˚C for 30 sec,
60˚C for 20 sec and 72˚C for 15 sec), followed by a final
incubation at 72˚C for 4 min. RT-semi-nested PCR resulted in a 350-
to 400-bp fragment of the VP1 gene. The water was included as
negative control for the first and second round PCR. All reactions
were performed in a Bio-Rad Thermal cycler (Bio-Rad, Hercules, CA,
USA) with thin-walled reaction tubes. Five microliters of the
nested PCR products was run on 1% agarose gel made with Tris-boric
acid-EDTA (TBE) buffered and strained with ethidium bromide (0.5
μg/ml). For sequencing, PCR products of the appropriate size that
produced visible bands upon UV illumination were purified from the
gel using QIAquick gel extraction kit (Qiagen) and directly
sequenced by an automated DNA sequence analyzer (Applied Biosystem,
Carlsbad, CA, USA). Sequences obtained were compared pairwise with
the enterovirus sequences available in GeneBank (http://www.ncbi.nlm.nih.gov/blast).
Phylogenetic analysis
Clustal W program was applied for multiple sequence
alignment. The dendrograms were constructed by the neighbor-joining
method in the MEGA program. The reliability of neighbor-joining
tree was estimated by bootstrap analysis with 1.000 pseudoreplicate
data sets. Genetic distances were calculated with the Kimura
2-parameter model nucleotide substitution (15).
Results
To determine the prevalence of HFMD in Zhejiang
Province, 399 stool specimens from children with typical symptoms
of fever and vesicular eruption on the palms and soles were
obtained and examined with reverse transcription-semi-nested PCR
approach adopted by Nix et al (14). We found that 35% (139/399) of the
specimens were positive for enterovirus. Of the children with
positive specimens, the ages ranged from 11 months to 6 years, with
a mean age being 2.3 years. There were 75 boys and 64 girls, for a
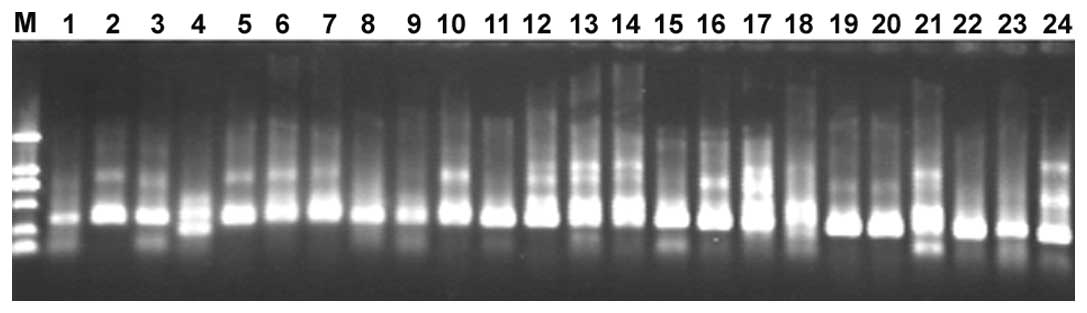
male to female ratio of 1.2–1. RT-semi-nested PCR products
targeting the 350–400 bp (Fig. 1)
fragment of the VP1 gene of 139 enterovirus-positive samples were
directly sequenced and 99 sequences were obtained. All 99 sequences
were assigned to 7 serotypes within the HEV-A species by comparing
them with all enterovirus sequences in the GenBank database. EV71
and CVA16 were the frequently detected serotypes, accounting for
38.4% (38/99) and 35.4% (35/99) respectively, in the HEV-A
species-positive cases. Other serotypes were responsible for the
remaining 26.2%.
