Introduction
The chronic venous leg ulcer (CVLU) is a severe
complication of venous insufficiency that is common worldwide.
Besides the significant social and economical load, CVLU is
currently recognized as a serious public health problem that
affects 5–8% of individuals above the age of 65 years (1). Therefore, the improvement of the
effectiveness of chronic leg ulceration treatment is of great
importance.
CVLU is characterized by a chronic inflammatory
reaction that involves the wound bed with surrounding skin and
subcutaneous tissue. Chronic inflammation involves an incessant
recruitment and activation of immune cells that is associated with
the secretion of various mediators of inflammation, including
cytokines, phospholipid metabolites, endogenous amines, free
radicals and proteolytic enzymes, particularly matrix
metalloproteinases (MMPs). They may all contribute to the extensive
destruction of affected tissues but may also impair the process of
healing (2,3). Therefore, it is clear that the shift
of balance between the damage and healing of tissue towards the
stimulation of repair should be considered as a key target for the
successful treatment of CVLU. Notably, several studies as well as
our recent one, suggest that an attractive solution to this issue
may be the use of biological dressings prepared from the amniotic
membrane (4,5).
The amnion is the innermost layer of the fetal
membranes that surround the amniotic cavity and protect the embryo.
It is covered by cuboidal epithelial cells, which produce numerous
factors that may promote cell proliferation and/or migration. The
amniotic membrane contains large amounts of hyaluronan polymer,
which is known to accelerate the regeneration of damaged tissue and
thus may facilitate wound healing (6). Therefore, the amnion is used as a
dressing material, mainly in ocular surgery, but also as a
substitute for pleura and pericardium, and in severe skin burns
treatment. As mentioned previously, the amniotic membrane has also
been used in the treatment of venous ulceration.
The use of fresh amnion is limited by its
availability. Due to the possible biohazard it should be subjected
to time-consuming microbiological tests, which are also associated
with the serological screening of donors. Therefore, various
procedures for the preparation and sterilization of amnion have
been developed. This processing may affect the biological
properties of the amnion dressing and impair its clinical
usefulness (7,8). However, findings of our recent study
have shown that irradiation-sterilized, deep frozen amniotic
membrane retained significant biological activity and effectively
stimulated the proliferation of HaCaT keratinocytes in vitro
(5). The aim of the present study
was to verify this finding clinically. Thus, we assessed whether
radiation-sterilized amnion dressing was able to improve the
healing of hard-to-treat venous leg ulcers. Furthermore, we
attempted to explain the possible mechanism of its action.
Materials and methods
Patients
The study involved 25 patients (16 women and 9 men,
mean age 76.3±12 years) with CVLU (C6 according to the CEAP
classification), attending the outpatient phlebology clinic
(Centrum Flebologii, Warsaw, Poland).
Inclusion in the clinical experiment required the
presence of a chronic wound (for a period of >6 months) with a
surface area of 10–100 cm2, with evident venous
insufficiency etiology, further confirmed by a Duplex-Doppler
ultrasound examination, with delayed healing (healing rate
<10%/week) regardless of at least 2 weeks of treatment
(screening period) using a hydrocolloid dressing (Granuflex Extra
Thin; ConvaTec) and effective compression with short-stretch
bandages (Pütterbinde; Hartmann). The exclusion criteria comprised
evident signs of wound infection (odorous, purulent exudates, wound
necrosis and significant pain), active deep vein thrombosis, leg
ischemia with ankle/brachial index <0.8, poor tolerance of
compression, pregnancy, diabetes and other systemic diseases
(particularly significant heart insufficiency) in unstable stage
and malignancy.
All individuals gave their informed consent to
participate in the study, which was approved by the local ethics
committee.
Amnion dressing application
The amniotic membrane specimens were obtained from
the National Center of Tissue and Cell Banking, at the Center of
Biostructure of the Medical University of Warsaw. The entire
preparation procedure, including epidemiological screening and
sterilization by irradiation with an accelerated electron beam, has
been described in detail elsewhere (9). The dressings were stored at −70°C
until use.
The amnion specimens were thawed immediately prior
to use, applied directly onto the wound bed and covered by a
secondary hydrocolloid dressing, followed by standard compression
with short-stretch bandages. The dressings were changed once per
week, however, in case of large exudates the outer wet dressing
layers were changed when necessary.
The clinical assessment of wounds was carried out 2
weeks (−14 days) prior to the first application of the amnion
dressing, at the time of its first application (day 0±1) and then
following 4 weeks (day 28±1) of treatment. The overall wound
condition, including wound edges, granular tissue formation, amount
and appearance of exudate, symptoms of inflammation and
epithelialization rate, was assessed using a modified Bates-Jensen
questionnaire (B-JQ), with the maximal score (75 points)
corresponding to the worst wound condition and the minimal score
(15 points) corresponding to a completely healed wound. The wounds
were photographed and their surfaces were measured using the public
domain image processing software, ImageJ, developed at the National
Institutes of Health, USA (http://rsbweb.nih.gov/ij).