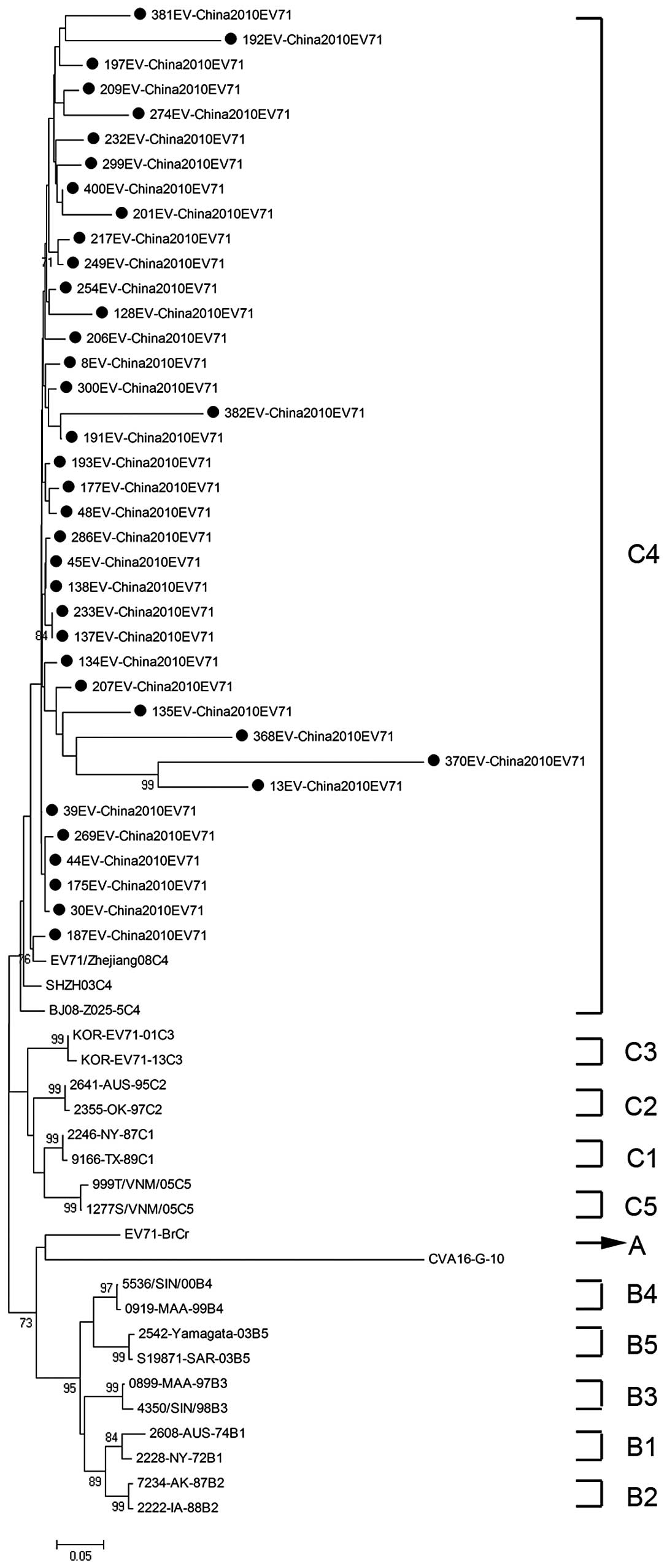
To determine the genetic characteristics of EV71 and
CVA16 strains circulating in their geographic location,
phylogenetic analysis of these strains was based on the alignment
of partial VP1 gene sequences. A total of 61 EV71 strains were used
for phylogenetic analysis of the VP1 gene including the 38 EV71
strains identified in this study, 3 EV71 strains from 3 provinces
in mainland China, and 20 international EV71 strains that
represented all 11 known genotypes or subgenotypes (A, B1-B5,
C1-C5) available from the GenBank (Fig. 2). All 38 EV71 strains from Zhejiang
Province belonged to the subgenotype C4, which was similar to EV71
sequences isolated from 3 provinces in mainland China.
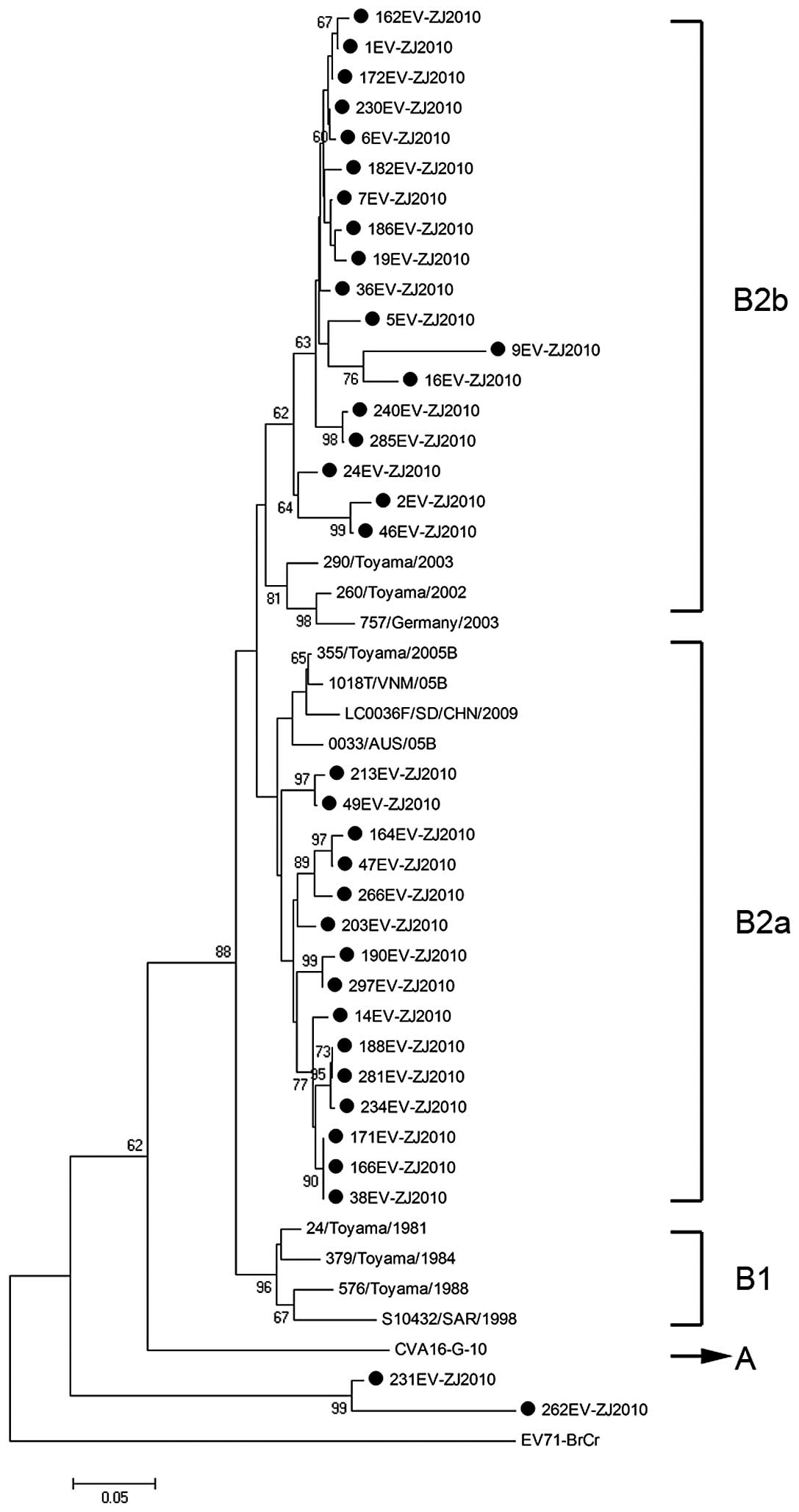
We performed a similar analysis of the CVA16
detection in this study. A total of 46 CAV16 strains were used for
phylogenetic analysis for the VP1 gene, including the 35 CAV16
strains identified in this study and 11 other CAV16 strains
available from the GenBank (Fig.
3). It shows that 33 out of the 35 identified strains herein
belong to clusters B2a and B2b which were found to be the prevalent
viruses circulating in China and in neighboring countries and
regions. However, the remaining 2 CAV16 strains could not be
classified and formed a cluster distinct from genotype A and B.