MMP assessment
Samples of wound exudates were collected on days 0
and 28, and centrifuged at 10,000 rpm. Supernatants were used for
quantitative gelatin/SDS zymography to assess the activities of
MMP-2 and MMP-9, according to the protocol described in detail
elsewhere (10).
To verify the putative effect of the amniotic
dressing on MMP activity, serial dilutions of amnion extracts were
incubated for 15 min with 50 ng/ml human recombinant MMP-2 or MMP-9
(purchased from R&D Systems, Minneapolis, MN, USA), which,
prior to use, were pre-activated with a 1 mM solution of
4-aminophenylmercuric acetate (Sigma-Aldrich, St. Louis, MO, USA),
according to the instructions provided by the manufacturer. A
fluorescein-labeled gelatin substrate (EnzCheck Gelatinase assay;
Invitrogen/Molecular Probes, Eugene, OR, USA) was then added to a
final concentration of 12 μg/ml and the mixture was incubated for
120 min at 37°C. The fluorescence of the sample was continuously
monitored using a ABI PRISM 7500 Real-Time PCR device (Applied
Biosystems, Foster City, CA, USA). The fluorescent substrate alone
was used as a negative control, whereas pre-activated MMP-2 and
MMP-9 with the fluorescent substrate but without amnion extracts,
served as the 100% enzyme activity reference.
Protein array
The proteomic analysis of three randomly selected
amnion specimens was performed using the Human Angiogenesis
Proteome Profiler (R&D Systems), according to the detailed
instructions provided by the manufacturer. Standardized amnion
extracts (200 μl) were prepared as described elsewhere (5), then mixed with a cocktail of
biotinylated detection antibodies and incubated overnight at 8°C,
with nitrocellulose membranes spotted with the respective capture
antibodies. Membranes were washed and incubated with
streptavidin-horseradish peroxidase conjugate, followed by
chemiluminescence detection reagent (ImmunoCruz Luminol Reagent,
Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA). The membranes
were then exposed to an X-ray film (Agfa-Geavert, Mortsel, Belgium)
for 15–30 min, to achieve an optimal signal intensity. The film was
scanned and the optical density of each analyzed spot was assessed
using GelWorks 2D software (UVP, Cambridge, UK).
Results
Clinical assessment
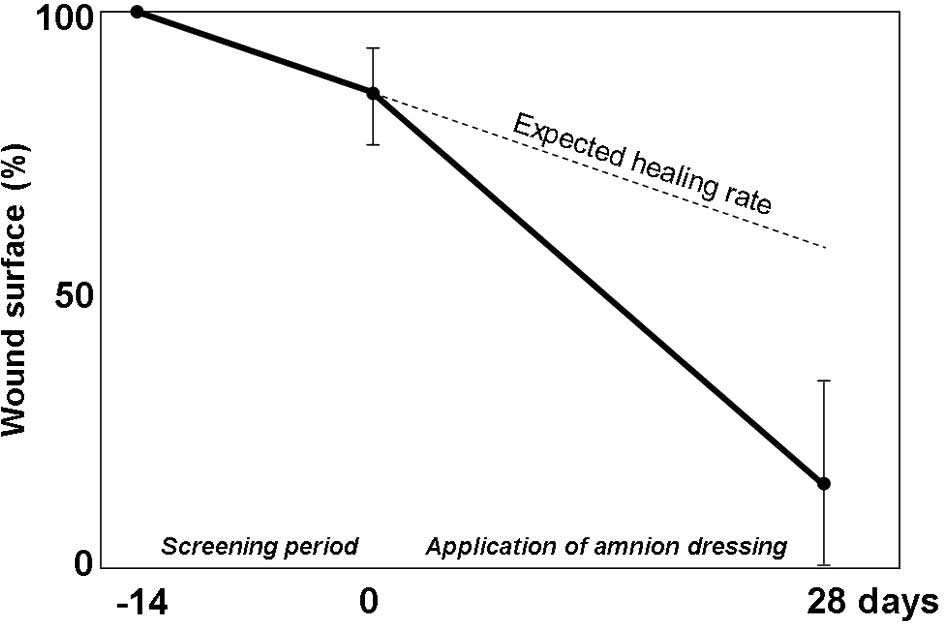
Despite a poor response to standard treatment in the
screening period, the application of amnion improved the overall
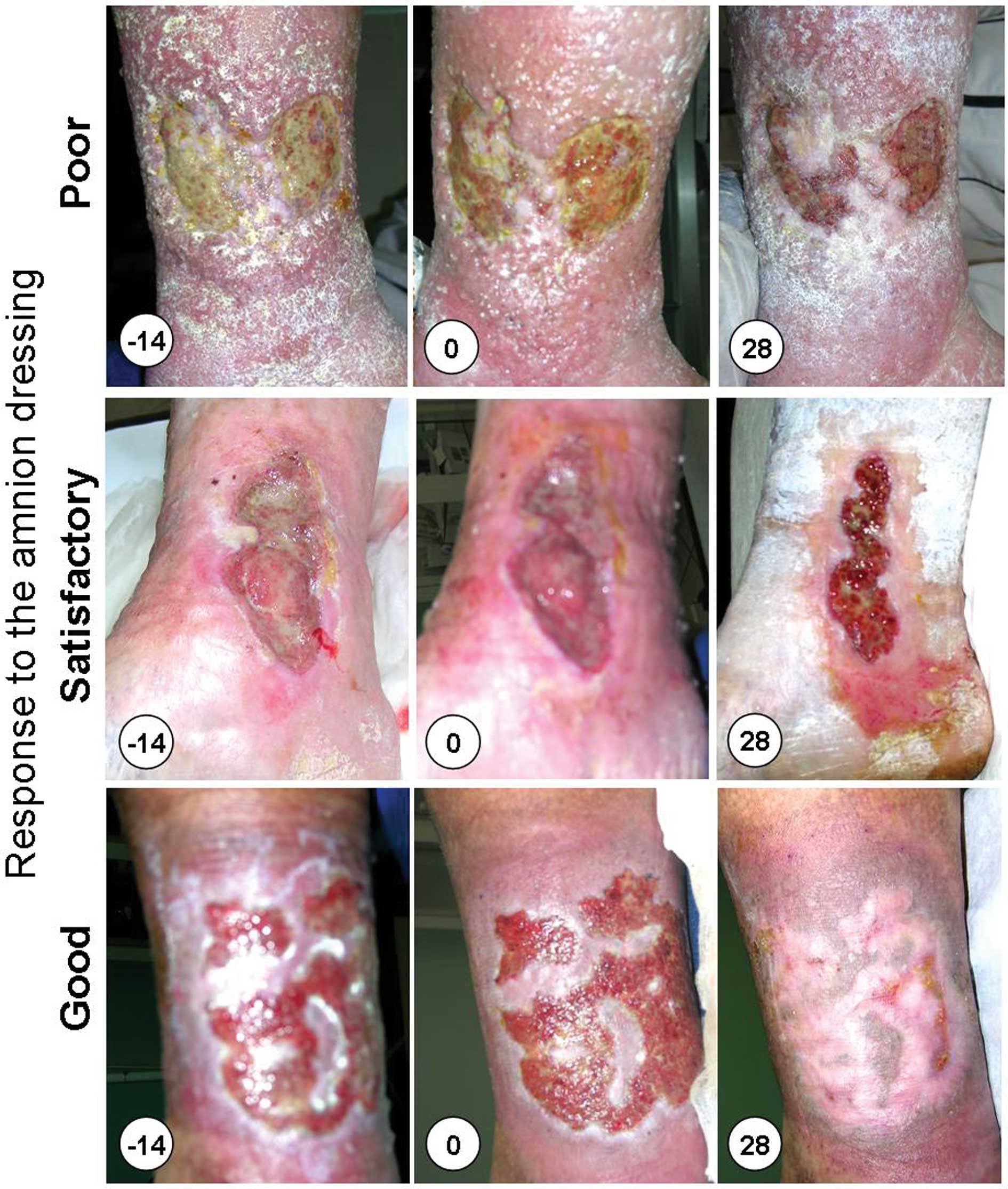
healing rate (Fig. 1). When
compared with the wound condition prior to the application of
amnion, the most notable differences in the amnion-treated wounds
concerned stimulation of granular tissue formation, less pronounced
irritation of the skin surrounding the wound by the ulcer exudates
and faster re-epithelialization (Fig.
2).
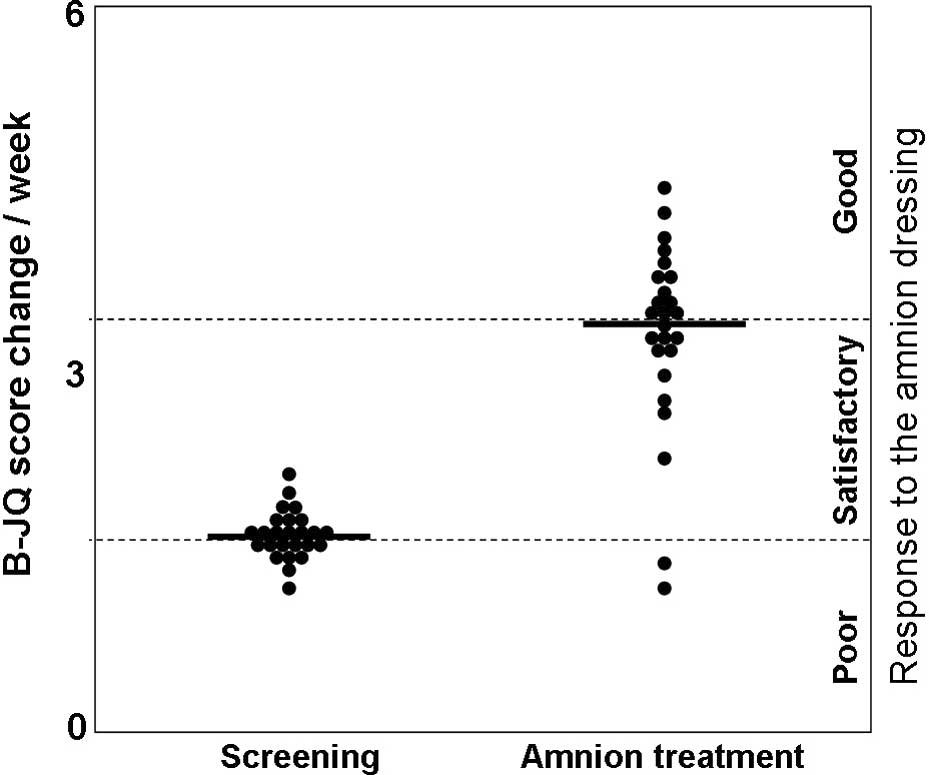
The use of a multi-factor assessment B-JQ score,
allowed a more reliable evaluation of the effectiveness of the
treatment and also enabled the comparison of various individuals.