Discussion
In the present study, we investigated the prevalence
of HFMD in Zhejiang Province between May and August 2010, and found
that EV71 and CVA16 were the major etiological pathogens. Although
there were no deaths caused by HFMD in the present study,
EV71-related deaths from encephalitis, pulmonary edema and
hemorrhage, have been previously noted (4,16,17),
and fatal CVA16 infections have also been described in children
with myocarditis (3) and in an
adult with pneumonitis (18).
Therefore, the identification of the major causal pathogen of HFMD
is imperative.
Based on a study of molecular characteristics of the
VP1 gene by Brown et al, 3 genotypes of EV71 (A, B, C) were
identified (9). The EV71 prototype
strain (BrCr-CA-70) isolated in California in 1970, is the sole
member of the genotype A (4). At
present, the B genotype is known to contain 5 subgenotypes (B1-B5),
and the C genotype is known to contain another 5 subgenotypes
(C1-C5). The genotype B was predominant in the US and Australia,
during the period from 1972 to 1968, in Colombia in 1994, and in
Malaysia in 1997 (9). Whereas the
genotype C was predominant in east Asia, particularly in mainland
China and Vietnam (11,19,20).
Based on phylogenetic analysis, the EV71 strains identified in this
study belong to the subgenotype C4 and show high homology with
isolates from 3 representative provinces of the mainland China.
Notably, the result was consistent with previous studies (7,20).
The C4 subgenotype of EV71 has been in continuous circulation for
at least 10 years since the first reported occurrence in ShenZhen
city in 1998 (11).
The prototype G-10 strain of CVA16, first isolated
in South Africa in 1951, is the sole member of genotype A (10). The genotype B can be further
divided into 2 subgenotypes (B1, B2). CVA16 strains isolated in
mainland China and the majority of international countries from
1981 to 2000 were all members of subgenotype B1. Since 1997,
subgenotype B1 has gradually been replaced by subgenotypes B2, and
CVA16 from clusters B2a and B2b has become the predominant virus
circulating in mainland China and in neighboring countries to date
(13). Based on phylogenetic
analysis, the majority of CVA16 strains detected in the present
study belong to clusters B2a and B2b, which was consistent with a
previous study (13). Briefly, the
genotypes of CVA16 identified in their study were similar to those
detected in other Chinese provinces and countries. In addition, the
other 2 CAV16 strains formed a new cluster distinct from genotype A
and B, which indicated that CAV16 circulating in Zhejiang Province
of China was genetically diverse and additional surveillance is
necessary.
In conclusion, our study reveals that genetic
characteristics of enteroviruses in China since 1998, reflect the
pattern of endemic circulation of the subgenotype C4 to EV71 and
clusters B2a and B2b within the genotype B2 to CVA16. We hypothesis
that EV71 and CVA16 strains in China may derive from a respective
ancestor associated with special geographic and climatic features
allowing it to be sustained with little external effect. Therefore,
future investigation of the respective ancestor of EV71 and CVA16
strains in China is warranted in order to take effective measures
to prevent an HFMD outbreak.
Acknowledgements
This study was funded by grants from the National
Basic Research Program of China (973 program) no. 2007CB513001,
China's National Science and Technology Major Project no.
2008ZX10002-009, and a Qiu Shi Professorship from Zhejiang
University to C.X. The authors thank Michael Brownstein for his
critical reading of our manuscript.