With an arbitrary threshold corresponding to double the median B-JQ
score change observed in a screening period, it was found that
almost half of the patients (13 of 25) had a good response to the
treatment (B-JQ score change/week >3.5). A satisfactory response
was observed in another 10 individuals (B-JQ score change/week
1.7–3.5), whereas the 2 remaining patients responded poorly to the
treatment, with a B-JQ score change/week of <1.7, which was
similar to that during the screening period (Fig. 3).
MMP assessment
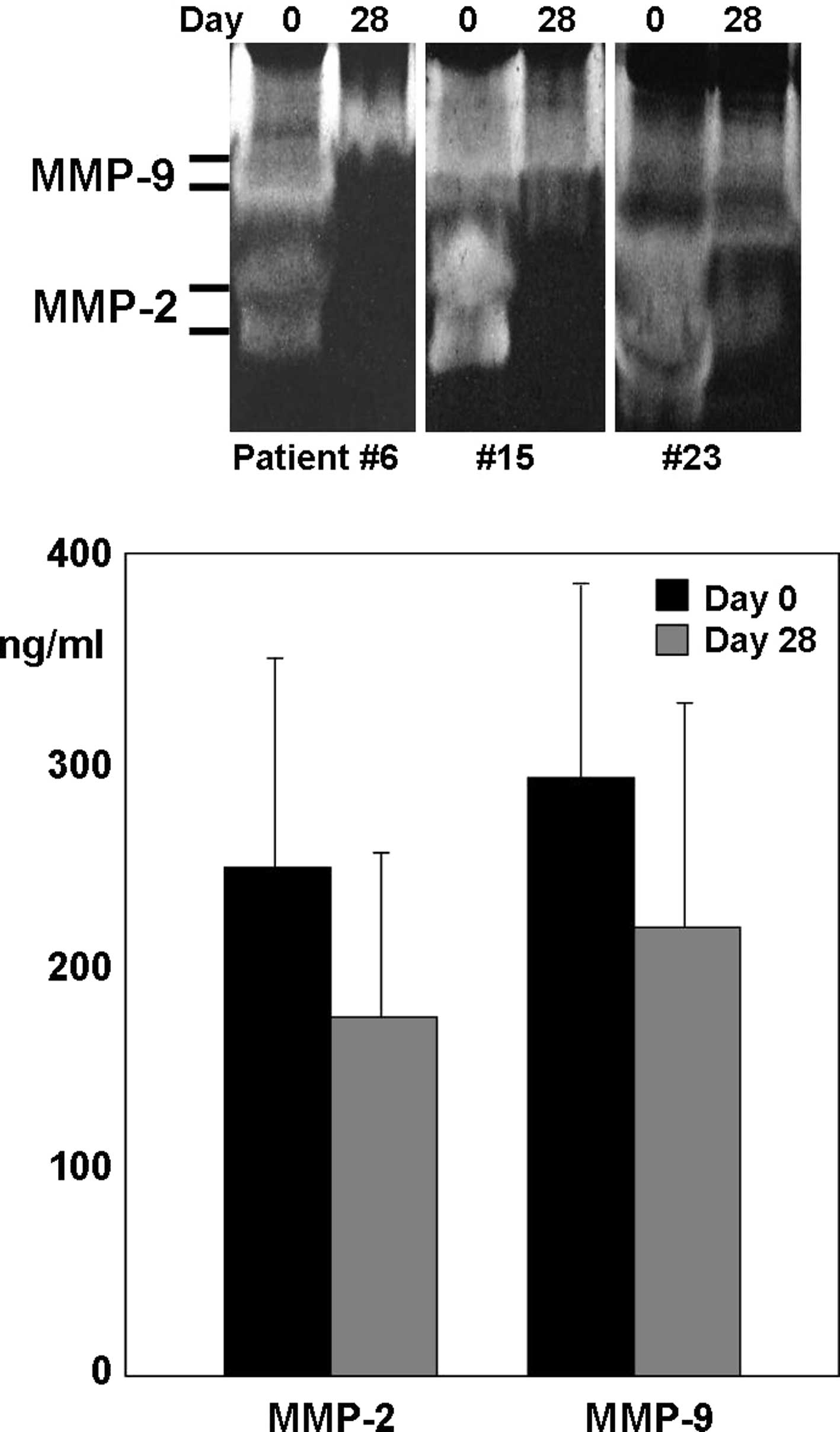
The quantitative SDS/substrate zymography revealed
significant activities of MMP-2 and MMP-9 in all analyzed exudate
samples. It was observed that the activities of the MMPs on day 0
were relatively high, with median levels of 251±101 ng/ml for MMP-2
and 293±96 ng/ml for MMP-9. The concentrations, measured on day 28,
were lower than those on day 0 (median 178±84 and 219±113 ng/ml,
respectively). Moreover, this difference appeared to be
statistically significant (Fig.
4).
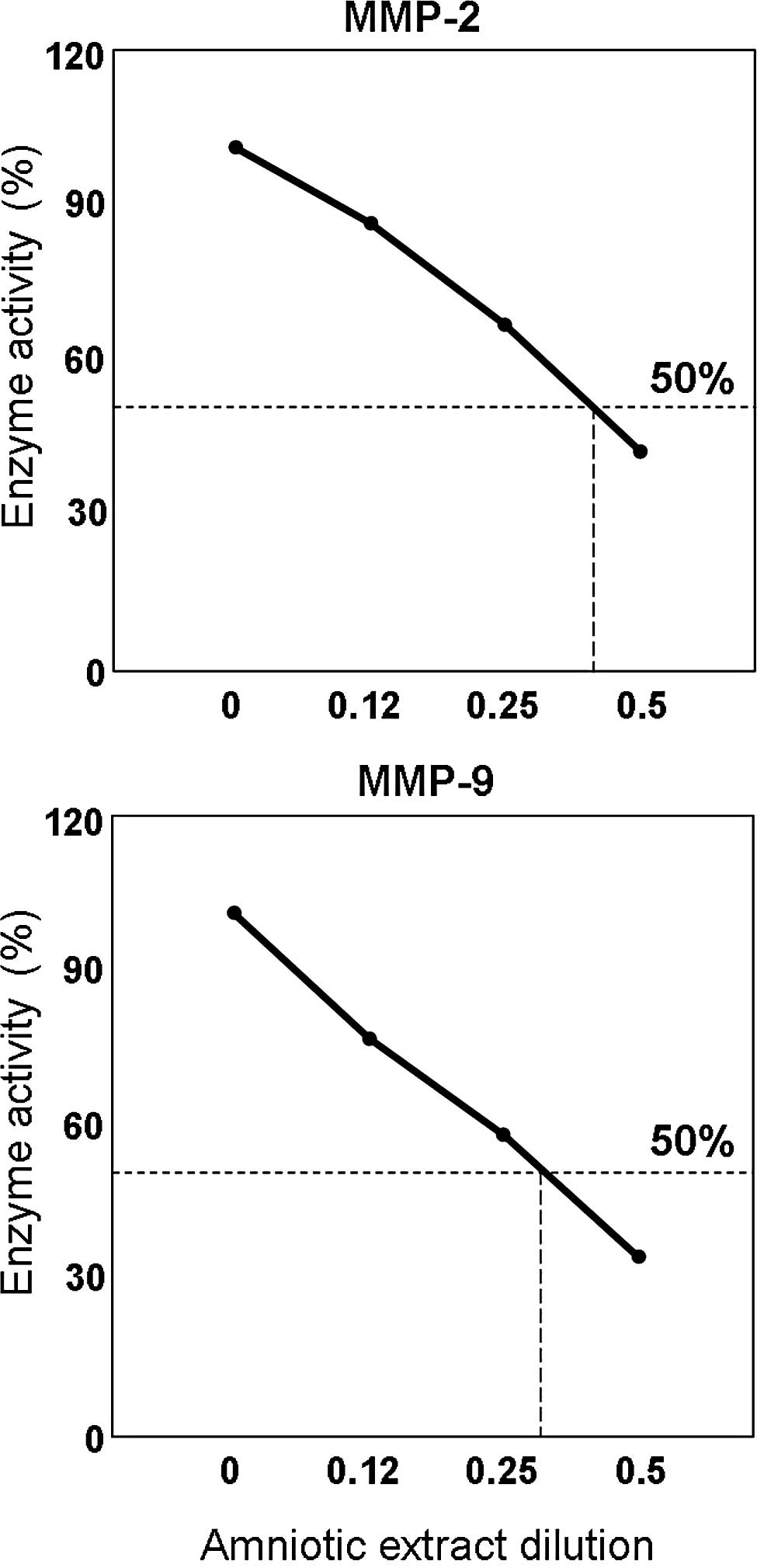
The MMP inhibition assay with fluorescein-labeled
gelatin, human amniotic membrane extracts and pre-activated
recombinant MMPs, revealed that the amnion extracts exhibited an
inhibitory effect on MMP-2 and MMP-9 activities in a
dilution-dependent manner. The dilution of the amniotic extract for
50% inhibitory activity of each MMP was calculated and was 0.4 for
MMP-2 and 0.32 for MMP-9 (Fig.