References
|
1
|
T YamashitaM ItoA TaniguchiK
SakaePrevalence of coxsackievirus A5, A6, and A10 in patients with
herpangina in Aichi Prefecture, 2005Jpn J Infect
Dis58390391200516377876
|
|
2
|
F YangJ DuY HuEnterovirus coinfection
during an outbreak of hand, foot and mouth disease in Shandong,
ChinaClin Infect Dis53400401201110.1093/cid/cir34621785005
|
|
3
|
P McMinnI StratovL NagarajanS
DavisNeurological manifestations of enterovirus 71 infection in
children during an outbreak of hand, foot and mouth disease in
Western AustraliaClin Infect
Dis32236242200110.1086/31845411170913
|
|
4
|
NJ SchmidtEH LennetteHH HoAn apparently
new enterovirus isolated from patients with disease of the central
nervous systemJ Infect
Dis129304309197410.1093/infdis/129.3.3044361245
|
|
5
|
H ShimizuA UtamaK YoshiiEnterovirus 71
from fatal and nonfatal cases of hand, foot and mouth disease
epidemics in Malaysia, Japan and Taiwan in 1997–1998Jpn J Infect
Dis521215199910808253
|
|
6
|
LY ChangTY LinYC HuangComparison of
enterovirus 71 and coxsackie-virus A16 clinical illnesses during
the Taiwan enterovirus epidemic, 1998Pediatr Infect Dis
J1810921096199910.1097/00006454-199912000-0001310608631
|
|
7
|
Y ZhangXJ TanHY WangAn outbreak of hand,
foot and mouth disease associated with subgenotype C4 of human
enterovirus 71 in Shandong, ChinaJ Clin
Virol44262267200910.1016/j.jcv.2009.02.00219269888
|
|
8
|
YP HuangTL LinCY KuoThe circulation of
subgenogroups B5 and C5 of enterovirus 71 in Taiwan from 2006 to
2007Virus
Res137206212200810.1016/j.virusres.2008.07.01518706461
|
|
9
|
BA BrownMS ObersteJP Alexander JrML
KennettMA PallanschMolecular epidemiology and evolution of
enterovirus 71 strains isolated from 1970 to 1998J
Virol7399699975199910559310
|
|
10
|
D PereraMA YusofY PodinMolecular phylogeny
of modern coxsackievirus A16Arch
Virol15212011208200710.1007/s00705-006-0934-517308978
|
|
11
|
L LiY HeH YangGenetic characteristics of
human enterovirus 71 and coxsackievirus A16 circulating from 1999
to 2004 in Shenzhen, People's Republic of ChinaJ Clin
Microbiol4338353839200510.1128/JCM.43.8.3835-3839.200516081920
|
|
12
|
M IwaiA MasakiS HasegawaGenetic changes of
coxsackievirus A16 and enterovirus 71 isolated from hand, foot and
mouth disease patients in Toyama, Japan between 1981 and 2007Jpn J
Infect Dis62254259200919628900
|
|
13
|
W ZongY HeS YuMolecular phylogeny of
coxsackievirus A16 in Shenzhen, China, from 2005 to 2009J Clin
Microbiol4916591661201110.1128/JCM.00010-1121325543
|
|
14
|
WA NixMS ObersteMA PallanschSensitive,
seminested PCR amplification of VP1 sequences for direct
identification of all enterovirus serotypes from original clinical
specimensJ Clin
Microbiol4426982704200610.1128/JCM.00542-0616891480
|
|
15
|
K TamuraJ DudleyM NeiS KumarMEGA4:
Molecular Evolutionary Genetics Analysis (MEGA) software version
4.0Mol Biol Evol2415961599200710.1093/molbev/msm09217488738
|
|
16
|
LY ChangYC HuangTY LinFulminant neurogenic
pulmonary oedema with hand, foot and mouth
diseaseLancet352367368199810.1016/S0140-6736(98)24031-19717926
|
|
17
|
LC LumKT WongSK LamKB ChuaAY GohNeurogenic
pulmonary oedema and enterovirus 71
encephalomyelitisLancet3521391199810.1016/S0140-6736(05)60789-19802304
|
|
18
|
JR WangYC TuanHP TsaiJJ YanCC LiuIJ
SuChange of major genotype of enterovirus 71 in outbreaks of hand,
foot and mouth disease in Taiwan between 1998 and 2000J Clin
Microbiol401015200210.1128/JCM.40.1.10-15.200211773085
|
|
19
|
PV TuNT ThaoD PereraEpidemiologic and
virologic investigation of hand, foot and mouth disease, Southern
Vietnam, 2005Emerg Infect
Dis1317331741200710.3201/eid1311.07063218217559
|
|
20
|
Y ZhangZ ZhuW YangAn emerging recombinant
human enterovirus 71 responsible for the 2008 outbreak of hand,
foot and mouth disease in Fuyang City of ChinaVirol
J794201010.1186/1743-422X-7-9420459851
|