5).
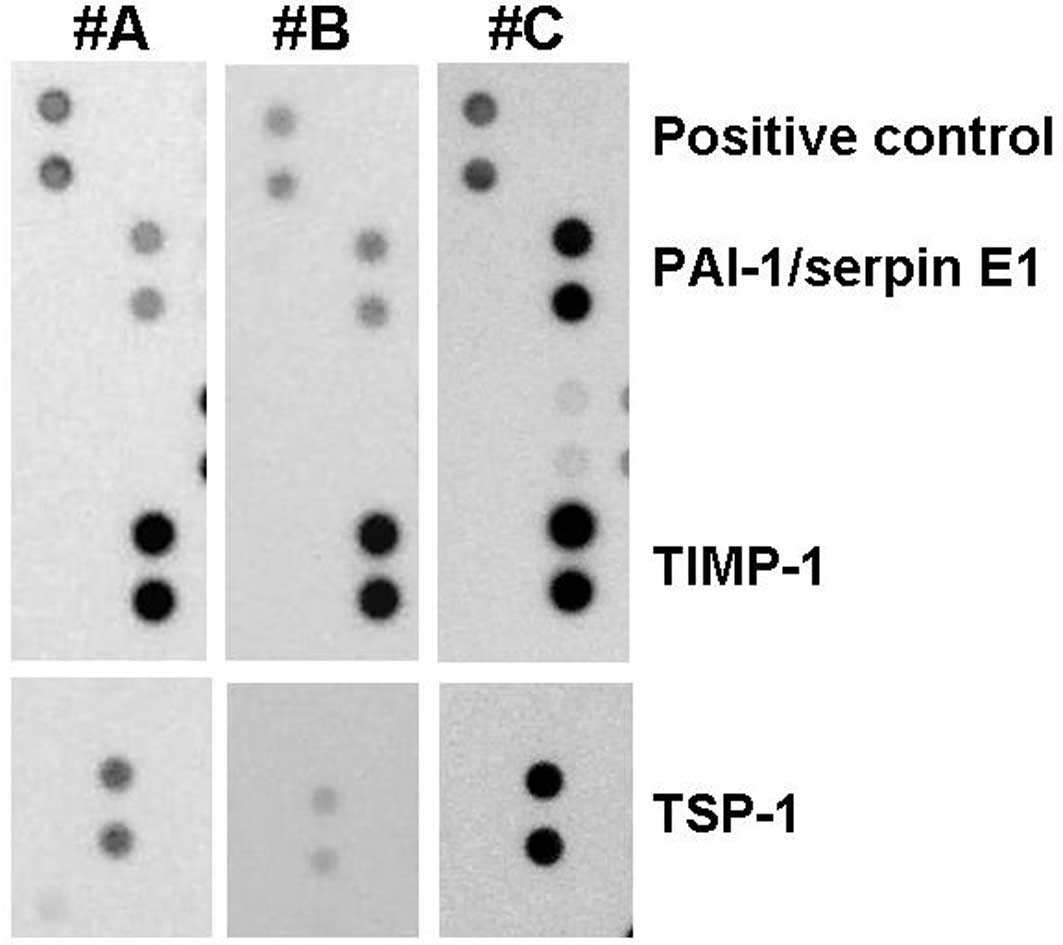
Protein array
The assessment of the amnion specimens using protein
microarray technology confirmed the presence of various cell growth
regulators. In addition, relatively large quantities of the tissue
inhibitor of metalloproteinases (TIMP)-1 and the type-1 plasminogen
activator inhibitor (PAI-1 or serpin E1) and less pronounced
amounts of another potent MMP inhibitor, thrombospondin (TSP)-1,
were detected (Fig. 6).
Discussion
Wound healing is a complex biological process,
comprising a series of consecutive events that aim to repair
injured tissue. It has been shown that any disturbances in the
sequence or duration of these events may result in the persistence
of the wound with a predominant chronic inflammatory reaction stage
(2,3). This result may be due to colonization
by bacteria, oxidative stress associated with repetitive
ischemia/reperfusion injury and/or impaired tissue response to the
stress conditions. Therefore, efforts have been undertaken to
improve the effectiveness of wound healing. These concern the
elimination of detrimental factors (e.g., bacterial load, tissue
ischemia or venous stasis), an attenuation of destructive
inflammatory hyper-response and/or induction and promotion of cell
proliferation, all of which may be achieved by providing a
supporting dressing and/or by exogenous stimulation with certain
growth factors. An attractive combination of both, a supporting
scaffold for cell growth (11,12)
and a rich source of various growth and differentiation factors,
could be the human amniotic membrane (5,7). As
reported by various authors, even preserved human amniotic membrane
contains a number of growth factors, including EGF, TGFα, TGFβ-1
and -2, KGF, HGF, bFGF, ANG and VEGF. These factors may enhance
epithelialization and suppress the inflammatory reaction, which is
beneficial for wound healing (4,8). In
addition to the aforementioned cytokines, high molecular weight
hyaluronan, a significant component of the amniotic membrane
dressing, has also revealed potent anti-inflammatory properties
(5,11).
Recent studies have shown that an excessive
expression and hyperactivation of MMPs, particularly MMP-2 and
MMP-9, may be important in the pathomechanism of delayed wound
healing. Although the two MMPs are crucial for the remodeling of
extracellular matrix and effective wound healing, when
overexpressed in affected tissue they act as potent injurious
factors (13). It has been shown
that increased MMP-9 activity correlates with the severity of the
ulcer (14), whereas during the
healing process the levels of MMP-9 in wound fluids decreased
relative to those observed in acute wounds (15). Therefore, the stabilization of the
wound environment through the inhibition of MMPs may be an
alternative option for effective chronic wound management.
In agreement with other reports (14,16),
we found that chronic wound exudates contained significant amounts
of MMP-2 and MMP-9. Notably, following 4 weeks of treatment with
the amniotic membrane, the MMP activity decreased, as identified by
SDS/gelatin zymography. This finding supports the hypothesis that
the inhibition/stabilization of MMPs is necessary for wound
healing. Moreover, the decrease in MMP activity may further
synergize with the previously mentioned beneficial properties of
amnion dressing, including possible immunosuppressive activity of
hyaluronan and the stimulatory role of various cytokines. It is
plausible that these mechanisms contribute equally to the
amnion-induced wound healing effect.
The results of SDS/gelatin zymography do not allow
us to discriminate between primarily active and artificially in
vitro-activated MMPs. In vitro activation may occur
during the contact of the latent form of the proenzyme with SDS in
the gelatin/polyacrylamide gel (17). Furthermore, the observed difference
in the activity of the MMPs, although statistically significant,
requires further verification in a larger patient group. The
standard SDS/gelatin zymography process does not enable any
monitoring of the presumed interaction between MMPs and their
inhibitors, therefore the investigation of this issue requires the
use of other methods. Thus, to clarify the potent anti-MMP
properties of the amniotic dressing, fluorescence real-time
zymography was used instead of the SDS/gelatin PAGE method. It was
found that amniotic membrane homogenates exerted a strong,
dose-dependent, inhibitory effect, directed against the
gelatinolytic activities of MMP-2 and MMP-9. The proteome analysis
of the amniotic membrane extracts using protein microarray
technology revealed the presence of significant amounts of three
potent protease inhibitors, TIMP-1, PAI-1 and TSP-1, in all
assessed samples. Although TIMP-1, a widely distributed natural
inhibitor for most of the known metalloproteinases (18), is the best known, it is plausible
that the remaining two factors may also contribute to the observed
inhibition of MMPs.
PAI-1/Serpin E1, primarily produced by endothelial
cells, is the principal inhibitor of two serine proteases, tissue
plasminogen activator (tPA) and urokinase (uPA), and is therefore a
suppressor of fibrinolysis. Studies focusing on the mechanism of
cancer metastasis have shown that PAI-1 may also exhibit an
inhibitory activity against MMPs (19,20).
TSP-1 was originally described as a natural
inhibitor of neovascularization. It has been shown to control
angiogenesis, particularly endothelial cell adhesion, motility and
growth, in both a positive and negative manner. Depending on the
particular domain involved in its action, TSP-1 interacts with a
number of cell receptors, adhesion molecules and proteases. TSP-1
has also been postulated to inhibit MMP-2 and MMP-9 activation
(21).
It is noteworthy that the protein array has revealed
certain differences in the amounts of TSP-1 and PAI-1 between
amnion samples prepared from various donations. It is plausible
that this is one of the explanations for the difference observed in
healing responses to the amnion dressing. However, to clarify this
issue it would be necessary to screen amnion dressing samples,
e.g., using a protein array system, prior to their clinical
application.
Taken together, our previous study and the present
study have demonstrated that radiation-sterilized amniotic membrane
dressing exerts a beneficial effect on chronic wounds. In addition
to the growth and differentiation factor-dependent stimulation of
wound healing or the immunosuppressive properties of high molecular
weight hyaluronan, amnion dressings may also restore the tissue
degradation/regeneration homeostasis by inhibiting MMPs. Therefore,
despite the large number of modern dressing materials developed
thus far, there is no synthetic dressing with such complex and
multidirectional activities as have been revealed for the amniotic
membrane.
References
|
1
|
MacKenzie RK, Brown DA, Allan PL, Bradbury
AW and Ruckley CV: A comparison of patients who developed venous
leg ulceration before and after their 50th birthday. Eur J Vasc
Endovasc Surg. 26:176–178. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mustoe TA, O’Shaughnessy K and Kloeters O:
Chronic wound pathogenesis and current treatment strategies: a
unifying hypothesis. Plast Reconstr Surg. 117:S35–S41. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Litwiniuk M, Grzela T and
Brawura-Biskupski-Samaha R: Clinical Immunology: Chronic
inflammation in venous leg ulcer - problems and perspectives. Centr
Eur J Immunol. 34:247–251. 2009.
|
|
4
|
Tauzin H, Humbert P, Viennet C, Saas P and
Muret P: Human amniotic membrane in the management of chronic
venous leg ulcers. Ann Dermatol Venereol. 138:572–579.
2011.PubMed/NCBI
|
|
5
|
Litwiniuk M, Bikowska B, Niderla-Bielińska
J, JóŸwiak J, Kamiński A, Skopiński P and Grzela T: High molecular
weight hyaluronan and stroma-embedded factors of
radiation-sterilized amniotic membrane stimulate proliferation of
HaCaT cell line in vitro. Centr Eur J Immunol. 36:205–211.
2011.
|
|
6
|
Jiang D, Liang J and Noble PW: Hyaluronan
in tissue injury and repair. Ann Rev Cell Dev Biol. 23:435–461.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wolbank S, Hildner F, Redl H, van
Griensven M, Gabriel C and Hennerbichler S: Impact of human
amniotic membrane preparation on release of angiogenic factors. J
Tissue Eng Regen Med. 3:651–654. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Russo A and Bonci P and Bonci P: The
effects of different preservation processes on the total protein
and growth factor content in a new biological product developed
from human amniotic membrane. Cell Tissue Bank. 13:353–361. 2012.
View Article : Google Scholar
|
|
9
|
Tyszkiewicz JT, Uhrynowska-Tyszkiewicz IA,
Kaminski A and Dziedzic-Goclawska A: Amnion allografts prepared in
the Central Tissue Bank in Warsaw. Ann Transplant. 4:85–90.
1999.PubMed/NCBI
|
|
10
|
Grzela T, Brawura-Biskupski-Samaha R,
Jelenska MM and Szmidt J: Low molecular weight heparin treatment
decreases MMP-9 plasma activity in patients with abdominal aortic
aneurysm. Eur J Vasc Endovasc Surg. 35:159–161. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Niknejad H, Peirovi H, Jorjani M,
Ahmadiani A, Ghanavi J and Seifalian AM: Properties of the amniotic
membrane for potential use in tissue engineering. Eur Cell Mater.
15:88–99. 2008.PubMed/NCBI
|
|
12
|
Chem PL, Baum CL and Arpey CJ: Biologic
dressings: current applications and limitations in dermatologic
surgery. Dermatol Surg. 35:891–906. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bjarnsholt T, Kirketerp-Moller, Jensen P,
et al: Why chronic wounds will not heal: a novel hypothesis. Wound
Repair Regen. 16:2–10. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rayment EA, Upton Z and Shooter GK:
Increased matrix metalloproteinase-9 (MMP-9) activity observed in
chronic wound fluid is related to the clinical severity of the
ulcer. Br J Dermatol. 158:951–961. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wysocki AB, Kusakabe AO, Chang S and Tuan
TL: Temporal expression of urokinase plasminogen activator,
plasminogen activator inhibitor and gelatinase-B in chronic wound
fluid switches from a chronic to acute wound profile with
progression to healing. Wound Rep Reg. 7:154–165. 1999. View Article : Google Scholar
|
|
16
|
Saito S, Trovato MJ, You R, et al: Role of
matrix metalloproteinases 1, 2, and 9 and tissue inhibitor of
matrix metalloproteinase-1 in chronic venous insufficiency. J Vasc
Surg. 34:930–938. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Grzela T, Bikowska B and Litwiniuk M:
Matrix metalloproteinases in aortic aneurysm - executors or
executioners? Etiology, Pathogenesis and Pathophysiology of Aortic
Aneurysms and Aneurysm Rupture. Grundmann R: Intech Publ; pp.
25–54. 2011, Available from: http://www.intechopen.com/articles/show/title/matrix-metalloproteinases-in-aortic-aneurysm-executors-or-executioners-.
|
|
18
|
Fu X, Parks WC and Heinecke JW: Activation
and silencing of matrix metalloproteinases. Semin Cell Dev Biol.
19:2–13. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Suzuki K, Nakayama H and Doi K: Kinetics
of matrix metalloproteinases and their regulatory factors in
mercuric chloride-induced tubulointerstitial fibrosis in Brown
Norway rats. Exp Toxic Pathol. 53:337–343. 2001. View Article : Google Scholar
|
|
20
|
Duffy M: The urokinase plasminogen
activator system: role in malignancy. Curr Pharm Des. 10:39–49.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bein K and Simons M: Thrombospondin type 1
repeats interact with matrix metalloproteinase 2. Regulation of
metalloproteinase activity. J Biol Chem. 275:32167–32173. 2000.
View Article : Google Scholar : PubMed/NCBI
|